
Abstract
Objectives:
Information on the impact of health insurance on smoking and quit attempts at the state level is limited. We examined the state-specific prevalence of cigarette smoking and past-year quit attempts among adults aged 18-64 by health insurance and other individual- and state-level factors.
Methods:
We used data from 41 states, the District of Columbia, and Puerto Rico, the jurisdictions that administered the Health Care Access module of the 2014 Behavioral Risk Factor Surveillance System. Data on quit attempts included current smokers with a past-year quit attempt and former smokers who quit during the past year.
Results:
Overall, smoking prevalence ranged from 14.6% among those with private insurance to 34.7% among Medicaid enrollees, and past-year quit-attempt prevalence ranged from 66.4% among the uninsured to 71.5% among Medicaid enrollees. By insurance group, differences in the prevalence of state-specific past-year quit attempts ranged from 15 to 26 percentage points. Regardless of insurance type, people who were non-Hispanic white and had lower education levels were less likely to attempt quitting than were Hispanic people, non-Hispanic black people, and adults with more than a high school education.
Conclusions:
We found disparities in smoking and quit attempts by insurance status and state. Opportunities exist to increase access to cessation treatments through comprehensive state tobacco control programs and improved cessation insurance coverage, coupled with promotion of covered cessation treatments.
Despite longstanding declines in cigarette smoking prevalence, smoking is the leading preventable cause of morbidity and mortality in the United States. Quitting smoking has immediate and long-term health benefits and yields health care cost savings. 1 Smokers who quit by age 40 reduce the excess risk of death associated with continued smoking by about 90%. 2 In 2015, more than half (55.4%) of US adult cigarette smokers reported making a quit attempt during the past year. 3 Healthy People 2020 objective TU-4.1 calls for increasing the proportion of US adult cigarette smokers who made a quit attempt during the past year to 80%. 4
Individual, group, and telephone cessation counseling and 7 US Food and Drug Administration (FDA)–approved cessation medications are effective in increasing quit rates. 5 Health insurance coverage of these treatments increases quit attempts, treatment use, and successful cessation. 5,6 Coverage of these treatments and barriers to accessing these treatments (eg, cost sharing and prior authorization) vary by type of health insurance, making insurance type an important correlate of cessation. 7,8 In 2015, smoking prevalence was significantly higher among adult Medicaid enrollees (27.8%) and uninsured adults (27.4%) than among adults with private health insurance (11.1%). 9 In contrast, no difference in interest in quitting and prevalence of past-year quit attempt was observed in 2015 between adult smokers enrolled in Medicaid and smokers with private health insurance. 3
Although several studies have examined state-specific prevalence of smoking and quit attempts, 10,11 data on the prevalence of cigarette smoking and quit attempts by insurance status at the state level are limited. We used data from the 2014 Behavioral Risk Factor Surveillance System (BRFSS) to estimate state-specific prevalence of cigarette smoking and quit attempts for 41 states, the District of Columbia, and Puerto Rico for people with Medicaid insurance, private health insurance, and no health insurance. Findings from this analysis could help inform state-level efforts to help smokers quit.
Methods
Data Source
The BRFSS is a random-digit-dial annual telephone survey of the noninstitutionalized civilian US population aged ≥18. 12 The BRFSS is conducted in all 50 states, the District of Columbia, Guam, Puerto Rico, and the US Virgin Islands. In 2014, 41 states, the District of Columbia, and Puerto Rico administered an optional Health Care Access (HCA) module in addition to the core BRFSS survey questionnaire. The HCA module included questions on health care coverage, access, affordability, and use. Response rates for the 2014 BRFSS ranged from 30.2% to 61.6% for the 41 states in this study, the District of Columbia, and Puerto Rico. 12
The study sample included 235 741 adults from 41 states, the District of Columbia, and Puerto Rico. We excluded adults aged ≥65 because most of them are covered by Medicare, a federal program that does not vary across states with regard to coverage of cessation treatments. 13 We did not conduct separate analyses by other types of insurance (Tricare, Veterans Administration, military, Alaska Native, Indian Health Service, Tribal Health Services) because estimates for these insurance types could not be generated for all states due to small numbers. Because this study used publicly available, deidentified secondary data, human subjects review did not apply.
Measures
We determined smoking status by using 2 questions from the survey: (1) “Have you smoked at least 100 cigarettes in your entire life?” and (2) “Do you now smoke cigarettes every day, some days, or not at all?” We classified adults who reported smoking ≥100 cigarettes during their lifetime and now smoking every day or some days as current smokers. Adult smokers included current smokers and former smokers (adults who reported smoking ≥100 cigarettes during their lifetime but not smoking currently) who quit during the past year.
Past-year quit attempts included both current smokers who reported a quit attempt during the past year and former smokers who quit during the past year. We defined a past-year quit attempt among current smokers as an affirmative answer to the question, “During the past 12 months, have you quit smoking for 1 day or longer because you were trying to quit smoking?” We assessed a past-year quit attempt among former smokers through the question, “How long has it been since you last smoked a cigarette, even 1 or 2 puffs?” We categorized those who responded that they last smoked during the past 12 months as former smokers with a past-year quit attempt.
We classified insurance status as private health insurance, Medicaid/state, or uninsured based on information from 2 questions: (1) “Do you have any kind of health care coverage, including health insurance, prepaid plans such as health maintenance organizations, or government plans such as Medicare or Indian Health Service?” We classified those who answered no as uninsured. Those who answered yes were asked the second question: (2) “What is the primary source of your health care coverage?” Response options included “a plan purchased through an employer or union (includes plans purchased through another person’s employer)” or “a plan that you or another family member buys on your own,” classified as private; “Medicaid or other state program,” classified as Medicaid/state; and “None (no coverage),” classified as uninsured.
Other individual-level variables included sex (male/female), age (18-24, 25-44, and 45-64), education (<high school education, high school education, >high school education), and race/ethnicity (Hispanic, non-Hispanic white, non-Hispanic black, and non-Hispanic other).
Because we examined only 1 year of data for this analysis, we controlled for state-level variations using the following variables: 2014 per-capita appropriations for state tobacco control programs,14 2014 state cigarette excise tax rates, 15 and percentage of state population covered by comprehensive state or local smoke-free laws. 16 We also included a state Medicaid expansion status variable. For this variable, we divided states into 3 categories: (1) states that expanded Medicaid eligibility before the beginning of 2014, (2) states that expanded eligibility during 2014, and (3) states that had not expanded eligibility by the end of 2014. 17
Statistical Analysis
We performed all statistical analyses by using SAS-callable SUDAAN, 18 which accounts for the complex survey design of the BRFSS. We weighted estimates to account for individual selection probabilities, nonresponse, and post-stratification. We calculated overall and insurance status-specific estimates of prevalence of current smoking and past-year quit attempts for adults aged 18-64 for all 41 states, the District of Columbia, and Puerto Rico. We used overall prevalence of current smoking and classified state current smoking prevalence into 4 groups using the following quartiles: ≤17.8%, 17.9% to 20.1%, 20.2% to 23.8%, and >23.8%. We used quartiles to create 4 state maps for current smoking prevalence, overall and for each insurance type. We then examined the distributions of demographic characteristics among cigarette smokers (including current smokers and former smokers who quit during the past year, hereinafter referred to as smokers) overall and by type of insurance. We used the χ 2 test of independence, Cochran-Mantel-Haenszel, and Wald F tests to assess significance, with P < .05 considered significant. Because we found that insurance was strongly associated with past-year quit attempts in the preliminary analysis, we used 3 multivariate logistic regression models in the final analysis to examine the relationship between the 3 insurance types and past-year quit attempts among smokers, adjusting for individual sociodemographic characteristics and state-level variables. We did not include state fixed effects in the model because including both state fixed effects and state-level covariates would lead to multicollinearity. We conducted sensitivity analyses and replaced all state-level variables with state fixed effects to control for contextual factors at the state level.
Results
In 2014, the prevalence of current cigarette smoking among adults aged 18-64 varied widely across the 41 states, the District of Columbia, and Puerto Rico, from 10.5% in Utah to 30.7% in West Virginia. Among the 43 states and jurisdictions, the combined smoking prevalence was 34.7% among Medicaid enrollees, 32.5% among adults with no insurance, and 14.6% among adults with private insurance, and all prevalences were significantly different from each other (P < .001).
Among adults with private insurance, smoking prevalence was in the third quartile in only 2 states (Kentucky and West Virginia), and none of the states had smoking prevalence in the fourth quartile (Figure 1). In contrast, among adults enrolled in Medicaid and uninsured adults, smoking prevalence was in the fourth quartile for 41 states and jurisdictions (all except New Jersey and Puerto Rico) and 37 states and jurisdictions (all except the District of Columbia, Illinois, Maryland, New York, Puerto Rico, and Utah), respectively.
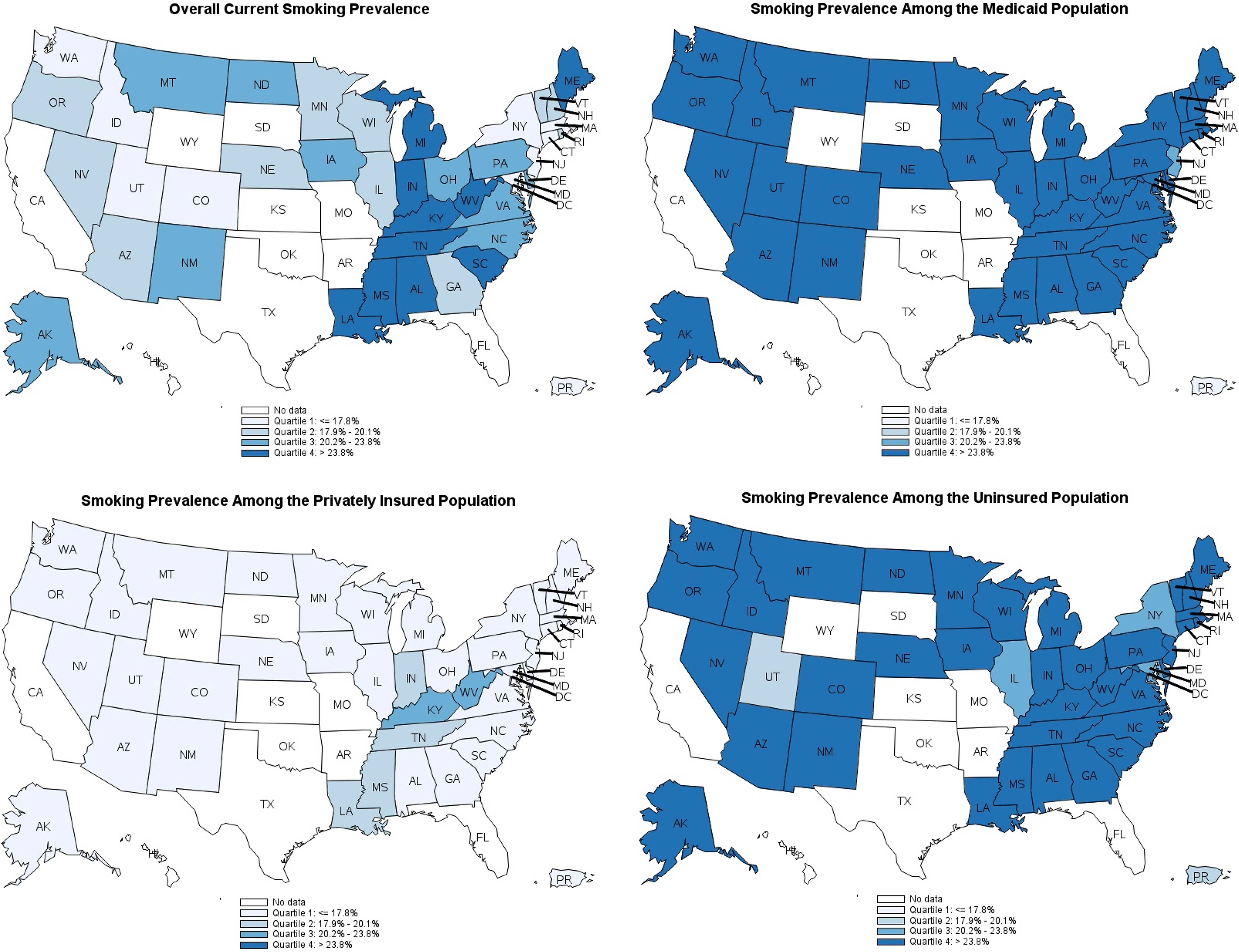
Quartiles of cigarette smoking prevalence among adults aged 18-64, by health insurance coverage, Behavioral Risk Factor Surveillance System (BRFSS) 2014,12 41 states, the District of Columbia, and Puerto Rico. Quartiles were determined by using the overall state smoking prevalence; the same quartiles were then used for the insurance-specific state smoking prevalence. People who smoked ≥100 cigarettes in their lifetime and currently smoked every day or some days were considered current smokers. No data were available from states that did not administer the Health Care Access module in the BRFSS.
Overall, among cigarette smokers in the 43 states and jurisdictions examined, we found variations in demographic characteristics by type of health insurance (Table 1). Compared with privately insured smokers, a higher proportion of uninsured smokers and smokers enrolled in Medicaid were aged 25-44, were Hispanic and non-Hispanic black, and had <high school education. Compared with privately insured and uninsured smokers, a higher proportion of smokers enrolled in Medicaid were women; in contrast, compared with privately insured smokers and smokers enrolled in Medicaid, a higher proportion of uninsured smokers were men.
Demographic characteristics of adult cigarette smokersa aged 18-64, by health insurance coverageb: 41 states, the District of Columbia, and Puerto Rico, Behavioral Risk Factor Surveillance System 201412
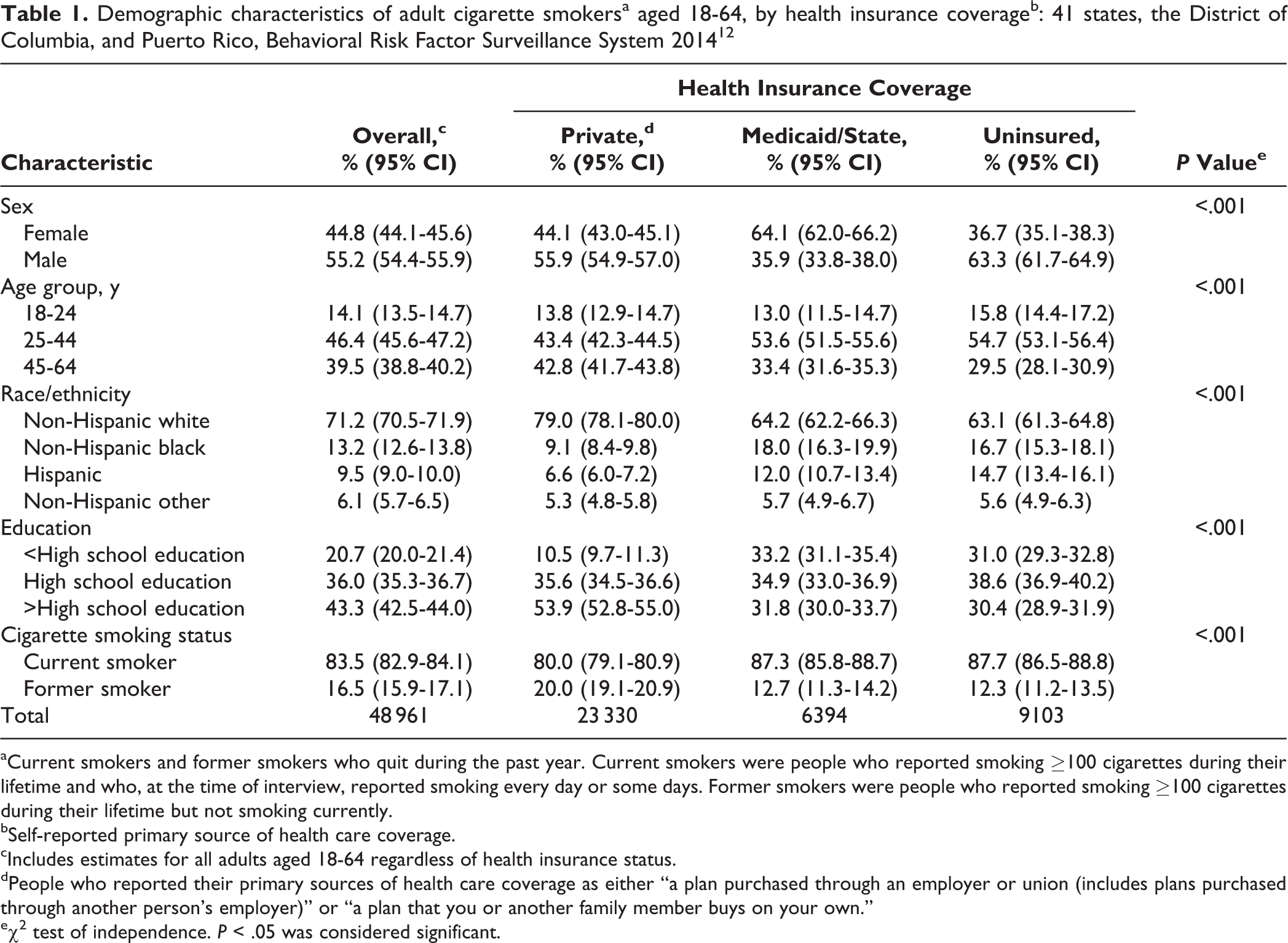
aCurrent smokers and former smokers who quit during the past year. Current smokers were people who reported smoking ≥100 cigarettes during their lifetime and who, at the time of interview, reported smoking every day or some days. Former smokers were people who reported smoking ≥100 cigarettes during their lifetime but not smoking currently.
bSelf-reported primary source of health care coverage.
cIncludes estimates for all adults aged 18-64 regardless of health insurance status.
dPeople who reported their primary sources of health care coverage as either “a plan purchased through an employer or union (includes plans purchased through another person’s employer)” or “a plan that you or another family member buys on your own.”
eχ 2 test of independence. P < .05 was considered significant.
Across the 41 states, the District of Columbia, and Puerto Rico, cigarette smokers enrolled in Medicaid (71.5%) had a significantly higher prevalence of having a past-year quit attempt than privately insured (67.9%) or uninsured (66.4%) smokers (P < .001). We found wide variations in state-specific quit-attempt prevalence by insurance group. The difference in state-specific past-year quit-attempt prevalence was smallest for private insurance (ranging from 59.6% in West Virginia to 74.8% in Georgia, for a difference of 15.2 percentage points); was 21.1 percentage points for the Medicaid group (ranging from 59.4% in Maine to 80.5% in Ohio); and was largest (26.2 percentage points) for the uninsured group (ranging from 54.8% in Indiana to 81.0% in Massachusetts). State-specific analyses generally followed the same pattern as the overall analyses: smokers with Medicaid had a higher prevalence of past-year quit attempts compared with both privately insured and uninsured smokers in 28 of 41 states and jurisdictions; however, this difference was significant only in Indiana (P = .03) and Ohio (P = .002) (Table 2). Similarly, when we compared quit attempts among insured and uninsured smokers, uninsured smokers in 26 states had a lower prevalence of quit attempts than smokers insured by Medicaid or private insurance, and these differences were significant in 3 states: Indiana (P = .011), Massachusetts (P = .042), and Michigan (P = .02).
Prevalence of past-year quit attempts, by health insurance coverage,a among cigarette smokersb aged 18-64, 41 states, the District of Columbia, and Puerto Rico, Behavioral Risk Factor Surveillance System 201412
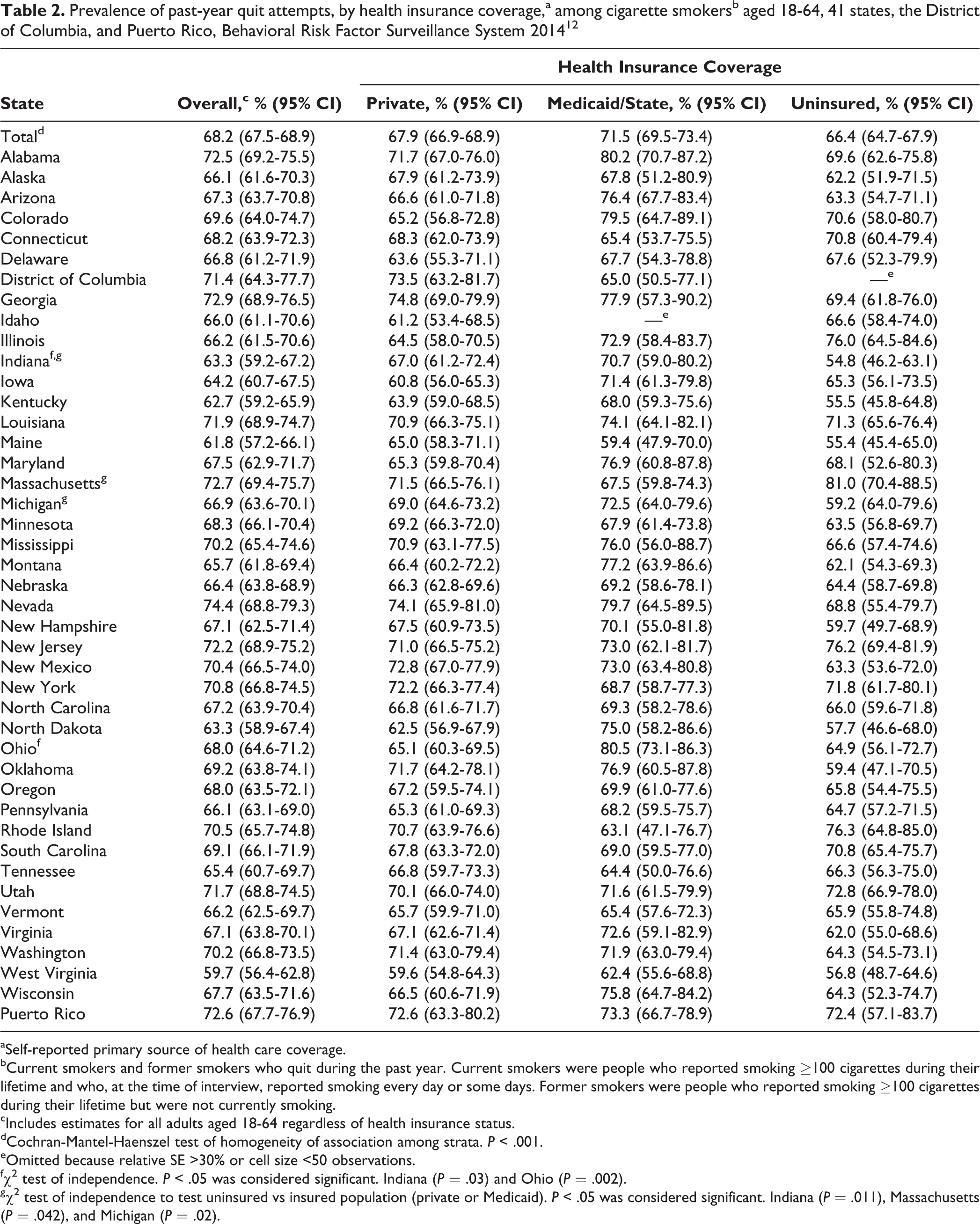
aSelf-reported primary source of health care coverage.
bCurrent smokers and former smokers who quit during the past year. Current smokers were people who reported smoking ≥100 cigarettes during their lifetime and who, at the time of interview, reported smoking every day or some days. Former smokers were people who reported smoking ≥100 cigarettes during their lifetime but were not currently smoking.
cIncludes estimates for all adults aged 18-64 regardless of health insurance status.
dCochran-Mantel-Haenszel test of homogeneity of association among strata. P < .001.
eOmitted because relative SE >30% or cell size <50 observations.
fχ 2 test of independence. P < .05 was considered significant. Indiana (P = .03) and Ohio (P = .002).
gχ 2 test of independence to test uninsured vs insured population (private or Medicaid). P < .05 was considered significant. Indiana (P = .011), Massachusetts (P = .042), and Michigan (P = .02).
Race/ethnicity and education were significant correlates across all 3 multivariate models. Non-Hispanic black and Hispanic smokers had significantly greater odds of making a past-year quit attempt than non-Hispanic white smokers; similarly, smokers with >high school education had significantly greater odds of making a past-year quit attempt than smokers with <high school education (Table 3). Among smokers enrolled in Medicaid and uninsured smokers, women had greater odds of making a quit attempt than men. Among uninsured and privately insured smokers, people aged 18-44 had greater odds of making a quit attempt than those aged 45-64. Among those with private insurance, the magnitude of the state cigarette excise tax was significantly associated with higher odds of quit attempts.
Odds ratios (ORs) and 95% CIs from multivariable logistic regression models of the relationship between demographic and state characteristics and past-year quit attempts among cigarette smokersa aged 18-64 with private insurance, Medicaid, and no insurance,b 41 states, the District of Columbia, and Puerto Rico, Behavioral Risk Factor Surveillance System 201412
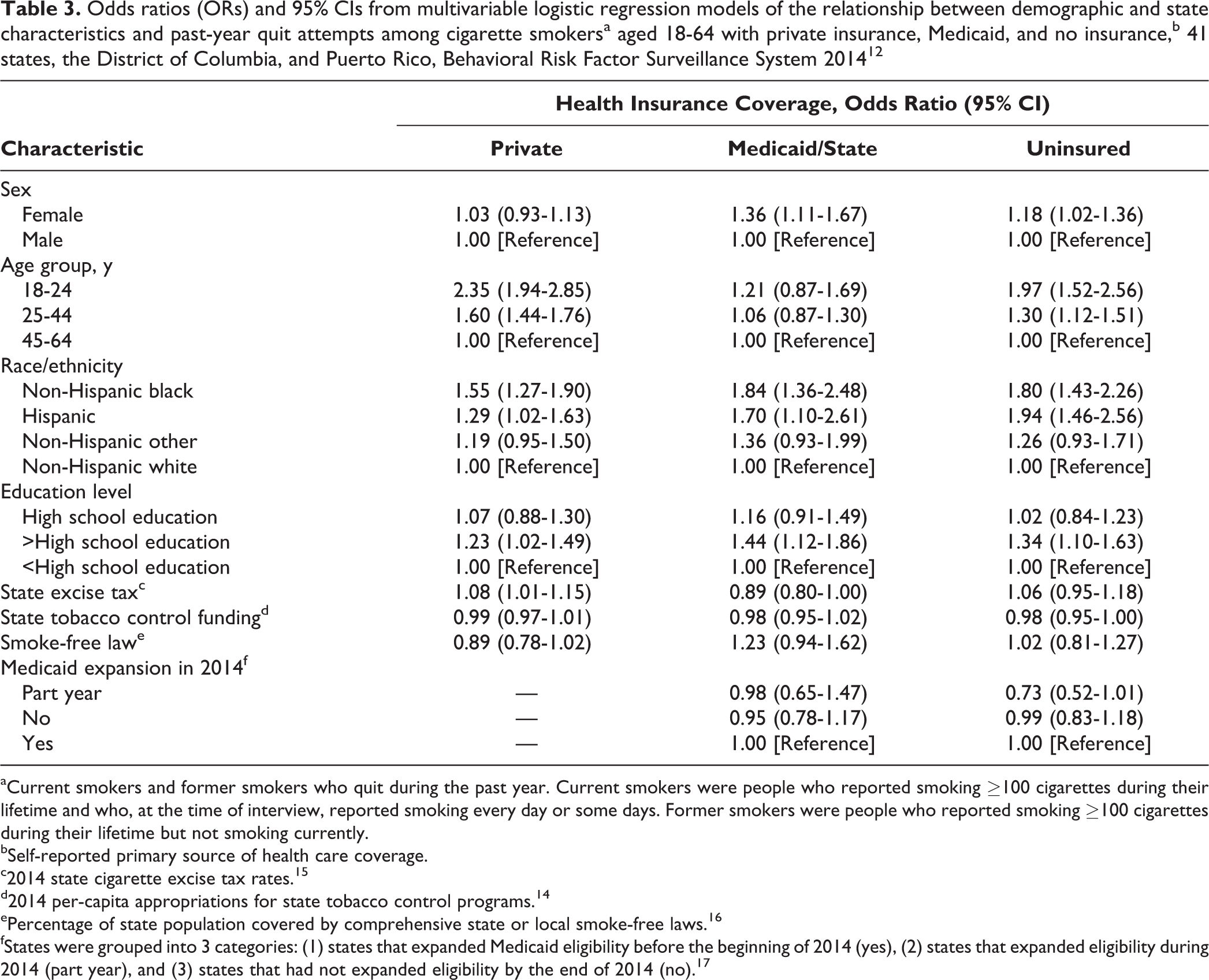
aCurrent smokers and former smokers who quit during the past year. Current smokers were people who reported smoking ≥100 cigarettes during their lifetime and who, at the time of interview, reported smoking every day or some days. Former smokers were people who reported smoking ≥100 cigarettes during their lifetime but not smoking currently.
bSelf-reported primary source of health care coverage.
c2014 state cigarette excise tax rates. 15
d2014 per-capita appropriations for state tobacco control programs. 14
ePercentage of state population covered by comprehensive state or local smoke-free laws. 16
fStates were grouped into 3 categories: (1) states that expanded Medicaid eligibility before the beginning of 2014 (yes), (2) states that expanded eligibility during 2014 (part year), and (3) states that had not expanded eligibility by the end of 2014 (no). 17
Discussion
This study found marked state-level variations in the prevalence of cigarette smoking and past-year quit attempts by health insurance status. In the 43 states and jurisdictions we examined, the smoking prevalence among adults who were enrolled in Medicaid or who were uninsured was more than twice that of adults with private insurance. We observed this pattern across all states and jurisdictions and found little overlap in the distribution of smoking across the 3 health insurance groups. These findings suggest the need to increase access to cessation treatments, in particular through comprehensive state tobacco control programs and improved cessation insurance coverage.
In almost all states, the state-specific smoking prevalence for adults enrolled in Medicaid fell in the highest quartile of overall smoking prevalence; in contrast, smoking prevalence among privately insured adults in most states was in the lowest quartile. A study using national data from the 2015 National Health Interview Survey found that smoking prevalence among both the uninsured and those enrolled in Medicaid was about 2.5 times higher than among those with private insurance. 9 In the present study, adults who were enrolled in Medicaid or were uninsured had a higher prevalence of smoking than privately insured adults, likely because those who were enrolled in Medicaid or were uninsured had lower education levels and were more likely to live below the federal poverty level, both of which are factors associated with cigarette smoking. 9
Overall, cigarette smokers enrolled in Medicaid were more likely to make a past-year quit attempt than were those with private insurance or no insurance. However, within states, the prevalence of quit attempts did not vary widely by type of health insurance. We found large variations in state-specific quit-attempt prevalence across the 3 insurance groups, ranging from 15 to 26 percentage points. These variations were likely due to differences in population demographic characteristics; tobacco control program infrastructure, programs, and policies; awareness, availability, accessibility, and use of smoking cessation treatments; and social and cultural norms. 1,19
In examining individual-level quit attempts, regardless of insurance status, non-Hispanic black and Hispanic smokers had greater odds of making a quit attempt than non-Hispanic white smokers, and smokers with >high school education had greater odds of making a quit attempt than smokers with <high school education. Among smokers enrolled in Medicaid and uninsured smokers, women had greater odds of making a quit attempt than men. Age was inversely associated with quit attempts among smokers with private insurance or no insurance. These patterns generally mirrored national patterns regardless of insurance status, although in an analysis of 2015 National Health Interview Survey data, sex was not significantly related to quit attempts. 3 The consistency of these findings possibly reflects differences in underlying attitudes and beliefs about cessation in general, as well as differences in use of cessation treatments. For example, younger adult smokers may be more optimistic about their ability to quit than older smokers, who likely have tried unsuccessfully to quit. 20
Most of the state tobacco control policies we examined were not significantly associated with quit attempts. These findings may have resulted from limiting our analysis to 1 year of data, which did not account for policy changes over time. However, even with limited variations in these policy variables, state excise tax was found to be associated with higher odds of a quit attempt among smokers with private insurance. This finding is consistent with previous studies that reported that state excise tax increases were associated with increased quit attempts. 21,22
Among cigarette smokers who were enrolled in Medicaid or were uninsured, we observed no relationship between living in a state that had expanded Medicaid eligibility and past-year quit attempts. It may be that cigarette smokers who moved from being uninsured or having another type of health insurance to having Medicaid coverage due to Medicaid expansion were similar to smokers previously enrolled in Medicaid in terms of factors related to quit attempts. Alternatively, this finding may be due to the correlations among state-level variables, especially given that we based our analysis on 1 year of BRFSS data. More research is warranted to assess the effects of Medicaid expansion on interest in quitting, quit attempts, use of cessation treatments, and successful cessation.
Given the high prevalence of smoking among Medicaid enrollees 9 and this population’s high level of interest in quitting, 3 an opportunity exists to reduce smoking and smoking-related disease and health care costs in this population. As of June 2015, only 9 states covered individual and group counseling and the 7 FDA-approved cessation medications for all Medicaid enrollees. 8 Moreover, all of these states still had some barriers (eg, copayments or prior authorization) in place for at least 1 cessation treatment that could make it more difficult for Medicaid enrollees to access these treatments. 8 Continued efforts by state Medicaid programs to improve their cessation coverage and to increase the use of evidence-based cessation treatments would be expected to result in improved health outcomes among Medicaid enrollees and reduced Medicaid health care costs. 23 -25
Limitations
This study had several limitations. First, the data were self-reported and may have been subject to recall or social desirability bias. As such, data may have been underreported. However, studies have found self-reported smoking status to be a valid indicator of actual smoking behavior. 26,27 Second, the response rates for the 2014 BRFSS ranged from 30.2% to 61.6%. Even after adjusting for nonresponse, low response rates can increase the potential for bias if systematic differences exist between respondents and nonrespondents; however, the BRFSS has been shown to be valid and reliable. 28 Third, health insurance status was reported at the time of the interview and may not have reflected coverage for the entire year. Fourth, data on state-level variables were captured for a single year and, therefore, could not reflect changes in policy initiatives. Fifth, state-level variables were captured for 2014, and some of the reported quit attempts in this analysis likely occurred in 2013. However, a sensitivity analysis using 2013 state-level variables yielded similar results (results not shown). Sixth, some of the state variables may be correlated; for example, states that had not expanded Medicaid generally had lower state cigarette excise taxes. 14,17 We ran various sensitivity models with individual state-level variables or with state fixed effects; findings from these sensitivity analyses indicated that these variables’ relationships with quit attempts did not deviate from the original findings. Finally, we did not include measures of coverage of cessation treatments by private plans or Medicaid because this information was not available in the BRFSS. These measures might have been helpful in interpreting differences in outcomes by insurance type.
Conclusions
This study found wide state-specific variations in the prevalence of smoking and past-year quit attempts by health insurance status. These findings underscore the importance of continued implementation of evidence-based, comprehensive state tobacco control programs and cessation insurance coverage to further increase smoking cessation and reduce smoking. 6,19,23 –25 In particular, insurance coverage that enables smokers to access proven cessation treatments with minimal barriers increases quit rates, thus contributing to reducing smoking and smoking-related disease, death, and health care costs. 5,23 -25,29 The impact of cessation insurance coverage on cessation behaviors and smoking rates can be further enhanced when covered cessation treatments are proactively promoted to smokers and health care providers to increase awareness and use of these treatments. Federal policies require private health insurers to cover cessation treatments with no cost sharing, and they require state Medicaid programs to cover FDA-approved cessation medications. 6 However, compliance with these requirements appears to vary considerably in practice. 6 -8
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors declared no funding with respect to the research, authorship, and/or publication of this article.