
Abstract
Objectives:
From 2000 to 2010, the Division of Nutrition, Physical Activity, and Obesity (DNPAO) at the Centers for Disease Control and Prevention (CDC) funded 37 state health departments to address the obesity epidemic in their states through various interventions. The objective of this study was to investigate the overall impacts of CDC-DNPAO statewide intervention programs on adult obesity prevalence in the United States.
Methods:
We used a set of an individual-level, interrupted time-series regression and a quasi-experimental analysis to evaluate the overall effect of CDC-DNPAO intervention programs before (1998-1999) and after (2010) their implementation by using data from CDC’s Behavioral Risk Factor Surveillance System.
Results:
States that implemented the CDC-DNPAO program had a 2.4% to 3.8% reduction in the odds of obesity during 2000-2010 compared with states without the program. The effect of the CDC-DNPAO program varied by length of program implementation. A quasi-experimental analysis found that states with longer program implementation did not necessarily have lower odds of obesity than states with shorter program implementation.
Conclusions:
Statewide obesity interventions can contribute to reduced odds of obesity in the United States. Future research should evaluate the CDC-DNPAO programs in relation to their goals, objectives, and other environmental obesity risk factors to inform future interventions.
Obesity is a major public health problem in the United States, resulting in chronic disease morbidity, premature mortality, and an increase in public health spending. The adult obesity prevalence rate in the United States more than doubled from the early 1970s (14 obese adults per 100 population) to 2010 (36 obese adults per 100 population). 1 In 1999, the US Congress authorized the Centers for Disease Control and Prevention (CDC) to establish the Division of Nutrition, Physical Activity, and Obesity (DNPAO) to address the growing obesity epidemic and other chronic diseases in response to obesogenic behaviors and environments. 2,3 The 5-level Social Ecological Model is the encompassing theoretical framework for CDC-DNPAO programs; it contends that human behavior can be influenced by distinct yet intertwined levels of society. 2,4 The model proposes 5 levels of interactions: intrapersonal, interpersonal, organizational, community, and societal. 5
Since the 1999-2000 fiscal year, the CDC-DNPAO granted federal funding to state health departments to implement obesity-related health promotion and intervention programs. 2,6 CDC-DNPAO programs are cooperative agreements between CDC and funded state health departments. 6 The purpose of the funded programs is to “reduce the prevalence of obesity and other chronic diseases by changing Americans’ behaviors and environments.” 2 Major target policy areas for CDC-DNPAO programs include (1) increasing breastfeeding initiation, duration, and exclusivity; (2) increasing physical activity; (3) increasing the consumption of fruits and vegetables; (4) decreasing the consumption of sugar-sweetened beverages; (5) reducing the consumption of high-energy dense foods; and (6) decreasing television viewing. 7
Five states received the initial pool of funding in 2000; until 2010, 37 states developed and implemented science-based nutrition and physical activity interventions with CDC-DNPAO programmatic funding. 2,8 Program funding was granted at either capacity-building or basic-implementation levels. Capacity-building funding was intended to help states build essential infrastructure and partnership including staffing, training, and developing a state plan. Basic-implementation funding was for expanding existing state plans through states’ policy implementation and collaboration with government and private sectors. 2,8 The amount of funding varied. For fiscal year 2007, capacity-building funding ranged from $270 000 to $526 000 per year (median: $450 000) and basic-implementation funding ranged from $800 000 to $1 100 000 per year (median: $1 000 000). 2,9
Each funded state program developed its own nutrition, physical activity, and obesity plans through public and/or private partnerships. Therefore, programmatic interventions were tailored to the needs of each state. In Michigan, for example, the Michigan Department of Community Health (currently, the Michigan Department of Health and Human Services) built a partnership with several county health departments and communities to address obesity by opening more farmers’ markets in disadvantaged neighborhoods, improving walking trails and bicycle facilities, and promoting healthy lifestyles through partnerships with nonprofit health promotion organizations. 3 CDC requested all funded states to submit annual performance reports on the effectiveness of the CDC-DNPAO program in their states at the end of their fiscal years. Based on these reports and new requests from other states, CDC-DNPAO made funding decisions to either continue the support for existing participants and/or provide new funding for nonparticipating states 2,10 (Table 1).
Thirty-seven states that received funding from the Centers for Disease Control and Prevention’s Division of Nutrition, Physical Activity, and Obesity (CDC-DNPAO), United States, 2000-2010a
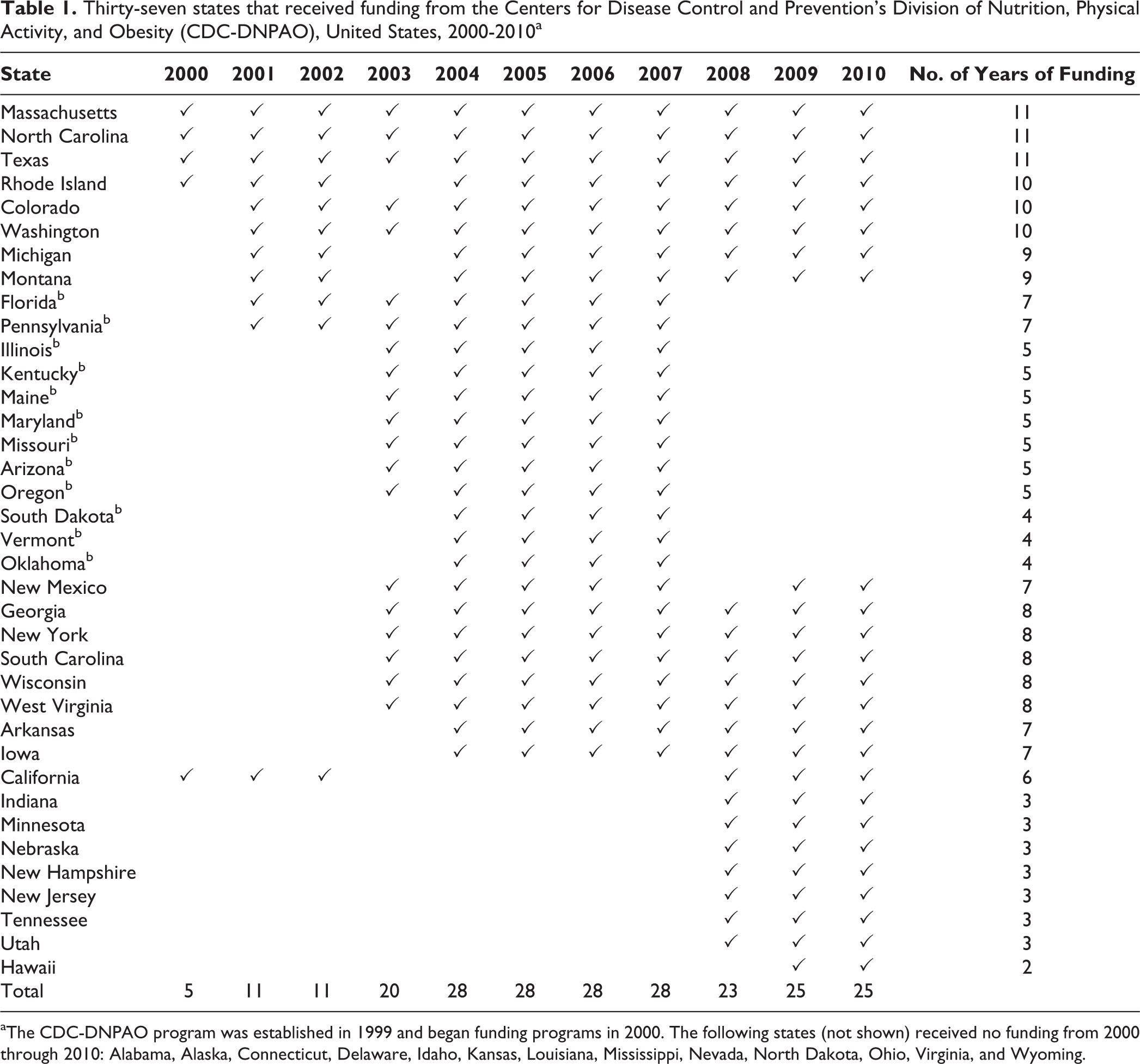
aThe CDC-DNPAO program was established in 1999 and began funding programs in 2000. The following states (not shown) received no funding from 2000 through 2010: Alabama, Alaska, Connecticut, Delaware, Idaho, Kansas, Louisiana, Mississippi, Nevada, North Dakota, Ohio, Virginia, and Wyoming.
To our knowledge, no non–state-directed studies have comprehensively evaluated the impacts of CDC-DNPAO–funded programs on adult obesity in the United States. Although each state’s annual performance report is submitted to CDC-DNPAO and provides important information on the effectiveness of its obesity program, the overall impact of state-county interventions on adult obesity in the United States is unknown. Understanding the impact of CDC-DNPAO–funded programs on the geography of obesity prevalence is important for identifying where programs are successful and where future intervention efforts should be focused. The objective of this study was to investigate the overall impact of CDC-DNPAO statewide intervention programs on adult obesity in the United States. We used repeated cross-sectional survey data from 1998 through 2010 and a quasi-experimental study design comparing before-and-after CDC-DNPAO implementation to produce valid results under naturally occurring circumstances. 11,12
Methods
Data
The area covered in this study included the 50 US states. The total sample of our study (N = 2 774 697) represented the number of US adults aged ≥18 from 1998 through 2010 obtained from CDC’s Behavioral Risk Factor Surveillance System (BRFSS). The BRFSS collects self-reported data by telephone on health risk behaviors, preventive health practices, health care access, and disease outcomes. 13 CDC and each state collaborate to conduct telephone interviews and manage survey data. Although the BRFSS included only landline telephone users before 2010, it adopted a new sampling methodology in 2011 that now surveys both landline telephones and cellular telephones to include more diverse demographic groups, especially young and low-income adults. Because of this change in sampling methodology, CDC advises against temporally comparing the BRFSS datasets collected before 2010 with BRFSS datasets collected thereafter. We tabulated data on states funded by CDC-DNPAO and the years of funding from 1999 through 2010 from CDC’s website and the National Alliance for Nutrition and Activity website. 9,14 On the basis of the 5-level Social Ecological Model, we assumed that all residents living in CDC-DNPAO participating states were exposed to the protective features of CDC-DNPAO programs.
Individual-level obesity risk factors used in the current study included: sex (male or female), age group (18-24, 25-34, 35-44, 45-54, 55-64, and ≥65), race (white, black, Asian/Pacific Islander, American Indian/Alaska Native, and other), marital status (divorced, widowed, separated, never married, and unmarried), educational attainment (<high school, high school, some college, and ≥college), annual household income (<$25 000, $25 000-$34 999, $35 000-$49 999, $50 000-$74 999, and ≥$75 000), and smoking behavior (current daily smoker, current occasional smoker, former smoker, and never smoker).
Analysis
Following the literature,
15,16
this study used a set of individual-level, interrupted time-series regression analyses and a quasi-experimental analysis to evaluate the overall effects of CDC-DNPAO on obesity prevalence, before and after program implementation. The first analysis included the total sample to investigate the overall effect of CDC-DNPAO from 1999 to 2010 on obesity prevalence using a logistic regression model. The default year of implementing CDC-DNPAO was 2000, which means we examined the effect of CDC-DNPAO on the odds of obesity before and after 2000.
In this model, the dependent variable (Obesity
ist
) was a binary outcome of the ith individual in state s at time t (Obesity
ist
= 1 when an individual is obese; otherwise 0). Obesity was defined by body mass index (BMI) of ≥30 kg/m
2
. The coefficients for State were state-specific fixed effects to account for time-invariant differences across states that may have resulted in differences in obesity. Year controlled for year-specific fixed effects that possibly contributed to obesity, ranging from –2 (1998) to 10 (2010). Trend was a linear time trend to account for secular changes in obesity apart from CDC-DNPAO implementation and state effects, ranging from 0 (before 2000) to 10 (2010). The interaction term (State × Trend) accounted for any time-varying state-specific changes in obesity. DNPAO was set to 1 for all years that a state was funded by CDC-DNPAO in a year and was 0 otherwise. Duration was the total number of years a state participated in the CDC-DNPAO program (coded 1 in 2000 and 11 in 2010). The vector
We also examined the effects of natural occurrence in obesity policy by using a quasi-experimental study design, which compared overall obesity prevalence before and after implementation of CDC-DNPAO. In this analysis, we compared the treatment group, which comprised 3 states (Massachusetts, North Carolina, and Texas) that were funded from 2000 through 2010, with the control group, which comprised 13 states (Alabama, Alaska, Connecticut, Delaware, Idaho, Kansas, Louisiana, Mississippi, Nevada, North Dakota, Ohio, Virginia, and Wyoming) that were never funded by the program.
All analyses included BRFSS sampling weights and post-stratification adjustments to account for differences in the probabilities of sampling selection and nonresponse, and to adjust for noncoverage of households without landline telephones. 13 We used Stata version 14 for all analyses. 17
Results
Interrupted Time-Series Regression Analyses
Living in a state with a CDC-DNPAO program was associated with a 2.4 percentage-point (95% confidence interval [CI], 1.0-4.0) reduction in the odds of obesity from 1998 to 2010. Longer total duration of a state’s CDC-DNPAO participation was associated with a 0.1 percentage-point (95% CI, 0.1-0.7) reduction in the odds of obesity (Table 2).
The effects of funding from the Centers for Disease and Control and Prevention’s Division of Nutrition, Physical Activity, and Obesity (CDC-DNPAO) and duration of funding (as a continuous variable) on the odds of obesity among adults, United States, 2000-2010
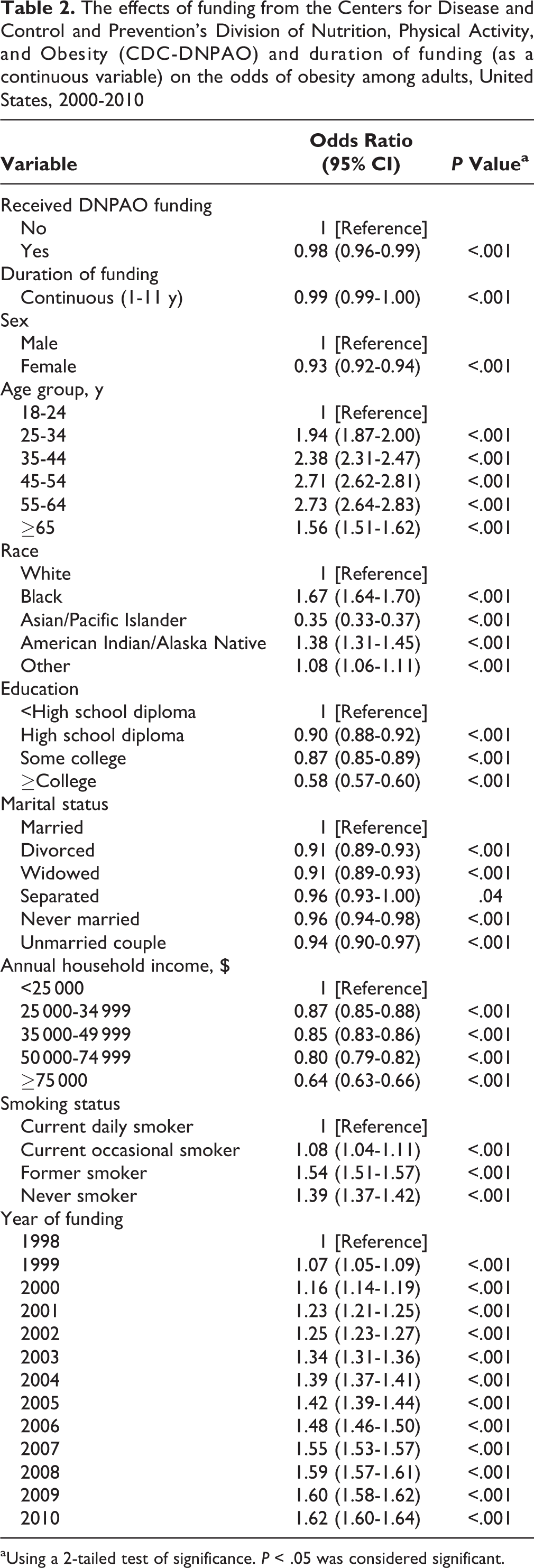
aUsing a 2-tailed test of significance. P < .05 was considered significant.
The effect of total duration of funding on obesity prevalence was mixed: 2 years of CDC-DNPAO participation was associated with a 3.9 percentage-point (95% CI, 0.5-7.3) increase in the odds of obesity, but 3 and 7 years of CDC-DNPAO participation were associated with a 3.1 percentage-point (95% CI, 0.1-6.0) and 4.4 percentage-point (95% CI, 1.7-7.0) reduction in the odds of obesity, respectively. Eleven years of CDC-DNPAO participation was associated with a 6.0 percentage-point (95% CI, 0.2-12.7) higher probability of obesity compared with no CDC-DNPAO funding. Other lengths of CDC-DNPAO participation were not significant. CDC-DNPAO participation was associated with a 3.8 percentage-point (95% CI, 1.6-6.1) reduction in the odds of obesity (Table 3).
The effects of funding from the Centers for Disease and Control and Prevention’s Division of Nutrition, Physical Activity, and Obesity (CDC-DNPAO) and duration of funding (as a categorical variable) on the odds of obesity, United States, 2000-2010
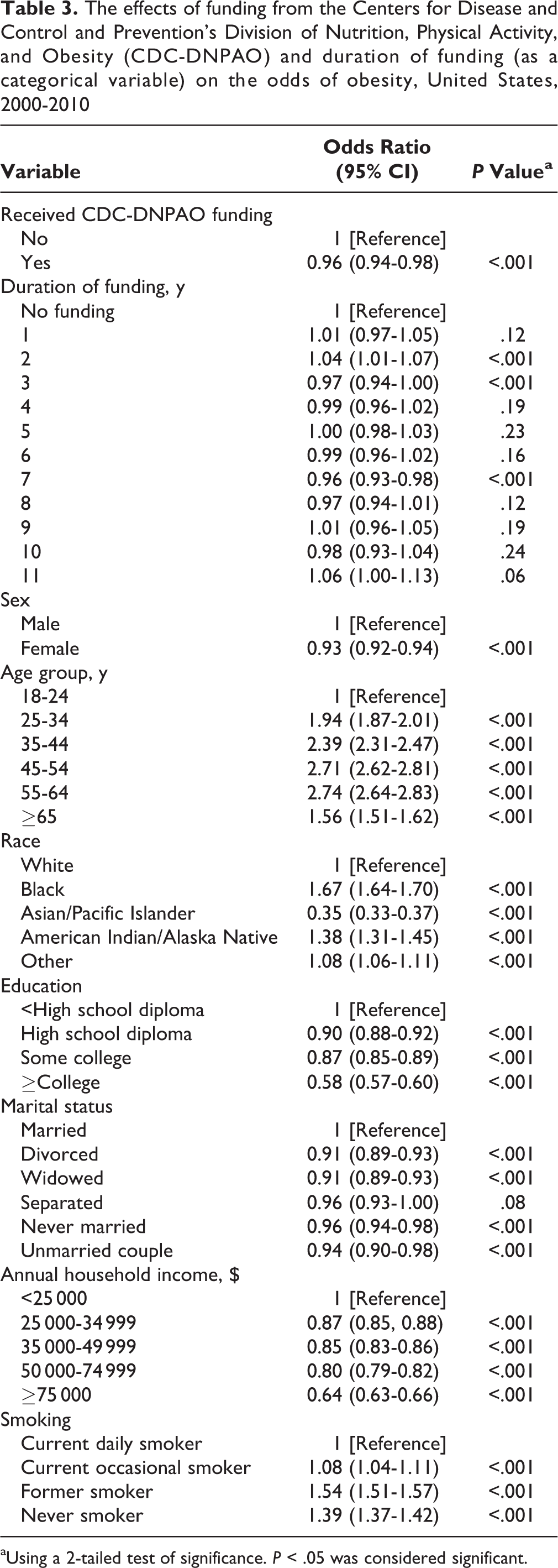
aUsing a 2-tailed test of significance. P < .05 was considered significant.
The associations between individual-level obesity risk factors and obesity prevalence were similar in all models. Compared with the youngest age group (18-24), all older age groups had higher odds of obesity. Compared with white people, Asian/Pacific Islanders were less likely to be obese, but all other racial groups, including black people, American Indians/Alaska Natives, and others, were more likely to be obese. People who had less than a high school diploma were more likely to be obese than were those with a high school diploma, some college education, or a college degree or higher. Married people had higher odds of obesity than did all other marital groups. Compared with people whose annual household income was <$25 000, the odds of obesity were lower for each level of income, and as household income level increased, the odds of obesity decreased. Finally, former smokers, nonsmokers, and current occasional smokers were more likely to be obese than were current daily smokers (Table 3).
Quasi-experimental Analysis
Before DNPAO funding, in 1998-1999, the prevalence of obesity was 21.2% in the 3-state treatment group and 19.9% in the 13-state control group, for a difference of 1.4 percentage points. In 2010, the prevalence of obesity was 30.5% in the treatment group and 29.4% in the control group, for a difference of 1.1 percentage points. Although the differences in obesity prevalence between the treatment and control group decreased by 0.2 percentage points from 2000 to 2010, this difference was not significant (Table 4).
Differences in prevalence of obesity between 3 states that received funding from the Centers for Disease and Control and Prevention’s Division of Nutrition, Physical Activity, and Obesity (CDC-DNPAO) during all years from 2000 through 2010 (treatment statesa) and 13 states that never received such funding (control statesb)
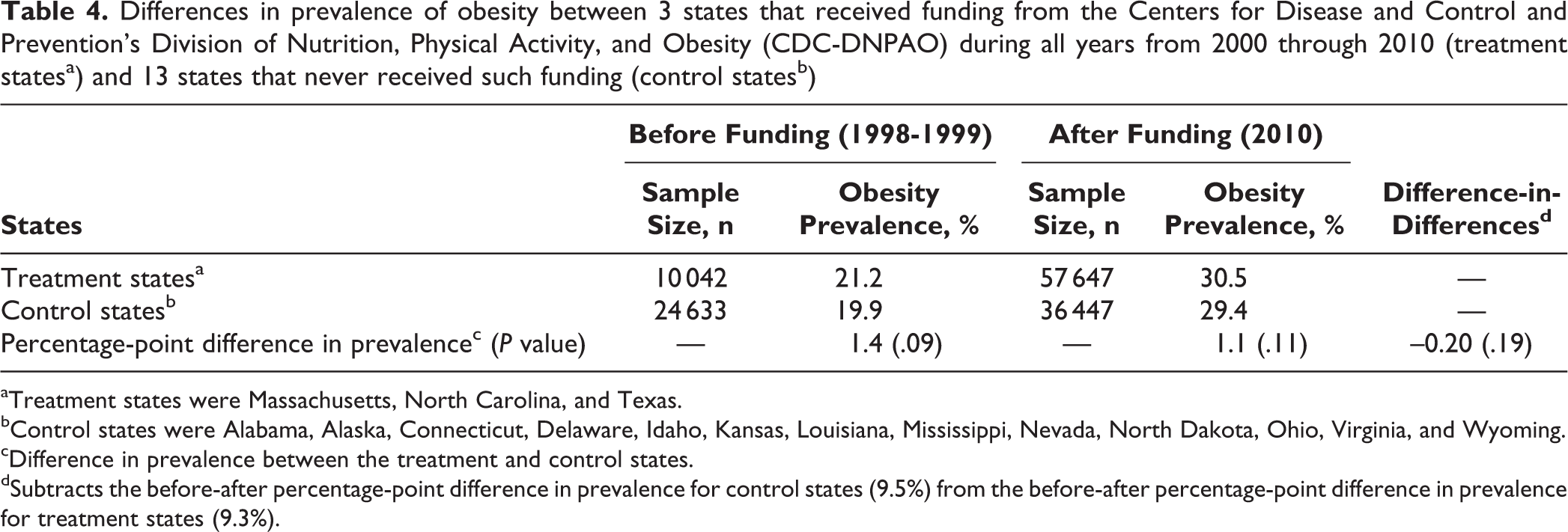
aTreatment states were Massachusetts, North Carolina, and Texas.
bControl states were Alabama, Alaska, Connecticut, Delaware, Idaho, Kansas, Louisiana, Mississippi, Nevada, North Dakota, Ohio, Virginia, and Wyoming.
cDifference in prevalence between the treatment and control states.
dSubtracts the before-after percentage-point difference in prevalence for control states (9.5%) from the before-after percentage-point difference in prevalence for treatment states (9.3%).
Discussion
This study had several important findings. First, the effect of CDC-DNPAO statewide interventions reduced the likelihood of obesity during the study period. With CDC-DNPAO funding, each state could develop its own obesity reduction interventions to increase physical activity, improve dietary habits, and decrease the prevalence of obesity. 2,3 Although it was assumed that all residents were equally exposed to statewide obesity interventions, in fact they may not have been; therefore, the positive effects of CDC-DNPAO in reducing the odds of obesity suggest that obesity interventions have far-reaching effects through social structures as outlined in the Social Ecological Model. For example, the Minnesota Department of Health, in partnership with several nongovernmental organizations, supported the building of bicycle rental kiosks throughout the Twin Cities (ie, Minneapolis and St. Paul) to increase physical activity among residents of all sociodemographic groups. This program was evaluated as a successful environmental change to increase physical activity in a CDC-DNPAO participating state. 18
Second, this study found that the effect of CDC-DNPAO on reducing obesity prevalence varied during the program. CDC’s guidelines for CDC-DNPAO–funded states described important milestones for the funding period. The CDC program’s objectives in years 1 and 2 included capacity building (ie, developing policy plans, building essential infrastructure and partnerships, and educating local health department staff members and collaborative partners). Objectives for years 3 to 5 included basic-implementation plans (ie, implementing, monitoring, and evaluating statewide obesity interventions). As such, the 3.9 percentage-point higher odds of obesity in the first 2 years of the CDC-DNPAO program indicates that state programs needed time for capacity building before demonstrating reductions in obesity prevalence. Furthermore, the likelihood of reducing the odds of obesity after 3 or 7 years of CDC-DNPAO implementation implies that CDC-DNPAO participating states successfully implemented their statewide obesity interventions.
In addition, CDC-DNPAO programs that were implemented for the longest periods of time had a 6.0 percentage-point (95% CI, 0.2-12.7) higher probability of obesity compared with states that did not have funding. This finding may suggest the need for adjustments during the expansion phase of the program (ie, from the initial implementation), because the protective effects of CDC-DNPAO may not have been fully delivered to all people as a result of variations in demographic and environmental characteristics across states. This finding was also compatible with the finding of the quasi-experimental analysis. Despite 11 years of CDC-DNPAO participation in Massachusetts, North Carolina, and Texas, substantial progress was not made in reducing obesity prevalence compared with the 13 states that were never funded by CDC-DNPAO. Future research should investigate why the effects of CDC-DNPAO varied by states, year of funding onset, and duration of implementation.
Finally, the findings on the associations between individual demographic risk factors and obesity prevalence were similar to the findings of other studies, contributing additional evidence for obesity reduction research. Our study confirms variations in being obese with individual-level obesity risk factors. Most important, black race, lower education, and lower household income significantly increased the likelihood of obesity. Future obesity interventions should focus on these populations to further reduce obesity in states.
Limitations
This study had several limitations. First, we evaluated only the overall effects of CDC-DNPAO program implementation across states from 2 years before its implementation (1998) to 2010 because of inaccessibility to detailed information about individual state programs (ie, total budget awarded and full descriptions of program interventions). Therefore, we did not evaluate the effect of individual CDC-DNPAO programs implemented within states and across years. Second, reverse causality may exist between the application and receipt of CDC-DNPAO funding. For example, a state public health department with more expertise in obesity than other chronic health outcomes may more actively pursue funding, resulting in a longer duration of funding than other states. Qualitative research on the application and receipt of funding among states’ public health departments may be necessary for future funding considerations, which were beyond the scope of this study. Third, the use of BRFSS data may have limited the validity of our findings. Because data on individuals in the BRFSS were collected via self-report, respondent errors or biases may have been introduced in the final dataset. Although we adjusted the results of our analysis with BRFSS’s sampling weights, other biases may have been introduced because of non-landline telephone users, remote areas, and small population groups. Fourth, this study examined the effect of CDC-DNPAO funding only on adult obesity. Future studies should focus on childhood obesity, as well as acute and chronic conditions such as diabetes, hypertension, cardiovascular disease, and cancer, all of which are known to be associated with obesity. Finally, the analysis models in this study could not control for other environmental risk factors (eg, the number of food stores per capita, rural/urban areas, the areas suitable for physical activity) or mediating factors (eg, the change in consumption of sugar-sweetened beverages or high-energy dense foods) that may have influenced individuals’ risk of obesity during the study period. Contrary to individual-level data, such as from the BRFSS, it is challenging to obtain timely and complete annual data about those factors. One way to address these limitations is to improve the collaboration between researchers and policy makers to build robust datasets and to share relevant data, information, and analytical methods to evaluate state-level CDC-DNPAO programs in the future.
This study also had several strengths. For one, it provided summary evaluative information on CDC-DNPAO statewide obesity programs that was previously unavailable. In addition, we evaluated the overall impact of CDC-DNPAO across US states from 1998 to 2010 using interrupted time-series regression analyses and a quasi-experimental study design to ensure robust findings, methods that had not been conducted in previous studies. The findings and implications from this study will help public health officials and experts design and refine future obesity interventions.
Conclusions
The implementation of CDC-DNPAO programs reduced the odds of being obese in funded states during the study period. However, the positive health effects of CDC-DNPAO programs varied by state and by total years of implementation. As more specific data on statewide CDC-DNPAO programs become available, researchers and public health officials may further evaluate intervention outcomes to specific goals and objectives and other important behavioral and environmental obesity risk factors to reduce obesity prevalence in states. This information may be widely disseminated for all states to learn from to reduce obesity and improve the health of their respective populations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by the Dissertation Completion Fellowship, Graduate School and Department of Geography, Environment, and Spatial Sciences at Michigan State University.