
Abstract

Collaborations between community health centers (CHCs), including federally qualified health centers (FQHCs), and academic partners can provide opportunities to conduct research designed to help vulnerable populations. Despite the potential to deepen understanding of health disparities and to develop means to ameliorate them, barriers to successful research collaboration exist. Barriers to collaboration include financial limitations for conducting research, a lack of experience in working together, minimal collaborative research infrastructure, CHC partners’ unfamiliarity with research methods, and incomplete knowledge about the CHC environment and academia’s mandate to address communities’ perceived needs. 1 Guided by historical context, this commentary offers suggestions to academic researchers for a more participatory approach for conducting research in collaboration with CHCs.
Background
The CHC movement took hold in the United States in the 1960s amid rampant poverty and racial tension in inner-city neighborhoods and rural communities 2 against the backdrop of the war on poverty declared by President Lyndon Johnson. The CHC movement was spearheaded by H. Jack Geiger who, as a young physician in the early 1960s, spent time in South Africa. 3 As in South Africa, the major goal of the CHC movement in the United States was community and economic development. 4 Tackling this goal in the United States included a critique of health care practices that focused heavily on biomedical causes of disease rather than comprehensive health promotion among individuals and their communities that takes into account environmental, social, and cultural factors. 5
Geiger’s interest in primary care medicine and civil rights activism 6 converged with a widespread recognition that systemic poverty in US inner cities and rural areas in the American South and Appalachia was creating major crises in health care and human development. He was instrumental in starting the first CHC demonstration projects and in motivating the legislation needed to turn the CHC movement into practical reality. CHCs became a reality in 1965, when the Office of Economic Opportunity approved funding for the first 2 CHC demonstration projects: in Boston, Massachusetts, and Mound Bayou, Mississippi. 2,5,6 These demonstration projects culminated in the creation of FQHCs in 1991.
It is important for researchers and CHC-based providers to realize that the model that emerged aimed to address the roots of poverty by bringing together local resources and federal funds to establish neighborhood clinics in rural and urban areas across the United States. The model also considered environmental, social, and cultural factors previously unaccounted for in traditional medical settings. This more encompassing focus served a dual purpose: (1) it empowered communities, and (2) it aimed to provide affordable and accessible health care to improve individuals’ health and provide economic development benefits for underresourced communities. These FQHCs created jobs and other investments in economically depressed communities. 4 They also reduced costs for the health care system by lowering the number of acute care visits at hospital emergency departments. 7
Currently, FQHCs are a main component of health care delivery through the provisions of the Patient Protection and Affordable Care Act. 8 Today, >7500 FQHCs across the United States provide patient-centered care to medically underserved populations regardless of socioeconomic and health insurance status. 9 FQHCs differ in size and can be part of a system of 1 to >100 clinics or delivery sites. FQHCs may focus solely on primary care or may incorporate specialty care, such as behavioral health care, dental care, and vision care.
Understanding Context for Effective Collaboration
It is important for academic researchers to understand that, from the beginning, providers at FQHCs made the connection between health and the social, cultural, and physical environment. For example, providers at the first CHCs in urban (Boston, Massachusetts) and rural (Mound Bayou, Mississippi) locations wrote prescriptions for food because it was the “specific therapy for malnutrition.” 2,3 Today, a farmers market located at an FQHC in Orangeburg, South Carolina, distributes prescriptions for fruit and vegetables. 10 The focus on food rather than prescription medicines is different from the typical biomedical perspective against which the pioneers in the field, such as Geiger, protested. 4
If academic researchers approach FQHCs in a manner that is insensitive to the perceived need to create social good, the collaboration is unlikely to go well. This imperative of “community beneficence,” 11,12 which is necessary for addressing health from a community perspective, is embedded in governance requirements that are unique to the CHC model. Researchers should understand the authority and responsibilities of the health center board of directors, which include providing strategic input and oversight of an organization’s fulfillment of its mission and compliance with federal requirements. Another critical factor is the composition of the board; for example, at least 51% of people who serve on the board of directors for a health center must be patients of the health center. A patient is defined in the requirements as “a current registered patient of the health center and must have accessed the health center in the past 24 months to receive at least one or more in-scope service(s) that generated a health center visit.” 13 Additionally, the patient composition on the board must represent the populations served by the health center, to include special populations (eg, homeless people, migrant/seasonal agricultural workers). 14 In addition to having a board, each FQHC has various administrative structures developed to meet its unique demographic and organizational needs, including, for example, socioreligious beliefs, substance abuse, land use, and environmental contamination. 15
Practical Suggestions for Academic Researchers in Working Effectively With FQHCs
We offer 10 suggestions and goals for enhancing research collaborations between academic institutions and FQHCs, describe the means for achieving them, and provide examples of how suggestions and goals have been or can be met (Table).
Suggestions to enhance research collaborations between academic institutions and FQHCs
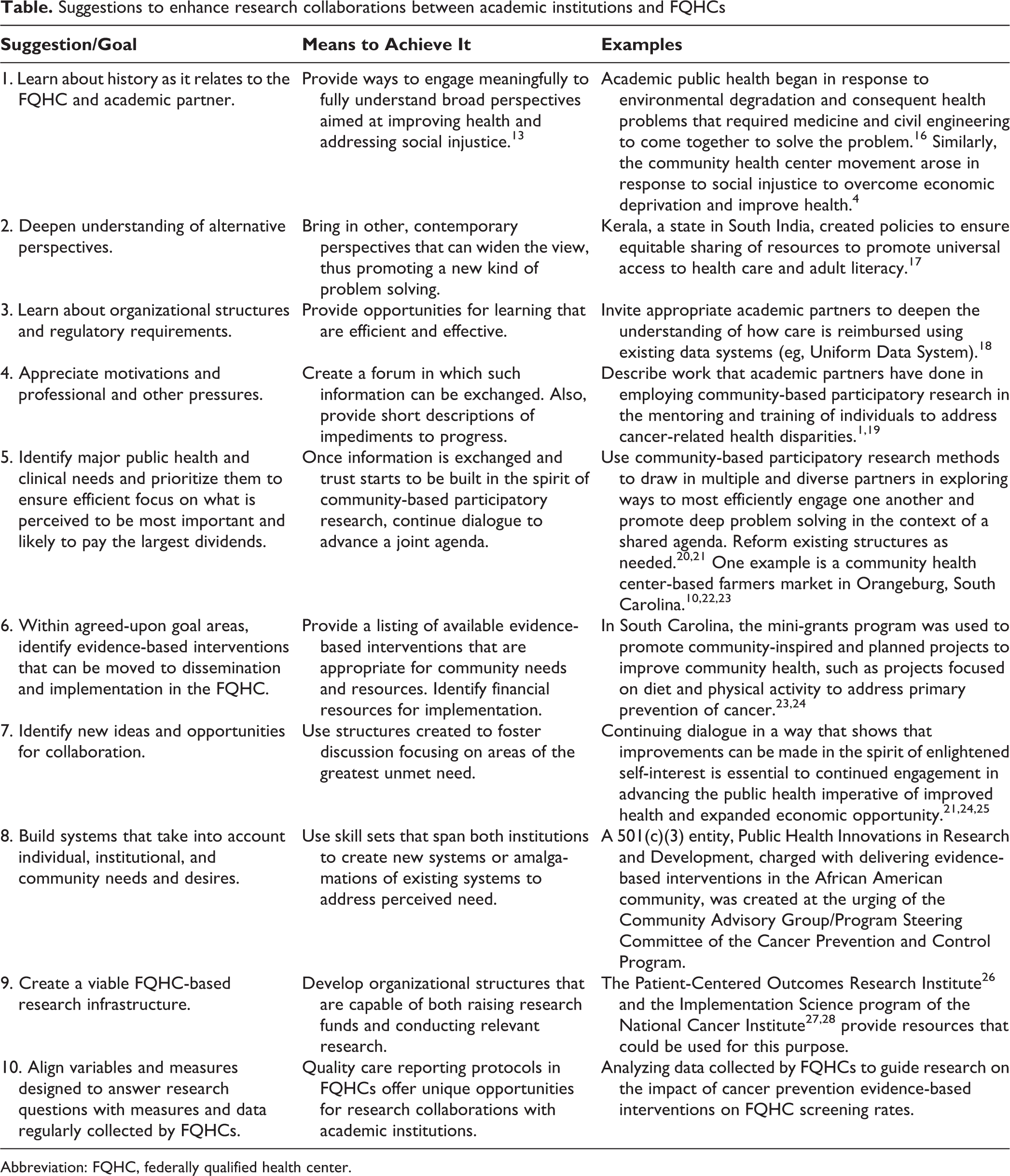
Abbreviation: FQHC, federally qualified health center.
1. Learn About History As It Relates to the FQHC and Academic Partner
Whereas most FQHC staff members are at least superficially aware of the requirements of academic research, the converse is rarely true. Therefore, it is incumbent on academic researchers to familiarize themselves with the history of the CHC movement and how FQHCs are charged to deliver care and address community needs in response to this long history.
2. Deepen Understanding of Alternative Perspectives
Many people who work in FQHCs appreciate the fact that the movement began in Zulu, South Africa, 3 with the imperative to improve economic prospects of the communities they serve. Many of them may have alternative ways of looking at things that involve international perspectives, in part because of their client base and in part because many of them may have personal or family histories that have encompassed or intersected other sociocultural and ethnic identities.
3. Learn About Organizational Structures and Regulatory Requirements
Because FQHCs, even individual practice sites within FQHCs, differ in how they function, it is important to learn about individual and collective philosophical perspectives and organizational characteristics.
4. Appreciate Motivations and Professional and Other Pressures
Just as academic researchers have complex motivations for choosing and conducting their life’s work and face unique pressures related to tenure and promotion, CHC professionals have unique motivations for choosing their work and pressures related to resource constraints and the needs of the patients and communities they serve. Community-based participatory research provides a framework for sharing perspectives to arrive at consensus decision making.
5. Identify Major Public Health and Clinical Needs and Prioritize Them
By identifying major public health and clinical needs and prioritizing them, one can ensure efficient focus on what is perceived to be most important and likely to pay the largest dividends. Community-based participatory research also provides a framework for identifying community needs. The task here is to understand how the needs and skill sets of people within academia mesh with the needs and skill sets of people in the FQHC. The example of the farmers market in Orangeburg, South Carolina, 10,21,22 highlights the intersection of the authors’ academic interest and expertise in nutrition and the FQHC’s interest in and perceived need to address nutrition.
6. Identify Evidence-Based Interventions That Can Be Moved to Dissemination and Implementation
Within agreed-upon goal areas, identify evidence-based interventions that can be moved to dissemination and implementation in the FQHC. Once agreement is reached on a topic on which to collaborate or a problem to solve, an evidence-based intervention that can be moved to dissemination and implementation in the FQHC should be identified. For example, an intervention study conducted in California in 2012 incorporated a “prescription” for caregivers and children from a pediatric primary care FQHC to spend time in a public park; the program used behavioral counseling to decrease caregiver stress, improve family members’ physical activity, and increase awareness about the health benefits of nature. 29
7. Identify New Ideas and Opportunities for Collaboration
Community-based participatory research methods can be used to expand the scope of the collaboration to include topics and concerns that may not have been within the boundaries of the original collaboration. These second-generation studies reflect expanded vision and deeper levels of trust, familiarity, and dedication to the common cause. At this juncture, all parties understand the potential mutual benefit that they derive and that can be extended to their constituencies.
8. Build Systems That Take Into Account Individual, Institutional, and Community Needs and Desires
At some point, it may be necessary to create various structures that can meet the mutual needs of the partners and those of the communities served by the FQHC. For example, a nonprofit organization developed to write community-oriented grants could be based at the university or the FQHC, across both, or in some other entity altogether. Doing so would help to enhance flexibility to expand the greater good.
9. Create a Viable FQHC-Based Research Infrastructure
In addition to the examples provided (Table), quality care reporting requirements in FQHCs offer unique opportunities for creating infrastructure on which research collaborations with academic institutions can be based. 1 In pursuing such research opportunities, academicians should be sensitive to efficiency and workload associated with their data collection operations. For example, research partners should not collect data on items that are routinely collected via other protocols in FQHCs. Doing so will help to ensure validity of the data captured (eg, the data are derived from a verified source as opposed to the perceptions of multiple providers) and will obviate the need to locate data or responses that have been reported previously. This practice, in turn, will allow FQHCs to focus their research efforts on pursuits that will result in new information, will lead to new insights, and can expand infrastructure meaningfully and efficiently. 7
10. Align Variables and Measures Designed to Answer Research Questions With Measures and Data Regularly Collected by FQHCs
At a national level, all FQHCs report certain quality-of-care measures to the centralized data repository, the Uniform Data System, 18 which collects data on patient demographic characteristics and services provided. These data may be aggregated at the clinic, state, and national levels and can be divided into subsets to allow for comparisons, such as geographic location (urban vs rural), race, and socioeconomic status. For example, we demonstrated that FQHCs can affect rates of cancer screening and survivorship and policies related to these outcomes. 30 –32 At a local level, research partners of FQHCs can use this information to support new research initiatives. For example, data on the number of patients receiving health-related care and the demographic characteristics of those patients can be used to provide context on other survey items or to plan interventions using evidence-based protocols. Linking data from the Uniform Data System with other public use data also offers opportunities for FQHCs to relate their quality care metrics with other meaningful outcomes. Local examples abound, 33 including a social and environmental intervention that involved establishing a 22-week farmers market at an FQHC practice site in South Carolina, which resulted in improvements in fruit and vegetable intake among people with diabetes. 9
Future Research Partnerships With FQHCs
By providing health care services to medically underserved patients, FQHCs are vital to the US primary care safety net. 34 Compared with private health care providers, FQHCs serve more people who are low income, who have public insurance or are uninsured, and who tend to have higher disease burdens. 35,36 Thus, FQHCs play an important role in efforts to reduce health disparities. 37 They also can provide opportunities to expand research into the community and to examine the community-clinic interface, with the goal of improving health status. Community-based participatory research methods are useful for garnering community-oriented input to extend research agendas and to improve patient and community participation in research. Engaging in this way can expedite the translation of new and effective clinical practices into primary care settings, particularly among racial/ethnic minority communities. It also may highlight community factors that may affect health outcomes and interactions between CHCs and communities.
When planning to work with an FQHC, academic partners should recognize that CHCs have clinical and administrative priorities that compete with those of the academic partners. To reduce perceived competition, researchers should recognize the need to adapt to the needs of the FQHC and its target population, with the goal of providing new information and skills that translate into action. Academic partners need to be patient and flexible and provide adequate lead time when requesting collaborations with FQHCs. Also, it is important to propose and conduct research that can benefit the community. 12 After all, the CHC movement was predicated on the desire to create resources to meet public health needs, and evidence-based measures are required to help address those needs. 38 –40
A research readiness and capacity survey administered in 2011 with FQHC representatives in South Carolina 23 indicated the possibility of fertile ground for collaborating on topics of academic interest. Resulting activities can help guide a community’s acceptance of and participation in programs and services. However, other opportunities to improve health status and enhance economic impacts by addressing more obvious community concerns may exist. To get such topics onto the research agenda, a genuine, participatory forum is needed that permits and encourages the engagement of knowledgeable, committed, and respected community leaders (who, by design, often sit on FQHC boards). The operation and governance structures of FQHCs offer many ways to engage the community (eg, board membership, administrative leadership, clinical leadership, non–board member patient participation). Determining the appropriate strategies depends on the goal of the engagement. CHC administrative staff members (ie, chief executive officer, executive director) can identify appropriate leaders to help design effective approaches.
When one is working with communities, it is vital to build on existing community assets to produce sustainable outcomes. 41 Thus, nonprofit organizations, communities of faith, community advocacy groups, and special interest groups (eg, community policing, neighborhood crime watch, downtown redevelopment initiatives, and health care organizations) can be good partners for community-based participatory research efforts. Community leadership, although sometimes narrow in scope, will already exist. Mechanisms for communication, training, and fiduciary responsibility may be in place. Experience with previous programs, planning, and even evaluation also may exist. The ability for such groups to advocate for the FQHC and the surrounding community agenda items is important and indicates current capacity and the potential for action. However, participants who lack experience in community-based participatory research efforts will often defer to the experts—that is, the ones with academic and professional degrees who bring promises of funding and a specific agenda. Regardless, allowing FQHCs and communities to express their values and to use their expertise and skills is vital to ensuring that research aims meet a meaningful need. It is worth the effort.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the South Carolina Cancer Prevention and Control Research Network under cooperative agreement U48/DP005000-01S2 from the Centers for Disease Control and Prevention (Prevention Research Centers) and the National Cancer Institute.