
Abstract
Disseminating public health recommendations to community members is an important step in protecting the public’s health. We describe a community–academic partnership comprising health-based organizations, community groups, academia, and government organizations. This partnership undertook an iterative process to develop an outreach plan, educational materials, and activities to bring lead-poisoning prevention recommendations from a health impact assessment of a roadway demolition/construction project to the residents of an affected neighborhood in Cincinnati, Ohio, in 2012. Community partners played a key role in developing outreach and prevention activities. As a result of this project, activities among members of the partnership continue.
Lead is a developmental neurotoxicant that has no safe level of exposure. 1 –3 Exposure to lead during early childhood is associated with decreases in a child’s intelligence quotient, behavioral problems, poor academic achievement, and delinquency, as well as adult incarceration. 1,4 –7 Deteriorating housing that contains lead-based paint is a major source of lead exposure among children, but demolition of decaying infrastructure is also associated with increased levels of lead in ambient dust and increases in child blood lead levels. 8 –12 Because the neurotoxic effects of exposure to lead are not reversible and exposure is additive, the Centers for Disease Control and Prevention emphasizes primary prevention. 13 To protect the public from lead dust, Ohio law requires control of fugitive dust emissions from worksites 14 and lead risk assessment of structures associated with lead-poisoned children.
Community Context
In spring 2012, residents of the Lower Price Hill neighborhood of Cincinnati, Ohio, expressed concern about the planned demolition and replacement of an elevated roadway bridge spanning their neighborhood. The half-mile-long, 60-year-old, elevated roadway bridge was 60 feet over the neighborhood at its highest point and carried >50 000 vehicles per day. It was painted with multiple layers of lead-based paint and was in poor condition. The neighborhood is located west of downtown Cincinnati and is bordered by hillsides, a railroad yard, and the Ohio River. As of 2012, Lower Price Hill had 1075 residents, nearly 37% of whom were aged <18; the median household income was $15 257; an estimated 340 households were occupied; the neighborhood was predominantly Appalachian in culture; 69% of residents were white and 23% were African American; and 63% of adults had completed high school. 15
The bridge spanned the south side of the neighborhood adjacent to residential housing and a neighborhood school (pre-kindergarten through 12th grade) that had undergone a Leadership in Energy and Environmental Design Silver renovation. 16,17 Bridge demolition was scheduled for October 2012 to March 2013. Although the community welcomed replacing the bridge, residents were concerned about how the demolition and construction would affect their health. They voiced these concerns at a community council meeting attended by a Cincinnati Health Department public health nurse, a pediatrician (N.C.N.), and a community professional (C.I.) approximately 5 months before the scheduled demolition.
In response to the community request for help through the public health nurse, the Cincinnati Health Department performed a health impact assessment and provided lead mitigation recommendations to city and state traffic departments, contractors, and neighborhood residents. The health impact assessment process included tours of the neighborhood with the Cincinnati Health Department, parents, and advocates. The University of Cincinnati has a Community Outreach and Engagement Core, which is codirected by members of the project team (E.N.H., N.C.N.), in its P30 Environmental Health Sciences Center. One function of the Community Outreach and Engagement Core is to translate environmental health research for community outreach. Using methods adapted from community-based participatory research, 18,19 we implemented a community–academic partnership to communicate the recommendations from the health impact assessment for neighborhood residents. Our group had previously developed a community–academic partnership to address environmental health risk communication for rural Appalachia. 20 During an initial community meeting, one community member expressed concern that residents were being studied to obtain a grant. This community had previously been studied by academics, and the community did not see the benefit. The partnership addressed this distrust of academics by showing respect for each community member’s expertise and acknowledging the community’s history. Additionally, the inclusion of local advocates and trusted organizations in the partnership was intended to increase community comfort.
We describe the process for engaging residents, the lessons learned from creating this partnership, and the ongoing work that stemmed from this partnership. We show how a community–academic partnership helped develop protection and outreach strategies to prevent lead exposure in a community at risk for lead exposure from a demolition project.
Methods
Health Impact Assessment Process and Partnership Building
During the spring and summer of 2012, the Cincinnati Health Department conducted the health impact assessment using published methods 21 ; a member of the Community Outreach and Engagement Core (S.E.) served as liaison to the health impact assessment committee and provided input on the community outreach plan. Briefly, the Cincinnati Health Department screened the project with community input (health concerns about the bridge demolition), identified health effects to consider (lead exposure), assessed risks and benefits, and made recommendations (monitor for airborne lead levels, modify steel cutting practices, provide residents with tacky mats, notify residents of housekeeping protocols, and notify residents of demolition activities). 22 Tacky mats, which consist of a pad of 30 clear plastic sheets with built-in adhesive (Sticky Mats, www.sticky-mats.com), are used in occupational and construction environments to prevent the spread of contaminated dusts. To develop and implement the outreach plan, the Cincinnati Health Department invited multiple partners to join the community–academic partnership, including The Arc of Hamilton County and Southwest Ohio, Talbert House, Urban Appalachian Council, Santa Maria Community Services, and the Pediatric Environmental Health Specialty Unit at Cincinnati Children’s Hospital Medical Center. These representatives brought diverse skills to the project, including knowledge of pediatric environmental health, expertise in lead-poisoning prevention, writing, graphic design, health communication, firsthand knowledge of the community members, and experience communicating scientific data to lay audiences. This educational project was deemed human subjects exempt by the University of Cincinnati Institutional Review Board.
Partners met and created prototype communication materials and then modified them to make them easy to understand by community members of various and potentially low education levels. One example was a refrigerator magnet. In its first version, the information was presented as a fact sheet containing 10 recommendations. The final version, “Keep Demolition Dust Down” (Figure), was a refrigerator magnet that presented 4 key recommendations (using alliteration of the letter d to enhance recollection) and 4 simple illustrations. A reader-friendly “Demolition Dust Fact Sheet” was based on materials developed by the Johns Hopkins Center in Urban Environmental Health.
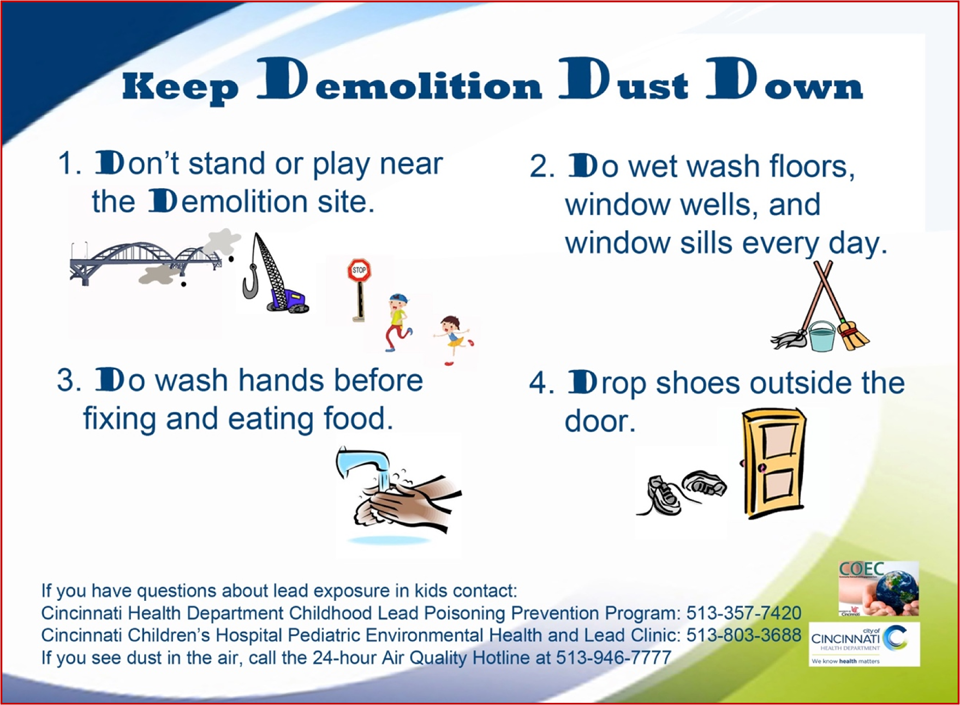
Refrigerator magnet distributed to community members at outreach activities related to lead-poisoning prevention during a bridge demolition project, Cincinnati, Ohio, 2012
Community Outreach Activities
Talbert House, a trusted nonprofit organization in the community, hosted 7 community sessions in fall 2012 focused on the demolition at which members of the community–academic partnership met with residents of the neighborhood. These meetings were held at 4 locations throughout the community to teach residents how to protect their families from the hazards of lead dust. Typically, meetings consisted of a brief expert-led discussion of the bridge demolition followed by an open forum with community members. Based on partner input, community meetings incorporated presentations, demonstrations, and interactive discussions. Presenters dressed casually, walked about the audience, and used easy-to-understand language, avoiding technical jargon or fear-mongering language. One member of the team (N.C.N.) presented a brief overview of the effects of lead on children using hand-drawn illustrations on flip charts followed by a question-and-answer session. Another team member (W.M.) instructed the families on the use of tacky mats: place the pads on a flat, dry area immediately outside the entrance of their home, step on the mats as they walk into the home, and pull off the top sheet when it becomes dusty to expose a new sheet below it. At meeting’s end, residents were offered tacky mat kits by members of the team and asked to complete a feedback questionnaire before they left the meeting. Meetings were designed to support parental involvement and included free childcare, a light meal (sandwiches), and $10 gift cards to a grocery store.
Statistical Analysis
A total of 7 community sessions were held, and 5-40 residents attended each session; in all, 107 unique residents submitted fully or partially completed feedback questionnaires. We entered responses from feedback questionnaire forms into Microsoft Excel. We coded free-text responses to open-ended questions for key concepts (eg, health, child/children, lead). We calculated descriptive statistics and mapped the addresses of households that received tacky mats using Epi Info 7. 23
Outcomes
Educational Materials
Community organizations distributed >100 demolition fact sheets to residents by including the fact sheet in the community newsletter and by leaving fact sheets at key sites in the community (eg, schools, community centers). Eighty-six tacky mat kits were distributed. The 107 residents who submitted questionnaires represented 53 unique addresses; some families lived in the same building but in different apartments. Therefore, although a single street address could be counted multiple times, it could represent different households. Eighty percent (68 of 86) of the tacky mat kits were distributed to families who lived within 1600 feet of the bridge. A total of 250 refrigerator magnets were distributed through educational sessions or left unattended in public places (eg, schools, community centers).
Feedback Questionnaire
The 2 most commonly reported sources of information about the bridge demolition were word of mouth and a community newsletter that was photocopied and hand-delivered by community members, under the auspices of the Lower Price Hill Community Council. Seventy percent (57 of 81) of respondents were concerned that the bridge demolition could affect their health. On a 5-point Likert-type scale (1 = not at all concerned and 5 = extremely concerned), the mean (standard deviation) level of their health concerns was 4.0 (1.2). The most commonly reported concerns were about lead, dust, and their children’s health. About half (51%, 40 of 78) of respondents had not completed high school (Table); staff members helped respondents complete the feedback questionnaire, if needed. Anecdotally, this assistance improved rapport between community members and project staff members.
Responses to 2 questions on a feedback questionnaire, administered at community training sessions on tacky mat usage, on residents’ concerns about the potential health effects of a bridge demolition project and how to protect families from the hazards of lead dust, Cincinnati, Ohio, 2012a
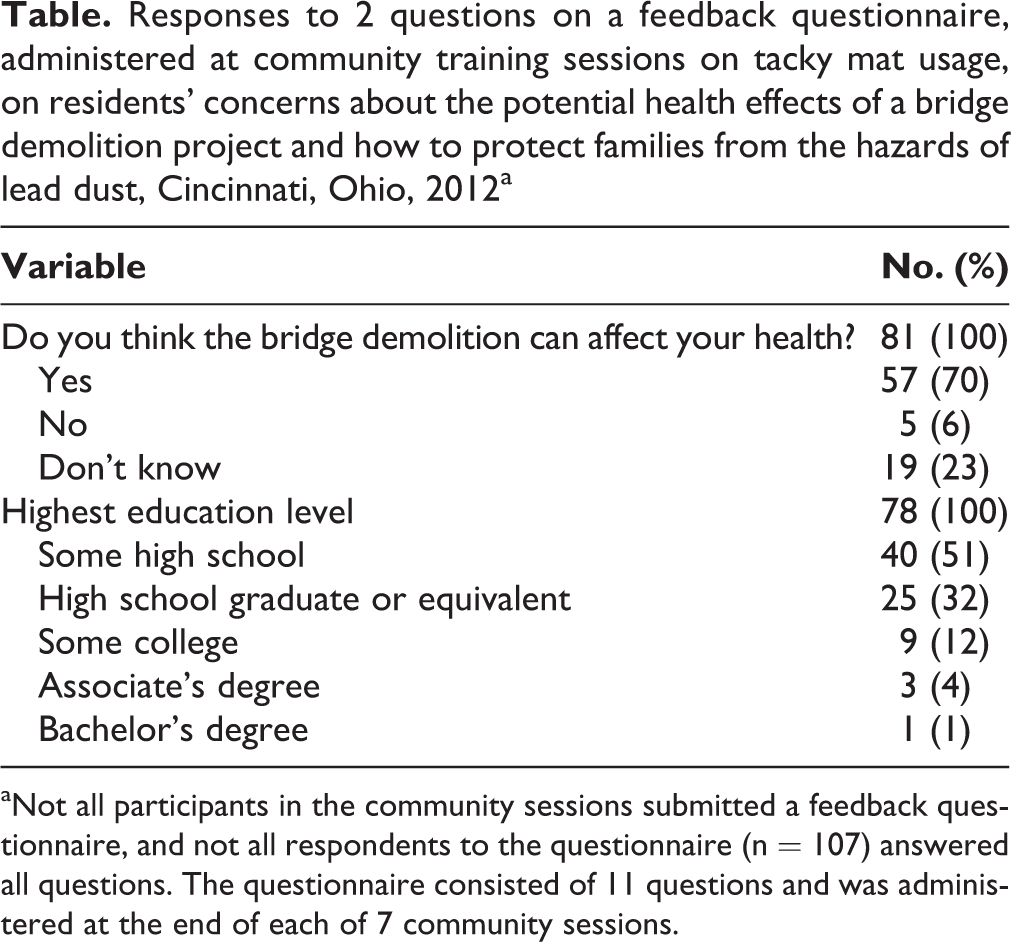
aNot all participants in the community sessions submitted a feedback questionnaire, and not all respondents to the questionnaire (n = 107) answered all questions. The questionnaire consisted of 11 questions and was administered at the end of each of 7 community sessions.
Of 82 respondents who provided feedback on the “Keep Demolition Dust Down” information sheet, 95% of respondents indicated that it clearly explained the dangers of demolition, 98% indicated that it clearly explained the potential lead exposure in the home, and 96% indicated that after reading the information sheet, they knew who to contact with more questions or for more information.
Lessons Learned
The Centers for Disease Control and Prevention recommends conducting a health impact assessment when planning for transportation projects. 24 Our project demonstrated that a community–academic partnership can help deliver the health messaging necessary to implement recommendations from a health impact assessment. The interactive style of our approach contributed to our success: participants reported that training sessions and educational materials were understandable, and tacky mat kits were distributed to residents living in the high-risk area near the bridge. In an evaluation of health impact assessments in the United States, Bourcier et al 25 reported that creating a compelling message tailored to community members’ needs predicts a successful health impact assessment; however, the process for creating this message has not been well described. Our approach illustrates one method for creating a compelling message.
To account for a range of literacy levels, the tacky mat training sessions were interactive and time was provided for questions and answers, thus ensuring that community members understood how to use the mats. To address our concern that written educational materials on lead-poisoning prevention may not be understandable, members of the community–academic partnership created a lead-poisoning prevention video (https://vimeo.com/mjrmedia/leadfreekids) that was used by public health home visitors and in clinics citywide.
The Cincinnati Health Department funded the health impact assessment, whereas the community–academic partnership activities were funded separately, which allowed pooling of financial and human resources across organizations to develop and disseminate the findings. Local funding also allowed flexibility in the kinds of community events that could be funded. For example, respondents received a free meal and gift card at events, which has been cited as a predictor of success. This partnership allowed us to disseminate the recommendations using an implementation plan that was created using community input, another cited factor of success. 25 The mix of funding for this project (local, federal government, and foundations) allowed for substantial flexibility in its implementation, limited the financial burden for individual groups, and allowed partners to leverage their resources.
Despite community involvement in the design process, anecdotal reports from public health nurses suggested that families were not consistently using the tacky mats as instructed. In the future, more rigorous evaluation should be part of the training, and follow-up and ongoing education of community members should be conducted. Lead testing statistics reviewed for this project identified the need for additional lead testing in this neighborhood; a community-based project to address this need is underway.
This community–academic partnership project increased the level of awareness of community groups about sources of lead in the Lower Price Hill neighborhood beyond dust fall from the bridge project. Members of the partnership continue to meet to improve childhood lead-poisoning prevention throughout the city and take steps to build trust with the community, by continuing to respond to requests from the community about lead-poisoning prevention.
We demonstrated that a community–academic partnership can leverage the expertise of public health, community-engaged methods, researchers, and content experts to aid a community affected by infrastructure renewal. With the current interest in renewing aging infrastructure, many communities may be at risk for these same hazards, and our approach may have broad applicability.
Footnotes
Authors’ Note
Information from this study was presented at the Ohio Healthy Homes Conference, Columbus, Ohio, April 18, 2013 (platform presentation); and the International Society of Environmental Epidemiology, Seattle, Washington, August 25, 2014 (poster presentation).
Acknowledgments
The US Environmental Protection Agency supports the Pediatric Environmental Health Specialty Unit by providing funds to the Agency for Toxic Substances and Disease Registry under Inter-Agency Agreement #DW-75-92301301-0. Neither the US Environmental Protection Agency nor the Agency for Toxic Substances and Disease Registry endorses the purchase of any commercial products or services mentioned in Pediatric Environmental Health Specialty Unit publications. The authors thank Florence Fulk, PhD, Allison Parsons, PhD, and Marilyn Goldfeder, RN, MPH, of the Lower Price Hill Community Council; Santa Maria Community Services; Urban Appalachian Council; St. Michael’s Church; Ohio Healthy Homes and Lead Poisoning Prevention Program; and The Johns Hopkins Center in Urban Environmental Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The University of Cincinnati Center for Environmental Genetics–Community Outreach and Engagement Core NIEHS P30-ES006096, City of Cincinnati general funds, Dater Foundation, and Crosset Family Foundation. This article was supported by the Association of Occupational and Environmental Clinics and funded (in part) by the cooperative agreement award #1U61TS000118-03 from the Agency for Toxic Substances and Disease Registry.