
Abstract
The objective of this study was to evaluate the satisfaction with, and the feasibility and effectiveness of, a public health detailing project focused on increasing routine human immunodeficiency virus (HIV) screening of people aged 13-64 by primary care providers working in areas of Baltimore City, Maryland, with high rates of HIV transmission (defined as a mean geometric viral load of ≥1500 copies/mL per census tract). In public health detailing, trained public health professionals (ie, detailers) visit medical practice sites to meet with providers and site staff members, with the intention of influencing changes in clinical practice policy and/or behavior. During 2014, detailers made personal visits and gave HIV Testing Action Kits containing maps, educational and guideline documents, and resource lists to 166 providers and office managers at 85 primary care sites. At follow-up, 88 of 91 (96.7%) providers and 37 of 38 (97.4%) clinic managers were very satisfied or satisfied with the project. Of the 79 sites eligible at follow-up (ie, those that had not closed or merged with another practice), 76 (96.2%) had accepted at least 1 HIV Testing Action Kit, and 67 of 90 (74.4%) providers had increased their HIV screening. Public health detailing projects can be used to educate and support providers, establish relationships between providers and local health departments, and disseminate public health messages.
The Centers for Disease Control and Prevention (CDC) estimated that as of 2015, 1.1 million people aged ≥13 in the United States were living with human immunodeficiency virus (HIV) infection, 15% of whom were unaware of their infection. HIV prevalence is particularly high for black men and women and for men who have sex with men. 1
To address lack of awareness of infection and disparities among demographic groups, CDC issued revised recommendations in 2006 that included routine, opt-out HIV screening for all people aged 13-64, regardless of risk factors. 2 In 2013, the US Preventive Services Task Force assigned an A grade to HIV screening, indicating a high certainty that the net benefit is substantial. 3
Recent US health care reform has changed the way that health services are delivered and paid for, which in turn may affect where people seek care, particularly for sexually transmitted diseases (STDs). In Massachusetts, after the institution of mandatory health insurance coverage in 2006, free STD services (including HIV screening at STD clinics) were eliminated because of state funding cuts. 4 Subsequently, a 2009 study in Massachusetts reported that STD visits increased by 107% to primary care clinics and decreased by 20% to local STD clinics. 5 Nationally, passage of the Patient Protection and Affordable Care Act in 2010 resulted in expanded public and private health insurance coverage and brought into question whether the federal government should continue providing publicly funded free STD services. 6 –9 In addition, implementation of the Affordable Care Act led to an increase in primary care visits by previously uninsured and underinsured people, those at greatest risk for HIV. 10 –12 Routine HIV screening conducted at both primary care sites and STD clinics would create a safety net for the US population.
Public health organizations could help increase routine HIV screening by primary care providers through the use of public health detailing, an approach developed by the New York City Department of Health and Mental Hygiene and similar to academic detailing. 13,14 Detailing draws from a pharmaceutical industry model in which trained public health or academic professionals (ie, detailers) visit medical practice sites for one-on-one meetings with providers and site staff members, building relationships over time with the intention of influencing changes in clinical practice policy and/or behavior. Detailing has been shown to be more effective in changing clinical practice and provider behavior than programs that rely solely on distributing materials without in-person contact. 15
Purpose
The objective of this study was to evaluate satisfaction with, feasibility of, and effectiveness of a public health detailing project that aimed to increase routine HIV screening among community primary care providers in areas with high rates of HIV transmission in Baltimore City, Maryland. Baltimore City is located in the Baltimore-Towson metropolitan statistical area, which faced one of the most severe HIV epidemics in the United States: an HIV diagnosis rate of 31.2 per 100 000 population in 2012, compared with 1.6 for the United States and 3.1 for Maryland. 16 During the same period, this area faced considerable racial/ethnic disparities: HIV was diagnosed in 85.6 black people per 100 000 population, compared with 8.1 non-Hispanic white people per 100 000 population. 17
Methods
The Protect Baltimore Campaign was a public health detailing project conducted by the Baltimore City Health Department (BCHD) in partnership with the Johns Hopkins University Center for Child and Community Health Research in 2014. The project involved multiple public health detailing visits to primary care sites in Baltimore City. The main objective of these visits was to encourage providers to increase their routine HIV screening of people aged 13-64. We evaluated the project using surveys at baseline and at 6-month follow-up. The project was approved by the Johns Hopkins University School of Medicine Institutional Review Board.
Site Identification and Selection
The project targeted primary care providers who were able to order an HIV test, including nurse practitioners, physician assistants, and physicians. To select primary care providers and sites for the project, the project coordinator compiled a list of all primary care providers and sites in Baltimore City using several sources, including local hospital provider directories, searchable insurance plan websites, and STD public health surveillance data. The project coordinator then refined the list through telephone calls, internet searches, site visits, geocoding (ie, converting addresses into geographic coordinates to place markers on a map), and block-by-block canvasing. This process ensured that all providers included in the project were located in Baltimore City and were actively delivering primary care services. Eligible primary care sites included hospital outpatient clinics, Federally Qualified Health Centers, community health centers, and group and individual primary care practices.
From this list, the project coordinator selected only the 85 primary care sites that were located in areas with high rates of HIV transmission. To identify these areas, we obtained HIV viral load test results from public health surveillance data on 2100 people who were diagnosed as HIV positive between January 2009 and January 2014. Of those, we identified 1313 (62.5%) who had at least 1 viral load test result and 1 geocodable address. We then aggregated the viral load test results for people residing in each US Census tract in Baltimore City, and we calculated a geometric mean of the viral loads for each census tract. We used the geometric mean rather than the arithmetic mean because it is less sensitive to extreme outliers. Next, we generated community viral load maps, classifying census tracts into 1 of 3 community viral load geometric mean categories: high (≥1500 copies/mL), low (<1500 copies/mL), and no viral load information. We used these categories as a proxy for HIV transmission risk. We chose the cutoff of 1500 copies/mL based on work by Quinn et al, who reported no HIV transmission events among discordant couples (ie, couples in which 1 partner is HIV positive and the other is HIV negative) in which the HIV-positive partner had a viral load <1500 copies/mL. 18 Baltimore City had 200 census tracts, 110 (55%) of which were categorized as areas with high rates of HIV transmission.
HIV Testing Action Kit
We used a multistep process to create an HIV Testing Action Kit (Figure 1). We met with personnel from the New York City Department of Health and Mental Hygiene, who shared the materials that they use in their public health detailing work. We asked students from the Maryland Institute College of Art to devise a compelling design. We also conducted 2 informal focus groups involving 5-7 primary care and infectious disease providers, from whom we received feedback on an initial version of the kit. In addition, we asked personnel at AIDS Education Training Centers, local HIV experts, and other primary care providers to review the kit and help us formulate the project’s key message.
HIV Testing Action Kit logo (upper left), list of items (lower left), and front cover (right) for the Protect Baltimore campaign, a public health detailing demonstration project, Baltimore City, Maryland, 2014. Detailing draws from a model in which trained public health or academic professionals (ie, detailers) visit medical practice sites for one-on-one meetings with providers and site staff members, building relationships over time with the intention of influencing changes in clinical practice policy and/or behavior. Abbreviation: HIV, human immunodeficiency virus.
The HIV Testing Action Kit included the following: Overviews of HIV in Baltimore and Maryland HIV-related laws Maps showing average annual HIV diagnosis rates, HIV mortality rates, and all-cause mortality rates in Baltimore City neighborhoods Recommendations from CDC and US Preventive Services Task Force on routine HIV screening (including rationale for and frequency of screening) Description of types of HIV tests HIV test result interpretation and scripts for communicating test results to patients Scripts to use when talking with patients about routine HIV screening and during HIV pre- and posttest counseling Current Procedural Terminology and International Classification of Diseases codes to use for routine HIV screening Information about linkage-to-care programs (for connecting newly diagnosed HIV-positive people to HIV care), partner notification services (for HIV-positive people and their sexual or needle-sharing partners), and notifiable disease reporting List of local HIV-related referrals and resources (including HIV treatment providers) Information for specific populations (ie, adolescents and older adults) and about specific services (ie, domestic/intimate partner violence, HIV prevention and trials, insurance assistance, legal services, medication assistance, and mental health support)
In addition to the HIV Testing Action Kit, we developed a Quick Reference Card for providers and a Learn Now brochure for patients. The Quick Reference Card provided a script for providers to use when offering the HIV test and requesting informed consent, an algorithm to use for HIV screening decisions, and relevant International Classification of Diseases and Current Procedural Terminology codes to use during patient visits. It also contained key steps for providers to take to connect patients to treatment or to partner notification services as well as to report a new HIV diagnosis to the BCHD. The Learn Now patient brochure provided basic information about HIV and HIV testing, HIV test result interpretation, and HIV prevention. We also offered providers and clinics extra Maryland Confidential Morbidity Report forms (to submit required notifiable disease reports of any new HIV diagnoses to the Maryland State Health Department), pamphlets about STD prevention and treatment, posters, and condoms.
Project Implementation
For this project, we hired 2 public health detailers who were personable, had interest in fieldwork, and could clearly communicate health information. The detailers received 3 weeks of formal training organized by the project coordinator that involved shadowing a nurse researcher involved in implementing routine HIV screening, taking a weeklong HIV course, participating in provider-patient role-playing, performing a detailed review of HIV testing recommendations, reading about HIV prevention and screening, and viewing detailing webinars by pharmaceutical companies. The detailers also received training at weekly meetings during the remainder of the project.
The detailers began their work in January 2014 with a goal of reaching all 85 sites during the first 6 months of the project. Prior to any site visits, the city health commissioner sent a letter to all primary care providers and clinic managers introducing the project and reviewing the importance of HIV screening. The detailers then made scheduled and unscheduled visits to the sites. Upon arriving at sites, the detailers introduced themselves as BCHD representatives, determined the number of providers at that site, requested to meet with providers and clinic managers, and conducted a brief baseline survey. Then, the detailers offered the HIV Testing Action Kit to the providers and explained the project’s primary objective (ie, to increase routine HIV screening among those aged 13-64) to the providers, clinic managers, and any other interested staff members.
At the end of each site visit, the detailers asked providers to commit to some level of action, ranging from reviewing the kit and sharing materials with their patients to fully implementing routine screening for all eligible patients in their practices. The detailers completed field notes after each visit describing the site’s needs, questions, and receptiveness to the project. During the 6 months after each initial clinic site visit, the detailers returned to the sites to answer questions, offer additional materials, and inform other clinic personnel about the project. The number of visits to each site varied and depended on how receptive the providers and clinic managers were to the project.
Evaluation
The detailers conducted baseline surveys at initial site visits from January through June 2014. The surveys were conducted face-to-face with providers and clinic managers, and the detailers entered responses into an electronic database using tablets. The goal for detailers was to interview at least 75% of providers at each site. The detailers then conducted follow-up surveys at eligible sites (defined as those that had not closed or merged with another practice) with the same interviewees about 6 months after the baseline surveys, from July through December 2014.
The baseline and follow-up surveys included questions about provider and patient demographic characteristics, patient volumes (numbers of patient visits and unique patients) at each site, and 3 outcome measures for the detailing project: satisfaction, feasibility, and effectiveness. We assessed satisfaction with the project among providers and clinic managers by asking 1 question with 5 possible responses (very satisfied, satisfied, neither satisfied nor dissatisfied, dissatisfied, and very dissatisfied). We measured the project’s feasibility using the number of sites that detailers were able to visit and the number of sites accepting at least 1 HIV Testing Action Kit. We measured the effectiveness of the project using the number of HIV Testing Action Kits used (among those sites accepting a kit), the number of providers reporting an increase in or an intention to increase HIV testing or other activities related to routine HIV screening, and the number of providers who requested additional support or resources to help with routine HIV screening. We assessed effectiveness by having the detailers rank providers on their HIV screening readiness to test at baseline and follow-up, using a 6-point scale: 0, refused to participate; 1, no interest; 2, some/minimal interest; 3, interested; 4, interested/in process of implementing; and 5, already routinely screening for HIV.
Statistical Methods
We tabulated data on demographic characteristics and outcomes as frequencies, proportions, means, and standard deviations. We compared baseline outcome measures with 6-month follow-up outcome measures using t tests for continuous values and χ 2 tests for proportions. We also calculated 95% CIs when appropriate and considered P ≤ .05 to be significant. We conducted all analyses using Stata release 10. 19
Outcomes
Study Population
Initially, 85 primary care sites met the eligibility criteria as a practicing site in an area with a high rate of HIV transmission in Baltimore City (Figure 2). At follow-up, 79 (92.9%) sites remained eligible, and 6 had closed or merged with another clinic.
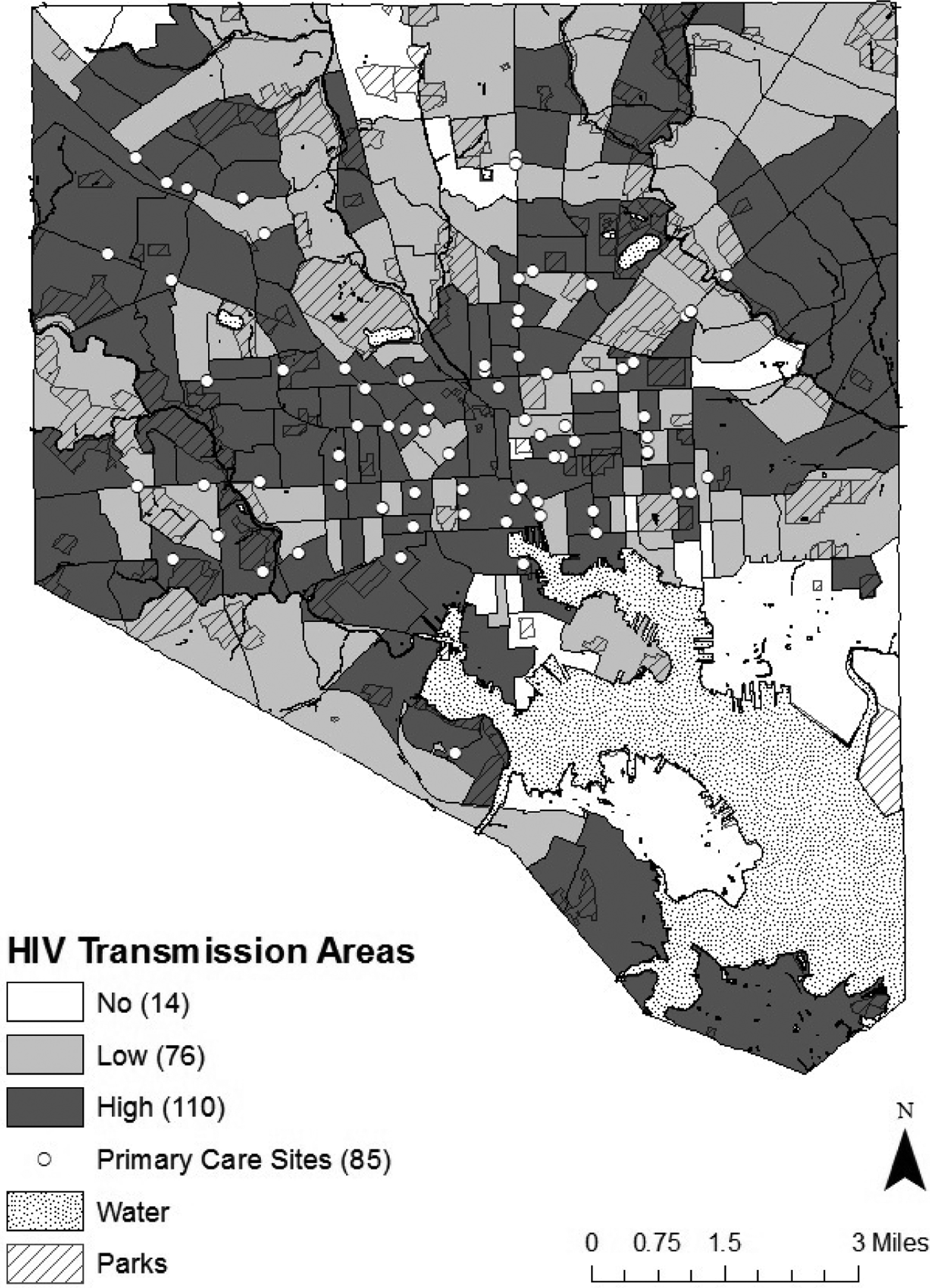
Map of Baltimore City, Maryland, used for a 2014 human immunodeficiency virus (HIV) screening public health detailing project, showing 2000 US Census tracts and 85 primary care sites in areas with high rates of HIV transmission, based on public health surveillance data from January 2009 to January 2014. Detailing draws from a model in which trained public health or academic professionals (ie, detailers) visit medical practice sites for one-on-one meetings with providers and site staff members, building relationships over time with the intention of influencing changes in clinical practice policy and/or behavior. US Census tracts (roughly equivalent to neighborhoods) were classified into 3 HIV transmission area categories, based on the geometric mean of aggregated HIV viral loads of HIV-diagnosed people: high (≥1500 copies/mL), low (<1500 copies/mL), and no viral load information. 18 Public health surveillance data consisted of HIV viral load test results from 1313 people (of a total of 2100 people who were diagnosed as HIV positive) who had at least 1 viral load test result and 1 geocodable address, between January 2009 and January 2014 in Baltimore City. Data source: Maryland Department of Health and Mental Hygiene, Baltimore City Health Department.
Providers
A total of 208 eligible primary care providers practiced at the 85 sites; detailers conducted baseline surveys with 166 (79.8%) of those providers. The providers completing baseline surveys included 134 (80.7%) physicians, 20 (12.0%) nurse practitioners, 8 (4.8%) physician assistants, and 4 (2.4%) others. Of the 166 providers, 59 (35.5%) reported being in practice for ≤10 years and 106 (63.9%) for >10 years; 1 provider did not answer the question.
Of the 166 providers who completed baseline surveys, 138 (83.1%) were eligible for a follow-up visit; 28 (16.9%) providers had retired or left practice. Of the 138 providers, 92 (66.7%) were surveyed, and 46 (33.3%) declined to participate or could not be contacted.
Clinic Managers
Detailers completed baseline surveys of 68 of 79 (86.1%) eligible clinic managers: 23 (33.8%) practice managers, 17 (25.0%) lead physicians, 6 (8.8%) chief operating officers, 2 (2.9%) in management, 1 (1.5%) physician supervisor, and 19 (27.9%) others. Of the 68 managers eligible, detailers surveyed 39 (57.4%) at follow-up; 29 (42.6%) managers declined to participate or could not be contacted.
Patients
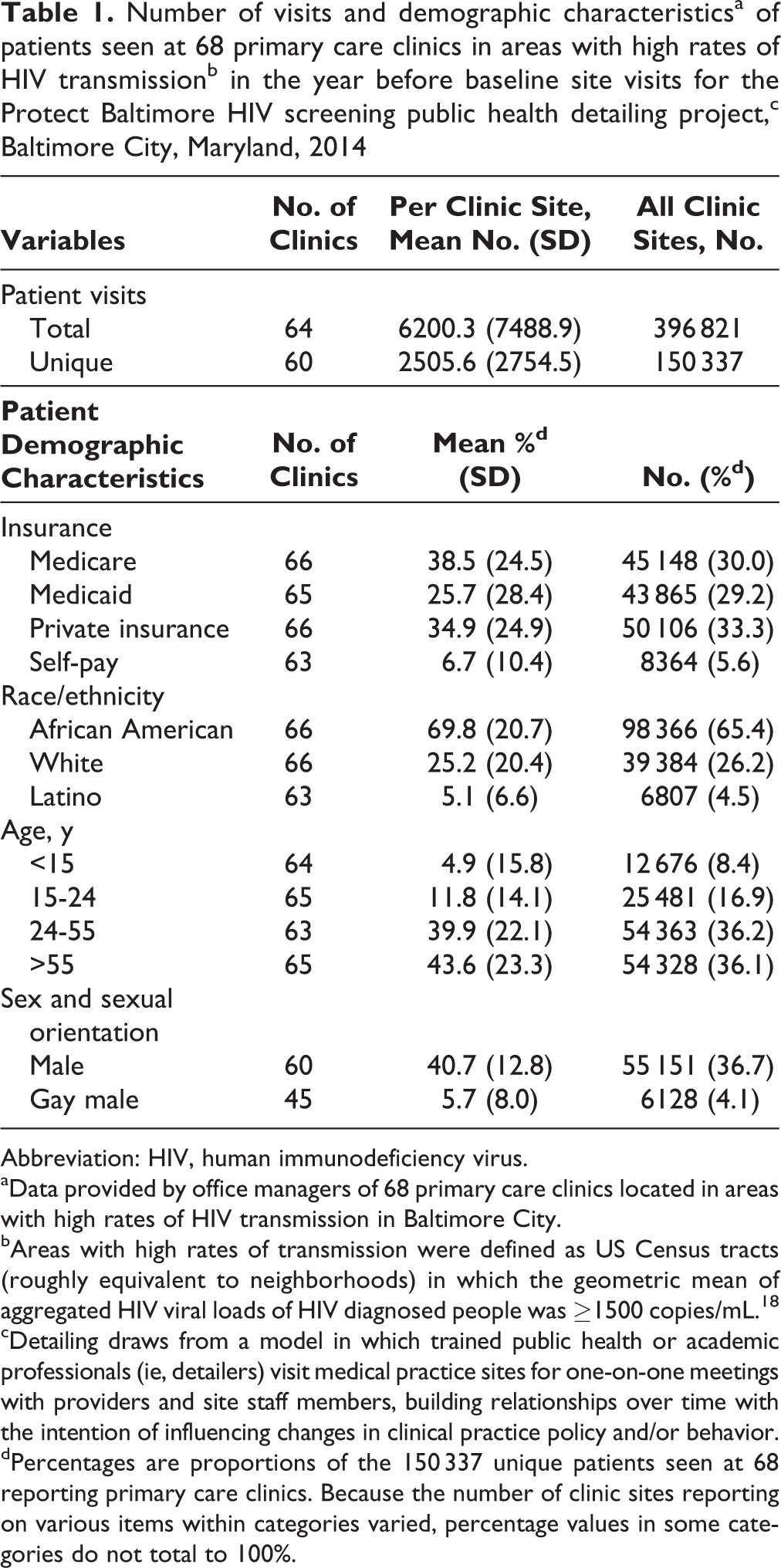
The 68 clinic managers who completed baseline surveys reported an aggregated total of 396 821 patient visits and 150 337 unique patients receiving care at their sites in the year before the baseline detailing site visits (Table 1). The managers reported that of all unique patients, 89 013 (59.2%) had Medicare or Medicaid; 98 366 (65.4%) were African American; 79 844 (53.1%) were aged 15-55; 55 151 (36.7%) were male; and 6128 (4.1%) were gay males.
Number of visits and demographic characteristicsa of patients seen at 68 primary care clinics in areas with high rates of HIV transmissionb in the year before baseline site visits for the Protect Baltimore HIV screening public health detailing project,c Baltimore City, Maryland, 2014
Abbreviation: HIV, human immunodeficiency virus.
aData provided by office managers of 68 primary care clinics located in areas with high rates of HIV transmission in Baltimore City.
bAreas with high rates of transmission were defined as US Census tracts (roughly equivalent to neighborhoods) in which the geometric mean of aggregated HIV viral loads of HIV diagnosed people was ≥1500 copies/mL. 18
cDetailing draws from a model in which trained public health or academic professionals (ie, detailers) visit medical practice sites for one-on-one meetings with providers and site staff members, building relationships over time with the intention of influencing changes in clinical practice policy and/or behavior.
dPercentages are proportions of the 150 337 unique patients seen at 68 reporting primary care clinics. Because the number of clinic sites reporting on various items within categories varied, percentage values in some categories do not total to 100%.
Outcome Measures
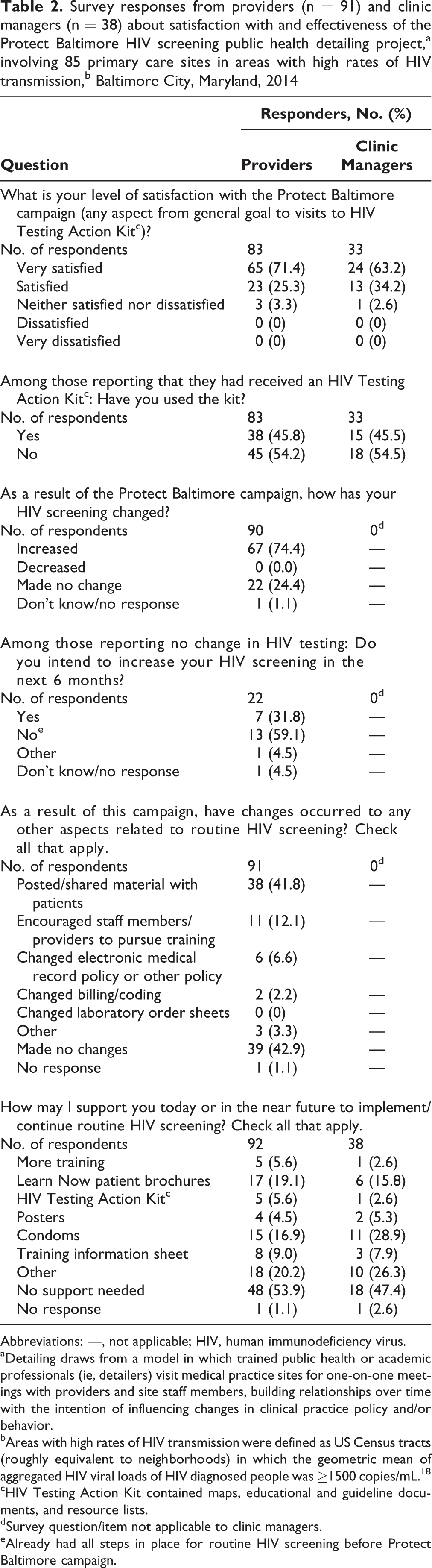
Based on responses from the 91 providers and 38 clinic managers who completed both baseline and follow-up surveys, 88 (96.7%) providers and 37 (97.4%) managers reported being very satisfied or satisfied with the project (Table 2). Initially, the 2 detailers (together or independently) visited all 85 eligible sites. Of the 79 sites that remained eligible at follow-up, 76 (96.2%) had accepted at least 1 HIV Testing Action Kit; a total of 281 kits were delivered to the sites.
Survey responses from providers (n = 91) and clinic managers (n = 38) about satisfaction with and effectiveness of the Protect Baltimore HIV screening public health detailing project,a involving 85 primary care sites in areas with high rates of HIV transmission,b Baltimore City, Maryland, 2014
Abbreviations: —, not applicable; HIV, human immunodeficiency virus.
aDetailing draws from a model in which trained public health or academic professionals (ie, detailers) visit medical practice sites for one-on-one meetings with providers and site staff members, building relationships over time with the intention of influencing changes in clinical practice policy and/or behavior.
bAreas with high rates of HIV transmission were defined as US Census tracts (roughly equivalent to neighborhoods) in which the geometric mean of aggregated HIV viral loads of HIV diagnosed people was ≥1500 copies/mL. 18
cHIV Testing Action Kit contained maps, educational and guideline documents, and resource lists.
dSurvey question/item not applicable to clinic managers.
eAlready had all steps in place for routine HIV screening before Protect Baltimore campaign.
Of the 83 providers and 33 clinic managers who reported receiving an HIV Testing Action Kit, 38 (45.8%) providers and 15 (45.5%) managers indicated in their follow-up surveys that they had used materials from the kit. Of 90 responding providers, 67 (74.4%) had increased HIV screening (Table 2). Among the 22 (24.4%) providers indicating no change in their HIV screening practices, 7 (31.8%) reported that they intended to increase HIV screening in the next 6 months and 13 (59.1%) said that they were already conducting routine screening before the project.
Of 91 responding providers, 57 (62.7%) reported that they had made other changes related to routine HIV screening as a result of the project, including posting or sharing material with patients, encouraging staff members or other providers to pursue training, and modifying their electronic medical record system (ie, adding an HIV screening prompt), billing or coding practices, and other related policies. Of 92 providers and 38 clinic managers responding to an inquiry about additional ways that they might be supported in implementing or continuing routine HIV screening, 43 (46.7%) providers and 19 (50.0%) managers reported support that they would welcome, including additional training, Learn Now brochures, HIV Testing Action Kits, posters, condoms, and training information sheets.
The detailers also ranked providers by their readiness to test, at baseline and follow-up (Table 3). A total of 156 providers were ranked at baseline, and 118 were ranked at baseline and follow-up. Of those, 79 (67.2%) providers increased their readiness to test (ie, moved up at least 1 point in their ranking); 34 (29.0%) did not change; and 5 (3.8%) decreased their readiness to test. The average increase in ranking was significant (1.1; 95% CI, 0.9-1.3; P < .001).
Primary care providers’ readiness to screen for HIV,a at baseline (January–June 2014) and follow-up (July–December 2014), in 85 primary care sites in areas with high rates of HIV transmission,b during an HIV screening public health detailing project,c Baltimore City, Maryland
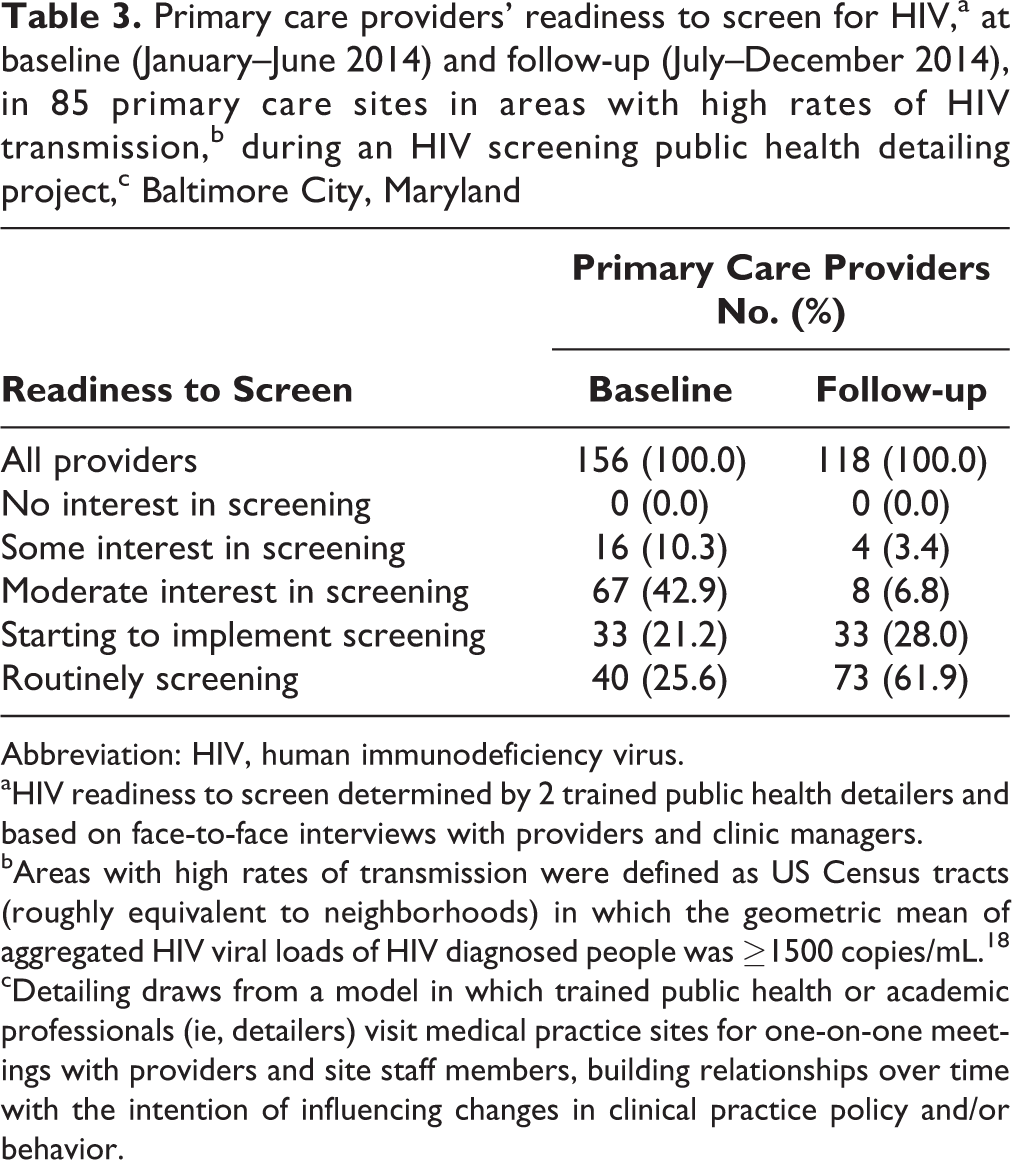
Abbreviation: HIV, human immunodeficiency virus.
aHIV readiness to screen determined by 2 trained public health detailers and based on face-to-face interviews with providers and clinic managers.
bAreas with high rates of transmission were defined as US Census tracts (roughly equivalent to neighborhoods) in which the geometric mean of aggregated HIV viral loads of HIV diagnosed people was ≥1500 copies/mL. 18
cDetailing draws from a model in which trained public health or academic professionals (ie, detailers) visit medical practice sites for one-on-one meetings with providers and site staff members, building relationships over time with the intention of influencing changes in clinical practice policy and/or behavior.
Lessons Learned
We demonstrated the effectiveness of the project with the findings that 74.4% of providers stated that their screening for HIV increased as a result of the project and that 67.2% of providers increased their readiness to test. Others have shown the benefits of public health detailing in assisting with the implementation of public health recommendations in clinical settings. 13 –15,20
Additional benefits resulted from this project. First, BCHD developed new connections with primary care sites. Several providers mentioned that this project was their first-ever direct contact with BCHD. This finding suggests that public health detailing may have the additional benefit of promoting relationships between local health departments and primary care providers in their jurisdictions. The relationships developed during this project will aid in the success of the Protect Baltimore Campaign and in future public health detailing and communication efforts.
The project also allowed us to obtain information on the practice patterns, familiarity with guidelines, and needs of providers and managers. For example, the amount of HIV screening and the level of awareness of recommendations varied among providers. Also, many providers had concerns about screening, questions about insurance, and interest in changing their practices if additional support were available. Furthermore, based on outcomes data, we identified 3 primary care sites that needed special assistance, and we obtained additional funds to provide intensive support to those sites. Another benefit of the project was the cooperation of regional and state academic institutions, our state health department, a managed care organization (Amerigroup), community-based groups, and other entities involved in HIV prevention and care—stakeholders that do not frequently collaborate.
Limitations
This project had several limitations. First, providers’ and clinic managers’ availability for lengthy engagement with detailers was limited, which may have limited detailers’ ability to gather key information. Second, most outcome measures were based on self-reporting by providers and clinic managers, making these data susceptible to reporting biases. Third, the criteria for selecting the detailers and the level of their previous training may not have been optimal. Clinically trained peer detailers might have been more effective in engaging with some providers. Fourth, some detailers were asked to field complaints about the health department or were pressed for information about health department processes or services unrelated to HIV screening. Future detailer training should include instructions on how to handle these complaints and requests.
Public Health Implications
Given the ongoing HIV epidemic, changes in where patients access STD care, and updated laws and policies encouraging more HIV screening, primary care providers need to prioritize routine HIV screening. A public health detailing project can support this goal by educating and supporting providers and by establishing relationships between providers and their local health department. Other jurisdictions might consider using public health detailing for similar efforts to disseminate key public health messages.
Footnotes
Acknowledgments
We gratefully acknowledge members of the New York City Department of Health and Mental Hygiene, who provided guidance on their jurisdiction’s HIV detailing project, and students from the Center for Social Design at the Maryland College Institute of Art for their design work. We are grateful for the guidance and support from the Johns Hopkins AIDS Education Training Center, the University of Maryland AIDS Education Training Center, and the STI/HIV Training and Prevention Center, as well as the hard work of graphic designer Hee Jin Suh. We thank the BCHD, the Baltimore City Disease Control Laboratory, and, in particular, Howard Abegesah, Barbara Bradshaw, Glen Olthoff, Phyllis Burnett, Sheridan Johnson, and Vince Marsiglia, without whom this work could not have been completed. We also thank Arielle Juberg and Daphne Washington from CDC’s public health advisors program. Finally, we thank the many providers and clinical managers in Baltimore City, Maryland, who participated in this project and dedicated themselves to increasing routine HIV screening.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the CDC’s Category C Innovative Demonstration Program (PS12-1201). Andrea Mantsios was supported by the National Institute of Allergy and Infectious Disease (T32 AI050056-12).