
Abstract
Objectives:
Public health detailing is an intervention in which a public health professional visits health care providers to educate them about evidence-based approaches to improve health. The San Francisco Department of Public Health conducted a public health detailing program from 2016 to 2018 to improve sexual health care and preexposure prophylaxis services in the city.
Methods:
We conducted a mixed-methods study to understand the implementation of detailing and explore examples of changes to clinicians’ clinical behaviors. We surveyed 203 clinicians, conducted 60-minute qualitative interviews with 7 clinicians and 4 detailers, and analyzed tracking forms. We used descriptive statistics to assess associations in the surveys. We used qualitative thematic analysis to understand facilitators and barriers to detailing and identify ways to improve the process and identify its potential benefits.
Results:
In interviews, both clinicians and detailers had a favorable view of detailing as a tool to connect health department expertise to clinicians. Detailers cited challenges such as limited clinic time, provider turnover, and policies that limit their access to clinicians. These challenges may attenuate the real-world benefits of detailing. Clinicians offered examples of how detailing altered their behaviors, such as taking sexual health histories, building knowledge and confidence about sexual health, and using health department services. Matched surveys (n = 21) showed preliminary changes to prescribing preexposure prophylaxis.
Conclusions:
Public health detailing is a promising approach to increase clinicians’ knowledge and confidence to offer sexual health care services, build buy-in, and support connection to health departments. Detailing programs require sufficient investment and staff support to build lasting and collaborative relationships between clinicians and public health departments and to assess the impact of the intervention.
Despite an impressive decline in HIV incidence resulting from the availability of preexposure prophylaxis (PrEP), a medication to prevent HIV transmission, success toward getting to zero new HIV infections has been blunted by limited PrEP access and uptake in communities of color and a staggering rise in rates of sexually transmitted infections (STIs). 1 This pattern is particularly evident in San Francisco, where HIV diagnoses decreased from 237 in 2017 to 132 in 2020, 2 while STI rates were among the highest in the country.1,3 New HIV diagnoses increased annually during 2016-2018 among non-Hispanic Black men (25% increase in rate per 100 000 population from 2017 to 2018), Latino men (30.8% increase), trans women, and people experiencing homelessness, 4 the groups least likely to have been prescribed PrEP, compared with non-Hispanic White men who have sex with men (MSM). 5
Several studies suggest that clinician familiarity and norms affect their willingness to prescribe PrEP.6-8 There is a need to engage primary care clinicians in preventing HIV and STIs by integrating high-quality sexual health care services into primary care. 9 Public health detailing (hereinafter, “detailing”) is an intervention in which a public health professional visits health care providers to educate them about evidence-based approaches to improve health while also addressing clinician- and system-level barriers to implementing these recommendations. Detailing’s theory of change has been used across the United States to address various health topics such as obesity and HIV screening.10-13 Detailing presents the opportunity to target clinicians serving populations most at risk of HIV to address disparities. PrEP detailing seeks to increase clinical ability to identify appropriate candidates for PrEP, initiate medication, and offer appropriate follow-up and STI testing. Addressing clinician barriers on these topics is an opportunity to alter clinicians’ clinical behaviors and improve sexual health care services.
From October 2016 through December 2018, the San Francisco Department of Public Health (SFDPH) conducted detailing to promote STI testing and PrEP prescribing. We conducted a mixed-methods study to understand detailing implementation, identify examples of clinicians’ behavior changes, and explore clinicians’ and detailers’ needs. We also explored facilitators and barriers to implementing the detailing program. Although we focused on PrEP detailing, we brought in perspectives of other detailing efforts (eg, hepatitis C virus, rapid treatment of HIV) in San Francisco to root these findings in the broader context of detailing as a clinician- and system-level intervention.
Methods
SFDPH has a Getting to Zero plan to reduce HIV transmissions and HIV-related deaths by 90% before 2025. 14 SFDPH developed detailing programs to support rapid HIV treatment, hepatitis C treatment, and PrEP. This mixed-methods study focused on outcomes of the PrEP detailing program. An external evaluator (K.S.), hired toward the end of the PrEP detailing program, conducted the study. The University of Michigan Health and Behavioral Sciences Institutional Review Board categorized this study as exempt from human subjects review.
SFDPH piloted the PrEP detailing program during the Centers for Disease Control and Prevention’s Project PrIDE (PrEP Implementation, Data to Care, and Evaluation), which funded health departments to implement high-impact HIV prevention strategies. SFDPH sought to reach public and private primary care practices serving key populations and clinics in geographic areas of San Francisco that were reporting elevated numbers of cases of STIs and HIV. Two people, a nurse practitioner and a consultant, were hired at separate time points to conduct PrEP detailing. The nurse practitioner (the lead detailer [A.D.]) had experience in HIV and PrEP, while the consultant had a background in pharmaceutical detailing. The 2 detailers received training on the program’s model and materials and how to address provider barriers. The detailing visits of both the nurse practitioner and the consultant included reviewing key messages, while the nurse practitioner offered additional consultation and technical assistance. The detailers gained access to clinicians by “cold calling” and scheduling visits during clinician meetings or administrative time during an 18-month period.
At the initial sessions with clinicians, detailers conducted a needs assessment to learn about the clinic, clinicians’ practices, and patient populations to understand strengths and gaps in the provision of sexual health care services. Although the original detailing model emphasizes a one-on-one approach in conducting these needs assessments, SFDPH found that this approach was not always feasible in busy clinic settings. In response, the detailers pivoted to group sessions, when needed, to gain access to clinicians. During the assessment, detailers provided information on local HIV and STI epidemiology, briefed clinicians about guidelines, and answered questions. In subsequent visits, detailers explicitly outlined STI and HIV testing algorithms, discussed preventive tools such as PrEP, and assisted with implementation of sexual health care services. Detailers also described SFDPH services, such as the linkage and retention program for people living with HIV (LINCS). 15 Detailers provided the practices with materials, such as HIV and STI testing pocket cards (Figure 1), patient tools (eg, posters describing self-collection of extragenital biological specimens for STI testing), and patient incentives (eg, branded pill holders).
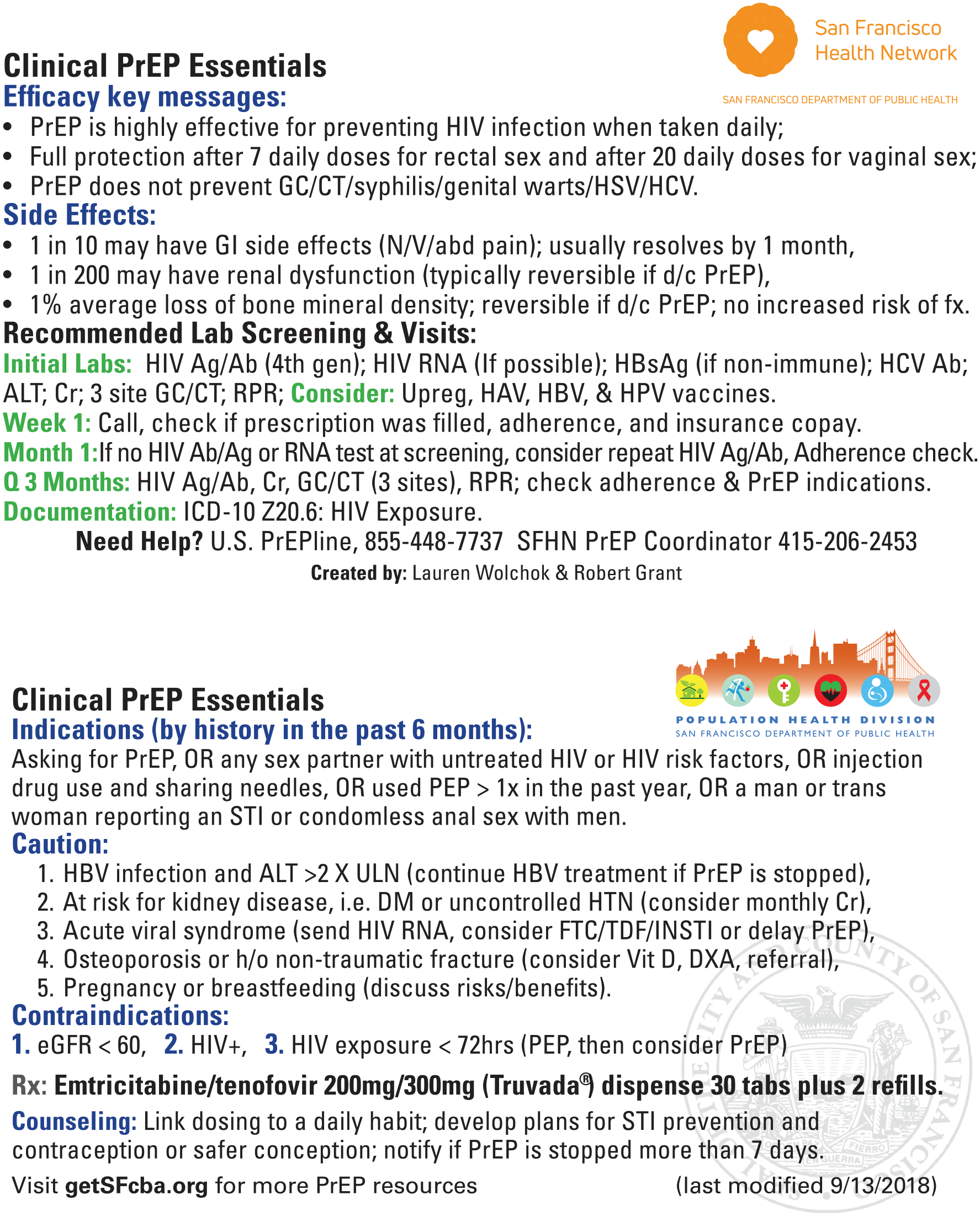
Pocket cards provided to clinicians to support clinical decision making. The San Francisco Department of Public Health conducted a public health detailing program from 2016 to 2018 to improve sexual health care and preexposure prophylaxis (PrEP) services in the city. Public health detailing is an intervention in which a public health professional visits health care providers to educate them about evidence-based approaches to improve health while also addressing clinician- and system-level barriers to implementing these recommendations. Abbreviations: Ab, antibody; Ag, antigen; ALT, alanine transaminase; Cr, creatinine; d/c, discontinue; DM, diabetes mellitus; DXA, dual-energy x-ray absorptiometry; eGFR, estimated glomerular filtration rate; FTC/TDF/INSTI, emtricitabine/tenofovir disoproxil fumarate/integrase strand transfer inhibitors; fx, fracture; GC/CT, gonorrhea/chlamydia; GI, gastrointestinal; HAV, hepatitis A virus; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HCV, hepatitis C virus; h/o, history of; HPV, human papillomavirus; HSV, herpes simplex virus; HTN, hypertension; ICD-10, International Classification of Diseases, Tenth Revision; N/V/abd, nausea/vomiting/abdominal pain; PEP, postexposure prophylaxis; RPR, rapid plasma reagin; SFHN, San Francisco Health Network; STI, sexually transmitted infection; ULN, upper limit of normal; Upreg, urine pregnancy test; Vit D, vitamin D.
Instruments and Data Collection
The study included a paper survey (Figure 2) that clinicians self-administered during the detailing visit. Clinicians were practitioners with prescribing privileges (ie, physician [doctor of medicine or doctor of osteopathic medicine], nurse practitioner, or physician assistant). The 10-question survey assessed clinician practices in collecting annual, detailed sexual health histories of patients; STI screening; knowledge of STI guidelines; PrEP prescribing patterns; and the characteristics of the participating clinicians and clinics. We entered all surveys into a Microsoft Office 365 Access 2021 database (Microsoft Corp). Given the pivot to group detailing, we could not crossmatch many surveys because they had missing names; thus, we removed these surveys from analyses (n = 101). We also excluded surveys from respondents without prescribing privileges (n = 15). This process left a sample of 203 clinicians (of 319 completed surveys).
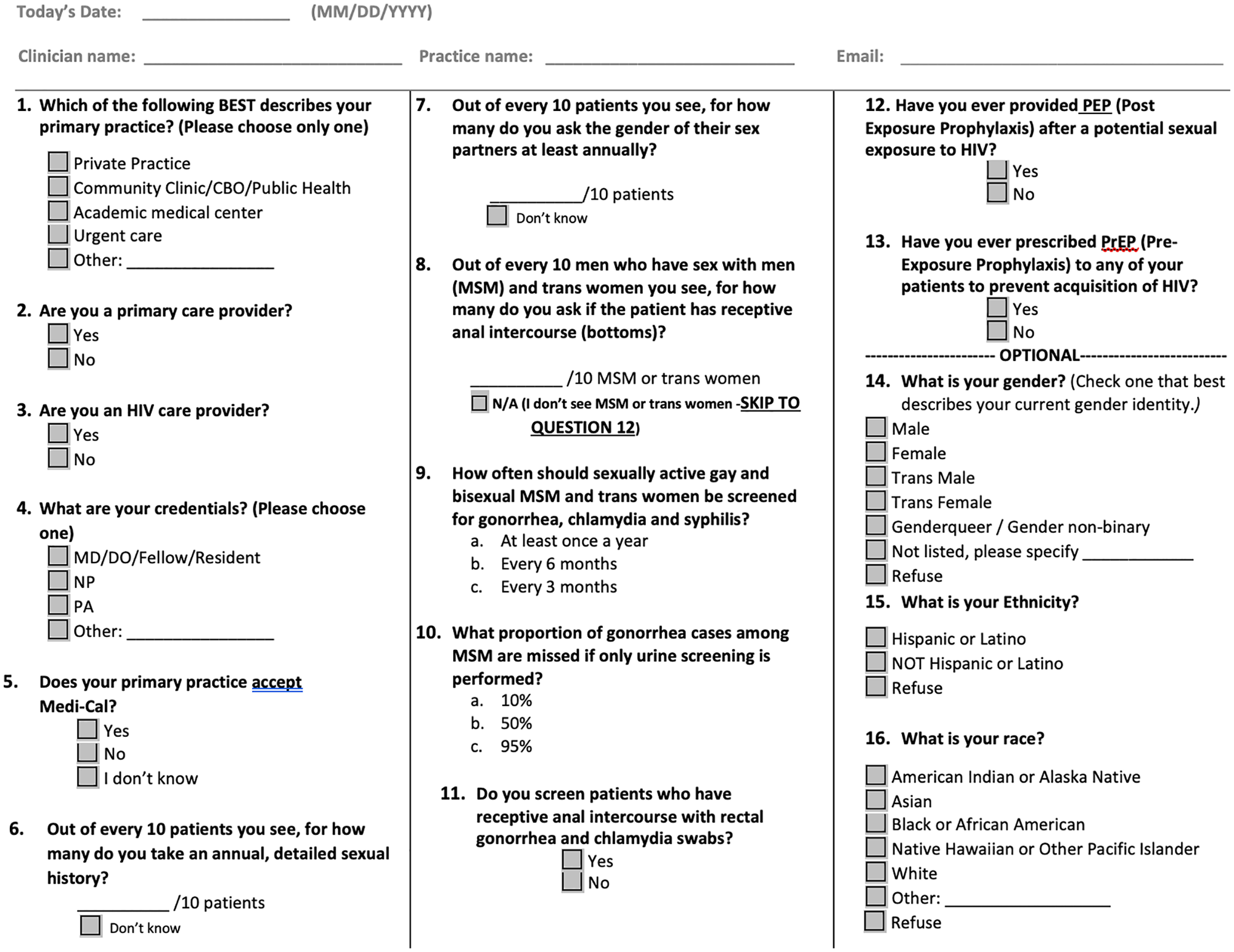
Self-administered paper survey used during detailing visits. The San Francisco Department of Public Health conducted a public health detailing program from 2016 through 2018 to improve sexual health care and PrEP services in the city. Public health detailing is an intervention in which a public health professional visits health care providers to educate them about evidence-based approaches to improve health while also addressing clinician- and system-level barriers to implementing these recommendations. Abbreviations: CBO, community-based organization; DO, doctor of osteopathy; MD, doctor of medicine; N/A, not applicable; NP, nurse practitioner; PA, physician assistant.
The evaluator conducted 60-minute interviews with 4 of the 5 SFDPH detailers who worked on SFDPH’s Getting to Zero plan; 1 detailer (a registered nurse focused on hepatitis C) was unavailable due to scheduling. The detailers interviewed were 3 clinically trained detailers; 1 was a nurse practitioner (A.D.) who worked on the PrEP detailing program. Two were registered nurses; 1 worked on hepatitis C and the other on rapid HIV treatment. The last interview was with the consultant who focused on PrEP detailing. The evaluator used an interview guide that probed on facilitators and barriers to implementing detailing and ideas for improvement.
The evaluator conducted 7 (of 10 contacted, 3 declined due to scheduling issues) 60-minute, qualitative, in-depth interviews with clinicians who had received detailing in the previous 12 months and for whom contact information was available. The lead detailer provided information on clinicians to contact. We purposefully sampled clinicians to include those with more than 1 detailing visit; we also considered geography in San Francisco, patient profiles, and health insurance type (private or public) to obtain representation of clinicians serving a diversity of patients (Box). Five of the 7 clinicians interviewed had multiple detailing sessions, and 2 clinicians had 1 session. The clinician interview guide asked the following questions, among others: What do you believe is the goal of detailing? What changes have you made to your practices after detailing? How might the health department support you in implementing changes? How could detailing be improved?
Demographic and clinic characteristics of clinicians interviewed (n = 7) as part of a mixed-methods study of detailing conducted by the San Francisco Department of Public Health to improve sexual health care and preexposure prophylaxis services in the city, 2016-2018. Public health detailing is an intervention in which a public health professional visits health care providers to educate them about evidence-based approaches to improve health while also addressing clinician- and system-level barriers to implementing these recommendations.
Analytic Methods
We analyzed survey data using descriptive statistics and Pearson χ2 measures of association for bivariate analyses that compared sexual health history taking and PrEP prescribing at baseline and follow-up. For the 21 matched pre- and post-surveys, we used a paired t test. We used an α of < .05 to indicate significance. We used thematic analysis to analyze information from the in-depth interviews. We triangulated the results across the qualitative data sources (ie, clinician and detailer) and then to the surveys to establish a holistic understanding of detailing. The first author (K.S.) conducted the thematic analysis and shared results with coauthors/detailers (A.D. and D.S.) to refine the analyses. The goal of the analyses was to understand how clinicians and detailers experienced the detailing program, examples of how detailing changed clinical practice behaviors, and strategies to improve detailing efforts. The use of clinician and detailer interviews helped to achieve saturation of the thematic findings. We analyzed the qualitative data in Atlas.ti version 8.4 (Scientific Software Development GmbH) and the surveys in R version 3.6.1 (R Core Team) and Stata release 16 (StataCorp LLC).
Results
From October 2016 through December 2018, detailers detailed a total of 503 health care staff. The nurse practitioner detailer visited 108 practices and reached 482 clinicians. The consultant detailer visited 77 practices and interacted with 73 clinicians, 52 of whom refused to participate during a 7-week campaign. Thirty (16.2%) of 185 practices received a follow-up visit. Of the 203 clinicians who completed surveys, 51 completed a follow-up survey. We matched pre- and post-surveys for 21 clinicians.
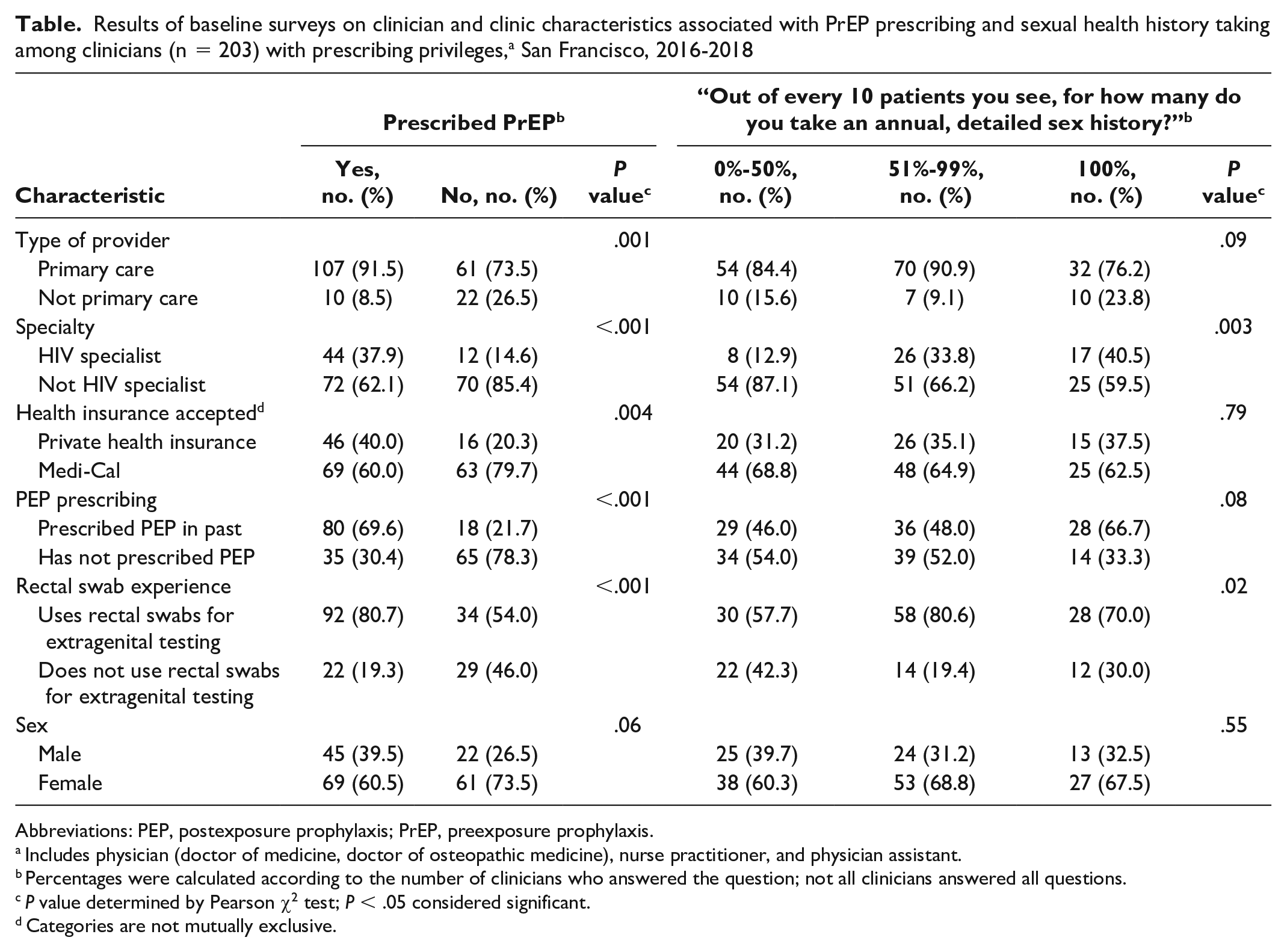
In baseline surveys, 58.5% (117 of 200) of clinicians reported prescribing PrEP (Table). Primary care clinicians, HIV specialists, type of health insurance accepted, past postexposure prophylaxis (PEP) prescribing, and use of rectal swabs for STI testing were associated with PrEP prescribing. Being an HIV specialist (vs not) and using rectal swabs (vs no use) were associated with higher rates of sexual health history taking. Clinician sex was not associated with PrEP prescribing or sexual health history taking.
Results of baseline surveys on clinician and clinic characteristics associated with PrEP prescribing and sexual health history taking among clinicians (n = 203) with prescribing privileges, a San Francisco, 2016-2018
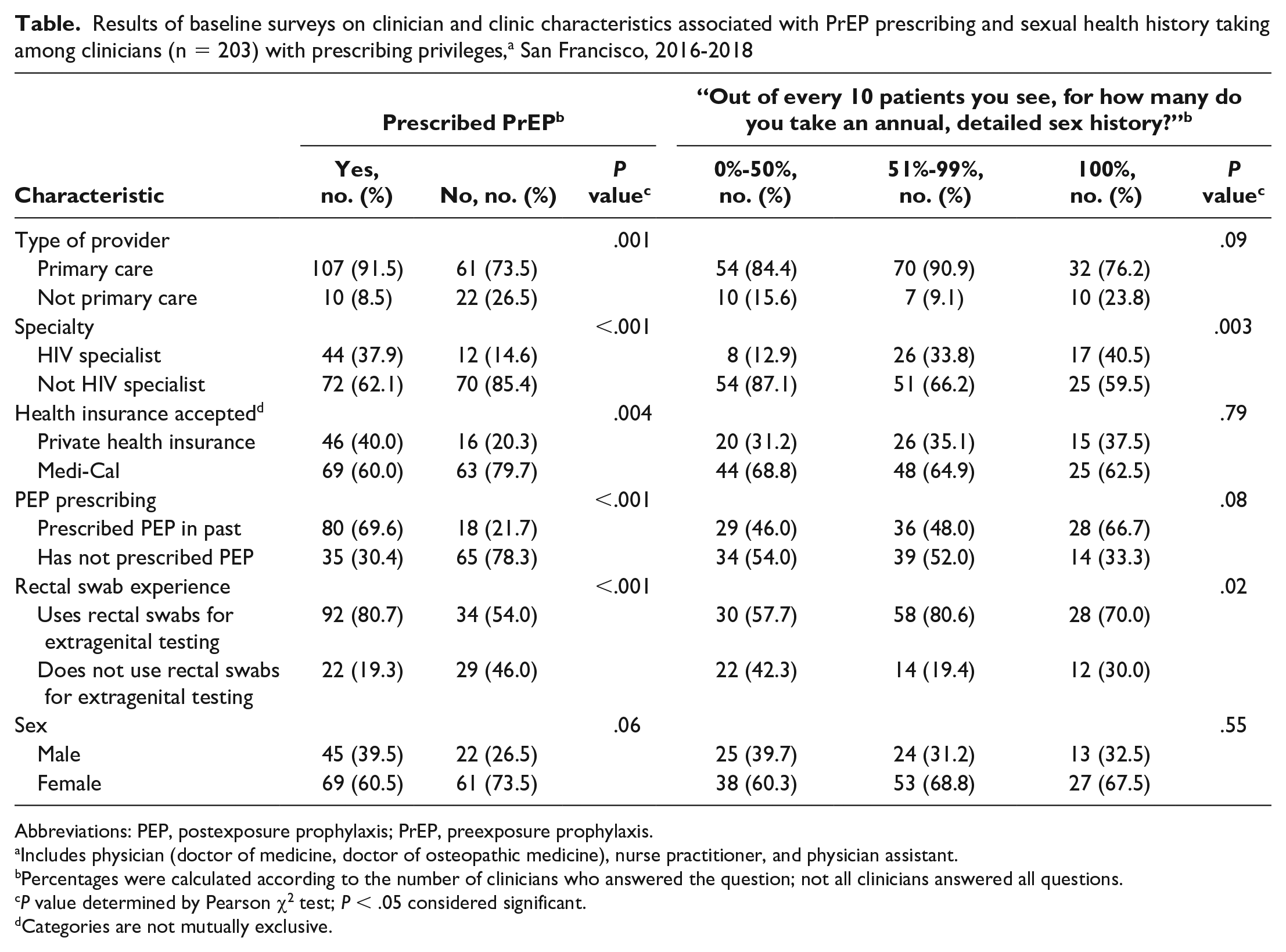
Abbreviations: PEP, postexposure prophylaxis; PrEP, preexposure prophylaxis.
Includes physician (doctor of medicine, doctor of osteopathic medicine), nurse practitioner, and physician assistant.
Percentages were calculated according to the number of clinicians who answered the question; not all clinicians answered all questions.
P value determined by Pearson χ2 test; P < .05 considered significant.
Categories are not mutually exclusive.
From the 21 matched follow-up surveys (10.3% of sample), the average number of patients to whom the clinician prescribed PrEP was 18 at baseline and 21 at follow-up (P = .09 for the 2-tailed test; P = .04 for the 1-tailed test). We found no change in the average number of patients screened for sexual health histories between baseline and follow-up. On average, health care clinicians took an annual sexual health history for 5 of every 10 patients. We found no significant difference in extragenital screenings (throat and rectal swabs) for STIs nor changes in the discussion of sexual position with patients who participated in receptive anal sex.
Understanding the Purpose of Detailing
All 4 detailers noted that most of the clinicians and practices they detailed were amenable to detailing. During interviews, detailers described the purpose of detailing as educating clinicians and practices; as the nurse practitioner (detailer-1) noted, “There is a sea of information [on sexual health].” Similarly, the purpose of detailing resonated with the 7 clinicians who agreed to be interviewed. As clincian-1, who received multiple visits, explained, “[I believe the goal of detailing] was to share best practices regarding sexual health.” Clinicians also viewed detailing as an opportunity to connect with SFDPH, as clinician-7, who had multiple visits, noted, “[Detailing is an] opportunity for me, as a primary care physician, to learn about what SFDPH can offer.”
Detailing Implementation Challenges and Facilitators
Detailers used various strategies to “get their foot in the door” to conduct detailing visits. Detailers described creating a sense of urgency about sexual health issues, leveraging the SFDPH “brand” and expertise, and linking the work to the broader Getting to Zero strategy. Many detailers described the importance of leveraging collaborative language, as the consultant (detailer-2) described, “I used terminology like partnership and collaboration. . . . [This] allowed practices and providers to see a role for themselves.” Such strategies helped to build camaraderie with clinicians.
Detailing was time-consuming. Of 130 clinicians who answered the question about time, 48 (36.9%) reported their detailing session lasted longer than 45 minutes. All detailers spoke about how clinician time constraints limited their ability to detail. As the consultant (detailer-2) noted, “Doctors have limited time to engage.” Norms within health systems that restrict access of “representatives” (eg, pharmaceutical representatives) to clinicians created barriers for the consultant-led strategy, because the consultant was not an official SFDPH staff member. Three detailers described conducting detailing in a group to facilitate access and meet the needs of busy clinics. Of the 129 clinicians who answered questions about the size of the group detailed, only 13 (10.0%) indicated receiving one-on-one detailing.
A benefit of detailing was the building of relationships and trust with clinicians. As the nurse practitioner (detailer-1) described, “At first, providers were skeptical about SFDPH detailing efforts because it was a novel intervention in the city.” As the consultant (detailer-2) noted, “[The detailing period of 7 weeks was] not enough time to create trust and relationships.” Clinicians and detailers reported wanting more time to work together to make changes to their practices. As clinician-1 described, “Give us time to make changes to our practices and policies.” Clinician-5, who received 1 visit, stated, “Glad we can have follow-up visits. There should be more communication with SFDPH.” The detailer interviews supported these claims, as 1 of the 2 registered nurses (detailer-4) said, “I have the pacing to allow processes [changes] to unfold. I have made inroads in many practices over months.” As described, the building of longer-term collaborative relationships is a beneficial outcome of detailing and a critical step in creating clinician-level change.
Benefits of Public Health Detailing
Generally, the interviewed clinicians thought detailing was beneficial and appreciated being connected with SFDPH. As clinician-7 stated, “Nice resource in being able to connect with DPH [Department of Public Health].” Such relationships helped clinicians use SFDPH’s expertise. Clinician-4, who received multiple visits, noted, “[It was] helpful to see the epidemiology.” The resources and handouts shared helped with education. Clinician-2, who had multiple visits, stated, “PrEP patient information is great. Keeping them on the wall has helped keep it on the radar.” The sharing of high STI incidence statistics helped solidify the importance of increasing extragenital STI screening. As clinician-6, who received 1 visit, noted, “[It was] illuminating [that] in doing MSM STI screening, doing just the urine screens [is] mostly useless.” All clinicians interviewed thought that patient-centered materials such as water bottles, pill storage keychains, and palm cards were useful for engaging in conversations with their patients.
Building clinician knowledge and confidence in providing sexual health care services was a critical part of detailing. The registered nurse (detailer-3), who focused on rapid HIV treatment, stated, “We presented the data [on rapid (<5 days) start of HIV treatment] and patient acceptance. But the deal was struck the first time they [provider] did it. Providers were skeptical and scared to go against the grain. They were blown away with how transformational it [rapid HIV treatment] was.” Clinicians gave credence to confidence building. Clinician-3, who had multiple visits, noted, “[Detailing] gave me the confidence to talk about anal sex. The data was impactful.” The other 6 clinicians described similar sentiments indicating that detailing supports building confidence and knowledge about sexual health and clinical care.
In clinician interviews, we found examples of changes to clinical behavior attributed to detailing. The detailing assisted some clinicians to increase the frequency of screening for STIs. Clinician-3, who worked with incarcerated patients, noted, “I am offering more STI screening to my patients.” Clinicians described how extragenital self-collection posters helped expand access to pharyngeal and rectal STI screening. Clinician-4 explained how they changed patient notes templates to include sexual health histories. Clinician-2 and clinician-4 described prescribing PrEP to methadone patients. As clinician-2 stated, “[Detailing] served as motivation to do directly observed therapy with PrEP in conjunction with methadone [treatment].” Detailing also taught clinicians about SFDPH’s services and programs. Clinician-1 described, “[LINCS] has been good for my practice. [LINCS] found the people [living with HIV] and got them back on treatment.”
Structural Barriers
Clinicians described policy and clinic challenges to making changes. Clinicians who worked with people who inject drugs expressed that health insurance policies limit the care they can provide. Clinician-3 noted, “Most [patients] should be on PrEP, most should be tested for STIs, but we can’t because they are not our primary care patients [according to health insurance policies].” Clinician time was also a constraint in conducting sexual health histories and screening. Family practice clinician-6 noted, “There is so much we are already doing as family doctors.”
Improvements to Detailing and Provider Collaboration
While clinicians described many benefits, they expressed ideas for improvement. Creating a sense of community between clinicians and SFDPH was an area of potential improvement. Clinician-3 questioned, “Can I leverage [DPH] connections better? How can I leverage clinics that have been detailed to support each other?” Clinicians described that they would like information to help them in the moment they are providing clinical care. Clinician-1 stated, “For PrEP, STI, and HIV testing, have simpler provider information sheets . . . help providers in the moment of care.” Another clinician suggested incorporating SFDPH services, such as LINCS, into the leave-behind materials.
Lessons Learned
Initial outcomes from our study of detailing in San Francisco suggest that the detailing model helps clinicians connect with public health department staff and learn about SFDPH and national sexual health care guidelines, programs, and resources. However, effectiveness of the detailing program is influenced by access to clinicians’ offices, the time they had available, and policy barriers such as health insurance.
Detailing requires extensive relationship building with practices to influence the plurality of behaviors necessary to improve sexual health care services. Our findings and previously published research highlight that structural- and clinic-level challenges, such as clinicians’ limited time and lack of knowledge about sexual health guidelines, must be addressed to improve sexual health care services. 16 In New York City, PrEP detailing reached 2500 clinicians, but challenges with implementation, such as time and perceived complexities of PrEP prescribing, were similarly described. 17 After detailing efforts to increase HIV screening in Baltimore, follow-up surveys showed that 73% of clinicians reported routinely screening for HIV, compared with 40% at baseline. 11 Detailing can work to improve clinician practices, especially if support from health departments includes discussions of guidelines, information on local scientific evidence, and support for making clinic and policy changes. In addition, it would be helpful to understand how to adapt the preferred one-on-one detailing18,19 in contexts where policies limit representatives from seeing clinicians. Moreover, formulating plans to address potential challenges with implementation is critical to be able to assess the impact of the intervention.
Appropriate patient materials also help improve services delivered. In Baltimore’s detailing program in 2014, clinicians noted that patient materials and training would help to increase routine HIV screening in practices. 11 Our study provides information about how to improve materials for use during clinic visits. Clinicians in our study noted that materials should support the clinician’s decision making and guide sexual history taking to build clinicians’ confidence in broaching sensitive topics, especially during appointments. Research indicates that perceived control, a construct from the Theory of Planned Behavior, shapes clinical care intentions. 7 Further enhancing detailing with theoretically informed strategies could elevate its utility.
Limitations
Several aspects of the study design could be improved. The evaluator (K.S.) was an outside consultant who began evaluation efforts toward the end of the detailing program. The later start hindered the establishment of data collection processes, such as linkage of quantitative data. The consultant strategy was a time-limited pilot to determine whether someone with expertise in detailing could reach a higher volume of clinicians, but policies in San Francisco that are strict against seeing outside representatives made this strategy nonoperable. The detailers had difficulties meeting clinicians for follow-up because of provider turnover, missing names on surveys, scheduling challenges, prioritization of practices not yet detailed, group detailing, and policy limitations on representatives. This lack of follow-up limited the ability to assess change. Clinicians who opted into detailing and agreed to be interviewed (<4% of the sample) may be more supportive of detailing than those who were not interviewed, which creates limitations for our interpretations. Lastly, while our study focused on PrEP, we included other sexual health detailing efforts; however, this “contamination” is not a major concern given that other detailing efforts did not focus on PrEP.
Conclusion
Evidence from this study suggests that detailing increases clinicians’ knowledge and confidence in offering sexual health care services and building the foundation for long-term relationships between clinicians and health departments. Our study shows that detailing can bridge the gap between clinical guidelines and real-world implementation. The success of the program depends on the implementation strategy, time, buy-in, and resources to build relationships with clinicians and clinic administrators. Because measuring the impact of detailing can be challenging, given the plurality of behavior changes needed, future detailing programs should carefully consider how they will evaluate their efforts prior to implementation. Incorporating information about HIV disparities and antiracist frameworks within detailing could further support clinicians in working with populations most in need of sexual health care services and HIV prevention.
Footnotes
Authors’ Note
The views expressed herein do not necessarily reflect the US Department of Health and Human Services’ official policies or the San Francisco Department of Public Health, nor does the mention of trade names, commercial practices, or organizations imply endorsement by the US government or the City and County of San Francisco. This publication’s contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention (CDC).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This publication was made possible by CDC under Funding Opportunity Announcements PS15:1506 and PS14-1403 (Cooperative Agreement Numbers 6NU62PS005027 and 5U65PS004411-02, respectively).