
Abstract
Objectives:
Motivational interviewing, a client-centered intervention method focused on enhancing intrinsic motivation for behavior change, shows a positive impact on children’s weight status (ie, stabilizing or slowing down weight gain as a child grows). We evaluated the impact of a training program on knowledge and adoption of evidence-based obesity prevention counseling strategies among counselors from Georgia’s Special Supplemental Nutrition Program for Women, Infants, and Children (WIC).
Methods:
Between July 2014 and September 2015, Children’s Healthcare of Atlanta’s Strong4Life program provided 388 WIC counselors in Georgia with a 2-hour training session on motivational interviewing, patient-centered counseling, and goal setting for obesity prevention. We evaluated the training using (1) self-administered pre- and post-training surveys that assessed knowledge of counseling strategies, (2) post-training observation of counseling interactions, and (3) a review of behavior change goal quality pre- and post-training in a random sample of 200 WIC client charts.
Results:
In a comparison of pre-training knowledge with immediate post-training knowledge among 388 counselors, 81% vs 91% (P < .001) knew that, to be effective, goals must be important to clients, and 66% vs 94% (P < .001) knew the 5 A’s (assess, advise, agree, assist, arrange) of counseling. Knowledge improvements were sustained at 3 months post-training. We observed no improvements in the quality of chart-documented behavior goals.
Conclusions:
WIC nutrition counselors in Georgia were aware of evidence-based counseling strategies but did not consistently apply them. The training program was helpful, but time and additional support are needed to adopt new practices.
In the United States, obesity prevalence among children aged 2-19 has tripled since the 1970s, rising from 5.2% in 1971-1974 to 17.2% in 2013-2014. 1 During the same periods, obesity prevalence rose from 4.0% to 17.4% among children aged 6-11 and from 5.0% to 9.4% among children aged 2-5, according to the National Health and Nutrition Examination Survey. 2 Interestingly, the trend among children aged 2-5 peaked at 13.4% in 2003-2004, fell to 8.4% in 2011-2012, 3 and then rose again to 9.4% in 2013-2014. 1
In 2014, among children enrolled in Georgia’s Special Supplemental Nutrition Program for Women, Infants, and Children (WIC)—a federal program serving low-income families with children aged <5 that provides free nutrition and physical activity education and counseling, vouchers for healthy foods, and referrals to other community resources 4 —13.4% of children aged 2-4 were obese, and 15.2% were overweight. 5 WIC nutrition counselors uniquely reach at-risk low-income households and are well positioned to support the development of healthy diet and activity patterns among the young children they serve.
In 2011, Children’s Healthcare of Atlanta, the largest pediatric hospital system in the southeastern United States, launched Strong4Life (www.strong4life.com), an initiative to address Georgia’s rapid rise in childhood obesity. Strong4Life uses evidence-based strategies to develop and implement primary health care and other community-based programs to reach key influencers in the lives of children, with the goals of improving the environments in which children live, learn, and play and fostering the development of healthy eating and activity practices. Research has shown that parents and caregivers largely rely on their children’s pediatricians for child health advice. 6 In 2011, Strong4Life developed the Provider Training Program to improve the obesity prevention and treatment-related counseling that pediatricians and other health care professionals provide to children and their families. The training program focuses on building providers’ skills in patient-centered counseling, motivational interviewing, and goal setting. 7,8 Motivational interviewing is a patient-centered method for behavior change that uses techniques focused on being empathetic, nonjudgmental, and supportive. Motivational interviewing techniques include asking open-ended questions, reflective listening, sharing the agenda setting, eliciting pros and cons of change, asking about the importance and confidence of making a change, and summarizing the conversation. 9 In 2011, we conducted a study of the Strong4Life Provider Training Program and found that, from before program completion to after program completion, providers’ self-efficacy in counseling increased from 44% to 81% and motivating patients increased from 28% to 64%. The frequency with which providers set behavior change goals with patients also increased.8
Other studies have demonstrated the positive effect that motivational interviewing has on children’s weight status. A recent review of 6 studies concluded that, despite limited available evidence, the application of motivational interviewing components to improve body mass index (BMI) and the risk of obesity-associated outcomes in children aged 2-11 is effective. The reviewed studies showed a decline or slower increase in BMI for children participating in motivational interviewing with their pediatricians, ranging from a mean decrease of 0.67 kg/m2 at 14 weeks post-intervention to 0.31 kg/m2 at 1 year post-intervention. 10 The results of a randomized controlled trial published in 2015 demonstrated that 6 counseling sessions based on motivational interviewing delivered by primary care providers and registered dietitians resulted in a significant reduction in BMI percentile among overweight children aged 2-8. During the 2-year study period, the mean BMI percentiles decreased 1.8 from a baseline of 91.5 among those who received usual care and decreased 4.9 from a baseline of 92.1 among those who received counseling with motivational interviewing. 11
The success of the Strong4Life Provider Training Program, combined with previous research demonstrating the positive effect that training WIC nutrition counselors can have on obesity prevention strategies and messages, 11 led to the development of a similar program for Georgia’s WIC nutritionists. In 2015, Strong4Life collaborated with the Georgia Department of Public Health, Georgia WIC, and Georgia Shape (a statewide initiative to address childhood obesity; georgiashape.org) to develop the Strong4Life WIC Training Program. The training portion of the program focused on building skills in evidence-based counseling techniques, including motivational interviewing, the 5 A’s of counseling (assess, advise, agree, assist, arrange), 7 the use of SMART goal setting (specific, measurable, assignable, realistic, and time related), 12 and goal documentation. Strong4Life also provided trainees with a toolkit to facilitate implementation of the behavior change counseling strategies discussed. 13 The toolkit included (1) a standardized Healthy Habits assessment form to be completed by WIC clients before meeting with the nutrition counselor to facilitate a conversation about current obesity-associated behaviors; (2) a color-coded BMI poster using green, yellow, and red zones instead of the terms “normal,” “overweight,” or “obese”; (3) a goal handout to document the health behavior goal that the client sets with the help of the nutrition counselor; (4) a take-home handout for the client with information on healthy habits to reinforce the goals that were set; and (5) educational posters for placement in clinic rooms and waiting rooms to support the healthy habits messaging.
We evaluated the knowledge and counseling practices of Georgia WIC nutrition counselors before and after participating in the Strong4Life training on evidence-based counseling strategies for obesity prevention.
Methods
Training Program
Strong4Life implemented its WIC Training Program in each of Georgia’s 18 WIC districts between July 2014 and September 2015. The state WIC office encouraged all WIC staff members who provide nutrition counseling to attend. This included all competent professional authorities (ie, nutritionists, dietitians, and registered nurses), breastfeeding counselors, dietetic interns, and office managers or directors who also provided counseling. Strong4Life offered the free 2-hour training session in collaboration with state and local WIC offices. At least 1 experienced and skilled nutrition counselor from each of the 18 WIC districts (n = 30) served as a post-training resource for his or her colleagues (ie, a champion) and assisted with post-training evaluation of the WIC Training Program by observing counseling sessions. Strong4Life program staff members provided ongoing training and support for champions throughout the program evaluation period.
Study Design
We used 3 methods to assess changes in knowledge and practices among Georgia WIC nutrition counselors participating in the WIC Training Program. First, participants completed self-administered surveys at 3 time points: before training (day of training), immediately after training (same day), and 3 months after training. Second, champions conducted post-training observations of WIC counseling sessions during a 9-month period after the training. Finally, the Georgia Department of Public Health randomly selected 200 WIC client charts throughout the state, and we evaluated the pre- and post-training quality of behavior change goals set by the nutrition counselors. We collected and managed study data using REDCap electronic data capture tools hosted at Children’s Healthcare of Atlanta. 14 The Emory University Internal Review Board determined that this evaluation study did not meet the definition of research with human subjects.
Participant Survey
In the pre-training survey, we collected data on participant race (white, black or African American, other), clinic location (rural or urban county), and years of experience providing nutrition-related counseling. All other survey components were identical for all time points. The self-administered surveys conducted at 3 time points included 2 multiple-choice questions assessing knowledge of evidence-based counseling techniques (“Which of the following are the best ways to counsel WIC clients on good nutrition and physical activity? Select all that apply.”) and goal-setting techniques (“A good behavior change goal will be…Select all that apply.”). For each question, we intentionally included 1 incorrect answer choice. We assessed counseling comfort and confidence with 2 items, based on 5-point Likert-scale responses (1 = strongly disagree to 5 = strongly agree): “I am comfortable counseling parents of overweight or obese WIC children about their nutrition or physical activity habits” and “I am confident in my ability to counsel WIC clients using patient-centered goal-setting techniques.” We used the last 4 digits of the participant’s cellular telephone number and birth month and day to maintain anonymity but enable matching of surveys for analysis.
Evaluation of Champion-Observed Counseling Sessions
After the training session, Georgia WIC and Strong4Life asked each champion to observe at least 1 counseling session per month with a participating WIC nutrition counselor. To determine which motivational interviewing skills were used during counseling sessions, champions answered 2 yes/no questions after observing a counseling session: “Were open-ended questions used to understand the WIC client’s feelings about the child’s weight status?” and “Was the Strong4Life Healthy Habits assessment used to facilitate a conversation with the client?” Champions selected all responses that applied to the question “Which of the following patient-centered counseling techniques were used?” Response options included “reflective listening,” “assessed motivation to change,” and “asked permission to share.”
Chart Review of Goal-Setting Quality
The evaluation also included an analysis of the quality of the goals documented in WIC client charts before and after the Strong4Life WIC Training Program. We included in the sample Georgia children aged 2-5 who attended a WIC clinic in a district that used an electronic health record system and who had at least 1 documented certification visit (ie, involving a nutrition counseling session) before and after the district’s WIC Training Program. The Georgia Department of Public Health randomly selected 200 Georgia WIC charts and provided de-identified data on the required variables to investigators. The sample included 67 charts randomly selected from urban metropolitan Atlanta WIC districts and 133 charts randomly selected from rural nonmetropolitan Atlanta WIC districts.
We scored goal-setting quality using a point system developed by the Georgia WIC office. A goal meeting all 5 of the SMART criteria received a score of 1, a goal missing 1 of the SMART criteria received a score of 0.5, and a goal missing ≥2 SMART criteria received a score of 0. If no goal was set, the chart was coded as “no goal.” Any goal that contained the language “patient agrees to,” “patient plans to try,” or “patient will try to” was not considered “patient centered,” because this language suggests that the Georgia WIC nutrition counselor had set the goal for the client. In this case, 0.5 was subtracted from the score.
Data Analysis
We used McNemar tests for paired nominal data to compare descriptive characteristics of the full sample with those of the subsample at the 3-month follow-up. We also used these tests to compare changes in participating WIC nutrition counselor knowledge and confidence from pre-training to immediately and 3 months post-training. We stratified the data by available potential confounders (race, years of counseling experience, and previous Strong4Life training) to evaluate differences in response levels and homogeneity. Because most counseling staff members were female (>90%), we did not assess differences by sex. We used the Cochran–Mantel–Haenszel test and Zelen exact test to assess homogeneity. To assess differences in goal-setting quality scoring, we used repeated measures ordinal logistic regression, controlling for clinic location. We used Cochran–Armitage trend tests for categorical data to examine trends in motivational interviewing skills and use of the toolkit materials, as observed by champions. We considered P < .05 significant. We used SAS version 9.4 and SPSS version 22.0 for all analyses. 15,16
Results
Demographic Characteristics of Nutrition Counselors
Of the 388 WIC nutrition counselors who completed pre- and post-training surveys (Table 1), 291 (75%) were competent professional authorities; 194 (50%) were white, 144 (37%) were black or African American, and 50 (13%) were other. Sixty-two (16%) participants had previously completed the Strong4Life Provider Training, and the mean number of years of experience providing nutrition-related counseling was 9.1 (SD = 7.3). Most participants (n = 287, 74%) were in rural WIC clinics located outside the metropolitan Atlanta area. In the 3-month follow-up survey, which was conducted among a convenience sample of 182 participants, we found no meaningful differences in demographic characteristics between the 2 groups (Table 1).
Characteristics of Strong4Life WIC Training Programa participants, Georgia, 2014-2015
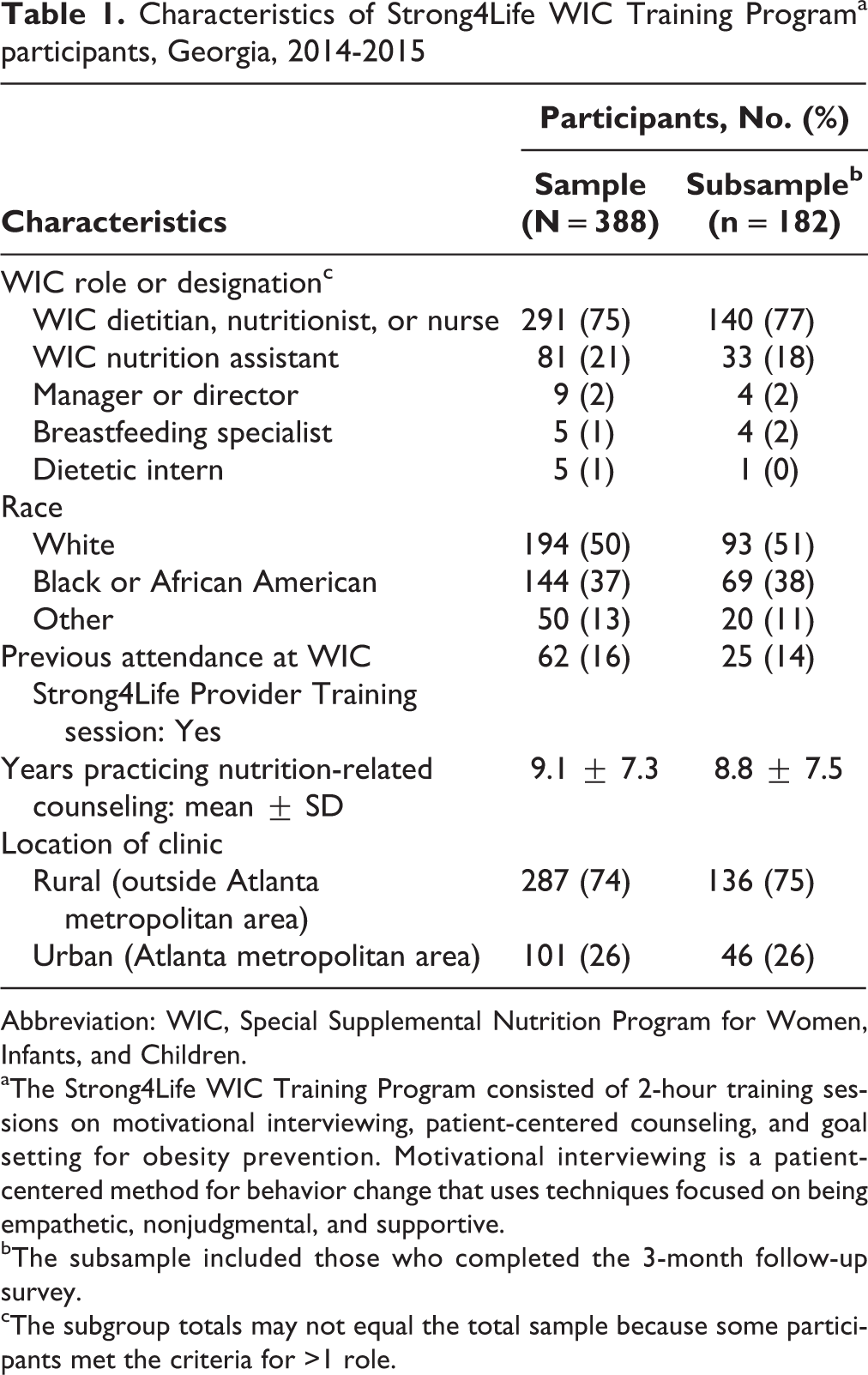
Abbreviation: WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
aThe Strong4Life WIC Training Program consisted of 2-hour training sessions on motivational interviewing, patient-centered counseling, and goal setting for obesity prevention. Motivational interviewing is a patient-centered method for behavior change that uses techniques focused on being empathetic, nonjudgmental, and supportive.
bThe subsample included those who completed the 3-month follow-up survey.
cThe subgroup totals may not equal the total sample because some participants met the criteria for >1 role.
Knowledge of Evidence-Based Strategies
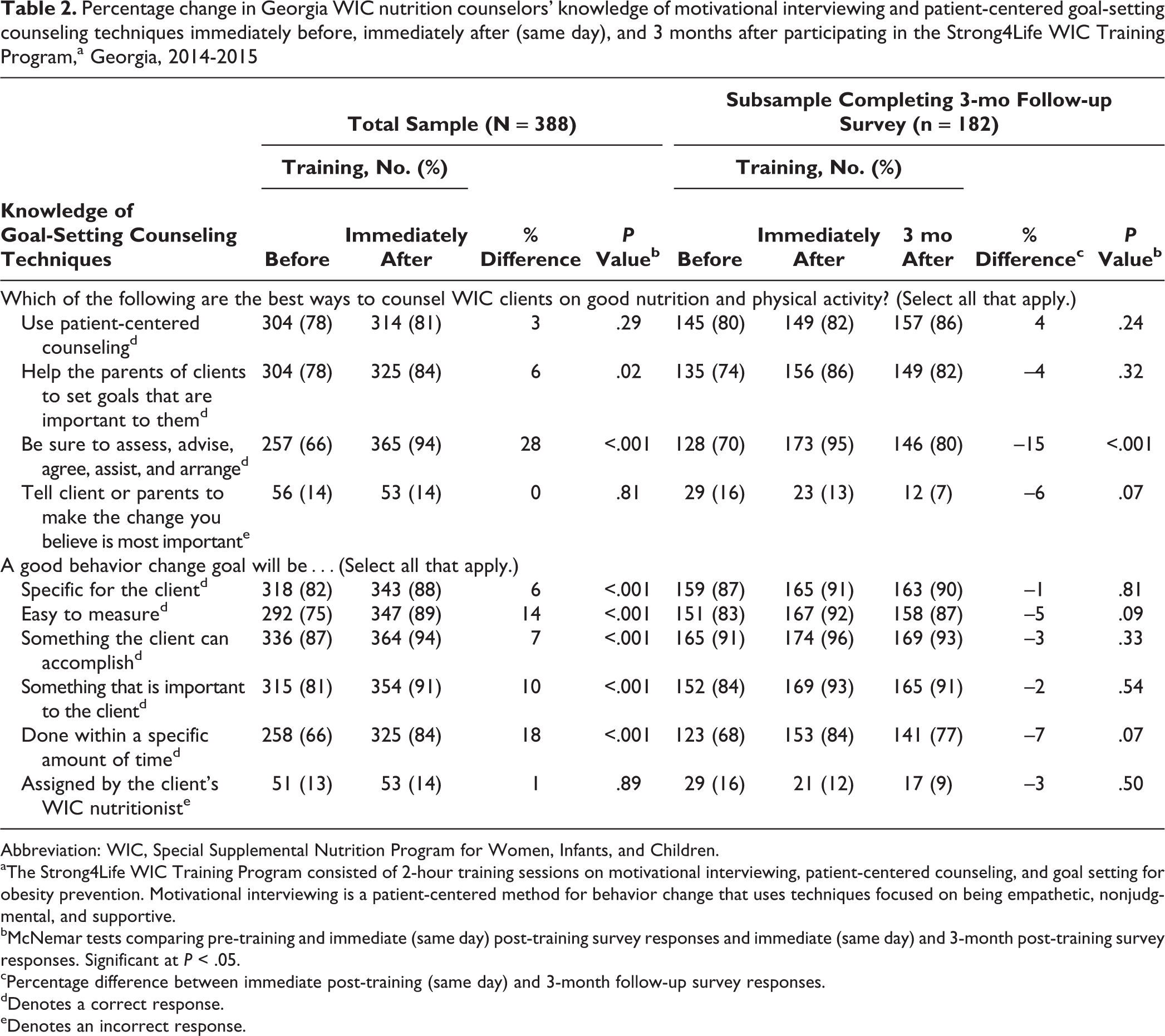
The proportion of participating Georgia WIC nutrition counselors who were knowledgeable about evidence-based counseling techniques was moderately high pre-training and increased immediately post-training (Table 2). The number of participants who selected “Help the parents of clients to set goals that are important to them” as an effective counseling strategy increased from 304 (78%) to 325 (84%; P = .02). The number of participants familiar with the recommended 5 A’s of counseling increased from 257 (66%) to 365 (94%; P < .001). The number of participants who recognized characteristics of a good behavior change goal also increased significantly from pre-training to immediately post-training: “specific for the client,” from 318 (82%) to 343 (88%); “easy to measure,” from 292 (75%) to 347 (89%); “something the client can accomplish,” from 336 (87%) to 364 (94%); “something that is important to the client,” from 315 (81%) to 354 (91%); and “done within a specific amount of time,” from 258 (66%) to 325 (84%; all P < .001). In the subsample of 182 participants who completed the 3-month follow-up survey, the only significant difference was a 15% decline in participant knowledge of the recommended 5 A’s (P < .001; Table 2). Stratification by potential confounders and testing with the Cochran–Mantel–Haenszel and Zelen exact tests did not reveal any meaningful differences from the combined results; therefore, only combined results are presented.
Percentage change in Georgia WIC nutrition counselors’ knowledge of motivational interviewing and patient-centered goal-setting counseling techniques immediately before, immediately after (same day), and 3 months after participating in the Strong4Life WIC Training Program,a Georgia, 2014-2015
Abbreviation: WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
aThe Strong4Life WIC Training Program consisted of 2-hour training sessions on motivational interviewing, patient-centered counseling, and goal setting for obesity prevention. Motivational interviewing is a patient-centered method for behavior change that uses techniques focused on being empathetic, nonjudgmental, and supportive.
bMcNemar tests comparing pre-training and immediate (same day) post-training survey responses and immediate (same day) and 3-month post-training survey responses. Significant at P < .05.
cPercentage difference between immediate post-training (same day) and 3-month follow-up survey responses.
dDenotes a correct response.
eDenotes an incorrect response.
Counselor Confidence and Comfort Using Evidence-Based Strategies
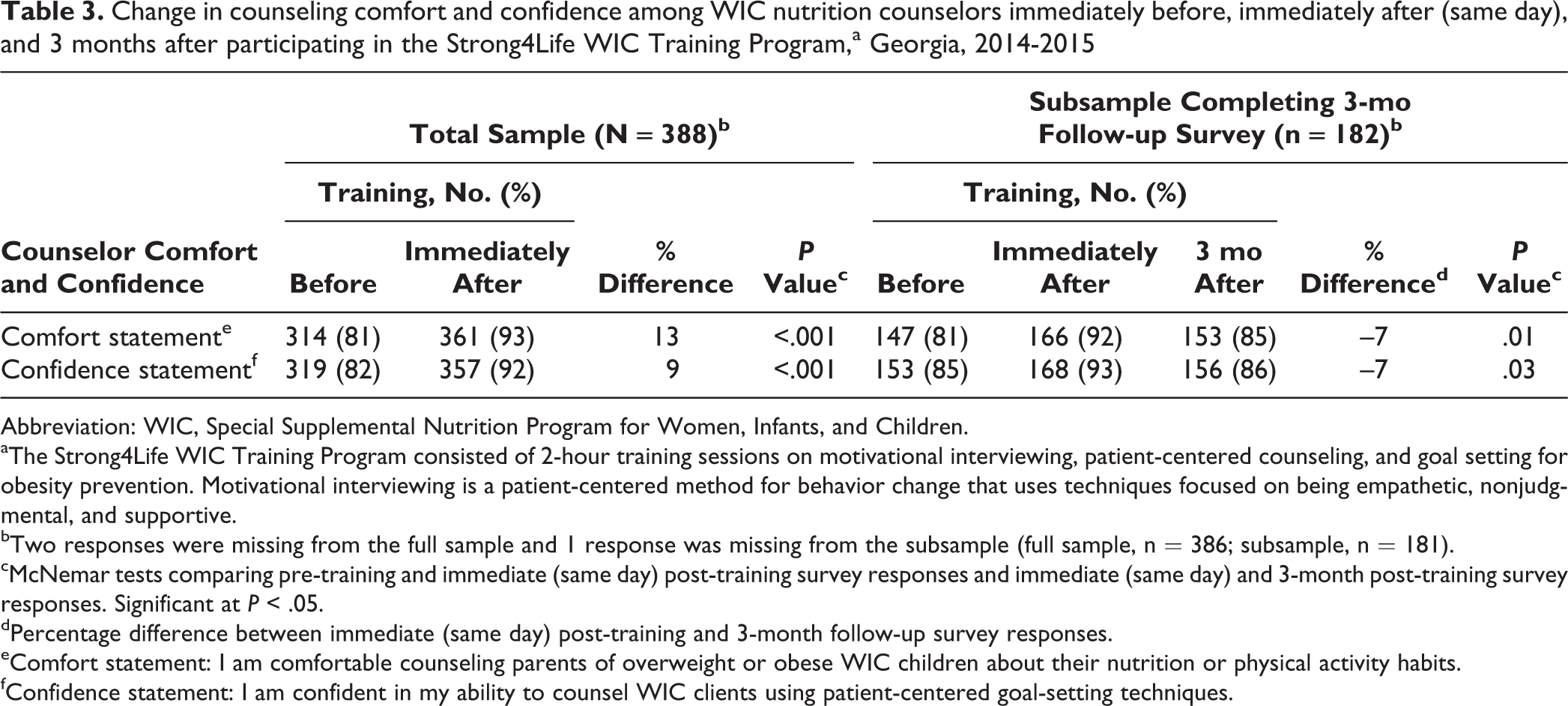
The number of WIC nutrition counselors who reported being comfortable counseling parents of at-risk children on their nutrition and physical activity habits increased from 314 (81%) before training to 361 (93%) immediately after training (P < .001; Table 3). The number of participants who reported being confident in their ability to counsel using patient-centered goal-setting techniques increased from 319 (82%) before training to 357 (92%) immediately after training (P < .001). From immediately post-training to 3 months post-training, however, participant comfort and confidence decreased by 7% (P = .01) and 7% (P = .03), respectively (Table 3). Because stratification by potential confounders did not reveal any major differences from the combined results after conducting Cochran–Mantel–Hanszel and Zelen exact tests for homogeneity, only the combined results are shown.
Change in counseling comfort and confidence among WIC nutrition counselors immediately before, immediately after (same day), and 3 months after participating in the Strong4Life WIC Training Program,a Georgia, 2014-2015
Abbreviation: WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
aThe Strong4Life WIC Training Program consisted of 2-hour training sessions on motivational interviewing, patient-centered counseling, and goal setting for obesity prevention. Motivational interviewing is a patient-centered method for behavior change that uses techniques focused on being empathetic, nonjudgmental, and supportive.
bTwo responses were missing from the full sample and 1 response was missing from the subsample (full sample, n = 386; subsample, n = 181).
cMcNemar tests comparing pre-training and immediate (same day) post-training survey responses and immediate (same day) and 3-month post-training survey responses. Significant at P < .05.
dPercentage difference between immediate (same day) post-training and 3-month follow-up survey responses.
eComfort statement: I am comfortable counseling parents of overweight or obese WIC children about their nutrition or physical activity habits.
fConfidence statement: I am confident in my ability to counsel WIC clients using patient-centered goal-setting techniques.
Use of Motivational Interviewing and Toolkit Items
During the 9-month post-training observation period of nutrition counseling sessions by WIC champions, use of the Healthy Habits assessment form during sessions increased significantly from 8 of 14 observed to 8 of 11 observed (P = .03; Figure). From the first to the last month of observation, the motivation to change increased from 5 of 14 observed to 8 of 11 observed, and asking permission to share concerns increased from 3 of 14 observed to 5 of 11 observed; however, the changes were not significant. In the first month of observation, of the 14 sessions observed, 9 counselors practiced reflective listening, and 10 counselors used open-ended questions; however, the proportion of counselors using these skills did not change significantly over time. Champions reported that other toolkit items (eg, take-home handouts, BMI posters, goal sheets) were used less than half of the time.
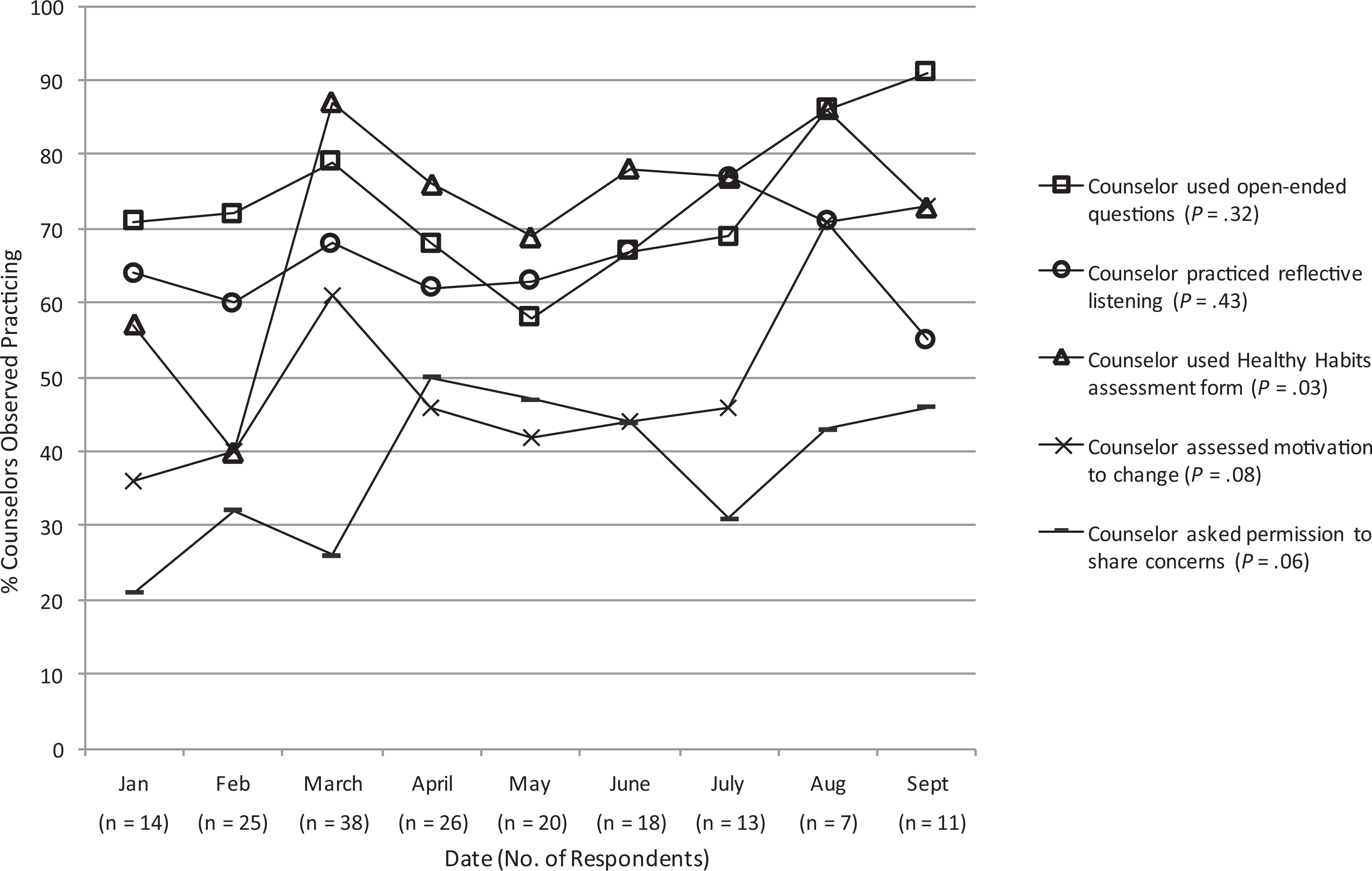
Results from observations by champions (ie, highly skilled WIC nutrition counselors) assessing the use of motivational interviewing by WIC nutrition counselors during counseling sessions with clients and their parents in the 9-month period (January to September) after counselor participation in the Strong4Life WIC Training Program, Georgia, 2014-2015. Cochran-Armitage trend tests for categorical data (P values) are shown in graph legend, with P < .05 considered significant. The Strong4Life WIC Training Program consisted of 2-hour training sessions on motivational interviewing, patient-centered counseling, and goal setting for obesity prevention. Motivational interviewing is a patient-centered method for behavior change that uses techniques focused on being empathetic, nonjudgmental, and supportive. The Healthy Habits assessment form is a short survey completed by parents identifying their child’s usual eating and activity habits. Motivation to change is measured from the Healthy Habits assessment form via a 4-point Likert scale (1 = not at all to 4 = very) to answer 2 questions: “How important is it to you that your child works on this healthy habit?” and “How confident are you that your child can improve on this healthy habit?” Permission to share concerns is a component of motivational interviewing whereby the counselor asks the patient if the counselor can share concerns about the patient’s goal setting. Abbreviation: WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Quality of Goal Setting
Of the 200 randomly selected WIC client charts analyzed for goal-setting quality before and after training, 78 (39%) received a score of 0 (ie, failure to comply with ≥2 SMART goal criteria) pre-training, compared with 70 (34%) post-training; 74 (37%) received a score of 0.5 (ie, failure to comply with 1 SMART criteria) pre-training, compared with 80 (40%) post-training; and 48 (24%) received a score of 1 (compliance with all 5 SMART criteria) pre-training, compared with 52 (26%) post-training (data not shown). However, the increases in quality scores were not significant.
Lessons Learned
Previous studies that examined the differences in BMI and adoption of healthy behaviors by children through motivational interviewing and goal setting showed mixed results in effectiveness. Some highlight provider uncertainty about which counseling techniques to use during motivational interviewing. 7 Our program, however, observed the transfer of knowledge and adoption of evidence-based counseling strategies by providers. Many of Georgia’s WIC nutrition counselors had previous knowledge of recommended behavior change counseling practices, but the Strong4Life WIC Training Program furthered this knowledge, particularly the characteristics of setting a good behavior change goal. However, some counselors did not retain this knowledge 3 months post-training.
Staff member turnover in Georgia is a challenge to improving the counseling skills of WIC nutritionists, suggesting that continuing education opportunities need to be repeated frequently to ensure that current and new staff members are properly trained. Staff member turnover in Georgia also highlights the value of using champions, such as those in the Strong4Life program, who are more likely to stay in their jobs and provide ongoing support and training. Incorporating and maintaining new counseling skills and tools into practice may take time. For example, in this study, WIC nutrition counselor use of the Healthy Habits assessment form dropped from January to February, rose in March, and then leveled off (Figure), and their comfort level in counseling parents of overweight or obese children and confidence in their ability to counsel using patient-centered goal setting increased initially and then decreased (Table 3). The challenges of many WIC nutritionists to document behavior change goals that meet WIC program requirements highlight a disconnect between knowledge and practice, suggesting the need for possible system-level changes to facilitate improvements in goal setting.
Strengths and Limitations
This evaluation had several strengths. First, we collected information on a new program, developed with evidence-based strategies, as it was being broadly implemented under real-world conditions. The information collected during this time frame will be critical for refining the Strong4Life WIC Training Program and guiding the development of future programs and training. Furthermore, the use of multiple assessment methods at 3 periods provided a means by which to collect data and evaluate, at least in part, all program components. Beyond the subjective participant surveys, the inclusion of independent observations by the champions using a standard assessment template and the data from chart reviews to assess goal quality provided objective means to evaluate key program components.
This evaluation also had several limitations. The lack of a control group compromised our ability to determine if the changes observed resulted from participation in the training or from other factors. In addition, the use of pre- and post-training surveys on the same day increased the risk of test-retest bias, in which the observed improvements in knowledge overestimate the actual effects of training. The assessment instruments were designed for this program evaluation and were not independently validated, which may have resulted in some reporting and information bias that could have compromised our ability to document the true impact of the training. Finally, data from a limited subsample restricted our assessment of the longer-term impact of the training, although descriptive characteristics between the full sample and the subsample were not significantly different.
Conclusion
The Georgia WIC program provides an opportunity to support healthy behavior change efforts among children at high risk of obesity and other chronic conditions related to poor diet and activity. Although many of Georgia’s WIC nutrition counselors were knowledgeable about evidence-based counseling strategies, and even though training can increase this knowledge, our evaluation indicated that the practical application of this knowledge is limited. Further research is needed to identify ways in which improvements can be achieved, possibly through increased use of decision prompts and other changes in the record systems to guide counselors toward recommended behaviors.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: At the time of the evaluation, all authors were affiliated with either the Strong4Life initiative of Children’s Healthcare of Atlanta or the Georgia WIC program and were part of the collaborative effort to develop and implement the WIC nutrition program.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.