
Abstract
Keywords
Introduction
It is recommended that clinicians should strive to provide integrated care for older adults (World Health Organization, 2015b). Such care can be provided within proactive comprehensive geriatric assessment services that combine a population screening strategy with an interdisciplinary multi-domain approach (Pilotto et al., 2016). Next to the need for integrated care, older adults and care professionals, each advocate the need for a more person-centered approach to care that increases well-being. This can be achieved by enhancing the involvement of older adults using behavior change and goal identification (Hopman et al., 2016). Motivational interviewing (MI) and goal setting are established methods for delivering these aims.
MI is a well-researched person-centered care communication strategy used by professionals to promote healthy behavior and achieve health benefits (Grandes et al., 2008). It involves a care professional exploring and resolving individual ambivalence to behavior change (Miller & Rollnick, 2014) rather than merely giving a diagnosis and advice. Four overlapping processes are involved: engaging (establishing a trusting relationship), focusing (determining the target for change), evoking (eliciting change talk, i.e., motivational statements about change), and planning (increasing commitment to change and formulating an individualized plan of action). The care professional should use adherent strategies for MI (i.e., affirmation, seeking collaboration, and emphasizing autonomy) and avoid non-adherent strategies (i.e., confronting and persuading).
Although MI was developed within psychiatry, it has since then been applied in various care settings, including primary care (Morton et al., 2015). The technique has been shown to be effective in increasing healthy behavior, treatment compliance, motivation, and emotional well-being (Lundahl et al., 2010), including the older adult population (Morton et al., 2015). A key element of MI is to identify goals during the focusing process. Indeed, the identification and setting of goals is considered a key aspect to delivering true person-centered care (World Health Organization, 2015a). Goal setting is also commonly used to increase patient involvement in decision-making and to increase their overall motivation (Levack et al., 2006; Schulman-Green et al., 2006). It has proven feasibility for use with older adults (Robben et al., 2015) and is effective as a behavior change technique (Herdman et al., 2019). The addition of MI and goal setting techniques to existing care could, therefore, help to enhance person-centeredness.
Previously, we incorporated MI and goal setting in a proactive outpatient assessment service for frail community-dwelling older adults, called Sage-atAge+ (in Dutch, Wijs Grijs 2.0). Although we had sought to increase well-being through increased patient involvement and behavior change, the inclusion of these techniques had no additional effects on the physical, psychological, or social well-being of older adults (Rietkerk Gerritsen, et al., 2019). However, before concluding that these strategies were ineffective, it is necessary to determine the extent to which they were actually applied. This is because it can be difficult to implement a multicomponent trial into daily practice, because the extent of performance cannot always be known, and because performance of different components may vary (Craig et al., 2008). Studying the extent of performance is crucial to preserve both the internal and external validity, and it can provide invaluable insights into the reasons for an intervention’s success or failure (Leontjevas et al., 2012). This ensures that results are interpreted accurately to facilitate the successful translation of evidence-based interventions into practice (Mackenzie et al., 2010).
The implementation of separate study components should be evaluated alongside the effect evaluation (Mackenzie et al., 2010), thereby allowing conclusions to be made about the efficacy of components and to understand the results of a multicomponent intervention. Understanding the reasons for inadequate implementation rates is important for two main reasons. On the one hand, the components can seem promising, but implementation (strategies) or components may need to be further adapted to the local context to improve implementation (Smit et al., 2018). On the other hand, it may be that further implementation of the intervention and its components add no benefit. Measuring the quality and the extent of MI performance, known as treatment fidelity, is already recognized to be a key factor when appraising trials of MI (Miller & Rollnick, 2014). For goal setting, it is important to determine the extent to which goals have the characteristics needed to promote behavior change (Michie et al., 2011).
Given that MI and goal setting during outpatient assessments could be beneficial for community-dwelling older adults’ well-being through health promotion and person-centeredness, we aimed to study the extent to which these strategies were adopted within Sage-atAge+ and to identify the factors that influenced their use. Since we found no effect on well-being in the Sage-atAge+ program, we hypothesized suboptimal implementation of at least one program component. In order to be able to improve future care programs, we searched for factors explaining this (hypothesized) suboptimal implementation.
Method
Design
We performed a mixed-methods process evaluation alongside our study into the effects of the Sage-atAge+ outpatient assessment service for community-dwelling older adults. This service was designed to increase the general well-being of participants by enhancing their involvement in resolving their unmet needs. We studied the implementation rate of MI and goal setting and their implementation quality (Leontjevas et al., 2012). We also searched for explanations for the extent of performance by analyzing the judgments and experiences of care professionals who had used MI and goal setting. The process analysis focused on the perspectives of care professionals because the perspectives of older adults were thoroughly considered in another study (Rietkerk, Smit, et al., 2019). Figure 1 shows the relation between the intervention components, the questions used in the process evaluation, and the data sources. Study design, intervention components, process evaluation questions, and data sources. Notes: Italic: Component’s aim. a comprising an assessment by a nurse or (for the most frail older adults) by an elderly care physician, oral screening by dental care worker, medication evaluation by a pharmacist, and, if applicable, consult from an allied care professional; b GFI ≥4 (possible range 0–15) (Peters et al., 2012) and/or care profile based on frailty and case complexity ≥2 (possible range 1–5) (Eissens van der Laan et al., 2014). Abbreviations: CGA = comprehensive geriatric assessment; GP = general practitioner; MI = motivational interviewing; MITI = MI Treatment Integrity (code)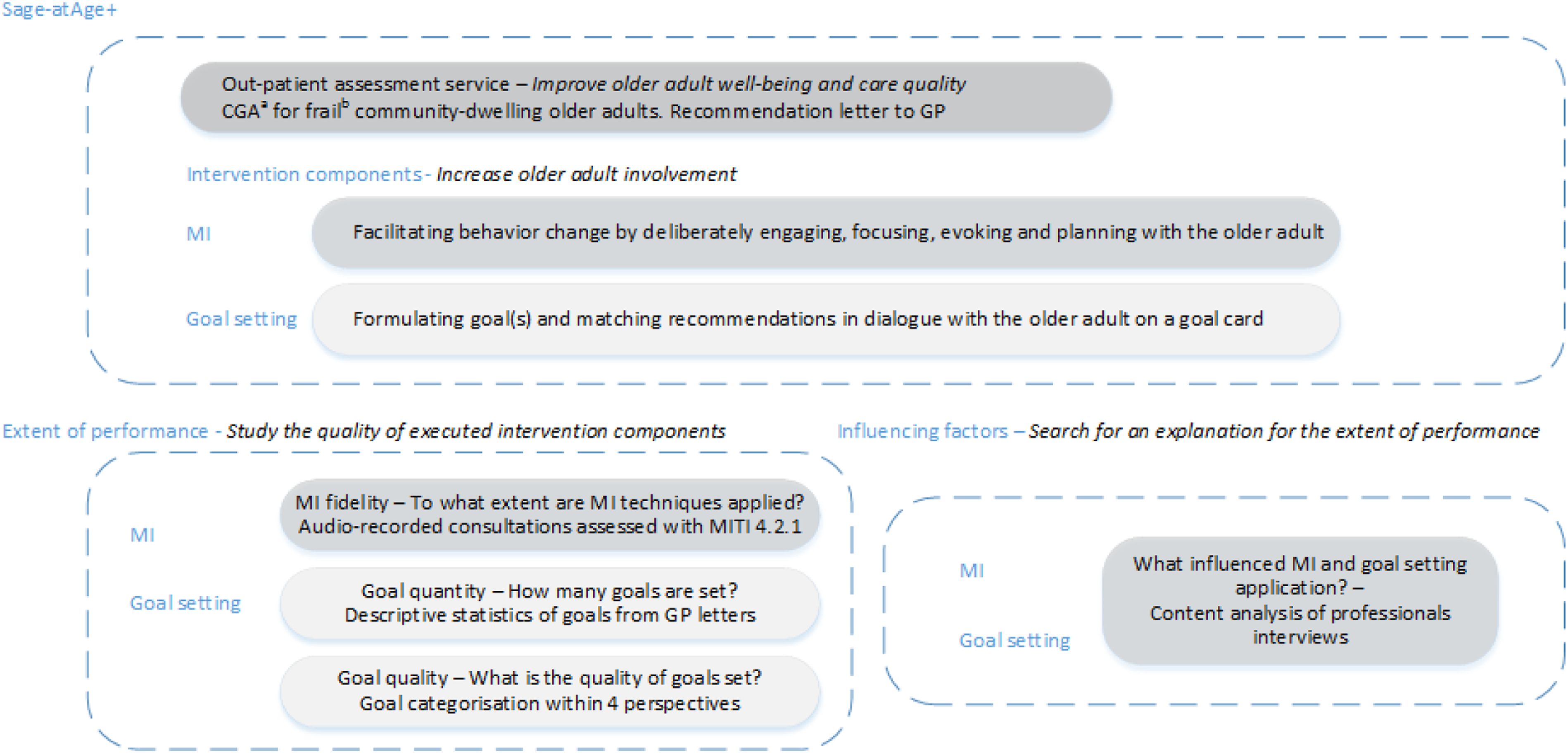
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and the Code of Conduct for Health Research (2004). The Ethics Committee of the University Medical Center Groningen confirmed that the study did not require ethical approval based on the Dutch law for medical trials (M12.120835). Because of the pragmatic nature of the intervention, older adults could also attain the assessment without giving informed consent for scientific data usage. Data in this study were only used from older adults who gave their written informed consent. All care professionals consented to the publication of the final manuscript.
Sage-atAge+ Service
The Sage-atAge+ service comprised two steps: (1) proactive screening of community-dwelling older adults for frailty and case complexity; and (2) assessment of needs and goals of older adults identified as frail. We then generated recommendations for the frail older adult and their general practitioner (GP). Older adult involvement in the intervention was promoted by using MI and goal setting techniques.
Patients were selected for assessment by sending a postal questionnaire and informed consent form to 1495 adults aged ≥65 years from seven primary care practices in the rural Northern part of the Netherlands. In total, 49% of the older adults (n = 725) returned the questionnaires. The questionnaires contained the Groningen Frailty Indicator (GFI) (Peters et al., 2012) and self-assessment version of the INTERMED for the elderly (Peters et al., 2013), respectively. With these, care profiles were attained as follows: (1) feeling vital, (2) psychosocial coping difficulties, (3) physical and mobility needs, and (4) difficulties in multiple domains (Eissens van der Laan et al., 2014). These profiles were constructed in previous research by factor mixture model analysis and were used to adapt the service to patient needs. Older adults with a substantial frailty level (GFI ≥ 4) and/or a high care profile (≥2) (44% (n = 322)) were invited for a CGA between September 1, 2014, and April 1, 2016. Overall, their mean age was 77 ± 6.9 years (range 65–94), 59% were women, 60% were married, 33% had a low educational level ((uncompleted) primary school or low-level vocational training), and 97% were of Dutch ethnicity. Mean frailty as measured with the GFI was 4.5 (±2.2). Details of the recruitment and selection procedure, as well as the participant characteristics, are published elsewhere (Rietkerk, Gerritsen, et al., 2019).
Comprehensive Geriatric Assessments
Comprehensive geriatric assessments were provided by a nurse or an elderly care physician (Koopmans et al., 2017), with the latter only performing assessments for the most complex and frail cases. The focus of these assessments was well-being, including social and functional participation, physical and psychological needs, and the living situation. A pharmacist performed a risk assessment of drug-related problems based on the triage score system (Van Roon et al., 2007) and the structured history-taking of medication use tool (Drenth-Van Maanen et al., 2011) and a dental care worker took an oral history and assessed the oral cavity. If considered necessary, optional diagnostic consultations could be added from a dietitian, physiotherapist, psychologist, or occupational therapist.
Written summaries of the assessments, consisting of one or more points of concern, corresponding life and health-related goals, and recommendations, were formulated and written on a goal card in collaboration with the older adult. MI was used to stimulate the older adult’s ability to reach the goals by deliberately improving their motivation through engaging, focusing, evoking, and planning. The content of the goal card was recorded in the older adult’s file and incorporated in the letter to his or her GP.
Between October 2014 and January 2015, all care professionals involved in the Sage-atAge+ study were invited for three 4-hour training sessions about MI. During these, didactic instruction was combined with role playing to allow practice with eliciting change talk, seeking collaboration, and goal setting. Participants received instructor and peer feedback on their performance. To improve compliance and sustained adoption of the newly acquired techniques, two booster sessions were held with care professionals that reinforced the training and provided an opportunity to discuss practical experiences.
MI Fidelity of Audio-Recorded Interactions
The MI fidelity was rated with the Motivational Interviewing Treatment Integrity (MITI) coding system (Moyers et al., 2014). The MITI is a reliable behavioral coding system which assesses the extent to which MI techniques are used during interactions by coding the remarks of care professionals. We audiotaped and transcribed 11 consecutive assessments by care professionals during December 2016 (four times by a nurse, three times by a pharmacist, and once each by an elderly care physician, a physiotherapist, a psychologist, and a dietitian). The median assessment length was 32 (range 16–65) minutes. Following the MITI, a 20-minute segment of each session was coded independently by two students studying for a master’s qualification in a health field. Whenever the audio-recorded assessments exceeded 20 minutes, a segment of that length was selected that focused on a target change behavior. Both coders had received 20 hours of training in coding with the MITI by an expert from the MI network of trainers (JJ) who also provided supervision while they performed the coding.
First, we scored four global MI qualities (i.e., partnership, empathy, cultivating change talk, and softening sustain talk) on a Likert scale that captured the coder’s overall judgment of the global qualities of an interaction. Summary scores were calculated with these and checked against expert-derived fair thresholds, which are considered the minimum extent of MI application needed to obtain the desired effects (Moyers et al., 2016): The relational score is the average of the partnership and empathy global scales. Higher scores indicate clinicians trying to foster a collaborative approach and genuinely seeking to understand a patient’s perspective. The possible range is 1–5, with the fair threshold set at 3.5. The technical score is the average of the softening sustain talk and cultivating change talk global scores. Higher scores indicate clinicians actively eliciting the patient’s arguments in favor of positive change (i.e., change talk) and decreasing the patient’s arguments for no change (i.e., sustain talk). The possible range is 1–5, with the fair threshold set at 4. The reflection to question ratio is calculated, with the fair threshold set to a ratio of one reflection to one question. Higher scores indicate that the clinician centers on engagement and evocation. The fair threshold is set at one or more reflections to one question. We calculated the percentage of complex reflections compared to the sum of complex and simple reflections. The fair threshold was set as >40%.
Each relevant utterance of a care professional was counted as an adherent (i.e., affirming, seeking collaboration, and emphasizing autonomy) or a non-adherent (i.e., confronting and persuading) behavior category of MI.
Goal Setting: Quantity and Quality Based on Medical Records
The recommendation letter to the GP was extracted from all participants’ medical records, and any goal(s) were recorded, if applicable. Goal quantity was described by the median number of goals per participant with the interquartile range (IQR) and total range. Goal quality was classified into four categories: desire language, goal level, magnitude specification, and time frame specification.
Desire language
We coded this language element because it is known to be associated with the potential for behavior change (Tonigan et al., 2018). Every goal using the words “want,” “desire,” “like,” or a synonym of those words was coded as desire language (e.g., “would like to improve walking”) (Miller et al., 2008).
Goal level
We classified goals at the behavior or the outcome level based on an adaptation of a taxonomy for behavior change techniques (Michie et al., 2011). Goals at the behavior level were those targeting behavioral solutions (e.g., “playing billiards again; going outside with the mobility scooter”), whereas goals at the outcome level were defined in terms of an expected consequence of one or more behaviors, without being a behavior in itself (e.g., “decrease in abdominal discomfort”; “stay independent for as long as possible”). In addition to the taxonomy of Michie et al., to improve our agreement on this discrimination, we coded as the behavior level when a goal could be a task that could be added to a to-do list. Whenever this seemed impossible or if we needed to give more specification on the next step (e.g., “being among people more frequently”), we coded as the outcome level.
Specification categories
Specificity was coded because it is considered to increase the potential for behavior change by increasing commitment to that change (Kaminer et al., 2018). These elements were adapted from a taxonomy of important goal elements for people with dementia (Bogardus et al., 1998). Magnitude was coded into three categories: magnitude or volume specified if the goal was objectively measurable (e.g., “having a daily walk”), mentioned but not quantified if the goal was specified without the amount (e.g., “stabilize weight loss”), and not mentioned if the evaluation criterion for a goal was unknown (e.g., “decrease stress”). Time frame was also coded into three categories, as follows: specified if the time to attain the goal could be measured on a calendar, mentioned but not specified if a vague time period was used (e.g., “soon or as long as possible”), and not mentioned if no time period was given.
Interrater Agreement
The interrater agreement for MITI coding was assessed on five recordings between the two coders with a two-way mixed effects model, absolute agreement, and average measures intra-class correlation coefficient. The mean interrater agreement for coding between the reviewers was excellent (interclass correlation coefficient 0.81 ± 0.15). All interclass correlation coefficients ranged between good for complex reflections (0.64) and excellent for affirmations (0.95), except for giving information, which was only fair (0.44) (Cicchetti & Sparrow, 1981). When applicable, the average of both raters’ scores was calculated. Finally, we calculated the means, SDs, and ranges for the behavior counts and summary scores. The number of interactions reaching the fair threshold was counted.
Two researchers (WR and CN) independently applied the taxonomy for goal setting, and their allocation was similar in 94% of categories (range 92%–95%). Cohen’s kappa was 0.48 for the goal level, and the linear Cohen’s kappa values were 0.79 for magnitude and 0.83 for time frame. Whenever there was disagreement over categorization, consensus was reached after discussion between WR and CN.
Identification of Influencing Factors
Influencing factors for applying MI and goal setting were identified based on interviews. Semi-structured interviews with all care professionals were held by WR, a physician, and researcher, within 3 months after the Sage-atAge+ program had ended. The topic list comprised questions about the feasibility and acceptability of the program and its intervention components and experience with various elements of the program (e.g., training, MI, goal setting, and goal cards). All interviews were audiotaped, but technical problems resulted in two tapes being unusable. These interviews were transcribed in detail by the interviewer and checked by the interviewee within a week. All other tapes were transcribed verbatim.
We used inductive content analysis to derive findings by focused evaluation of questions phrased by WR and DG (Elo & Kyngäs, 2008). The analysis of transcripts was supported by the software package Atlas.ti 7. WR analyzed all interviews, and discussed themes, and corresponding quotes with JJ and DG regularly. All identified experiences and influencing factors were substantiated with relevant quotes.
Results
Sample: Care Professionals and Assessments
Overall, 322 comprehensive geriatric assessments were performed as part of the Sage-atAge+ program. Of these, 29% (n = 92) were excluded from analysis due to a lack of informed consent (n = 79) or missing medical record data (n = 13). Thus, the medical records of 230 participants were available and included in the analysis. All assessments were executed by three specialist geriatric nurses, except for 7% (n = 15), which were performed by the elderly care physician. Additional assessments by the pharmacist and the dental care assistant, which were offered to all participants, were undertaken by 94% (n = 217) and 29% (n = 67), respectively. Consultations with other allied healthcare professionals were attended by 25% (n = 57). Finally, a goal card was provided during 53% (n = 121) of the assessments.
Among the 10 professionals involved in the Sage-atAge+ program, four attended all training sessions, one attended only one session, two attended no sessions (logistical reasons), and three reported that they had already received training in MI. All participants were interviewed, except for the occupational therapist due to logistical reasons. An overview of data about the care professionals, the number of assessments, and their attendance at MI training is presented in Supplementary Table S1.
Extent of Performance: MI Fidelity
MITI Coding Results of Audiotaped Interactions (n = 11).
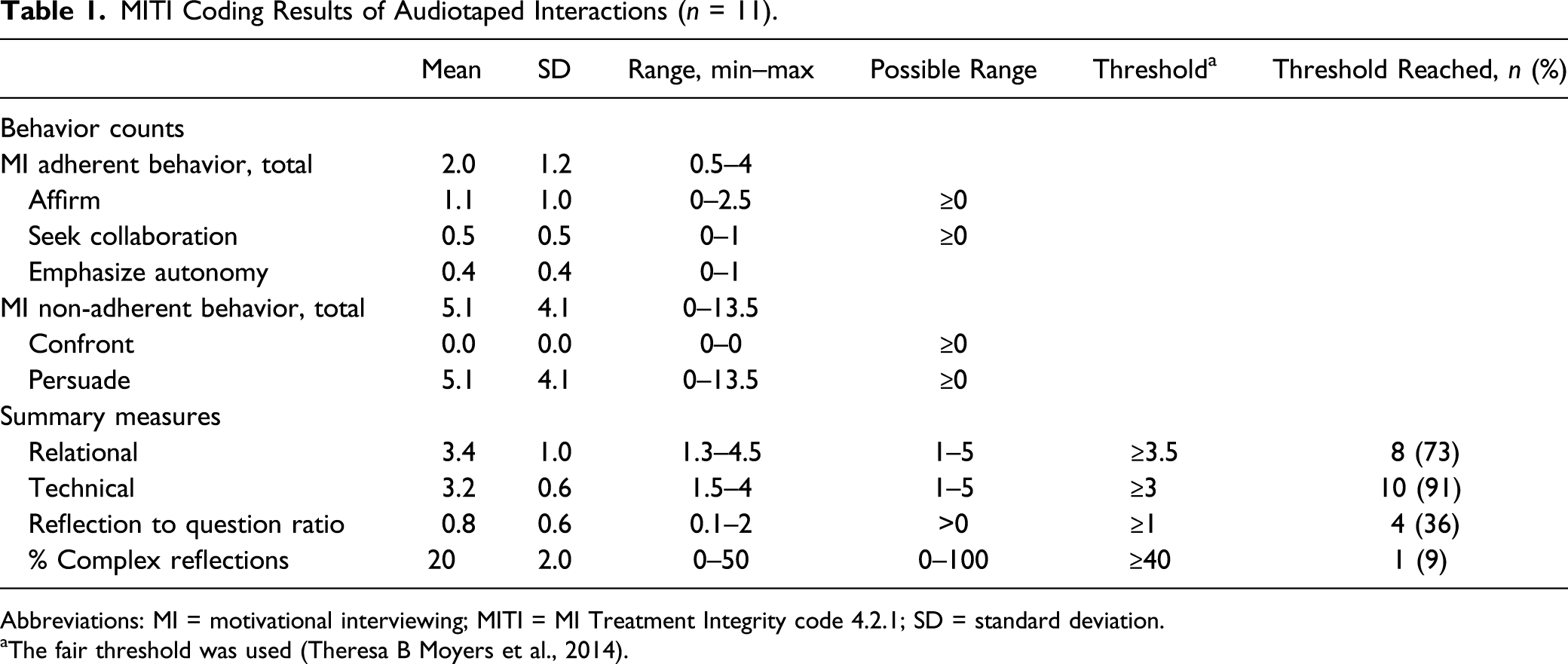
Abbreviations: MI = motivational interviewing; MITI = MI Treatment Integrity code 4.2.1; SD = standard deviation.
aThe fair threshold was used (Theresa B Moyers et al., 2014).
Concerning the summary measures, one interaction met none of the four thresholds and only one interaction met all four thresholds. The threshold on the relational scale was met in eight interactions, whereas that on the technical global scale was met in all but one. The reflection to question ratio was above the threshold in four of 11 interactions. Only in one interaction was the threshold for the complex reflection ratio reached.
Extent of Performance: Goal Setting
Goal Quality From Four Different Perspectives (n = 280).
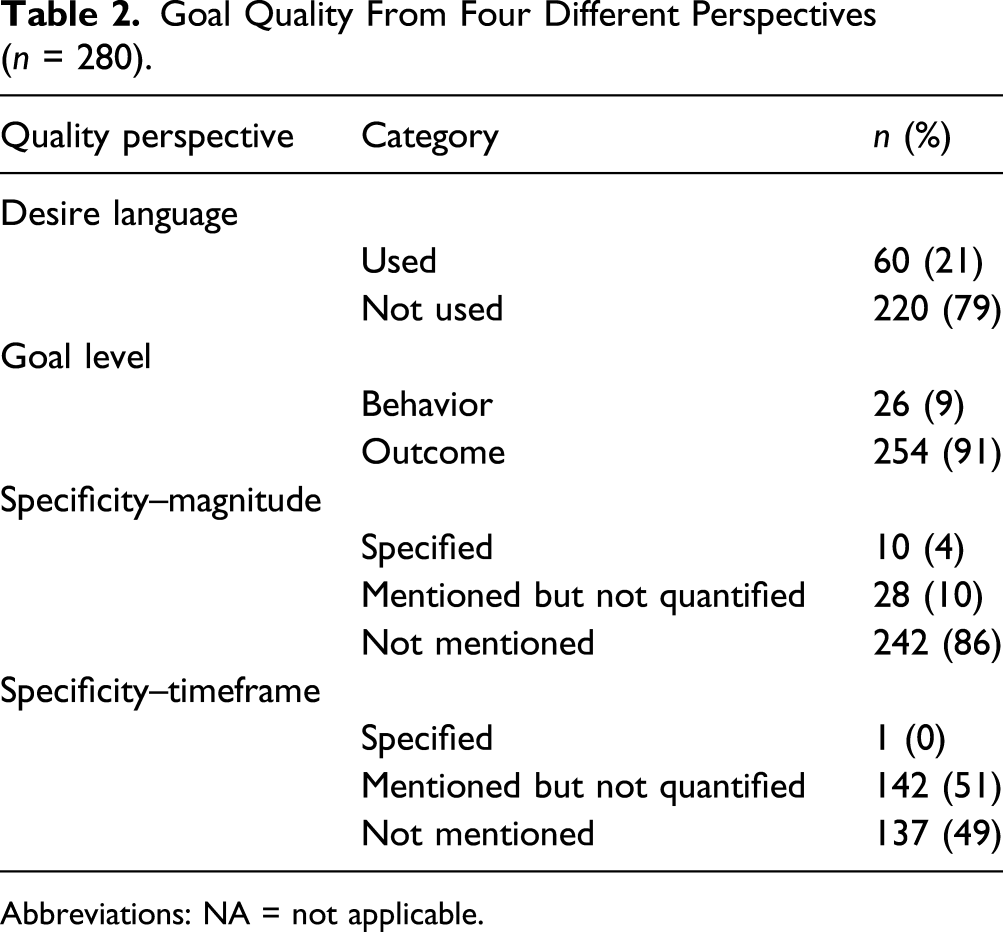
Abbreviations: NA = not applicable.
Influences on Applying MI and Goal Setting
The interviews revealed that the extents to which MI and goal setting were applied were influenced by the context and the care professional’s proficiency. Moreover, not all MI processes were sufficiently applied and are described in Figure 2 and in detail in the following text. Factors influencing the extent of performance of MI and goal setting within a proactive assessment program. Legend: green lines = positive influence; red lines = negative influence; solid line = strongly substantiated within our data; dashed line = moderately substantiated within our data. Abbreviations: MI = motivational interviewing.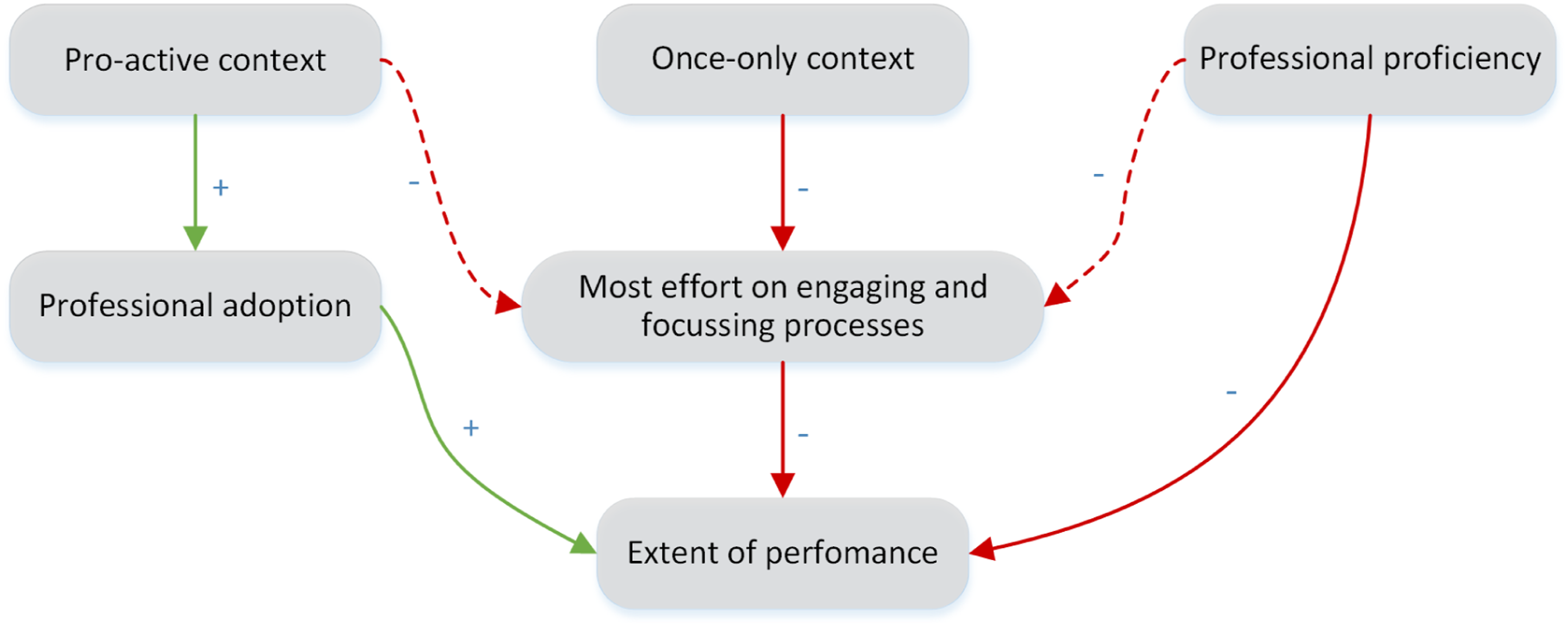
Context: Sage-atAge+ was proactive and once only
Care professionals expressed the need to increase participant motivation because of the proactive approach. However, because the older adults did not volunteer for the service, they experienced low ownership, did not expect benefit, felt no urgency, and started with a passive attitude. This resulted in care professionals needing to focus on overcoming significant motivational barriers. “Since you start from scratch in this visit, both for yourself and the one in front of you, one hour might not be enough to create internal motivation. So, during the conversation something will come up, but they also need to be motivated. “..” Only when it is something urgent, something they would have wanted to do for a long time, it will succeed.” (Elderly care physician)
Thus, there was high motivation among the care professionals to adopt MI techniques and goal setting. They believed these techniques could be of real benefit in engaging older adults and helping them to formulate and reach their goals. “[Sage-atAge+] is a supplement for frail older adults since they take their frailty for granted most of the time, or they don’t see it. By having a conversation with them, many things will come up. Things that they do not discuss with their [GP] or that just had slipped in.” (Dental care worker)
The proactive approach not only influenced the motivation of care professionals but also made engagement a delicate process. This was because the professionals often felt less authority and experienced friction during the engaging process. “At a certain moment you feel when people are having resistance, that you are meddling some one’s autonomy. I don’t think that is ok. “..” As a screener, without having a relationship with the patient, I should not cross that line.” (Nurse B)
The once-only context negatively influenced whether MI and goal setting were applied, often leaving the professionals feeling reluctant to engage in depth, specifically regarding psychological topics. “At some moments I was wary to get an intimate discourse by asking a certain question. And then I would never see them again. Yes, that is definitely a disadvantage.” (Nurse A)
The once-only context also made it difficult to reflect on earlier attempts and engagement with health behavior change, which hampered the evoking process. “That is also a disadvantage of seeing them only once. Otherwise you could ask them whether they succeeded or what challenges they experienced, since that is something we can work on together.” (Nurse C)
Care professional’s proficiency
Suboptimal proficiency in MI negatively influenced effective delivery. For example, the evoking process was hampered because some care professionals feared achieving an opposite result when triggering sustain talk. “It could be a sensitive issue for people, especially if you give them the feeling they are not performing well. “..” And since I did not know how to deal with that, I avoided the topic, to prevent saying the wrong things and making them grab their cigarettes. I did not feel familiar with that, so I preferred to avoid these topics.” (Nurse C)
Most care professionals expressed a need for ongoing training or booster sessions to improve their knowledge and to exchange their experiences (e.g., dealing with barriers). “And we also discussed the way we wrote stuff down [on the goal cards]. “..” You can consult each other … that would have been good, and I think it has been done too little, since that is something you can learn from.” (Nurse A)
Most effort was spent on the engaging and focusing processes
Professionals felt they lacked the time to execute all MI processes because of the need to overcome the barrier of low participant motivation during assessments. “You need to become acquainted with people, you need to win their trust, you are talking about what they have raised in the questionnaire, and you hope that they will find some motivation to start working on things that might have been considered obvious but could become a problem. That is a lot to do within a one-hour visit.” (Nurse B)
When mentioning a follow-up context, however, less time was spent on the engaging and focusing processes of MI. “And you notice, when people come for a follow-up visit, they will get back to the first conversation, and then it is easier to continue with what has been discussed before. It is easier to step in, so to speak. Because you have already won their trust.” (Nurse B)
The limited proficiency with MI of care professionals, especially with the evoking process, meant they felt more comfortable with the engaging and focusing processes. “For example, a man who is smoking and does not consider this an issue. At these moments I think ‘never mind, who am I to say something about this?’” (Nurse C)
Overall, the extents of performing MI and goal setting were positively influenced by the high motivation and attempted adoption by professionals. However, although the Sage-atAge+ context contributed to this motivation, it also hampered the extent of performance mostly because a lot of effort needed to be spent on the engaging and focusing processes. We found that the proficiency of participating care professionals was insufficient to overcome these barriers.
Discussion
Implementation research is essential for the successful translation of evidence-based interventions into practice. Using a mixed-methods strategy, we studied the extent to which MI and goal setting were performed within the Sage-atAge+ proactive assessment program for community-dwelling older adults (65+) to identify why we failed to show the hypothesized effect on well-being (Rietkerk, Gerritsen, et al., 2019). In the current study, we showed that goal setting was prevalent, but that MI fidelity and the quality of goals were suboptimal, despite high motivation by care professionals. Overall, the proactive and once-only context of the service, as well as the limited proficiency of the care professionals, were the main factors hindering successful implementation.
MI fidelity was low in our research, with only one in 11 interactions reaching all thresholds for which effect on behavior change was expected. Adherent behavior was also infrequent during the motivational interviews, despite its known effectiveness for improving healthy behaviors (Tonigan et al., 2018). When compared to GPs without training in MI (McKenzie et al., 2021), the consultations in our study had much better scores on the relational and technical summary scores, implying these care professionals performed better at engaging with their patients and in delivering patient-centered or patient-friendly consulting. However, the professionals did report limited proficiency, especially when evoking change talk, which is consistent with reports that it is the most difficult MI skill to acquire (Resnicow & McMaster, 2012). Limited proficiency is often seen in trials of MI (Forsberg et al., 2017) and can be attributed both to limited training and the need to update and consolidate skills over time through booster sessions (Miller & Rollnick, 2014).
Goal setting was highly implemented, with 90% of all letters to GPs containing at least one goal for which desire talk was prevalent. The mapping of these individual needs and wishes within goals is central to person-centered care (World Health Organization, 2015a) and was reflected in the positive attitudes of participants toward the service (Rietkerk, Smit, et al., 2019). However, only a minority of the formulated goals contained aspects that were expected to increase the potential for behavior change. The fact that professionals spent most effort and time in engaging and focusing participants meant that less time was available to specify goals further or to elaborate on goal planning.
Most goals that we identified were aimed at maintaining the status quo and not at delivering tangible improvements, which is in line with other recent research on proactive goal setting with community-dwelling older adults (Javadi et al., 2018). The fact that we detected preventive or long-term needs rather than urgent needs likely results from the proactive approach of Sage-atAge+. However, to achieve the actual benefits of preventive behavior change, much more effort is needed for goal planning compared to the requirement of goals that seek to achieve short-term benefits, especially for older people (Hall & Fong, 2007).
The proactive and once-only context of Sage-atAge+ was probably the main reason for care professionals spending most of their interaction time on the engaging and focusing processes of MI, and having very little time for evoking and planning. This represented the care professionals adapting to the needs of older adults, who often first required to set goals, before discussing their ambivalence for behavior change and starting action planning. However, by failing to complete all processes, the necessary tools to achieve meaningful change were not delivered. If a professional is to complete an assessment after only achieving engagement and focus, follow-up will be needed to specify goals through evoking and planning. This could explain the limited effect of any outpatient assessment service that lacks direct influence over the implementation of recommendations (Chen & Steinman, 2016). The modifying effect of this influence has also been reported in earlier reviews on the effects of outpatient assessment services (Pilotto et al., 2016). To date, we are unaware of any studies describing the role of failure to execute the goal planning process on the limited impact of those services.
Methodological Considerations
Some remarks can be made about the methods and validity of the current study. The mixed-methods strategy allowed us to explain the results of implementation, with the quantitative results complementing the qualitative results. Together, they formed the basis of our conclusion that suboptimal MI and goal setting explained the failure to achieve the hypothesized outcomes of the Sage-atAge+ program.
We complied with the criteria proposed by Jelsma et al. when coding and reporting the MI fidelity (Jelsma et al., 2015) but not with the minimum recommended collection of 20 interactions. Although this could have hampered the validity of our assessment of MI fidelity, it should be noted that we substantiated our fidelity findings by including the experiences of care professionals and by assessing the quality of goal setting. Consequently, we expect our conclusion about suboptimal MI to be valid.
We are not aware of a feasible goal taxonomy for coding comprehensive goal quality, consistent with an existing report that currently available goal setting evaluation tools are inadequate (Vermunt et al., 2017). Therefore, we combined several existing goal characteristic classifications from the literature. By doing so, we created a taxonomy that was feasible and had high agreement and reasonable kappa scores. The discussions between raters led to full agreement. With this taxonomy, we could provide insights into the characteristics and quality of goals, the proficiency of care professionals in goal setting, and the potential of goals to result in desired effects. However, external validation is needed before we can advocate further usage of this taxonomy.
It should also be noted that the care professionals who participated in this research did not receive specific training on the goal characteristics we reviewed with the taxonomy, which may have contributed to the low quality we found. In addition, this gives a useful insight into the reality of adding goal setting to daily practice without specific training.
Recommendations for future research and practice
Our current study results help to explain not only the extent of performance (i.e., how the older adult involvement was enhanced within the outpatient proactive assessment service) but also the factors that influenced that extent of performance. This may lead to service enhancements and adaptations, including the addition of behavior change techniques (Michie et al., 2011). For example, by allowing for follow-up to deliver goal planning services, we may improve participant engagement and increase effect on well-being. Equally, the implementation of MI could be enhanced to increase fidelity: this may involve extending the initial training, offering booster sessions, or better adapting to the needs of professionals by focusing on the process of evoking. Fidelity could even be monitored during service delivery to control for whether MI thresholds are reached.
In terms of future research goals, the impact of proactive approaches on participant engagement requires further study. It could be tested whether this is a key barrier in other integrated proactive programs for older adults. Such research into implementation may improve our understanding of the additional value of MI strategies within person-centered care for older adults. Designs can be improved to overcome the barriers to motivation and goal planning, such as implementing case management instead of once-only assessment strategies. However, if we are to deliver true person-centered care, we must avoid striving blindly for behavior change if it is at the expense of recognizing the goals of the older adult, who may not want behavior change.
Conclusions
In this mixed-methods implementation study, we aimed to identify the reasons for failure to achieve improved well-being in a previous study (Rietkerk, Gerritsen, et al., 2019). We found that MI fidelity and goal quality were suboptimal despite a high prevalence of goal setting. Several issues contributed to these problems. It is true that care professionals lacked some proficiency with MI, especially with the evoking process, resulting in less time being spent on evoking and planning, and decreasing the opportunity to resolve ambivalence to behavior change among the older adults. However, our findings indicate that this was not the full extent of the problem. Perhaps of even greater importance was the proactive and once-only context of the Sage-atAge+ service. To improve MI and goal setting implementation in the future, we should not only seek to focus on adding booster training sessions but also on adopting a case management approach that allows for adequate patient follow-up over multiple sessions. Lessons learned from implementation studies that are conducted alongside effect evaluations can help both to improve care and to develop effective and efficient care programs.
Supplemental Material
sj-pdf-1-jah-10.1177_0898264321993321 – Supplemental Material for Increasing Older Adult Involvement in Geriatric Assessment: A Mixed-Methods Process Evaluation
Supplemental Material, sj-pdf-1-jah-10.1177_0898264321993321 for Increasing Older Adult Involvement in Geriatric Assessment: A Mixed-Methods Process Evaluation by Wanda Rietkerk, Jannet de Jonge-de Haan, Joris P. J. Slaets, Sytse U. Zuidema and Debby L. Gerritsen in Journal of Aging and Health
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Innovation fund of Friesland Care Insurance (In Dutch: Innovatiefonds De Friesland Zorgverzekeraar), Leeuwarden, the Netherlands, (0710-14,599/ DS44).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.