
Abstract
To collect data on public health collaborations with schools of pharmacy, we sent a short electronic survey to accredited and preaccredited pharmacy programs in 2015. We categorized public health collaborations as working or partnering with local and/or state public health departments, local and/or state public health organizations, academic schools or programs of public health, and other public health collaborations. Of 134 schools, 65 responded (49% response rate). Forty-six (71%) responding institutions indicated collaborations with local and/or state public health departments, 34 (52%) with schools or programs of public health, and 24 (37%) with local and/or state public health organizations. Common themes of collaborations included educational programs, community outreach, research, and teaching in areas such as tobacco control, emergency preparedness, chronic disease, drug abuse, immunizations, and medication therapy management. Interdisciplinary public health collaborations with schools of pharmacy provide additional resources for ensuring the health of communities and expose student pharmacists to opportunities to use their training and abilities to affect public health. Examples of these partnerships may stimulate additional ideas for possible collaborations between public health organizations and schools of pharmacy.
Keywords
Through public health activities, the health of people, communities, and populations is protected and improved. 1 Pharmacists have been incorporated into an increasingly wide range of public health initiatives, including surveillance, community outreach, chronic disease management, vaccinations, emergency preparedness, and global health. 2 –9 Documents issued by the US Public Health Service, 10 the Centers for Disease Control and Prevention, 11 and the National Association of County and City Health Officials 6 support these roles. Prominent public health organizations have addressed the role of pharmacists in public health and called for expanded public health training for student pharmacists. 12 In 2014, the American Public Health Association established the Special Primary Interest Group for Pharmacy, a group within the organization that members can join in if they are interested in pharmacy and/or work in pharmacy. 13 Major pharmacy organizations have also published statements calling for greater public health roles for pharmacists, 14,15 and many provide forums for members interested in public health (eg, American Association of Colleges of Pharmacy Public Health Special Interest Group [AACP PH-SIG]). 16
In parallel with these developments, key milestone reports and documents in academic pharmacy have addressed the importance of preparing student pharmacists for public health service. Public health has been highlighted as an important area of pharmacy education in every outcome document of the Center for the Advancement of Pharmaceutical Education, 17 –19 and the Accreditation Council for Pharmacy Education (ACPE) standards have subsequently required training in population and public health. 20,21 Although public health is a requirement in the curricula of pharmacy schools, administrators and faculty at each institution can incorporate this topic as they deem appropriate. Consequently, schools of pharmacy have developed a wide range of programs, including stand-alone public health courses, incorporating public health topics into existing didactic coursework, establishing dual doctor of pharmacy/master of public health (PharmD/MPH) degrees, and offering experiential opportunities. 22
The emergence of public health pharmacy practice in the United States has also created opportunities for partnerships among schools of pharmacy and public health–oriented organizations and agencies. Pharmacy faculty members have reached out to public health departments and organizations and responded to their inquiries to collaborate on projects often involving student pharmacists. These partnerships provide valuable experiences for students and faculty, and such partnerships have helped both fields expand their public health services and access across multiple settings. Through public health–academic pharmacy partnerships, collaborative learning environments can be established while striving to affect community and public health. 23
These partnerships offer enhanced learning experiences for students, in the form of service learning, active learning, place-based education, and interprofessional education, and they give students an opportunity to work on authentic projects that directly serve communities. 19 However, no systematic surveys have been conducted to describe the status of public health collaborations with schools of pharmacy. The objective of this project was to collect quantitative and qualitative data describing public health collaborations with schools of pharmacy accredited and preaccredited by ACPE.
Methods
Members of the Development Committee of the AACP PH-SIG developed a brief survey in February 2015 to collect information about public health collaborations with schools of pharmacy. The following information was collected from 3 main survey items: (1) name and address of the school of pharmacy (free-text box); (2) type of collaboration or partnership with state and/or local public health departments, state and/or local public health organizations, academic schools or programs of public health, or other public health collaborations (check all that apply); and (3) description of other collaboration type (free-text box). Respondents were then asked in an open-ended item to describe each type of reported public health collaboration. Respondents could include their contact information in a free-text box if they were willing to be contacted for follow-up information.
The survey was administered electronically by Qualtrics Labs Inc (Provo, Utah). Initially, the survey was sent to people who were registered in the AACP PH-SIG email list during the 2015 spring semester. One follow-up email was sent. If >1 response was received from the same school of pharmacy, the answers were combined into 1 survey response representing that school of pharmacy. Nonresponding schools were identified through the ACPE directory 24 during the fall 2015 semester. The survey was sent to administrators (deans or department chairs) or selected faculty members at nonresponding schools. The email encouraged respondents to complete the survey, even if the institution was not currently involved in any public health collaborations. Two follow-up emails were sent.
We analyzed quantitative data with descriptive statistics by using Microsoft Excel 2013. A thematic analysis was performed on open-ended responses for each type of public health collaboration. The responses about types of collaborations with local and/or state public health departments and local and/or state public health organizations were similar, so they were combined into 1 category. Coding was performed on these open-ended responses to generate common themes. A common theme was deemed to be any thought, idea, or experience noted by ≥2 respondents. The project was considered exempt by the Ohio Northern University Institutional Review Board.
Results
Of 134 schools of pharmacy accredited or preaccredited by ACPE, surveys from 65 programs were received, for a 49% response rate. Institutions in 32 states, from all geographic regions of the United States, Washington, DC, and Puerto Rico, and an ACPE-accredited program in Lebanon responded to the survey. A similar number of responses were received from public and private institutions: 51% (33 of 65) and 49% (32 of 65), respectively. As of July 2016, ACPE reported that 48% of schools of pharmacy were in publicly supported universities and 52% were in private institutions. Of the 65 institutions that completed the survey, 59 were fully accredited, 4 were candidates for preaccreditation, and 2 were precandidates for preaccreditation. Accreditation status among public and private institutions was similar. Among public institutions responding to the survey, 30 were accredited, 2 had candidate status, and 1 had precandidate status; among private institutions, 29 were accredited, 2 had candidate status, and 1 had precandidate status. The profiles of respondent schools (ie, proportion of public vs private institutions and accreditation status) paralleled that of the entire population.
Of the 65 responding institutions, 46 indicated collaborations with local and/or state public health departments, 24 with local and/or state public health organizations, 34 with schools or programs of public health, and 13 with other public health entities. Eleven institutions reported no collaborations with public health departments, organizations, or academic schools or programs of public health (Table 1).
Types of public health collaborations reported by Accreditation Council for Pharmacy Education accredited and preaccredited schools of pharmacy (n = 65) in an electronic survey administered in spring and fall 2015
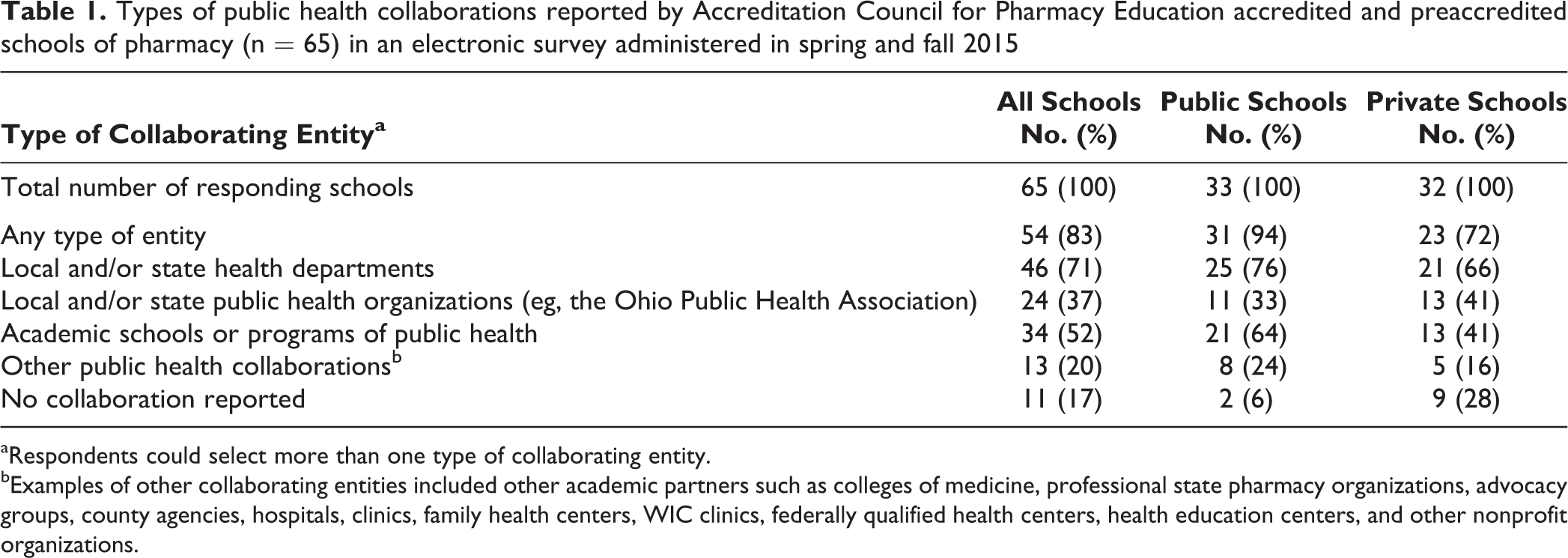
aRespondents could select more than one type of collaborating entity.
bExamples of other collaborating entities included other academic partners such as colleges of medicine, professional state pharmacy organizations, advocacy groups, county agencies, hospitals, clinics, family health centers, WIC clinics, federally qualified health centers, health education centers, and other nonprofit organizations.
Participants were also asked to describe their public health collaborations using open-ended responses (Table 2). Seven themes emerged about collaborations with local and/or state public health departments/public health organizations: student and faculty representation in public health organizations, public health engagement, clinical training partner, research, community outreach, teaching, and contracts and consulting. Respondents reported various types of collaborations. For example, local and state health departments and schools of pharmacy partnered to provide vaccinations, antibiotic stewardship, and tobacco cessation and control programs. Students assisted with events focused on medication reviews and patient education about chronic disease states (eg, diabetes, hypertension, asthma). Pharmacy students educated community members on topics such as substance abuse and immunizations in multiple settings (eg, middle schools, health fairs). Students also assisted health departments with projects such as rabies assessments and naloxone outreach. Respondents described emergency preparedness training, protocol development, and simulation (eg, emergency response point-of-dispensing drills). Partnerships to secure funds to increase access to public health services were also reported. For example, a faculty member at a school of pharmacy provided expertise in data collection and analysis, which enabled regional county health departments to obtain grant funding from the state health department to ensure the quality and accessibility of local public health services. Along with local and state public health departments, other funding sources included the Centers for Disease Control and Prevention, National Institutes of Health, and Health Resources & Services Administration, which supported such activities as medication therapy management, provision of services in rural areas, and research.
Collaborations reported by the Accreditation Council for Pharmacy Education accredited and preaccredited schools of pharmacy (n = 65) in an electronic survey administered in spring and fall 2015, by types of collaborations and common themes
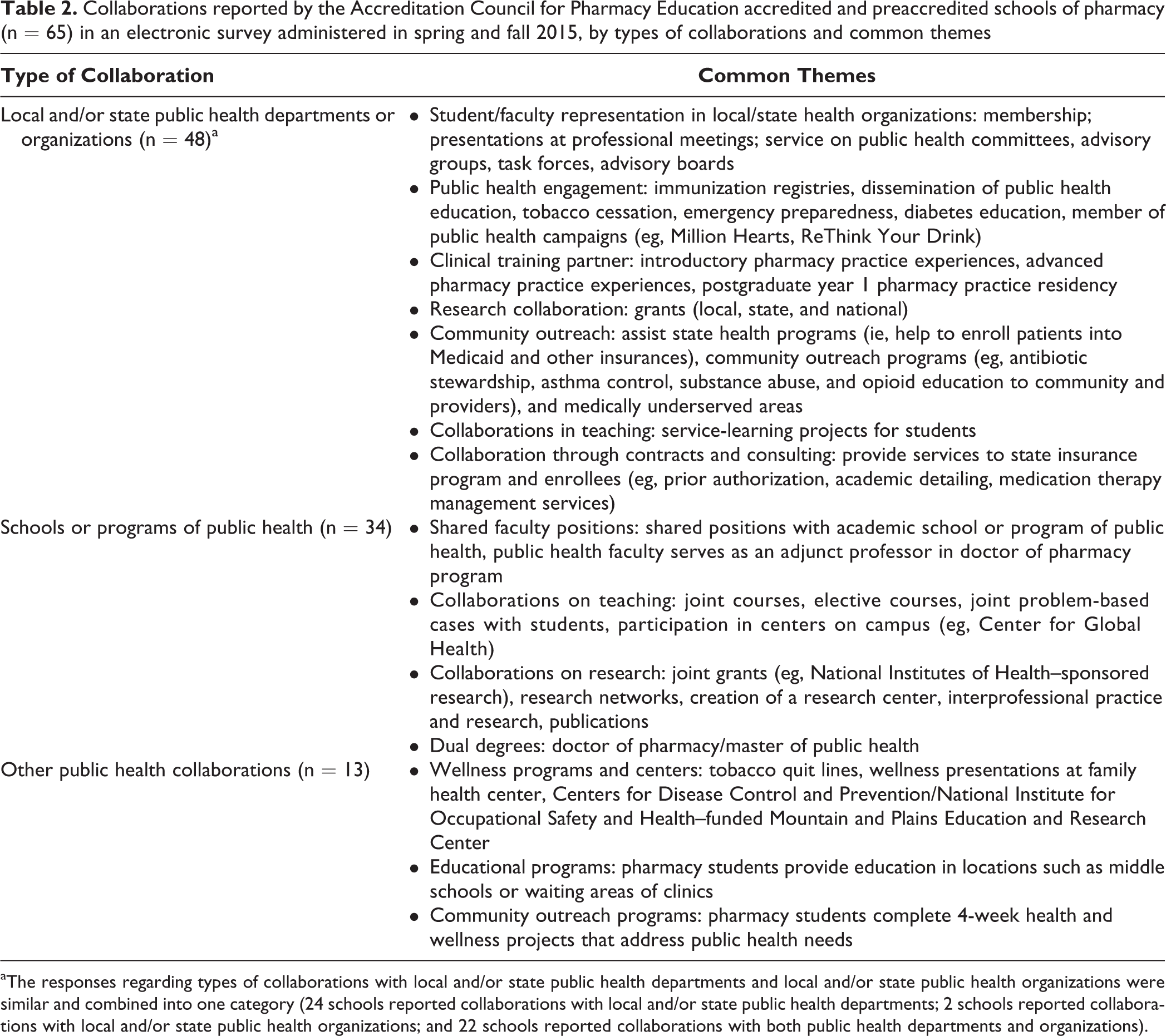
aThe responses regarding types of collaborations with local and/or state public health departments and local and/or state public health organizations were similar and combined into one category (24 schools reported collaborations with local and/or state public health departments; 2 schools reported collaborations with local and/or state public health organizations; and 22 schools reported collaborations with both public health departments and organizations).
Respondents also collaborated with academic schools and programs of public health through shared faculty positions, teaching, research, and dual-degree programs (eg, PharmD/MPH). For example, 1 respondent described how a school of public health and school of pharmacy partnered to coteach a public health course that was required for first-year pharmacy students and was an elective for public health students. Several faculty members indicated that pharmacy students could take courses offered by their university’s school or program of public health for elective credit or that public health faculty provided content for pharmacy courses. Cross-program faculty appointments were reported in areas of health equity and cancer health disparities.
Discussion
These survey results illustrate how schools of pharmacy are collaborating with local and/or state public health departments, local and/or state public health organizations, and academic schools and programs of public health. Survey respondents reported integrating pharmacy and public health in practice and education for student pharmacists and pharmacy faculty. These partnerships can help to provide services in public health settings with limited funding. Respondents also reported on collaborations in the provision of didactic courses and cross-program faculty appointments for schools and programs of public health and schools of pharmacy, which integrates educational and service-related training and fosters interprofessional learning environments. Collective efforts toward improving the health of communities, while providing unique learning experiences for student pharmacists, depends greatly on finding opportunities across diverse public health settings and sectors. For schools of pharmacy that currently lack involvement with public health organizations, the results of this survey may provide ideas for future partnerships or educational opportunities.
We gathered data for this study using an open-ended survey item that prompted respondents to describe public health collaborations. To collect data on all collaborations with public health entities, a more general and broader survey item allowed respondents to describe collaborations and public health activities in their own words. Future studies could gather more detailed information from all schools of pharmacy about collaborations with public health organizations by using more structured and guided survey items with example collaborations provided from this survey.
No studies have queried public health organizations or academic schools and programs of public health on their collaborations with schools of pharmacy, including determining if these opportunities were valuable. Future studies should evaluate the effectiveness of these collaborations, including measuring public health outcomes and conducting cost-benefit analyses of these interdisciplinary partnerships. In addition, as the demand for preventive health services increases, the need for additional resources to provide these services will also increase. Understanding the perceptions of academic pharmacy as an added gateway to preventive services will be important when developing new collaborations and partnerships. Documentation of public health services provided, perceptions of collaborative partnerships with schools of pharmacy, and the value of student pharmacists in these settings should be evaluated.
Limitations
Our study had several limitations. First, the response rate was low. However, respondents were a representative sample of all schools of pharmacy accredited and preaccredited by ACPE, and schools from all regions of the country participated in the survey. The profiles of respondent schools (ie, proportion of public vs private institutions and accreditation status) paralleled that of the entire population, and schools from all regions of the country participated in the survey. Second, administrators or faculty members from nonresponding programs were not sent follow-up emails to determine their reasons for not responding. A cover letter accompanying the survey asked recipients to complete the survey even if the school had no current partnerships in public health. Therefore, we do not know whether nonresponding schools had public health collaborations to report.
Conclusion
Interdisciplinary public health collaborations with schools of pharmacy have created partnerships that provide additional resources to ensure the health of communities, while allowing student pharmacists the opportunity to collaborate with public health professionals, agencies, and organizations to affect public health nationwide. Examples of these partnerships may stimulate additional ideas for possible collaborations between public health organizations and schools of pharmacy.
Footnotes
Acknowledgments
We thank Christine Orosz, PharmD candidate, Ohio Northern University Raabe College of Pharmacy, for her assistance in identifying some of the contact information used for the fall 2015 survey.
Author Notes
A subset of these data was presented at the American Association of Colleges of Pharmacy Annual Meeting (July 2015) and the American Public Health Association Annual Meeting (November 2016).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.