
Abstract

National Vaccine Advisory Committee
Chair
Walt A. Orenstein, MD, Emory University, Atlanta, GA (former NVAC chair) Kimberly M. Thompson, ScD, University of Central Florida College of Medicine, Orlando, FL (NVAC chair as of June 2016)
Designated Federal Official
Bruce G. Gellin, MD, MPH, National Vaccine Program Office, US Department of Health and Human Services, Washington, DC
Public Members
Richard H. Beigi, MD, MSc, Magee-Womens Hospital, Pittsburgh, PA Sarah Despres, JD, Pew Charitable Trusts, Washington, DC David Fleming, MD, PATH, Washington, DC Ann Ginsberg, MD, PhD, Aeras, Rockville, MD Ruth Lynfield, MD, Minnesota Department of Health, St Paul, MN Yvonne Maldonado, MD, Stanford University School of Medicine, Stanford, CA Saad Omer, PhD, MBBS, MPH, Emory University, Atlanta, GA Wayne Rawlins, MD, MBA, Aetna, Hartford, CT Mitchel C. Rothholz, RPh, MBA, American Pharmacists Association, Washington, DC Nathaniel Smith, MD, MPH, Arkansas Department of Health, Little Rock, AR
Representative Members
Timothy Cooke, PhD, NovaDigm Therapeutics, Grand Forks, ND Philip Hosbach, Sanofi Pasteur, Swiftwater, PA
Executive Summary
Recognizing the importance and impact of maternal immunizations on public health, the Assistant Secretary for Health of the US Department of Health and Human Services charged the National Vaccine Advisory Committee (NVAC) in June 2012 with reviewing the state of maternal immunizations and existing best practices to identify programmatic gaps and/or barriers to the implementation of current recommendations regarding maternal immunization. The NVAC established the Maternal Immunization Working Group in August 2012 to conduct these assessments and to provide recommendations for overcoming identified barriers. The report that follows reflects the work of the group charged with identifying barriers to and opportunities for developing vaccines for pregnant women and making recommendations to overcome these barriers. The NVAC working group initially focused its efforts on 4 areas: (1) ethical issues, (2) policy issues, (3) preclinical and clinical research issues, and (4) provider education and support issues.
Introduction
Infants are vulnerable to vaccine-preventable diseases (VPDs) during the first months of life due in part to the susceptibility gap that occurs when they are too young to be vaccinated but are still at a considerable risk of morbidity and mortality from those diseases. Early infancy, including the neonatal period (the first 28 days of life), is the most vulnerable time for childhood survival. 1 The risk of influenza hospitalization in infants <6 months of age is higher than in older children or the elderly. 2,3 Furthermore, although infants are at a substantially higher risk of influenza-related complications, the available influenza vaccines are not licensed for use in infants <6 months of age. 4
NVAC Maternal Immunization Working Group Phase II
Maternal Immunization Working Group Chairs
Richard H. Beigi, MD, MSc, Magee-Womens Hospital, Pittsburgh, PA Saad Omer, PhD, MBBS, MPH, Emory University, Atlanta, GA
NVAC Members
Seth Hetherington, MD, Genocea Biosciences, Cambridge, MA (former NVAC member) Ruth Lynfield, MD, Minnesota Department of Health, St Paul, MN
NVAC Liaison Representatives
Carol J. Baker, MD, Infectious Diseases Society of America, Arlington, VA Niranjan Bhat, MD, MHS, PATH, Seattle, WA Jan Bonhoeffer, MD, Brighton Collaboration, Basel, Switzerland Gina Burns, BSN, The Group B Strep Association, Chapel Hill, NC Leonard Friedland, MD, Biotechnology Innovation Organization, Washington, DC Debra Hawks, MPH, American College of Obstetricians and Gynecologists, Washington, DC Deborah Higgins, PATH, Seattle, WA Sharon Humiston, MD, MPH, American Academy of Pediatrics, Vancouver, WA Cynthia Pellegrini, March of Dimes, Washington, DC Jeanne Sheffield, MD, Society for Maternal-Fetal Medicine, Washington, DC Ajoke Sobanjo-ter Meulen, MD, MSc, Bill & Melinda Gates Foundation, Seattle, WA Danitza Tomianovic, PhD, Brighton Collaboration, Basel, Switzerland
NVAC Subject Matter Experts
Steven Black, MD, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH Fran Cunningham, PharmD, US Department of Veterans Affairs, Washington, DC Kathryn M. Edwards, MD, Vanderbilt University, Nashville, TN Catherine Mary Healy, MBBCh, Baylor College of Medicine, Houston, TX Flor M. Muñoz, MD, MSc, Baylor College of Medicine, Houston, TX Fernando Polack, MD, Fundacion INFANT, Buenos Aires, Argentina Geeta K. Swamy, MD, Duke University, Durham, NC
NVAC Ex Officio Members
Karen R. Broder, MD, Centers for Disease Control and Prevention, Atlanta, GA Cheryl Broussard, PhD, Centers for Disease Control and Prevention, Atlanta, GA Marion F. Gruber, PhD, US Food and Drug Administration, Silver Spring, MD Avril Houston, MD, MPH, Health Resources and Services Administration, Rockville, MD Emily Levine, JD, Office of the General Counsel, US Department of Health and Human Services, Washington, DC Jennifer Liang, DVM, MPVM, Centers for Disease Control and Prevention, Atlanta, GA Valerie Marshall, MPH, US Food and Drug Administration, Silver Spring, MD Stacey Martin, MSc, Centers for Disease Control and Prevention, Atlanta, GA Richard Martinello, MD, US Department of Veterans Affairs, Washington, DC Pedro L. Moro, MD, MPH, Centers for Disease Control and Prevention, Atlanta, GA Barbara Mulach, PhD, National Institutes of Health, Bethesda, MD Mirjana Nesin, MD, National Institutes of Health, Bethesda, MD Jennifer S. Read, MD, MS, MPH, National Institutes of Health, Bethesda, MD Jeffrey Roberts, MD, US Food and Drug Administration, Silver Spring, MD Amina White, MD, National Institutes of Health, Bethesda, MD COL Margaret Yacovone, MD, US Department of Defense, Washington, DC
Contributors and Technical Advisors
Karin Bok, PhD, MS, National Vaccine Program Office, US Department of Health and Human Services, Washington, DC Bruce G. Gellin, MD, MPH, National Vaccine Program Office, US Department of Health and Human Services, Washington, DC Jennifer Gordon, PhD, National Vaccine Program Office, US Department of Health and Human Services, Washington, DC Cristina H. Messina, PhD, MS, National Vaccine Program Office, US Department of Health and Human Services, Washington, DC
The lack of measures to protect infants from complications caused by a disease for which a vaccine is available for older children needs to be addressed. Immunizing pregnant women to allow for transplacental transfer of maternal antibodies to the infant, who will thus be born with existing antibodies against VPDs (eg, influenza, pertussis, tetanus), has reduced the burden of these diseases in infants in the United States. 5 This strategy has led to an exploration of using the same approach to protect infants from complications caused by other infectious diseases that could also be prevented by immunization (eg, respiratory syncytial virus [RSV] and group B streptococcus [GBS]). 6 –8
Influenza
In the 1960s, the Advisory Committee on Immunization Practices, which is managed by the Centers for Disease Control and Prevention (CDC), acknowledged the benefits of maternal influenza immunization in preventing disease in the infant and in the mother. It was then that CDC first recommended that the influenza vaccine be administered to pregnant women with high-risk medical conditions. 9 An update of this recommendation in 2004 called for pregnant women to be vaccinated for influenza during any trimester and to vaccinate women who may become pregnant during the influenza season. 10,11
The coverage rate for the influenza vaccine administered during pregnancy since the recommendation was implemented has varied, but coverage reached 47% after the 2009 H1N1 pandemic. 12 For the 2013-2014 influenza season, CDC reported an increase in coverage up to 52.2% among pregnant women (17.6% of women received the vaccine before pregnancy and 34.6% during pregnancy). The percentage of coverage was steady during subsequent influenza seasons. 13
Maternal influenza vaccination is an effective strategy for protecting infants <6 months of age from influenza-like illness and influenza-related hospitalizations. A retrospective study of 245 386 women and 249 387 infants showed that infants who were born to vaccinated mothers had a 64% reduced risk for influenza-like illness, a 70% reduced risk for laboratory-confirmed influenza, and an 81% reduced risk for influenza-related hospitalization within the first 6 months of life. 14 Other studies have shown an association between maternal influenza vaccination and reduced incidence of hospitalization for acute respiratory illness (regardless of etiology) among infants <6 months of age. 15 Preventing maternal influenza infection might additionally reduce the risk of the mother passing the infection to the infant and could result in transmission of antibodies to the infant through breast milk. 16 Furthermore, some studies have suggested that influenza vaccination during pregnancy may have other indirect benefits, such as a decrease in the rate of infants born small for gestational age, a decrease in the rate of preterm birth, and improvement in other birth outcomes. However, these findings were not consistent among recent randomized clinical trials and observational studies. 15,17 –19 These studies suggest that vaccinating pregnant women against influenza not only protects the infant from influenza disease-like symptoms but may also provide additional health benefits for the mother and the infant.
Pertussis
Infants are also exposed to other VPDs, such as pertussis (whooping cough). Infants have higher rates of pertussis infections than the rest of the population and constitute the largest burden of pertussis-related deaths, revealing the need to protect infants against whooping cough. 20 From 2012 to 2013, CDC reported 3159 cases of pertussis in infants <6 months of age and 892 cases of pertussis in infants aged 6-11 months. 20 In 2014, most pertussis-related deaths occurred among infants <3 months of age. 21 Maternal immunization with the tetanus, diphtheria, and pertussis (Tdap) vaccine has been shown to effectively protect infants through the passive transfer of antibodies from mother to baby. Thus, in 2012, CDC recommended the routine administration of a Tdap booster dose for pregnant women 22 and further recommended that women be revaccinated between 27 and 36 weeks of gestation with each subsequent pregnancy. 23 Although this recommendation has been in place for several years, rates of coverage for Tdap vaccination among pregnant women are low. An observational study of 438 487 live births from 2007 to 2013 found that only 14% of the mothers had received the Tdap vaccine during pregnancy. Efforts by CDC and professional societies helped increase Tdap rates in pregnant women to 41.7% as of 2013, but efforts are needed to increase these rates. 24
Maternal Tdap administration has been shown to be both safe and immunogenic; no acute maternal safety events or increased risks to the infant or mother have been reported to date. 24 –28 In the United Kingdom, infants born to mothers vaccinated with Tdap during pregnancy were less likely to have confirmed pertussis and more likely to have a reduction in pertussis-associated hospitalizations as compared with infants born to unvaccinated mothers, demonstrating the effectiveness of Tdap immunization in decreasing infant disease. 29 Tdap immunization during pregnancy is also associated with higher levels of pertussis antibodies in the infant, which remain present at 2 months of age, 25,30 and these high levels of pertussis antibodies in the cord blood have been correlated with protection against pertussis infection. 31 These studies further validate the potential for maternal immunization as a strategy to protect infants from diseases such as pertussis.
Tetanus
Prenatal tetanus toxoid immunization is another example of how maternal immunization strategies have reduced the burden of infant disease. 5 Implementation of a tetanus immunization program during pregnancy in countries where neonatal tetanus is an issue resulted in a reduction of 94% in neonatal mortality. 5,32,33 Although neonatal tetanus is not a concern in the United States, the implementation of maternal tetanus toxoid immunization globally is another example of how immunizing pregnant women against VPDs reduces and prevents disease in infants. 5,32
Additional Targets for Maternal Immunization: RSV and GSB
Immunizing pregnant women against influenza has had such a positive outcome that the same approach should certainly be taken with immunizations against other diseases that put infants at risk, such as RSV and GBS, 34,35 among others.
RSV infection often leads to viral pneumonia in infants <2 years of age and is responsible for high infant morbidity and mortality globally. RSV vaccination during pregnancy would most likely provide temporary protection to vulnerable infants, for whom the burden of hospital admission and death is the greatest. 36 GBS infection acquired during birth (ie, perinatal transmission from mother to newborn) may be prevented by vaccinating pregnant women and thereby eliciting high levels of GBS-specific antibodies. This, in turn, could potentially prevent perinatal transmission of GBS. High concentrations of antibodies in the pregnant mother may also protect infants against late-onset GBS disease by passively transferring these protective antibodies transplacentally. 37,38 These infectious diseases, which are still highly prevalent in infants, are just a few examples of why maternal immunization efforts need to continue to be supported as a strategy to protect infants.
Maternal immunizations have been an effective strategy to protect both the mother and the infant against VPDs. However, substantial barriers remain that prevent the development and licensing of additional vaccines for maternal immunization strategies. These barriers include ethical and policy considerations about including pregnant women in research, the need for continued support of preclinical and clinical research on immunity, the impact and safety of immunizations during pregnancy, and the need to educate obstetric providers about the benefits of immunizations during pregnancy and the importance of including pregnant women in clinical research trials to provide high-quality health care. The US Department of Health and Human Services recognized the need to address these barriers and subsequently charged the National Vaccine Advisory Committee (NVAC) with making recommendations to address the problem.
Charge to the NVAC
Recognizing the importance and impact of maternal immunizations on public health, the Assistant Secretary for Health (ASH) charged the NVAC in June 2012 with reviewing the state of maternal immunizations and existing best practices to identify programmatic gaps and/or barriers to implementing current recommendations for maternal immunization. The NVAC tasked the Maternal Immunization Working Group in August 2012 with conducting these assessments and providing recommendations for overcoming any identified barriers. The NVAC separated the charge into 2 sections: (1) reviewing the current state of maternal immunizations and existing best practices to identify programmatic gaps and/or barriers to the implementation of current recommendations regarding maternal immunization and (2) identifying barriers to and opportunities for developing vaccines for pregnant women.
These 2 objectives were studied and considered, and recommendations were issued separately, mainly because they necessitated different subject-matter expertise. The first report, which was published in January 2015, recommended that the use of vaccines during pregnancy, such as those against influenza and pertussis, be incorporated as a standard of obstetric care as well as a standard of practice among all health care providers who administered health care services to pregnant women. 39 The current report reflects the work on the second objective on the charge. The NVAC working group initially identified 4 main focus areas: (1) ethical issues, (2) policy issues, (3) preclinical and clinical research issues, and (4) provider education and support issues (Table).
Invited speakers and topic presentations to the National Vaccine Advisory Committee Maternal Immunization Working Group Phase II, 2015-2016
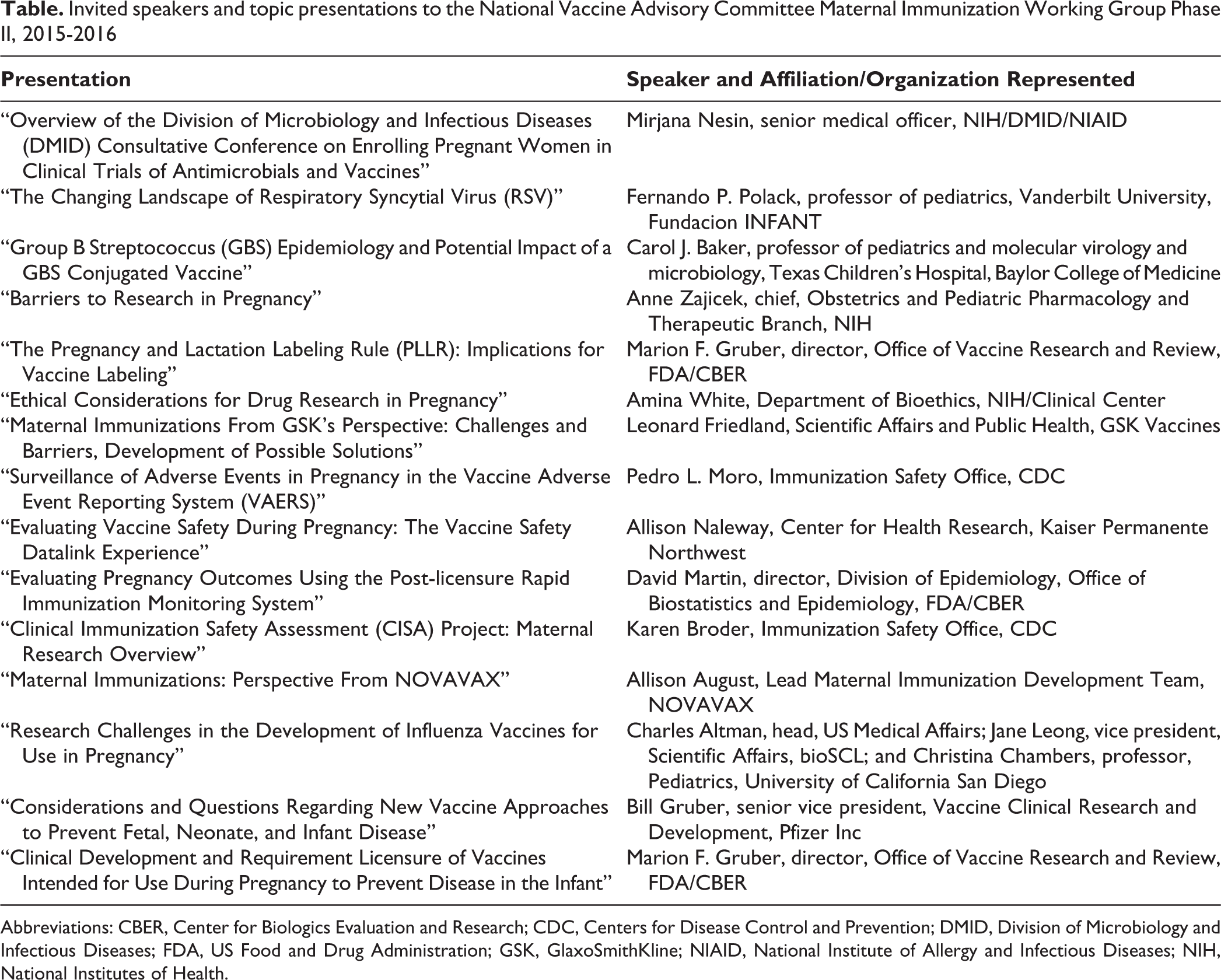
Abbreviations: CBER, Center for Biologics Evaluation and Research; CDC, Centers for Disease Control and Prevention; DMID, Division of Microbiology and Infectious Diseases; FDA, US Food and Drug Administration; GSK, GlaxoSmithKline; NIAID, National Institute of Allergy and Infectious Diseases; NIH, National Institutes of Health.
NVAC Recommendations
Focus Area 1: Ethical Issues
The ASH should work with the Office for Human Research Protections and other relevant stakeholders and agencies to revise the current exclusionary climate of research in pregnancy. Such areas of focus include but are not limited to the following:
Institutional review board (IRB) guidance on interpretation of minimal risk Code of Federal Regulations (CFR) language surrounding research in pregnancy Collaboration with bioethics experts, regulatory agencies, and the scientific community to optimize the design of studies to minimize the risk of interventions for research in pregnancy Relevant regulations, statutes, and policies that should be modified to indicate that pregnant women are not a vulnerable population for the purposes of ethical review
The ASH should work with the Office for Human Research Protections and the stakeholder community to develop policy and regulatory guidelines that would promote inclusion of pregnant women in clinical trials when scientifically appropriate.
Exclusion of pregnant research subjects
Participation in important areas of research continues to fall behind among women in general compared with men, especially among pregnant women, who are not frequently recruited to participate in vaccine research trials. One could argue that the systematic exclusion of pregnant women from clinical research that might lead to substantial benefits to the mother and the infant is harming rather than protecting the woman and fetus from injuries and that it is highly consequential. Although there is concern that including pregnant women in the study of new drugs and vaccines could lead to fetal harm, it is important to recognize that excluding pregnant women from research can also lead to harm. 40
Most pregnant women are affected by illnesses that require treatment or immunizations during pregnancy or immunizations administered for the infant’s benefit. Nonetheless, few drugs and no immunizations are currently approved or specifically indicated for use in pregnancy by the US Food and Drug Administration (FDA). If the medical treatment of pregnant women is based on studies from which they were excluded as participants, a concern of generalizability must be raised, because pregnant women are at risk of not receiving the same level of care available to the rest of the population. 40
Another challenge that contributes to the exclusionary climate toward pregnant women in clinical trials is that researchers currently must justify the inclusion of pregnant women to regulatory authorities and specify the special protections that will be in place during product testing.
34
Interestingly, there is no requirement to justify the exclusion of pregnant women from a protocol. To modify this approach, the wording of Subpart B of the CFR (the human research subject protection rules that deal specifically with pregnant subjects) was changed in 2001 (45 CFR §46 Subpart B). The new language states that pregnant women may be involved in research if all of the following conditions are met: (a) Where scientifically appropriate, preclinical studies, including studies on pregnant animals, and clinical studies, including studies on nonpregnant women, have been conducted and provide data for assessing potential risks to pregnant women and fetuses; (b) The risk to the fetus is caused solely by interventions or procedures that hold out the prospect of direct benefit for the woman or the fetus; or, if there is no such prospect of benefit, the risk to the fetus is not greater than minimal and the purpose of the research is the development of important biomedical knowledge which cannot be obtained by any other means; (c) Any risk is the least possible for achieving the objectives of the research; (d) If the research holds out the prospect of direct benefit to the pregnant woman, the prospect of a direct benefit both to the pregnant woman and the fetus, or no prospect of benefit for the woman nor the fetus when risk to the fetus is not greater than minimal and the purpose of the research is the development of important biomedical knowledge that cannot be obtained by any other means, her consent is obtained in accord with the informed consent provisions of subpart A of this part; (e) If the research holds out the prospect of direct benefit solely to the fetus then the consent of the pregnant woman and the father is obtained in accord with the informed consent provisions of subpart A of this part, except that the father’s consent need not be obtained if he is unable to consent because of unavailability, incompetence, or temporary incapacity or the pregnancy resulted from rape or incest. (f) Each individual providing consent under paragraph (d) or (e) of this section is fully informed regarding the reasonably foreseeable impact of the research on the fetus or neonate; (g) For children as defined in § 46.402(a) who are pregnant, assent and permission are obtained in accord with the provisions of subpart D of this part; (h) No inducements, monetary or otherwise, will be offered to terminate a pregnancy; (i) Individuals engaged in the research will have no part in any decisions as to the timing, method, or procedures used to terminate a pregnancy; and (j) Individuals engaged in the research will have no part in determining the viability of a neonate. (45 CFR §46.204)
Pregnant women are not a vulnerable population
One reason that pregnant women are excluded from participating in clinical trials is that they are perceived as being a “vulnerable population.” A vulnerable population is defined as one that has a compromised ability to protect its interests and provide informed consent. 45 However, pregnant women have the same capacity to make decisions, ability to judge risks and benefits, and ability to provide informed consent as their nonpregnant counterparts. Thus, in 2010, a workshop sponsored by the National Institutes of Health Office of Research on Women’s Health proposed that pregnant women in clinical trials be defined as a scientifically complex population rather than as a vulnerable population. 40,45 This classification is intended to reflect a combination of physiologic and ethical complexities that should be considered when balancing the interests of pregnant women and the interests of their newborns. This proposal was later supported by the American College of Obstetricians and Gynecologists expert committee opinion and the American Academy of Pediatrics. 40
IRB interpretation of minimal risk
Another barrier to including pregnant women in clinical trials is the inconsistency of interpreting regulations across IRBs. IRBs are tasked with reviewing and approving research protocols that protect the rights and welfare of human subjects. One of the most problematic issues that IRBs face is the interpretation of minimal risk. Without clear standards that define a threshold of acceptable risk associated with research, IRBs have to strike a delicate balance between what they consider to be acceptably low harm or discomfort and what they consider to be the benefit of the research. This concern about interpretation of minimal risk was raised by federal and nonfederal stakeholders and currently affects clinical research in other populations as well. However, it is an especially sensitive topic during the review of research that calls for protecting mothers and infants.
In 2008, the Secretary’s Advisory Committee on Human Subjects Research issued recommendations advising on the interpretation of minimal risk related to all subjects involved in clinical research but did not address the population of pregnant women specifically. Although the advisory committee gave its view and expanded on the definition of minimal risk as stated in the CFR (45 CFR part 46), it also clearly pointed out that “in its estimate of research-related risk, the IRB should carefully consider the characteristics of subjects to be enrolled in research including an evaluation of subject susceptibility, vulnerability, resilience, and experience in relation to the anticipated harms and discomforts of research involvement.” 49 In view of the IRB’s responsibilities, the government may still have a role, informed by the Secretary’s Advisory Committee on Human Subjects Research and other specialized committees, in educating IRB members on requirements, ethical standards, and regulations for research for scientifically complex populations, such as pregnant women. Clear and standardized definitions of minimal risk interventions for the mother and infant would ensure that all IRBs have access to shared guidance to decide (1) whether to include pregnant women in clinical trials and (2) the quantity and quality of interventions that could be approved in the protocol to maximize the benefit of such research.
Finally, in addition to the active development of vaccines for pregnant women and the prevention of infections during the newborn period and similar to the 2009 H1N1 influenza pandemic, the current Zika virus outbreak has once again raised awareness of the need for developing and articulating a pregnancy-specific ethical framework that can offer guidance to IRBs and investigators for clinical trials to promote the inclusion of pregnant women. 50 The ongoing necessity for developing vaccines for use during pregnancy highlights the need for manufacturers, researchers, IRBs, providers, and the public to understand that creating a culture of inclusion of pregnant women in clinical research is paramount.
Focus Area 2: Policy Issues
The ASH should continue to support maternal immunization as an important public health strategy to encourage manufacturer investment in the development of new and currently licensed vaccines for additional indications for use specifically in pregnant women.
The ASH should advocate to the Secretary of Health and Human Services to resolve the uncertainties around coverage under the Vaccine Injury Compensation Program (VICP) for vaccines administered to pregnant women that are not recommended for use in children by CDC and for liability protections for live-born infants born to mothers vaccinated during pregnancy.
Maternal immunization as a public health strategy
Despite remarkable strides by the global community to reduce mortality in children <5 years of age, the rate of infant deaths from infectious diseases is unacceptably high. 1,51 Maternal immunizations have emerged as a promising global strategy to protect infants against VPDs. 14,15,29,34,52,53 CDC already routinely recommends the administration of 2 vaccines, seasonal inactivated influenza and Tdap, during pregnancy, 9,20,23,54 although there are currently no vaccines specifically indicated for use in pregnant women by the FDA. The lack of a specific indication for pregnancy for current vaccines, with the fact that there are additional disease targets with substantial morbidity and mortality affecting infants, 35,52,55 motivates prioritizing the need for the development of new and improved vaccines for use by expectant mothers to successfully protect infants during the first months of life. Several immunizations that could be efficacious against infant disease are already being developed and include vaccines against RSV and GBS. The public health community’s support in moving these prototypes through the pipeline is essential to ensure the success of vaccines already in development and to promote the innovation of new vaccines that would address additional needs.
Liability protection
Another substantial hurdle preventing vaccine developers and manufacturers from fully committing to obtaining specific indications for use during pregnancy for new and developed vaccines is the uncertainty about the scope of coverage and liability protection for these vaccines under the VICP (42 USC §300aa-10 to 300aa-15). 56 The VICP was created by the Childhood Vaccine Injury Act of 1986, as amended (Vaccine Act; 42 USC §§300aa-1 to 300aa-34), which also established the National Vaccine Program Office and the Health Resources and Services Administration’s Advisory Commission on Childhood Vaccines, which makes recommendations to the secretary on issues related to the operation and implementation of the VICP. The VICP provides compensation to people (regardless of age) found to have been injured by, or to have died as a result of, the administration of certain covered vaccines. Even in cases in which such a finding is not made, petitioners may receive compensation through a settlement. Compensation may be available for vaccine injuries sustained by adults or children so long as the general category of vaccines is covered by the VICP. For a vaccine to be covered by the VICP, the category of vaccine must be (1) recommended by CDC for routine administration to children (adults immunized with these vaccines may also submit a claim to the VICP) and (2) subject to an excise tax by federal law.
CDC currently recommends 2 immunizations for routine use among pregnant women: seasonal inactivated influenza and Tdap. These vaccines are covered under the VICP because they are also recommended for routine administration to children and are subject to an excise tax. Because these vaccines are covered under the VICP, the manufacturers and administrators of such vaccines generally are afforded the Vaccine Act’s liability protections. 57 Although these 2 vaccines are currently covered under the provisions of the VICP, maternal immunizations in general still have several coverage gaps that endanger the manufacturer’s liability protection. Although influenza and Tdap vaccines are covered under the VICP, new categories of vaccines that would potentially be indicated only for use during pregnancy and not routinely recommended for use in children would not be covered under this program if they were not also recommended for use in children. Therefore, pregnant women receiving such vaccines would not be eligible to pursue claims related to such vaccines under the VICP. For such vaccines to be covered under current law and absent a statutory amendment to cover other categories of vaccines, Congress would need to enact an excise tax for such vaccines, and CDC would need to recommend this category of vaccines for routine administration to children (42 USC §§300aa-1 to 300aa-34).
Immunization recipient
Even regarding vaccines currently covered under the VICP, a more detailed inspection of the Vaccine Act and VICP case law reveals another coverage gap with the potential to threaten liability protection. In the case of vaccines administered during pregnancy, uncertainty remains about whether a claim concerning an injury sustained in utero (after a pregnant woman’s vaccination) can be pursued under the VICP on behalf of the child. The reason for this uncertainty is, in part, that petitioners claiming a vaccine-related injury to the VICP must demonstrate that the person who suffered a vaccine-related injury or death “received a vaccine set forth in the Vaccine Injury Table [a covered vaccine]” (42 USC §300aa-11[c][1][A]). In claims alleging that a child had an injury in utero because of a vaccine administered to the pregnant mother, the question is whether the child received a vaccine under the meaning of the statute. The question of whether a vaccine is received in utero was a central issue in a few VICP cases involving allegations of injuries sustained in utero. 56 However, there is no binding case law resolving the issue, so it remains unsettled.
The “one-petition rule.”
The Vaccine Act also specifies that “only one petition may be filed with respect to each administration of a vaccine” (the “one-petition rule”; 42 USC §300aa-11[b][2]). To the extent that >1 VICP petition is filed with respect to a single vaccine administration, the second petition may be dismissed as barred by the Vaccine Act. In the event that 2 VICP petitions are filed with respect to a vaccine administration to a pregnant woman (ie, 1 petition on behalf of an injured child and a separate petition on behalf of an injured mother), it would appear that the one-petition rule would be violated. However, in this case, there is not a binding case law interpreting the provision either, so the issue is also unresolved.
Also administered by the Health Resources and Services Administration, the Countermeasures Injury Compensation Program compensates for serious injuries and deaths directly caused by the administration or use of covered countermeasures identified by the secretary in declarations issued under the Public Readiness and Emergency Preparedness Act (42 USC §247d-6d). The Public Readiness and Emergency Preparedness Act gives the secretary the authority to promulgate regulations to govern the procedures and requirements of the Countermeasures Injury Compensation Program. The regulation issued pursuant to that authority addresses the issue of injuries sustained by children born to women who were administered or used a covered countermeasure during pregnancy. The Countermeasures Injury Compensation Program’s regulation specifies that a child can qualify as an injured countermeasure recipient for purposes of the program if the child survives birth and is born with, or later sustains, a covered injury as the direct result of the mother’s administration or use of a covered countermeasure during pregnancy (42 CFR 110.3[n][3]; 75 FR 63 660).
Recognizing the effect that certain changes to the VICP could have on such an important public health objective as the protection of infants, 2 of the US Department of Health and Human Services’ advisory committees, the Advisory Commission on Childhood Vaccines and the NVAC, have recommended the coverage of claims submitted to the VICP alleging injuries to the pregnant woman and/or her live-born infant for injuries sustained in utero that result from maternal immunization (which also may result in liability protections for the vaccines’ manufacturers and administrators). This recommendation has also been supported by relevant stakeholders such as the American Association of Pediatrics, the American College of Obstetricians and Gynecologists, members of Congress (including authors of the original legislation that established the VICP), and representatives of the pharmaceutical industry.
Unfortunately, uncertainties regarding maternal immunizations and liability protections under the VICP represent a barrier that discourages manufacturers and vaccine developers from (1) investing in developing new vaccines for use in pregnancy and (2) pursuing pregnancy-specific indications for vaccines already recommended by CDC to be routinely administered to women during pregnancy. Modifications to the VICP program to resolve these uncertainties should be a priority to incentivize manufacturers to invest in safe and effective vaccinations specifically formulated for use during pregnancy.
Focus Area 3: Preclinical and Clinical Research Issues
The ASH should prioritize increased support for preclinical and early clinical research to understand the immune response during pregnancy and to develop vaccines for pregnant women.
The ASH should work with federal and nonfederal stakeholders to create or promote mechanisms that support investigator-initiated and other types of research that foster innovation and expand the field of vaccines for pregnant women.
The ASH should emphasize the need for a better understanding of the public health burden of diseases preventable by maternal immunization.
The ASH should work with all relevant federal agencies and nonfederal stakeholders to support evaluation of the maternal and neonatal outcomes of vaccines administered during pregnancy with respect to (1) the safety of vaccines and (2) the effectiveness of vaccines to reduce maternal and infant morbidity and mortality caused by VPDs and (3) to better understand the potential risks and benefits of maternal immunization.
The ASH should support continuing evaluation of vaccines in pregnant women and infants born to vaccinated mothers while advocating for the adoption of standardized approaches to data collection, analysis, and safety evaluation.
The ASH should support the adoption and utilization of standardized definitions of possible maternal and neonatal outcomes to evaluate the safety and effectiveness of vaccines administered during pregnancy.
The ASH should convene stakeholders and other federal agencies to work on the expansion of pharmacovigilance systems that readily link maternal and infant electronic health records and safety surveillance systems.
Preclinical and Clinical Research Barriers to Advancing Vaccine Development for Pregnant Women
Despite the scientific advances in understanding vaccines and human immune response to vaccines, the knowledge on maternal-fetal physiology and immunology, especially the immunologic role of the placenta and the potential effects that maternal immunizations can have on the fetus, is limited and poorly understood. A better understanding of the following topics is still needed to fully understand the benefits and risks of maternal immunizations: immunologic responses in women during pregnancy; antibody transfer from mother to fetus (transplacental transfer); antibody kinetics (the rate at which maternal antibodies are transferred to the fetus and the half-life of maternal antibodies, especially after transfer to the fetus); the optimal period for greater maternal immunization in relation to the period of disease and infectivity risk; the rate of antibody waning in the infant and its correlation with protection against infection or other outcomes of disease and whether maternal antibodies persist during infancy; the potential effect of maternal antibodies on the infant’s responses to primary immunization; and the role of breast milk antibodies. 34 The knowledge gap in maternal immunization immunology is partially caused by the lack of available funding mechanisms to address these questions. Expanding federal funding to allow for investigator-initiated or exploratory research is a way to increase the studies that would address some of the aforementioned areas. Alternative pathways of funding would also promote research flexibility to explore the unknowns about the biology and immunology of maternal immunization and advance the field of maternal immunization.
Additional information on the safety and effectiveness of vaccines recommended for use during pregnancy could also improve implementation of maternal immunization recommendations and, consequently, vaccination rates. The currently recommended maternal vaccines—influenza and Tdap—are not specifically indicated by FDA for use in pregnant women, because prelicensure trials did not include testing the safety and efficacy of these vaccines in the population of pregnant women. The limited data available on pregnant women are usually obtained from nonrandomized or observational clinical trials, which often exclude pregnant women. 34 Observational or retrospective studies present a problem because they are not designed to understand aspects of vaccine physiology, such as the effects and benefits of vaccines when administered early in pregnancy (ie, during the first and second trimesters).
Because of this lack of prelicensure testing by the vaccine sponsor and the potential public health importance of maternal immunization against influenza and pertussis, the Advisory Committee on Immunization Practices and CDC gathered additional research data to support the wisdom of immunization recommendations for pregnant women, although the vaccine sponsor had not sought a specific indication for use in pregnancy. 9,20,23,54 However, the inconsistency between federal recommendations and specific indications leads obstetric providers to be unsure about making strong recommendations for maternal vaccinations, because the understanding of the immunogenicity and safety of vaccine delivery during pregnancy is limited. 50 Finally, the exclusion of pregnant women from prelicensure clinical trials has also influenced the availability of safety information, because vaccine safety data on maternal immunizations have been obtained primarily from retrospective population-based cohort studies and database reviews, which are not ideal study designs to determine the safety of a vaccine before or after licensure. 34
Understanding disease burden to better inform maternal immunization programs
A more thorough understanding of the VPD burden among infants in the first 6 months of life would also help to accurately determine the effectiveness of maternal immunizations on both the infant and the mother and could help justify the importance of this intervention to policy makers and the general public as they prioritize health resources. Systems capable of tracking epidemiologic data and disease burden for poorly surveyed diseases in the United States and globally would enhance evidence-based decision making for the recommendation and administration of vaccines during pregnancy and support increased funding for research into maternal vaccine development.
Two national efforts are already implementing some of the additional features needed to estimate disease burden. The CDC-managed National Notifiable Diseases Surveillance System incorporated the new Modernization Initiative, which has the main goal of “modernizing the systems and processes used to receive nationally notifiable disease data to provide more comprehensive, timely, and higher quality data than ever before for public health decision making.” 58 The Modernization Initiative is an effort to strengthen and modernize the infrastructure supporting CDC’s system for notifiable diseases as part of its existing surveillance system and to improve the system to allow for more comprehensive, timely, and higher-quality data for public health decisions. 59 The US Department of Defense uses the Global Emerging Infections Surveillance and Response System, which focuses on surveying emerging infectious diseases that could affect the US military, 60 often used to make informed public health decisions. 61 Systems already in place could be used as infrastructure to collect data on the burden of disease by including and focusing on specific populations, such as pregnant women and infants, which are needed to better assess the justification and need for vaccine development. 62 –64
Enhancing safety surveillance for maternal immunizations
Vaccine safety surveillance and research on pregnant women and their infants present unique challenges compared with immunization safety research conducted in other populations. Well-established postmarketing vaccine adverse events reporting and surveillance systems allow for the study of vaccines currently in use and for research on diverse safety outcomes, even in the absence of reports of a specific adverse event. Implementing new or adapting existing surveillance systems can facilitate maternal immunization research studies to improve the understanding of vaccine safety and immunogenicity in pregnant women and their infants and can help identify rare outcomes potentially associated with vaccine administration, such as some types of congenital anomalies.
In the United States, the increased availability of nationwide electronic health records and interconnected state-based immunization information systems are potentially underused yet invaluable resources to study the effects of vaccination on pregnant women and follow their infants. Two pharmacovigilance systems use electronic health records to assess the safety of immunizations: the CDC-managed Vaccine Safety Datalink 65 –67 and the FDA-managed PRISM system (Post-licensure Rapid Immunization Safety Monitoring). 68,69 These safety systems systematically analyze and link immunization registry and electronic health outcome data from several large integrated health plans to conduct near-real-time vaccine safety surveillance for prespecified outcomes and targeted studies using automated data. Any potential safety signals identified from these automated studies can be further refined by accessing individual electronic health records to validate cases.
Adapting VSD and PRISM to survey and assess safety outcomes of maternal immunizations is challenging because it requires the modification of analytic algorithms to directly link maternal and infant clinical records. These existing surveillance systems use such prototype algorithms that could be modified, expanded, and improved to allow for additional capabilities in areas such as direct linking of maternal and infant records and to enhance studies of rare birth outcomes (ie, some types of congenital anomalies).
Standardization of data collection, analysis, safety evaluation, and outcomes definitions
To maximize the benefits of maternal immunization studies, it is important to recognize that clinical trials need to be conducted in a systematic manner to fully benefit from the results obtained. Several considerations make research including pregnant women uniquely challenging: IRBs lack proper guidance when approving protocols for research during pregnancy; pregnant women are notoriously harder to recruit for clinical trials than the general population; some clinical end points might be rare or difficult to define; and risks for safety outcomes that are usually found with extremely low prevalence in other populations are hard to estimate given the background rate of common pregnancy complications. 50 These considerations emphasize the need for standardized data collection, analysis, and safety surveillance in the United States and globally to correlate results and disseminate findings that are reproduced in multiple settings.
One of the critical aspects of reproducible data collection for surveying of maternal and infant safety outcomes is the standardization of vaccine safety terminology and common case definitions, which may have surprisingly varied interpretations among obstetric and pediatric practitioners. Standardizing vaccine obstetric, fetal, and neonatal safety terminology and case definitions would enable the United States and other countries to combine clinical study results when investigating vaccines during pregnancy and to obtain risk determinations even for very rare maternal and infant birth outcomes. The Brighton Collaboration—a nonprofit, primarily volunteer-based, and scientifically independent global research network—is a leader in this effort, with the mission of advancing the science of immunization safety and defining globally acceptable common terminology for adverse events after immunization. 70 –72 Along with the Brighton Collaboration, the World Health Organization shares the objectives of (1) raising awareness of the availability of standardized case definitions and guidelines for data collection, analysis, and presentation for global use and (2) developing and implementing standard study protocols to evaluate case definitions. 73 In collaboration, they provide independent, high-level, technical, and strategic advice on developing an interim set of key terms and concept definitions to assess the safety of vaccines administered during pregnancy in the mother and the infant, which can be used to improve vaccine safety monitoring and evaluation.
Standardizing definitions that can be implemented globally is a complex process that requires thoroughness. The process involves recruiting international working groups that conduct systematic literature reviews to develop the case definitions, having the definitions revised by a reference group, and then finalizing the definitions to be distributed for global use. 74 Examples of standardized safety outcomes definitions include “stillbirth” and “congenital abnormalities,” among others, which were recently released to aid collaborative immunization safety research studies. 75 –77 These efforts will ensure that the vaccine safety field is on the right path toward effective and reproducible surveillance of the safety of immunizations administered during pregnancy.
Focus Area 4: Provider Education and Support Issues
The ASH should encourage professional societies to continue to support the inclusion of pregnant women in clinical research.
The ASH should work with relevant stakeholders to increase awareness among obstetric providers and pregnant women about the importance of vaccine research during pregnancy.
The ASH should work with professional societies to educate obstetricians and other obstetric providers on vaccination and interpretation of new regulations regarding labeling (ie, the Pregnancy and Lactation Labeling Rule) so that they can make informed decisions and counsel their patients more effectively.
Support from professional societies
Maternal immunizations are an investment in better health outcomes for pregnant women and their infants. 34 Professional societies and maternal immunization stakeholders have a critical role in educating providers about the benefits of involving pregnant women in clinical trials. Their community engagement efforts are essential to support a shift toward including pregnant women in clinical trials so that the mother and infant can benefit from safe and effective vaccines that have been appropriately tested during the prelicensure phase. These efforts will ensure that pregnant women have access to the same standard of care that other members of society have been afforded.
Even when the policy, regulatory, and ethical barriers to licensing safe and effective immunizations for use in pregnancy are addressed, recruitment and participation of pregnant women in clinical trials are the cornerstones for developing any vaccine with a specific indication for use during pregnancy. However, pregnant women may be reluctant to enroll in clinical trials because of a general lack of awareness about research in their community, which could lead them to express unease and distrust of the research. 78 Pregnant women’s hesitancy to participate could be assuaged by consulting with obstetric providers, who are the most trusted advisors for a pregnant patient and are uniquely positioned to advocate for increased participation of pregnant women in clinical research. 79,80 It is at this time when the work of professional societies and other relevant stakeholders to influence health care professionals becomes invaluable, because the former have the ability to conduct outreach efforts to community providers, educate them, and encourage them to promote research studies to their patients. In many cases, a clinician’s promotion of clinical trials could increase a pregnant woman’s willingness to participate in them. 81 Increases in maternal immunization rates for influenza and Tdap have recently occurred following similar educational support efforts by federal agencies and professional societies, as detailed previously.
The Pregnancy and Lactation Labeling Rule
Professional societies that advocate for the safe use of medications and vaccines during pregnancy should facilitate clinicians’ transition into understanding new and unique immunization product information. For example, professional societies should help clinicians understand FDA’s new Pregnancy and Lactation Labeling Rule (21 CFR 201.57 and 201.80; 79 FR 72 064). A critical step in FDA’s review process of a Biologics License Application includes evaluation of the product package insert. 82 Until recently, FDA required biologics’ labels (for biologics, including vaccines) to contain a letter code summarizing the determination of a risk category in the biologics’ letter coding (A, B, C, D, or X) for use during pregnancy. A determination in the letter coding was required for any biologic, including vaccines, without a specific indication for use during pregnancy (sometimes erroneously referred to as “off-label” use) and was intended to provide the practitioner with a classification of the product according to the level of risk for pregnant women and infants, depending on the data available to the sponsor at the time of licensing. However, this system was difficult to interpret in practice and cumbersome to convey to the patient when explaining the risk-benefit balance of administering a medication during pregnancy.
In response to these challenges, FDA recently amended the letter category rules with the Pregnancy and Lactation Labeling Rule (21 CFR 201.57 and 201.80; 79 FR 72 064). The rule eliminates the old classification system and provides a new framework that more clearly describes the available data on potential risks associated with the use of drugs and biologics during pregnancy and lactation. This change not only provides a consistent format for communicating risk and benefit information of a vaccine relevant to pregnant and lactating women but also enables the incorporation of exposure information from various sources, including non–industry-sponsored epidemiologic and intervention studies. 50 As with any new regulation, implementation of the rule will be challenging. Obstetric and other health care providers who are unfamiliar with the new classification system will require guidance on how to best interpret the new package inserts. A clear understanding by clinicians and patients of the labeling of vaccines administered during pregnancy will also promote confidence in the safety and efficacy of these products, which may lead to more active participation of this population in clinical trials during pregnancy.
Conclusion
Maternal immunization has been implemented as a successful national and global strategy to protect infants against VPDs such as influenza, pertussis, and tetanus. Although CDC already recommends the use of vaccines during pregnancy, certain ethical, policy, educational, and research barriers need to be addressed to improve uptake of currently recommended vaccines and promote the development of additional maternal immunizations. This NVAC report describes the barriers and opportunities for developing vaccines for pregnant women and makes recommendations to overcome these barriers, and the NVAC submits these recommendations to the ASH for her consideration.
Footnotes
Authors’ Notes
The views represented in this report are those of the National Vaccine Advisory Committee. The positions expressed and recommendations made in this report do not necessarily represent those of the US Department of Health and Human Services, the US government, or the individual working group members who served as authors of, or otherwise contributed to, this report. This document is published as voted upon and submitted by the National Vaccine Advisory Committee.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.