
Abstract
Objectives:
Previous state interagency collaborations have led to successful tobacco cessation initiatives. The objective of this study was to assess the roles and interaction of state Medicaid and public health agency efforts to support tobacco cessation for low-income Medicaid beneficiaries.
Methods:
We interviewed Medicaid and state public health agency officials in 8 states in September and October 2015 about collaborations in policy development and implementation for Medicaid tobacco cessation, including Medicaid coverage policies, quitlines, and monitoring.
Results:
Collaboration between Medicaid and public health agencies was limited. Smoking cessation quitlines were the most common area of collaboration cited. Public health officials were typically not involved in developing Medicaid coverage policies. States covered a range of US Food and Drug Administration–approved tobacco cessation medications, but 7 of the 8 states imposed limitations, such as charging copayments or requiring previous authorization. States generally lacked data to monitor implementation of tobacco cessation efforts and had little ability to determine the effectiveness of their policies.
Conclusions:
To strengthen efforts to reduce smoking and tobacco-related health burdens and to monitor the effectiveness of policies and programs, Medicaid and public health agencies should prioritize tobacco cessation and develop and analyze data about smoking and cessation efforts among Medicaid beneficiaries. Recent multistate initiatives from the Centers for Disease Control and Prevention and the Centers for Medicare & Medicaid Services seek to promote stronger collaborations in clinical prevention activities, including tobacco cessation.
Smoking, the leading cause of preventable morbidity and mortality in the United States, poses a particularly serious hazard for those enrolled in Medicaid, the nation’s largest health insurance program. 1 Data from the 2015 National Health Interview Survey revealed that 27.8% of adults on Medicaid smoked, compared with 11.1% of those who were privately insured. 2 The United States has made strides in reducing the overall rate of smoking, but low-income people remain at elevated risk. 1 Medicaid insurance benefits can pay for cessation services, including cessation medications and counseling, that could help millions of low-income people in their efforts to quit.
Under the Triple Aim, the overarching health policy goals are to promote population health, improve patient care, and contain cost growth. 3 Policies to help smokers quit are ideally suited to integrate mutual goals of health care and public health policy. Federal health policies, including Healthy People 2020 and the US Department of Health and Human Services’ strategic action plan on tobacco use, include goals to enhance tobacco cessation for Medicaid beneficiaries. 4,5 The Centers for Disease Control and Prevention (CDC) declared reducing tobacco use a priority “winnable battle,” that is, an attainable health goal. 6 The Affordable Care Act requires all state Medicaid programs to offer tobacco cessation services without cost sharing to those eligible under Medicaid expansions, to cover tobacco cessation medications for all Medicaid enrollees, and to offer comprehensive cessation coverage for pregnant women. 7,8
Tobacco cessation by Medicaid beneficiaries can be effectively promoted when Medicaid and public health agencies work together. For example, a Medicaid tobacco cessation project launched in 2006 in Massachusetts enhanced cessation efforts and saved $3 for every $1 invested because of a relatively rapid reduction in hospitalizations for cardiovascular problems. 9 A Wisconsin educational campaign during 2005-2007 substantially increased medication use by those on Medicaid. 10 Examples of other successful state initiatives and collaborations exist. 11 However, recent analyses found that the use of tobacco cessation medications in Medicaid is generally low and varies widely across states, suggesting the need for greater promotion of smoking cessation. 12
In this study, we assessed quantitatively the extent to which Medicaid and public health agencies have collaborated to help Medicaid beneficiaries quit or curtail smoking. We conducted comparative case study interviews in 8 states to understand (1) collaborations between state Medicaid and public health agencies, including tobacco cessation quitlines, (2) the development of Medicaid coverage policies, and (3) efforts to monitor the effectiveness of tobacco cessation efforts in Medicaid.
Methods
We selected a convenience sample of 8 states to reflect diversity in smoking prevalence (ie, the percentage of low-income people who smoked in each state) and tobacco cessation use (ie, the percentage of Medicaid beneficiaries receiving tobacco cessation medications), geographic region, and state policies on Medicaid expansion (Table 1). Respondents were program staff members in Medicaid and public health agencies.
Characteristics of 8 states interviewed in 2015 about collaboration between Medicaid and public health agencies in policy development and implementation for Medicaid tobacco cessation
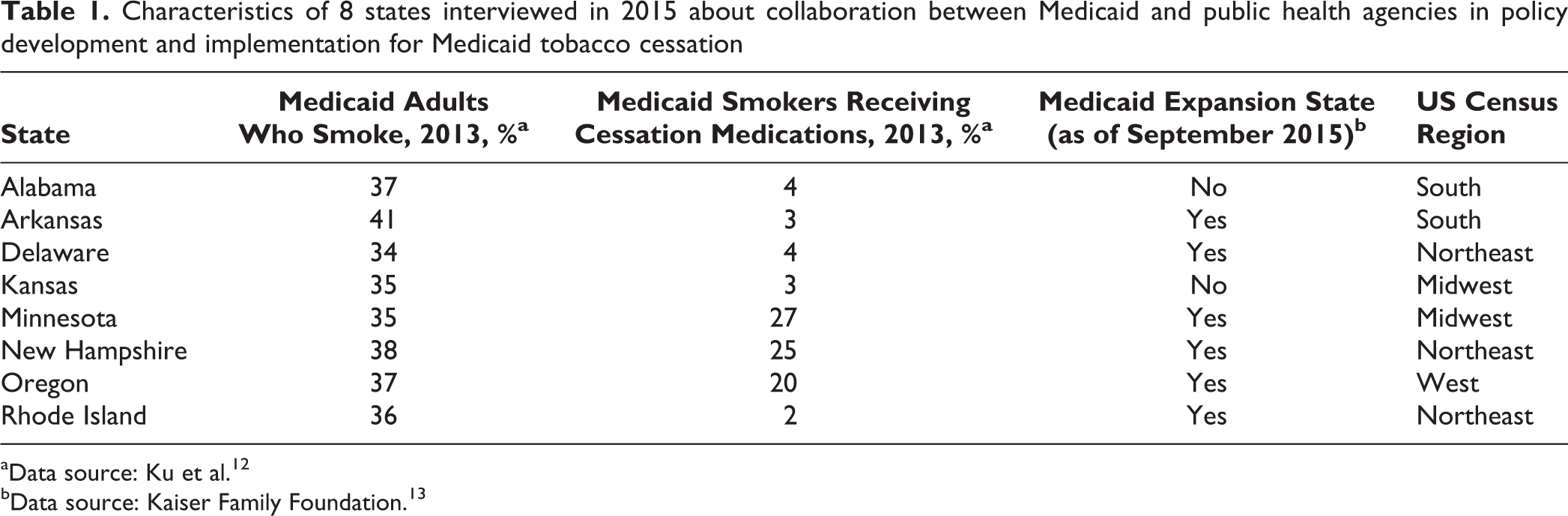
aData source: Ku et al. 12
bData source: Kaiser Family Foundation. 13
We initially selected 10 states, but 2 (Missouri and Tennessee) were unable to participate, leaving 8: Alabama, Arkansas, Delaware, Kansas, Minnesota, New Hampshire, Oregon, and Rhode Island. We identified potential contacts by first approaching public health staff members associated with the Tobacco Control Network, composed of state tobacco control program managers in public health agencies (tobaccocontrolnetwork.org). Medicaid agencies do not typically designate tobacco control staff members, so we identified Medicaid contacts by asking Tobacco Control Network officials about their Medicaid counterparts or by asking Medicaid agencies for referrals to officials involved in tobacco cessation. Respondents were generally staff members or midlevel managers who were responsible for program policies or operations. We conducted interviews with 27 Medicaid and public health respondents in 15 interviews from September to October 2015, and we contacted respondents in those 8 states again in March and April 2016 to confirm key details. We interviewed Medicaid staff members and public health department staff members separately, except for 1 joint interview for Kansas and only public health department staff members for Alabama, because Medicaid staff members were not available for interview.
We sent a factsheet describing the project and informed assent terms, along with a semistructured interview guide to respondents. The factsheet, which was customized for each state, summarized state-specific data about the prevalence of smoking among Medicaid adults (as measured by the percentage of low-income insured adults who smoked in the Behavioral Risk Factor Surveillance System), the percentage of Medicaid smokers who received tobacco cessation medications from 2010 to 2013 (as measured by Medicaid drug use data), 13 and Medicaid tobacco cessation coverage policies, such as the types of US Food and Drug Administration (FDA)–approved medications covered and requirements for copayments or prior authorization. 14 We asked respondents to confirm or amend information about Medicaid coverage policies.
We conducted interviews in teams of 2 or 3, and each interview lasted 30 to 60 minutes. After completing the interviews, 2 of the interviewers compiled notes and reviewed recordings, following themes in the interview guide. All 4 interviewers met and used a consensus process to articulate key themes. The George Washington University Institutional Review Board approved the project, and respondents gave informed assent for recorded interviews.
Results
Interagency Collaboration
Most states reported limited collaboration between state Medicaid and health department staff members about smoking cessation. Alabama reported that 1 public health staff member served as the general agency liaison to Medicaid and helped to coordinate activities, including tobacco policy. In Delaware, although a memorandum of understanding was being developed, no active collaboration had occurred by the time of the interview. Kansas had a tobacco cessation stakeholder group, but the group had not met very often. In Minnesota, Clearway Minnesota, a nonprofit organization that administered tobacco control programs and worked with both the Medicaid and public health agencies, participated in the interview.
Some respondents felt that greater collaboration would be beneficial but that barriers such as functional separation of agencies and missions, a sense that tobacco issues were a low priority to agency leadership, and staff turnover were impediments. In some cases, public health or Medicaid staff members reported a lack of regular contact between the 2 agencies. In many cases, agency officials did not know counterparts in the other agency, making collaboration impossible.
Many respondents reported that organizations such as the American Lung Association or American Cancer Society were tobacco control advocates, but policy champions at higher government levels to encourage interagency collaboration and establish priorities were scarce. One state Medicaid official noted, “We have a drug czar in the governor’s office. If we had a smoking czar, that would be great, but we don’t. We are a small state, so we wear many hats.” Although public health agencies have tobacco control units and staff members, Medicaid agencies do not usually have staff members dedicated to that area.
Medicaid Tobacco Cessation Policies
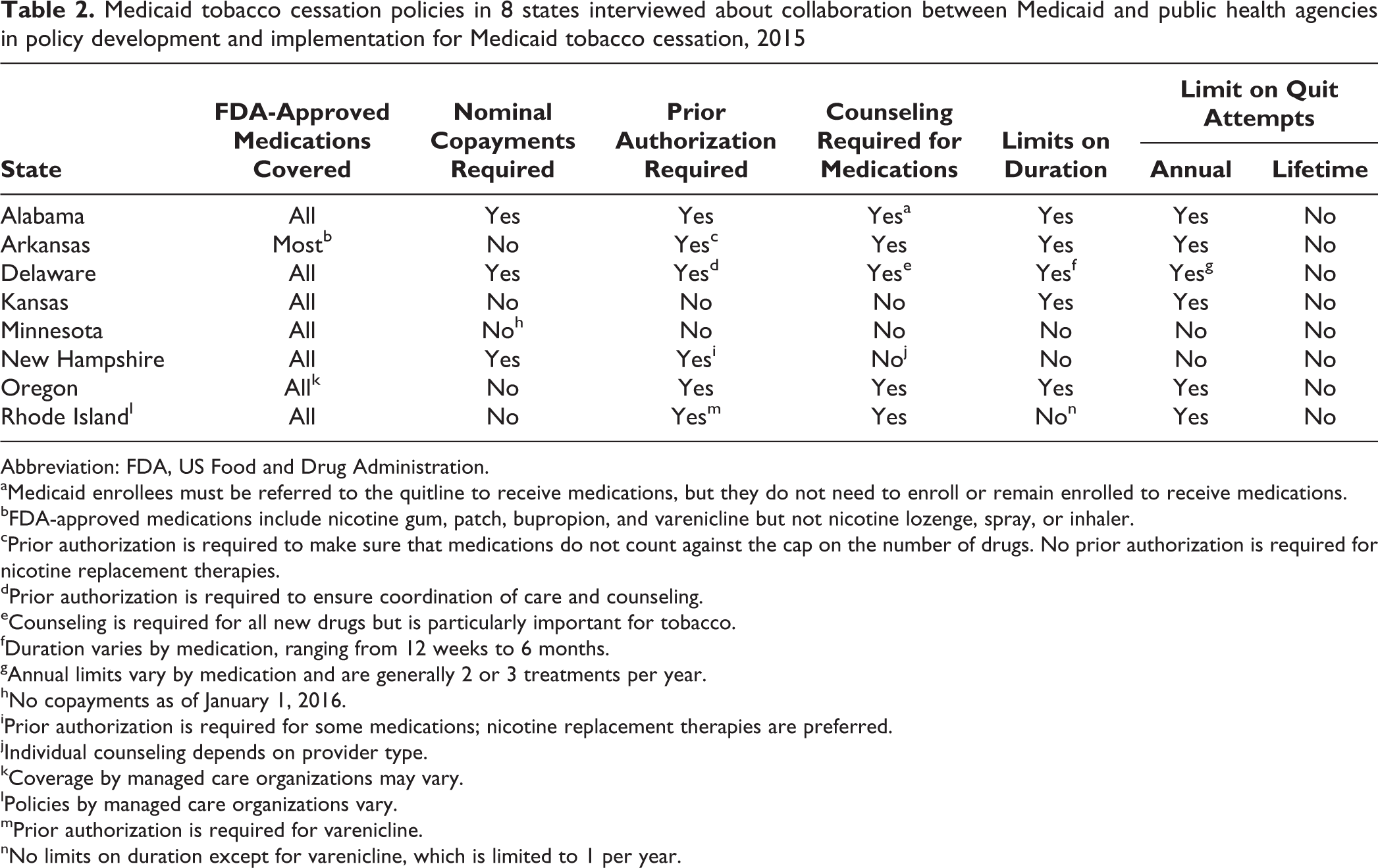
All 8 states covered most FDA-approved medications, including nicotine replacement therapies (NRTs), bupropion, and varenicline, although states varied in some details (Table 2). Although the Affordable Care Act requires Medicaid coverage of FDA-approved medications, some states or managed care plans used methods such as preferred drug lists that effectively limit the range of medications available. Although NRTs are typically sold over the counter, Medicaid may also pay for them with a prescription. However, because private insurance and Medicare generally do not pay for over-the-counter medications, Medicaid coverage may be confusing to physicians, pharmacists, and beneficiaries. Minnesota had a state law allowing pharmacists to write NRT prescriptions to ease access to NRT prescriptions for Medicaid reimbursement.
Medicaid tobacco cessation policies in 8 states interviewed about collaboration between Medicaid and public health agencies in policy development and implementation for Medicaid tobacco cessation, 2015
Abbreviation: FDA, US Food and Drug Administration.
aMedicaid enrollees must be referred to the quitline to receive medications, but they do not need to enroll or remain enrolled to receive medications.
bFDA-approved medications include nicotine gum, patch, bupropion, and varenicline but not nicotine lozenge, spray, or inhaler.
cPrior authorization is required to make sure that medications do not count against the cap on the number of drugs. No prior authorization is required for nicotine replacement therapies.
dPrior authorization is required to ensure coordination of care and counseling.
eCounseling is required for all new drugs but is particularly important for tobacco.
fDuration varies by medication, ranging from 12 weeks to 6 months.
gAnnual limits vary by medication and are generally 2 or 3 treatments per year.
hNo copayments as of January 1, 2016.
iPrior authorization is required for some medications; nicotine replacement therapies are preferred.
jIndividual counseling depends on provider type.
kCoverage by managed care organizations may vary.
lPolicies by managed care organizations vary.
mPrior authorization is required for varenicline.
nNo limits on duration except for varenicline, which is limited to 1 per year.
All but 1 state (Minnesota) had restrictions on access to cessation therapies, such as copayments, prior authorization, required linkage to counseling, or limits on the duration of benefits. Minnesota eliminated cost sharing for tobacco cessation as of January 2016 and had no other limitations before that time. Federal Medicaid policy allows states to charge nominal copayments for medications, except for children, pregnant women, and a few other subgroups. Five states did not charge copayments for cessation medications.
Prior authorization requires advance permission from the Medicaid agency or a pharmaceutical benefits manager for benefits, such as drugs that are not on a preferred drug list. Only 2 states (Kansas and Minnesota) did not require prior authorization for tobacco cessation; New Hampshire required it for higher-cost tobacco cessation medications, such as varenicline. Alabama used prior authorization to avoid counting these medications against an overall monthly cap on the number of authorized prescriptions per month. Delaware required that medications be prescribed only in conjunction with counseling; it also used step therapy (a variation of prior authorization) to shift the preference to lower-cost therapies, such as NRTs. In Rhode Island, the use of step therapy varied by managed care plan.
States may limit the duration of cessation medications, whether for a given quit attempt, a year, or a lifetime. Manufacturers typically recommend treatment for 8 to 12 weeks and a transition to a full quit. Minnesota and New Hampshire had no limits, and Rhode Island had a limited duration for varenicline but not for other medications.
Medicaid officials reported that public health staff members generally were not involved in decisions about Medicaid benefit policies. Medicaid decisions were often linked to broader state policies for prescription drugs (eg, copayments, authorization for generic vs brand name drugs), and managed care organizations had discretion in policies for their members.
Monitoring Smoking and Cessation in Medicaid
Neither Medicaid nor public health staff members in the 8 states routinely monitored data about the level of smoking by Medicaid beneficiaries or the use of tobacco cessation. They had not seen state-specific utilization data such as those we shared. The state agencies did not appear to be analyzing data about the effectiveness of their policies.
Medicaid claims and encounter data systems can monitor utilization, but the states interviewed were not mining those data. One Medicaid official indicated realizing that the state had utilization data but said that analysis resources were unavailable.
Quitlines
An area in which Medicaid and public health agencies often reported interaction was smoking quitlines. In 7 states, the health agency administered quitlines; a nonprofit organization administered 1 in Minnesota. All states had quitlines offering a toll-free number for counseling for state residents. Public health and Medicaid agencies reported that clinicians and Medicaid managed care plans may be encouraged to refer smokers to quitlines. Public health agencies also operated other educational programs to promote smoking prevention and cessation. States indicated that Medicaid beneficiaries were major users of quitline services. Of the 8 states interviewed, Medicaid beneficiaries constituted 17% to 40% of quitline users (Table 3).
Medicaid and smoking quitlines in 8 states in a study of collaboration between Medicaid and public health agencies in policy development and implementation for Medicaid tobacco cessation, 2015
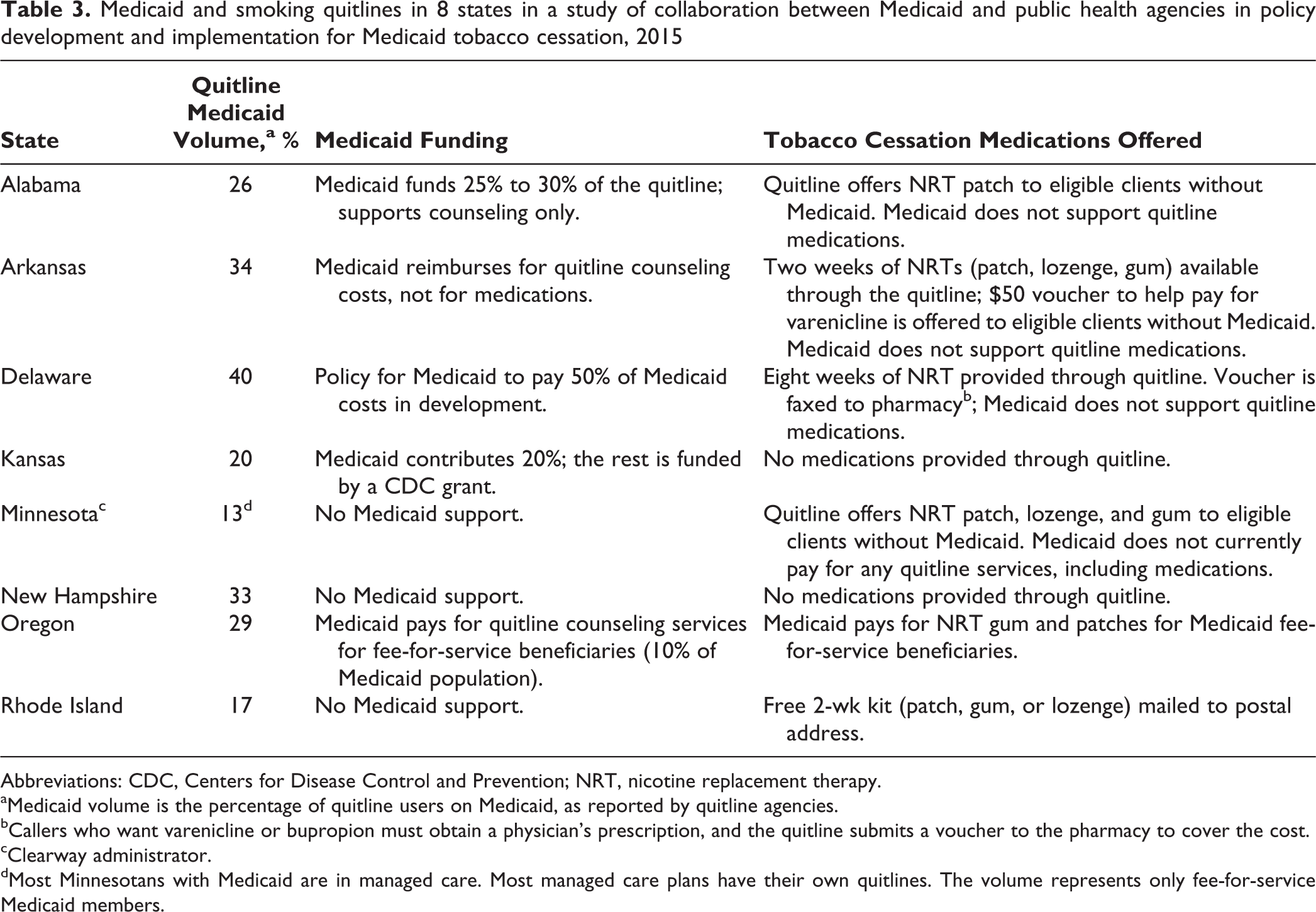
Abbreviations: CDC, Centers for Disease Control and Prevention; NRT, nicotine replacement therapy.
aMedicaid volume is the percentage of quitline users on Medicaid, as reported by quitline agencies.
bCallers who want varenicline or bupropion must obtain a physician’s prescription, and the quitline submits a voucher to the pharmacy to cover the cost.
cClearway administrator.
dMost Minnesotans with Medicaid are in managed care. Most managed care plans have their own quitlines. The volume represents only fee-for-service Medicaid members.
State Medicaid programs may help health agencies by supporting funding for quitlines and other cessation services. Four states in our study received Medicaid quitline funding, and a fifth state was in the process of developing a policy about quitline funding.
Quitlines often provide free or discounted tobacco cessation medications, such as NRT patches or gum. They primarily provide NRTs, which are relatively inexpensive and can be available over the counter. Of our 8 study states, 1 state (Oregon) indicated receiving Medicaid funding to help cover the cost of medications provided through quitlines.
Responses from Minnesota provided an interesting example about differences in agencies’ interpretation of Medicaid coverage and funding. Initially, the Medicaid agency said that it covered quitline medications, but the quitline disagreed. After we probed, Medicaid staff members explained that they had a policy to cover medications from a Medicaid-approved pharmacy and had paid for medications from a prior quitline contractor, but funding stopped when a new contractor was selected that lacked a Medicaid-approved pharmacy. As an insurance agency, Medicaid interpreted coverage as meaning that it had policies that could be used to pay for services under approved circumstances, whereas the quitline agency viewed the issue from the perspective of receiving funding.
Discussion
Reducing tobacco use among Medicaid beneficiaries is an area of mutual importance for Medicaid and public health agencies; however, institutional barriers and inertia have created challenges in establishing collaborations to bolster smoking cessation. The challenges and potential rewards of interagency collaboration are common issues in public policy and health policy. 15 Differing priorities, hierarchies, and even personalities can create barriers. Both types of agencies often had their own separate priorities (eg, Medicaid expansions, managed care initiatives, opioid or other emergencies) that preempted attention at higher levels from longer-term health problems, such as smoking. Some keys to success include having shared goals, including the appropriate parties from agencies, and having credible champions with the ability to make collaboration a priority. 16
An area of interagency discussion was funding for quitlines. Research has demonstrated quitlines’ effectiveness in smoking cessation. 17,18 Quitlines are often funded by CDC or Tobacco Master Settlement Agreement lawsuit funds. 19 Although Medicaid funds can be used for quitline services and Medicaid beneficiaries are major users of quitline services, fewer than half of state quitlines nationwide receive Medicaid support, which is permitted under federal rules. 20,21 Given the limited funding available from other sources, Medicaid support could be a cost-effective way to enhance services.
Broader collaboration to support Medicaid tobacco cessation, such as the development of new campaigns or initiatives, was absent in these 8 states.
The North American Quitline Consortium’s 2015 state survey reported that 38% of quitline users nationwide were on Medicaid. 19 According to the consortium, 16 quitline programs received federal Medicaid matching funds in 2015, and another 10 quitline programs planned to seek funding. 20 Although about one-third of states received federal matching funds for quitlines, state-level Medicaid funds were rarely shared; only 4 states did so. Of the 4 states in which Medicaid and the health agency were in the same department, Medicaid helped fund the quitline only in Kansas, whereas Delaware was in the process of developing a policy. Of the 4 states in which Medicaid and health agencies were in separate departments, Arkansas, Kansas, and Oregon had Medicaid funding for quitlines, and Minnesota had policies that permitted funding of quitline medications. Being in the same department did not necessarily promote collaboration.
A recent nationwide study found that broader coverage of cessation medications leads to higher utilization by Medicaid enrollees. 22 Medicaid coverage policies were established despite relatively little contact with health agencies, and public health agencies generally did not focus on Medicaid. For most prescription drugs, state Medicaid programs asked beneficiaries to make nominal copayments, 23 so the fact that so many states eliminated copayments for these medications indicates that policies for tobacco cessation medications were less restrictive than for other medications. Affordable Care Act policies about cost sharing for preventive services could have contributed to these changes.
Interviews with these 8 states indicated that they were doing little to track utilization of tobacco cessation benefits in Medicaid, making it difficult to know how successful they were or whether policy or program changes led to improvements. Many states required that Medicaid managed care organizations collect Consumer Assessment of Health Plans data about how many smokers were advised to quit by their physicians and had discussed cessation medications or strategies with their physicians, but respondents did not appear to be aware of these data. 24 Public health agencies often collected survey data about smoking behaviors but did not always include Medicaid coverage in their data collection.
Of the 8 states interviewed, 5 (Alabama, Arkansas, Delaware, Kansas, and Rhode Island) had relatively low utilization of tobacco cessation medications: only 2% to 4% of Medicaid smokers received medications in 2013. However, 3 states (Minnesota, New Hampshire, and Oregon) had moderate utilization of cessation mediations, ranging from 20% to 27%. All states offered most or all tobacco cessation medications. Minnesota, the state with the highest tobacco cessation utilization rate, had the fewest limitations, and agencies had some collaboration on policies and quitlines. Two other states, New Hampshire and Oregon, restricted medication access through copayments or policies (eg, prior authorization).
Collaborative efforts may be increasing. Increased emphasis on the importance of quality and population health improvement, as under the Triple Aim, 3 can increase health insurers’ efforts to improve and monitor preventive care. Both the Centers for Medicare & Medicaid Services and CDC recently began multistate initiatives that encourage Medicaid and public health agencies to collaborate to increase the use of clinical prevention services. CDC’s 6|18 Initiative seeks to accelerate the use of evidence-based interventions in health insurance programs in 6 areas, including tobacco control. 25 The Centers for Medicare & Medicaid Services developed a Medicaid Prevention Learning Network, including a tobacco cessation affinity group, that promotes working with public health counterparts. 26 These initiatives promote high-level discussions and plans, although it is too early to know the outcomes.
Limitations
This study had several limitations. First, this study was exploratory. A quantitative study that analyzed factors promoting the use of tobacco cessation therapy was published in 2016, but it lacks the nuanced qualitative information that resulted from the present study. 15 Second, although we included multiple states in our sample, our data are not generalizable to other states. Data collected were affected by respondents’ perspectives, and interviews with other respondents might have yielded different views. Finally, circumstances may have changed since the time these data were collected; although interagency collaborations were sparse at that time, they may have grown since, spurred by recent federal initiatives, as described previously.
Conclusions
Ultimately, the public health goal should be to encourage Medicaid patients and their clinicians to engage in behavior change and self-management and to offer proper medical support for medications and counseling to make quitting easier and sustainable. Some practices that could enhance tobacco cessation in Medicaid include broadening coverage to all FDA-approved medication and eliminating barriers such as copayments or requirements to get counseling to receive medications 4,15 ; further support for telephone and digital quitline and counseling systems 27 ; clearer guidance for physicians, pharmacists, and patients on cessation benefits; educational campaigns encouraging clinicians to use the 5 A’s (ask, advise, assess, assist, and arrange) 28 ; electronic health records that prompt clinicians in smoking cessation 29 ; and financial incentives for patients and/or physicians. 30 State agencies and managed care organizations should consider whether such strategies are appropriate.
The fundamental changes required are to (1) make smoking cessation a priority for Medicaid and public health agencies, (2) collaborate to identify innovative approaches and promote promising and best practices, such as those described previously, and (3) collect and analyze data to monitor progress. The critical starting place is to make tobacco cessation a mutual priority. Based on our discussion, our impression is that tobacco control has been a priority for public health officials at federal and state levels but less of a priority in Medicaid. The advent of health care quality initiatives that encompass population health have prompted attention to the development of performance objectives to track these objectives. The Centers for Medicare & Medicaid Services and CDC can highlight these issues to strengthen efforts. Combining the expertise of Medicaid and public health agencies could lead to more successful outcomes than either agency could attain on its own.
Footnotes
Acknowledgments
We gratefully acknowledge advice from Erin Brantley, MPH, of George Washington University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Cancer Institute (grant 1R15CA176600-01A1).