
Abstract
Objectives:
Although many service members successfully cope with exposure to stress and traumatic experiences, others have symptoms of depression, posttraumatic stress disorder (PTSD), and anxiety; contextual factors may account for the variability in outcomes from these experiences. This work sought to understand mechanisms through which social support influences the mental health of service members and whether dyadic functioning mediates this relationship.
Methods:
We collected cross-sectional data as part of a larger study conducted in 2013; 321 military personnel who had at least 1 deployment were included in these analyses. Surveys were completed online; we collected data on demographic characteristics, social support, mental health measures (depression, PTSD, and anxiety), and dyadic functioning. We performed process modeling through mediation analysis.
Results:
The direct effects of social support on the mental health of military personnel were limited; however, across all types of support networks, greater social support was significantly associated with better dyadic functioning. Dyadic functioning mediated the relationships between social support and depression/PTSD only when social support came from nonmilitary friends or family; dyadic functioning mediated social support and anxiety only when support came from family. We found no indirect effects of support from military peers or military leaders.
Conclusion:
Findings here highlight the need to continue to explore ways in which social support, particularly from family and nonmilitary-connected peers, can bolster healthy intimate partner relationships and, in turn, improve the well-being of military service members who are deployed.
Although some research focuses on the quality of resilience among combat-deployed military personnel, 1,2 most of it focuses on the prevalence of mental health difficulties caused by stressors among service members and their families. Personnel returning from Iraq and Afghanistan combat operations report high rates of depression, generalized anxiety, and posttraumatic stress disorder (PTSD) 3 -6 ; these rates appear to be increasing for members serving in Operation Iraqi Freedom or Operation Enduring Freedom. 7 Because of the stigma of mental illness and a reluctance to seek health care, reported rates are likely underestimates. 8 Combat exposure is particularly problematic, with PTSD prevalence increasing linearly with the number of exposures to direct combat. 9,10 Although rates of psychological distress and exposure to stress and potentially traumatic experiences are high, many service members appear to cope successfully. Contextual factors, such as social support and dyadic functioning (coping and relationship functioning in couples), may account for this variability but are less frequently explored and are consequently less well understood.
Social support is hypothesized to influence how service members cope with exposure to stress. In the civilian context, social support has long been understood as protective. 11 For military personnel, social support includes formal support from military leadership and informal support from unit members and civilian family and friends. 12,13 Although both sources of support can be important, informal social support is shown to be more important to overall functioning. 14 Overall, lower levels of social support are associated with an increase in PTSD and depressive symptoms and a decrease in psychosocial functioning among military personnel. 13,15
Much research has examined the effect of service members’ mental health on dyadic functioning. 16 In contrast, little research has considered how healthy dyadic functioning contributes to or protects against adverse outcomes among military personnel. Some evidence suggests that a healthy spousal relationship could be associated with better outcomes for service members. 17
Dyadic relationships may be influenced by the support that military personnel and their families receive from broader social networks (ie, nonmilitary coworkers, members of one’s faith community, or classmates). The limited research examining this influence demonstrates a positive association between social support and dyadic adjustment. 18 For military families, the burden of military-related stressors is linked to marital dissatisfaction. 19 To the extent that support from other sources (ie, extended family or friend networks) alleviates some of the burden on military spouses, this support may also affect dyadic functioning and, subsequently, service members’ mental health.
The objective of this study was to examine social support and dyadic functioning among service members, with special attention to the possible mediating role that dyadic functioning may exert on the association between social support and mental health outcomes. Although social support and dyadic functioning appear to be associated with mental health outcomes for service members, little clarity exists about how these factors may work together to contribute to or protect against mental illness in this population. We considered the direct and indirect effects of dyadic functioning and social support from family members, civilian peers (nonmilitary friends), military peers, and military leaders on service members’ mental health (depression, PTSD, and anxiety). We hypothesized the following:
Hypothesis 1: Higher levels of social support from family, nonmilitary friends, military peers, and military leaders will be associated with higher levels of dyadic functioning.
Hypothesis 2: Higher levels of social support from family, nonmilitary friends, military peers, and military leaders will be associated with fewer symptoms of depression, PTSD, and anxiety.
Hypothesis 3: Dyadic functioning will mediate the relationship between social support and mental health symptoms.
Methods
These data were part of a larger national study on problems with sexual functioning in young military populations (N = 399). 20 Recruitment and data collection took place in October and November 2013. Recruitment occurred online through social media and through existing networks with military organizations. Invitations and study information were sent via email and through a study website and other social media outlets. Study data were confidential. The survey took an average of 30 minutes to complete. The study was approved by the University of Southern California Institutional Review Board, and informed consent was collected online at the beginning of each survey. Respondents received a $25 gift card as compensation. Study details are available elsewhere. 20
Participants
For these analyses, our sample consisted of partnered people (those who self-identified as being in a long-term relationship, regardless of marital status) who had been deployed at least once (n = 321). The sample represented all branches of service: air force, 4.4% (n = 14); army, 69.2% (n = 222); Marine Corps, 10.0% (n = 32); navy, 5.3% (n = 17); coast guard, 0.6% (n = 2); and National Guard, 10.6% (n = 34). Participants were predominantly male (n = 296, 92.2%) and ranged in age from 23 to 40 years (mean = 31.8, standard deviation [SD] = 3.8). Racial/ethnic distribution was as follows: non-Hispanic white, 70.7% (n = 227); Hispanic, 10.3% (n = 33); non-Hispanic black, 10.6% (n = 34); and other, 8.4% (n = 27). All participants had been deployed for ≥30 days at least once, with most deploying multiple times (n = 240, 74.8%). Most were married (n = 260, 81.0%).
Measures
Social Support
We used a modified Multidimensional Scale of Perceived Social Support 21 to assess perceptions of supports. We added 2 sources of support (military peers and leaders) to the 3 original sources of support (family, friends, and significant other; “significant other” was removed from analyses because we were unable to determine from responses if the significant other was a romantic partner). Additionally, questions in the “friends” subscale were reworded to “nonmilitary friends.” The modified scale consisted of 20 items rated on a 7-point Likert scale (1 = very strongly disagree, 7 = very strongly agree). We created a summary score for each source of social support (range, 4-20). We rated internal consistency of the original scale as α = 0.88. 20 In this sample, overall α was 0.93, and α for the subscales ranged from 0.84 to 0.92.
Depression
We used the Patient Health Questionnaire–9 to assess depression severity. 22 This measure assesses how often a person was bothered by depressive symptoms during the previous 2 weeks (0 = not at all, 3 = nearly every day). We calculated a total score (range, 0-27) and used the following categories to define level of anxiety: minimal (1-4), mild (5-9), moderate (10-14), moderately severe (15-19), and severe (20-27). 23 The Patient Health Questionnaire–9 had good internal consistency in previous research (α = 0.89) 21 and in this sample (α = 0.96).
PTSD
We assessed PTSD using the 17-item PTSD Checklist–Military Version. 24 This measure asks participants to rate the level and frequency of complaints related to a stressful military experience during the previous month (1 = not at all, 5 = extremely). We calculated the total score by summing all items (range, 17-85), with a score ≥38 indicating probable PTSD. The PTSD Checklist–Military Version has adequate internal consistency with military service members (α = 0.89-0.91) 25,26 ; here, α = 0.99.
Anxiety
We used the 7-item Generalized Anxiety Disorder scale 27 to assess how often participants were bothered by anxiety, such as feeling nervous or being unable to control worry, during the previous 2 weeks. The items were rated on a 4-point Likert scale (0 = not at all, 3 = nearly every day). We calculated the total score by summing the items (range, 0-21) and used the following categories to define level of anxiety: minimal (0-4), mild (5-9), moderate (10-14), and severe (15-21). The scale has strong internal consistency (α = 0.89) 27 ; in this sample, α = 0.96.
Dyadic Functioning
We used the Dyadic Adjustment Scale 28 to assess the relationship quality of romantic partners. The 32 items were rated on a 5-point Likert scale (0 = always disagree to 5 = always agree). We calculated the total score by summing all items (range, 0-151; scores vary by item); higher scores indicate a more positive dyadic relationship. Internal consistency in the original work 29 was rated as α = 0.92; here, α = 0.87.
Controls
We assessed age (in years), marital status (married, not married, divorced/separated/widowed), race/ethnicity (non-Hispanic black, non-Hispanic white, Hispanic, other), and combat disclosure and exposure. We examined combat disclosure 30 with a 6-item measure evaluating a service member’s willingness to disclose thoughts and feelings about combat experiences to an intimate partner. Items were measured on a 4-point Likert scale (1 = strongly disagree, 4 = strongly agree; range, 6-24). Cronbach α in the original work was 0.94; here, it was 0.93. The Combat Exposure Scale 31 is a 7-item measure assessing wartime stressors. Items were rated on scales measuring occurrence (1 = no or never, 5 = more than 50 times), duration (1 = never, 5 = more than 6 months), frequency (1 = no, 4 = more than 12 times), or degree of loss (1 = no one, 4 = more than 50%). 31 Cronbach α in this study was 0.87.
Statistical Analyses
We analyzed data with SPSS version 22. 32 We performed process modeling through mediation analysis to examine (1) the direct relationship between each source of social support with each mental health outcome and dyadic functioning and (2) the effects of perceived social support on mental health, with dyadic functioning as an intermediate variable. 33 We used a bootstrapping procedure with 4000 bootstrap samples in which source of social support was the independent variable, dyadic functioning was the mediating variable, and mental health was the dependent variable. We tested a structural model (Figure) in analyses. In the method proposed by Hayes, 33 significant direct effects are not necessary prerequisites for proceeding with mediation analysis. All analyses controlled for age, marital status, race/ethnicity, combat exposure, and combat disclosure. We found no indications of multicollinearity in our models, as assessed by examining tolerance and the variance inflation factor. The use of listwise deletion resulted in the omission of data on 46 of 321 participants (14.3%) from the depression models and 47 of 321 participants (14.3%) from the PTSD and anxiety models.
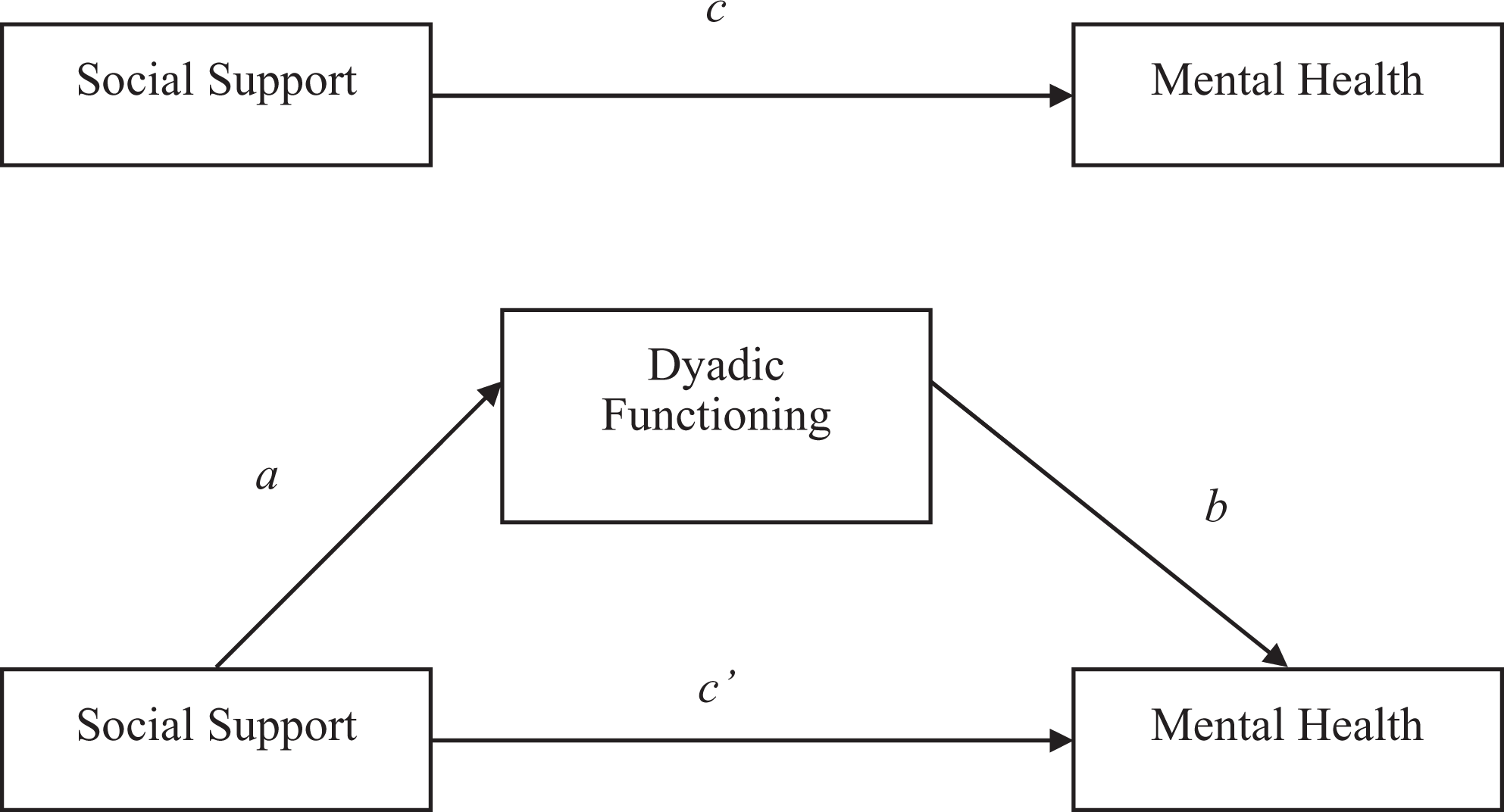
Sources of social support on mental health—total effect (above) and dyadic functioning as a mediator of the effect (below): a, direct effect of social support on dyadic functioning; b, direct effect of dyadic functioning on mental health; c, total effect of social support on mental health, including direct and indirect effects; c′, direct effect of social support on mental health. Adapted from the process mediation model developed by Hayes. 33
Results
Dyadic adjustment had moderate positive correlations with sources of social support (r = 0.21-0.44) and modest negative correlations with mental health outcomes (r = −0.08 to −0.11; Table 1). Directionality of the bivariate relationship, however, varied by source of support. Although support from family was negatively associated with mental health outcomes, support from military peers and military leaders was positively associated with mental health outcomes. Support from nonmilitary friends was positively associated with depression but negatively associated with PTSD and anxiety.
Mean scores for and correlations among social support, mental health outcomes, and dyadic adjustment: study of US military service members (n = 321), October-November 2013
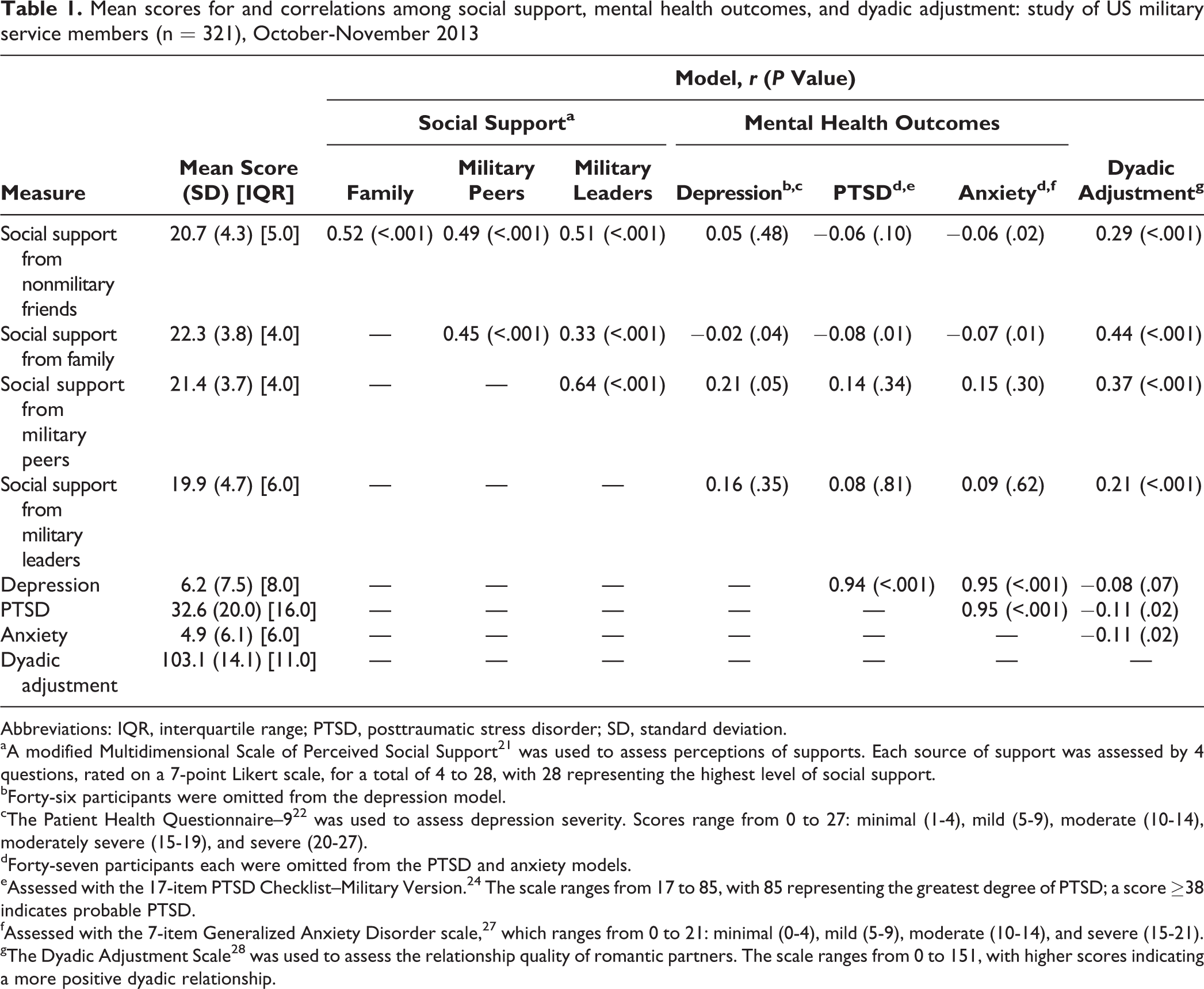
Abbreviations: IQR, interquartile range; PTSD, posttraumatic stress disorder; SD, standard deviation.
aA modified Multidimensional Scale of Perceived Social Support 21 was used to assess perceptions of supports. Each source of support was assessed by 4 questions, rated on a 7-point Likert scale, for a total of 4 to 28, with 28 representing the highest level of social support.
bForty-six participants were omitted from the depression model.
cThe Patient Health Questionnaire–9 22 was used to assess depression severity. Scores range from 0 to 27: minimal (1-4), mild (5-9), moderate (10-14), moderately severe (15-19), and severe (20-27).
dForty-seven participants each were omitted from the PTSD and anxiety models.
eAssessed with the 17-item PTSD Checklist–Military Version. 24 The scale ranges from 17 to 85, with 85 representing the greatest degree of PTSD; a score ≥38 indicates probable PTSD.
fAssessed with the 7-item Generalized Anxiety Disorder scale, 27 which ranges from 0 to 21: minimal (0-4), mild (5-9), moderate (10-14), and severe (15-21).
gThe Dyadic Adjustment Scale 28 was used to assess the relationship quality of romantic partners. The scale ranges from 0 to 151, with higher scores indicating a more positive dyadic relationship.
Source of Social Support and Dyadic Functioning
We found significantly positive direct effects of social support on dyadic functioning for all sources of support, supporting hypothesis 1. Thus, as expected, social support from nonmilitary friends (β = 1.21, standard error [SE] = 0.19; 95% confidence interval [CI], 0.83-1.59; P < .001), family (β = 2.20, SE = 0.20; 95% CI, 1.81-2.60; P < .001), military peers (β = 1.98, SE = 0.22; 95% CI, 1.56-2.41; P < .001), and military leaders (β = 0.94, SE = 0.19; 95% CI, 0.57 -1.30; P < .001) was associated with higher levels of dyadic functioning.
Source of Social Support, Dyadic Functioning, and Depression
Of the 321 participants, 186 (57.9%) reported minimal depression symptoms; 52 (16.2%), mild; 27 (8.4%), moderate; 15 (4.7%), moderately severe; and 41 (12.8%), severe. Contrary to expectations (hypothesis 2), the process model showed positive direct effects for each source of social support on depression (Table 2). Although the association between social support from military peers and depression symptoms was not significant (β = 0.15; 95% CI, −0.04 to 0.35), social support from nonmilitary friends (β = 0.26; 95% CI, 0.12-0.41), family (β = 0.31; 95% CI, 0.11-0.51), and military leaders (β = 0.14; 95% CI, 0.01-0.28) was significantly associated with higher levels of depression. Results indicated partial support for hypothesis 3: dyadic functioning did mediate the relationship between social support and depression symptoms for support from nonmilitary friends (β = −0.06; 95% CI, −0.15 to −0.01) and family (β = −0.14, 95% CI, −0.31 to −0.02) but not from military peers or leaders.
Results of process model showing effects of social support on mental health outcomes and the role of dyadic functioning in mediating the relationship between social support and mental health outcomes: study of US military service members (n = 321), October-November 2013a
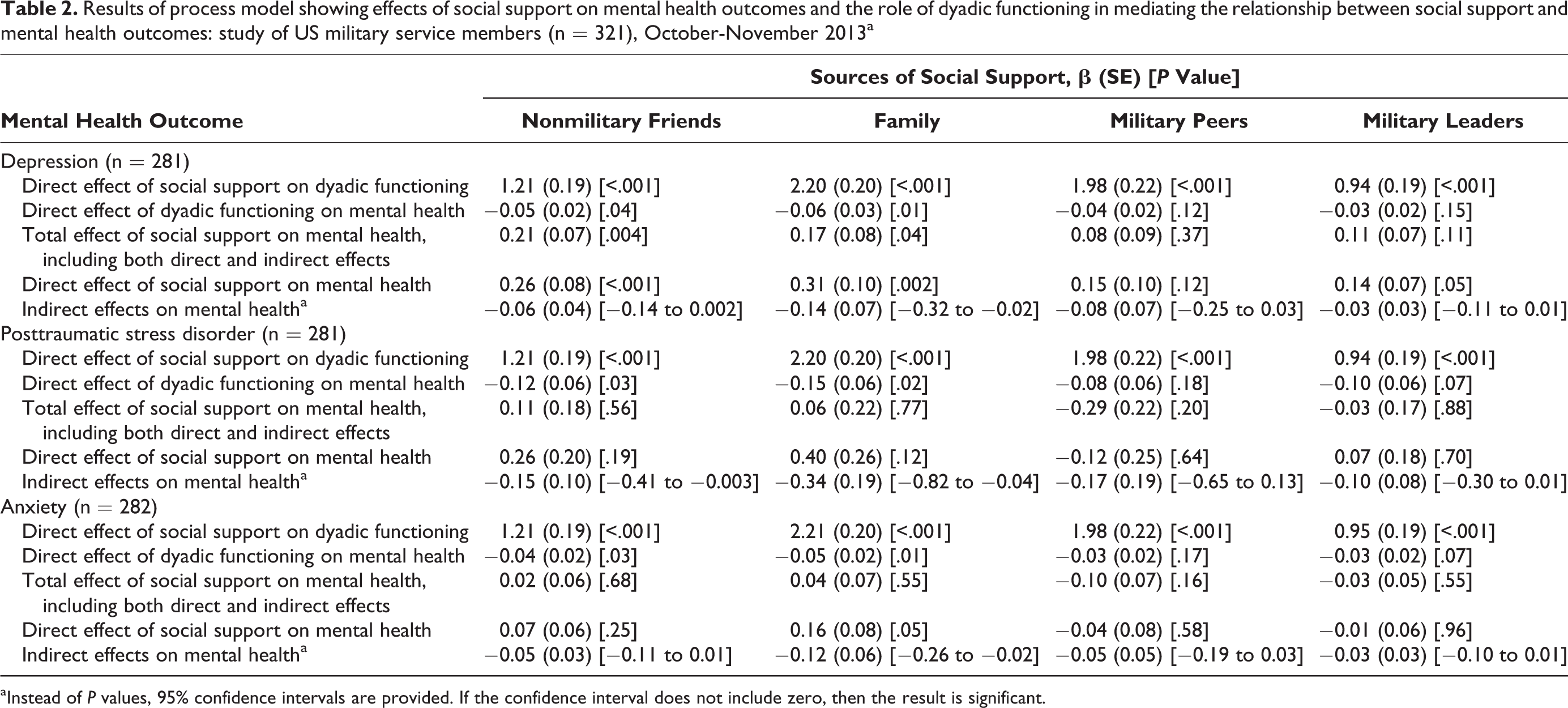
aInstead of P values, 95% confidence intervals are provided. If the confidence interval does not include zero, then the result is significant.
Source of Social Support, Dyadic Functioning, and PTSD
Of the 321 participants, 66 (20.6%) reported probable PTSD. The process model (Table 2) showed positive direct (but not significant) effects for social support from nonmilitary friends (β = 0.26; 95% CI, −0.26 to 0.48), family (β = 0.40; 95% CI, −0.11 to 0.91), and military leaders (β = 0.07; 95% CI, −0.29 to 0.43) and a negative direct (but not significant) effect for social support from military peers (β = −0.12; 95% CI, −0.62 to 0.38) on PTSD. Thus, hypothesis 2 was not supported by the evidence on PTSD. The process model did indicate that dyadic functioning mediated the relationship between social support and PTSD symptoms for support from nonmilitary friends (β = −0.15; 95% CI, −0.41 to −0.01) and family (β = −0.34; 95% CI, −0.82 to −0.04), partially supporting hypothesis 3.
Source of Social Support, Dyadic Functioning, and Anxiety
Of the 321 participants, 203 (63.2%) had minimal anxiety symptoms; 46 (14.3%), mild; 27 (8.4%), moderate; and 43 (13.4%), severe. The process model (Table 2) showed positive (but not significant) direct effects for social support from nonmilitary friends (β = 0.07; 95% CI, −0.05 to 0.19) and negative (but not significant) direct effects for social support from military peers (β = −0.04; 95% CI, −0.20 to 0.11) and military leaders (β = −0.01; 95% CI, −0.12 to 0.11) on anxiety. Only social support from family members showed a significant (positive) direct effect (β = 0.16; 95% CI, 0.01-0.32). Thus, hypothesis 2 was partially supported by the evidence on anxiety. The process model also indicated that dyadic functioning mediated the relationship between social support and anxiety symptoms for support from family (β = −0.12; 95% CI, −0.26 to −0.02), partially supporting hypothesis 3.
Discussion
Although our findings on the influence of social support on mental health did not fully support our hypotheses and were sometimes counterintuitive, greater social support was significantly associated with better dyadic functioning across all types of social supports. However, this dyadic functioning mediated only the role of nonmilitary social support. Although study participants reported similar levels of support from military and nonmilitary sources, support from military sources may not have been robust enough to influence the overall mental health of the participants, or it may have been a better form of support for other stressors (eg, employment-related stress). Nevertheless, social support from military and nonmilitary sources was associated with better dyadic functioning. This finding suggests that although support from outside the nuclear family does not directly influence the functioning of intimate partner relationships, it may benefit couples who have experienced deployment.
Overall, the results partially supported our hypotheses on the association between social support and depression, PTSD, and anxiety. The negative outcomes of anxiety, depression, and PTSD among military personnel, including reduced levels of social integration, are well known. 34,35 Less social support is associated with more symptoms of depression and PTSD, 36,37 although the direct effects of less support may be fully mediated by resilience 15 or coping self-efficacy, 38 which, like dyadic functioning in this study, accounted for the influence of social support. Unexpectedly, when social support directly influenced mental health in our sample, the effects were positive: greater levels of social support were associated with a greater number of symptoms. Similar to findings among other populations, 39 this finding may be explained by considering that people who have more symptoms of mental illness may be more likely to seek support from those around them. Seeking the support of others during challenging mental health events should be framed as a positive coping strategy (a form of resilience), providing insights into ways in which interventions for this population might use positive external processing techniques (ie, group work) or other strategies that build networks of emotional support to military personnel.
Although some evidence suggests that social support and better (perceived or actual) relationships with partners can buffer the effects of PTSD and depression symptoms, 35 our results only partially supported our hypothesis that dyadic functioning would mediate the relationship between social support and mental health. In all 3 models (depression, PTSD, and anxiety), dyadic functioning mediated the relationship between family/nonmilitary friends and mental health; these findings were not replicated in any of the models for support from military peers or leaders. The lack of findings related to military-connected social network members may be explained, at least in part, by the mixed influence of support members found in previous work. For example, although active duty members report experiencing protective factors associated with greater connectivity to military support systems, deployments may result in additional stressors for National Guard families, including lack of social support. 14,40
Furthermore, maintaining social networks that consist mostly of military members, particularly if the service member is no longer active, is associated with increased anxiety, depression, and PTSD. 33 Alternatively, having mental health symptoms may impede social support or dyadic functioning. Factors associated with mental distress include self-imposed social exclusion or isolation, 41 apathy, 42,43 and volatility. 44 Any of these factors can strain relationships with partners or other support network members, influencing the mediation explored in our study. Furthermore, participants in our study may have perceived social support (as measured by the Multidimensional Scale of Perceived Social Support) but not actually used it, a signal of reluctance to seek help from others. Our study sheds light on factors that should be investigated in future studies, particularly support from family and nonmilitary peers, that can bolster healthy intimate partner relationships and reduce symptoms of mental distress among military personnel who have been deployed.
Limitations
Although our sample included participants from all service branches who resided throughout the United States, participants were self-selected, making findings nongeneralizable. Self-selection likely excluded service members who had more severe mental health symptoms, a known barrier to engaging in research. Second, we did not collect social network data but rather assessed social support; we could not provide a nuanced understanding of social network members and whom participants designated as part of which member group. Third, our study measured perceived social support, which may differ from objectively measured social support. Future studies should consider including objective measures of social support or collecting formal social network data to explicate network structure, creating opportunities for testable prevention and intervention points. Similarly, future research should consider collecting couple-level data to triangulate dyadic functioning. Finally, data were cross sectional, so causality could not be inferred. Future longitudinal research that assesses contextual factors, including social support and dyadic functioning, before assessing mental health may elucidate causal processes and provide accurate estimates of meditational effects. 45 However, given our limited understanding of the role of mediated social support on the mental health of military service members, we believe that our findings contribute to the knowledge base and provide the foundation for future research and clinical decision making.
Conclusion
Much of the research exploring the mental health of military personnel failed to account for potential important differences in support and how variations in social networks may be associated with individual well-being. This exploratory study adds to the limited understanding of how social support and dyadic functioning are associated with mental health symptoms in military personnel, and it provides preliminary insights into areas of intervention for military service members and their families. Bolstering social support from military and nonmilitary sources may be particularly beneficial for healthy dyadic functioning among service members who have been deployed and their partners. Given the high rates of adverse outcomes among recently deployed service members, future research should continue to investigate how social support, dyadic functioning, and other contextual variables influence health and mental health in this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a grant from the Iraq Afghanistan Deployment Impact Fund of the California Community Foundation (CALCOM/HASSAN/2013; principal investigator, S. Wilcox).