
Abstract
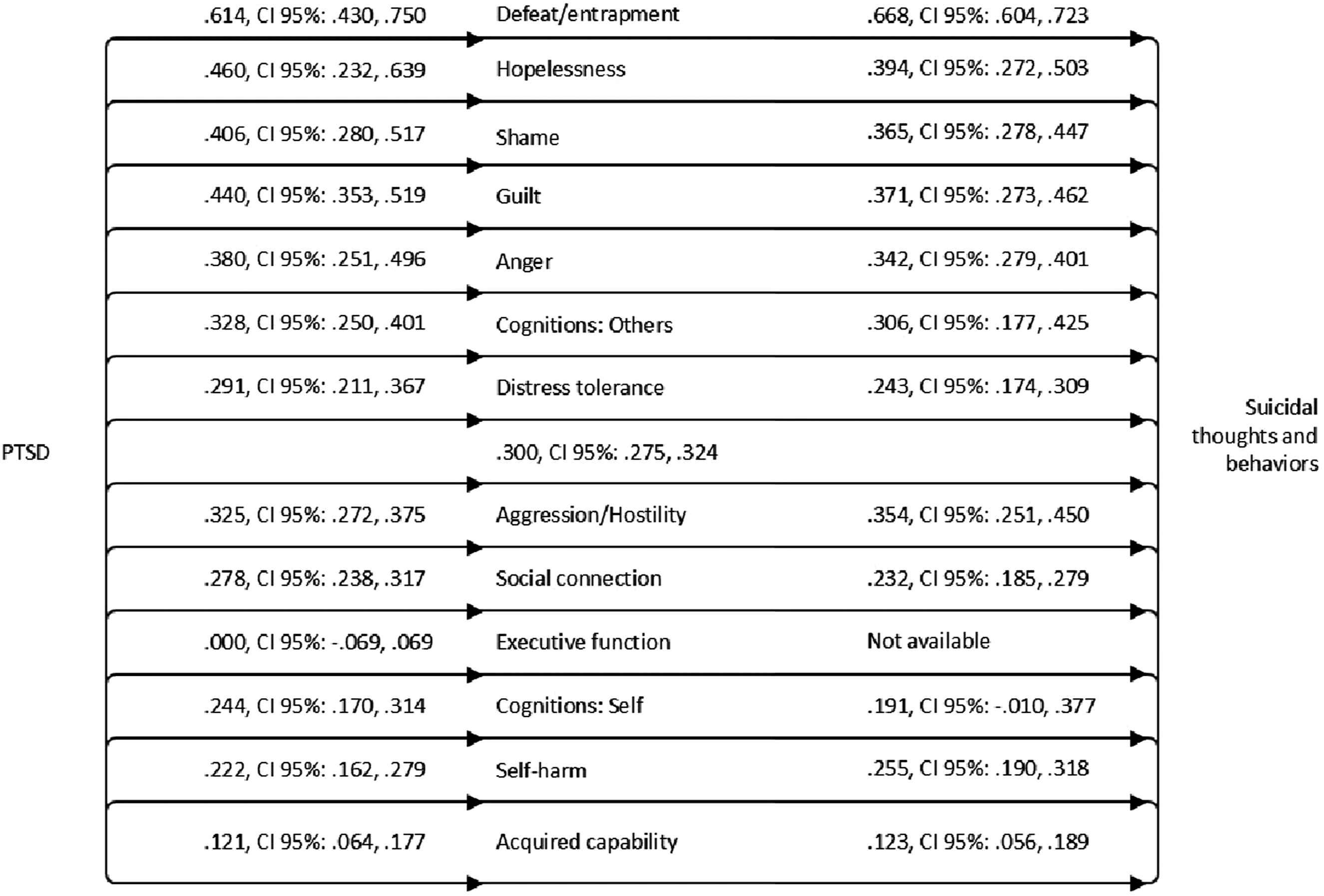
Posttraumatic stress disorder is a well-known risk-factor for suicidal ideation and attempts, but there have been few attempts to systematically evaluate correlates of this association. Using purported mechanisms of the development of suicidal thoughts and behaviors across nine theories as a guide, a series of meta-analyses (K = 191 studies, N = 79,106) were conducted. Posttraumatic stress disorder had a moderate association with suicidal thoughts and behaviors. Defeat and entrapment had large associations with both posttraumatic stress disorder and suicidal thoughts and behaviors. Hopelessness, shame, guilt, anger, and negative cognitions about other people each had moderate associations with both posttraumatic stress disorder and suicidal thoughts and behaviors. Smaller but significant associations were observed for distress tolerance, aggression/hostility, social connection, negative cognitions about the self, self-harm, and acquired capability for suicide. Significant heterogeneity was detected in the meta-analyses and explored quantitatively to examine reasons for heterogeneity. These findings are consolidated into a new framework, the CEASE Framework, reflecting changes in
Rates of suicide have steadily increased over the past two decades in the United States, and over 45,000 individuals die by suicide annually in the United States alone (Centers for Disease Control and Prevention, 2021). Posttraumatic stress disorder (PTSD) is associated with increased risk of suicidal ideation, suicide attempts, and suicide death (Brown et al., 2016; Gradus et al., 2015; May & Klonsky, 2016; Stein et al., 2010). Patients with PTSD are between 3–7 times more likely to die by suicide compared to patients without PTSD, even after adjusting for other psychiatric comorbidities (Fox et al., 2021). Despite the well-established link between PTSD and suicide risk, mechanistic research has yet to converge on a unifying theory to explicate the multitude of potential explanatory factors driving this effect. Theories about the development of suicide risk generally point to a variety of potential factors that can help inform an explanatory model about the relationship between trauma, PTSD, and suicide risk.
To meet criteria for PTSD, an individual must first experience, witness, or learn about a traumatic event (criterion A), which can include actual or threatened death, physical injury or sexual violation (American Psychiatric Association, 2013). In addition, an individual must endorse one symptom each from the intrusion symptoms cluster (criterion B) and the avoidance symptoms cluster (criterion C), and two symptoms from each of the negative alterations in mood and cognition cluster (criterion D) and the alterations in arousal and reactivity cluster (criterion E). Finally, an individual must report symptom distress for over one month (criterion F), clinically significant distress or impairment (criterion G), and the symptoms cannot be attributable to a medical condition or substance use (criterion H).
Many individual studies have attempted to demonstrate how PTSD symptoms uniquely contribute to suicide risk. Brown et al. (2018a) found that each of the four PTSD symptom clusters were uniquely associated with suicidal ideation across two samples, but the alterations in arousal and the negative alterations in mood and cognitions clusters were most strongly associated with suicidal ideation (Brown et al., 2018a). These findings have largely been replicated in other reports (Chu et al., 2021; Stanley et al., 2019; Surís et al., 2011), but some studies have reported that other PTSD symptoms (e.g., externalizing) are more closely tied to suicide risk depending on how the models are constructed (Chu et al., 2021). Some trauma types (e.g., childhood maltreatment, assault), are more closely associated with suicidal ideation and behavior than others (e.g., life-threatening injury or exposure to a terrorist attack; LeBouthillier et al., 2015). Each additional trauma is associated with a 20.1% increase in the likelihood of suicidal ideation and a 38.9% increase in the likelihood of suicide attempts (LeBouthillier et al., 2015). Rather than attempting to understand the link between PTSD and suicide risk through its symptoms or types of traumatic exposures, there may be value in exploring common correlates of PTSD and suicide risk to help inform an underlying conceptual model linking the two.
Numerous theories about the development of suicidal thoughts and behaviors are useful for understanding the association between PTSD and suicide risk; examples of such models include the Interpersonal Theory of Suicide (Joiner, 2005), Cognitive Theory of Suicidal Behavior, informed by Beck’s (1967) theory of depression (Wenzel & Beck, 2008), Fluid Vulnerability Theory (Rudd, 2006), Integrated Motivational-Volitional Model of Suicidal Behaviour (O’Connor, 2011; R. C. O’Connor & Kirtley, 2018), Three-Step Theory of Suicide (Klonsky & May, 2015), Diathesis Stress Model of Suicide (Mann & Arango, 1992; Mann et al., 1999; Rubinstein, 1986), Escape Theory of Suicide (Baechler, 1980; Baumeister, 1990), Cry of Pain Model (Bolton et al., 2007; Williams, 1997; Williams et al., 2005), and the Schematic Appraisal Model (Johnson et al., 2008). While most of these prior models included traumatic and/or threatening stressful event exposure as an important risk factor for suicide, none of these prior models intended to present a coherent, mechanistically derived explanation for how the cognitive, emotional, and behavioral impact of trauma exposure (e.g., symptoms of PTSD) increases risk for suicide.
The goal of these meta-analyses is to provide the first in-depth consideration of how PTSD may operate according to the tenets of these nine conceptual models of the development of suicidal thoughts and behaviors. Core components of these theories, both shared and unique, are briefly reviewed below and compared against the scientific literature on features of PTSD and risk for suicidal thoughts and attempts. Then, meta-analyses evaluated the evidence base supporting these variables as key correlates of both PTSD and suicide risk. To consolidate across theoretical frameworks, an overarching conceptual model is proposed (“CEASE”) that harnesses empirically supported features of the PTSD-suicide link based on this evaluation. This theory is inspired by recent calls to conduct rigorous descriptive research on the building blocks of features that are presumed to increase suicidal thought and behaviors, and to consider the possibility that suicide in the context of trauma exposure and PTSD-related distress results from dynamic interactions from multiple processes (Millner et al., 2020). The consolidated CEASE theory is offered to inform future research on the link between PTSD and suicide risk that considers more systematic evaluations of the multitude of factors that change following exposure to a trauma and increase risk for suicide among patients with PTSD.
Interpersonal Theory of Suicide
According to the Interpersonal Theory of Suicide (sometimes called the Interpersonal Psychological Theory of Suicide; Joiner, 2005), suicidal desire is a function of two interpersonal factors, namely thwarted belongingness and perceived burdensomeness. Thwarted belongingness reflects one’s perception of being disconnected from a social network. In contrast, perceived burdensomeness reflects an individual’s perception that he or she is a liability to the world, including cognitions of self-hatred and other negative cognitions about the self. Both thwarted belongingness and perceived burdensomeness are assumed to be fluid states of suicidal desire, rather than stable cognitive-affective states. However, suicidal desire alone is rarely sufficient to initiate suicidal behaviors, and the Interpersonal Theory of Suicide was one of the first theories to explain differential pathways to suicidal ideation and suicidal behavior. According to the Interpersonal Theory of Suicide, suicide attempts occur in the context of acquired capability for suicide, which reflects low fear of death and high physical pain tolerance. Unlike variables constituting suicidal desire, presumed to be fluid, acquired capability is presumed to be an emergent variable that develops in some individuals over time. Recent meta-analyses have demonstrated support for the Interpersonal Theory of Suicide, though the effect sizes for each construct have only modest predictive power (Chu et al., 2017).
Interpersonal Theory of Suicide and PTSD
Negative cognitions about the self, others, and the world are a core feature of PTSD (American Psychiatric Association, 2013). For some individuals with PTSD, these negative cognitions take the form of perceived burdensomeness or thwarted belongingness. Thwarted belongingness is related to persistent detachment/estrangement, one of the negative alterations in cognitions and mood included in the DSM-5 diagnostic criteria for PTSD (e.g., a persistent feeling of detachment or estrangement from one’s social network; American Psychiatric Association, 2013). Additionally, individuals with PTSD commonly report mistrust of other people, leading to isolation and loneliness, consistent with thwarted belongingness. Thwarted belongingness cognitions are included on the Posttraumatic Cognitions Inventory (PTCI; Foa et al., 1999), including “I feel isolated and set apart from others,” “People can’t be trusted,” “You can never know who will harm you,” and “I can’t rely on other people”, among many others. Perceived burdensomeness perceptions of being a liability and self-hatred are also reflected on the PTCI, including “I am inadequate”; “The trauma happened to me because of who I am”; “There is something wrong with me as a person”; and “I can’t rely on myself”, among many others. Scores on the PTCI are consistently elevated among individuals with PTSD relative to both individuals with trauma exposure who do not have PTSD and to healthy controls (Brown et al., 2019). Furthermore, trauma-related cognitions are a core mechanism of response to PTSD treatment (Brown et al., 2019). Thus, perceived burdensomeness and thwarted belongingness are well-represented in the PTSD literature, although they have been referred to as trauma-related cognitions more broadly.
The connection between PTSD and acquired capability is also robust. Van Orden and colleagues (2010) offered several examples of traumatic events that may increase acquired capability for suicide, including a family history of suicide, clustering or exposure to suicide risk in the social network, combat exposure and childhood abuse (Bryan et al., 2017; Cerel et al., 2015). This list is not exhaustive. Given that PTSD was characterized as an anxiety disorder prior to the release of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013), one might assume that an individual with PTSD would have higher degree of fear about death, which would theoretically reduce acquired capability for suicide. Indeed, a certain subset of individuals with PTSD report high levels of fear about death. However, a growing body of evidence suggests that some individuals with PTSD report hypoarousal, characterized by numbing and dissociation, rather than elevations in fear and hyperarousal. For instance, individuals with more severe PTSD demonstrate blunted heart rate and skin conductance reactivity to startle cues compared to individuals with less severe PTSD (d’Andrea et al., 2013). This subset of individuals with a blunted physiological response may be more likely to report fearlessness about death.
In terms of altered pain sensitivity as a component of acquired capability, data on this construct are mixed for patients with PTSD. Individuals with PTSD are more likely to have significant chronic pain than individuals without PTSD (Siqveland et al., 2017), and PTSD severity is correlated with pain severity and pain interference (Lang et al., 2014). For some individuals with PTSD, their pain is caused by physical injuries sustained during their index trauma. For others, pain is caused by medical comorbidities that are also more likely among individuals with PTSD, including metabolic, cardiovascular diseases, musculoskeletal and neurological diseases (Lihua et al., 2020; McFarlane et al., 1994). In a sample of trauma-exposed undergraduates, PTSD numbing symptoms were positively associated with pain tolerance (Zuromski et al., 2014). In a small sample, outpatients with PTSD had lower initial pain thresholds compared to healthy controls, and they had significantly greater increases in pain threshold and tolerance and decreases in pain intensity compared to healthy controls throughout the painful task (Diener et al., 2012). A robust literature suggests that pain is an important risk factor for suicide (Fishbain, 1999), especially among individuals who engage in catastrophizing about their pain (Brown et al., 2020b). Per the Interpersonal Theory of Suicide, individuals who are suicidal have a greater capacity to withstand pain. Thus, associations between PTSD, pain, and suicidal thoughts and behavior are complex.
Bryan and colleagues (2016) studied acquired capability in the context of active duty military service members who had been exposed to combat traumas. Service members appeared to have a “set-point” for acquired capability from which they occasionally deviated but eventually returned. Thus, acquired capability did not meaningfully change from pre-to post-deployment, regardless of intensity of exposure to violence or history of trauma at pre-deployment. Contrary to predictions from the Interpersonal Theory of Suicide, this finding implies that acquired capability does not continually increase as a function of exposure to trauma. Instead, individuals have an “unstable” score on this construct that may fluctuate over time, but eventually will return to baseline. We discuss the idea of a set-point for suicide risk in general in more detail below under the Fluid Vulnerability for Suicide section.
Theoretical Correlates of PTSD and Suicide from the Interpersonal Theory of Suicide
Van Orden et al. (2010) presented three key hypotheses stemming from the Interpersonal Theory of Suicide. First, thwarted belongingness and perceived burdensomeness are proximal and sufficient causes of suicidal ideation. Second, suicidal intent is the product of suicidal desire and lowered fear of death. Third, high lethality suicide attempts are a product of perceived burdensomeness, thwarted belongingness, lowered fear of death, and increased physical pain tolerance.
PTSD increases negative cognitions about the self (perceived burdensomeness), detachment and/or estrangement from ones’ social network (thwarted belongingness), and alters pain tolerance (acquired capability for suicide) depending on the type of trauma exposure (e.g., family history of suicide) and degree of numbing sequelae. Given that the Interpersonal Theory of Suicide proposes a key role each of these factors in the development of suicide risk, we posit each as possible correlates of the association between PTSD and suicidal thoughts and behaviors: negative cognitions about the self, the world, or other people, altered social connections, acquired capability for suicide (including family history of suicide and increased pain tolerance).
Cognitive Model of Suicidal Behavior
Wenzel and Beck (2008) developed a cognitive model for suicidal behavior. According to this Cognitive Theory, three main factors are associated with risk, namely: dispositional vulnerability factors, cognitive processes associated with both psychiatric disturbances, and suicidal acts, in order from least to most direct predictors of suicidal behavior. According to the Cognitive Model of Suicidal Behavior, dispositional vulnerability factors are trait-like factors that are associated with psychiatric symptoms and suicidal behavior. Wenzel and Beck (2008) proposed five types of dispositional vulnerability factors, including impulsivity (an indication of executive functioning deficits) and related factors (e.g., aggression and hostility), over-general memory style, trait-like maladaptive cognitive style (i.e., the tendency to make non-specific cognitive distortions and endorse non-specific dysfunctional attitudes), and personality (including perfectionism). In the context of stress, dispositional vulnerability factors activate cognitive processes associated with psychiatric disturbances or suicidal behavior, consistent with a diathesis-stress model (see below).
Cognitive processes associated with psychiatric disturbances include both distorted cognitive content and information processing biases that are associated with psychiatric symptoms. Underlying schemas dictate cognitive distortions or information processing biases. Information processing biases related to suicidal thoughts and attempts include an attention bias toward suicide-related stimuli and attentional fixation, or “tunnel vision” toward suicide-related stimuli. Cognitive processes related to suicidal thoughts and behavior include hopelessness and perceptions of unbearability, among others.
Cognitive Model of Suicidal Behavior and PTSD
Individuals with PTSD are characterized by many of the dispositional vulnerability factors that are proposed in the Cognitive Model of Suicidal Behavior. These include a tendency toward impulsive and risk-taking behavior (American Psychiatric Association, 2013), aggression and hostility (Jakupcak et al., 2007), problem-solving deficits (e.g., executive functioning deficits; Sutherland & Bryant, 2008), and perfectionism (Egan et al., 2014). PTSD is also characterized by over-general memory, with poor specificity in both their positive and negative memories (Sutherland & Bryant, 2008).
There is a significant body of research implicating hopelessness in the conceptualization of PTSD (Brown et al., 2019; Mihaljević et al., 2012), in addition to other negative cognitions about the self, the world and other people. Examples of hopelessness cognitions about the self include “I will never be able to feel normal emotions again,” “I have permanently changed for the worse,” and “Nothing good can happen to me anymore,” all of which are reflected on the PTCI. Core negative cognitions about the world include perceptions about elevated danger, such as “I have to be on guard all the time” and “The world is a dangerous place.” Other common negative cognitions in PTSD focus on self-blame, such as “The event happened because of the way I acted” and “Somebody else would have stopped the event from happening.” The cognitions are conceptualized to exacerbate psychological suffering in the aftermath of a trauma. Attentional bias and attentional fixation toward suicide-related cues are under-researched topics within the PTSD literature. More research needs to be conducted on these topics.
Theoretical Correlates of PTSD and Suicide from the Cognitive Model of Suicidal Behavior
The Cognitive Model of Suicidal Behavior suggests that the risk for suicidal behavior increases as the frequency, intensity or duration of the cognitive distortions and information processing biases increases in the presence of the dispositional vulnerability factors. In this model, the timing of suicidal behavior depends on the threshold of tolerance, or the point at which an individual can no longer tolerate distress stemming from cognitions and emotions. This threshold of tolerance is different for each person and is influenced by their history of suicidal behavior, social support, and other factors.
As described above, PTSD increases the likelihood of several of the dispositional vulnerability factors included in the Cognitive Model of Suicidal Behavior (e.g., impulsivity/executive functioning deficits, aggression/hostility, altered memory processing, and maladaptive cognitions). Additionally, given the exacerbated psychological suffering individuals experience given the pervasive negative cognitions about the self, the world, or other people, the theory of increased Cognitive Model for Suicidal Behavior clearly indicates that those with PTSD may be more likely to cross the theoretical threshold of distress tolerance. Given these theoretical links, we posit each of these as possible correlates of the association between PTSD and suicidal thoughts and behaviors based on this model: negative cognitions about the self, the world, or other people, aggression/hostility, executive functioning/impulsivity deficits, and altered memory processing.
Fluid Vulnerability Theory
Fluid Vulnerability Theory (Rudd, 2006) was developed as a conceptual model to distinguish between individuals who think about suicide, make one suicide attempt, and make multiple suicide attempts. This theory also endeavors to explain the intensity and duration of single suicide episodes, as well as how single episodes may lead to multiple episodes. Fluid Vulnerability Theory considers both acute activation of risk as well as chronic risk factors. The theory is based on the suicidal mode (Rudd, 2000), which has three key components: predispositions, activating events, and acute risk factors. Predispositions include: cognitive baseline factors, such as low self-esteem/self-regard and cognitive inflexibility; emotional baseline factors, such as psychiatric disorders or general mood lability; physical baseline factors, such as genetics or medical conditions; and behavioral baseline factors, such as prior suicide attempts and interpersonal skills (Bryan & Rudd, 2012). According to Fluid Vulnerability Theory, these predisposing factors constitute an individual’s resting baseline for suicide risk. The transition toward an acute risk episode is contingent upon a triggering event, which can include a relationship conflict, financial concern, perceived loss, physical sensation, or negative memory. An acute risk mode includes: cognitive factors, such as perceptions about being a burden or unlovable; emotional factors, such as anxiety, sadness, shame or guilt; physical factors, including agitation or pain; and behavioral factors, such as isolation or preparatory suicidal behaviors (Bryan & Rudd, 2012).
Fluid Vulnerability Theory and PTSD
Individuals with PTSD demonstrate several of the baseline risk factors, or predispositions, for suicide. In terms of cognitive baseline factors, individuals with PTSD often report low self-esteem, which interferes with recovery from PTSD (Benight & Bandura, 2004). Individuals with PTSD also often struggle with cognitive rigidity, which is correlated with PTSD severity (Kanagaratnam & Asbjørnsen, 2007; Keith et al., 2015; Palm & Follette, 2011). Emotional baseline factors among individuals with PTSD include the diagnosis itself as well as chronic shame, guilt, depression, and anxiety. In terms of physical baseline factors, individuals with PTSD are significantly more likely to report physical health conditions compared to healthy controls, and more exposure to trauma is associated with a greater likelihood of medical condition diagnoses among individuals with PTSD (McLeay et al., 2017; Sledjeski et al., 2008). In terms of behavioral baseline factors, individuals with PTSD are significantly more likely to have made a suicide attempt compared to the general population (Tarrier & Gregg, 2004), as described above. Some research suggests that individuals with PTSD experience a deficit in behavioral interpersonal skills (LaMotte et al., 2017), consistent with the Fluid Vulnerability Theory.
Fluid Vulnerability Theory posits that the development of acute suicidal risk is contingent upon exposure to a triggering event, such as a relationship conflict or income/financial stressor. Individuals with PTSD have a tendency toward heightened reactivity to non-traumatic life events that occur after the development of PTSD (Koopman et al., 2001). In other words, events that may provoke little affect for a person without PTSD can trigger a strong response in individuals with pre-existing PTSD. No research has explored whether non-traumatic stressful life events trigger suicidal crises among patients with PTSD to a greater extent than patients without PTSD, though this would be a reasonable prediction from the Fluid Vulnerability Theory.
Individuals with PTSD commonly report several of the features described in the acute risk mode of Fluid Vulnerability Theory. As described in the Interpersonal Theory of Suicide above, perceptions of being a burden on others or being unlovable are commonly reported among patients with PTSD (Foa et al., 1999). In addition to the chronic negative affect that characterizes PTSD, acute emotional factors include exacerbation in anxiety, shame, or depression in response to internal or external trauma-related triggers. As mentioned above, the chronic medical conditions often experienced among patients with PTSD contribute to physical pain (Defrin et al., 2008), one of the acute physical factors. Finally, in terms of behavioral factors, individuals with PTSD commonly engage in social withdrawal (Laffaye et al., 2008), consistent with the Fluid Vulnerability Theory.
Theoretical Correlates of PTSD and Suicide from the Fluid Vulnerability Theory
There are several key assumptions of the Fluid Vulnerability Theory. One assumption of the Fluid Vulnerability Theory is that suicidal episodes are time limited, or fluid. A second assumption of the theory is that the level of baseline risk for suicide episodes varies across individuals, such that the suicide mode is activated more easily for some individuals than others. Third, after resolution of a suicide episode, an individual returns to their baseline level of risk. Fourth, individuals who have made multiple suicide attempts are thought to have higher baseline risk compared to individuals with one or no prior attempts. Fifth, activating events, or internal/external stressors, elevate suicide risk. Sixth, the severity of the episode is a function of the severity of both the activating event and the baseline risk. Seventh, activating events elevate risk for a short period. Finally, in a suicidal episode, risk is reduced with the resolution of activating events, not with the resolution of baseline risk factors.
Given that PTSD increases the level of reactivity to life events, it would be fruitful to examine additional factors that may increase the likelihood of a person transitioning from PTSD symptoms to suicide attempt. As described above, PTSD increases the likelihood that someone will endorse baseline risk factors described in the Fluid Vulnerability Theory (e.g., lower self-esteem, cognitive rigidity, intense feelings of guilt or shame, negative cognitions about the self like as being a burden or unlovable, physical pain, and changes to social connection). Thus, possible links of the association between PTSD and suicidal thoughts and behaviors based on this model include lower distress tolerance, negative cognitions about the self, cognitive inflexibility, guilt and shame, increased experiences of physical pain, and altered social connections.
Integrated Motivational–Volitional (IMV) Model of Suicidal Behaviour
The Integrated Motivational-Volitional Model of Suicidal Behaviour (O’Connor & Kirtley, 2018) was developed to incorporate features of many prior theories of suicidal ideation and behavior and was inspired by the Theory of Planned Behavior (Ajzen, 1991). First, a pre-motivational phase is characterized by a variety of background factors and life events that set the stage for eventual suicidal thoughts, intent, and behavior, operating in a diathesis-environment-life events triad. In other words, the pre-motivational phase is the context in which suicidal thoughts may emerge. Examples include a background characterized by neglect, the loss of a loved one, and trait social perfectionistic tendencies. The theory suggests that diathesis-stress interactions more strongly affect individuals with some vulnerability to suicide risk. The pre-motivational phase is followed by a motivational phase, which is comprised of factors that lead to suicidal ideation and intent. The third and final phase is the volitional phase, which is comprised of factors that lead to suicidal behavior.
This theory suggests that the proximal predictor of suicidal behavior is behavioral intention. Behavioral intention is theorized to develop because of feelings of entrapment, which is driven by appraisals related to defeat and humiliation (see also Cry of Pain model, described below). Similar to the Escape Theory (described below), individuals are theorized to view suicide as a solution to escape from entrapment. According to the Integrated Motivational-Volitional Model, escalation from defeat/humiliation to entrapment, from entrapment to suicidal ideation/intent, and from suicidal ideation to behavior depends on the presence or absence of key moderators. These moderators include state-specific variables, threat to self, motivational and volitional factors.
Threat-to-self moderators include problems with social problem solving, over-general autobiographical memory, and brooding rumination. These threat-to-self moderators influence perceptions of entrapment following defeat. Motivational moderators are factors that change the likelihood that the experience of entrapment will escalate into suicidal ideation and intent. Examples include lack of future thinking, lack of goal re-engagement (redirecting attention to a new goal in the presence of failure to achieve a current goal), and social disconnection, which are theorized to be largely independent of mood state. Finally, volitional moderators are factors presumed to result in the transition from suicidal ideation to suicidal behavior. Examples of volitional moderators include access to lethal means, suicide plans, exposure to suicide in the social network, acquired capability for suicide (from the Interpersonal Theory of Suicide, physical pain sensitivity and fearlessness about death), mental imagery about suicide, impulsivity, and prior suicidal behavior.
Integrated Motivational-Volitional Model of Suicidal Behaviour and PTSD
According to the Integrated Motivational-Volitional Model of Suicidal Behaviour, traumatic experiences are critical life events that characterize the pre-motivational phase (e.g., the context in which suicidal thinking might emerge). In addition, as described in the Cognitive Model of Suicidal Behavior section, individuals with PTSD have a tendency toward elevations in perfectionism, consistent with pre-motivational phase of the Integrated Motivational-Volitional Model of Suicidal Behaviour (Egan et al., 2014).
In terms of the motivational phase of the model, suicidal thinking is conceptualized to emerge when an individual experiences defeat or humiliation. Individuals with PTSD often struggle with strong emotions of shame and humiliation (Leskela et al., 2002). Additionally, individuals with PTSD often report elevations in the perception of defeat (Panagioti, Gooding, Taylor, et al., 2012). According to the Integrated Motivational-Volitional Model, defeat and humiliation lead to entrapment, which is also often elevated among individuals with PTSD (Panagioti et al., 2013). Defeat and entrapment are significantly associated with suicidal behavior among individuals with PTSD (Panagioti, Gooding, & Tarrier, 2012). Furthermore, perceptions of defeat and entrapment mediate the relationship between PTSD symptom severity and suicidal behavior in patients with PTSD (Panagioti et al., 2013). As described above (Cognitive Model of Suicidal Behavior), individuals with PTSD are more likely to demonstrate deficits in social problem solving (Sutherland & Bryant, 2008), a purported threat-to-self moderator of the association between defeat and entrapment, compared to healthy controls. Also, as described above, individuals with PTSD exhibit over-general autobiographical memories compared to healthy controls (Brown et al., 2013). There is some evidence that deficits in social problem solving in patients with PTSD are associated with overgeneralized autobiographical memories (Sutherland & Bryant, 2008). Furthermore, individuals with PTSD have memory biases toward negative memories and away from positive memories (Contractor et al., 2018), another purported threat-to-self moderator.
In terms of motivational moderators that may lead to the development of suicidal ideation from feelings of entrapment, individuals with PTSD tend to report a lack of future orientation. While this was included as a criterion of PTSD in prior versions of the DSM, it is no longer explicitly mentioned and may instead be reflected as part of the negative cognition symptom cluster. However, recent research suggests that individuals with PTSD tend to have over-general future thinking compared to healthy controls, which is associated with appraisals of foreshortened future (Brown et al., 2013; Kleim et al., 2014). As described above, individuals with PTSD are also more likely to report feelings of social disconnection compared to the general population (Laffaye et al., 2008).
Finally, in terms of volitional moderators, several of these moderators were discussed under the Interpersonal Theory for Suicide and PTSD section above, including acquired capability factors. The chronic state of hypervigilance that often characterizes PTSD may lead an individual to alter their environment such that they have easier access to lethal means for suicide. For instance, if an individual feels that the world is unsafe, they may be more likely to purchase a firearm to protect their home. When in a suicidal crisis, easy access to a firearm may significantly increase the likelihood of engaging in suicidal behavior (Conwell et al., 2002). In addition, exposure to the suicide of a family member or friend can lead to the development of PTSD (Brent et al., 1996). Veterans with PTSD tend to engage in more impulsive behaviors than healthy controls (James et al., 2014). Some research suggests that impulsivity is a consequence of exposure to trauma and a key mediator of the association between PTSD and suicidal behavior, especially in the context of poor cognitive control and emotional reactivity (Braquehais et al., 2010). In fact, Bernanke et al. (2017) proposed that individuals with exposure to childhood trauma were more likely to engage in impulsive suicidal behavior. Given that individuals with PTSD are more likely to have a history of suicidal behavior compared to the general population (Brown et al., 2016), prior suicidal behavior is another notable volitional moderator. While there is a robust body of literature demonstrating alterations in mental imagery to trauma-focused cues among patients with PTSD (Brown et al., 2018b), mental imagery to suicidal cues has not been explored in the literature.
Theoretical Correlates of PTSD and Suicide from the Integrated Motivational-Volitional Model of Suicidal Behaviour
A refinement of the Integrated Motivational-Volitional model (O’Connor & Kirtley, 2018) specified the cyclical and dynamic nature of suicidal thoughts and behaviors, such that suicide risk is non-linear. Furthermore, individuals with a history of suicidal behavior are conceptualized to have more severe levels of motivational moderators and volitional moderators. Finally, the theory indicates that the transition from suicidal ideation to suicidal behavior may become quicker following increasing instances of suicidal behavior.
As described above, individuals with PTSD are more likely to have a history of prior suicidal behavior (Brown et al., 2016), in addition to motivational moderators (e.g., lack of future orientation and social disconnection) and volitional moderators (e.g., acquired capability, access to lethal means, history of suicide in social network, and impulsivity) described in this model. These theoretical links lead us to propose each of these as possible mechanisms of the transition from PTSD and suicidal behaviors, in addition to the shared factors in the pre-motivational and motivational phases of this model: perfectionism, feelings of entrapment (shame/humiliation), over-general autobiographical memory, executive functioning deficits (e.g., over-general future thinking), social disconnection, acquired capability, access to lethal means (e.g., firearms), history of suicide in social network (e.g., family history of suicide), and impulsivity.
Three-Step Theory of Suicide (3ST)
Like the Interpersonal Theory of Suicide, the Three-Step Theory of Suicide (Klonsky & May, 2015), was developed as a theory rooted in understanding the ideation-to-action dimension of suicidal thoughts and behaviors. The first step of the Three-Step Theory requires that an individual experiences pain (typically but not exclusively emotional pain), which is a necessary but insufficient condition for the development of suicidal ideation. Klonsky and May (2015) provided numerous examples of pain that may instigate suicidal ideation, including social isolation, physical suffering, negative self-perceptions, and defeat or entrapment. In order for the experience of pain to translate into suicidal ideation, the Three-Step Theory hypothesized that an individual must experience hopelessness about their pain. The second step of the Three-Step Theory is that a person experiences stronger suicidal ideation (as opposed to moderate suicidal ideation) if they are connected, defined broadly and including social connection but also connection to work, hobbies or some other critical domain. The third step of the Three-Step Theory postulates that the development of suicidal behavior is based on a variety of dispositional, acquired, and practical factors. Dispositional factors include genetic and physiological factors. Acquired factors include habituation to physical pain and fear of death. Practical factors include concrete factors associated with suicidal behavior, such as access to lethal means.
Three-Step Theory and PTSD
The experience of PTSD is often emotionally, and sometimes physically, painful. Individuals with PTSD report struggling with chronic negative emotions including fear, shame, guilt, sadness, and anger (American Psychiatric Association, 2013). PTSD is characterized by frequent bouts of strong negative emotional reactions to reminders of the trauma, often coupled with physiological sensations that accompany these emotional reactions. Similarly, many individuals with PTSD have heightened startle reactivity (Glenn et al., 2016) and report an inability to relax, a deeply painful cognitive state. Additionally, as described in two sections above, individuals with PTSD are significantly more likely to report chronic pain and to have medical diagnoses compared to individuals without PTSD.
As discussed in relation to earlier theories, hopelessness-related cognitions about pain are also characteristic of PTSD. Individuals with PTSD will commonly report cognitions such as “I will not be able to control my anger and will do something terrible”, “I will never be able to feel normal emotions again”, and “I have permanently changed for the worse” (Foa et al., 1999). The perception of hopelessness about the pain caused by the trauma is one factor that often delays or prevents treatment-seeking, as some patients with PTSD are skeptical that their life can improve or that treatment can be useful, which reduces the benefit of treatment (Ehlers et al., 1998). Therefore, not only is hopelessness about pain a likely contributor to suicidal ideation among individuals with PTSD, but it may also prevent them from receiving evidence-based treatment to reduce their pain.
Connection is often challenging for patients with PTSD. First, patients with PTSD commonly report feeling disconnected from others (American Psychiatric Association, 2013). Some patients describe their disconnection as though there is a wall between them and the world that prevents them from intimate closeness. Some individuals with PTSD report a desire, but inability, to connect with other people. Others with PTSD report a reluctance to build closeness due to negative cognitions about the world and people in general. Individuals with PTSD also struggle with low interest in previously enjoyed activities. Whereas hobbies or a career may have been a former source of connection to the world, some individuals with PTSD report reduced motivation to engage in these activities. This loss of interest contributes to them feeling more disconnected from the world. Finally, an impaired ability to experience positive emotions, such as joy, humor, or love, contribute to further disconnection for many individuals with PTSD (American Psychiatric Association, 2013). The combination of these challenges with connection likely precipitates increased severity of suicidal ideation.
The experience of trauma and the development of PTSD can alter one’s biological reactivity, an indication of a dispositional risk factor for suicidal behavior. For instance, some individuals with PTSD report enhanced physiological reactivity to trauma-related cues, including skin conductance response, heart rate, and electromyography startle response (d’Andrea et al., 2013; Glenn et al., 2016). As mentioned in the Interpersonal Theory of Suicide section above, physiological blunting often occurs among patients with the most severe PTSD (d’Andrea et al., 2013). This physiological blunting is consistent with the dissociative presentation of PTSD and may represent a dispositional risk factor for suicidal behavior. In other words, if an individual is less likely to experience fear in circumstances where fear is biologically adaptive, that blunted response may translate into less physiological reactivity to a life-threatening scenario, leading to more lethal suicidal behavior. Similarly blunted physiological responding has also been observed among patients with PTSD along the hypothalamic-pituitary-adrenal (HPA) axis (Ströhle et al., 2008). Blunted HPA axis activity is, in turn, associated with suicidal behavior (Melhem et al., 2016).
In terms of acquired factors, as described in response to the Interpersonal Theory of Suicide, trauma-exposure often includes exposure to actual or threatened death or physical injury. Most individuals who develop PTSD have been exposed to more than one traumatic event, and exposure to multiple traumas is associated with higher PTSD severity (Kilpatrick et al., 2013). It is possible that exposure to violent acts promotes habituation to pain and to the fear of death. Therefore, exposure to trauma alone may be sufficient to meet criteria for acquired factors that precipitate suicidal behavior.
Finally, as described above under the Integrated Motivational-Volitional Model of Suicidal Behaviour, the chronic state of hypervigilance that often characterizes PTSD may lead an individual to alter their environment such that they have easier access to lethal means for suicide, consistent with the practical factors component of the Three-Step Theory. Similarly, if an individual with PTSD feels that they cannot trust others, they may be more likely to live alone, which is an independent risk for suicidal behavior (Heikkinen et al., 1993). As described above, individuals with PTSD are already more likely to engage in impulsive behaviors than the general population, such as reckless driving, promiscuous sex, or being in unsafe situations. These behaviors may also promote access to practical factors that make it easier to engage in suicidal behaviors.
Theoretical Correlates of PTSD and Suicide from the Three-Step Theory of Suicide
As described above, individuals with PTSD are more likely to experience physical and emotional pain, as well as hopelessness-related cognitions about their pain, which is an essential factor for developing suicidal ideation in the Three-Step Theory. Additionally, those with PTSD are likely to experience connection-interfering factors (particularly social connection disruptions) that lead individuals to transition to severe ideation in step two of this model and acquired factors and access to lethal means, which increase their vulnerability to engage in suicidal behavior as described in the third transition of this model. These theoretical links lead us to propose each of these as possible mechanisms of the transition from PTSD to suicidal ideation and behaviors: physical pain, painful emotions (shame/guilt), negative cognitions (particularly hopelessness-related ones), social disconnection, acquired capability, and access to lethal means (e.g., firearms).
Diathesis Stress Model of Suicide
The Diathesis Stress Model of Suicide (also called the stress-diathesis theory of suicide; Mann et al., 1999; Mann & Arango, 1992; Rubinstein, 1986) suggests that an individual’s genetics and biological make-up can confer increased risk for suicide, especially under the context of life stressors and other states. According to one version of the model (Mann et al., 1999), low serotonergic activity is thought to interact with other subjective states (e.g., hopelessness-related cognitions, mental pain, suicide-related cognitions) to increase risk. Low serotonergic activity is also thought to directly impact executive function/impulsivity, which is hypothesized to have direct effects on suicidal behavior and aggression. Executive dysfunction is simultaneously impacted by states including hopelessness, suicidal ideation, and suicide planning. The entire system is thought to be impacted by life events, which are thought to increase hopelessness and suicidal ideation, with downstream effects on suicidal planning, executive dysfunction, and suicidal behavior.
Diathesis Stress Model of Suicide and PTSD
According to the Diathesis Stress Model, exposure to a traumatic event may increase hopelessness and suicidal ideation among individuals who are at a biological risk for these outcomes. Suicidal ideation may increase the risk for suicidal planning. As described above, individuals with PTSD are at higher risk for impulsivity, which may increase the risk for suicidal behavior according to this model.
Theoretical Correlates of PTSD and Suicide from the Diathesis Stress Model of Suicide
These theoretical links lead us to propose each of these as possible correlates of the transition from PTSD to suicidal ideation and planning: negative cognitions (particularly hopelessness-related ones) and executive dysfunction/impulsivity.
Escape Theory of Suicide
Similar to the diathesis stress model of suicide, in the escape theory of suicide (Baechler, 1980; Baumeister, 1990), a decision-tree approach to predicting suicidal behavior was hypothesized. First, the theory supposes that a suicidal crisis is initiated by high expectations or standards coupled with an experience of stress or failure in which expectations are not met. In contrast, instances of low expectations are perceived as less likely to initiate a suicidal crisis. Second, in circumstances in which a stressful experience or failure occurs in the face of high expectations, a suicidal crisis may escalate when an individual makes internal attributions about the source of the stressor or failure. Self-blame is an example of an internal attribution for a stressor or failure that may contribute to a suicidal crisis. Third, the individual has awareness of the discrepancy between their performance and their ideal performance, thus contributing to global interpretations of inadequacy, incompetence, or unattractiveness. Fourth, negative emotions are experienced in response to categorizing oneself in a negative manner. Fifth, the onset of negative emotions instantiates a desire to escape from the experience, which an individual attempts to achieve through an absence of meaningful thought or cognitive numbing, termed “cognitive deconstruction.” This cognitive deconstruction may serve the function of avoiding thinking about a painful future. Finally, this state of cognitive numbing is hypothesized to reduce inhibition, which is thought to increase willingness to engage in suicidal behavior.
PTSD and the Escape Theory
According to the Escape Theory, the experience of trauma might constitute a relevant stressor that violates expectancies about the future. An individual with PTSD may attribute their own behavior as a cause for the trauma, as was discussed in early sections about trauma-related negative cognitions about the self (see Interpersonal Theory and Cognitive Model). Similarly, individuals with PTSD may begin to perceive that they are incompetent or inadequate, which are common trauma-related cognitions. As described in sections above, these cognitions are known to drive negative affect within individuals with PTSD, such as increased feelings of guilt and shame. The aversive experience of negative affect and trauma-related cognitions may contribute to executive functioning deficits in patients with PTSD. As described above, impulsivity and executive functioning challenges in PTSD, including mind wandering, are relevant possible risk factors for suicide.
Theoretical Correlates of PTSD and Suicide from the Escape Theory of Suicide
These theoretical links lead us to propose each of these as possible mechanisms of the transition from PTSD to suicidal ideation and behavior: negative cognitions about the self, self-blame-related emotions (e.g., guilt and shame), and executive functioning deficits.
Cry of Pain Model
The Cry of Pain model (Bolton et al., 2007; Williams, 1997; Williams et al., 2005) was developed in response to characterizations of suicide attempts and suicide death as a “cry for help.” In contrast, the Cry of Pain model principally suggests that suicidal behavior is predicted when a person feels entrapped and helpless in the face of actual or threatened loss.
Some predictors of entrapment come from long-term vulnerability factors, including past events, current relationships, and living conditions. Entrapment is viewed as likely to emerge under conditions of chronic stress, such as among individuals who are chronically bullied or in domestic violence relationships. According to this theory, an individual may have been raised in a situation where they had little control over their environment; lack of control may cause the person to engage in submissive behaviors, consistent with learned helplessness. Being in a chronically submissive position fosters heightened sensitivity to social threats as well as perceptions of low self-regard, sometimes to the point of seeing oneself as worthless. In addition, low ability to recall specific details of positive memories is conceptualized as a predictor of suicidal thinking, a concept referred to a “mnemonic interlock” and conceptually similar to the over-general memory referenced in other theories above (see Integrated Motivational-Volitional Model of Suicidal Behaviour and Cognitive Model of Suicidal Behavior).
Examples of living situations that may increase risk include a history of being in care (e.g., foster care, juvenile justice, etc.) or living with only one caregiver. The model suggests that parenting style plays an important role, with a parenting style that combines rejecting and overprotective tendencies as the riskiest profile as these reduce one’s sense of being in control. The theory points to sexual abuse as a particularly relevant risk factor because of its impact on relationship functioning, sense of life fulfillment, and learned helplessness. Individuals who perceive stressful events as stable and global (i.e., impacting all areas of life) are most likely to struggle with suicidal thoughts. Additionally, the Cry of Pain model suggests that individuals at risk for suicide have short-term vulnerability factors, including more frequent stressful life events, interpersonal discord, work difficulties, and physical illness. Some of these short-term vulnerability factors are thought to reduce perceived ability to cope with stress and to directly precipitate a suicidal crisis. Additionally, the Cry of Pain model suggests that individuals who are at risk for suicide are more likely to have a foreshortened sense of the future, including a reduced ability to elaborate on their future plans, consistent with the Escape Theory’s sense of “cognitive deconstruction.” Specifically, this theory suggests that individuals who are at risk for suicide have a difficult time identifying future positive events, consistent with hopelessness. This inability to anticipate positive future events is thought to be one reason why individuals who are at risk for suicide report fewer reasons for living. According to the Cry of Pain model, individuals who make suicide attempts report more hostility, whereas individuals who die by suicide appear more apathetic, which is conceptualized to reflect an inability to regulate emotional pain. Finally, the Cry of Pain model points to the importance of access to lethal means as a predictor of suicidal behavior.
Cry of Pain Model and PTSD
Past traumatic experiences may operate as long-term vulnerability factors for feeling entrapped, which is exacerbated by recent stressors or traumas. Exposure to situations in which an individual is chronically abused or maltreated results in accurate perceptions of being trapped. Among individuals with PTSD, this sense of entrapment may continue well beyond the trauma duration, consistent with learned helplessness (Seligman, 1972). Entrapment may be exacerbated among individuals with PTSD who were raised in households in which their autonomy was reduced by overprotective parenting. Similarly, being raised in a household with a combination of a rejecting style (for instance, a parent who abuses their child) and overprotection in other domains may result in significant confusion about autonomy and may enhance the sense of lack of control over their environment. It is common for individuals with PTSD to report negative cognitions related to defeat (“the event happened to me because of the sort of person I am”) and entrapment (e.g., “I can’t stop bad things from happening to me”). Similarly, family history of suicide may constitute a traumatic experience that also increases risk in this model. According to this theory, over-general memory is an indication that traumatic events have been insufficiently processed, as discussed above.
Theoretical Correlates of PTSD and Suicide from the Cry of Pain Model
These theoretical links lead us to propose each of these as possible mechanisms of the transition from PTSD to suicidal ideation and behaviors: feelings of entrapment (shame/guilt), negative cognitions (particularly about the self), over-general memory, and a family history of suicide.
Schematic Appraisals Model
The Schematic Appraisal Model (Johnson et al., 2008) was developed as an extension of the Cry of Pain Model. According to the Schematic Appraisal Model, information processing biases in attention, memory and reasoning drive suicide schema. These suicide schemas are thought to have a mutually influential relationship on self-appraisals, including self-esteem, personal agency, “rescue” factors (e.g., social support availability, social support importance), and evaluation of cognitive abilities. Suicide schemas are also thought to influence the appraisal system, including appraisals of the current situation (including stressors), historical factors, and of the future. The appraisal system is also influenced by self-appraisals. The constellation of negative appraisals about the self, other people, the current situation, historical factors, and the future are all hypothesized to increase perceptions of defeat and entrapment.
Schematic Appraisals Model and PTSD
A history of repeated or isolated traumatic events are relevant historical factors that may increase risk for suicide by their capacity to bias the appraisal system. As was discussed above, individuals with PTSD tend to struggle with problem solving deficits, which impacts their appraisal of the future. They also tend to appraise the future more negatively and to report more hopelessness than individuals without PTSD. According to the Schematic Appraisals Model, hopelessness about the future may lead an individual with PTSD to perceive that they have no alternative other than to escape by dying by suicide. In terms of their self-appraisals, as has been discussed above, individuals with PTSD tend to report lower self-esteem, more negative self-image, and more negative expectations of others than individuals without PTSD, all of which are associated with suicidal thoughts. These negative appraisals may increase perceptions of defeat and entrapment, which may be amplified by appraisals that an individual is defeated by their PTSD symptoms. According to this model, as an individual with PTSD gains more agency over their life and greater perceptions of external agency (especially social support), their perception of defeat and entrapment will be reduced, which will reduce suicidal thoughts.
Theoretical Correlates of PTSD and Suicide from the Schematic Appraisals Model
These theoretical links lead us to propose each of these as possible mechanisms of the transition from PTSD to suicidal ideation and behaviors: negative cognitions about the self, others, and the future, and executive functioning deficits.
Summary
These nine theories offer important hypotheses about how PTSD may increase risk for suicidal thoughts and behaviors. In these meta-analyses, core tenets of these nine theories were evaluated for their relative association to trauma exposure, PTSD, suicidal thoughts and suicidal behaviors. After conducting a comprehensive search of available databases, articles which included evaluations of PTSD, core tenants of these nine theories, and suicide-related outcomes were evaluated. Each is presented in separate meta-analyses by construct to allow for an understanding of the relative importance of each of these tenets on associations between PTSD and suicide risk. These findings offer insights into possible mechanisms of action underlying the association between PTSD and suicide risk, and are distilled into a unifying model, “CEASE.”
Methods
When this project was originally conceived, it was intended to focus on a conceptual overview of theories of suicidal ideation and attempts and their relevance to understanding PTSD-related risk-factors for suicide. Throughout the project, the scope evolved to include meta-analyses. Given the evolution of the project, it was not pre-registered, and when the project shifted into a meta-analysis, several searches had already commenced. However, each of the other 26 steps of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting standards were followed.
Inclusion criteria were: (1) an empirical evaluation of theories on suicidal thoughts or behaviors among patients with PTSD or the effect of PTSD symptoms in non-clinical samples listed in nine key theories on suicidal thoughts and behaviors; (2) inclusion of a measure of PTSD symptom severity or trauma exposure; (3) inclusion of a measure of correlates of the association between PTSD and suicidal thoughts and behaviors, including: negative cognitions about the self, the world or other people; perfectionism/cognitive inflexibility; aggression/hostility; guilt/shame; memory issues; executive functioning deficits/impulsivity; distress tolerance; acquired capability; pain-related conditions; family history of suicide; altered social/interpersonal connections; and firearm ownership. Based on our searches, we added secondary analyses focused on self-harm and risk-taking behaviors given that numerous papers included these specific factors for further analysis.
Search Terms
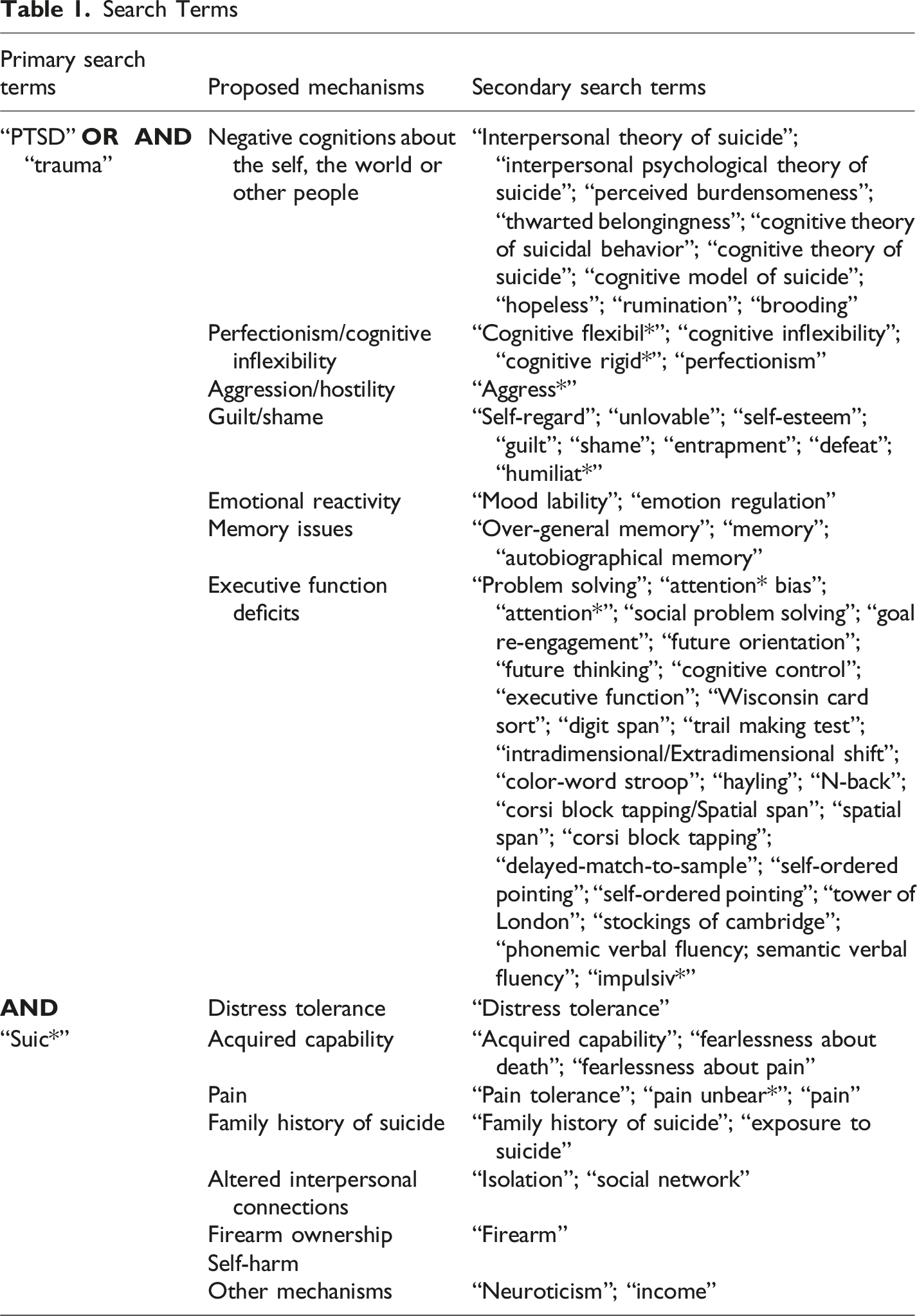
This search resulted in 5,290 articles, 191 of which (N = 79,106) had sufficient information for inclusion in the meta-analyses (see Figure 1). A full table of extracted articles is available on the Open Science Framework (https://osf.io/gvpba/overview?view_only=ba67f05a94ed4678bbbf4eb01940c36d). Two authors independently reviewed all possible articles for determination about appropriateness for inclusion and to rate possible sources of bias in the articles. Discrepancies in decisions about inclusion or bias were resolved through consensus meetings with the two coders. Some articles did not sufficiently report statistical values for inclusion in the meta-analysis. The corresponding authors for all such articles were contacted to request data for inclusion in the meta-analysis. PRISMA 2020 flow diagram for new systematic reviews.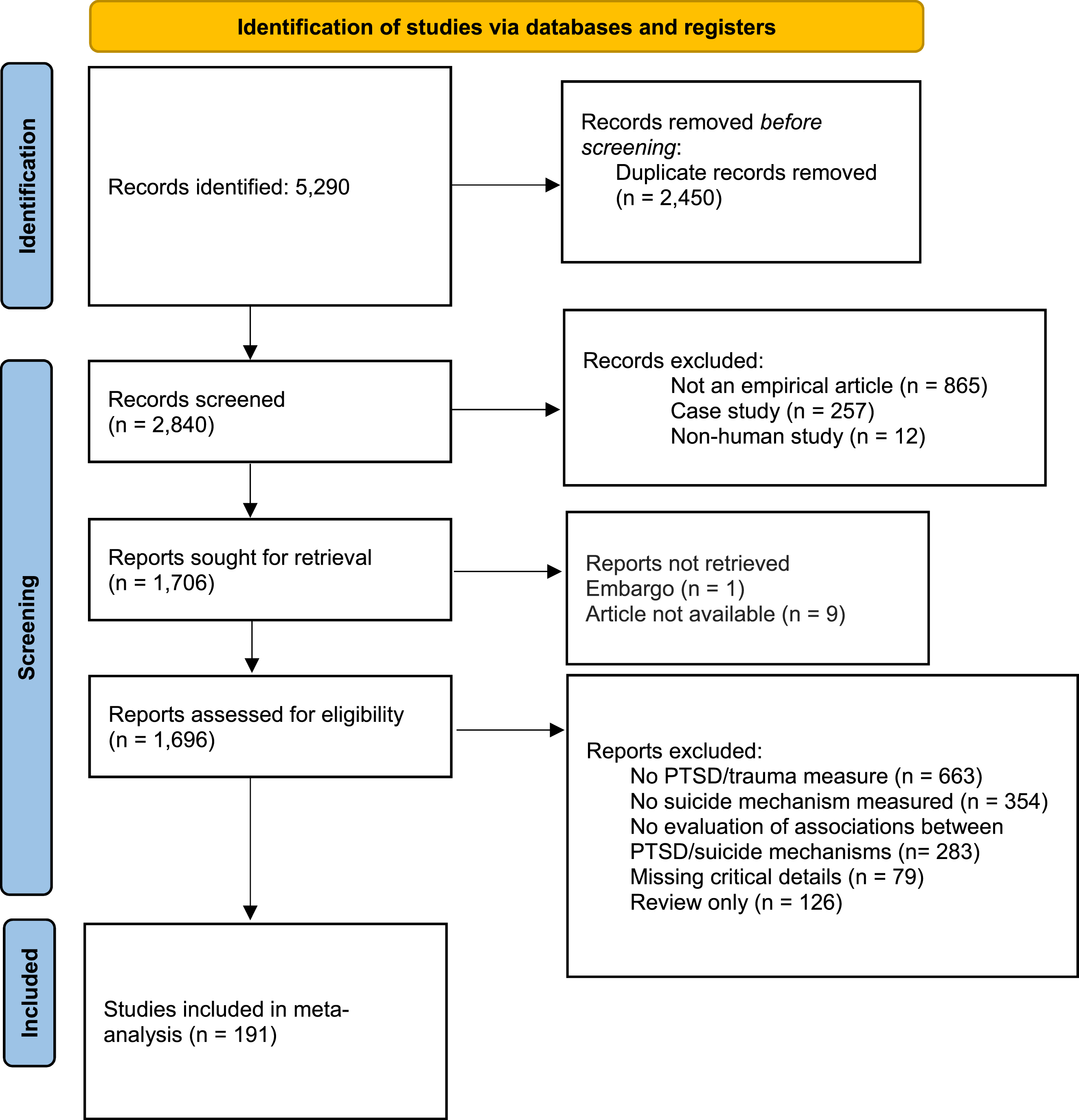
Meta-Analyses
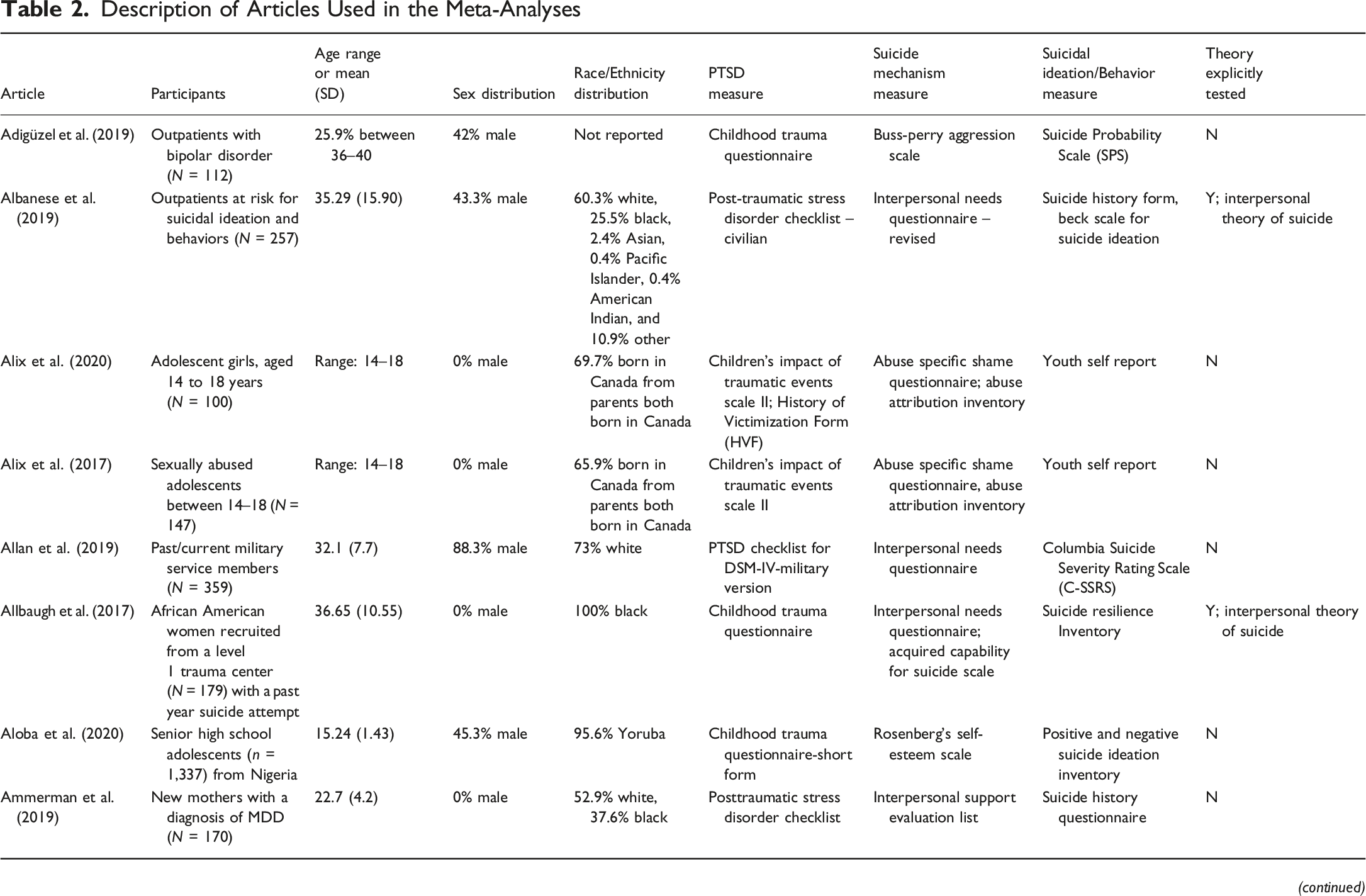
Description of Articles Used in the Meta-Analyses
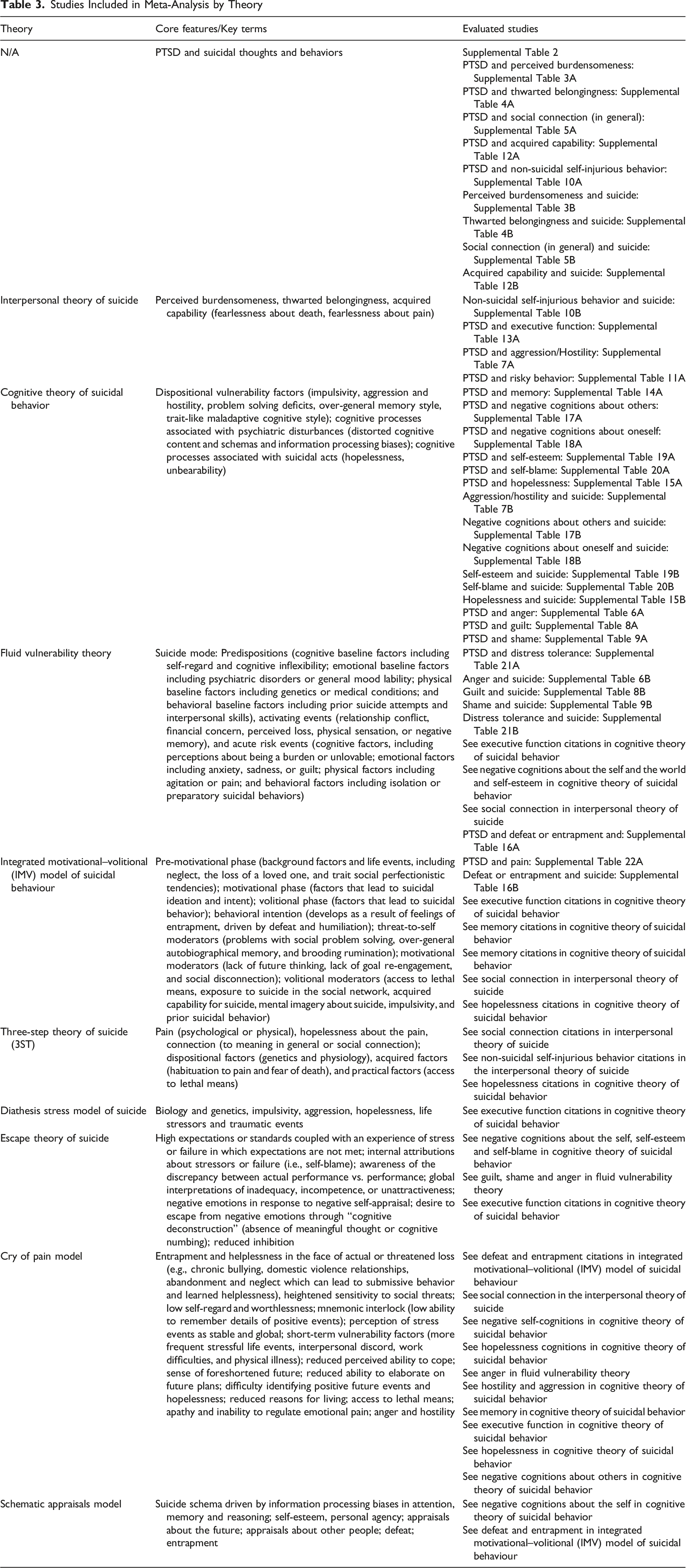
Studies Included in Meta-Analysis by Theory
Summary of random effects from meta-analysis
Effect sizes were calculated using correlation value (r), which reflects the strength and direction (positive or negative) of the association between the predictor (either PTSD or the suicide mechanism) and the outcome (either the suicide mechanism or the suicidal thoughts or behaviors variable). Given that we only included studies that directly reported a correlation value, no transformations of effect-sizes were required. In studies that offer multiple effect size estimates (either due to a longitudinal design or because different outcomes related to a construct of interest were reported), it is ideal to record all possible effect sizes to offer a complete report. When a clinician-rated measure overlapped with a self-report measure of the same construct, only the clinician-rated measure was retained. When a total score was included along with subscales that were subsumed within a given construct (e.g., subscale scores for PTSD symptom clusters presented alongside PTSD total scores), only the total scores were included. To avoid violating the independence assumption, we followed standard recommendations to aggregate effect sizes (Borenstein et al., 2009; Rosenthal & Rubin, 1986). For studies with multiple subgroups, the subgroup was selected as the unit of analysis. For studies with multiple outcomes within a subgroup, the outcomes were combined for analysis within a subgroup of a study. To evaluate between-study heterogeneity, we reported Cochran’s Q and I2 and calculated a 95% CI around I2.
Transparency and Openness
All Comprehensive Meta-Analysis files were uploaded for review and are available for additional analyses.
Risk of Bias Assessment
Following established procedures (Jennissen et al., 2018; Ross et al., 2011), risk of bias was calculated using a 16-item scale that assesses the sample, measures, psychometric property of measures, timing of assessments, clarity of reporting and selective reporting (Appendix 1). Items were scored using a 0 (no risk of bias), 1 (unclear risk of bias), 2 (definite risk of bias), or not applicable. Then, a ratio was calculated whereby the number of unclear or definite bias items was divided by the number of applicable items, resulting in a value ranging from 0 (low bias) to 1 (high bias).
All articles included in the meta-analysis were coded by both authors. Following preliminary scores, interrater reliability was calculated and was perfect for two items (items 4, 8), substantial for five items (item 6, 7, 9, 12, 14), moderate for four items (item 3, 5, 10, 11), fair for two items (item 1, 13), and low for three items (items 2, 15, and 16). All discrepancies were resolved through discussion until complete consensus was reached. Bias scores are reported in Supplemental Table 1.
Results
PTSD and Suicide Risk
Across 106 studies (N = 41,924) that evaluated associations between PTSD and suicidal thoughts or suicidal behaviors, there was a significant random effect (r = .300, CI95% .275, .324, p < .001) of PTSD on suicidal thoughts and behaviors (Q = 1,002.664, I2 = 89.528 [CI95%: 87.884, 90.949], p < .001, Τ2 = .016, SE = .004, df = 109; Supplemental Table 2). Given that heterogeneity was so large, a series of sensitivity analyses were run to determine the source of heterogeneity.
The funnel plot of standard error by Fisher’s Z is reported in Figure 3. Duval and Tweedie’s (2000) trim-and-fill technique was used to evaluate the presence of extreme observations for potential trimming and imputation. Zero were detected to the right of the mean, and 13 studies were trimmed to the left of the mean, but the random effect point estimate was not meaningfully altered (r = .262, CI95% .234, .291). Funnel plot for PTSD and suicidal thoughts and behaviors meta-analysis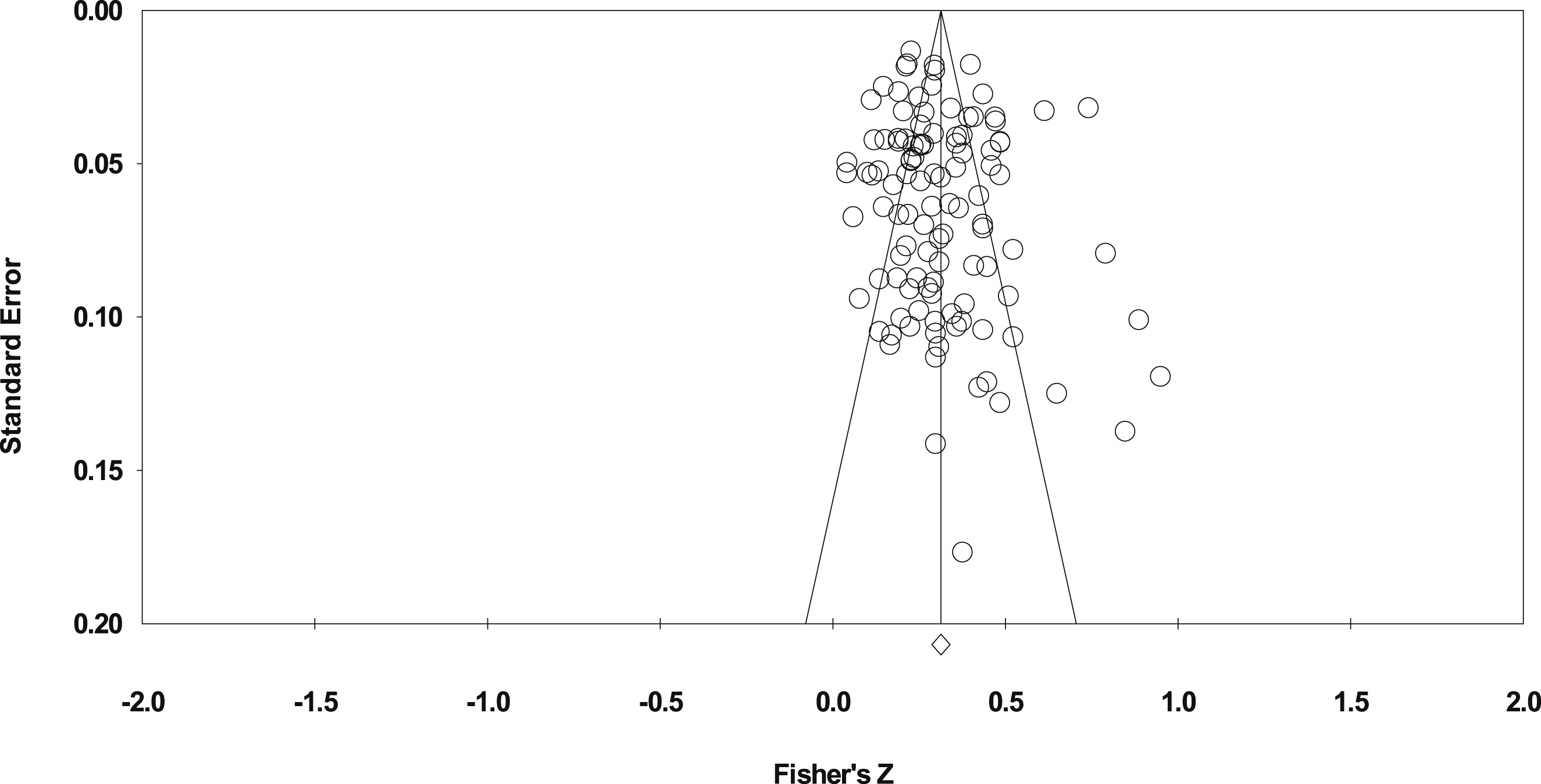
Sensitivity Analyses
This sensitivity analysis was conducted cumulatively removing variables that could contribute to heterogeneity using 20 different steps, including: (1) removing multiple time-points, and always using the first time-point where possible; (2) remove non-clinical samples; (3) remove all PTSD subscales when a PTSD total score was available; (4) for studies that had a straightforward PTSD measure plus a “back-up” measure (e.g., exposure to sexual assault), remove the back-up measure; (5) for studies with multiple suicide-related outcomes, if one was less commonly used (e.g., suicide probability scale), remove the less commonly used measure; (6) separate suicide ideation from attempts where possible; (7) in situations where a study had two samples (both of which were clinical), remove the one with a smaller sample size; (8) for the C-SSRS, remove the Intensity of Ideation subscale given psychometric work that shows that this subscale has less than ideal performance (Brown et al., 2020a); (9) removed the Positive and Negative Suicide Ideation Scale; (10) removed measures that were developed exclusively for the study; (11) removed instances of neglect when abuse variables were present; (12) removed child studies; (13) removed studies that used the Suicide Resilience Inventory; (14) deleted studies that only included PTSD subscales in the absence of a total PTSD score; (15) deleted suicide plan outcomes; (16) in situations where the Beck Scale for Suicide Ideation (BSS) was included along with other measures, retain only the BSS; (17) removed any PTSD measure that was included less than 3 times; (18) deleted any suicide outcome that was included less than 3 times; and (19) removed any study that did not use the Posttraumatic Diagnostic Scale, Clinician-Administered PTSD Scale, or PTSD Checklist for PTSD severity. Heterogeneity as well as the random effect sizes were explored at each step in the sensitivity analyses. While heterogeneity was substantially reduced in terms of the Q value (489.257) in the remaining 33 study, I2 remained high (93.459, CI95%: 91.78, 94.80), and the association between PTSD and suicidal thoughts and behavior was not meaningfully changed (random effect: r = .338, CI95% .275, .398, p < .001).
Interpersonal Connection
Perceived Burdensomeness: Meta-Analysis
Across 37 studies (N = 12,404) that evaluated perceived burdensomeness, there was a significant effect (r = .375, CI95% .309, .437, p < .001) of PTSD on perceived burdensomeness (Q = 938.892, I2 = 96.166 [CI95%: 95.395, 96.807], p < .001, Τ2 = .049, SE = .020, df = 36; Supplemental Table 3A, Supplemental Figure 1). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left or right of the mean.
Across 28 studies (N = 10,170) that evaluated perceived burdensomeness, there was a significant random effect (r = .412, CI95% .354, .468, p < .001) of perceived burdensomeness on suicidal ideation (Q = 315.699, I2 = 91.448 [CI95%: 88.796, 93.471], p < .001, Τ2 = .030, SE = .011, df = 27; Supplemental Table 3B, Supplemental Figure 2). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left of the mean and 1 to the right of the mean but the random effect point estimate was not meaningfully altered (r = .420 CI95%. .362, .476).
Thwarted Belongingness: Meta-Analysis
Across 36 studies (N = 15,293) that evaluated thwarted belongingness, there was a significant random effect (r = .356, CI95% .271, .436, p < .001) of PTSD on thwarted belongingness (Q = 1,715.422, I2 = 97.960, [CI95%: 97.625, 98.247], p < .001, Τ2 = .080, SE = .033, df = 35; Supplemental Table 4A, Supplemental Figure 3). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left or right of the mean.
Across 27 studies (N = 13,059) that evaluated thwarted belongingness, there was a significant random effect (r = .294, CI95% .239, .348, p < .001) of thwarted belongingness on suicidal ideation and behavior (Q = 276.736, I2 = 90.605 [CI95%: 87.532, 92.920], p < .001, Τ2 = .021, SE = .009, df = 26; Supplemental Table 4B; Supplemental Figure 4). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left of the mean or right of the mean.
All Other Social Variables (Reported in Figure 2): Meta-Analysis
When all other social variables were combined (e.g., abandonment, alienation, family stress, parental rejection, loneliness, social connection, social constraints), across 44 studies (N = 14,774) that evaluated social support there was a significant random effect (r = .278, CI95% .238, .317, p < .001) of PTSD on social support (Q = 267.660, I2 = 83.935 [CI95%: 79.216, 87.582], p < .001, Τ2 = .015, SE = .006, df = 43; Supplemental Table 5A, Supplemental Figure 5). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 7 outliers to the left of the mean, but the random effect point estimate was not meaningfully altered (r = .245, CI95% .204, .285).
Across 26 studies (N = 10,250), there was a significant effect (r = .232, CI95% .185, .279, p < .001) of social support on suicidal ideation and behavior (Q = 225.723, I2 = 88.924 [CI95%: 85.009, 91.817], p < .001, Τ2 = .012, SE = .007, df = 25; Supplemental Table 5B, Supplemental Figure 6). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left or right of the mean.
Anger: Meta-Analysis
Across 9 studies (N = 4,996) that evaluated anger (including anger, anger control, frustration and irritability), there was a significant random effect (r = .380, CI95%: .251, .496, p < .001) of PTSD on anger (Q = 364.628, I2 = 97.806 [CI95% 96.968, 98.413], p < .001, Τ2 = .046, SE = .032, df = 8; Supplemental Table 6A, Supplemental Figure 7). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left of the mean and 1 outlier to the left of the mean, but the random effect point estimate was not meaningfully altered (r = .403, CI95% .282, .512).
Across 7 studies (N = 3,076), there was a significant random effect (r = .342, CI95%: .279, .401, p < .001) of anger on suicidal thoughts and behaviors (Q = 21.846, I2 = 72.535 [CI95%: 40.737, 87.272], p < .001, Τ2 = .006, SE = .005, df = 6; Supplemental Table 6B, Supplemental Figure 8). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left or right of the mean.
Aggression and Hostility: Meta-Analysis
Across 27 studies (N = 11,135), there was a significant random effect of PTSD on aggression/hostility (r = .325, CI95%: .272, .375, p < .001; Q = 495.442, I2 = 94.752 [CI95%: 93.346, 95.861], p < .001, Τ2 = .020, SE = .008, df = 26; Supplemental Table 7A, Supplemental Figure 9). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left of the mean and 7 outliers to the right of the mean, but the random effect point estimate was unchanged (r = .379, CI95% .319, .436).
Across 10 studies (N = 3,743), there was a significant random effect of aggression/hostility on suicidal thoughts and behaviors (r = .354, CI95%: .251, .450, p < .001; Q = 115.692, I2 = 92.221 [CI95%: 87.783, 95.047], p < .001, Τ2 = .029, SE = .019, df = 9; Supplemental Table 7B, Supplemental Figure 10). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left or the right of the mean.
Guilt: Meta-Analysis
Across 16 studies (N = 4,297), there was a significant random effect of PTSD on guilt (r = .440, CI95%: .353, .519, p < .001; Q = 180.955, I2 = 91.711 [CI95%: 88.144, 94.204], p < .001, Τ2 = .038, SE = .019, df = 15; Supplemental Table 8A, Supplemental Figure 11). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 3 outliers to the left of the mean, but the random effect point estimate was not meaningfully changed (r = .391, CI95% .299, .476).
Across 11 studies (N = 3,554), the there was a significant random effect of guilt on suicidal thoughts and behaviors was significant (r = .371, CI95% .273, .462, p < .001; Q = 141.516, I2 = 92.934 [CI95%: 89.281, 95.342], p < .001, Τ2 = .029, SE = .021, df = 10; Supplemental Table 8B, Supplemental Figure 12). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 2 outliers to the left of the mean, but the random effect point estimate was not meaningfully changed (r = .328, CI95% .234, .421).
Shame: Meta-Analysis
Across 12 studies (N = 2,305), there was a significant random effect of PTSD on shame = (r = .406, CI95% .280, .517, p < .001; Q = 162.971, I2 = 93.250 [CI95%: 90.009, 95.440], p < .001, Τ2 = .058, SE = .031, df = 11; Supplemental Table 9A, Supplemental Figure 13). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left or right of the mean.
Across 9 studies (N = 1,865), there was a significant random effect of on suicidal thoughts and behaviors in random effects (r = .365, CI95% .278, .447, p < .001; Q = 31.196, I2 = 74.356 [CI95% 50.258, 86.779], p < .001, Τ2 = .015, SE = .012, df = 8; Supplemental Table 9B, Supplemental Figure 14). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left or right of the mean.
Family History of Suicide: Meta-Analysis
There was insufficient information in the studies that evaluated PTSD, family history of suicide, and suicidal thoughts and behaviors for inclusion in the meta-analysis.
Self-Harm: Meta-Analysis
Self-harm was included as a secondary analysis given that searchers for factors related to acquired capability and lethal means revealed an opportunity to explore its effect as a correlate of PTSD and suicide risk. Across 14 studies (N = 12,974), there was a significant random effect (r = .222, CI95%: .162, .279, p < .001) of PTSD on self-harm (Q = 141.917, I 2 = 90.840 [CI95%: 86.397, 93.831], p < .001, Τ2 = .010, SE = .009, df = 13; Supplemental Table 10A, Supplemental Figure 15). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left of the mean and 3 to the right of the mean, but the random effect point estimate was not meaningfully changed (r = .222, CI95% .162, .279).
Across 6 studies (N = 1,072), there was a significant random effect (r = .255, CI95%: .190, .318, p < .001) of self-harm on suicidal thoughts and behaviors (Q = 6.130, p = .294, I2 = 18.430 [CI95%: 0.000, 63.220], Τ2 = .001, SE = .005, df = 5; Supplemental Table 10B, Supplemental Figure 16). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 3 outliers to the left of the mean, but the random effect point estimate was not meaningfully changed (r = .204, CI95% .128, .278).
Firearm Ownership: Meta-Analysis
There were insufficient studies to conduct a meta-analysis on firearm ownership and PTSD or suicidal ideation.
Risk Taking: Meta-Analysis
Risk-taking was included as a secondary analysis given that searchers for factors related to acquired capability, lethal means, and impulsivity revealed an opportunity to explore its effect as a correlate of PTSD and suicide risk. Eight studies (N = 2,072) evaluated associations between risk-taking behaviors and PTSD, with a significant random effect (r = .189, CI95%: .125, .251, p < .001; Q = 17.195, I2 = 59.292 [CI95%: 11.207, 81.336], p = .016, Τ2 = .005, SE = .005, df = 7; Supplemental Table 11A, Supplemental Figure 17). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left and 2 outliers to the right of the mean, but the random effect point estimate was not meaningfully changed (r = .217, CI95% .150, .283).
However, only two studies (with four total comparisons, N = 464; Bach & Fjeldsted, 2017; Stewart et al., 2018) evaluated associations between risk-taking behaviors and suicidal thoughts and behaviors, with associations ranging from small to medium (range r: .04–.490), though these two studies were not entered into a meta-analysis.
Acquired Capability: Meta-Analysis
In 23 studies (N = 10,052) on acquired capability (the Acquired Capability Scale, Fearlessness about Death, Fear about Suicide (reverse scored), there was a significant random effect (r = .121, CI95%: .064, .177, p < .001) of PTSD on acquired capability (Q = 333.908, I2 = 93.411 [CI95% 91.313, 95.003], p < .001, Τ2 = .017, SE = .008, df = 22; Supplemental Table 12A, Supplemental Figure 18). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left or right of the mean.
In 15 studies (N = 6,614) that evaluated associations between acquired capability and suicidal thoughts or behaviors, there was a significant random effect (r = .123 CI95% .056, .189, p < .001; Q = 96.314, I2 = 85.464 [CI95% 77.535, 90.595], p < .001, Τ2 = .014, SE = .007, df = 14; Supplemental Table 12B, Supplemental Figure 19). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 4 to the left of the mean, which substantially lowered the random effect point estimate (r = .062, CI95% −.011, .134).
Executive Function: Meta-Analysis
Executive function is often used broadly in the literature. To narrow the scope of the analyses, conventions recommended by Miyake and colleagues (2012) and used in prior meta-analytic studies on executive functioning in depression were used (Snyder, 2013). Specifically, a literature review included PTSD or trauma, suic*, and: Wisconsin Card Sorting Test (WCST); Trail Making Test; Intradimensional/Extradimensional Shift; Color-Word Stroop; Hayling; n-Back; Corsi Block Tapping/Spatial Span; Delayed-Match-to-Sample; Self-Ordered Pointing; Digit Span; Tower of London/Stockings of Cambridge; Phonemic Verbal Fluency and Semantic Verbal Fluency. However, this literature search revealed only four studies (N = 373) that included such tasks for the analyses between PTSD and executive functioning, and the association between PTSD and executive functioning was not significant (r = .000, CI95%: −0.069, 0.069, p = .996; Q = 1.829, p = .609, I2 = .000 [CI95% 0.000, 47.378], Τ2 = .000, SE = .006, df = 3; Supplemental Table 13A and Supplemental Figure 20). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 2 to the left of the mean, which lowered the random effect point estimate (r = −.016, CI95% −.081, .047).
The reduced tasks resulted in only one study (Hausman et al., 2020) that explored the associations between executive function and suicidal thoughts or behaviors (in which the Wisconsin Card Sort Task and a variant on the Color-Word Stroop task was weakly negatively associated with the Inventory of Depression and Anxiety Symptoms suicidality subscale, r = −.010 & r = −.200, respectively, and moderately negatively associated with suicide attempt history, r = −.35 & r = −.32, respectively), though a meta-analysis was not run on these due to the limited sample size.
Memory: Meta-Analysis
Nine studies (N = 1,414) met inclusion criteria for evaluating some components of memory alterations with PTSD symptoms, including: over-general memory, verbal learning and memory, and working memory. The association between PTSD and memory was not significant (r = .028, CI95%: −.078, .133, p = .603; Q = 37.657, I 2 = 81.411 [CI95%: 60.038, 88.706], p < .001, Τ2 = .018, SE = .013, df = 8; Supplemental Table 14A, Supplemental Figure 21). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left or right of the mean.
Only two studies (N = 476; Ely et al., 2009; Jiang et al., 2020) met inclusion criteria for evaluating some component of memory associations with suicidal thoughts and behaviors, with associative strength in the small to medium range (range r: .098 - .39), though a meta-analysis was not run on these due to the limited number of studies.
Negative Cognitions: Meta-Analysis
Hopelessness: Meta-Analysis
Across 14 studies (N = 7,950), there was a significant random effect of PTSD on hopelessness (r = .460, CI95%: .232, .639, p = .001; Q = 1,516.412, I2 = 99.077 [CI95% 98.813, 99.175], p < .001, Τ2 = .256, SE = 201, df = 15; Supplemental Table 15A, Supplemental Figure 22). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left of the mean and 8 outliers to the right of the mean, that when removed meaningfully increased the effect (r = .762, CI95% .596, .866).
Across 11 studies (N = 7,569), there was a significant random effect of hopelessness on suicidal thoughts and behaviors (r = .394, CI95%: .272, .503, p < .001; Q = 253.843, I2 = 96.076 [CI95%: 94.416, 97.221], p < .001, Τ2 = .047, SE = .042, df = 10; Supplemental Table 15B, Supplemental Figure 23). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 2 outliers to the left of the mean, but the random effect point estimate was not meaningfully changed (r = .315, CI95% .189, .430).
Defeat and Entrapment: Meta-Analysis
Across 6 studies (N = 808), there was a significant random effect of PTSD on defeat/entrapment (r = .614, CI95%: .430, .750, p < .001; Q = 59.081, I2 = 91.537 [CI95%: 84.346, 95.425], p < .001, Τ2 = .091, SE = .076, df = 5; Supplemental Table 16A, Supplemental Figure 24). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 3 outliers to the left of the mean, which lowered the point estimate was substantially (r = .423, CI95% .180, .617).
Across 7 studies (N = 899), there was a significant random effect of defeat/entrapment on suicidal thoughts and behaviors (r = .668, CI95%: .604, .723, p < .001; Q = 30.544, I2 = 80.356 [CI95%: 60.087, 90.332], p < .001, Τ2 = .016, SE = .013, df = 6; Supplemental Table 16B, Supplemental Figure 25). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 2 outliers to the left of the mean, but the random effect point estimate was not meaningfully changed (r = .636, CI95% .570, .696).
Cognitions About Others and the World: Meta-Analysis
Across 9 studies (N = 2,374), there was a significant random effect of PTSD onnegative cognitions about others and the world (r = .328, CI95%: .250, .401, p < .001; Q = 31.964, I2 = 74.972 [CI95%: 51.645, 87.056], p < .001, Τ2 = .011, SE = .009, df = 8; Supplemental Table 17A, Supplemental Figure 26). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left or right of the mean.
Across 6 studies (N = 1,793), there was a significant random effect of negative cognitions about others and the world on suicidal thoughts and behaviors (r = .306, CI95%: .177, .425, p = .001; Q = 34.480, I2 = 85.499 [CI95%: 70.401, 92.896], p < .001, Τ2 = .023, SE = .02, df = 5; Supplemental Table 17B, Supplemental Figure 27). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 1 outlier to the left of the mean, but the random effect point estimate was not meaningfully changed (r = .259, CI95% .120, .388).
All Self-Cognitions: Meta-Analysis
Across 25 studies (N = 15,323) using a variety of self-focused cognitions (self-esteem, self-blame, failure, feeling inadequate, self-hatred, negative self-evaluations, negative self-statements, and self-compassion), there was a significant random effect (r = .244, CI95%: .170, .314, p < .001; Q = 739.629, I2 = 96.755 [CI95%: 95.986, 97.376], p < .001, Τ2 = .034, SE = .026, df = 24; Supplemental Table 18A, Supplemental Figure 28) for associations with PTSD. Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 8 outliers to the left of the mean, but the random effect point estimate was not meaningfully changed (r = .146, CI95% .072, .218).
Across 16 studies (N = 3,648) using a variety of self-focused cognitions (self-blame, negative self-statements, negative cognitions about the self, self-compassion, self-concept, and self-esteem), the random effect was not significant (r = .191, CI95%: −.010, .377, p = .062; Q = 812.819, I2 = 98.155 [CI95%: 97.691, 98.524], p < .001, Τ2 = .165, SE = .100, df = 15; Supplemental Table 18B, Supplemental Figure 29) with suicidal thoughts and behaviors. Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 4 outliers to the left of the mean, which further reduced the effect size (r = .059, CI95% −.1230, .244). Given that this category included a multitude of outcomes, subsequent analyses were run to pull out individual outcomes where possible when at least 4 comparisons were available, as described below.
Self-Esteem: Meta-Analysis
Across 16 studies (N = 14,536), there were significant random effect of PTSD on self-esteem (r = .295, CI95%: .223, .364, p < .001; Q = 272.216, I2 = 95.224 [CI95%: 93.389, 96.550, p < .001, Τ2 = .018, SE = .015, df = 13; Supplemental Table 19A, Supplemental Figure 30). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 7 to the left of the mean that, when removed, reduced the effect size substantially (r = .180, CI95% 0.108 – 0.250).
Across 4 studies (N = 501; Duprey et al., 2019; Ely et al., 2009; Lamis et al., 2016; Prigerson & Slimack, 1999), there was a significant association between self-esteem and suicidal thoughts and behaviors (r = .363, CI95%: .124, .562, p = .004; Q = 24.103, I2 = 87.553 [CI95%: 70.3603, 94.773], p < .001, Τ2 = .059, SE = .056, df = 3; Supplemental Table 19B, Supplemental Figure 31). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left and 1 to the right of the mean which, when removed increased the effect size (r = .438, CI95% .214 - .618).
Self-Blame: Meta-Analysis
Across 4 studies (N = 1,086), there was a significant random effect of PTSD on self-blame (r = .337, CI95%: .247, .421, p < .001; Q = 8.753, I2 = 65.727 [CI95% −0.665, 88.331], p = .001, Τ2 = .006, SE = .008, df = 3; Supplemental Table 20A, Supplemental Figure 32). Duval and Tweedie’s trim-and-fill technique revealed 0 outliers to the right of the mean and 2 to the left of the mean which did not meaningfully change the random effect when removed (r = .389, CI95% .300 - .471).
Across 4 studies (N = 1,086), there was a significant random effect of self-blame on suicidal thoughts and behaviors (r = .238, CI95%: .102, .365, p < .001; Q = 20.059, I2 = 85.044 [CI95%: 62.889, 93.973], p < .001, Τ2 = .016, SE = .019, df = 3; Supplemental Table 20B, Supplemental Figure 33). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 1 outlier to the left of the mean that, when removed, reduced the random effect point estimate (r = .167, CI95% .021, .306).
Distress Tolerance: Meta-Analysis
Across 14 studies (N = 6,063), there was a significant random effect of PTSD on distress tolerance (r = .291, CI95%: .211, .367, p < .001; Q = 147.150, I2 = 91.165 [CI95% 86.935, 93.026, p < .001, Τ2 = .022, SE = .014, df = 13; Supplemental Table 21A, Supplemental Figure 34). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left of the mean, and 2 to the right of the mean which slightly reduced the random effect size when removed (r = .242, CI95% .154, .326).
Across 10 studies (N = 3,211), there was a significant random effect of distress tolerance on suicidal thoughts and behaviors was significant (r = .243, CI95%: .174, .309, p < .001, Q = 37.000, I2 = 75.676 [CI95%: 54.846, 86.897], p < .001, Τ2 = .009, SE = .007, df = 9; Supplemental Table 21B, Supplemental Figure 35). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the left or right of the mean.
Perfectionism: Meta-Analysis
Only three studies were eligible for inclusion focused on perfectionism (Bloch-Elkouby et al., 2020; Cohen et al., 2018; Egan et al., 2014), and therefore a meta-analysis was not conducted on this topic. In one (Bloch-Elkouby et al., 2020), the association between perfectionism and PTSD (r = .07) and suicidal thoughts and behaviors (r = .16) was small. In the second (Cohen et al., 2018), the association between perfectionism and PTSD was not reported, but the association between perfectionism and suicidal thoughts and behaviors on two separate measures was small (range r = .16 - .18). In the third (Egan et al., 2014), multiple measures of perfectionism and associations with PTSD ranged from small (r = .24) to large (r = .69).
Pain-Related Conditions: Meta-Analysis
Across nine studies (N = 2,457), there was a significant random effect of PTSD on pain-related conditions (pain intensity, pain catastrophizing, pain tolerance, and pain acceptance) was significant (r = .208, CI95%: .062, .345, p < .001; Q = 131.872, I2 = 93.934 [CI95%: 90.542, 96.109], p < .001, Τ2 = .044, SE = .040, df = 8; Supplemental Table 22A, Supplemental Figure 36). Duval and Tweedie’s trim-and-fill technique revealed no outliers to the right of the mean and 3 outliers to the left of the mean, and the random effect point estimate was meaningfully reduced when removed (r = .079, CI95% −.075, .230).
While not included in the meta-analysis due to slight differences in the construct under study, one study also found that a variety of types of childhood trauma were associated with reduced ability to register sensory input (physical neglect r = .27, emotional abuse r = .25, emotional neglect r = .33, sexual abuse r = .22), enhanced sensory sensitivity (physical neglect r = .22, emotional abuse r = .25, emotional neglect r = .29; Serafini et al., 2016). Two studies (N = 1,515; Moreno et al., 2019; Vogel et al., 2017) reported small associations between pain-related conditions and suicidal thoughts and behaviors (range r = .100–.290).
Synthesized Model: CEASE Framework
Synthesizing information across the meta-analytic results, a new conceptual model of the transition from PTSD to suicidal thoughts and behaviors is offered (Figures 4 and 5). This model proposes changes in CEASE framework: New conceptual model on transition from PTSD to suicidal thoughts and attempts Connection of theories of suicide to CEASE factors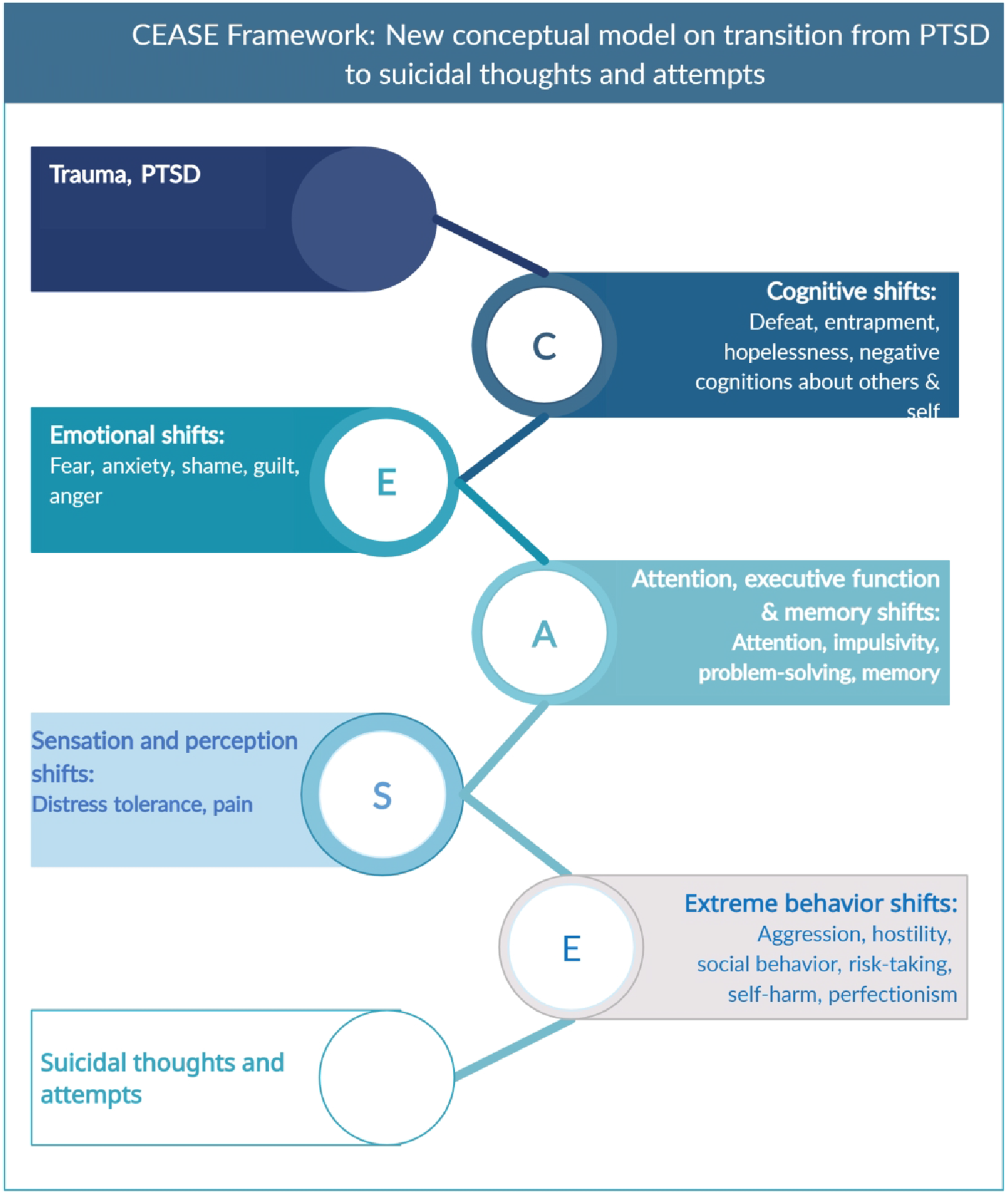
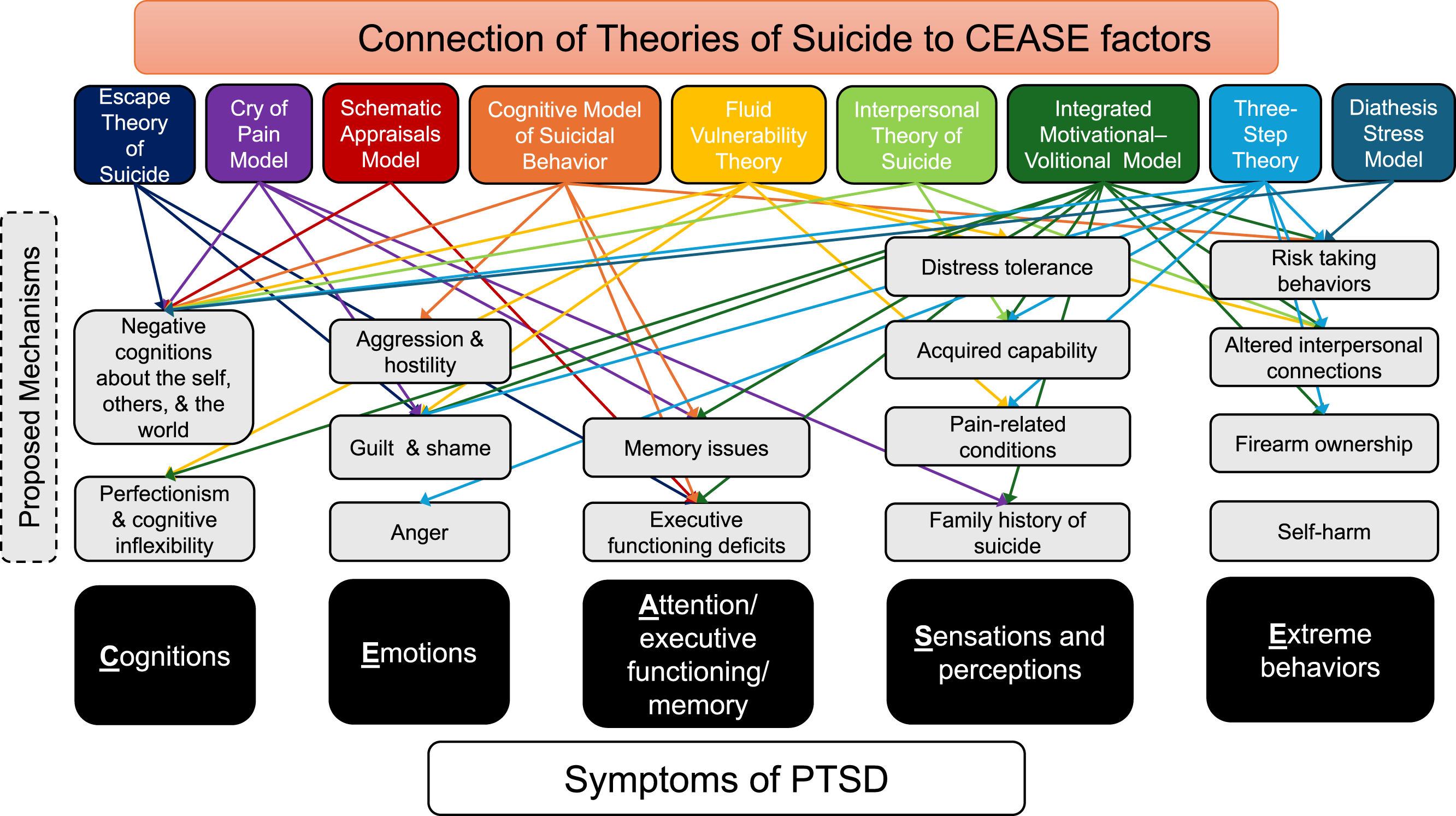
Discussion
In this meta-analysis, several potential correlates of the association between PTSD and suicidal thoughts and behaviors were identified and synthesized in the CEASE model. Correlates with the strongest evidence included changes in cognitions (e.g., defeat, entrapment, negative thoughts about others and the world), emotional shifts (e.g., guilt, shame, anger), and changes in distress tolerance (a component of sensation and perception). There was also evidence that some extreme behavioral shifts (e.g., aggression, risk-taking behaviors, changes in social behaviors and connection, self-harm) are also important, though effect sizes were smaller for these factors. More research is needed on the attention/executive functioning/memory (e.g., impulsivity, autobiographical memory) domains. Whereas interpersonal factors are integral to most theories on the development of suicidal thoughts and behaviors, meta-analytic findings suggested that this factor was only modestly important for both associations with PTSD and with suicidal thoughts and behaviors. This finding may have been attributable to some of the overlap between social cognitions and trauma-related cognitions about other people and the world more generally. Inconsistent with some major theories, acquired capability had a small effect; however, some features of acquired capability (risk-taking and self-harm) were relatively more important in the meta-analysis.
The mechanisms of action that were identified as critical in this meta-analysis were partially consistent with several theories on the development of suicidal thoughts and behaviors. Given that theories on suicidal thoughts and behaviors were not developed to focus on PTSD as a core etiological factor, several deviations from these theories require consideration among trauma-exposed samples. Cognitive alterations have received a great deal of attention as key risk factors for both the development, maintenance, and recovery from PTSD (Brown et al., 2019). Whereas PTSD researchers and clinicians commonly focus on changes in cognitions about the self, others, and the world, the types of cognitions that appear most relevant to suicidal thoughts and behaviors include perceptions about hopelessness, defeat, and entrapment. In the context of suicide risk, alterations in cognitions about the future (e.g., hopelessness, entrapment, defeat) are well-reflected in the Cognitive Model of Suicidal Behavior (Wenzel & Beck, 2008), the Integrated Motivational-Volitional Model of Suicidal Behaviour (R. C. O’Connor & Kirtley, 2018), the Three-Step Theory of Suicide (Klonsky & May, 2015), the Schematic Appraisals Model (J. Johnson et al., 2008), the Cry of Pain Model (Bolton et al., 2007), and the Escape Theory (Baechler, 1980). Thus, negative cognitions about the future and about being trapped have a long history of importance in understanding suicidal thoughts and behaviors, a finding further supported by this meta-analysis in patients with post-traumatic stress symptoms. Rather than focusing on social connection or disconnection per se in this model, which includes a variety of possible variables (Millner et al., 2020), we propose that building blocks of social connection (including negative thoughts about the self, others, or aggressive behavior) might improve future modeling of suicide risk among patients with PTSD. This will be an important direction for future research to validate CEASE, as well as to confirm directional effects in CEASE.
While PTSD is often characterized as an anxiety-related disorder, other strong emotional reactions are common. Shame, guilt, and anger are three emotions that are experienced intensely among individuals with PTSD. In this meta-analysis, these three emotions were strongly associated with both PTSD and suicidal thoughts and behaviors. In the Interpersonal Theory of Suicide, thwarted belongingness may be more common among individuals struggling with strong emotions of shame, as individuals struggling with shame report cognitions about being defective or less than other people. Similarly, individuals struggling with perceived burdensomeness may also experience strong guilt, including feeling that the manner in which an individual has offended others (the source of their guilt) is evidence of being a burden. While social connection did not emerge among the strongest mechanisms of action for the association between PTSD and suicidal thoughts and behaviors in this meta-analysis, the emotional experiences of shame, guilt, and anger at other people may better explain some of the variance that is typically attributed to interpersonal effects on suicide in the general population. Similarly, cognitions about other people (described above) may be more important than perceptions of social support among patients with PTSD. Further disentangling the associations between these affect constructs, negative trauma-related cognitions, and social connection will be critical for future evaluations of CEASE.
Biological perturbations are clearly documented among individuals with PTSD or who are at risk for suicide. Consistent with this, this meta-analysis found evidence that distress tolerance was associated with PTSD and suicidal thoughts and behaviors, such that individuals with PTSD have lower distress tolerance, which was associated with higher risk for suicidal thoughts and behaviors. However, distress tolerance is a complicated concept in the context of differential experiences of arousal. Individuals with chronic abuse and neglect are more likely to demonstrate hypoarousal in physiological reactivity compared to healthy controls or individuals with single incident traumas (d’Andrea et al., 2013). Distress tolerance is difficult to measure among individuals with baseline differences in sensation and perception, which impact both distress and the need for tolerance of that distress. In our meta-analysis, there was also a significant association between pain and PTSD. However, there were a limited number of studies evaluating pain and suicidal thoughts and behaviors among patients with PTSD. Longitudinal research in individuals with chronic pain reveals that catastrophic cognitions about chronic pain predicts future suicidal ideation (Brown et al., 2020b). The extent to which this pain-suicide risk pathway is altered among individuals with PTSD is unclear and should be a direction for future research. Perhaps paradoxically, repeated exposure to painful stimuli is associated with reduced subjective intensity of pain among women with PTSD compared to healthy controls (Strigo et al., 2010). Further, the numbing cluster of PTSD is associated with greater reports of heightened pain tolerance (Zuromski et al., 2014). More research is necessary to understand why some individuals with PTSD experience habituation to pain whereas others experience elevated or sustained pain, and how those experiences contribute to or reduce risk for suicide. This will be an important future direction to evaluate in longitudinal studies of CEASE.
The association between executive functioning, memory and planning with PTSD and suicidal thoughts and behaviors was complex. Part of the complexity lies in the lack of clarity in the term “executive functioning”, which has been used to refer to everything from challenges in attention to task-shifting, and which is measured using a variety of self-report, clinician-rated and objective indicators. To reduce complexity, an analysis was run based on measures recommended from Miyake and colleagues (2012) and used in a prior meta-analysis on depression (Snyder, 2013). With this limited set of measures, there was not a significant association between executive functioning and either PTSD or suicidal thoughts and behavior. Too few studies were available for a meta-analysis on the association between executive function and suicidal thoughts and behaviors, though individual studies reported tentative support for an association between these variables. Associations with memory were also complex. Meta-analytic findings generally did not support associations between memory disturbances and either PTSD or suicidal thoughts and behaviors, but some review studies reported meaningful associations. More research is needed to understand both executive functioning and memory changes among individuals with PTSD who are at risk for suicide.
Behavior changes are also important to the development and maintenance of PTSD and suicidal thoughts and behaviors. For instance, increased risk-taking behaviors is a recently recognized core symptom of PTSD (American Psychiatric Association, 2013). According to the Interpersonal Theory of Suicide (Joiner, 2005), the Three-Step Theory of Suicide (Klonsky & May, 2015), the Cognitive Model of Suicidal Behavior (Wenzel & Beck, 2008), and the Integrated Motivational-Volitional Model of Suicidal Behaviour (R. C. O’Connor & Kirtley, 2018), these risk-taking behaviors are important risk factors for suicidal behavior. In this meta-analysis, aggression and hostility, risk-taking behaviors, and self-harm each were associated with PTSD and suicidal thoughts and behaviors. However, the strength of these associations was modest, and more research is needed on this validate the importance of these factors in CEASE.
There are a few important limitations of this meta-analysis. First, our results included investigations from cross-sectional and longitudinal studies. Future research should closely measure the constructs suggested as critical mechanisms of PTSD and suicidal thoughts and behaviors (Figure 4). Second, given the complexity of the meta-analyses (and the approach taken in included studies to combine suicide-related outcomes), we attempted to reduce complexity by reporting suicidal thoughts and attempts in combined analyses. Now that some factors have been identified as relatively more fruitful than others, future studies should study suicidal thoughts separate from suicide attempts. For most of our analyses, there are insufficient studies available to separate thoughts and behaviors, which is why that was not prioritized in this study. Third, many pieces of the meta-analysis violated the assumption of homogeneity, which is to be expected given the large number of studies included for Q2 (Higgins et al., 2003). For this reason, we report random effects. There were also no meaningful differences when sensitivity analyses were run to identify and attempt to contain up to 20 sources of heterogeneity.
In summary, this meta-analysis offers insights into the association between PTSD and suicide risk using nine key theories. Across these disparate theories, several key themes emerged that suggest cognitive, biological, behavioral, and social factors that may serve as key correlates that link PTSD and suicidal thoughts and behaviors. A variety of cross-sectional and some longitudinal studies support these correlates. This meta-analysis resulted in a new model of the underlying correlates linking PTSD and suicide risk (Figure 4) that can be explored in future longitudinal research. In this CEASE Framework, shifts in core cognitions (e.g., defeat, hopelessness, negative cognitions about other, the world, and the self), emotions (e.g., shame, guilt, anger), attention, executive function and memory (e.g., impulsivity), sensations and perceptions (e.g., changes in distress tolerance and pain sensitivity), and extreme behavior (e.g., risk-taking, aggression, social changes, self-harm) are all proposed as critical to the development of suicidal thoughts and behaviors among individuals with PTSD.
Supplemental Material
Supplemental Material - Explaining the Link Between PTSD and Suicide: A Meta-Analysis to Introduce the CEASE Framework
Supplemental Material for Explaining the Link Between PTSD and Suicide: A Meta-Analysis to Introduce the CEASE Framework by Lily A. Brown, Yiqin Zhu, Marin Kautz, Erica Weitz in Psychological Reports.
Supplemental Material
Supplemental Material - Explaining the Link Between PTSD and Suicide: A Meta-Analysis to Introduce the CEASE Framework
Supplemental Material for Explaining the Link Between PTSD and Suicide: A Meta-Analysis to Introduce the CEASE Framework by Lily A. Brown, Yiqin Zhu, Marin Kautz, Erica Weitz in Psychological Reports.
Supplemental Material
Supplemental Material - Explaining the Link Between PTSD and Suicide: A Meta-Analysis to Introduce the CEASE Framework
Supplemental Material for Explaining the Link Between PTSD and Suicide: A Meta-Analysis to Introduce the CEASE Framework by Lily A. Brown, Yiqin Zhu, Marin Kautz, Erica Weitz in Psychological Reports.
Supplemental Material
Supplemental Material - Explaining the Link Between PTSD and Suicide: A Meta-Analysis to Introduce the CEASE Framework
Supplemental Material for Explaining the Link Between PTSD and Suicide: A Meta-Analysis to Introduce the CEASE Framework by Lily A. Brown, Yiqin Zhu, Marin Kautz, Erica Weitz in Psychological Reports.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was in part supported by the Military Suicide Research Consortium (MSRC) under Award No (W81XWH-16-2-0004). Opinions, interpretations, conclusions and recommendations are those of the authors and are not necessarily endorsed by the MSRC or the Department of Defense. Funding was also provided by the National Institute of Mental Health (5P50MH127511 and R21MH123888). This publication resulted (in part) from research supported by an inter-CFAR collaboration between the District of Columbia Center for AIDS Research (P30 AI117970), the University of Pennsylvania CFAR (P30 A1 045008), and the Johns Hopkins University CFAR (P30 A1 094189). This collaboration is supported by the following NIAID, NCI, NICHD, NHLBI, NIDA, NIMH, NIA, FIC, NIGMS, NIDDK, and OAR. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available upon request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.