
Abstract
Perceived social isolation (PSI) predicts adverse health and behaviour problems better than objective social isolation (OSI). PSI is related to higher sensitivity to negative emotional states and emotional dysregulation. Some studies suggest that the more socially isolated people feel, the more sensitive they are to the suffering of others, yet the less empathic they are. However, no study has tested the association between social isolation and empathy while distinguishing their state and trait forms. This study examined how individuals with high- and low-PSI trait perceived and empathized with virtual agents displaying facial expressions. Sixty-six healthy young adults (38 women) were equally divided into high- or low-trait PSI subgroups. All participants reported their current state of PSI and then watched short videos of virtual agents showing facial expressions of physical pain or sadness. For each video, participants rated the perceived intensity of affective states and empathy felt (state empathy). They also completed questionnaires on trait empathy, OSI, moods, and depressive symptomatology. The results showed no effect of group (high- or low-trait PSI), facial expression (pain, sadness), or their interaction on state empathy and intensity mean ratings. However, regression analyses revealed that OSI specifically predicted perspective-taking and empathic concern aspects of trait empathy, whereas trait PSI predicted the personal distress aspect. These findings suggest that social skills may play a role in maintaining and developing relationships but are not linked to one’s perception of their quality. This work highlights the importance of differentiating objective from perceived social isolation, given their distinct associations with specific social processes and skills, such as empathy. This distinction could further help develop more targeted interventions to alleviate social isolation.
In 2024, one in three American adults reported suffering from social isolation at least once a week over the past year (American Psychiatric Association, 2024). Social isolation poses serious health threats, as it is associated with heightened stress response (Zilioli & Jiang, 2021), higher rates of depression (Mushtaq et al., 2014), poorer sleep quality (McLay et al., 2021), and even increased mortality (Holt-Lunstad et al., 2015). Social isolation is thus a major public issue that warrants appropriate attention in research.
Social isolation can be either objective or subjective (Gierveld et al., 2018). Objective social isolation (OSI) is a lack of social interactions between a person and their social network. It differs from perceived social isolation (PSI; or loneliness), an aversive psychological experience prompted by the subjective perception of being socially isolated. The experience of PSI stems from the perceived gap between the desired and the actual quality and quantity of a person’s interpersonal relationships. Therefore, one person might not feel lonely, even though they have few social contacts and are, objectively speaking, socially isolated. Inversely, another person may have many social interactions and not be isolated, yet still feel alone, separated, or apart from others and suffer from a perceived lack of social connectedness. PSI can be further described as situational (i.e., state PSI), such as when it is experienced as an aversive acute feeling after a breakup or a relocation (Cacioppo & Patrick, 2008). However, it is most typically defined in studies as a relatively stable trait (i.e., trait PSI) when this feeling occurs over an extended period rather than following a transient situation (Mund et al., 2020).
Trait PSI and OSI are moderately associated (Taylor et al., 2023), yet they have distinct adverse impacts (Cacioppo & Cacioppo, 2018; Gierveld et al., 2018). Trait PSI more strongly predicts health and behavioural changes than OSI (Cacioppo et al., 2011; Rico-Uribe et al., 2016), and PSI (as assessed by one question) is the item of a neuroticism questionnaire most strongly associated with premature mortality, including deaths from intentional self-harm (Deason et al., 2025). Trait PSI is also associated (if not confused) with negative psychological experiences that are closely related but conceptually distinct, such as social exclusion (Cacioppo & Patrick, 2008) and depression. Some researchers have even questioned whether trait PSI and depression are truly distinct (Mushtaq et al., 2014), given their moderate correlation (Russell et al., 1980) and that trait PSI predicts depression levels in longitudinal studies (Cacioppo et al., 2010). Nonetheless, these two constructs remain statistically distinguishable (Cacioppo et al., 2006; Russell et al., 1980).
Despite its negative consequences, short-term PSI is considered an adaptive response that helps individuals, according to cognitive and evolutionary theories, detect social isolation and its associated survival threat, and restore social bonds (Cacioppo & Cacioppo, 2018). A large body of data shows that loneliness increases sensitivity to negative social cues, which contrast with the sparsity of support for the more context-dependent positive cues (for a summary of theoretical approaches on loneliness and social information processing, see Blandl & Eisenberger, 2025). Trait PSI has also been linked to sensitivity toward negatively experienced affective states, including physical (i.e., pain; Wolf & Davis, 2014; Yamada et al., 2021) and emotional (e.g., sadness; Yang et al., 2023) suffering. An individual with high trait or state PSI tends to experience physical pain more frequently and intensely (Allen et al., 2020; Wolf & Davis, 2014; Yamada et al., 2021). PSI thus seems to be frequently associated with self-related negativity.
However, less is known about the relationship between PSI and perceived negativity in others. In other words, it remains unclear whether individuals who feel isolated are generally negative or whether this negativity is specific to their own feelings. Some studies have examined the influence of PSI on emotion perception and recognition in others, which are low-level social cognition processes (Eikelboom et al., 2025). The results indicate that trait PSI is associated with a heightened sensitivity to negative affective states in others, either through a greater likelihood of misidentifying affective facial expressions as painful or angry (Smith et al., 2022), or through potentially lower response time to identify sadness and fear depicted on faces (Vanhalst et al., 2017). Taken together, these findings suggest a possible relationship between trait PSI and greater sensitivity to negative affective states, both felt and perceived in others.
Trait PSI may also affect higher-level social cognition processes, such as empathy. Empathy refers to the ability to understand, feel, and share another person’s experiences, while maintaining a clear distinction between oneself and others (Håkansson Eklund & Summer Meranius, 2021). It can be divided into three interrelated components (Decety & Jackson, 2004). The cognitive component allows inferring a mental or affective state (e.g., intention, belief, emotion). The affective component enables sharing the target’s emotional state. The emotional regulation component distinguishes between what is experienced by the self and what is experienced by the other. This component also helps to balance the affective and cognitive components so that the target’s emotion does not cause distress to the observer. Distinguishing between these components is essential, as one may be more affected than others in certain situations or within specific clinical populations. For instance, individuals with autistic spectrum disorder mainly experience difficulties with the cognitive component of empathy (Fatima & Babu, 2024). Much like PSI, empathy can also be described as situational (i.e., state empathy) or dispositional (trait empathy; Nezlek et al., 2001). State empathy is the feeling of empathy that varies according to context and person (e.g., empathy felt during a behavioural task). In contrast, trait empathy refers to a stable characteristic that persists over time. According to Davis (1983), trait empathy can be divided into distinct aspects linked to specific components of empathy. For instance, the perspective-taking aspect (i.e., the tendency to spontaneously adopt the point of view of others) relates to the cognitive component, while the empathic concern aspect (i.e., “other-oriented” feelings of sympathy and concern for unfortunate others) aligns with the affective component (Wang et al., 2020).
Some correlational studies have shown that trait empathy is significantly and negatively associated with trait PSI (e.g., Beadle et al., 2012; Davis, 1983). People with low empathy skills may struggle to accurately identify the emotions and thoughts of others. Such difficulties may lead them to judge their social interactions negatively, thereby contributing to their feelings of PSI. However, a recent study revealed a negative but nonsignificant association between these concepts after controlling for confounding factors, including OSI (Mwilambwe-Tshilobo et al., 2023). Taking into account OSI and other confounding factors, like state PSI and depressive symptomatology, is thus essential when examining PSI and its relationship with empathy.
To our knowledge, only the study of Hu et al. (2020) has yet explicitly explored PSI and its influence on empathy in a situational setting. State PSI was experimentally manipulated using a recall task during which participants wrote about a time when they felt lonely and isolated. A control group of participants wrote about their daily routine instead. Participants in whom feelings of PSI had been elicited were less likely to empathize with static pictures depicting facial expressions of worry and anger than the participants in the control group. However, the generalizability of these results is specific to state PSI. Both state and trait PSI should be evaluated in parallel to understand their influence on empathy, given the clear distinction between the two. Other negative affective states that can trigger empathy for physical and emotional suffering, such as pain and sadness, were also not studied. In addition, static pictures of facial expressions depicting negative emotions also lacked external validity due to the absence of dynamism. Using computer-generated faces (“virtual agents”) that express various affective states offers a valuable alternative for measuring empathy. This approach enables more precise manipulation of parameters such as dynamism and better control of facial expressions, surpassing the limitations typically associated with databases of real individuals (Dildine & Atlas, 2019; Dildine et al., 2023). It also has a better balance between internal and external validity. Recent studies have demonstrated that virtual agents can elicit reactions similar to those observed in real-life human interactions (e.g., Bélanger et al., 2025; Glikson & Woolley, 2020).
Present Research
Despite the numerous and well-documented negative impacts of PSI on physical and mental health, few studies have investigated the relationship between PSI and essential social skills for maintaining and developing relationships, such as perceiving suffering in others and empathizing with them. Identifying potential factors associated with PSI (e.g., empathy deficits) is thus crucial and the first step in developing more targeted interventions. Furthermore, published studies on these relationships have relied predominantly on self-report questionnaires, often neglecting the multifaceted nature of social isolation and failing to adequately control for confounding variables. The present study aimed to address these gaps by using a multi-method approach that combined questionnaires with measures obtained during a behavioural task.
The first objective of the present study was to investigate the differences in trait and state empathy for physical and emotional suffering (i.e., empathy for others’ distress; Morelli et al., 2015) between two groups of healthy adult individuals differing in their levels of trait PSI (i.e., low and high). Based on the same group comparison, the second objective was to examine the differences in the sensitivity to physical and emotional suffering, assessed by the perceived intensity of facial expressions depicting pain and sadness. To meet these two objectives, statistical control of the contribution of confounding factors, such as state PSI, OSI, and depressive symptomatology, was planned. The hypotheses were that individuals scoring high on trait PSI levels, compared to individuals scoring low, would report lower levels of state and trait empathy (regardless of the specific aspect; Hyp. 1); and perceive affective states as more intense even after accounting for levels of state PSI, OSI, or depressive symptomatology (Hyp. 2).
Method
Participants
The number of participants needed was based on previous studies with a similar design (Coll et al., 2017; Gingras et al., 2021; Tremblay et al., 2020) and an a priori power analysis. The analysis was conducted with G*POWER for the between-subjects effect of a mixed multivariate analysis of variance (MANOVA). A multivariate analysis was planned, as the two main dependent variables (i.e., state empathy and intensity of the affective state) are strongly associated (Coll et al., 2017; Tremblay et al., 2020). The following parameters were entered: effect size f = .30, α = .05, β = .80, number of groups = 2, number of measurements = 4, and correlation among repeated measures = .50. The analysis resulted in a minimum total sample size of 58 participants.
Participants’ Frequencies and Mean Responses to the Questionnaires Divided Into Subgroups (Low and High UCLA-LS)
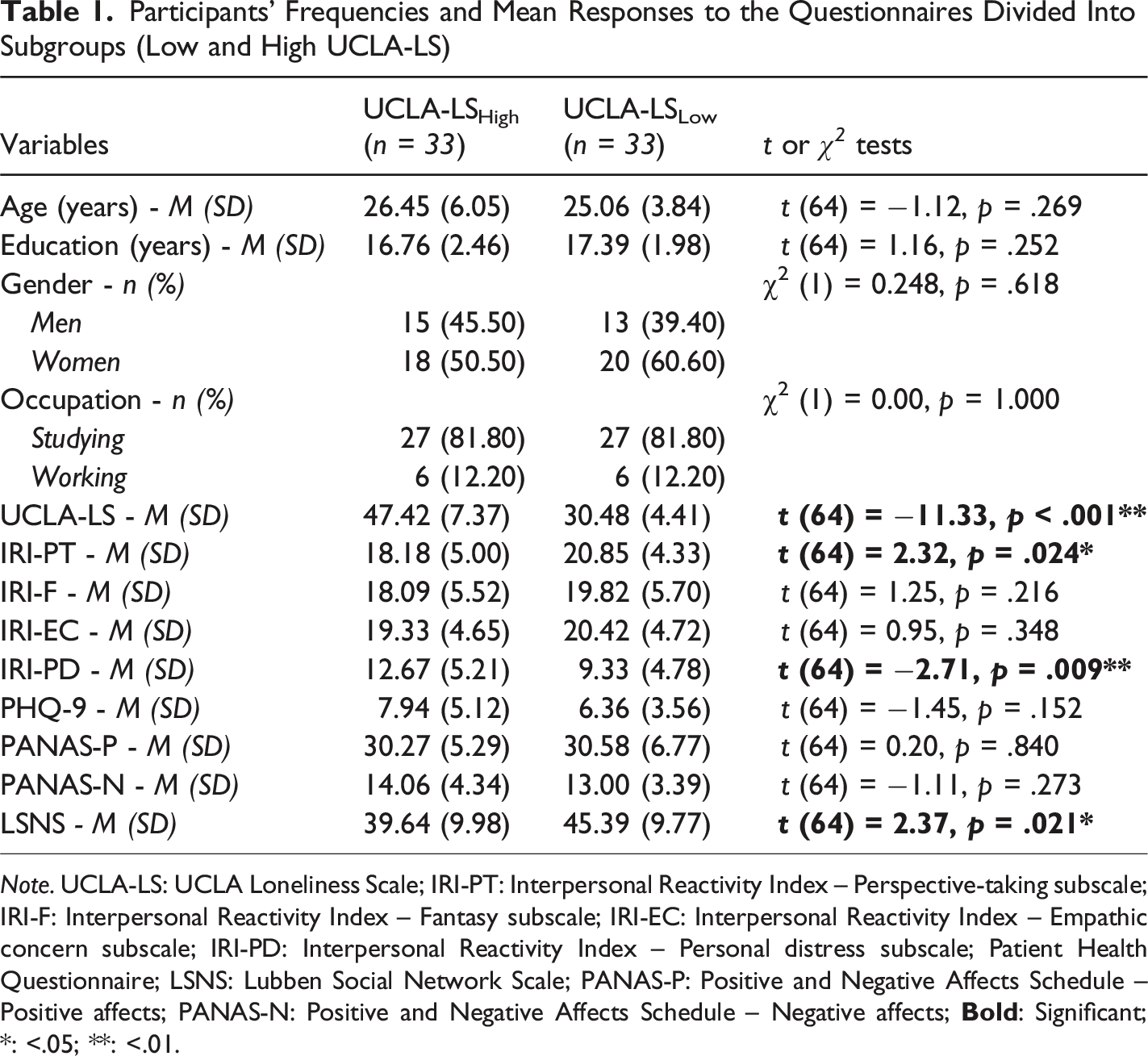
Note. UCLA-LS: UCLA Loneliness Scale; IRI-PT: Interpersonal Reactivity Index – Perspective-taking subscale; IRI-F: Interpersonal Reactivity Index – Fantasy subscale; IRI-EC: Interpersonal Reactivity Index – Empathic concern subscale; IRI-PD: Interpersonal Reactivity Index – Personal distress subscale; Patient Health Questionnaire; LSNS: Lubben Social Network Scale; PANAS-P: Positive and Negative Affects Schedule – Positive affects; PANAS-N: Positive and Negative Affects Schedule – Negative affects;
Material
Stimuli
The stimuli were 2000 ms videos of virtual agents displaying various facial expressions. These expressions, along with the agents’ appearances, were previously validated for their perceived affective state and intensity (Trieu et al., 2025). Facial expressions, especially those conveying pain, are an effective way to elicit empathy, as demonstrated by neuroscience research (e.g., Jauniaux et al., 2019). As key nonverbal cues, they can communicate emotions and elicit responses from observers, such as empathic ones (Frith, 2009). Such emotional expressions are perceived rapidly and automatically (Matt et al., 2021). They are among the most effective methods for inducing affective states, outperforming methods, such as autobiographical recall or story reading (Joseph et al., 2020). All virtual agents were generated using the MetaHuman Creator. They were animated in Unreal Engine software (Epic Games, Inc.), in which 161 facial controls can reproduce facial movements. Facial controls can be associated with Action Units (AUs; smallest visually discriminable facial movements) of the Facial Action Coding System (Ekman et al., 2002). According to this system, facial expressions can be broken down into AUs. Certain configurations of AUs are associated with specific affective states (e.g., pain = AUs 4, 6-7, 9-10 and 25-26-27, and sadness = AUs 1,4, 6, 15 and 17; Ekman et al., 2002; Kunz et al., 2019; Simon et al., 2008). Eight virtual agents (four representing women) with physical features stereotypical of four different phenotypes (i.e., Black, White, Latin American, or Asian; one per gender) were used. Each virtual agent displayed a moderate-to-intense (as perceived in average by participants in the validation study) facial expression of pain or sadness, or a neutral expression. A total of 24 stimuli were thus presented, corresponding to eight virtual agents each displaying three distinct expressions. For the pain and sadness stimuli, the videos showed a facial expression gradually changing from a neutral state to the target expression. A neutral expression (i.e., static image without facial movement) was used to ensure an adequate understanding of the task.
Questionnaires
Procedure
The questionnaires in the online survey were remotely administered using the Dexero web platform (Dexero, Inc.). They required around 20 minutes to complete, and included a consent form, a sociodemographic questionnaire, and the UCLA-LS and IRI scales.
The in-person experiment was conducted in the presence of a research assistant. Written consent was first obtained, followed by the completion of the PANAS questionnaire. Participants’ moods were assessed prior to the main task to account for their potential impact on the results. This allowed for a better interpretation of whether participants’ baseline emotional states may have influenced their responses during the experiment. This consideration is important, as positive and negative moods can influence empathy (Nezlek et al., 2001). Then, participants started a computer task created using the PsychoPy software (Peirce et al., 2019). The state PSI was first assessed by asking the participant to indicate their current level of loneliness (i.e., state PSI) with a VAS ranging from “No loneliness” to “Maximum loneliness” (1-100). The VAS was displayed until a response was confirmed by pressing the space bar. Previous studies used similar techniques to investigate the relationship between trait and state PSI (e.g., Tam & Chan, 2019).
Three experimental blocks followed (see Figure 1): Empathy, Intensity, and Recognition. The order of the first two blocks (Empathy and Intensity) was counterbalanced across participants to avoid potential carry-over effects. The third block (Recognition) was always administered last, as it was used as a manipulation check to ensure adequate recognition of the stimuli. Before each block, instructions were presented, followed by a training phase comprising eight trials with virtual agents different from those used in the study phase. In the Empathy block, the participant was asked to put themselves in the person’s shoes and report their empathy on a VAS. This behavioral measure was selected to assess state empathy under controlled conditions and to provide a complementary measure to the IRI questionnaire, thereby facilitating a more comprehensive understanding of this concept. The following definition was provided at the beginning of the block: “Empathy refers to the ability to understand and feel to a lesser degree what another is experiencing”. Each trial started with a fixation cross presented for 1000 ms. The 24 stimuli (i.e., videos of the eight virtual agents expressing three different affective states each) were presented three times for the Empathy and Intensity blocks (72 trials per block) and only once for the Recognition block (24 trials). After the presentation of each stimulus, participants rated their felt empathy for the virtual agent using a VAS ranging from “No empathy” to “Maximum empathy” (1-100) in the Empathy block, or the intensity level perceived on a VAS ranging from “No intensity” to “Maximum intensity” (1-100) in the Intensity block. In each block, the VAS was displayed until a response was confirmed by pressing the space bar. In the Recognition block, the participant identified the emotional states (i.e., affective states) perceived among the following three choices: “Neutral”, “Pain”, or “Sadness”. Response order was counterbalanced between participants. The choices were displayed until a response was confirmed by pressing the space bar. Computer Task Trial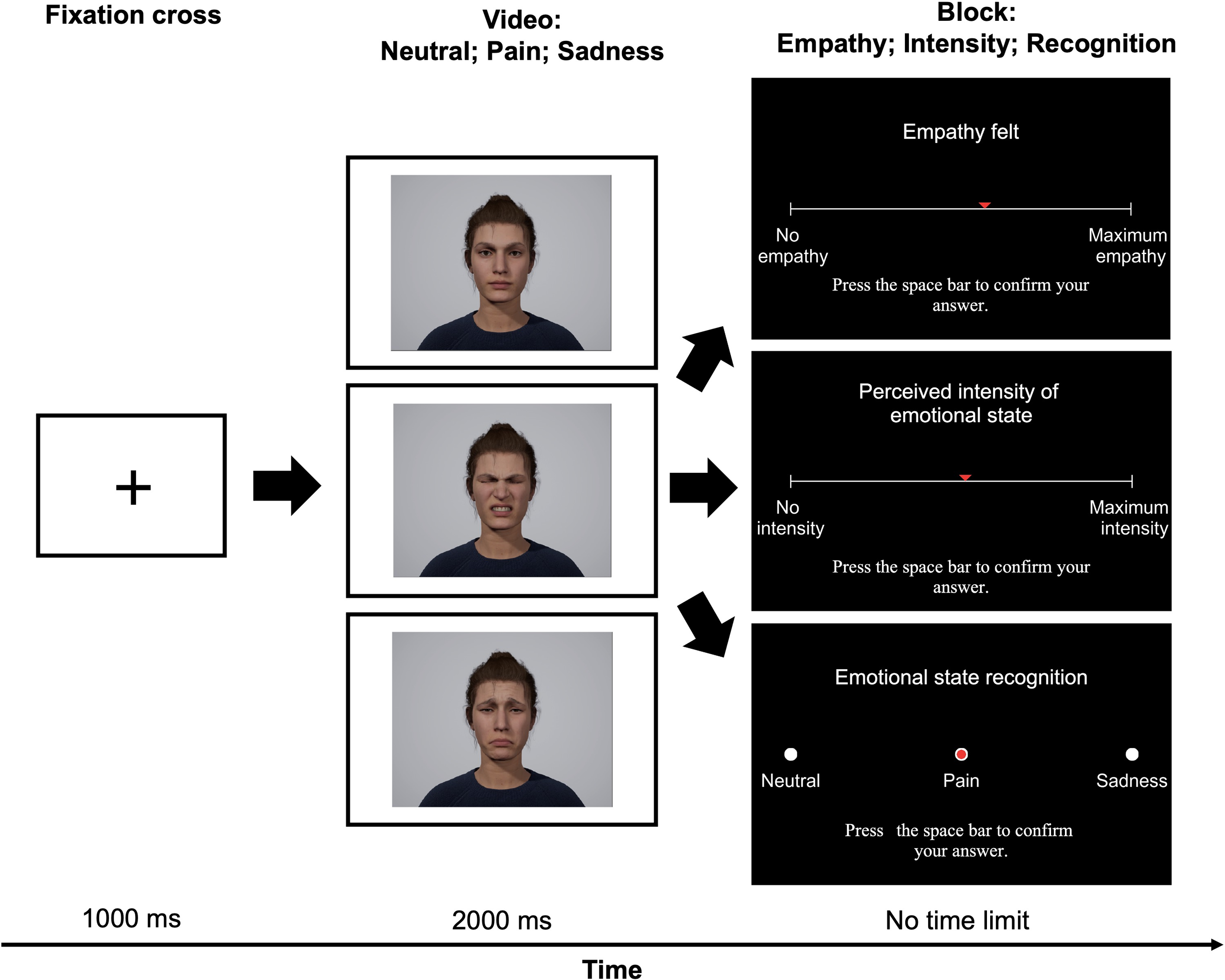
After the task, participants filled out the LSNS and PHQ-9 questionnaires. Participants who had not previously responded to the sociodemographic questionnaire and the UCLA-LS and IRI scales completed these measures at that moment (i.e., participants who had not completed the online questionnaires prior to the in-person experiment). The in-person experiment lasted approximately between 45 and 60 minutes.
Analyses
Data Preprocessing and Manipulation Checks
All statistical analyses were performed using SPSS (IBM, Corp.) with a significance threshold set at α = .05. The online survey only included the trait questionnaires for the PSI and empathy. No significant differences in levels of trait PSI (t (64) = .196, p = .845) or any aspects of trait empathy (PT: t (64) = −1.211, p = .230; FS: t (64) = 1.346, p = .183; EC: t (64) = .021, p = .983; PD: t (64) = 1.241, p = .219) were found between groups based on data collection method. Accordingly, individuals (n = 28) who completed specific questionnaires remotely (sociodemographic, UCLA-LS, and IRI) and later participated in an in-person experiment did not differ from those (n = 38) who completed all questionnaires and the experiment in a single in-person setting.
No data were missing for the analyses, and no participants were excluded due to univariate or multivariate outliers. Neutral facial expressions were not included in the planned analyses, as they were used solely to verify participants’ understanding of the task (i.e., by examining whether neutral facial expressions were indeed perceived on average as more intense than painful or sad ones) and were not part of any objective or hypothesis. No participants were excluded based on this criterion, and descriptive statistics for the full sample (N = 66) revealed a clear distinction between average ratings of empathy (M = 13.70, SD = 15.90) and intensity (M = 7.07, SD = 10.70) for neutral expression, and non-neutral expressions (empathy for pain: M = 58.00, SD = 21.20; intensity for pain: M = 71.20, SD = 17.90; empathy for sadness: M = 58.30, SD = 23.00; intensity for sadness: M = 57.90, SD = 19.90). The normality of the data distribution for all analyses was verified by visual inspection of the residual distribution. No data set needed to be transformed to normalize the distribution.
Based on a median split of the score distribution, two subgroups were created to binarize the trait PSI variable and enable group comparisons: UCLA-LSHigh (UCLA-LS >37) and UCLA-LSLow (UCLA-LS ≤37). Although dichotomizing continuous variables is generally discouraged due to loss of statistical power (Cohen, 1983), it remains a common and acceptable practice in psychological research to facilitate group comparisons and for clarity in interpretation (DeCoster et al., 2011). A median split was used to create two equal groups, allowing for the inclusion of individuals across the full range of trait PSI scores. This approach yields a sample that is more representative of the general population than one composed solely of individuals with extreme scores. The absence of a clear consensus in the literature regarding cut-off values for high and low trait PSI supported this decision (Cacioppo & Patrick, 2008). Recent studies on trait PSI also used this method (e.g., Arnold & Winkielman, 2021; Baek et al., 2023). As expected, participants in the UCLA-LSHigh subgroup (M = 47.42, SD = 7.37) showed significantly higher levels of trait PSI than those in the UCLA-LSLow subgroup (M = 30.48, SD = 4.41), t (64) = −11.33, p < .001, d = 2.79). The score distribution (ranging from 21 to 63) and effect size were comparable to those reported in prior studies also using a dichotomized trait PSI variable with the same questionnaire (Arnold & Winkielman, 2021; Cacioppo et al., 2016).
Independent samples t-tests and χ2 tests were performed on the sociodemographic variables with the binarized trait PSI variable as the group factor to assess equivalency. No significant differences were found between the subgroups for any sociodemographic characteristics (see Table 1; all ps > .05). Additionally, no significant differences were observed between subgroups in terms of empathy (t (64) = −1.30, p = .198) and intensity (t (64) = −1.40, p = .166) mean ratings for the neutral facial expression used to control participants’ understanding of the task.
Recognition rates in the computer task were calculated to check that stimuli were adequately recognized. Rates obtained were similar for painful (M = 98.87 %, SD = 4.63 %), sad (M = 98.77 %, SD = 4.80 %), and neutral facial expressions (M = 97.35 %, SD = 9.44 %). These recognition rates were high above the chance level (33.33%). Scores for all VAS (i.e., state PSI, empathy and intensity ratings) were obtained by transposing the cursor position into pixels on a scale of 1 to 100.
Hypotheses Testing
Group comparisons analyses were first computed using the binarized trait PSI variable as the group factor. A series of t-tests were carried out on all mean scores of the questionnaires assessing psychological characteristics, including trait empathy and state PSI mean ratings, to respond in part to the first objective. To respond to both the first and second objectives, the primary analysis conducted was a 2 (Facial Expression: Pain, Sadness) x 2 (Group: UCLA-LSHigh, UCLA-LSLow) mixed MANOVA, which was performed on empathy and intensity mean ratings. Univariate tests and pairwise comparisons with Bonferroni correction were performed to decompose the effects.
To address the limitations associated with dichotomization, complementary relationship analyses were also conducted using the non-binarized continuous trait PSI variable. Pearson’s correlation coefficients were computed to identify whether there were significant associations between the main dependent measures (i.e., state and trait empathy, and intensity of affective state) and potential predictors, including non-binarized trait PSI, and confounding variables (i.e., state PSI, OSI, and depressive symptomatology). If so, linear regressions (standard or stepwise, depending on the number of predictors) were carried out.
Results
Trait Empathy
Mean scores of the questionnaires for each subgroup (low and high on UCLA-LS) are shown in Table 1, including IRI subscales. There was a significant difference between subgroups in IRI-PT (t (64) = 2.32, p = .024, d = 0.57), and IRI-PD scores (t (64) = −2.71, p = .009, d = 0.67). Participants in the UCLA-LSHigh subgroup showed lower levels of perspective-taking than those in the UCLA-LSLow subgroup (M = 18.18, SD = 5.00 vs. M = 20.85, SD = 4.33, respectively) but higher levels of personal distress (M = 12.67, SD = 5.21 vs. M = 9.33, SD = 4.78, respectively). No significant differences were detected between subgroups for IRI-F and IRI-EC (all ps > .05). Other questionnaire results are discussed in the Confounding Influence of Situational Perceived Social Isolation PSI, Objective Social Isolation, and Depressive Symptomatology section.
State Empathy and Perceived Intensity of Affective State
Empathy and intensity mean ratings can be found in Figure 2. There was no significant effect of Group (Pillai’s Trace = .006, F (2, 63) = 0.196, p = .822) on empathy and intensity means ratings. There was a significant effect of Facial Expression (see Figure 2; Pillai’s Trace = .402, F (2, 63) = 21.188, p < .001, ηp2 = .402). The effect was significant for intensity (F (1, 64) = 28.224, p < .001) but not empathy (F (1, 64) = 0.006, p = .936). The pain facial expression was perceived as more intense than the sadness facial expression (p > .001). There was no significant interaction between Group and Facial Expression (Pillai’s Trace = .011, F (2, 63) = 0.342, p = .712). Empathy and Intensity Mean Ratings according to the Affective State and Trait Perceived Social Isolation Subgroup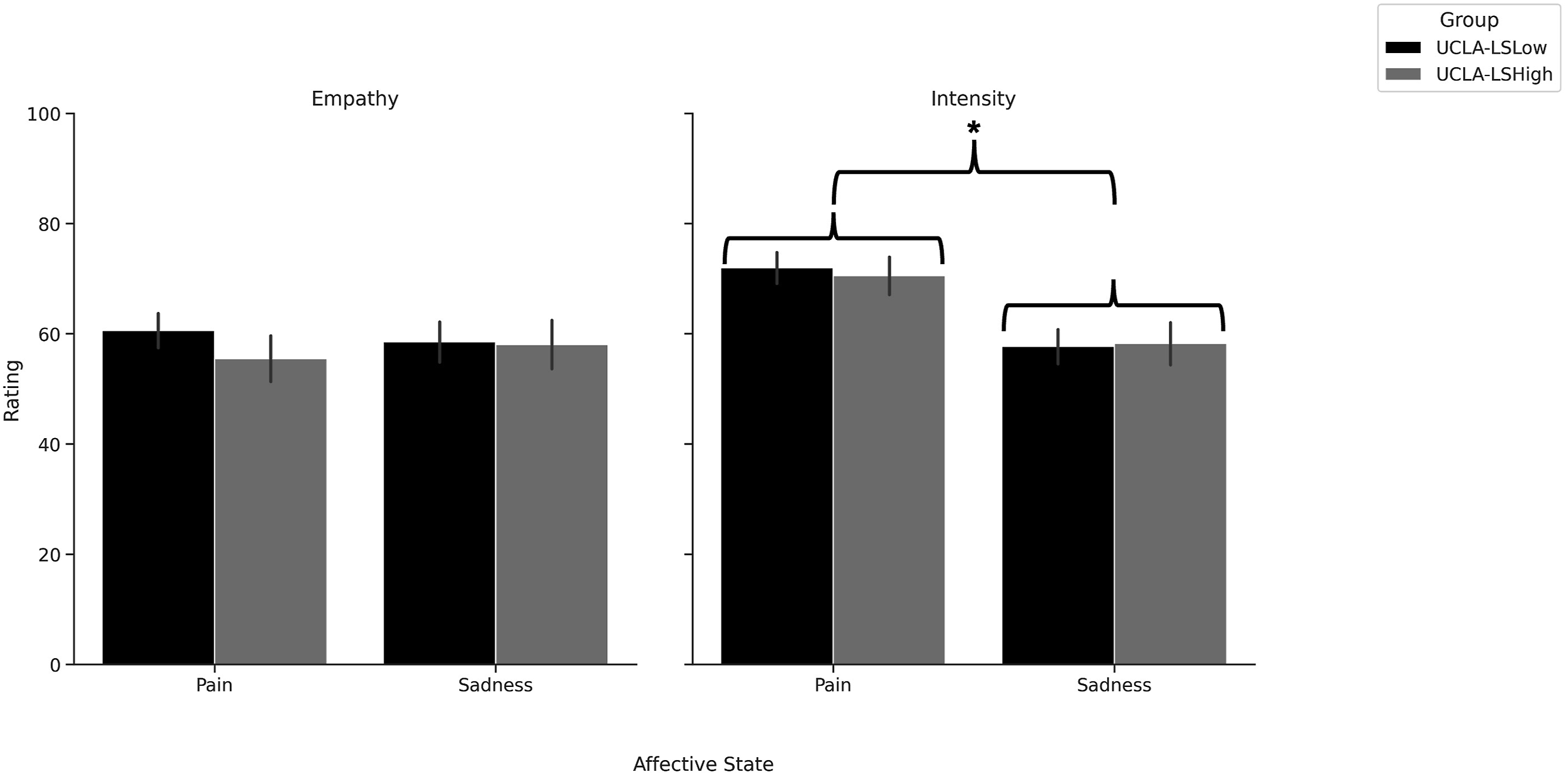
Confounding Influence of Situational Perceived Isolation, Objective Social Isolation, and Depressive Symptomatology
Social network levels, including frequency of interpersonal contacts, were significantly higher (t (64) = 2.37, p = .021, d = 0.58) in the UCLA-LSLow subgroup (M = 45.39, SD = 9.77) compared to the UCLA-LSHigh subgroup (M = 39.64, SD = 9.98), meaning less OSI in the UCLA-LSLow subgroup and more OSI in the UCLA-LSHigh subgroup. No significant differences were detected between subgroups for PHQ-9, PANAS-N, and PANAS-P scores (all ps > .05). Participants in the UCLA-LSHigh subgroup (M = 50.90, SD = 24.34) reported significantly higher state PSI (t (64) = −3.15, p = .002, d = 0.78) compared to those in the UCLA-LSLow subgroup (M = 31.68, SD = 25.24).
Correlations Between Mean Scores of the Questionnaires and Computer Task Mean Ratings
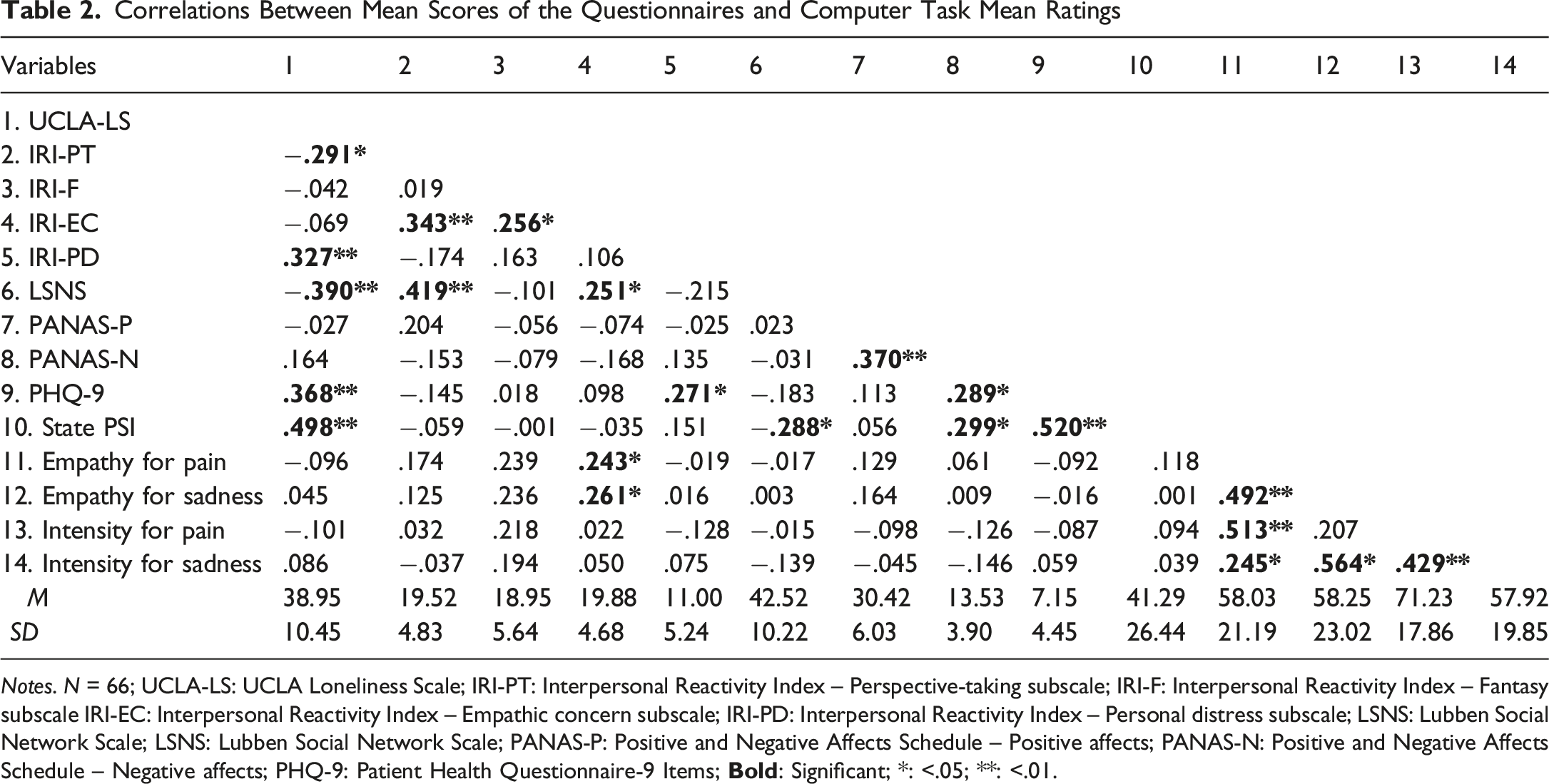
Notes. N = 66; UCLA-LS: UCLA Loneliness Scale; IRI-PT: Interpersonal Reactivity Index – Perspective-taking subscale; IRI-F: Interpersonal Reactivity Index – Fantasy subscale IRI-EC: Interpersonal Reactivity Index – Empathic concern subscale; IRI-PD: Interpersonal Reactivity Index – Personal distress subscale; LSNS: Lubben Social Network Scale; LSNS: Lubben Social Network Scale; PANAS-P: Positive and Negative Affects Schedule – Positive affects; PANAS-N: Positive and Negative Affects Schedule – Negative affects; PHQ-9: Patient Health Questionnaire-9 Items;
As for the IRI subscale scores, IRI-PT was significantly negatively associated with UCLA-LS (r (64) = −.291, p = .018; small effect size) but positively with LSNS (r (64) = .419, p < .001; moderate effect size) scores. IRI-EC was significantly positively associated with LSNS (r (64) = .251, p = .042; small effect size) scores, and IRI-PD was significantly positively associated with UCLA-LS (r (64) = .327, p = .007; small to moderate effect size) and PHQ-9 (r (64) = .271, p = .018; small effect size) scores. State PSI was not related to any IRI subscales scores (all ps >.05). No significant associations (all ps > .05) were found between IRI-F scores and potential predictors. As for other questionnaires, UCLA-LS scores were significantly negatively associated with LSNS (r (64) = −.390, p = .001; small to moderate effect size), and positively with PHQ-9 (r (64) = .368, p = .002; small to moderate effect size) and State PSI (r (64) = .498, p < .001; moderate effect size) scores. LSNS scores were significantly negatively related to State PSI scores (r (64) = −.288, p = .019; small effect size). Finally, PHQ-9 were significantly positively related to PANAS-N (r (64) = .289, p = .018; small effect size) and State PSI (r (64) = .520, p < .001; moderate effect size) scores.
Multiple linear regressions were then carried out to predict the three IRI subscale scores (i.e., IRI-PT, IRI-EC, and IRI-PD) associated with potential predictors found in the correlation analyses. A stepwise multiple regression was carried out to predict IRI-PT scores with UCLA-LS and LSNS scores as predictors. The model was statistically significant (R = .419, p < .001) with 16% variance explained (adjusted-R2 = .163). UCLA-LS was excluded (p > .05) from the final model, which contains only LSNS as a predictor (β = .419, p < .001). A standard regression was carried out to predict IRI-EC scores because LSNS scores were the sole predictor. The model was statistically significant (R = .251, p < .042) with 4.8% variance explained (adjusted-R2 = .048). A stepwise regression was carried out to predict IRI-PD scores with UCLA-LS and PHQ-9 as predictors. The model was statistically significant (R = .327, p = .007) with 9.3% variance explained (adjusted-R2 = .093). PHQ-9 was excluded (p > .05) from the final model, which contains only UCLA-LS as a predictor (β = .327, p = .007). The final models of the three regressions are illustrated in Figure 3. Results of the Regression Models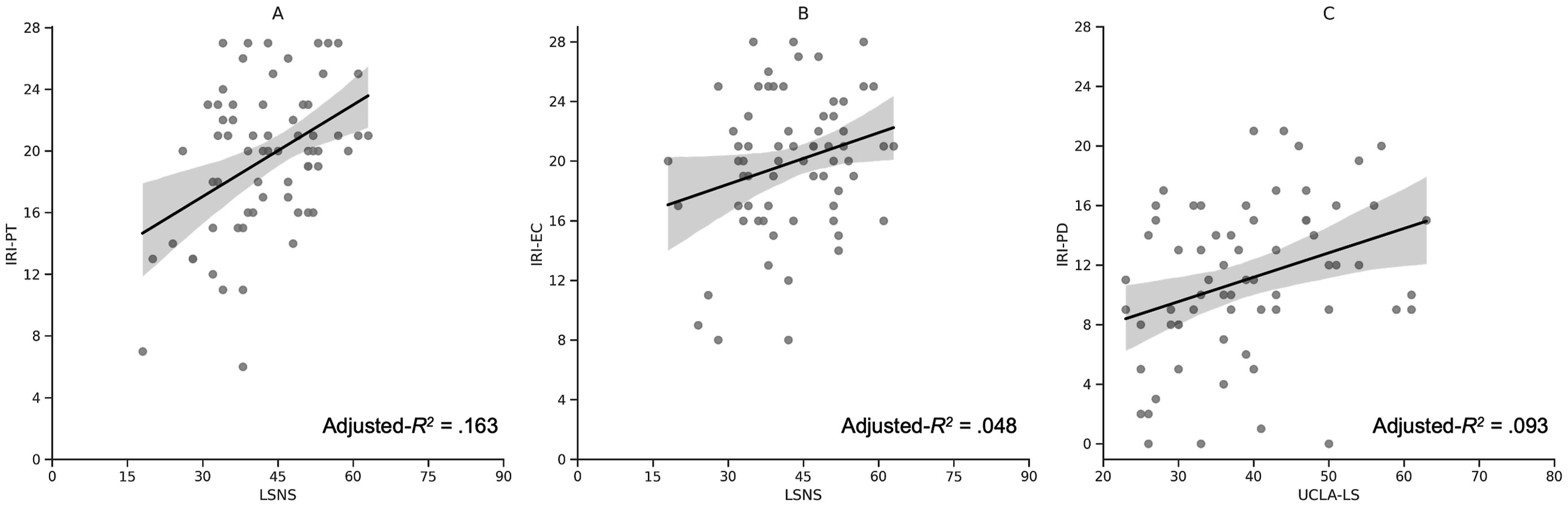
Discussion
This study aimed to identify factors contributing to trait PSI by assessing its relationship with components essential to maintaining and developing interpersonal relationships, namely empathy and the perception of suffering in others. The study also considered various confounding factors, such as state PSI, OSI, and depressive symptomatology.
Objective and Subjective Social Isolation Predict Distinct Aspects of Trait Empathy
It was hypothesized in the first objective that trait empathy, regardless of its specific aspect, would be lower in individuals with high-trait PSI and that this difference would not be accountable by other variables. As expected, the tendency to spontaneously adopt the view of others (i.e., perspective-taking) was lower in individuals with high-trait PSI. Still, it was found that the objective facet of social isolation contributes the most to perspective-taking, even if a person feels isolated. The contribution of PSI trait levels was thus negligible when OSI was also considered, consistent with a recent study (Mwilambwe-Tshilobo et al., 2023). According to Davis (2017), perspective-taking is essential in interpersonal relationships and is frequently positively associated with relationship quality indicators (e.g., global relationship satisfaction) and different types of relationship support. Contrary to expectations, we did not find any difference in empathic concern (i.e., “other-oriented” feelings of sympathy and concern for unfortunate others) levels between the subgroups. Furthermore, a significant but weak relationship was found between empathic concern and OSI, but no association was found between empathic concern and trait PSI. Other authors also found that empathic concern shows only weak associations with measures of relationship quality (Davis, 2017). These first two results suggest that specific aspects of trait empathy (i.e., perspective-taking and empathic concern) may play an essential role in having an actual broader social circle but are unrelated to its subjective perception. According to Morelli et al. (2017), people with high trait empathy are central to social networks characterized by trust among members, suggesting that empathy supports close relationships and may ultimately lead to additional and stronger social bonds. Still, it seems that specific aspects of trait empathy, such as perspective-taking, may be more critical than others. Moreover, Fu et al. (2022) showed that social support mediated the relationship between prosocial behaviour and trait empathy. Thus, promoting social support could ultimately enhance prosocial actions, such as helping behaviour to alleviate the distress of others, which some authors argue would be the primary purpose of an empathic response (Batson et al., 2015).
As predicted, participants with high-trait PSI reported greater personal distress, reflecting “self-oriented” feelings of personal anxiety and unease in tense interpersonal settings, compared to those with low-trait PSI, even after controlling for depressive symptoms. This result could be explained by emotional dysregulation in individuals showing high-trait PSI, who may exhibit poor cognitive and behavioural strategies (e.g., rumination, catastrophizing, blame attribution, less use of cognitive reappraisal, and active rejection or withdrawal from others; Preece et al., 2021). Emotional dysregulation in individuals with high-trait PSI may increase discomfort in tense interpersonal settings and heighten focus on their own distress. One key aspect of emotional regulation is the ability to differentiate between self and others. Although participants did not report any psychiatric disorders, some may have experienced psychological symptoms linked to reduced self-other distinction, contributing to elevated personal distress. Beyond depression, conditions such as social anxiety (Sun et al., 2024) and schizotypy (Badcock et al., 2016) have been associated with trait PSI. Personal distress may also predict schizotypal traits, including excessive social anxiety, cognitive disorganization, and ideas of reference, possibly due to impaired self-other distinction (Eddy, 2025). This confusion may lead to difficulty identifying the origin of one’s own thoughts, emotions, and actions. However, this explanation seems less applicable to trait PSI, as neuroimaging evidence indicates that individuals high in trait PSI exhibit lower self-other overlap (Courtney & Meyer, 2020). More personal distress in high-trait PSI individuals could also, in part, be attributable to self-centeredness. According to Cacioppo et al. (2017), trait PSI increases implicit motivation for self-preservation and predicts self-centeredness in the subsequent year. This chronic tendency to self-centeredness could thus lead individuals with high-trait PSI to focus more on their distress rather than on that of others.
State Empathy and Sensitivity to Suffering Unrelated to Perceived Social Isolation
Contrary to the first hypothesis, individuals with high-trait PSI did not report diminished state empathy compared to individuals with low-trait PSI. These results are inconsistent with those reported in other studies manipulating feelings of PSI (Hu et al., 2020) or social exclusion (DeWall & Baumeister, 2006; Twenge et al., 2007), possibly due to design differences. For instance, trait and state PSI were measured in the present study rather than experimentally manipulated by a recall task, as in Hu et al. (2020)’s study. Thus, eliciting feelings of PSI may only temporarily blunt the empathic response, which would be more similar to the experience of social exclusion than to trait PSI (DeWall & Baumeister, 2006; Twenge et al., 2007), reinforcing the idea that social exclusion and PSI differ. The divergence in results could also be explained by the differentiation between empathic ability and the spontaneous tendency to express it (i.e., empathic propensity), as proposed by some authors (Keysers & Gazzola, 2014; Rameson et al., 2012; Tremblay et al., 2020). For instance, Tremblay et al. (2020) showed that an instruction to actively empathize compared to a passive observation could increase empathy ratings for individuals with lower empathic propensity (e.g., people with high autistic, alexithymic, or psychopathic traits). The paradigm used to probe empathy (i.e., the empathy selection task) by Hu et al. (2020) differed from the one used in the present study in which participants were instructed to empathize with the target actively. Thus, individuals with high-trait PSI may have a lower propensity for empathy that can be circumvented when asked to empathize with a target actively. Moreover, it is also possible that the relationship between trait PSI and state empathy is context dependent. For instance, individuals with high-trait PSI could be less likely to be empathic in a context where they feel emotionally overwhelmed. This would make sense, as one of our first results showed that individuals with high-trait PSI were more prone to personal distress. As Kim and Han (2018) proposed, personal distress could block empathic interaction instead of enhancing it.
It was also hypothesized that individuals with high-trait PSI would perceive higher intensity in facial expressions depicting physical and emotional suffering compared to individuals with low-trait PSI. This hypothesis was refuted, as participants perceived the same level of intensity regardless of the group to which they belonged. This result does not align with those reported in studies by Smith et al. (2022) and Vanhalst et al. (2017). This incongruity could once again be due to methodological discrepancies. The methods used by Smith et al. (2022) and Vanhalst et al. (2017) were implicit (i.e., time response and categorization) in comparison to the one used in the present study, in which intensity was operationalized as an explicit measure using a VAS ranging from “No intensity” to “Maximum intensity”. Trait PSI may be related to subtle differences in facial emotional decoding that need to be assessed using more implicit measures that may give higher sensitivity. Finally, social desirability could also explain the absence of a difference in perceived intensity between individuals presenting distinct levels of trait PSI. This interpretation can also be applied to empathy. Regardless of trait PSI, all participants could have been prone to social desirability, as the measures used were explicit, which may have been a problem, especially as society values empathy (Kämpfe et al., 2009).
Strengths, Limitations, and Future Perspectives
To our knowledge, this study is the first to examine in the same experiment the relationships between PSI, empathy, and sensitivity to the suffering of others. This study has the strength to distinguish PSI as a state or a trait and to explore their associations in a behavioural experiment without manipulating PSI feelings. PSI can be transitional or prolonged over time, and it is a problematic psychological construct to manipulate in an experimental setting without changing its nature. PSI is sometimes inferred to stem from the manipulation of social exclusion. However, this approach is problematic, since PSI can originate from various reasons beyond being excluded. Controlling confounding factors, such as OSI, allowed better targeting of the specific facet of social isolation at stake. Virtual agents also gave more significant control over the facial expressions employed, which can be easily reproduced to ensure replicability.
Notwithstanding these strengths, this study has several limitations, for which future directions are suggested. Its cross-sectional design first precludes inference of causal relationships. Longitudinal research could provide a more comprehensive assessment of PSI and empathy over time. Other key factors frequently associated with PSI, such as social anxiety or social avoidance (Sun et al., 2018), schizotypal traits (Badcock et al., 2016; Eddy, 2025) and autism spectrum disorder (Grace et al., 2022), age (Terán-Mendoza & Cancino, 2025), and culture (Barreto et al., 2021), were not considered and should be included in future work. For example, misperceptions in social anxiety can interact with those associated with PSI and worsen social difficulties (Fung et al., 2017). Clinical samples may also help clarify the link between loneliness and empathy by amplifying differences in loneliness levels. Moreover, self-report measures assessing empathy are prone to subjectivity and social desirability bias (Neumann et al., 2015). Including a social desirability questionnaire in future studies could mitigate such influence.
As previously described, virtual agents offer several advantages. Still, the results may not fully translate to dynamic real-world interactions. Conducting dyadic studies could help bridge this gap. The empathy task did not distinguish between cognitive, affective, and emotional regulation components, making it unclear which best predicts trait PSI. Evidence from specific populations (e.g., autism spectrum disorder; Fatima & Babu, 2024) suggests specific components may be more affected in individuals with high PSI (e.g., Preece et al., 2021). Using separate VAS could help clarify this. While facial expressions are effective in eliciting empathy, the results may also not generalize to other stimuli, such as voices. People may infer emotions more accurately from voices than from faces (Kraus, 2017). Whether the PSI-empathy relationship varies by stimulus type is yet to be determined. Finally, the overlap between social exclusion, OSI, and PSI (both trait and state) remains unclear. Comparing subgroups (e.g., individuals with experience of social exclusion, those with high OSI, and those with high PSI) could help distinguish these constructs.
Conclusion
Overall, this study highlights the importance of distinguishing objective and perceived social isolation when examining their relationships with social skills, such as empathy. The results also reinforce the idea that social skills may play an essential role in maintaining and developing relationships but are not related to one’s perception of their quality. This study ultimately enhances the understanding of the distinct aspects of social isolation and trait empathy. These findings are an essential first step toward developing interventions to promote specific aspects of empathy and enhance social support, and thus, mitigate the negative impacts of social isolation within the population.
Footnotes
Ethical Considerations
The study was approved by Université Laval’s ethics committee (#2022-483) on February 6, 2023.
Consent to Participate
All participants voluntarily gave their written informed consent for their participation.
Author Contributions
EG: conceptualization, methodology, acquisition of data, analysis, and interpretation of data, and writing of the original draft. AM: interpretation of data. MHT: virtual agents’ creation and validation, and interpretation of data. PLJ: conceptualization, funding acquisition, supervision, and interpretation of data. All authors contributed to critically revising the paper and approved the final paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: EG, AM, and MHT received scholarships from the Natural Sciences and Engineering Research Council of Canada and the Fonds de Recherche du Québec—Nature et Technologies. This work was supported by grants from the Canada Foundation for Innovation and the Natural Sciences and Engineering Research Council of Canada awarded to PLJ.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.