
Abstract
Although loneliness is typically associated with adolescence and old age, research has revealed that it is prevalent across the life span. The present study contributes to the loneliness literature by investigating a broad range of risk factors in a Dutch sample (N = 52,341) ranging from late adolescence to old age using a cross-sectional survey administered by the regional public health services in the province of Limburg in the Netherlands. Risk factors associated with higher levels of self-reported loneliness across the life span were being male, lower education levels, inadequacy of financial resources, mental health, informal caregiving that is experienced as burdensome, and limited social contact or network type. In addition, in early adulthood, having a non-western migration background and having a physical disability were associated with higher levels of loneliness, whereas living alone, having a non-western migration background, and not having a paid job were risk factors of loneliness in middle adulthood. In late adulthood, living alone and having a physical disability were associated with loneliness. The present study demonstrates that different stages of life are associated with different vulnerability factors of loneliness. Hence, the prevention of loneliness might require different interventions in different age groups.
Interpersonal relations are a fundamental human need (Baumeister & Leary, 1995). The painful feeling that is experienced when the quantity or quality of one’s social relationships is perceived as deficient is called loneliness (Peplau & Perlman, 1982). Hence, loneliness is an unpleasant emotional state that is linked with psychological well-being (Peplau & Perlman, 1982; Weiss, 1973). According to the evolutionary theory of loneliness, the adaptive functions of loneliness that promote short-term survival can harm physical and mental health in the long term (Cacioppo & Cacioppo, 2018). Indeed, loneliness has been found to increase the risk of premature mortality (Holt-Lunstad et al., 2015) and has been associated with severe mental health disorders (Nuyen et al., 2019) for example. The negative consequences of loneliness emphasize the importance of social connectedness and the need for targeted interventions to combat loneliness (Masi et al., 2011).
Despite a persistent stereotype associating loneliness with older adults (Tornstam, 2007), research has revealed that loneliness is prevalent in all age groups and peaks in adolescence and early adulthood as well as in old age (e.g., Luhmann & Hawkley, 2016; Pinquart & Sörensen, 2003; Qualter et al., 2015; Victor & Yang, 2012; Weeks & Asher, 2012). Although loneliness is prevalent across the life span, the sources of loneliness might vary with age. From a life-span perspective, the risk factors of loneliness might be expected to differ for different stages in life. Although Erikson’s (1959) stages of psychosocial development present individuals with unique crises, each of these stages is concerned with intra- and interpersonal challenges. Hence, relationships and social interaction are reoccurring themes in psychosocial development and it has been suggested that social effectiveness is what enables individuals to successfully navigate the different developmental stages (Dunkel and Harbke, 2017). This suggests that risk factors associated with relationships and social interaction are universal predictors of loneliness.
On the other hand, the unique interpersonal challenges of each developmental stage might influence the sources of loneliness (Parkhurst & Hopmeyer, 1999; Qualter et al., 2015). For example, young adulthood is characterized by forming intimate relationships, in particular romantic relationships. Hence, having a partner might become an important predictor of loneliness when an individual transitions into young adulthood. Furthermore, one’s personal context could contribute to loneliness if it does not conform with age-related norms (Luhmann and Hawkley, 2016). For example, not having a job in middle adulthood does not conform with age-related expectations (Erikson, 1959), and this non-normative context could increase one’s risk of feeling lonely. Furthermore, an off-time occurrence of life events (e.g., finding a romantic partner) is associated with loneliness (Zoutewelle-Terovan & Liefbroer, 2018). Individuals whose transitions do not conform with norms of ideal timelines have been argued to not have access to immediate social support (Wrosch & Freund, 2001) and to run the risk of becoming stigmatized (Thornton & Young-DeMarco, 2001).
This life-span perspective raises the question as to whether the risk factors of loneliness differ for different age groups. The present study explores the age distribution of loneliness from late adolescence to old age by investigating a broad range of risk factors of loneliness in early, middle, and late adulthood in a nationally representative sample of the Dutch population.
Risk factors of loneliness
Loneliness has been studied from an evolutionary (e.g., Cacioppo & Cacioppo, 2018), neuroscience (e.g., Cacioppo et al., 2014), epidemiological (e.g., Holt-Lunstad et al., 2015), clinical (e.g., Heinrich & Gullone, 2006), and developmental (e.g., Hutten et al., 2021) perspective and has been associated with physical health and clinical outcomes and a variety of risk factors. Although a clear theoretical framework on the relationship between risk factors and loneliness is lacking (Clark et al., 2021), previous studies have established that sociodemographic factors, physical functioning, mental health, societal participation, and social relationships are risk factors of loneliness.
In early adulthood, loneliness is associated with self-reported health, functional status, mental health, and the quantity of social relationships (e.g., Bosma et al., 2015; Victor & Yang, 2012). Sex, marital status, education and income level, self-reported health, functional status, mental health, and the quantity and quality of social relationships have been found to correlate with loneliness in middle adulthood (e.g., Beutel et al., 2017; Hawkley et al., 2008; Victor & Yang, 2012). In late adulthood, loneliness is associated with sex, marital status, having a migration background, household composition, income and education level, self-reported health, functional status, mental health, volunteering, informal caregiving, having a local support network, and the quality of social relationships (Carr et al., 2018; Cohen-Mansfield et al., 2016; de Jong Gierveld et al., 2015; Ekwall et al., 2004; Fokkema & Naderi, 2013; Golden et al., 2009; Victor et al., 2012; Wenger et al., 1996). Finally, previous studies have found a hierarchy among the aforementioned risk factors whereby distal factors such as socioeconomic status have been found to influence loneliness through more proximal factors such as someone’s social interactions (Hawkley et al., 2008).
Although numerous studies have investigated the risk factors of loneliness for a specific age group (e.g., Franssen et al., 2020; Pinquart & Sörensen, 2003; Qualter et al., 2015; Victor & Yang, 2012), several problematic issues come forward in explaining the age differences in loneliness that are addressed by the present study. First, the majority of studies have been conducted among adolescents or older adults leaving middle adulthood relatively understudied (Luhmann & Hawkley, 2016; Mund et al., 2020). Second, studies primarily focused on one age group at a time. Furthermore, the sample and measurement characteristics of these studies differ quite substantially and a comparison of the results—also across nations—is difficult (de Jong Gierveld & Van Tilburg, 2010; Hawkley et al., 2015). Also, most studies used a direct, single-item measure of loneliness asking participants whether they feel lonely. Though direct, single-item measures have been reported to have good face and predictive validity (Routasalo et al., 2009), they are less reliable compared to an indirect scale (de Jong Gierveld & Van Tilburg, 2010) because it requires self-labeling (Jylhä, 2004; Marangoni & Ickes, 1989) and may elicit socially desirable responses.
Luhmann and Hawkley (2016) have been the first to investigate a broad range of risk factors among different age groups using a multi-item loneliness scale in a nationally representative German sample. Although their results revealed that income, functional limitations, social engagement, and the quantity of social relationships were risk factors of loneliness for all ages, other risk factors were found to be age-specific (Luhmann & Hawkley, 2016). In early adulthood, having a part-time job and living alone were associated with lower levels of loneliness after controlling for other covariates. Employment and having a romantic partner were protective factors of loneliness in middle adulthood. In late adulthood, living alone and having a romantic partner were associated with lower levels of loneliness. Given the fact that loneliness rates differ substantially between nations (Yang & Victor, 2011), it is important that these results are replicated in a different sample. The present study aims to replicate these results in a Dutch sample and add to Luhmann and Hawkley (2016) by investigating additional risk factors.
The current study
The existing body of research on the risk factors of loneliness generally agrees that demographics, socioeconomic status, mental health, physical disabilities, societal participation (e.g., having a job, informal caregiving, volunteering) and social contact are correlated with loneliness (e.g., Franssen et al., 2020; Hawkley et al., 2008; Luhmann & Hawkley, 2016; Victor & Yang, 2012). However, little is known about age differences in the risk factors of loneliness. Luhmann and Hawkley (2016) were the first to investigate a broad range of risk factors among different age groups using a multi-item loneliness scale. Although this study is the most comprehensive account of risk factors in different age groups, it is important that these results are verified and replicated in a different sample because loneliness scores have been found to differ between countries (de Jong Gierveld & Van Tilburg, 2010).
The present study will contribute to the literature on loneliness by investigating the prevalence and risk factors of loneliness in a large Dutch sample of adults with ages ranging from 18 to 103. The risk factors included in the study are demographic factors, socioeconomic status, physical disabilities, mental health, societal participation, and social contact. By investigating the risk factors of loneliness in different age groups, the present study is able to explore whether different developmental stages in life are associated with different risk factors of loneliness. Furthermore, this knowledge can be used to design interventions that effectively target loneliness in specific age groups.
Adding to the study by Luhmann and Hawkley (2016), the present study included mental health and informal caregiving as possible risk factors. Although the relationship between loneliness and mental health is bidirectional (Domènech-Abella et al., 2019; Nuyen, et al., 2019), depression might cause loneliness because it is associated with withdrawal and disengagement and impacts intimacy and attachment (McHugh Power et al., 2020). Furthermore, previous studies have consistently demonstrated a strong correlation between depression and anxiety and loneliness. Hence, including mental health when studying risk factors of loneliness is important. Furthermore, informal caregiving might cause loneliness because it can restrict the caregivers’ ability to engage in social activities (Clark & Bond, 2000) or change the caregivers’ spousal relationship when the care recipient is the caregivers’ partner (Beeson, 2003). However, mixed results have been found regarding the association between informal caregiving and loneliness (Beeson, 2003; Ekwall et al., 2004; Vasileiou et al., 2017) and since the level of informal caregiving is rising with the aging population (de Boer et al., 2019), further investigation of this relationship is warranted.
Methodology
Sample
Cross-sectional data from a large epidemiological survey by regional public health services in the south of the Netherlands, the Community Health Services of North and South Limburg (GGD Noord-Limburg and GGD Zuid-Limburg), were used in the study. The data were obtained in 2016 from 60,800 randomly selected local residents and weighted to accommodate regional policymaking. The data from this survey were made available to the researchers for secondary data analysis.
The sample size used in the study was N = 52,341 (53.0% female, age range from 17 to 101 with Mage = 58.4, Mdnage = 63, and SDage = 18.0). Approximately, 3% of the total sample were students. The data were collected by a collaboration of the Netherlands Statistics, the National Institute for Public Health and the Environment (RIVM), and the Community Health Services (GGD) by drawing samples from adult and older adult residents of Limburg. Two different questionnaires were administered to adults and older adults, respectively. Although both questionnaires were very similar, they differed with respect to some measures. Of interest to the current study is the fact that the questions on the frequency of social contact differed between both questionnaires. The sample was split into three different age groups to accommodate the analyses. Consistent with the age groups used in the literature and major developmental stages (Luhmann & Hawkley, 2016), the sample was split into the following age groups: early adulthood (<30), middle adulthood (30–64), and late adulthood (>64).
Measures
Loneliness was measured using the 11-item De Jong Gierveld loneliness scale (DJG) (de Jong Gierveld & Kamphuis, 1985). The scale contains 11 items aimed at assessing both emotional and social loneliness (e.g., “I miss having people around”). The scores range from not lonely (0–2), moderately lonely (3–8), to severely lonely (9–11).
The present study included seven types of loneliness risk factors: demographic variables (age, sex, migration background, and living alone), indices of socioeconomic status (educational attainment and adequacy of financial resources), having a physical disability, mental health, societal participation (having a paid job, informal caregiving, and volunteering), and frequency of social contact (limited contact with family, friends, and acquaintances or neighbors) or network type (locally supported or other).
Age was included as a continuous variable and sex as a dummy variable with 0 = female (reference category) and 1 = male. Migration background was assessed using 13 categories and recoded into the following categories: no immigration background (reference category), western migration background, and non-western migration background. Living alone was included as a dummy variable indicating whether one is living alone with 0 = no (reference category) and 1 = yes. Educational level and inadequacy of financial resources were used as indicators of socioeconomic status. Participants were asked to indicate their highest level of completed education using eight categories ranging from no completed education (0) to scientific education (7). This item was recoded into three categories of completed education levels: low (reference category), middle, and high. To identify inadequacy of financial resources the following question was formulated: “Did you experience any difficulty to make ends meet with your household income the past 12 months?” This question had four response categories ranging from no difficulty at all (0) to yes great difficulty (3) but was recoded into 0 = no difficulty and 1 = yes or somewhat.
Having a physical disability was assessed using seven questions related to vision, hearing, and mobility (e.g., “Are you able to walk 400 m without standing still (with a walking stick if necessary)?”) with four response categories ranging from yes without effort (0) to no I cannot (3) that were recoded into 0 = no impairment related to vision, hearing, or mobility (reference category) and 1 = at least one impairment related to vision, hearing or mobility.
Mental health was assessed using the Kessler Psychological Distress Scale (K10) (Kessler et al., 2002). This scale consists of 10 questions concerning experienced anxiety and depressive symptoms in the past 4 weeks (e.g., “In the past 4 weeks how often did you feel hopeless?”) with response categories ranging from never (0) to always (4). The scores obtained using this scale range from 10–50. This variable was recoded into the following categories: <25 (no or low risk; reference category), 25–29 (moderate risk), and >30 (severe risk; Kessler et al., 2002). Although loneliness has also been associated with other mental health problems (e.g., Nuyen et al., 2019), risk of anxiety and depression was the only mental health factor included in the questionnaires, and thus available for analysis.
The level of societal participation was assessed by asking three questions about one’s roles in society. First, employment status was assessed using 10 categories ranging from yes, I have a paid job for 32 hours or more per week (0) to I am a student (10). This question was recoded into a dummy variable with 0 = not having a paid job (reference category) and 1 = having a paid job for at least 1 hour per week. Second, informal caregiving was assessed with the following question: “Did you provide informal care in the past 12 months?” with two response categories (yes and no). Participants that answered “yes” were subsequently asked how burdened they felt by the care they provided on a 5-point scale ranging from barely or not burdened (0) to overburdened (4). These questions were recoded into a categorical variable with the following categories: no informal caregiving (reference category), informal caregiving that is not considered burdensome and informal caregiving that is considered burdensome. Third, volunteering was assessed using one item with 0 = no volunteering (reference category) and 1 = volunteering.
The frequency of social contact of adults was measured using three questions asking participants how often they had contact with one or more family members/friends or acquaintances/neighbors or people living in the same street with response categories ranging from at least once a week (0) to seldom or never (5). Participants were instructed that contact meant encounters and written, telephone, or e-mail contact. Answers were recoded as three dummy variables with 0 = contact with family/friends/neighbors at least twice a month (reference category) and 1 = contact with family/friends/neighbors less than twice a month.
For older adults, social network type as distinguished by Wenger (1991) was used to investigate their pattern of social contact. Wenger’s typology of social networks consists of five types varying with respect to network size, composition, and function. Participants’ network type was assessed using 10 questions (e.g., “How often do you meet your children or other relatives?”) and included as a categorical variable with the following categories: locally integrated support network (reference category), local family dependent support network, private restricted support network, local self-contained support network, and wider-community focused support network. The locally integrated support network was chosen as reference category because this type of social network was deemed optimal in old age by Wenger.
Data analysis
All analyses were performed using SPSS Complex Samples. This procedure calculates variance estimates by taking into account the non-random sampling design of the survey by weighting for sex, age, city district, household size, income, marital status, and ethnicity. Means and standard deviations of loneliness scores as well as percentage scores for different degrees of experienced loneliness (not lonely, moderately lonely, and severely lonely) were calculated to assess the prevalence of loneliness across the life span. These descriptive statistics were obtained for two sets of age groups: the three age groups described earlier (<30, 30–64, and >64) and smaller, 5-year age groups (starting with 19–24 and ending with 90+). The latter set was added to allow for a more detailed investigation of the age distribution of loneliness.
Linear regression models were used to investigate the risk factors for loneliness for the three age groups. The regression analyses were conducted in six steps corresponding to the different categories of risk factors: demographics, socioeconomic status, physical disabilities, mental health, societal participation, and frequency of social contact or network type. These steps are arranged from the most distal to the most proximal risk factor to investigate to what degree the more distal factors such as socioeconomic status operate through the more proximal factors such as the frequency of social contact.
Results
Descriptive statistics of the variables included in the study for the different age groups distinguished in the analysis.
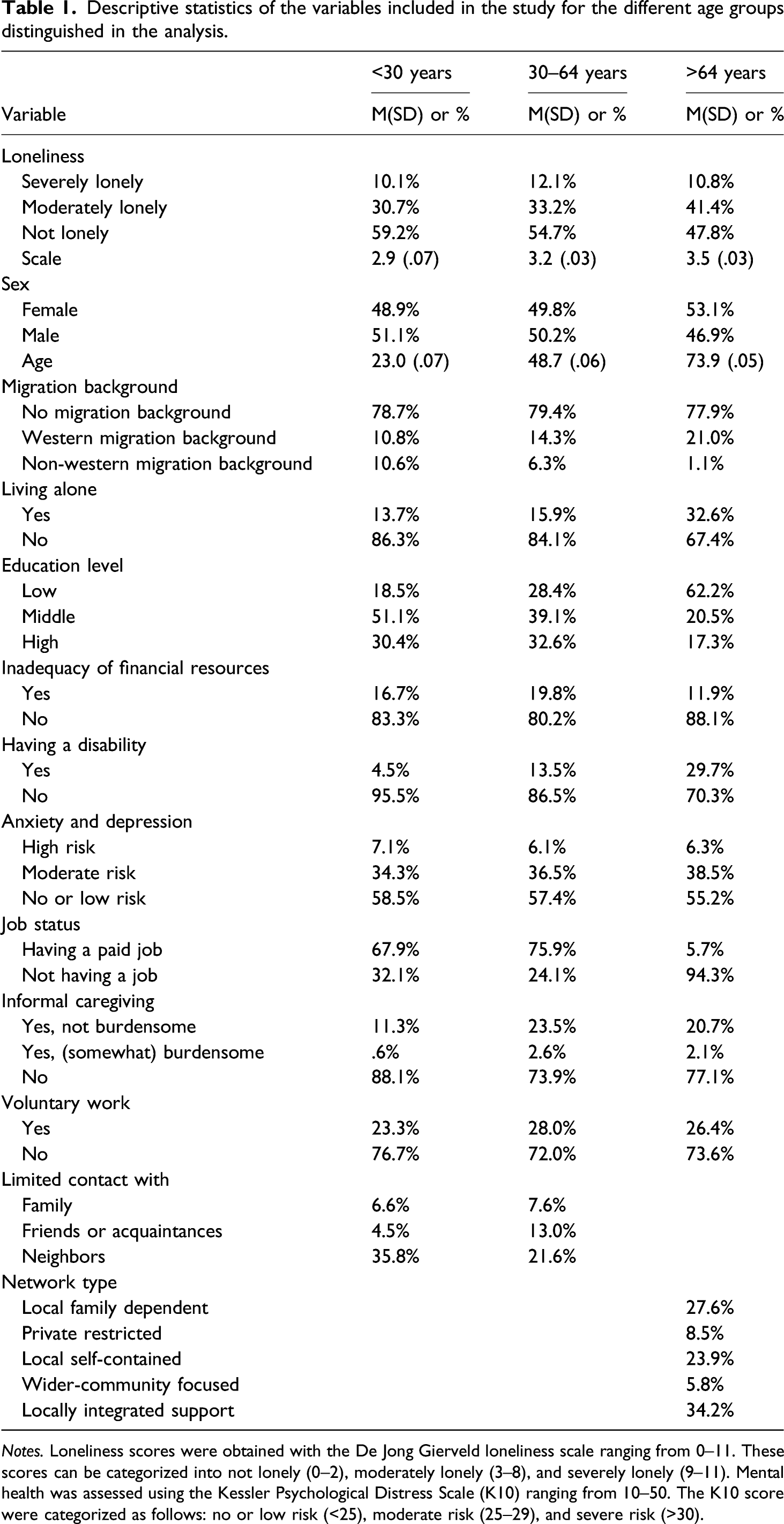
Notes. Loneliness scores were obtained with the De Jong Gierveld loneliness scale ranging from 0–11. These scores can be categorized into not lonely (0–2), moderately lonely (3–8), and severely lonely (9–11). Mental health was assessed using the Kessler Psychological Distress Scale (K10) ranging from 10–50. The K10 score were categorized as follows: no or low risk (<25), moderate risk (25–29), and severe risk (>30).
Age differences in loneliness
The age distribution of loneliness, mean loneliness scores, and the severity of the experienced loneliness were compared for different age groups (Figure 1). The results reveal an upward trend of loneliness scores with increasing age. The mean loneliness scores support this positive linear relationship: 2.9, 3.2, and 3.5 for age group <30, 30–64, and >64 years, respectively. An ANOVA test confirmed that the mean loneliness scores per age group differed significantly, F (2, 47,266) = 42.85, p < .001. The age distribution of loneliness. The bar chart contains the mean loneliness scores per age group. The three lines illustrate the percentage of people experiencing severe, moderate or no loneliness per age groups.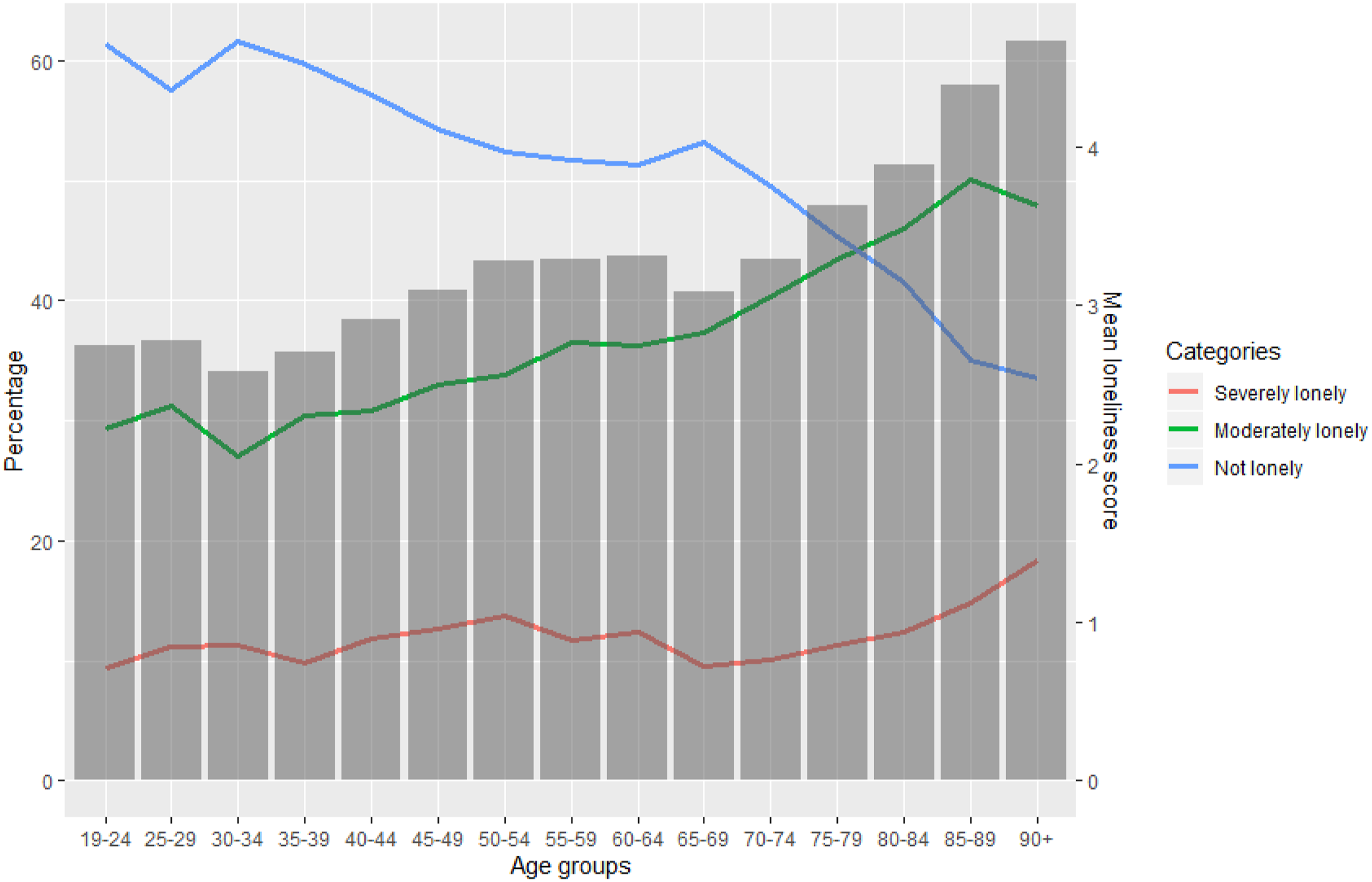
Risk factors of loneliness
Correlations with loneliness for the three age groups.
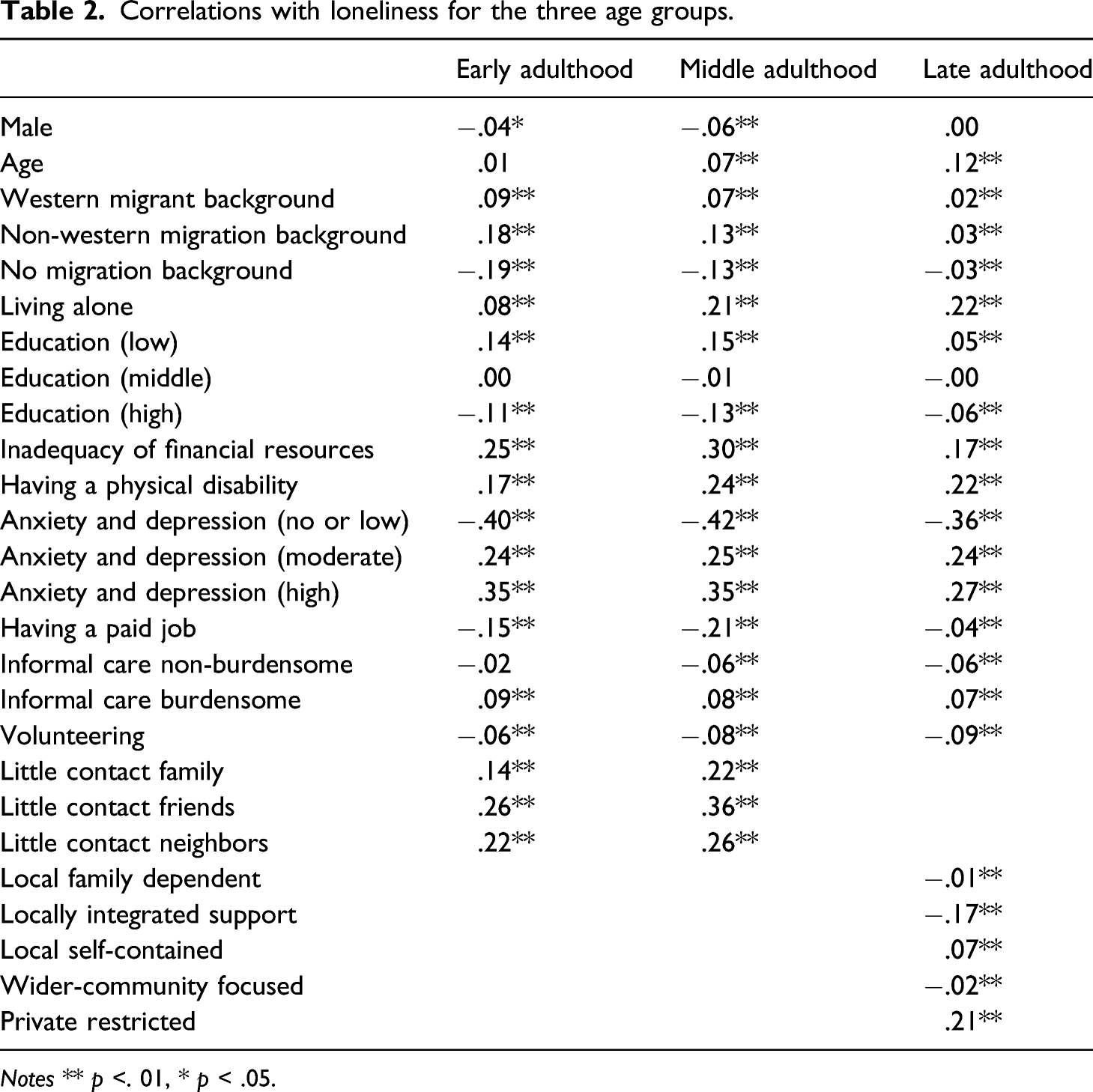
Notes ** p <. 01, * p < .05.
Results of the regression analysis with loneliness as the dependent variable for participants <30 years.
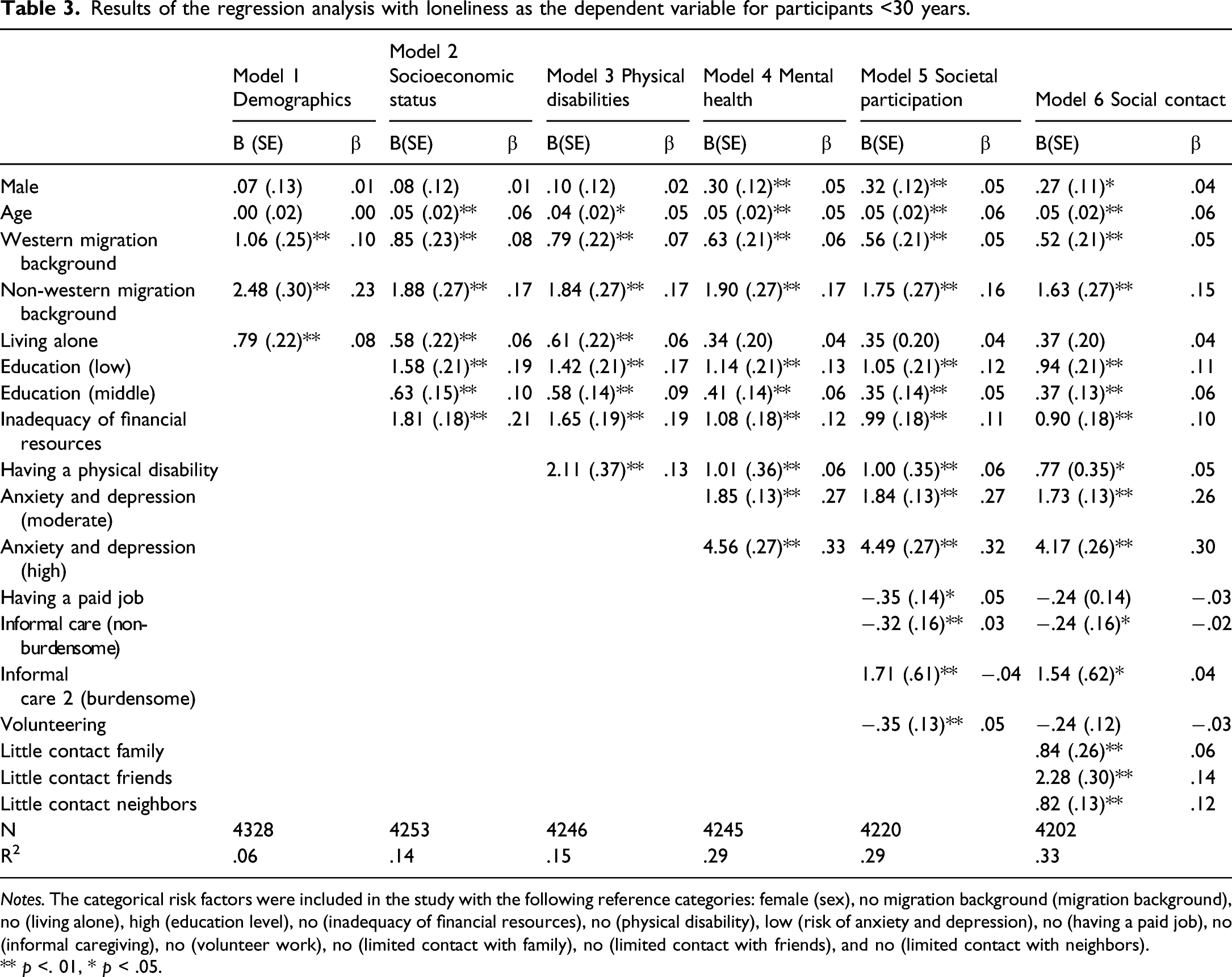
Notes. The categorical risk factors were included in the study with the following reference categories: female (sex), no migration background (migration background), no (living alone), high (education level), no (inadequacy of financial resources), no (physical disability), low (risk of anxiety and depression), no (having a paid job), no (informal caregiving), no (volunteer work), no (limited contact with family), no (limited contact with friends), and no (limited contact with neighbors).
** p <. 01, * p < .05.
Results of the regression analysis with loneliness as the dependent variable for participants 30–64 years.
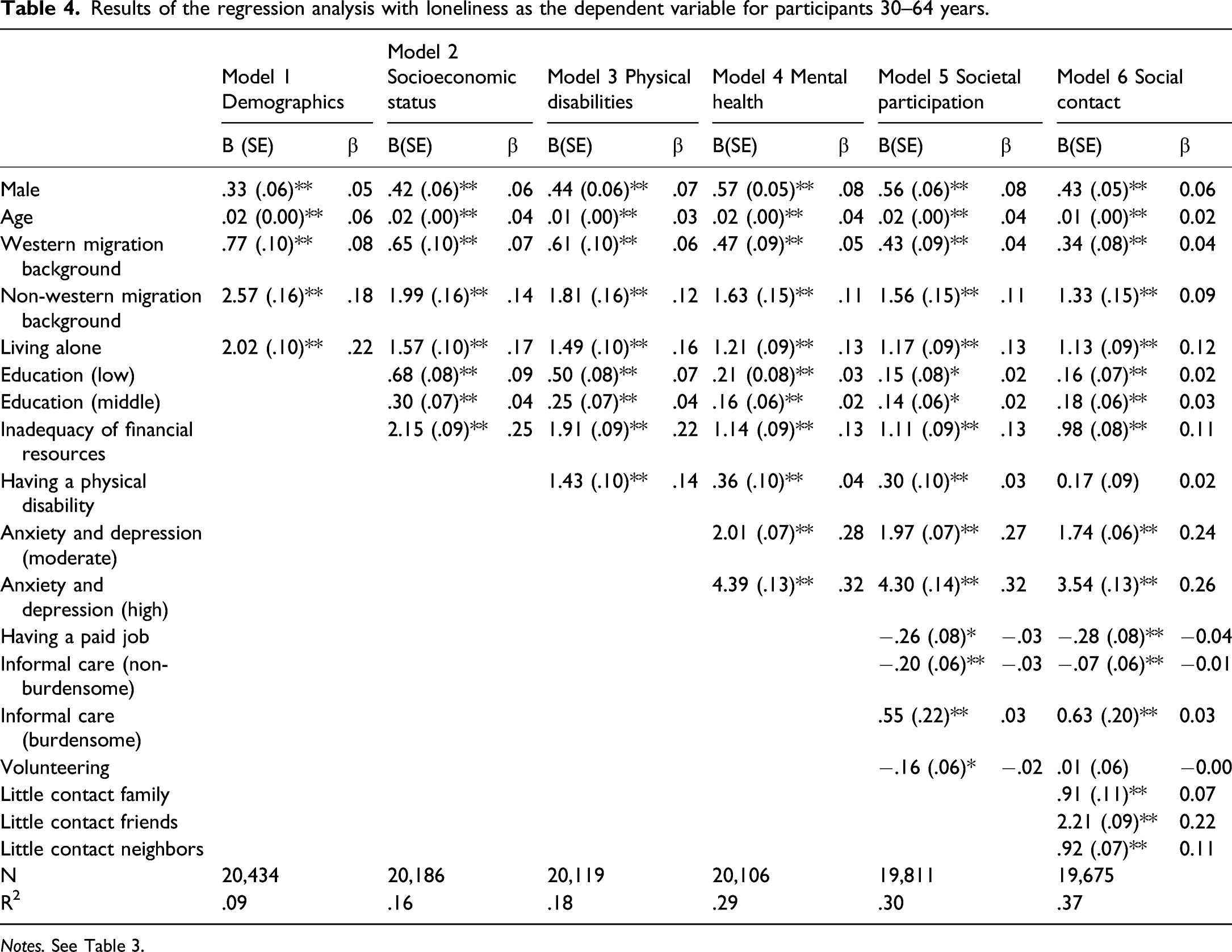
Notes. See Table 3.
Results of the regression analysis with loneliness as the dependent variable for participants >64 years.
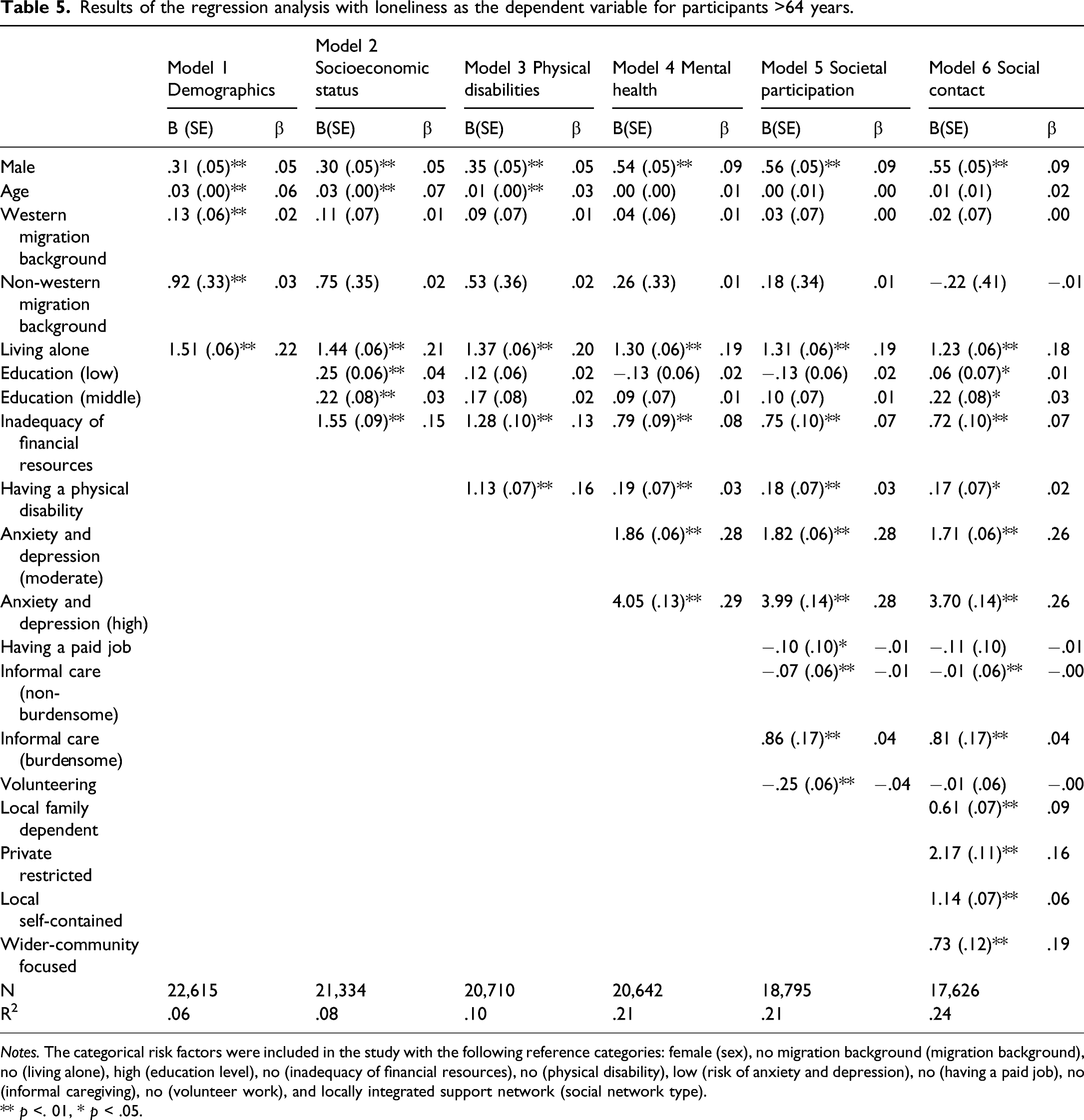
Notes. The categorical risk factors were included in the study with the following reference categories: female (sex), no migration background (migration background), no (living alone), high (education level), no (inadequacy of financial resources), no (physical disability), low (risk of anxiety and depression), no (having a paid job), no (informal caregiving), no (volunteer work), and locally integrated support network (social network type).
** p <. 01, * p < .05.
The standardized beta coefficients of model 6 (see Table 3) reveal that the risk factors of loneliness in early adulthood with the strongest unique contributions are: risk of anxiety and depression for both moderate risk and high risk, having a non-western migration background, having little contact with friends or neighbors, and having inadequate financial resources. Other significant risk factors of loneliness in early adulthood are being male, higher age, low and middle education level, having a physical disability, providing non-burdensome informal care (negative association) and burdensome informal care, and little contact with family. Sex and age only became significant after adding other covariates. Being male was significantly associated with loneliness after controlling for mental health. Age was significantly correlated with loneliness after adding socioeconomic status.
The risk factors of loneliness with the strongest unique contributions in middle adulthood are moderate and high risk of anxiety and depression, little contact with friends, living alone, having inadequate financial resources, and little contact with neighbors (see Table 4). Other significant risk factors of loneliness in middle adulthood are being male, higher age, having a western or non-western immigration background, and low and middle education levels. Furthermore, having a paid job, providing non-burdensome (negative association) or burdensome informal care, and little contact with family were risk factors of loneliness in middle adulthood.
The results of the regression analyses in late adulthood reveal that moderate and high risk of anxiety and depression, living alone and one’s social network (local family dependent, private restricted, local self-contained, wider-community focused) are the risk factors with the strongest unique contributions (see Table 5). Other significant risk factors of loneliness are being male, low and middle education levels, inadequacy of financial resources, having a physical disability, and providing non-burdensome (negative association) and burdensome informal caregiving.
Discussion
The life-span perspective predicts that the risk factors of loneliness differ for different stages in life. To develop interventions that effectively target loneliness (Masi et al., 2011), it is important to understand the risk factors of loneliness across the life span. The present study contributes to the literature on loneliness by investigating a broad range of risk factors of loneliness (demographics, socioeconomic status, having a physical disability, mental health, societal participation, and social contact or network type) in three age groups: early, middle, and late adulthood.
Age as risk factor of loneliness
Mean levels of loneliness differed significantly between the three age groups with the highest levels of loneliness in late adulthood, followed by middle adulthood, and early adulthood. Hence, an increasing trend in mean loneliness levels with age was found, suggesting a linear relationship between age and loneliness. This observation indicates that loneliness is not only an issue in early and late adulthood, as suggested by the quadratic relationship derived from the literature but in middle adulthood as well. Hence, it is important that future research further investigates loneliness in middle adulthood. This upward trend does not support the results obtained by previous studies that found a quadratic (e.g., Victor & Yang, 2012), a non-linear (Clark et al., 2021; Luhmann & Hawkley, 2016), or no relationship (Mund et al., 2020). Taking into account that age ceased to be a significant risk factor of loneliness for older adults after controlling for anxiety and depression, the level of anxiety and depression among the samples of these different studies could be an explanation for these inconsistent results. Furthermore, the prevalence of severe loneliness appears to increase with age from late adulthood onward and to peak in oldest old age (>85).
The observed upward trend of loneliness with age was supported by the regression analyses. After controlling for other covariates, higher age remained a significant risk factor of loneliness in young and middle adulthood. In older adults, the positive relationship between age and loneliness became insignificant after controlling for mental health. This finding reveals that the high levels of loneliness observed among older adults can be explained by a higher risk of anxiety and depression in late adulthood. Hence, old age is not a risk factor of loneliness per se. Rather, the positive association between age and loneliness is a consequence of age-related differences in the risk factors consistent with previous studies (Golden et al., 2009; Luhmann & Hawkley, 2016).
Universal predictors of loneliness
The regression analyses suggested that several factors are related to loneliness across the life span. Mental health, frequency of social contact and network type, informal caregiving, socioeconomic status, and sex were significant correlates of loneliness in the three age groups. A possible explanation for the fact that these risk factors were universal predictors of loneliness might be their ability to directly or indirectly influence an individuals’ relationships or level of social contact. Such an explanation is consistent with the fact that relationships and social interaction are universal themes in psychosocial development (Erikson, 1959).
Similar to the results obtained by Luhmann and Hawkley (2016), low frequency of social contact with family, friends, or neighbors were found to correspond with a higher risk of loneliness in young and middle adulthood. Although objective (e.g., frequency of social contact) and subjective (i.e., loneliness) social isolation are different constructs, this result supports the idea that the two concepts are strongly related. The type of social network was related to loneliness levels in late adulthood. More specifically, having a locally integrated support network was associated with lower levels of loneliness compared to the other four network types. These results are in line with previous research indicating that a local support network is associated with lower levels of loneliness (Golden et al., 2009; Wenger et al., 1996).
The remainder of the predictors might influence social contact and relationships indirectly. Both informal caregiving and inadequacy of financial resources might cause loneliness by influencing the individuals’ spousal relationship. Informal caregiving can change the caregivers’ spousal relationship when the care recipient is the caregivers’ partner (Beeson, 2003) and lower socioeconomic status has been associated with lower levels of marital quality (Sweeney, 2002). Being male might be a risk factor of loneliness across the life span because males have been argued to become lonelier than women from adolescence onward (Koenig & Abrams, 1999). During this developmental transition men tend to replace time spent with their family with spending time alone whereas women seem to replace family time more with time spent with peers (Koenig & Abrams, 1999). Finally, depression might negatively impact one’s relationships and social interaction through withdrawal and disengagement and its impact on intimacy and attachment (McHugh Power et al., 2020). The fact that being male was associated with loneliness across the life span is in line with a meta-analysis by Maes et al., (2016) but contrary to the results by Luhmann and Hawkley (2016). The latter might be attributable to the fact that Luhmann and Hawkley (2016) did not include mental health in their model. The results of the present study revealed that the risk of mental health problems is more prevalent among women than men. 1 Hence, the positive association between being female and loneliness observed by Luhmann and Hawkley (2016) might be explained by their higher risk of mental health problems. Contrary to the results of Luhmann and Hawkley (2016), having a physical disability was not consistently associated with loneliness across the three age groups. For midlife adults, the association between having a physical disability and loneliness became insignificant after controlling for the frequency of social contact, suggesting that the relationship between having a physical disability and loneliness is mediated by the frequency of social contact. Hence, the higher levels of loneliness experienced by those with physical disabilities in middle adulthood might be explained by higher levels of social isolation among the physically impaired.
Age-specific risk factors
Although many factors investigated by the present study were relevant across the life span, some differences between the age groups were observed as well in line with Franssen et al., (2020) and Luhmann and Hawkley (2016). The age-specific risk factors in early adulthood will be discussed first, followed by the risk factors specific to middle and late adulthood.
In early adulthood, higher levels of loneliness were associated with having a migration background even after controlling for socioeconomic status. Having a non-western migration background was the most important risk factor for loneliness in this age group after mental health. The largest groups of immigrants in the Netherlands can be traced back to its colonial history (e.g., Surinamers and Antilleans) and demand for labor immigrants (e.g., Turks, Moroccans, and Polish). Previous research has revealed that the cultural distance between the Dutch majority members and Turks and Moroccans is larger compared to Surinamers and Antilleans, especially with respect to family and marital values (Arends-Tóth & Van de Vijver, 2009). The relationship between having a migration background and loneliness might be explained by the fact that immigrants experience cultural barriers and feel stigmatized and discriminated (Treas & Mazumdar, 2002; Victor et al., 2012; Visser & El Fakiri, 2016). Since early adulthood is characterized by the development of intimate peer relationships (Erikson, 1959), these negative associations with being an immigrant might be particularly important for this age group. Furthermore, having a migration background is non-normative for this age group (Table 1), which might contribute to feelings of loneliness. Finally, there is evidence that migrants in the Netherlands have less diverse social networks and lower social capital compared to Dutch inhabitants (Völker et al., 2008), which might provide another explanation for the higher levels of loneliness associated with having a migration background.
Having a physical disability was a significant risk factor of loneliness in early adulthood, even after controlling for other covariates. This result fits the age-normative perspective on loneliness. For young adults, having a physical disability is non-normative (Table 1), and this might contribute to feelings of isolation and loneliness (Luhmann & Hawkley, 2016; Victor & Yang, 2012).
In middle adulthood, living alone was the most important risk factor of loneliness after mental health and infrequent contact with friends. As middle adulthood is characterized by finding a romantic partner and starting a family (Erikson, 1959; Heckhausen et al., 2010), living alone might signal a struggle with these developmental goals. Furthermore, having a migration background was a risk factor of loneliness even after controlling for other covariates. Similar to the situation observed in early adulthood, the proportion of midlife adults that have a migration background constitutes a minority (Table 1), which might contribute to their feelings of social isolation.
Having a paid job is a protective factor of loneliness after controlling for other covariates in middle adulthood only in line with the results by Luhmann and Hawkley (2016). Since middle adulthood largely overlaps with one’s professional life, having a job might be particularly important for this age group. Furthermore, employment provides individuals with the opportunity to form social ties with co-workers, clients, and supervisors as well as a collective purpose (Paul and Batinic, 2010). In young and late adulthood, having a paid job becomes insignificant after controlling for social contact. An explanation for the lack of a significant relationship between having a paid job and loneliness in late adulthood (>64) is the low level of labor participation (see Table 1) since the retirement age was 65 in 2016.
In late adulthood, living alone was the second most important risk factor of loneliness. In older adulthood, living alone might indicate widowhood which has been found to be the most important risk factor of loneliness among older adults (Golden et al., 2009). Indeed, O'Súilleabháin et al., (2019) argue that the association between living alone and loneliness among older adults can be explained by bereavement. Furthermore, living alone was more prevalent among older adults compared to young and midlife adults. Having a physical disability was associated with higher levels of loneliness in late adulthood. This result can be explained by the fact that having a physical disability is more prevalent among older adults (Table 1).
Finally, the proportion of variance explained by the full model was different for the three age groups. The R-squared of the model is .33, .37, and .24 for young, middle, and late adulthood, respectively. The fact that the explanatory power of the model for older adults is lower might indicate that important age-related risk factors have been omitted such as widowhood or the quality of social relationships.
Limitations and future directions
The present study has some limitations which should be considered when interpreting the results. First, the data used in this study were cross-sectional. As a result, the observed age differences in loneliness could be caused by generation effects as opposed to the assumed age effects. Hence, a longitudinal study covering all phases of adulthood that is able to distinguish between cohort and age effects would move the literature on loneliness forward and might help to explain the different age-related patterns that have been observed in the literature.
Second, the present study was unable to investigate the risk factors of loneliness across the entire age range in a single model due to differences in the surveys used. The questionnaire administered to older adults contained questions that assessed their network type whereas the questionnaire administered to the adults assessed the frequency of their social contact.
Another limitation is that no measure for the quality of social relationships was included in the study. Previous findings have indicated that the perceived quality of social relationships as well as having a spousal confidant are important protective factors of loneliness and are considered more important than the quantity of social contact (Hawkley et al., 2008; Pinquart & Sörensen, 2003). Furthermore, two demographic variables that have been associated with loneliness—gender identity (Eres et al., 2020) and income level (e.g., Luhmann & Hawkley, 2016)—were not included in the current study. Future research could further investigate any age differences in the relationship between these demographics and loneliness.
An important avenue for future research is to move away from observational to intervention studies. By designing and testing interventions, the current knowledge can be used to analyze causal mechanisms, alleviate feelings of loneliness and potentially reduce the risk of other mental health problems.
Conclusion
Contrary to other relationships that have been found in the literature, the age distribution of loneliness observed by the present study suggests a positive linear pattern with the highest levels of loneliness in oldest old age (>85). Regression analyses confirmed that age is positively correlated with loneliness in early, middle, and late adulthood, but after controlling for other covariates, age was a risk factor of loneliness in early and middle adulthood only. This positive trend of loneliness with age stresses the importance of more research on loneliness in middle adulthood. The present study found that being male, lower education levels, inadequacy of financial resources, higher risk of anxiety and depression, informal caregiving that is experienced as burdensome and social contact were associated with higher levels of loneliness across the life span. Having a migration background, living alone, having a physical disability, and having a paid job were found to be age-specific risk factors. Taken together, these results demonstrate that the risk factors of loneliness vary with age. Hence, addressing loneliness might require different targeted interventions depending on the sufferer’s stage of life.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Open research statement
As part of IARR’s encouragement of open research practices, the authors have provided the following information: This research was not pre-registered. The data used in the research cannot be publicly shared but are available upon request. The materials used in the research cannot be publicly shared but are available upon request. The data or materials can be obtained by emailing: