
Abstract
The aim of the present cross-sectional study was to address a gap in the literature regarding the potential role of workaholism and social support in the development of social anxiety and loneliness. This study involved 338 individuals from Romania, with 53.8% females and 45.9% males, ranging in age from 18 to 45 (M = 24.79, SD = 4.75). Participants completed instruments assessing workaholism, social anxiety, loneliness, social support, and socio-demographic data. Our findings showed that workaholism and social support predicted social anxiety and loneliness. This study may contribute to the existing body of knowledge on key constructs related to workaholism, while highlighting its potential negative impact on mental health. Theoretical and practical implications are discussed, along with recommendations, while acknowledging the limitations of the research design and the inability to infer causal relationships from the data.
Introduction
The term “workaholism” was first coined through the definition “addiction to work, the compulsive and uncontrollable need to work incessantly” (Oates, 1971). However, much more recently, this definition of the construct implies that workaholism is characterized by a compulsive and often extreme need to work, which features the desire to work hours on end, taking on more work responsibilities, and prioritizing work and work-related aspects over various areas of personal life, including family or friends (Andreassen, 2014; Karner-Huțuleac & Huțul, 2023). It is important to note that factors such as demographic characteristics or personality traits are only weakly associated with workaholism, whereas contextual factors—such as an overwork culture—appear to play a more significant role (Taris & De Jonge, 2024). Moreover, workaholism can be understood as a combination of an uncontrollable internal drive and excessive work behavior (Andreassen et al., 2012; Spence & Robbins, 1992). Individuals identified as workaholics often experience persistent thoughts about work even during their leisure time and tend to invest both more time and effort into their work than is objectively required, regardless of external demands (McMillan & O’Driscoll, 2006; Scott et al., 1997). Despite their elevated effort, workaholism is rarely associated with enhanced job performance (Clark et al., 2016). Workaholism has harmful effects in multiple areas, affecting both physical and psychological health (Andreassen et al., 2012). Among the negative consequences of workaholism are sleep problems or insomnia (Andreassen et al., 2011; Kubota et al., 2010), conflicts with family and poor functioning outside the workplace (Andreassen et al., 2013; Bonebright et al., 2000; Russo & Waters, 2006; Taris et al., 2005), an unsatisfactory social life (Andersen et al., 2023), reduced well-being and happiness (Chamberlain & Sahakian, 2007; Del Líbano et al., 2010), or poor oganizational outcomes (Andersen et al., 2023).
Considering the consequences it can have on numerous areas of life, workaholism is regarded as one of the main social issues in contemporary society (Karner-Huțuleac & Huțul, 2023; Malinowska et al., 2015). One of the primary characteristics of a workaholic individual, as suggested by the very definition of this construct, is the tendency to work excessively (Karner-Huțuleac & Huțul, 2023; Oates, 1971; Spence & Robbins, 1992). Consequently, the more they work, the less time they have for their personal lives and friends, which can lead to feelings of increased loneliness (King et al., 2011). In this context, a vicious cycle can emerge wherein the more workaholic individuals become and the more they work, the less they find themselves in social situations (Rapee & Spence, 2004). This lack of social interaction may contribute to the development of social anxiety and loneliness, as suggested by previous findings, although this relationship warrants further investigation. Therefore, given that social anxiety and loneliness can play a key role in the mechanisms involved in workaholism, they must be studied in this regard, especially as they may serve as predisposing factors for various other psychopathological disorders (Kashdan et al., 2011; Park et al., 2020).
Social Anxiety
Social Anxiety Disorder (SAD) represents one of the most prevalent psychiatric ailments (Butler et al., 2023), with its lifetime prevalence estimated to be 13% in the United States (Kessler et al., 2012), similar figures being encountered across Europe (Fehm et al., 2005). According to the “Diagnostic and Statistical Manual of Mental Disorders – Fifth Edition (DSM-V)”, SAD refers to a condition characterized by marked fear or anxiety about at least one social situation in which the individual is exposed to possible examination by other individuals (APA, 2013).
The presence of a psychiatric disorder, including an anxiety disorder, can increase the risk of developing an addiction (Kessler, Chiu, et al., 2005). Approximately 20% of people will experience depression at least once, no fewer than about 30% of individuals will experience some type of anxiety disorder (Baxter et al., 2013; Kessler, Berglund, et al., 2005). In addition, there is a link between depression, anxiety disorders, and workaholism (Andreassen et al., 2016; Clark et al., 2016; Matsudaira et al., 2013; Nie & Sun, 2016; Patel, 2011).
Even though to our knowledge, studies directly linking the specific concepts of workaholism and social anxiety are limited (Aziz & Moyer, 2018), or even non-existent, the literature suggests that workaholism could be a factor in explaining social anxiety (Loscalzo & Giannini, 2017). However, it is important to note that individuals with workaholic tendencies may develop heightened internal tension or irritability, which can contribute to the onset of anxiety (Andreassen et al., 2016; Serrano-Fernández et al., 2021). Excessive involvement in work activities can deplete the mental and emotional resources typically required to sustain healthy social relationships (Andreassen et al., 2018) . As such, the compulsive nature of workaholism may undermine social interactions that would otherwise help alleviate anxiety. Additionally, several studies suggest that workaholism mediates a range of mental health outcomes, including insomnia and social dysfunction, both of which are closely linked to increased anxiety symptoms (Alshammari et al., 2023; Molino et al., 2018). Other research has shown that excessive work engagement can erode existing interpersonal relationships, as individuals may increasingly prioritize work over social connection, leading to reduced interaction with others (Bakker et al., 2009; Kasemy et al., 2020). Moreover, the association between workaholism and psychiatric conditions—including social anxiety—is supported by findings indicating that compulsive work behaviors are linked to reduced well-being and greater psychological distress (Andreassen et al., 2018; Serrano-Fernández et al., 2021). Finally, the compulsive drive inherent in workaholism often entails maladaptive coping strategies (Shimazu et al., 2010), such as avoidance of social situations (Dobrowolska & Izydorcyzk, 2017), which may further reinforce and perpetuate symptoms of social anxiety (Rachman et al., 2008).
Taking this into consideration, studying social anxiety in the context of workaholism could fill a gap in the literature and provide valuable insights into this issue.
Loneliness
Loneliness, frequently linked with social anxiety (Eres et al., 2021; Lim et al., 2016), represents one of the most common states and experiences that any individual can undergo (Huțul et al., 2024). In the literature, it is described as a sensation of suffering that individuals feel when their social needs are not met, and the quality of their social relationships is unsatisfactory (Hawkley et al., 2008; Peplau & Perlman, 1982; Pinquart & Sorensen, 2001). It is important to underline that any individual can experience loneliness, regardless of aspects such as age, sex, social class, or economic status, with consequences potentially leading to negative outcomes in areas such as cognition, emotions, behavior, and health, loneliness being linked with a dramatic decline in mental health (Beutel et al., 2017; Richardson et al., 2017).
It is important to mention that there is a significant association between loneliness and SAD, considering that they both have at their core an impaired interaction of the individual with the social environment, as well as the fact that emotional distress is caused as a result of a subjective evaluation that the individual makes in their social interactions (Jones et al., 1986).
The influence of workaholism also extends to loneliness, considering that workaholics spend more time at the workplace (Harpaz & Snir, 2003), thereby severely limiting the time they can spend with family or friends (Ng et al., 2007). In accordance with these aspects, it is known that loneliness can result from an individual being overly anchored in work and neglecting their social life (King et al., 2011). This relationship is dual, with the workaholic distancing themselves from family and friends, and in turn, them distancing themselves from the workaholic due to their behavior towards work (King et al., 2011).
Social Support: A Protective Factor for Workaholism, Social Anxiety Disorder, and Loneliness
One of the protective factors against workaholism and loneliness is represented by social support, defined by those functions of social networks that can improve both the physical and psychological health of the individual (Rodriguez & Cohen, 1998). However, in the absence of social support, negative outcomes of workaholism on mental health may exacerbate, considering that the lack of this support implies that workaholics do not have quality relationships, do not receive support from others, and, implicitly, are more anchored in work (Bonebright et al., 2000). In the literature, it is known that social support is negatively linked with workaholism, considering aspects such as employees being driven to fulfill tasks themselves to increase their need for appreciation from others (Matsudaira et al., 2013), but also because workaholics are more rigid and prefer to “go their own way” (Schaufeli et al., 2008).
Similarly, numerous studies have shown that individuals with a low level of social support are more likely to experience negative outcomes of SAD or social avoidance (Aras & Tel, 2009; Calsyn et al., 2005; Potoczniak et al., 2007; Wonderlich-Tierney & Vander Wal, 2010). At the same time, social support also functions as a protective factor against SAD, considering that individuals with SAD symptoms tend to avoid interaction with others, and through social support, they may alleviate their symptomatology (Rapee & Spence, 2004). In addition, social support is an important factor in alleviating loneliness (Xin & Xin, 2016; Zhang & Dong, 2022).
We consider that social support can function as a mediator in the relationships between workaholism and social anxiety, and workaholism and loneliness, due to the fact that it provides individuals with a sense of connection and belonging (Cossin et al., 2021; Moynihan et al., 2023), which can counteract the negative outcomes associated with workaholism and social anxiety. Additionally, social support can offer new resources and perspectives on the difficulties individuals face (Lakey & Orehek, 2011; Lazarus & Folkman, 1984). Furthermore, it can create a safety net, providing support and creating a framework in which emotions and feelings can be expressed (Chaudoir & Fisher, 2010; Liang et al., 2011; Pierce & Quiroz, 2019). Thus, through this support framework, the negative impacts on the individual can be alleviated.
The present study
Based on the literature review, the main objectives of the present study are to examine how workaholism may contribute to the development of social anxiety and to investigate variables contributing to negative outcomes of mental health in the context of workaholism, focusing on an understudied population and context – the population of Romania and the Eastern European context.
Thus, the novelty of this work lies in (I) exploring the impact of workaholism and social support on social anxiety and loneliness, (II) improving the foundational understanding from the literature regarding workaholism and negative mental health outcomes, and (III) examining an understudied population and context, which may contribute to the generalization of global results from the existing literature.
To achieve our goals, we formulated the following hypotheses.
Hypotheses
Workaholism and social support predict social anxiety.
Workaholism and social support predict loneliness.
Method
Participants and Procedure
This study involved 338 individuals from Romania, ranging in age from 18 to 45 years (M = 24.79; SD = 4.75). Out of the total number of participants, 182 (53.8%) are female, while 156 (45.9%) are male. Additionally, 105 (31.1%) reside in rural areas, while 233 (68.9%) come from urban areas. Regarding the level of education completed, 212 participants (62.7%) have completed at least a bachelor’s degree, while 126 participants (37.3%) have completed only high school without attending any higher education institution.
On another note, at the time of completing our questionnaire battery, all participants were employed. In terms of work schedule, 267 participants (79%) work on a regular schedule. Among those who work in shifts, 263 (75%) work with a normal schedule and 71 (25%) work in shifts. Among those who work in shifts, 48 (45.5%) work both day and night shifts, 4 (3.8%) work only night shifts, and 50 (50.7%) work only day shifts.
Regarding the data collection method, this study involved snowballing technique with convenience sampling. All scales used in this research were embedded within a formulated Google Forms platform. Subsequently, the survey link was distributed across various social media groups such as Facebook, Reddit, or Telegram. The groups in which the link was distributed were as general as possible, thus avoiding responses solely from one category of people. Specifically, groups such as “Bucharest student groups” were avoided, and instead, the link was disseminated in groups such as “Bucharest city residents” or “Botoşani city residents”. Consequently, the data were obtained from individuals with diverse backgrounds. This approach of searching for groups to distribute research-related links has been successfully used in other studies on the Romanian population involving addictive behaviors (Huțul & Karner-Huțuleac, 2024a, 2024b).
On a different note, it is important to underline that all participants in the current study were volunteers. They did not receive any remuneration for their participation. Additionally, before completing our battery of instruments, they were asked to read informed consent information specifying all necessary provisions according to the law, including the fact that they could withdraw at any time without any consequences. Furthermore, the current research follows the principles of the 2013 Helsinki Declaration and has been approved by The Ethics Committee of the Faculty to which the authors are affiliated (Protocol Number 810/28.06.2024).
Regarding the criteria we selected for eligibility in this study, we included the following: (1) a minimum age of 18 years at the time of completing the questionnaire, the legal age of majority recognized in Romania, and (2) employment status at the time of completing the questionnaire battery.
At the end of the data collection process, responses provided by volunteers were manually screened by the authors of the present study to identify potential bot interference or responses from so-called “mischievous respondents” (Lawrence et al., 2023). This manual screening process involved, for example, checking for contradictory answers to key items, identifying similar or identical response patterns across participants, assessing the presence of patterned responding, and flagging submissions completed in an unreasonably short amount of time (e.g., under 7 minutes), in accordance with existing recommendations (Golds, 2023). No such responses were identified; therefore, all collected responses were retained for analysis.
Measures
All instruments used in this research were translated from English into Romanian using the back-translation method, adhering to all recommendations for adapting and translating the scales from the protocols found in the literature (Beaton et al., 2000; Maneesriwongul & Dixon, 2004; Sousa & Rojjanasrirat, 2011).
Workaholism
The level of workaholism was assessed through the “Dutch Work Addiction Scale” (DUWAS; Schaufeli, 2006). This scale was constructed based on previous works in the literature (Robinson, 1999; Spence & Robbins, 1992) and comprises 17 items, divided into two subscales: “working excessively” (e.g., “I find myself doing two or three things at one time such as eating lunch and writing a memo, while talking on the telephone”) and “working compulsively” (e.g., “It is hard for me to relax when I’m not working”). The items were on a 4-point Likert scale, where 1 = “almost never”, and 4 = “almost always”. The scale has demonstrated its psychometric properties in other studies involving the Romanian population (Butucescu & Uscătescu, 2019; Tecău et al., 2020). A high score indicates a high level of workaholism. In the current study, the scale’s reliability was excellent, both for the subscales “working excessively” (Cronbach’s α = 0.81) and “working compulsively” (Cronbach’s α = 0.82), as well as for the total scale (Cronbach’s α = 0.89).
Social Anxiety
The level of social anxiety was assessed through the self-report version of the “Liebowitz Social Anxiety Scale” (LSAS-SR; Baker et al., 2002), initially developed as a clinician-administered instrument (LSAS; Liebowitz, 1987). This instrument consists of 24 statements (e.g., “Acting, performing, or speaking in front of an audience”), each offering 4 choices divided into two categories: (I) “Fear” (with choices 1 = “none”; 2 = “mild”; 3 = “moderate”, and 4 = “severe”) and (II) “Avoidance” (with choices 1 = “never”; 2 = “occasionally”; 3 = “often”; and 4 = “usually”). Specifically, each respondent is required to provide a score for each of the two subscales for each of the 24 statements. The total score is calculated by summing all choices from both subscales, with the maximum score being 144; a score of 30 or above indicates social anxiety, which is recommended as a cut-off point in literature for an accurate index of social anxiety (Rytwinski et al., 2009). The scale has demonstrated its psychometric properties in the Romanian population (Podină & Vîslă, 2014; Tulbure et al., 2015). In the current research, the scale’s reliability was excellent, both for the subscales “Fear” (Cronbach’s α = 0.81) and “Avoidance” (Cronbach’s α = 0.82), as well as for the total scale (Cronbach’s α = 0.89).
Loneliness
For measuring the level of loneliness, we used the “UCLA Loneliness Scale” (Russell et al., 1980). The instrument comprises 20 items (e.g. “I find myself waiting for people to call or write”), scored on a 4-point Likert Scale, ranging from zero = “I never feel this way” to 3 = “I often feel this way”. The scale has demonstrated its psychometric properties in the Romanian population (Huțul et al., 2024). In this study, the reliability of the scale was excellent (Cronbach’s α = 0.89).
Social Support
To assess the level of social support, we employed the “Oslo Social Support Scale” (OSSS-3; Kocalevent et al., 2018). Originally developed by Dalgard (1996), the scale has demonstrated high acceptability and feasibility, making it a common instrument for researchers in studies concerning mental health or quality of life (Meltzer, 2003). The instrument comprises 3 items. The first item (e.g. “How many people are so close to you that you can count on them if you have great personal problems?“) ranges on a 4-point Likert scale, where 1 = “none”, and 4 = “5+“. The second and third items in the questionnaire (e.g. “How much interest and concern do people show in what you do?“, and “How easy is it to get practical help from neighbours if you should need it?“) range on a 5-point Likert scale, where for second item 1 = “none”, and 5 = “a lot”, and for the third item, 1 = “very difficult”, and 5 “very easy”. The total score of the instrument is obtained by summing each item. The final result ranges from 3 to 14, with higher values indicating a high level of social support (Bøen et al., 2012; Kocalevent et al., 2018). Additionally, the scores can be operationalized according to three categories of social support, as follows: scores from 3 to 8 indicate “poor social support”, scores from 9 to 11 indicate “moderate social support”, and scores from 12 to 14 indicate “strong social support” (Bøen et al., 2012; Kocalevent et al., 2018).
Socio-Demographic Data
The participants reported their age, sex, place of origin (rural or urban), level of education, and work schedule (regular/normal schedule or shift work).
Overview of the Statistical Analysis
Firstly, we conducted preliminary analysis, and then we tested the associations between the main variables, using Pearson Correlation. Finally, we conducted a hierarchical linear regression to assess whether workaholism and social support significantly predict social anxiety and loneliness, while controlling for age, sex, education, urbanicity, shift work, and work schedule.
Results
Preliminary Data Analyses
Descriptive Statistics and Associations Among the Main Variables.
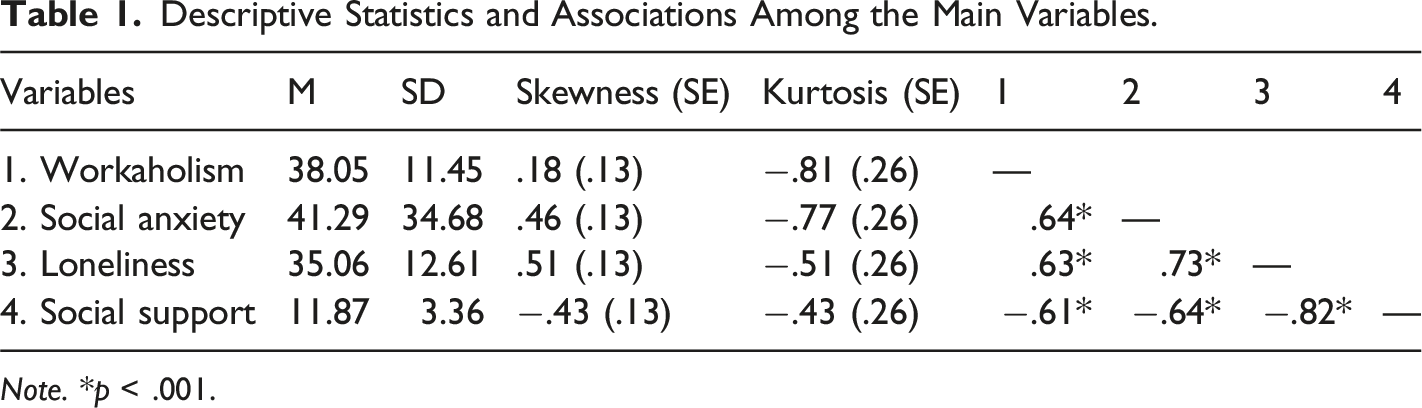
Note. *p < .001.
The Association Between Main Variables
The results of Pearson correlation analysis suggested that there are significant associations between the main concepts – workaholism, social anxiety, loneliness, and social support. The results can be observed in Table 1.
Testing the Regressions
In the first block, we introduced workaholism and social support, and in the second block, we introduced age, sex, education, urbanicity, shift work, and work schedule to control their effects, with social anxiety and loneliness as the dependent variables, respectively.
Social Anxiety Prediction Model.
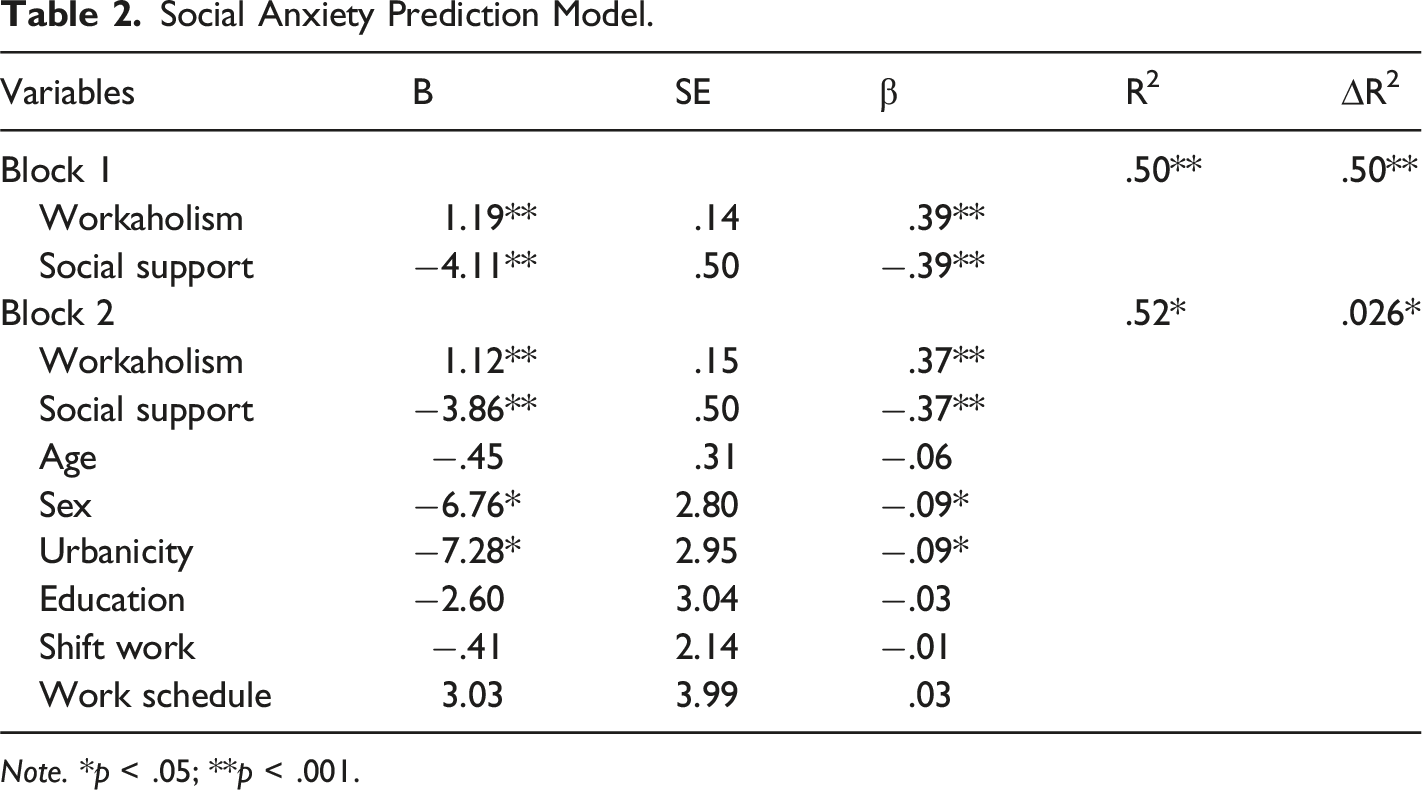
Note. *p < .05; **p < .001.
Loneliness Prediction Model.
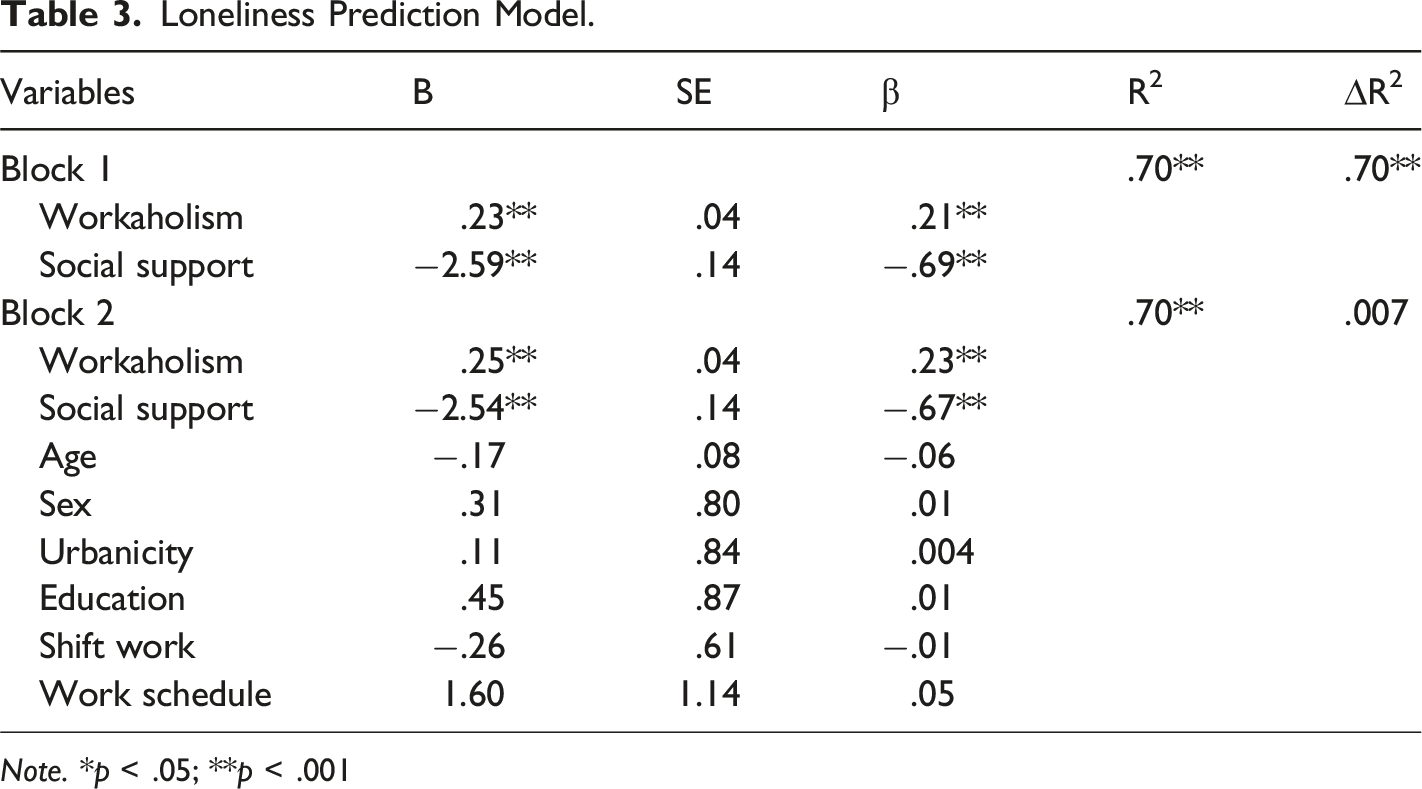
Note. *p < .05; **p < .001
Discussions
First and foremost, our study aligns with the existing literature, which has highlighted that workaholism has a negative impact on individuals’ mental health and social life (Karner-Huțuleac & Huțul, 2023; Malinowska et al., 2015).
Our results have revealed that workaholism predicts social anxiety, when controlling for age, sex, education, urbanicity, shift work, and work schedule. Despite the fact that, to our knowledge, this finding has not been studied until now, it should not be surprising, given that the presence of a psychiatric disorder, including an anxiety disorder, inherently increases the risk of developing a dependence (Kessler, Chiu, et al., 2005). In this regard, our study aligns with the literature suggesting that workaholism may be an explanatory factor for social anxiety (Loscalzo & Giannini, 2017) and that, in general, various addictions are linked to social anxiety (Buckner et al., 2008; Butler et al., 2018; Grant et al., 2005; Lemmens et al., 2015). A potential explanation for our findings is that individuals who are more involved in their work tend to neglect their personal lives and interpersonal relationships (Ng et al., 2007). This neglect of interpersonal relationships causes people to spend more time alone and, consequently, by rarely placing themselves in situations where they interact with others, they may develop anxiety in this regard. Additionally, due to the focus on work and meeting work-related standards, individuals may become overinvolved and encounter difficulties in establishing quality relationships with others, thereby increasing the risk of social anxiety (Alden et al., 2002).
Additionally, besides social anxiety, workaholism also predicts loneliness in our sample, when controlling for age, sex, education, urbanicity, shift work, and work schedule. This result is not surprising, considering that workaholics spend more time at work (Harpaz & Snir, 2003) and, consequently, less time with family and friends (King et al., 2011; Ng et al., 2007). In this situation, inevitably, workaholic individuals may feel much lonelier because they don’t have time to invest in quality social relationships, and the quality of these relationships becomes unsatisfactory (Hawkley et al., 2008; Peplau & Perlman, 1982; Pinquart & Sorensen, 2001). In the long term, high scores on loneliness can lead individuals to develop a psychiatric disorder.
With regard to the finding that social support predicts both social anxiety and loneliness when controlling for age, sex, education, urbanicity, shift work, and work schedule, this may be explained by the fact that social support can provide individuals with a sense of connection and belonging (Cossin et al., 2021; Moynihan et al., 2023). These feelings can counteract negative outcomes such as social anxiety and loneliness. Consequently, individuals with workaholism might still feel that they are part of a group and have healthy social relationships. This aspect can function as a safety net for individuals, providing them with a protective framework in which both their emotions and feelings can be expressed (Chaudoir & Fisher, 2010; Liang et al., 2011; Pierce & Quiroz, 2019). Thus, social support offers new resources and perspectives regarding social anxiety and loneliness, as well as other difficulties individuals may face (Lakey & Orehek, 2011).
However, social support can act as a protective factor for workaholic individuals, helping them to mobilize for their own psychological well-being, including through the construction of healthy and quality relationships with those around them. It is imperative that future mental health prevention programs also focus on addressing workaholism.
Limitations and Future Directions
Even though our study has numerous strengths, we must also mention a significant set of limitations. The first of these is represented by the fact that our research used self-reported instruments, which imply a high degree of subjectivity. Thus, in this regard, there may be potential recall bias and social desirability from the individuals who participated (Adams et al., 1999). In this regard, future studies could include more objective measurements and methods regarding the behavior of workaholic individuals, such as observational methods or even scales provided by family members of workaholic individuals to mitigate the subjective perception related to work involvement. A second limitation of the current study lies in the fact that the socio-cultural context was not explored. In certain cultures, working overtime and generally having a high level of work involvement may be considered meritorious and may confer a sense of pride. Discussing these aspects in relation to the cultural context, including through cross-cultural studies on workaholism, could improve the knowledge from the literature. Similarly, we consider that the relational and familial context may be significant in workaholism. Thus, future works could consider how individuals have or do not have healthy and happy social and familial relationships. We believe that if they are not satisfied with their personal lives, they may engage in work as a coping mechanism. A third limitation of the present study is its cross-sectional design, which inherently restricts the ability to draw causal inferences between the variables examined. Although our findings suggest a directional relationship from workaholism to social anxiety and loneliness, the reverse pathway—particularly from social anxiety to workaholism—may be equally plausible. Indeed, individuals with heightened social anxiety might engage in excessive work as a coping mechanism to avoid social interactions or to gain a sense of competence and control. Therefore, while our results are informative, the present study should be regarded as hypothesis-generating rather than confirmatory. Future research should employ longitudinal designs to more rigorously test the directionality and causal nature of the relationships between workaholism, social anxiety, and loneliness.
A fourth limitation concerns the external validity of our findings. The use of a convenience sample—recruited through snowballing and online platforms—may introduce self-selection bias, as individuals who chose to participate might systematically differ from those who did not, potentially limiting the representativeness of the sample. Furthermore, while the study offers valuable insights into the Romanian context, caution should be exercised when generalizing the results to other cultural or socio-economic settings, including other Eastern European countries. Despite sharing some regional similarities, countries in Eastern Europe may differ in terms of work culture, social structures, and access to mental health resources, which may influence the dynamics between workaholism, social anxiety, loneliness, and social support. Future research should aim to replicate these findings using more representative samples and across various national contexts to enhance cross-cultural generalizability.
Another potential recommendation for future studies is to investigate workaholism in the context of formal employment, as well as informal employment, the latter being highly prevalent in Romania (Mațcu et al., 2023). Such an approach can be valuable in the context of workaholism, considering that individuals working without a contract are often compelled to work overtime under the threat of not being paid if they do not comply, and the lack of a legal contract may further obligate them to work even more.
Finally, a potential direction for future research would be to consider job type, as it may be an important factor in the development of workaholism. Certain types of jobs, particularly those with high demands, low autonomy, or irregular hours, may foster a workaholic mindset more than others, thus influencing both the intensity and consequences of work involvement.
Theoretical and Practical Implications
From a theoretical standpoint, our results contribute to the development of knowledge regarding workaholism, an extremely important topic in contemporary society (Karner-Huțuleac & Huțul, 2023). This relevance is further underscored by its high prevalence, as various studies have reported rates of workaholism ranging from 8.3% (Andreassen et al., 2014) to 15.2% (Andersen et al., 2023), or even 39.7% (Kang, 2020). Identifying the relationship between workaholism and social anxiety opens the door to potential new lines of theoretical research that could provide significant insights into the negative effects workaholism can have on mental health. Additionally, our work enhances the knowledge from the literature by addressing an understudied context, that of Eastern Europe and particularly Romania, a highly understudied population. Ultimately, our findings contribute to a more detailed understanding of the relationships between workaholism, social anxiety, and loneliness, as well as how social support influences these relationships.
From a practical point of view, our results can help organizational and human resource practitioners who face problems related to overwork and its effects on social anxiety and loneliness. In this vein of ideas, our findings showed that a high level of social support improves the individual’s mental resources and contributes to the effective management of one’s own actions (Hill & Hamm, 2019). In addition, our findings can be used in most areas of the work field, being useful for both the employer and the employees. Moreover, the findings of the present study may have important practical implications for mental health professionals, including psychotherapists, clinical psychologists, and other practitioners who may encounter workaholism in their clinical practice. Given that our results suggest workaholism can be considered a risk factor for social anxiety and loneliness, mental health specialists may benefit from implementing targeted interventions addressing these issues. Specifically, clinicians could incorporate discussions related to work-life balance during clinical interviews and assess the perceived social support of individuals exhibiting workaholic tendencies. Such an approach may help identify underlying psychosocial vulnerabilities and guide appropriate therapeutic strategies. Furthermore, general practitioners and psychiatrists, who are often the first point of contact for individuals experiencing psychological distress, should be aware of the potential signs of workaholism—such as sleep disturbances, somatic complaints, or social withdrawal—as these may signal underlying mental health vulnerabilities requiring further assessment or referral.
On a broader scale, we believe our findings can contribute to raising awareness regarding the necessity of education on employee rights, which should include understanding what constitutes rational work and various methods of managing the work-life balance (time spent with family, leisure time, etc.). Additionally, we consider our results can serve as a practical starting point for NGOs addressing workaholism issues in terms of the need for psychoeducation regarding responsibility for one’s mental health and personal life quality through recognizing personal needs, such as the need to work, the need to socialize, the need for deeper and healthier relationships with family members and friends, and finding healthy methods of prioritization and managing personal resources. Finally, we underscore that our work highlighted the necessity of mental health services for reducing social anxiety in both professional and personal contexts.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to the editor and the anonymous reviewers for their valuable support throughout the publication process and for their insightful suggestions that helped improve the quality of the manuscript. We extend special thanks to the anonymous reviewer who supported us throughout both rounds of revisions. We firmly believe that this study would not have reached its current form without the guidance and feedback we received. We also wish to express our deep appreciation to each participant who voluntarily completed our survey. We are fully aware of how valuable each person’s time is, and we are truly grateful for their contribution.
Author Contributions
Veronica Ciobanu, Tudor-Daniel Huțul, Adina-Karner Huțuleac, and Andreea Huțul contributed equally to conceptualization, methodology, formal analysis, writing-original draft, writing-review, editing, and data curation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data supporting the findings of this research are available from the corresponding author upon request. All data associated with the article are available upon request to the corresponding author.