
Abstract
The proportion of the population who are vaccinated against an infectious disease is significant – not only because vaccination keeps the virus from spreading, but also because learning about how many members of one’s community have decided to get vaccinated has been shown to affect individual vaccination intention. In three preregistered online experiments featuring country-level vaccination rates against a hypothetical disease, we tested two theoretical approaches which offer contrasting predictions on how public health messaging should leverage vaccination rates. If selfish rationality is assumed, a high uptake would tempt people to free-ride on herd immunity (so low uptake should be emphasized); conversely, if vaccination rates exert a descriptive normative influence, a high uptake would signal that vaccination is the best choice, and vice versa (so high uptake should be emphasized). In the pilot (N = 75) and Experiment 1 (N = 174), communicating a high (90%) vaccination rate (vs. 10% vs. no rate) increased vaccination intentions, with no detectable effect of a low vaccination rate. In Experiment 2 (N = 217), decisions to get vaccinated were frequently justified based on reasons involving self-protection, but also the protection of others and the collective, irrespective of the vaccination rate level (20% vs. 80%); participants, on the other hand, rarely endorsed any of the tested reasons for non-vaccination, including free-riding; furthermore, descriptive norms were perceived as more relevant for vaccination than non-vaccination decisions. Experiment 3 (N = 1060) tested the effectiveness of different messages when the majority have been vaccinated (60%) but the coverage is still not optimal. Alongside a weak descriptive norm, the self-benefit message worked better than other- and collective-benefit messages. We argue that public health messaging should incorporate both theoretical approaches, closer to the notion of reasonableness (rather than pure rationality or normativity), which is context-sensitive and pragmatic.
Introduction
Vaccination rates, representing the proportion of a population that received a particular vaccine, are an inevitable part of public health communication, especially during crises such as outbreaks of infectious diseases or pandemics. In addition to having an apparent informational purpose, they seem to be often used with the intention to help encourage more people to get vaccinated, especially by the news media (Lazić & Žeželj, 2022; Leask & Chapman, 2002). Lamenting low vaccination rates has been identified as a part of pro-vaccine rhetoric in Australia’s newspapers (Leask & Chapman, 2002). Similarly, during the measles outbreak in Serbia, online news media predominantly framed vaccination rates in a negative light (e.g., “the coverage is very low, almost 40% of children haven’t received the vaccine”, “only 50% vaccinated”) (Lazić & Žeželj, 2022).
From society’s perspective, it is desirable that as many people as possible get vaccinated as that slows down the spread of disease, which benefits everyone, especially those who are more vulnerable and cannot get vaccinated. This effect is called herd immunity (Fine et al., 2011). The term is also often used in reference to a critical threshold percentage of immune individuals (Fine et al., 2011). For example, the threshold for measles is typically set at a minimum of 95% (e.g., Nokes & Anderson, 1988). The herd immunity threshold is often thought of as a target that, once attained, will always result in disease elimination (Fine et al., 2011; Robertson et al., 2024); this view was, for example, promoted early in the COVID-19 pandemic (Robertson et al., 2024). However, from the public health perspective, this understanding is overly simplistic. It overlooks factors such as non-random interaction between people, varying transmission rates across communities, imperfect vaccine protection, differences in individual infection risk, waning immunity, reinfection, and evolving pathogens (McDermott, 2021; Robertson et al., 2024). Therefore, the herd immunity threshold is better thought of as a proportion of the people in a community who need to be immune for the rate of new infections to slow down significantly (McDermott, 2021).
That said, it is crucial to understand which types of messages communicating vaccination rates, and under what conditions, are most likely to elicit the desired public response. Is the strategy of drawing people’s attention to those who have decided not to get vaccinated by highlighting low vaccination rates, often employed by the news media, truly effective? Two theoretical approaches offer diverging answers to this question.
Two Approaches to Public Communication of Vaccination Rates
Selfish-Rational Approach
One approach frames vaccination as a social dilemma (Van Lange et al., 2014): while vaccination benefits both the individual and the community, it can prove costly for someone to get vaccinated. Out of rational selfishness, individuals would be less likely to get vaccinated, the more people in their community are vaccinated. This is because, due to the effect of herd immunity (Fine et al., 2011), a higher vaccination rate lowers their risk of catching the disease. Individuals are incentivized to become a free-rider who indirectly benefits from the vaccination of others while avoiding certain personal costs, such as money, time, inconvenience or vaccine adverse events [VAEs] (Bauch & Earn, 2004). The selfish-rational approach has found support in studies using interactive games (Böhm et al., 2016; Ibuka et al., 2014; Korn et al., 2017) and hypothetical scenarios (Betsch et al., 2017; Vietri et al., 2011).
Descriptive Social Norms Approach
Social norms are “rules or standards that are understood by members of a group, and that guide and/or constrain social behavior without the force of laws” (Cialdini & Trost, 1998, p. 152). The Focus Theory of Normative Conduct (e.g., Cialdini et al., 1990; Cialdini et al., 2006) distinguishes between two types of social norms – descriptive (what behaviors are common or uncommon) and injunctive (what behaviors are commonly approved or disapproved of) – and assumes that norms influence behavior directly only when they are made salient or focused upon. A similar distinction can be found in Bicchieri and colleagues’ work (e.g., Bicchieri & Xiao, 2009), which differentiates between empirical expectations (i.e., the belief that most people will follow the norm) and normative expectations (i.e., the belief that others think one ought to conform to the norm).
As they present summary information about the behavior of a reference group, vaccination rates may be the most straightforward way of shaping the perceived descriptive norm around vaccination (Tankard & Paluck, 2016), provided that vaccination is seen as predominantly voluntary and not driven by mandates or coercion. As such, they are theorized to motivated behavior by providing evidence about what would likely be an effective and adaptive course of action in a given situation, serving as a kind of a decision-making shortcut (Cialdini et al., 1990). It follows that a high vaccination rate would trigger a descriptive norm motivating individuals to get vaccinated, and vice versa (a low vaccination would discourage vaccination). This prediction contrasts with the selfish rational approach.
While correlational studies tend to link perceptions of peer’s behavior to stated vaccination intentions (e.g., Allen et al., 2009; Graupensperger et al., 2021), results from experimental studies are mixed. When knowing that the majority of their peers are vaccinated, compared to when most peers are not, participants are more willing to get vaccinated too (Belle & Cantarelli, 2021; Hershey et al., 1994; Lyu et al., 2024; Romley et al., 2016; Ryoo & Kim, 2021); however, this was not replicated in some experiments (Clayton et al., 2021; Sinclair & Agerström, 2021; Xiao & Borah, 2020). There is some indication that descriptive norms work better when they invite people to work together toward a common goal (e.g., “Do it together”, “Join in!”) by helping mitigate reactance that can be provoked by social influence; this was, however, so far only studied on charitable giving and pro-environmental behavior (Howe et al., 2021).
Thus, according to the selfish-rational approach, public communication of high vaccination rates can be detrimental as it tempts people to free-ride on herd immunity and refuse vaccination (e.g., Betsch et al., 2017). However, if public communication is more focused on low vaccination rates, this can activate a powerful descriptive norm – “many people are not getting vaccinated” – unintendedly promoting non-vaccination as the right thing to do (Cialdini et al., 2006). Therefore, the descriptive norms approach would recommend that public messaging should focus on high vaccination rates.
Mitigation of the Effect of Vaccination Rates
While public communication can refrain from biased portrayal of vaccination rates (e.g., framing them negatively even though they are above 50%, Lazić & Žeželj, 2022), their concrete values, be they low or high, cannot be hidden from the public. Previous studies have, therefore, tested if the supposed negative effect of vaccination rates can be mitigated. The most consistent finding seems to be that explaining the concept of herd immunity increases vaccination intentions (e.g., Betsch et al., 2017; Lazić et al., 2021; Logan et al., 2018; Pfattheicher et al., 2022), especially when social benefits (protecting others) are emphasized. This could be because such messaging activates people’s prosocial or altruistic tendencies (e.g., Betsch et al., 2013; Böhm et al., 2016; Chapman et al., 2012; Vietri et al., 2011). Some studies pointed to the usefulness of communicating only social (e.g., Schwarzinger et al., 2021; Zhu et al., 2022) or both social and individual benefits at the same time (Mussio & de Oliveira, 2022). However, this effect might be dependent on the vaccination rate and vaccine hesitancy levels. For example, highlighting social benefits alongside herd immunity was beneficial when uptake was high, while highlighting individual benefits was beneficial when uptake was low (Betsch et al., 2017). In one study, message type had no effect for pro-vaccination individuals and only emphasizing individual benefits managed to increase vaccination intentions in people who were strongly hesitant (Freeman et al., 2021).
Reasons for (Non-)Vaccination
Interventions to increase vaccination depend on understanding people’s motives for vaccination and non-vaccination, though, to our knowledge, there have thus far been no studies investigating this under varying levels of vaccination rates. A review by Yaqub et al. (2014) found that healthcare professionals’ advice, advice from friends and family, and self-protection were among the most cited reasons for vaccination in previous literature, while safety concerns and perceived low risk of catching the disease were among the most cited reasons for non-vaccination. In the study by Attari et al. (2014), main self-reported reasons for vaccination against flu were self-protection, protection of one’s family, and avoiding spreading the disease to others, while main reasons for non-vaccination were perceived invulnerability to illness and mistrust in vaccine effectiveness. In addition to confidence (trust in the effectiveness and safety of vaccines), complacency (low perceived risks of diseases), and collective responsibility (protecting others), studies relying on the 5C model also related constraints (structural or psychological barriers in daily life) and calculation (weighing personal costs and benefits) to vaccine uptake (e.g., Betsch et al., 2018).
Overview of Studies
Three preregistered experiments investigated communication of vaccination rates. Experiment 1 examined how communicating a low versus high country vaccination rate affects intention to get vaccinated by testing diverging hypotheses derived from two theoretical approaches, contrasting rationality versus normativity. Experiment 2 was designed to better understand the reasons people give for getting or not getting vaccinated as well as whether those reasons differ under low versus high country vaccination rate and whether they correspond to the reasons stemming from the two theoretical approaches. Informed by previous experiments, Experiment 3 tested the effectiveness of interventions when the majority (60%) of the country have been vaccinated, which is, nonetheless, usually not enough to reach the herd immunity threshold.
The experiments are comparable in that they were conducted with samples of Serbian participants, who were presented with the same disease and vaccination fact sheet and asked to rate their vaccination intention (main outcome) in the same way. In addition to comprehensively testing two influential theoretical approaches in the context of vaccination-rate communication and identifying important directions for future research and practice, this work contributes to the field by studying a country that has been underrepresented in health communication research (Kim et al., 2010).
Open Data
Datasets and questionnaires for all studies are openly available at https://osf.io/2wy9q/. Analyses were performed using R version 4.4.0 (R Core Team, 2023); code and the citations of used R packages are openly available at https://osf.io/2wy9q/.
Experiment 1
Using a one-factor repeated measures design, Experiment 1 compared three types of messages to improve vaccination intention: a baseline with no information on the vaccination rate and two experimental messages featuring low (10%) versus high (90%) country-level vaccination rate. We opted for a within-subjects design because, in addition to being able to control for a variety of individual-level differences, this setting is arguably more externally valid compared to a between-subjects design: in real life, vaccination rate information is dynamic and an individual would likely be exposed to varying levels of vaccination rates against the same disease.
Hypotheses
Relying on the selfish-rational approach described above, we hypothesized that learning about a high vaccination rate will decrease vaccination intention, compared to when a low vaccination rate is communicated (
Relying on the descriptive norms approach described above, we hypothesized that learning about a high vaccination rate will increase vaccination intention, compared to when a low vaccination rate is communicated (
Method
Preregistration
This study was preregistered at https://aspredicted.org/cfv2-kg7w.pdf. To develop the materials and ensure the appropriateness of the measures, we conducted a pilot experiment (N = 75); a detailed report on its methods and results is available at https://osf.io/2wy9q/.
Power Analysis
An a priori repeated measures ANOVA power analysis with a minimum overall effect size of f = 0.3 (estimated based on the overall effect obtained in the pilot of partial Omega-squared = 0.11), 95% power, and the .05 alpha error probability, revealed a target sample size of N = 174.
Data Quality and Exclusion
There were two attention-check questions, asking participants to choose a specific response option. Participants who failed both attention checks were excluded from the analyses.
Participants
Out of 191 participants who completed the survey, 17 (8.9%) were excluded due to failed attention checks. The remaining N = 174 participants (131 female), all Serbian residents, were aged 18–73 (M = 36.3, SD = 11). Recruitment was done through advertisements on social media in April 2021. At the time of data collection, mass vaccinations against COVID-19 in Serbia had been going on for three months (“Vaccination against COVID-19”, nd).
Materials and Procedure
After informed consent, an online survey first assessed age, sex, and country of residence. Next, participants read a disease and vaccination fact sheet and were asked to imagine themselves in a scenario in which they have to decide whether or not to get vaccinated against the fictitious disease. Participants then rated their intention to get vaccinated three times, following the presentation of different vaccination-rate messages. Lastly, perceived relative severity of the disease and VAEs, disease concern, and general attitude towards vaccination were assessed.
Disease and Vaccination Fact Sheet
The fact sheet presented a fictitious contagious disease called Hebdo fever and the vaccine against it. Fictitious materials were chosen because they exclude potential confounding variables, such as real infections and VAEs experienced or observed by the participant, and allow unconstrained manipulation of the vaccination-rate levels.
The sheet informed about the path of infection (via droplets or particles in the air) and described the vaccine as being recently developed, tested, with an efficacy of 100%, and easily available at no out-of-pocket cost. Following Connolly and Reb (2003), the symptoms of the disease and VAEs were described as equally likely (appearing “in a small number of cases”) and very similar in content, to assure equal perceived riskiness. We expressed probabilities qualitatively rather than quantitatively as such a setting is arguably more externally valid. Most decisions in everyday life are based on values that are imprecise or qualitative (Shiffrin, 2021), and the same is true for real-life public communication surrounding vaccination.
The combinations of symptoms had been pretested in a battery of 62 symptoms, with a convenience sample of N = 39, and assembled in a way that assured equal perceived severity. A detailed description of the pretest procedures and results is available at https://osf.io/2wy9q/. The fact sheet was shown as a screenshot of a simulated web page on the Institute of Public Health of Serbia website. To prevent participants from skipping it, the continue button was disabled for a specified minimum amount of time.
Message Manipulation and Outcome Measure
All participants first received no information on vaccination rate in their country; all of them then went through both of the remaining two conditions in a counterbalanced order, in which they learned about a low (10%) and high (90%) vaccination rate. They were warned that they might be presented with a different value of the vaccination rate than before. The rates were presented both as a number out of 10 and a percentage, to ease comprehension (e.g., “Currently, one out of ten (10% of) citizens of Serbia have gotten vaccinated”). The Institute of Public Health of Serbia was named as the source of this information. We decided to present country-level rates to avoid introducing variability in how participants define some less specific terms used in previous studies (such as “community”, “population” or “society”); furthermore, country-level vaccination rates are often featured in media and public health messages (e.g., Lazić & Žeželj, 2022).
In all three conditions, participants reported their intention to get vaccinated. Participants were informed that, roughly six months before, first cases of the disease were reported in the country and that the vaccination is ongoing. They then assessed their vaccination intention (“You have the opportunity to get vaccinated against Hebdo fever. What will you do?”) on a slider ranging from 0 = I will definitely not get vaccinated to 100 = I will definitely get vaccinated (later transformed into a 1–101 scale), in increments of 1%.
Other Measures
Perceived Relative Severity
To check whether the symptoms of the disease and VAEs were perceived as equally severe, participants were asked the following questions: “From what you have read, how do the disease symptoms and vaccine side-effects compare in terms of overall seriousness?” (1 = The symptoms of Hebdo fever are more serious than the vaccine side-effects, 2 = The symptoms of Hebdo fever and the vaccine side-effects are equally serious, 3 = The vaccine side-effects are more serious than the symptoms of Hebdo fever) (adapted from Connolly & Reb, 2003); the options appeared in randomized order.
Disease Concern
Participants were asked about their degree of concern that they or their families would get sick from the disease (“How worried would you be, if at all, that you or someone in your family will get sick from Hebdo fever?”, 1 = not at all worried, 2 = not too worried, 3 = somewhat worried, 4 = very worried).
General Attitude Towards Vaccination
This was assessed on a slider ranging from 0 = absolutely against vaccinations to 100 = absolutely in favor of vaccinations (later transformed into a 1–101 scale), in increments of 1%.
Results and Discussion
Primary analyses were done using a repeated-measures, within-subjects ANOVA, with post-hoc contrast TukeyHSD tests. In addition to the partial Eta-squared (η p 2), partial Omega-squared (ω p 2) was computed based on the F-statistic (Albers & Lakens, 2018, p. 194) to provide a less biased effect size estimator.
Hypotheses Testing
Condition Means and Standard Deviations, With Correlations Among Outcome Measures.
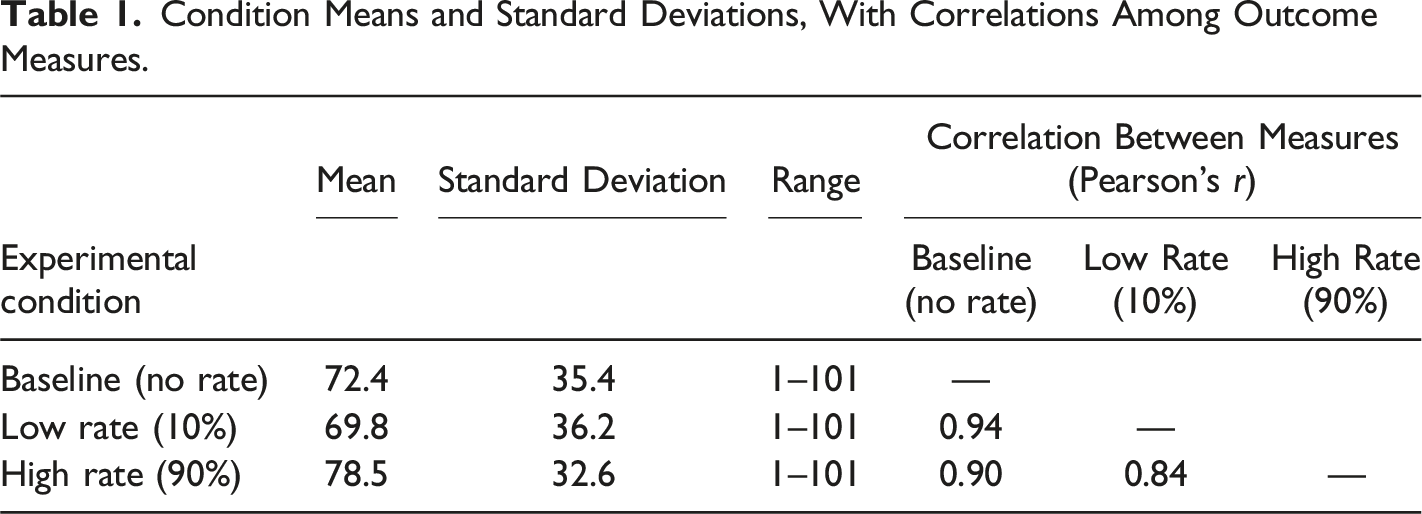
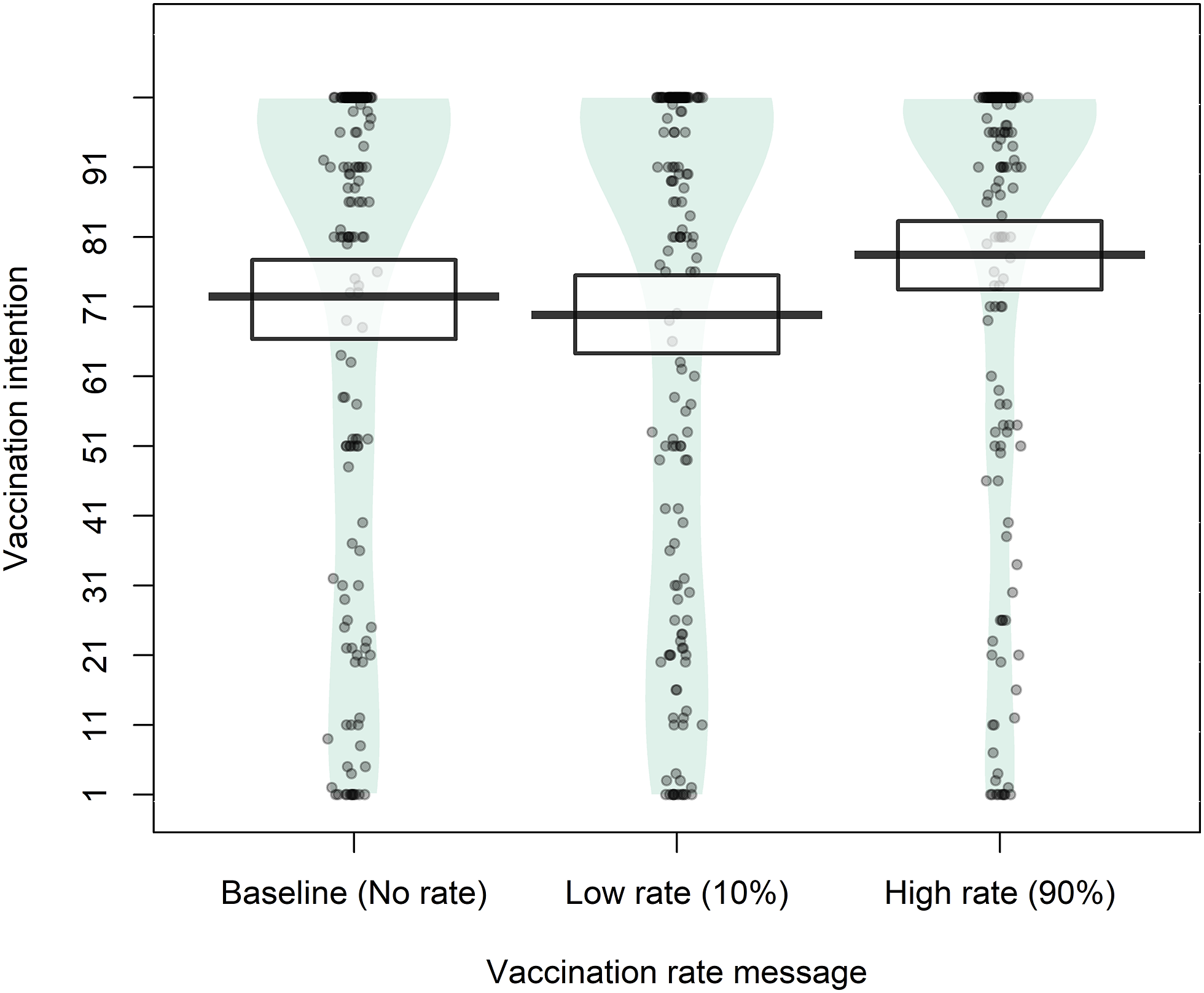
Vaccination intentions depending on the vaccination-rate message.
Learning about a high vaccination rate significantly increased vaccination intentions, both compared to learning about a low rate (estimate = 8.63, SE = 1.24, p < .001, 95% CI [5.73, 11.53]) and to receiving no vaccination-rate information (estimate = 6.01, SE = 1.24, p < .001, 95% CI [3.11, 8.91]), supporting H1b and H2b derived from the descriptive norms approach, respectively. On the other hand, communicating a low vaccination rate did not significantly affect baseline vaccination intentions (estimate = −2.62, SE = 1.24, p = .086, 95% CI [−5.52, 0.28]), not supporting H3b. Contrastingly, the results indicated no support for any of the hypotheses derived from the selfish-rational model (H1a, H2a, H3a). This pattern of results fully replicated the findings previously observed in the pilot.
Additional Descriptive Analyses
While 33.9% of the participants thought that the disease symptoms and VAEs were equally severe, 56.3% rated disease symptoms and 9.8% rated VAEs as more severe; our attempt to make the disease and the VAEs seem equally severe was, thus, only partially successful. Most participants were somewhat (49.4%) or very (23%) worried about the fictional disease; the rest were not too (22.4%) or not at all (5.2%) worried about it. On average, participants reported a highly positive vaccination attitude (M = 91, SD = 19.2, range 3–101).
Experiment 2
Experiment 1 found partial support for the descriptive norms approach and no support for the selfish-rational approach. However, this does not imply that participants would justify their vaccination choices by relying (solely) on descriptive norms or that they would not justify them by using notions stemming from the selfish-rational approach, such as free-riding. Therefore, in Experiment 2, we explored the reasons people endorse for getting or not getting vaccinated under a low and high vaccination rate. Apart from further testing of the two approaches, this experiment would inform the succeeding design of message interventions.
We chose to restrict the sample to younger people (below the age of 35), since that group seemed to be most polarized regarding vaccination. According to a 2021 representative survey in Serbia, the lowest proportion of vaccinated individuals and the highest proportion of those decidedly refusing to get vaccinated against COVID-19 was in the 18–39 age cohort (Žeželj et al., 2021, p. 9). This was done to reach the sufficient number of participants deciding against vaccination under both the low and high vaccination rate more efficiently and because a sample that is more diverse in vaccination attitudes allows us to better gauge people’s reasons for (non-)vaccination.
Unlike Experiment 1, this experiment used a between-subjects design. We decided against repeated measures because requiring participants to describe their personal reasons and exposing them to different types of motivations for (non-)vaccination in one condition might influence their responses in the next one. Furthermore, while Experiment 1 one featured vaccination rates of 10% and 90%, here we chose to change them to 20% and 80% because reflecting on an extremely high vaccination rate might affect participants’ endorsement of different reasons as it could be perceived as neither selfish rational or collectively optimal (“if the uptake is that high, the disease could have been already eliminated”).
Method
Preregistration
This study was preregistered at https://aspredicted.org/46p2-crq5.pdf. Open-ended reasons for (non-)vaccination against a fictitious disease and reasons for COVID-19 (non-)vaccination will be reported in a separate publication.
Data Quality and Exclusion
Participants who provided poor-quality responses to an open-ended question asking them to describe their main reason for (non-)vaccination against the fictitious disease were excluded from the analyses. Signs that suggested poor quality included gibberish, nonsensical, and inconsistent responses (e.g., justifying non-vaccination when asked about vaccination).
Participants
Out of 229 participants who completed the survey, 12 (5.2%) were excluded due to poor-quality responses to the open-ended question. A total of N = 217 participants (157 female), all Serbian residents, aged 18–35 (M = 26.7, SD = 4.8), remained. The majority of them (71%) had some higher education experience, 23.5% finished only high school, and the rest had less education. Recruitment was done through advertisements on social media in April–May 2022.
Materials and Procedure
After informed consent, an online survey first assessed age, sex, education, and country of residence. Participants then read the same fictitious disease and vaccination fact sheet that was administered in Experiment 1. Next, participants were randomly assigned to learn either about a low (20%) or a high (80%) vaccination rate in their country (the presentation followed the same wording as in Experiment 1), after which they assessed their vaccination intention on the same 0%–100% slider used in Experiment 1. Immediately afterwards, participants were also asked to select an option which best describes their choice (1 = Yes, I will definitely get vaccinated, 2 = Yes, I will probably get vaccinated, 3 = No, I will probably not get vaccinated, 4 = No, I will definitely not get vaccinated). Depending on whether they reported they would definitely/probably get vaccinated or that they would definitely/probably not get vaccinated, participants were divided into two groups – vaccinators and non-vaccinators. An open-ended question asked (non-)vaccinators to describe their main reason for (non-)vaccination.
Vaccinators were then shown a closed-ended list of nine possible reasons for vaccination, while non-vaccinators were shown a closed-ended list of nine possible reasons for non-vaccination. They were asked to indicate how closely each reason matches their personal reasons on a 4-point scale (1 = Completely describes my reasons, 2 = Mostly describes my reasons, 3 = Mostly does not describe my reasons, 4 = Does not describe my reasons at all).
Formulation of Reasons for (Non-)Vaccination
Percentage of Participants Endorsing Each of the Reasons for Vaccination.
Percentage of Participants Endorsing Each of the Reasons for Vaccination.
Results
Out of 106 participants in the low vaccination rate condition, 38 were categorized as vaccinators and 68 as non-vaccinators; mean vaccination intention was 41.7 (SD = 36.1, range 1–101). Out of 111 participants in the high vaccination rate condition, 49 were categorized as vaccinators and 62 as non-vaccinators; mean vaccination intention was 43.0 (SD = 39.6, range 1–101). Therefore, the intended polarization of the sample regarding vaccinations was achieved.
Endorsement of Reasons for (Non-)Vaccination
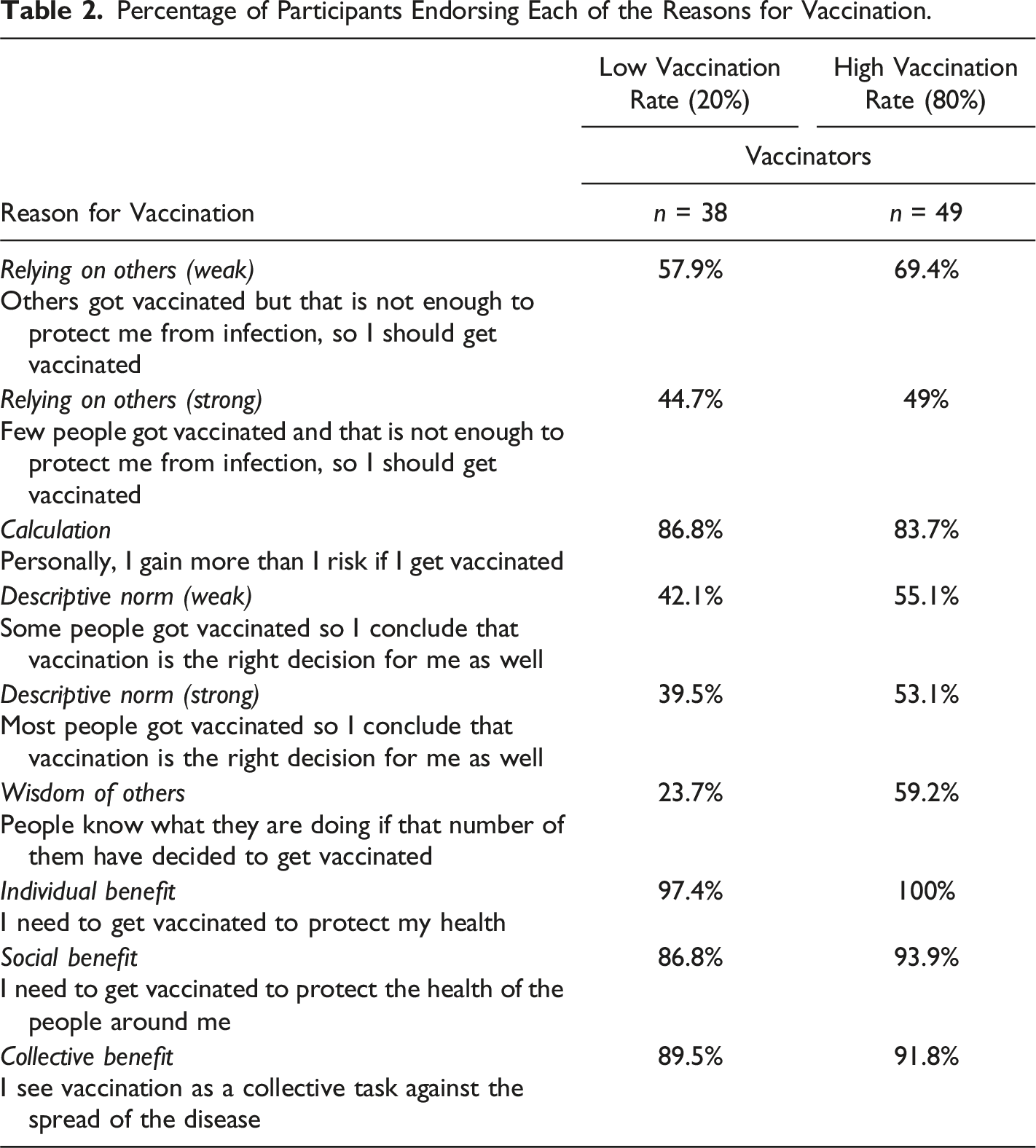
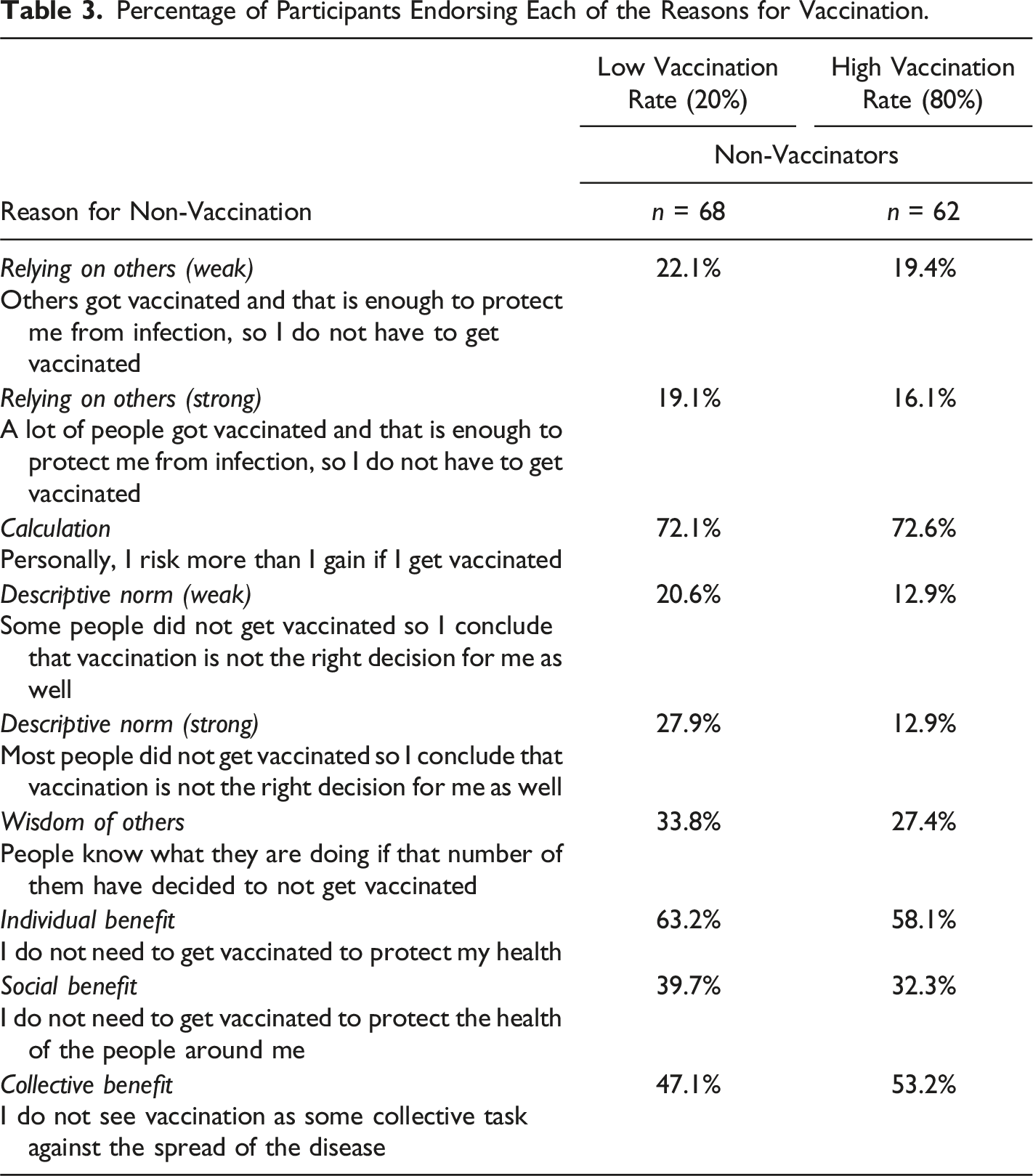
Tables 2 and 3 show the percentage of participants endorsing each of the listed reasons for vaccination and non-vaccination, respectively, across low and high vaccination rate conditions. “Endorsement” indicates that the participant reported the reason “completely” or “mostly” corresponded to their own personal ones. These options were collapsed to ease interpretation; the descriptive statistics for all four original options are available at https://osf.io/2wy9q/.
Three reasons stood out as most frequently endorsed among the vaccinators: viewing vaccination as necessary to protect oneself and others and as a collective task to stop the disease. Personal benefits outweighing risks was also a highly common reason for vaccination. Around a half of vaccinators tended to agree they cannot rely on others for personal protection and that the behavior of the majority (descriptive norm) was relevant for them. Around a half of vaccinators also reported they trusted the wisdom of the common man, and this was the only reason where there appeared to be a noticeable difference between low and high vaccination rate conditions (23.7% vs. 59.2%).
In general, non-vaccinators tended to endorse fewer reasons than vaccinators did. However, three reasons were endorsed by the majority of non-vaccinators: personal risks outweighing benefits, believing vaccination is not necessary to protect oneself, followed by believing that vaccination is not a collective effort. All other reasons were rarely endorsed, including free-riding (reliance on others) and descriptive norms.
Discussion
The results suggest that at least some vaccinators take personal risk of infection into account and that most of them engage in cost-benefit calculations. Even though they were similarly calculating and saw vaccination as costly, non-vaccinators did not endorse free-riding, at either low or high vaccination rate. Though it was initially assumed that calculation encourages non-vaccination (Betsch et al., 2018), this was not always replicated (e.g., Schindler et al., 2020), in line with the present findings. Low endorsement of free-riding among non-vaccinators was also found by Attari and colleagues (2014). As pointed out by these authors, this could reflect social desirability motives and motivated cognition (desire to retain a prosocial self-image), but it could also happen out of ignorance (i.e., not understanding how one benefits from others’ vaccination) (Attari et al., 2014). Not endorsing free-riding might also reflect general vaccination mistrust as well as belief that vaccination is unnecessary to protect one’s health. In fact, in the present study, more than half of participants agreed they do not need vaccination to protect their health. Descriptive norms (including the “wisdom of the common man” formulation) were more frequently endorsed as a reason for vaccination than non-vaccination, which might explain why low vaccination rates in Experiment 1 did not lower vaccination intention, even though this was hypothesized by the descriptive norms approach.
Experiment 3
Experiment 1 found that communicating a high vaccination rate of 90% increases people’s vaccination intention. In Experiment 3, we investigated if and how it was possible to leverage this positive descriptive social norm when the country-level vaccination rate is 60%. This is when, from the public policy perspective, motivating more people to get vaccinated is crucial: while the majority of the population have been vaccinated, this is usually not enough to reach the herd immunity threshold. At that point, vaccination uptake is also likely to stall. For example, many European countries appear to have reached their ceiling on COVID-19 vaccinations at around 60% of vaccinated adults. Roughly a year following the start of COVID-19 vaccination, the percentage of people who were fully vaccinated was 61% across Europe, and 47% in Serbia (December 31, 2021); six months later, vaccination rate remained at similar levels, 65% and 48%, respectively (July 23, 2022) (Mathieu et al., 2021).
Experiment 3 used a 2 (intervention: absent vs. present) x 4 (intervention message: only the 60% norm vs. “protect your health” appeal alongside the norm vs. “protect others’ health” appeal alongside the norm vs. “join-in” appeal alongside the norm) mixed design, with repeated measures on the first factor. The three intervention appeals were chosen to reflect the top three reasons for vaccination observed in Experiment 2: individual, social, and collective benefit, respectively. Furthermore, individual benefit and prosocial messaging was found to be effective in some previous studies (e.g. Betsch et al., 2017; Pfattheicher et al., 2022), while one multi-country investigation identified prosociality as a determinant of COVID-19 vaccination (Enea et al., 2022). The “join-in” appeal, reflecting collective benefit, contained the invitation to join the others in stopping the disease; following the work of Howe et al., 2021, this was supposed to make the norm more motivating.
Hypotheses
We hypothesized that, compared to baseline, communicating only the descriptive norm (i.e., the vaccination rate) will increase vaccination intention (
Method
Preregistration
This study was preregistered at https://aspredicted.org/hw45-f8yg.pdf.
Power Analysis
An a priori repeated measures t test power analysis with a minimum overall effect size of Cohen’s d = 0.2, 90% power, and the .05 alpha error probability, revealed a target sample size of 265, per each of the four experimental groups. We expected the effect size to be small based on some previous published research (Betsch et al., 2017; Lazić et al., 2021).
Data Quality and Exclusion
There were two attention-check questions, asking participants to choose a specific response option. Participants who failed both attention checks were excluded from the analyses.
Participants
Out of 1303 participants who completed the survey, 243 (18.6%) were excluded due to failed attention checks. The remaining N = 1060 participants (814 female), all Serbian residents, were aged 18–77 (M = 47.8, SD = 12.9). There was a total of n = 265 in each experimental group, comparable in terms of age and sex (a full report is available at https://osf.io/2wy9q/). The majority of participants (59.1%) had some higher education experience, 37.1% finished only high school, and the rest had less education. Recruitment was done through advertisements on social media in December 2023.
Materials and Procedure
After informed consent, an online survey first assessed age, sex, education, and country of residence. Following the presentation of the fictitious disease and vaccination fact sheet, all participants assessed their vaccination intention on a 0%–100% slider (these materials were the same as in Experiment 1 and 2), which constituted the baseline. Participants were then randomly assigned to one of the four experimental message conditions, when they were asked to assess their vaccination intention one more time. Each experimental message showed the same value of the vaccination rate – “According to the Institute of Public Health, currently six out of ten (60%) of Serbian citizens have gotten vaccinated against Hebdo fever” – with a different call to action. In the only-norm condition, the message was “Get vaccinated too!”; in the protect-self, it was “Get vaccinated too to protect your health!”; in the protect-others, “Get vaccinated too to protect the health of the people around you!”; and in the join-in condition, the message was “Get vaccinated too to join the others in helping stop the spread of the disease!”. On the survey page featuring the experimental message, the continue button was disabled for a specified minimum amount of time. Finally, participants rated their general attitude towards vaccination (on the same slider measure used in Experiment 1).
Results
Condition Means, With Correlations Among Outcome Measures, and the Results of Statistical Tests Comparing Baseline and Interventions Means.
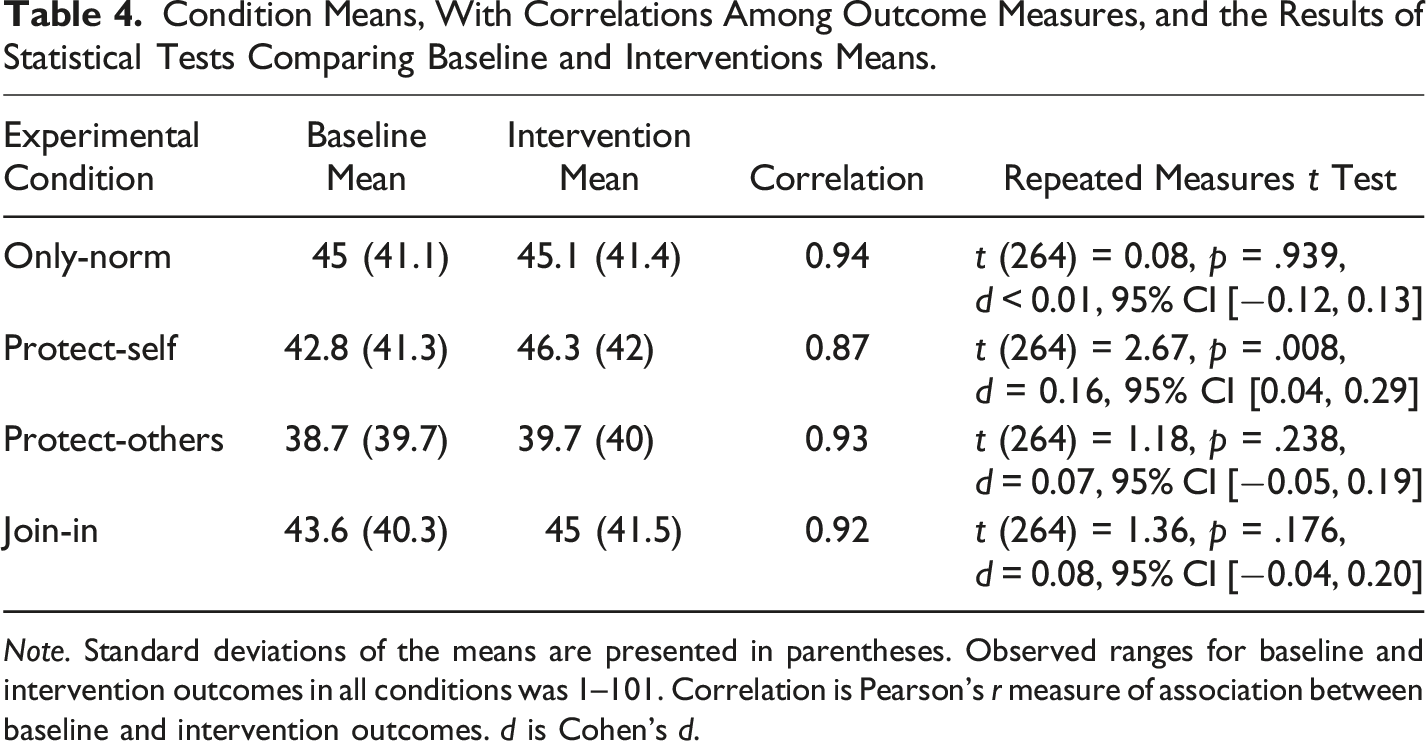
Note. Standard deviations of the means are presented in parentheses. Observed ranges for baseline and intervention outcomes in all conditions was 1–101. Correlation is Pearson’s r measure of association between baseline and intervention outcomes. d is Cohen’s d.
The only statistically significant difference between baseline and intervention vaccination intentions was observed in the protect-self condition, with the effect size of Cohen’s d = 0.16, supporting H2 (but not H1, H3, and H4). All of the differences, however, were in the expected direction (Figure 2). Across all conditions, an exploratory analysis revealed a statistically significant effect of intervention messages (t (1059) = 2.87, p = .004, d = 0.09), slightly larger when the only-norm condition was excluded (t (794) = 3.14, p = .002, d = 0.11). Vaccination intentions depending on the vaccination-rate message (Experiment 3). Note. Outcome at baseline versus when an experimental message (a)–(d) was presented; only the protect-self message was effective in increasing vaccination intentions. The plots show the full distribution of the data and jittered raw data. Horizontal bars represent means; boxes represent 95% confidence intervals. (a) Only norm, (b) Protect self, (c) Protect others, (d) Join on.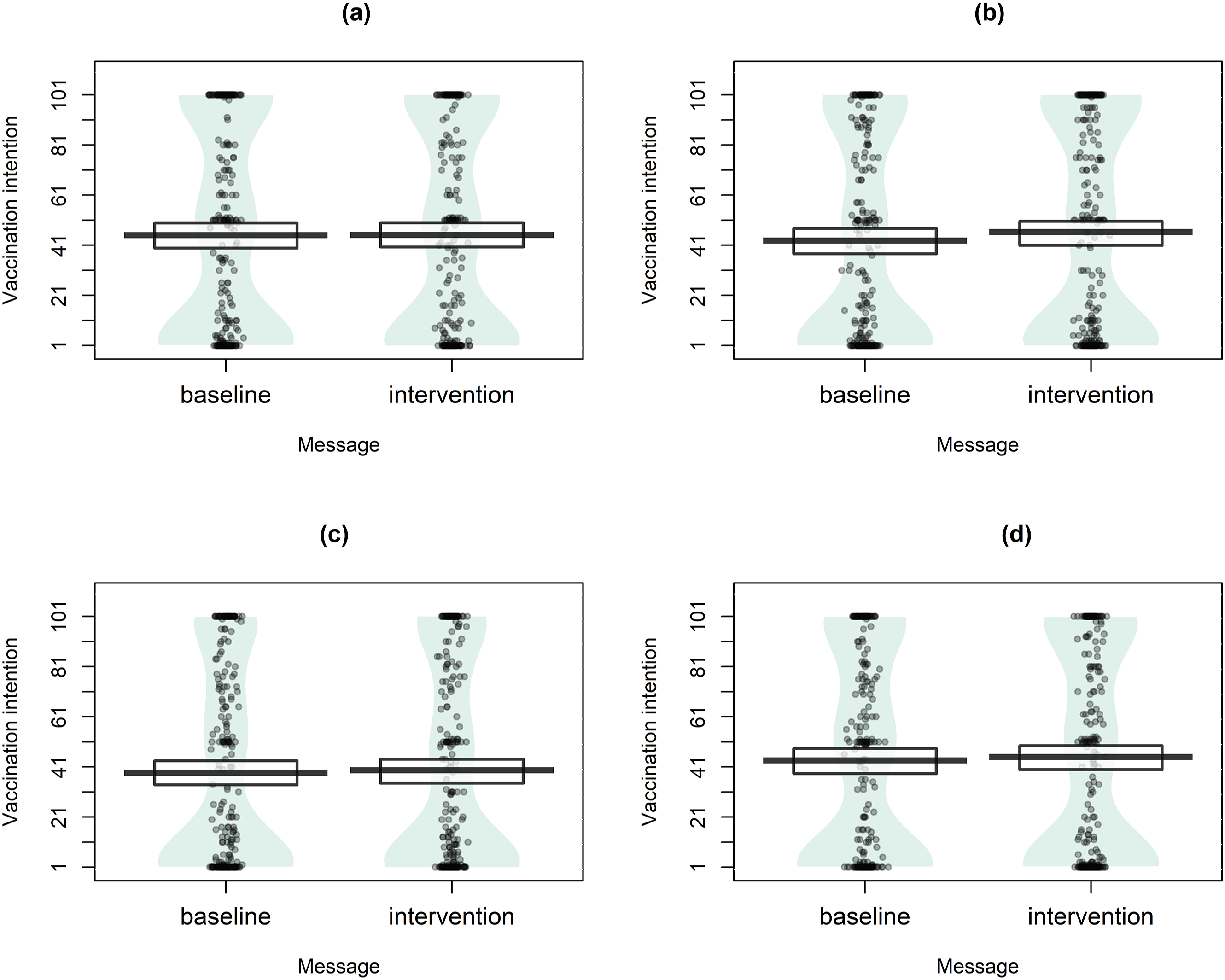
The difference between intervention means in the only-norm and join-in conditions was not statistically significant (t (528) = −0.03, p = .975), not supporting H5. In an exploratory analysis, the differences in vaccination intention from baseline in these two conditions were also found not to be statistically significantly different (t (528) = 0.97, p = .331).
General Vaccination Attitude
On average, participants reported slightly more positive than negative vaccination attitude (M = 64.1, SD = 38, range 1–101). Mean attitudes across experimental groups were similar and are reported at https://osf.io/2wy9q/.
In an exploratory analysis, we checked if the effectiveness of the messages depended on participants’ vaccination attitude using a multiple regression model, with the differences in vaccination intention from baseline as the dependent variable. Since there was no significant interaction between attitude and message type (F (1,1056) = 1.58, p = .209), even after the only-norm group was excluded (F (1,791) = 0.07, p = .784), we did not proceed with testing the moderating effect further.
Discussion
The vaccination rate of 60%, contrary to our hypothesis, did not exert a detectable descriptive normative influence; it is possible that these values need to be more extreme (e.g., 90% in Experiment 1) so that they are more salient in an individual’s attention (Cialdini et al., 1990) and able to influence vaccination intentions. All of the intervention messages tested in Experiment 3, taken together across all participants, positively influenced vaccination intentions, even alongside a weak social norm; while this effect was significant, it was rather small (with the analysis being likely overpowered). The message with the largest effect was the one featuring an individual benefit appeal: as hypothesized, vaccination intentions increased after communicating that getting vaccinated protects one’s health. While it is promising that the other two tested appeals (social benefit and join-in) did not backfire, we did not, contrary to our hypotheses, detect a significant positive effect.
The ineffectiveness of these prosocial appeals is surprising given some previous experimental research (e.g., Pfattheicher et al., 2022; Schwarzinger et al., 2021; Zhu et al., 2022). Since Serbia has a collectivistic cultural background (“Country comparison tool”, nd), one could further expect that prosocial appeals would be more effective than individual ones.
The finding that (only) the individual benefit appeal was effective might be, however, explained by taking the selfish-rational approach into account. When vaccination rates were lower, one study found that explaining individual, but not social, benefits alongside the concept of herd immunity increased vaccination intentions (Betsch et al., 2017); the opposite was true when vaccination rates were higher. This is because lower rates encourage vaccination as a selfish-rational strategy, while, when rates are high, vaccination is no longer selfishly rational but only collectively optimal (Betsch et al., 2017).
In Experiment 2, individual benefit was endorsed as a reason for vaccination by almost all participants. While social and collective benefits were also among the most frequently endorsed reasons, it is possible that, as intervention messages, they need to be further explained to participants. For example, it might be relevant to assure that participants understand collective effects of vaccination or to specify whom individual vaccination benefits (e.g., friends or the society, Stoffel & Herrmann, 2021).
General Discussion
We conducted three preregistered experiments, starting with diverging recommendations for public communication of vaccination rates stemming from two influential theoretical approaches. If people are selfishly rational, a high uptake will tempt them to free-ride, while a low uptake will motivate them to get vaccinated (Bauch & Earn, 2004); it follows that high rates harm, while low rates benefit public vaccination campaigns. Conversely, if vaccination rates exert a descriptive normative influence (Cialdini et al., 1990), a high uptake will encourage, while a low uptake will discourage vaccination; it follows that low rates harm, while high rates benefit public vaccination campaigns.
Partially in line with the descriptive norms approach, Experiment 1 found that communicating a 90% rate improved vaccination intentions, which were, however, not affected by a 10% rate. Lowering one’s intention to get vaccinated in response to a low uptake might have been construed as unreasonable, that is, participants’ choices might have aligned more with the concept of reasonableness: context sensitive balancing of maximizing individual gains and socially conscious norms (Grossmann et al., 2020). Participants in Experiment 1 were, on average, highly provaccine, and the low uptake might not have provided a good enough reason not to get vaccinated. Furthermore, pro-vaccination choices in Experiment 2 were more frequently justified based on reasons involving considerations of individual benefits and risks as well as protecting others than on reasons reflecting descriptive normative influence. As a future line of research, we propose to study the reasonableness of vaccination choices.
The absence of a negative effect of communicating a low uptake in Experiment 1 might also be explained by a limitation of its scenario: it introduced possible VAEs, but the fictitious vaccine was presented as 100% effective and easily available for free. While such a scenario excludes potential confounding variables, it might have caused a ceiling effect. Future studies should include more realistic depictions of personal costs of vaccination (e.g., monetary cost or the requirement to visit a hospital), which might be a more valid test not only of the mechanisms behind descriptive norms (Lyu et al., 2024) but also of the selfish-rational approach, which frames vaccination as a social dilemma. Strictly speaking, vaccination can be considered a social dilemma only by those participants who perceive the costs of vaccination to be higher than the costs of the disease (Betsch et al., 2013). The opposite was true for the majority of participants in Experiment 1. Furthermore, while non-vaccinators in Experiment 2 endorsed fewer reasons in general, the endorsement of free-riding reasons was especially rare (Table 3). Taken together, these findings point to certain caveats when testing the assumptions of the selfish-rational approach, which can be addressed by future studies (e.g., the need to assure that vaccination costs are tangible or that participants understand the herd immunity mechanism).
To further explore the complex relationship between vaccination rates and vaccination intention, future studies would benefit from testing more than two or three levels of vaccination rates (e.g., Moussaoui et al., 2024) and from testing so-called dynamic descriptive norm messages (e.g., Milkman et al., 2022), such as “More and more people are getting vaccinated”.
Our analysis points to several potential boundary conditions for testing both the selfish-rational and the descriptive norms approach, representing important directions for future research. At the present state of empirical evidence, it seems that public communication surrounding vaccination rates will profit most by accounting for both approaches, closer to the notion of reasonable judgments. Specifically, our results suggest that when vaccination rates are low or unlikely to exert positive normative influence, public communication may emphasize individual benefit, overcoming the belief that vaccination is unnecessary to protect one’s health; when vaccination rates are high, public communication may leverage the power of descriptive norms and emphasize prosocial reasons for getting vaccinated. Self- versus other-benefit messages studied in Experiment 3 are, however, likely to be differentially effective for different groups of people (e.g., Ruggeri et al., 2024), for example, in terms of age, vulnerability or vaccine hesitancy, pointing to the need for public communication to assume a targeted approach.
Footnotes
Acknowledgments
This work is part of Aleksandra Lazić’s PhD thesis titled “Communicating vaccination coverage: Testing the selfish versus the social rationality hypothesis”, under the supervision of Iris Žeželj, PhD.
Author Contributions
Aleksandra Lazić (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Validation; Visualization; Writing - original draft; Writing - review & editing); Iris Žeželj (Conceptualization; Methodology; Supervision; Writing - review & editing).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was financially supported by the Ministry of Science, Technological Development and Innovation of the Republic of Serbia as part of the funding of scientific research at the University of Belgrade - Faculty of Philosophy (contract number 451-03-137/2025-03/200163). Experiments 2 and 3 were additionally supported by the SPSSI Researchers in the Global South Grant awarded to Aleksandra Lazić.