
Abstract
The vividness with which people can imagine positive events happening in their future has been linked to a number of different aspects of psychopathology and wellbeing. These relationships are hypothesised to arise from the role of mental imagery in thinking about the future and its close links to emotion. The current research investigated the associations between the vividness of positive future-oriented imagery, anhedonia, and positive affect via two cross-sectional studies. In a first study, a predominantly healthy young student sample (N = 79) completed measures of imagery, anhedonia, positive affect, and both questionnaire and lab-based measures of a range of aspects of psychopathology and wellbeing. A second study used baseline data from a clinical trial that recruited a transdiagnostic sample (N = 58) from two inpatient clinics. Results indicated a strong positive relationship between positive future-oriented imagery vividness and the experience of positive affect in both samples, whereas relationships between positive imagery vividness and anhedonia were also present but weaker. These results can inform further research to understand the role of mental imagery in both psychopathology and healthy functioning, and how it can be harnessed in interventions to reduce symptoms of psychopathology and increase wellbeing.
The experience of emotional mental imagery has been proposed to play a key role in anticipation of the future (e.g., Moulton & Kosslyn, 2009; Szpunar et al., 2007). The ‘as if reality’ nature of mental imagery (Ji et al., 2016) means that via imagery-based simulation of upcoming or potential future events we can ‘pre-experience’ how enjoyable or otherwise they may be, and this in turn can influence our motivation and behaviour (Renner et al., 2019). For example, if someone receives a message from a friend inviting them to join them for a walk, they might then imagine the experience of walking in pleasant weather through beautiful scenery while enjoying a lively conversation. Such a positive image-based simulation would likely increase their anticipation of the walk as enjoyable, and increase their motivation to accept their friend’s invitation. However, there are substantial variations between people in how vividly they are able to imagine such positive future experiences, and this has been linked to a number of different aspects of psychopathology and wellbeing.
One area of psychopathology that has been linked to reduced vividness of positive future-oriented mental imagery is anhedonia. Anhedonia is defined as the loss of interest in or pleasure from previously-enjoyed activities, and is a core symptom of major depressive disorder (American Psychiatric Association, 2013). Both theoretical conceptualisations and empirical research indicate that reduced anticipation of future enjoyment or reward is a key component of anhedonia (e.g., Hallford & Sharma, 2019; Pizzagalli, 2014). If imagery-based simulation of potential upcoming activities does play a core role in the extent to which these activities are anticipated as enjoyable or rewarding, then deficits in the ability to generate vivid positive future-oriented imagery could therefore plausibly contribute to anhedonia.
Preliminary empirical support for a relationship between deficits in the vividness of positive mental imagery and anhedonia comes from a number of sources. For example, one study found that within a sample of depressed individuals, lower ratings for vividness/detail when imagining positive future events were associated with lower ratings for how pleasurable it was to think about these events (Hallford et al., 2020a). While this ‘anticipatory pleasure’ (i.e. pleasure experienced when thinking about the event) is theoretically distinct from anticipated pleasure (the pleasure someone expects to experience when the event takes place), it is often seen as an important prerequisite, and lower levels of both have been found amongst people diagnosed with major depression or schizophrenia, disorders where anhedonia is a core symptom (Hallford & Sharma, 2019). A number of studies have in fact found that depression itself is associated with generation of less vivid positive future-oriented mental imagery (Holmes et al., 2016). Depression has also been found to be associated with reduced specificity for positive future episodic thinking, which can be considered indicative of difficulty generating future-oriented mental imagery (Gamble et al., 2019). In the context of schizophrenia spectrum disorders, reduced vividness of mental imagery has been shown to be related to lower levels of both anticipated and anticipatory pleasure (Pillny et al., 2024), although in this study it was general mental imagery vividness rather than the vividness of positive imagery specifically that was assessed. Convergent evidence has come from interventional studies suggesting that practice in generating positive imagery can increase anticipatory pleasure and reduce anhedonia (e.g., Blackwell et al., 2015; Hallford, Sharma, et al., 2020; Pictet et al., 2016).
While most of the research investigating the links between mental imagery and anhedonia has focussed on the role of imagery in anticipating in the future, deficits in the ability to experience vivid positive mental imagery could also be linked to anhedonia via other mechanisms. Anhedonia can be conceptualised as reflecting dysfunctions in positive affect systems (e.g., Pizzagalli, 2014), and thus factors that reduce the experience of positive affect could also lead to higher levels of anhedonia. Deficits in positive imagery could be one such factor, as retrieval of image-based representations from memory is thought to play an important role in processing of emotional events or scenes (e.g., Fiorito & Simons, 1994; Lang, 1979). Consistent with this perspective, one study found that people who can generate more vivid positive imagery show larger increases in positive mood when viewing positive (soothing) pictures (Wilson et al., 2017). Another study found that, when compared to repeated generation of positive sentences, repeated generation of positive imagery led to higher levels of emotional arousal when viewing positive (relative to neutral) pictures (Blackwell et al., 2025).
Better understanding the relationships between the ability to generate vivid positive future-oriented imagery, anhedonia, and positive affect is important not just in developing our theoretical understanding of these phenomena and their interplay, but also in helping development of interventions to reduce anhedonia and increase positive affect, which is an area of great clinical need (e.g., Alsayednasser et al., 2022; Craske et al., 2016, 2024). However, understanding these relationships requires not just examining them in isolation, but also in combination with other processes thought to be important in these contexts. For example, anhedonia is common in the context of depression, which is associated with a number of cognitive biases, such as a tendency to interpret ambiguous information negatively (Everaert et al., 2017). Individual differences in the vividness of positive future imagery have been associated with optimism, that is, people’s generalized tendency to expect the future to turn out well (Blackwell et al., 2013; Ji et al., 2017). Relationships found between positive imagery vividness and anhedonia or positive affect could therefore simply reflect shared variance with these other processes (e.g., interpretation biases or optimism) or other aspects of mental imagery (e.g., general tendency to experience imagery, or vividness of imagery in general).
We therefore aimed to investigate the relationship between vividness of positive future-oriented imagery and measures related to anhedonia and positive affect, while also taking into account their relationships with other potentially relevant processes, in order to shed further light on the hypothesised links. Specifically, we investigated whether the vividness with which people imagine positive events in their future is related to anhedonia, general levels of positive affect, and emotional reactions to positive stimuli, including when controlling for potentially confounding variables (e.g., other aspects of the experience of imagery, interpretation bias, optimism). To do so we first conducted a cross-sectional study collecting measures of these variables within an unselected student sample (Study 1). We expected to find that higher levels of vividness for positive future-oriented imagery would be associated with lower levels of anhedonia, higher levels of positive affect, and stronger positive emotional reactions to positive stimuli, including when controlling for other included variables. However, we did not have strong hypotheses about the relative strength and specificity of these relationships. Based on the results of the first study we then repeated our analyses within the baseline data collected as part of a clinical trial in two inpatient mental health clinics (Westermann et al., 2021), to see whether a similar pattern of results would be found within a clinical sample (Study 2).
Study 1
Methods
Design
The study was lab-based with a cross-sectional correlational design (“lab study”). It was pre-registered via uploading of the study protocol to the Open Science Framework prior to start of data collection (https://osf.io/c752u/).
Participants and Recruitment
Participants were recruited primarily from students at Ruhr-Universität Bochum, via methods such as posters on university premises, social media (e.g., Facebook), and the department Web site. Participants could enter a prize draw for one of 8 €15 Amazon.de vouchers as an incentive for participation, and psychology students at Ruhr-Universität Bochum could also receive course credit. The inclusion criterion was age 18–35 (to recruit a relatively homogenous sample), and the exclusion criterion was self-reported blood/injury/injection phobia or risk of fainting when seeing blood (to avoid very negative reactions to negative visual stimuli used in the study). A sample size of N = 80 was planned; this was a pragmatic decision in the absence of relevant data to guide a power calculation. It would provide sufficient participant numbers to carry out linear regressions with a small number of predictors, and 80% power to detect small-to-medium changes in R2 in a multiple regression. For practical reasons related to availability of researchers to conduct testing and the COVID-19 pandemic, the study was stopped after 79 participants had been tested.
Materials
Measures of Mental Imagery
Prospective Imagery Test (PIT; Holmes et al., 2008; Stöber, 2000)
The PIT is a measure of the vividness with which people can imagine positive or negative events happening in their future, and has been widely-used in both clinical (e.g., Morina et al., 2011) and healthy (e.g., Blackwell et al., 2013) samples. Participants read a list of 10 positive and 10 negative hypothetical future scenarios and are asked to form a mental image of each, before rating how vivid their image is from 1 (not at all vivid) to 5 (very vivid). Mean vividness ratings were calculated separately for positive and negative items. The German version from Morina et al. (2011) was used. Cronbach’s alpha in our sample was α = 0.78, 95% Confidence Intervals (bootstrapped) = [0.70, 0.83] for the positive items, and α = 0.82 [0.74, 0.87] for the negative items.
Spontaneous Use of Imagery Scale (SUIS; Reisberg et al., 2003)
The SUIS is a measure of the tendency to experience (non-emotional) imagery in everyday life. It comprises 12 items that participants rate on a scale from 1 (never appropriate) to 5 (always completely appropriate). A total score was created by summing the individual item scores. The 12-item German version by Görgen et al. (2016) was used. Cronbach’s alpha in our sample was α = 0.59 [0.36, 0.72].
Involuntary Autobiographical Memory Inventory (IAMI; Berntsen et al., 2015)
The IAMI measures how frequently participants experience past (10 items) and future-oriented (10 items) involuntary autobiographical memories in daily life. It was included in this study as a measure of another aspect of the experience of imagery. Each item asks about the experience of involuntary memories or future projections in different everyday situations, and participants rate their frequency with which they experience these on a scale from zero (never) to 4 (once an hour or more). An additional four items measure the valence and intensity of these involuntary memories / future projections on scales from −2 (extremely negative) to +2 (extremely positive) or zero (not at all intense) to 4 (extremely intense) respectively. The German translation from Blackwell et al. (2020) was used. For our analyses we used the total score, obtained via summing all 20 items, and Cronbach’s alpha in our sample was α = 0.93 [0.90, 0.95].
Measures of Anhedonia and Positive Affect
Dimensional Anhedonia Rating Scale (DARS; Rizvi et al., 2015)
The DARS is a self-report measure of different facets of anhedonia (desire, motivation, effort and consummatory pleasure) across different hedonic domains (hobbies/past-times, food/drinks, social activities, and sensory experiences), and has been validated in both clinical (Rizvi et al., 2015) and healthy (Wellan et al., 2021) samples. For each hedonic domain participants are asked to list two or three of their favourite activities or experiences, and they then answer questions assessing desire, anticipated enjoyment, and other facets of anhedonia on scales from zero (not at all) to 4 (very much). An extended 26-item version was used in a German translation as reported by Blackwell et al. (2018), with the individual item scores summed to create a total score. Cronbach’s alpha in our sample was α = 0.91 [0.84, 0.94].
Positive and Negative Affect Schedule – Positive Subscale (PANAS-P; Watson & Clark, 1994)
The 21-item positive subscale of the PANAS (i.e. including the joviality, self-assurance, attentiveness, and serenity scales) was administered as a measure of positive affect, with participants instructed to rate to what extent they had experienced each of the 21 emotion words listed over the “past few weeks” on a scale from 1 (very slightly or not at all) to 5 (extremely). The PANAS has been validated across both clinical and healthy samples (e.g., Watson & Clark, 1994). The German translation by Grühn et al. (2010) was used. Cronbach’s alpha in our sample was α = 0.93 [0.90, 0.95].
Emotional Picture Rating Task (EPRT)
The EPRT was administered as a measure of emotional reactivity to positive, negative, and neutral material, specifically photographs of scenes/objects, and adapted from that used by Craske et al. (2023). Participants viewed a series of pictures (8 positive, 8 negative, and 8 neutral) from the International Affective Picture System (IAPS; Lang et al., 2008). Pictures were presented for 6 s each on the computer screen, and afterwards participants were asked to rate their emotional response to the image in terms of valence and arousal, both using a 1 to 9 Self-Assessment Manikin (SAM; Bradley & Lang, 1994). Pictures were presented in a random order, with the constraint that not more than two pictures of the same valence should be presented in a row. The EPRT was implemented as a Java desktop application. Split-half reliabilities for valence ratings were: positive: 0.62 [0.40, 0.76]; negative: 0.74 [0.60, 0.84]; neutral: 0.74 [0.59, 0.83]. Split-half reliabilities for arousal ratings were: positive: 0.77 [0.63, 0.85]; negative: 0.91 [0.86, 0.94]; neutral: 0.93 [0.88, 0.95].
Other Measures
Depression Anxiety Stress Scales – 21 item version (DASS-21; Lovibond & Lovibond, 1995)
The DASS is a questionnaire comprising three subscales of 7-items each: depression, stress, and anxiety. Participants are asked to respond according to how applicable each item is to how they have been feeling in the past week on a scale from zero (Did not apply to me at all) to 3 (Applied to me very much, or most of the time). The German version by Nilges and Essau (2015) was used. Cronbach’s alpha in our sample was α = α = 0.87 [0.80, 0.91] for the depression subscale, α = 0.73 [0.55, 0.83] for the anxiety subscale, and α = 0.84 [0.75, 0.89] for the stress subscale.
Positive Mental Health Scale (PMH; Lukat et al., 2016)
This questionnaire consists of 9 items designed to assess positive mental health, each rated on a scale from zero (not at all true) to 3 (completely true). It was included to explore its potential relationships with the measures of positive affect/anhedonia and positive imagery. Cronbach’s alpha in our sample was α = 0.87 [0.82, 0.90].
Life Orientation Test - Revised (LOTR; Scheier et al., 1994; German version: Glaesmer et al., 2008)
The LOTR is a self-report measure of dispositional optimism, in which participants rate the appropriateness to themselves of 10 statements, 3 of which are positively worded (e.g., “In uncertain times, I usually expect the best”), 3 of which are negatively worded and reverse-scored (e.g. “If something can go wrong for me it will”), and 4 of which are filler and not used in scoring. In the German version the items are rated on a scale from zero (completely appropriate) to 4 (does not apply at all), such that higher scores indicate lower levels of optimism. Cronbach’s alpha in our sample was α = 0.77 [0.68, 0.83].
Scrambled Sentences Test (SST; Rude et al., 2002; Würtz et al., 2022)
The SST was used as a measure of negative interpretation bias, to assess a non-imagery cognitive bias and potentially control for these in analyses (as in Ji et al., 2017). A paper-based version of the SST was the primary version used for this purpose in the study. A newly-developed computerized version was also administered, but this was used in this study for piloting purposes only and is described in the Supplemental Material. All participants completed both versions of the SST, with the order counterbalanced (see Procedure section). In the paper-based version, participants were presented with a set of 20 scrambled sentences (e.g. “winner born I am loser a”) and instructed to write a number above five of the six words in order to construct a grammatically correct sentence, while holding in mind a six digit number (‘cognitive load’). This is intended to measure the tendency of participants to interpret ambiguous information either positively (“I am a born winner”) or negatively “I am a born loser”). A German version adapted from that by Rohrbacher and Reinecke (2014) was used. A ‘negativity’ score, calculated as the proportion of sentences completed correctly that were completed with a negative valence, was the main outcome. Two different sets of 20 sentences were used (set A, set B), with allocation following a preset counterbalancing scheme. For set A (n = 42), split-half reliability was 0.52, 95% CIs [0.42, 0.83], with 37 (88%) participants recalling the cognitive load number correctly; for set B (n = 37), split-half reliability was 0.48, 95% CIs [0.31, 0.82], with 31 (84%) participants recalling the cognitive load number correctly.
Single Target Implicit Association Test (STIAT; Bluemke et al., 2017; Wigboldus et al., 2004)
The STIAT was included as an assessment of automatic associations between positive/negative affect-relevant attributes and targets related to the self. Positive attribute words were happy, relaxed, excited, optimistic, active, cheerful, lively, determined; negative attribute words were sad, anxious, apathetic, hopeless, tired, depressed, tense, stunned 1 . Target words were self, mine, I, me. Participants were asked to categorise words appearing in the middle of the screen using the keys E and I. The STIAT started with a practice attribute block (20 trials), in which the attribute words were presented in the centre of the screen and participants were asked to categorise according to the attribute labels “Positive” and “Negative” on the top left and top right of the screen, respectively. This was followed by two ‘compatible’ blocks of 20 and then 40 trials in which either attribute or target words were presented in the centre of the screen, and the target label “I” was shown underneath the attribute label “Negative” in the top-right corner of the screen. Attribute words and labels were shown in white, and target words and the target label were shown in green. Finally, there were two ‘incompatible’ blocks of 20 and then 40 trials in which the either target and attribute words were shown in the centre of the screen, but the target label ‘I’ now joined the attribute label “Positive” in the top-left corner of the screen. The STIAT was introduced as a reaction time task, and participants were asked to respond as quickly as possible but also make as few mistakes as possible. If participants made an error, a red cross was shown on the screen and the task continued once participants had corrected their error. We expected that people with stronger self-positive associations (compared to self-negative associations) should be slower to categorise words in the ‘compatible’ blocks compared to the ‘incompatible’ blocks. Scoring for the STIATs followed the procedure detailed by Bluemke and Friese (2008), and more positive values indicated stronger self-positive associations. This task was also used in the clinical study by Westermann et al. (2021) and was included to find out more about its relationship with the other measures and assess its suitability as an indirect measure of positive affect. Split-half reliability (based on 5000 randomly-determined split halves) was 0.64 [0.50, 0.74].
Procedure
Participants were tested individually by one of four student researchers in one of 3 different laboratories at the university. The researcher guided the participants through the study procedures according to a written experimental protocol. All questionnaires were completed on paper. On arrival at the lab, participants were asked to read the study information sheet again and given the opportunity to ask questions, after which they provided written informed consent. Participants then completed the measures in the following (fixed) order: Demographic information, SST (either the paper or computerized version according to counterbalance order), DARS, Emotional Picture Rating Task (ERPT), SUIS, PIT, PMH, LOT-R, IAMI, IAT, PANAS, DASS-21, SST (whichever version, paper or computerized, the participant had not yet completed). At the end of the procedure participants were debriefed and thanked for their time.
Statistical Analyses
Statistical analyses were conducted in RStudio v.2024.04.2 Build 764 (RStudio, Inc., 2016) running R version 4.3.2. (R Core Team, 2023), and followed the statistical analysis plan outlined in the pre-registration. The main dependent variable was vividness ratings for positive items on the PIT (PIT-PV), and the main independent variables of interest were anhedonia (measured by the DARS), positive affect (measured by the PANAS-P), and emotional reactions to positive stimuli (measured by the EPRT). As a first step, zero-order correlations between the variables collected were calculated. For each relevant independent variable (DARS, PANAS-P, EPRT) found to have a statistically significant zero-order relationship with vividness ratings for positive items on the PIT (PIT-PV) a separate regression was then conducted with PIT-PV as outcome variable. The predictor variable of interest was entered as a first step in the regression, and then other potentially relevant predictor variables (e.g. age, gender, DASS scores) entered in subsequent steps to probe the potential specificity of the relationship between the predictor variable of interest and PIT-PV (see e.g. Ji et al., 2017). Those measures shown to have a robust relationship with PIT-PV were then entered together into a regression to explore possible shared/unique variance in these measures of different aspects of anhedonia/positive affect and their relationship with positive prospective imagery vividness. The assumptions underlying the regression were checked following the steps outlined by Field et al. (2012, pp. 288–301), and robustness of the results further checked via calculation of 10,000 bootstrapped 95% confidence intervals for the regression coefficients.
Results
Correlations with Positive Imagery Vividness
Participant Characteristics and Correlations With Imagery Variables in Study 1 (Non-Clinical Sample).
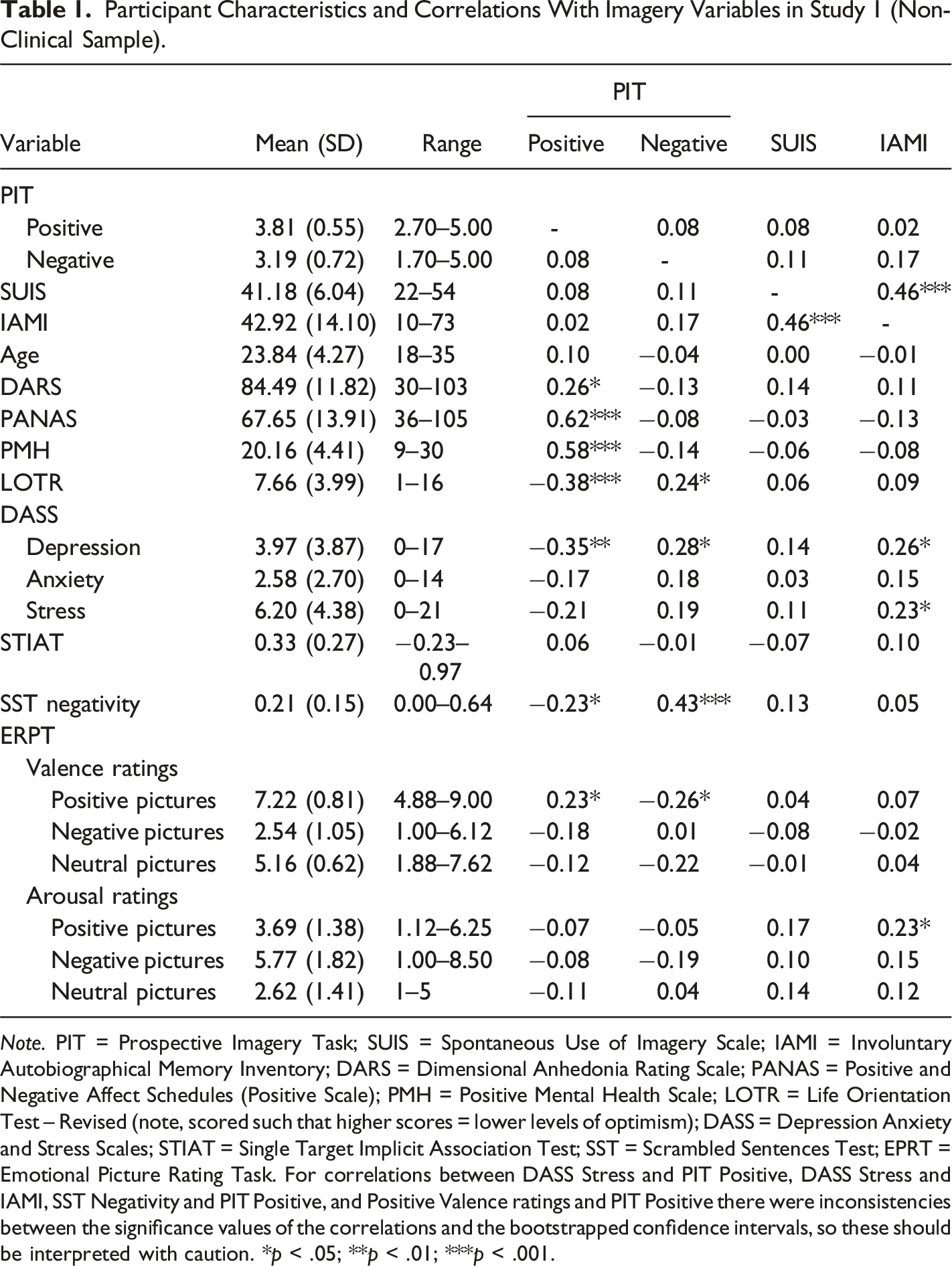
Note. PIT = Prospective Imagery Task; SUIS = Spontaneous Use of Imagery Scale; IAMI = Involuntary Autobiographical Memory Inventory; DARS = Dimensional Anhedonia Rating Scale; PANAS = Positive and Negative Affect Schedules (Positive Scale); PMH = Positive Mental Health Scale; LOTR = Life Orientation Test – Revised (note, scored such that higher scores = lower levels of optimism); DASS = Depression Anxiety and Stress Scales; STIAT = Single Target Implicit Association Test; SST = Scrambled Sentences Test; EPRT = Emotional Picture Rating Task. For correlations between DASS Stress and PIT Positive, DASS Stress and IAMI, SST Negativity and PIT Positive, and Positive Valence ratings and PIT Positive there were inconsistencies between the significance values of the correlations and the bootstrapped confidence intervals, so these should be interpreted with caution. *p < .05; **p < .01; ***p < .001.
Relationship between Positive Imagery Vividness, Anhedonia, Positive Affect, and Valence Ratings for Positive Pictures
Anhedonia
In a series of regressions with mean vividness rating for positive items on the PIT as dependent variable, in the final model (including scores on the DARS, gender, age, SUIS, negative PIT vividness, IAMI, and DASS depression as predictors), DARS remained a statistically significant predictor of PIT Positive vividness ratings, B [95% CIs] = 0.01 [0.0006, 0.02], SEB = 0.01, β [95% CIs] = 0.24 [0.02, 0.46], SE β = 0.11, t = 2.22, p = .030.
Positive Affect
When PANAS scores were included instead of DARS scores in a similar series of regressions, in the final model (including PANAS, gender, age, SUIS, negative PIT vividness, IAMI, and DASS depression as predictors), PANAS remained a statistically significant predictor of PIT Positive vividness ratings, B [95% CIs] = 0.03 [0.02, 0.04], SEB <0.01, β [95% CIs] = 0.68 [0.44, 0.91], SE β = 0.12, t = 5.70, p < .001.
Valence Ratings for Positive Pictures
When valence ratings for positive pictures were included instead of DARS or PANAS scores in a similar series of regressions, inclusion of DASS depression scores in the final model (including positive valence ratings, gender, age, SUIS, negative PIT vividness, IAMI, and DASS depression as predictors), rendered positive valence ratings no longer a statistically significant predictor of PIT Positive vividness ratings, B [95% CIs] = 0.14 [−0.03, 0.28], SEB = 0.08, β [95% CIs] = 0.20 [−0.02, 0.42], SE β = 0.11, t = 1.81, p = .074.
Combined Regression Analysis
Regression From Study 1 (Non-Clinical Sample) With PIT Positive Vividness Ratings as Dependent Variable.
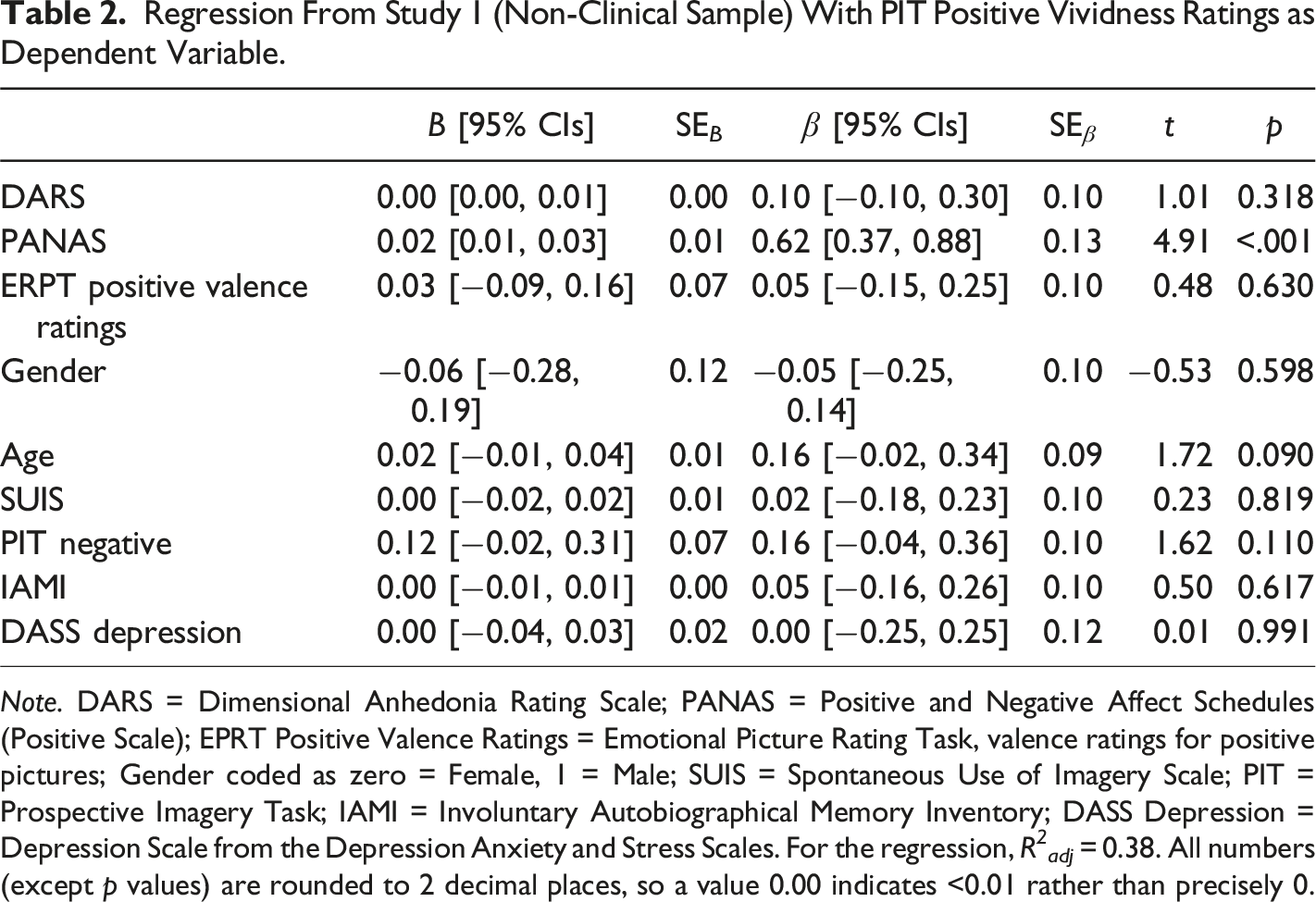
Note. DARS = Dimensional Anhedonia Rating Scale; PANAS = Positive and Negative Affect Schedules (Positive Scale); EPRT Positive Valence Ratings = Emotional Picture Rating Task, valence ratings for positive pictures; Gender coded as zero = Female, 1 = Male; SUIS = Spontaneous Use of Imagery Scale; PIT = Prospective Imagery Task; IAMI = Involuntary Autobiographical Memory Inventory; DASS Depression = Depression Scale from the Depression Anxiety and Stress Scales. For the regression, R 2 adj = 0.38. All numbers (except p values) are rounded to 2 decimal places, so a value 0.00 indicates <0.01 rather than precisely 0.
Discussion
In a predominantly healthy sample of students we found the expected relationships between vividness of deliberately generated positive future imagery, as measured by the Prospective Imagery Test, and measures related to experience of positive emotions and anhedonia: positive affect over the past few weeks (PANAS), anhedonia (DARS), and ratings of the valence of (but not arousal from) positive pictures, as well as further measures of positive mental health (PMH) and optimism (LOTR) that had been investigated in previous studies (Bibi et al., 2021; Blackwell et al., 2013; Ji et al., 2017). The measures of positive affect and anhedonia explained unique variance in positive imagery vividness above that explained by demographic factors, other imagery measures, and symptoms of depression. However, of the three main measures investigated (positive affect, anhedonia, valence rating of positive pictures), only positive affect explained unique variance in positive imagery vividness when all three were included in a final regression. Additionally, the relationship between positive affect and positive imagery vividness remained statistically significant when further controlling for other positive measures (PMH, LOTR), further providing evidence for specificity of this relationship. Interestingly, in this exploratory additional regression PMH scores were also a significant predictor of scores on the PIT, indicating some non-shared variance with positive affect.
One limitation of the study however is that while many of the measures are relevant to mental health and psychopathology, the sample was predominantly healthy with few experiencing clinical or sub-clinical symptoms of depression or anxiety. Finding similar patterns in a clinical sample would provide greater confidence in drawing conclusions about mental health and psychopathology.
Study 2
In study 2 we investigated whether we would find a similar pattern of results using data collected from a clinical sample, specifically inpatients in two mental health clinics in Germany, using baseline data from a feasibility trial (see Blackwell et al., 2018; Westermann et al., 2021 for full details).
Method
Design
The study was a randomized controlled feasibility trial, but here only baseline (i.e. cross-sectional, pre-randomization) data is presented. It was approved by the ethics committee of the Faculty of Psychology, Ruhr-University Bochum (No. 325), and prospectively registered (clinicaltrials.gov: NCT02958228). Study materials (with the exception of standardized questionnaires available from the provider), original protocol, computer software for the training interventions, anonymous research data, and analysis scripts for the trial publication (Westermann et al., 2021) are available at https://osf.io/gm4fw/.
Participants and Recruitment
Participants (n = 58; Gender: 30 men and 28 women, Age: M = 45.3 years, SD = 13.20, range = 18–65) were recruited from two clinics offering inpatient treatments for mental health in Germany. Inclusion criteria were: aged 18 or above, sufficient German language skills, and receiving treatment in the inpatient clinic during the timeframe of the study. The exclusion criterion was existence of a condition or circumstances that could interfere with completion of the study procedures (e.g., severe visual impairment, neurological problem, acute psychosis, or substance withdrawal symptoms). If the participant was judged to meet these inclusion/ no exclusion criteria a next meeting for a next assessment was arranged, at which the baseline data reported in this paper were collected. The final sample size was determined by pragmatic constraints (see Westermann et al., 2021).
Materials
Measures of Mental Imagery
In this study, only the PIT was collected, using a shorter version with 5 positive and 5 negative items from the full scale as reported in study 1. The remaining 5 positive and 5 negative items were administered at the post-training assessment and not reported here. Cronbach’s alpha [95% CIs] was 0.86 [0.80, 0.91] for positive items and 0.75 [0.63, 0.84] for negative items.
Measures of Positive Affect and Anhedonia
The DARS, PANAS and STIAT were collected in this study as per study 1, with the exception that the PANAS asked about “the past week” rather than “the past few weeks”. Cronbach’s alphas were 0.93 [0.89, 0.95] for the DARS, and 0.94 [0.91, 0.96] for the PANAS, and split-half reliability for the STIAT was 0.66 [0.43, 0.80]. The EPRT was not administered.
Other Measures
The PMH and the paper-based SST were administered as described in Study 1, but the LOT-R was not used. As measures of depression and anxiety, instead of the DASS-21, the Quick Inventory of Depressive Symptomatology (QIDS; Roniger et al., 2015; Rush et al., 2003) and the GAD-7 (Hinz et al., 2017; Spitzer et al., 2006) were used. The QIDS is a 16-item self-report questionnaire assessing symptoms of depression over the previous week, with answers provided on a scale from zero to 3 (unique anchors for each item). Cronbach’s alpha was 0.80 [0.71, 0.87]. The GAD-7 asks about frequency of symptoms of generalized anxiety over the past 2 weeks, with answers provided on a scale from zero (not at all) to 3 (nearly every day). Cronbach’s alpha was 0.88 [0.82, 0.92].
Procedure
Data reported here were collected by one of two researchers in a face-to-face assessment prior to randomization and first intervention session. Participants completed the PANAS-P, PMH, QIDS-SR, GAD-7, PIT, SST and STIAT in this order.
Statistical Analyses
Statistical analyses were as for study 1.
Results
Comparison of Sample Characteristics with Study 1
In comparison to the study in study 1, the sample in study 2 was older, had a smaller proportion of female participants, scored lower on the PIT-Positive and on the DARS, and scored higher on the SST (all ps < .05). There was no difference between the two samples for scores on the PIT-Negative or STIAT (ps > .30). Due to differences in the measures used, the other measures could not be compared between the two samples.
Correlations with Positive Imagery Vividness
Participant Characteristics in Study 2 (Clinical Sample).
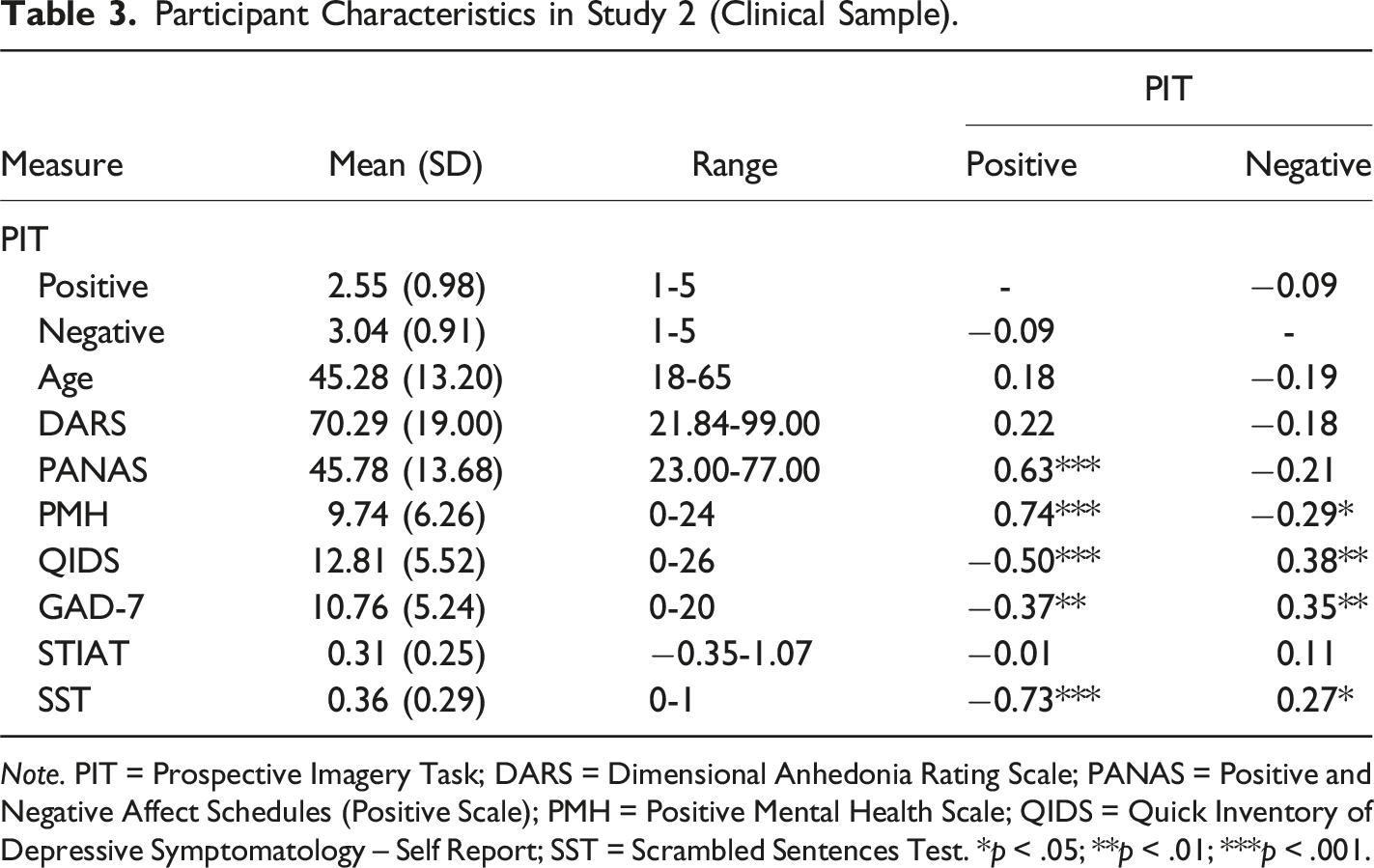
Note. PIT = Prospective Imagery Task; DARS = Dimensional Anhedonia Rating Scale; PANAS = Positive and Negative Affect Schedules (Positive Scale); PMH = Positive Mental Health Scale; QIDS = Quick Inventory of Depressive Symptomatology – Self Report; SST = Scrambled Sentences Test. *p < .05; **p < .01; ***p < .001.
Regression From Study 2 (Clinical Sample) With PIT Positive Vividness Ratings as Dependent Variable.
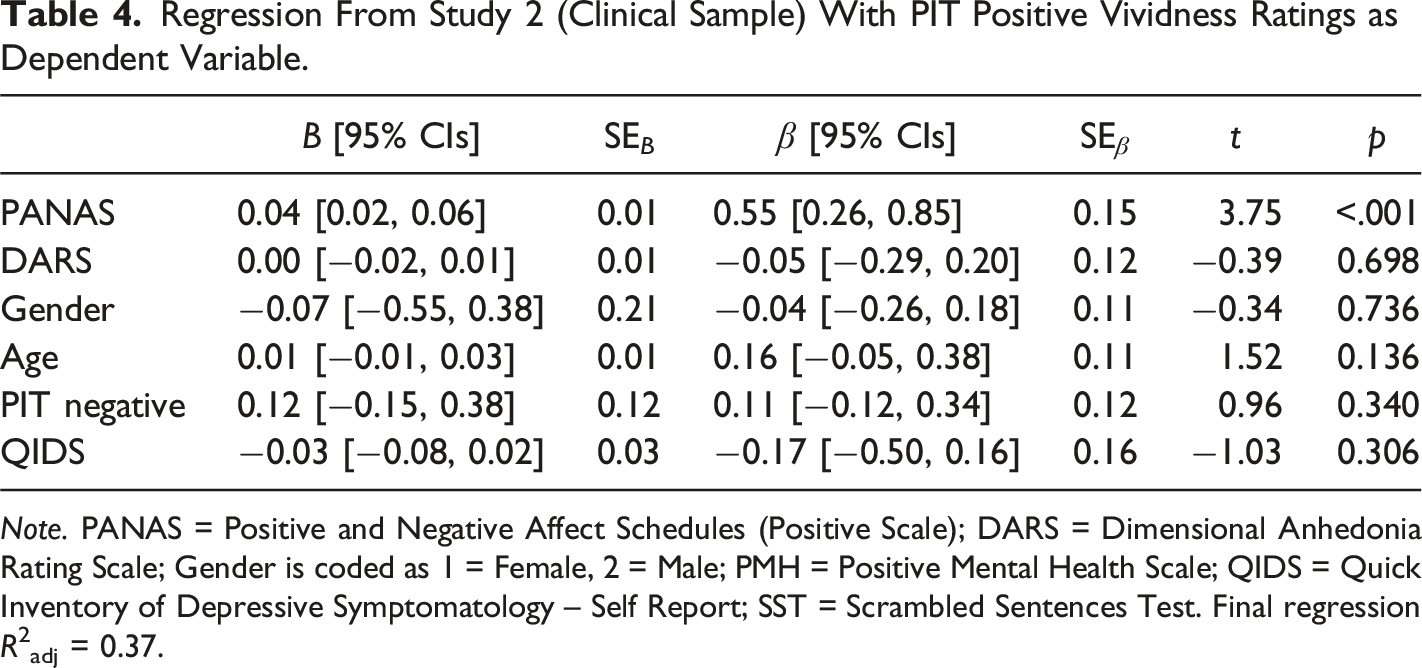
Note. PANAS = Positive and Negative Affect Schedules (Positive Scale); DARS = Dimensional Anhedonia Rating Scale; Gender is coded as 1 = Female, 2 = Male; PMH = Positive Mental Health Scale; QIDS = Quick Inventory of Depressive Symptomatology – Self Report; SST = Scrambled Sentences Test. Final regression R2adj = 0.37.
Relationship between Positive Imagery Vividness, Anhedonia and Positive Affect
As the zero-order correlation between DARS score and PIT positive vividness scores was not statistically significant, we only investigated specificity of relationship between PANAS scores and PIT positive vividness scores. In a final regression, when controlling for age, gender, QIDS score, PIT negative vividness score, and DARS score, PANAS score remained a significant predictor of PIT positive vividness scores, B [95% CIs] = 0.04 [0.02, 0.06], SEB = 0.01, β [95% CIs] = 0.55 [0.26, 0.85], SE β = 0.15, t = 3.75, p < .001 (Table 4).
As in Study 1, we ran an additional exploratory analysis further including PMH scores in the regression. In contrast to the findings of Study 1, we found that having included PMH scores, the relationship between PANAS scores and PIT-Positive was much reduced and no longer statistically significant, B [95% CIs] = 0.01 [−0.02, 0.03], SEB = 0.01, β [95% CIs] = 0.13 [−0.19, 0.46], SE β = 0.16, t = 0.85, p = .401, whereas PMH was a statistically significant predictor of PIT-Positive, B [95% CIs] = 0.11 [0.06, 0.17], SEB = 0.03, β [95% CIs] = 0.73 [0.39, 1.07], SE β = 0.17, t = 4.30, p < .001.
Discussion
As in Study 1, positive affect showed strong associations with positive future imagery vividness, and seemed to explain unique variance above age, gender, depression, and anhedonia. While anhedonia, as measured by the DARS, had a similar zero-order correlation with positive future imagery vividness, this was not statistically significant and further potential specificity was not explored in detail. In contrast to the exploratory analyses in Study 1, the relationship between PANAS and PIT-Positive was subsumed by the shared variance with PMH scores.
General Discussion
In a cross-sectional study with an unselected student sample and baseline data from an RCT amongst an inpatient sample with a range of diagnoses, self-reported vividness of positive future imagery was found to have strong and relatively specific associations with positive affect. While positive future imagery vividness was found to show a moderate zero-order relationship with anhedonia (albeit not statistically significant in the smaller patient sample), there did not appear to be unique shared variance between these measures after controlling for levels of positive affect. Affective response to positive pictures, as indexed by ratings of valence, was positively associated with vividness of positive future imagery in the student sample, but this was a weaker and relatively unspecific relationship.
The strong and apparently specific relationship between positive affect and positive future imagery, whether over the past few weeks as in the student sample (Study 1) or the past week as in the inpatient sample (Study 2) could be understood in a number of ways. It seems plausible that for people who are experiencing higher levels of positive emotions in their daily life, the positively-valenced autobiographical material that forms the basis for positive future projections would be more accessible (Kensinger & Ford, 2020; Lewis et al., 2005), and thus it would be easier for them to generate more vivid positive mental imagery; from this perspective very vivid positive prospective imagery would be understood as a consequence of high levels of positive affect. Another possibility is that people with high vividness ratings for positive items on the PIT may tend to experience more vivid future-oriented imagery in daily life, leading to more frequent and intense experiences of positive affect; observational data suggest that spontaneous future thoughts in daily life that are richer in imagery are associated with a higher level of emotional response (Barsics et al., 2016). From this perspective, higher levels of positive affect would be understood as a consequence of the experience of more vivid positive imagery. Of course, these two explanations are not mutually exclusive, and both mechanisms could contribute to the relationship observed in this study. A third possibility is that the relationship between positive imagery vividness and positive affect in daily life is best understood in terms of higher vividness ratings for positive future-oriented imagery on the PIT reflecting greater accessibility of positive autobiographical material in memory. Previous research has found that people who generate more vivid positive future imagery (on the PIT) experienced greater emotional reactions to viewing positive pictures (Wilson et al., 2017). Further, research into aphantasia (lack of mental imagery) has indicated that the spontaneous experience of imagery may be crucial in emotional responses when reading text (Wicken et al., 2019). In line with Peter Lang’s bioinformational theory of mental imagery (Ji et al., 2016; Lang, 1979), emotional responses to many situations likely involve (and are influenced by) activation and retrieval of image-based representations in memory; if positive image-based representations are easily accessible and readily retrieved, then many more situations are likely to trigger experience of positive affect, or more intense positive affect, and such people would also tend to generate more vivid positive imagery on the PIT.
The weaker and less specific relationships between anhedonia and positive imagery vividness found in these studies is surprising given the hypothesised role of imagery in anticipating future events, a core component of anhedonia. From the perspective of a causal role for imagery generation in anticipated enjoyment from events or activities, it is possible that some other aspect of imagery rather than vividness is more important, such as relative tendency to experience imagery when thinking about the future, or a bias to experience positive relative to negative imagery (although we might expect these to be correlated with vividness ratings on the PIT). Another possibility is that the mechanism via which imagery is related to anhedonia (in terms of anticipated pleasure) is via its effect on emotion, that is a mediation model that would be consistent with the results of our regression in the student sample (i.e. that when controlling for positive affect, the relationship between positive imagery vividness and anhedonia is no longer statistically significant, with the caveat that this is partially-retrospective cross-sectional data). However, it is also important to consider the possibility that the DARS may have limitations in measuring anhedonia, as it is dependent on participants’ ratings of their expectations in that moment, which be affected by current mood, the task context, and other factors such as the extent to which participants spontaneously imagine the activities while making their ratings (Ji et al., 2025), all of which may make it more variable and ‘noisy’ than a retrospective evaluation over a longer time period. Further, within a healthy sample scores tend to be skewed and show ceiling effects, reducing its sensitivity. Notably however it was in the clinical sample (study 2) that the zero-order correlation between scores on the DARS and positive imagery vividness ratings on the PIT was not statistically significant. Given that the magnitude of the correlation was similar to that found in the healthy sample, the most plausible explanation may be that this reflects the smaller sample size in study 2. Overall, the conclusion that the association between positive imagery vividness and anhedonia was weaker than that between positive imagery vividness and positive affect applies to the results of both studies.
In relation to emotional response to pictures, this was only measured within the student sample and although valence ratings of positive pictures correlated with positive imagery vividness, this seemed to be a relatively unspecific relationship that potentially reflects shared variance with a third variable such as depressed mood or interpretation bias. Our results are however partially consistent with those of Wilson et al. (2017), who found that people scoring higher on the PIT showed greater positive emotional reactions to soothing pictures. However, we did not measure mood change directly in the current study and potentially this is where a more specific relationship would be found.
An interesting contrast in the results between the student and inpatient sample is the relationship between scores on the positive mental health scale (PMH) and PIT positive imagery vividness in our exploratory analyses. In the student sample, inclusion of the PMH (and optimism, measured by the LOT-R) left the relationship between PANAS scores and PIT positive vividness scores still statistically significant, providing further evidence for the specificity of this relationship. By contrast, including the PMH in a regression in our inpatient sample rendered the relationship between PANAS scores and PIT positive vividness no longer statistically significant (whereas the relationship between PMH scores and PIT positive vividness was significant). It is difficult to speculate as to why this specific different pattern of results might be found in the two samples, but one possibility might be that within the clinical sample, positive affect was simply one aspect of positive mental health and thus subsumed under this measure, whereas within the healthy sample, there could be meaningful variations in positive affect independent of (generally higher) levels of positive mental health. Overall, this finding highlights the possibility that the relationship between the different variables (or the aspects of experience that they measure) likely varies depending on their level. Notably, the lowest score on the PIT positive vividness scale in the student sample was higher than the mean in the inpatient sample; it may be that variations in vividness corresponding to scores between 3 and 5 on the PIT have little impact, whereas variations corresponding to scores between 1 and 3 are more important. For example, if imagery is below a certain ‘threshold’ vividness it may not be noticed if it occurs spontaneously in daily life (e.g., Barzykowski & Staugaard, 2016). This therefore highlights the importance of investigating psychological processes across different levels of wellbeing and psychopathology, as individual differences may only start to become consequential towards the upper or lower limits of the range.
The findings of the current study complement those that have investigated the relationships between vividness of positive future imagery, as measured via the PIT, and depression (see e.g., Holmes et al., 2016, for a review), optimism (e.g., Blackwell et al., 2013; Ji et al., 2017), and positive mental health (Bibi et al., 2021), as well as those focussing on broader or other measures of future imagery and other aspects of psychopathology such as anticipatory pleasure (Hallford et al., 2020a) or anxiety (Du et al., 2022). The overall picture that emerges is that vividness of positive future imagery shows associations with these ‘positive’ measures that do not simply seem to reflect general use of imagery or emotional imagery in general, but are rather specific to imagery that is positive in valence. The results of the current study further indicate (similar to those of Bibi et al., 2021) that these reltionships are not simply due to the PIT being a positively-worded measure (for positive items at least), but rather due to there being something specific about what it is asking participants to do – potentially the requirement to generate imagery (although in the absence of a completely comparable non-imagery control measure this remains to be tested). The results of the current study indicate that at least within a relatively healthy sample the relationship is most specifically with positive affect in daily life, which subsumes other relationships with anhedonia, optimism, or positive mental health more broadly; within the patient sample the broader measure of positive mental health showed the stronger relationship. These results can therefore be used to guide development or theoretical models of the relevance of positive imagery in healthy functioning and the routes via which it may impact of aspects of healthy functioning, which could then be tested out via suitable longitudinal and experimental methods.
The results also support the suggestion that interventions that increase individuals’ vividness ratings for positive items on the PIT could be beneficial in improving the experience of positive affect (either as an intervention, or for preventive purposes) and reducing anhedonia. However, an important question here is whether such interventions should best be constructed with a view to increasing imagery vividness per se, or whether the ‘beneficial’ aspect of higher scores on the PIT instead reflects something else that would be better targeted, such as accessibility of positive imagery – how this is conceptualised might lead to different kinds of interventions. Of studies investigating the potential of positive imagery generation to reduce anhedonia, the majority of these have used a positive imagery cognitive bias modification (positive imagery CBM) approach (Blackwell et al., 2015; Blackwell & Holmes, 2010). In the most commonly-used form of positive imagery CBM, participants listen to audio recordings of a series of training scenarios, which are descriptions of mostly everyday situations that start ambiguous but always resolve positively. Participants are instructed to imagine themselves experiencing the scenarios while they listen, as if they were actively involved. The aim of this intervention is not so much to increase the vividness with which participants can imagine positive imagery, but rather to increase their tendency to imagine positive outcomes for ambiguous situations in daily life. It has been suggested that a potential mechanism via which this could have an impact in daily life is that the positive imagery generated during the training is spontaneously retrieved when the participants encounter similar situations in daily life (Blackwell & Holmes, 2017); from this perspective the training may be seen as increasing the accessibility of positive autobiographical material in memory. Several studies have investigated the impact of positive imagery CBM on imagery vividness as measured by the PIT, and the results are somewhat mixed in that some studies find a pattern of result consistent with a greater increase in positive imagery vividness after imagery compared to a control condition (Bibi et al., 2020; Blackwell et al., 2023; Murphy et al., 2015), others do not (Blackwell et al., 2015; Westermann et al., 2021). When it comes to the effect of the training on positive affect, while earlier experimental studies had shown the effect of a single session of imagery CBM on state positive affect (e.g., Holmes et al., 2009), the effects on positive affect in daily life are relatively under-researched. Bibi et al. (2020) found a greater increase in positive affect (self-reported over the past week) after a brief imagery CBM training schedule compared to a sham training control condition, albeit in a pilot study. In contrast, Westermann et al. (2021) did not find a pattern of results consistent with a greater increase in positive affect after a two-week imagery CBM training compared to treatment as usual or cognitive control training in an inpatient sample, albeit in small feasibility study. However, when it comes to the effect of imagery CBM on anhedonia, the results are more consistent: Several studies have found greater reductions in anhedonia compared to a sham training control when measured via anhedonia items on a depression questionnaire (Blackwell et al., 2015; Pictet et al., 2016; Williams et al., 2015), and some subsequent studies have also found results consistent with this using the DARS as a dedicated anhedonia measure (Bibi et al., 2020; Blackwell et al., 2023; Westermann et al., 2021). In general, the results from these studies suggest anhedonia, measured via the DARS, may be better targeted by imagery CBM than positive affect in daily life. However, in the absence of larger trials showing these results this remains an open question. Studies using other kinds of interventions involving imagining positive situations have found effects on optimism (e.g., Meevissen et al., 2011) or future anticipation (Hallford, Sharma, et al., 2020), and positive imagery plays a key role in other interventions aiming to target positive affect and anhedonia (e.g., Craske et al., 2023); this seems an important and fruitful avenue to follow up. Further dissecting which aspects of positive imagery leads to changes in which measures may help further specify the underlying theory.
The results of the study need to be interpreted in light of a number of limitations. While study 1 used a wide variety of measures and has the advantage of measuring these in the lab, it had a relatively small sample size for regressions and was restricted to a relatively healthy sample. The ability to analyse the data from study 2 reduces this latter limitation to some extent, but the measures used were not identical and the sample in study 2 was smaller still. It would also be helpful in future to use measures that were not restricted to lab-based or self-report measures as used in the current study, for example via measuring positive affect, anhedonia, and imagery in daily life via ecological momentary assessment (e.g., Heininga et al., 2017; Slofstra et al., 2018). These measures could also be complemented by psychophysiological measures of affective responding. While study 1 was pre-registered, the analysis plan was not highly specified. Further, as there were 12 measures completed in the same fixed order for all participants, this may have influenced the precise pattern of results found (e.g., via increased noise in later-completed measures due to fatigue). Finally, including measures that allow greater differentiation between different aspects of imagery would help disentangle some of the suggested relationships further. These could include measures of different aspects of positive future imagery itself (e.g., both quality, such as vividness, and quantity, i.e., tendency to experience positive imagery in various situations; see e.g., Ji et al., 2025), as well as measures of neutral imagery and the different components of imagery generation and maintenance (see e.g., Di Simplicio et al., 2016), which in some studies have shown associations with psychopathology (e.g., social anxiety; Guarnera et al., 2019; Morrison et al., 2011).
The research presented here indicates a strong and relatively specific relationship between the ability to vividly imagery positive events in one’s future and the experience of positive affect in daily life in both a relatively healthy student sample and an older sample receiving inpatient treatment for mental health problems; relationships between positive imagery vividness and anhedonia were also present but weaker and less specific. These results can inform further research to understand the role of mental imagery in healthy functioning and how it can be harnessed in interventions to increase wellbeing.
Supplemental Material
Supplemental Material - The Relationship Between Vividness of Positive Future-Oriented Mental Imagery, Anhedonia, and Positive Affect
Supplemental Material for The Relationship Between Vividness of Positive Future-Oriented Mental Imagery, Anhedonia, and Positive Affect by Simon E. Blackwell, Katharina Westermann, Jürgen Margraf, and Marcella L. Woud in Psychological Reports
Footnotes
Acknowledgments
We would like to thank Tamara Klaus-Karwisch, Marina Salehin, Sofia Karamavrou, and Julia Grönwald for their help with participant recruitment and testing for Study 1, and Ina Külpmann for her help with participant recruitment and testing for Study 2.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Note
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.