
Abstract
Perceived social support has been posited as an important factor in non-suicidal self-injury (NSSI) cessation. Although, previous research suggests that social connectedness is the mechanism through which perceived social support influences psychological wellbeing. Thus, the present study investigated whether social connectedness is the mechanism through which perceived social support functions to influence NSSI engagement. Fifty-six women with (M age = 20.18, SD = 2.07) and 84 without (M age = 20.24, SD = 1.98) a history of NSSI completed online measures of perceived social support and social connectedness. A mediation model was conducted with social connectedness in the relation between perceived social support from family, friends, and significant others and NSSI engagement. Findings revealed that social connectedness fully explained the relation between perceived social support from all sources and NSSI engagement. The results suggest that the relation between perceived social support and NSSI engagement is fully explained by the degree to which individuals report feeling connected to others. Implications for future research and practice will be discussed.
Introduction
Non-suicidal self-injury (NSSI) is defined as the deliberate destruction of one’s own bodily tissue, without a conscious suicidal intent and for purposes that are not socially sanctioned; therefore, excluding tattooing and piercing (American Psychiatric Association, 2022; International Society for the Study of Self-injury [ISSS], 2007). Emerging adults (i.e., typically 18–29 years of age) commonly report cutting, carving, burning, biting, scraping, picking and scratching of the skin, and self-hitting as methods of NSSI engagement (Anestis et al., 2015). After adolescence, emerging adulthood is the second most frequently reported age at onset of NSSI (Klonsky & Muehlenkamp, 2007). Notably, this developmental stage is associated with transition periods marked by heightened stress (Taliaferro & Muehlenkamp, 2015). For instance, the transition to university (and college) is a highly stressful period that puts emerging adults at an increased risk of engaging in NSSI. The lifetime prevalence rate of NSSI among university students is as high as 27–32% (Hamza & Willoughby, 2016; Muehlenkamp et al., 2018). Importantly, research has found that emerging adults who report persistent engagement in NSSI across their university studies are at increased psychosocial risk (Hamza & Willoughby, 2014). NSSI behaviours have also been found to be predictive of future suicide ideation and attempts (Hamza & Willoughby, 2016), whereby a higher frequency of NSSI engagement predicts a higher risk for suicide over time (Willoughby et al., 2015). Thus, NSSI is a significant risk factor for, and correlate of suicidal behaviours (Kiekens et al., 2018; Klonsky et al., 2013; Whitlock et al., 2013).
Given that elevated rates of NSSI engagement among emerging adults have become a concern for the abovementioned reasons, it is imperative that research continue to investigate this behaviour for the purposes of informing interventions to support this population of young adults. Accordingly, research has been exploring the functions of NSSI (i.e., reasons why individuals engage in NSSI). Empirical research has found that NSSI functions can be categorized as serving intrapersonal (e.g., emotion regulation) or social purposes (e.g., communicating one’s distress; Klonsky et al., 2015; Nock & Prinstein, 2004). Research has consistently documented the intrapersonal functions more commonly, as emotion regulation is the most endorsed reason for engaging in NSSI (Taylor et al., 2018). In fact, a meta-analysis found that 66–81% of individuals reported engaging in NSSI for intrapersonal reasons, and that 33–56% of individuals reported social reasons (Taylor et al., 2018). Thus, it appears that although intrapersonal reasons are most commonly reported, a significant percentage of emerging adults report social reasons for engaging in NSSI. Therefore, there is a need to better understand the social functions of NSSI, given that they are posited as an important factor in the onset and cessation of NSSI (e.g., Tatnell et al., 2014).
A social factor that has demonstrated a clear association with NSSI engagement is perceived social support (Muehlenkamp et al., 2013), and is operationalized as one’s subjective rating of adequate social support from different sources (Zimet et al., 1988). Although, it is unclear whether a particular supportive source (e.g., family, friends, significant others) has greater relative importance in NSSI engagement, as previous studies have demonstrated varying results. For example, an early study found that perceived social support from peers and not from family members was lower among emerging adults with a history of NSSI compared to individuals with no such history (Heath et al., 2009). These findings suggested the importance of perceived social support from peers for individuals who engage in NSSI. Alternatively, Trepal et al. (2015) found that emerging adults currently engaging in NSSI perceived their social support from family and friends no differently than individuals with a past history of NSSI but perceived their social support from significant others to be significantly lower. In addition, individuals who reported currently engaging in NSSI perceived their social support from all three sources lower than those who never engaged in NSSI (Trepal et al., 2015). Previous research has also suggested that the family context may be particularly important for individuals who engage in NSSI. For example, Trujillo and Servaty-Seib (2018) found that university students who reported experiencing parental absence were more likely to report NSSI engagement compared to their peers who had not experienced parental absence. Perceived social support has also been found to be a mediator in the relation between childhood maltreatment and NSSI engagement, such that Danish adults who experienced childhood maltreatment but had higher perceived social support were at a lower risk of NSSI engagement (Christoffersen et al., 2015). Similar results were also found among Chinese middle school students whereby increased perceived social support moderated the relation between experiencing negative life events and NSSI engagement, by decreasing the likelihood of NSSI engagement (Xin et al., 2020). Overall, the literature emphasizes that cultivating supportive interpersonal relationships is associated with a lower likelihood of NSSI engagement (Trepal et al., 2015).
Beyond investigating the degree of perceived social support, it has been theorized that the development of an enduring sense of connectedness is an important component for individuals’ positive perception of their interpersonal relationships (Lee et al., 2001). Social connectedness has been defined as one’s beliefs and attitudes about the strength of their relationships with different members of their social environment, such as with family, friends, strangers and society (Lee & Robbins, 1998). Whereas social support may refer to one’s perceived adequacy of support from various sources, social connectedness is believed to represent one’s persistent ability to connect with others (Lee & Robbins, 1995). Thus, an individual can perceive having high available support but still report a low sense of connectedness, whereby they feel alone despite acknowledging having people in their life that would like to support them.
Moreover, social connectedness has been hypothesized as the mechanism through which interpersonal events and relationships are understood and processed (Williams & Galliher, 2006). Early research has demonstrated that social connectedness mediates the relation between perceived social support and psychological health for emerging adults (Williams & Galliher, 2006). Williams and Galliher (2006) posit that these findings support the idea that social connectedness is a central conduit through which interpersonal interactions and relationships are associated with psychological well-being. In particular, social connectedness has been found to be lower among university students with a history of NSSI (Macrynikola et al., 2018; Rotolone & Martin, 2012) compared to those with no such history). Additionally, Whitlock et al. (2015) found that quantitatively, higher reports of perceived social support were associated with NSSI cessation; although, building positive social connections with others was found to be the most important contributor to NSSI cessation, as qualitatively reported by participants. Whitlock et al. (2015) suggest that the mere presence of supportive sources is not what drives NSSI cessation, but rather, it is one’s ability to feel connected with others that is important. However, perceived social support and social connectedness were not examined together quantitatively, to understand how they influence each other.
In summary, the reviewed literature suggests that social connectedness may in part explain the relation between perceived social support and various psychological outcomes, such as engagement in NSSI; however, no studies have tested perceived social support and connectedness in the same model to further understand NSSI engagement. It may be that one’s degree of social connectedness is the mechanism through which perceived social support influences the likelihood of NSSI engagement. Thus, the objectives of the present study were to (1) examine differences in perceived social support from various sources (i.e., family, friends, significant others) and social connectedness between the groups (NSSI/no-NSSI); and (2) evaluate whether social connectedness mediates the relation between perceived social support from the various sources and NSSI. The corresponding hypotheses are as follows. It was hypothesized that the NSSI group would report significantly lower levels of perceived social support from family
Methods
Participants and Procedures
The university’s research ethics board approved all the procedures of the study prior to any data collection (IRB # 325-0118). Participants were either recruited by email from an existing database of students that previously completed a general screener questionnaire on stress and coping and expressed a desire to be contacted for research study opportunities or through social media postings and flyers around the university campus. Individuals with a history of NSSI were actively recruited through study advertising and a pre-existing database of individuals with a history of NSSI to obtain a substantial number of individuals within this group. Due to an overrepresentation of women, and an inability to recruit a comparable subsample of individuals self-identifying as men (n = 23 total men; n = 8 with a history of NSSI), and non-binary (n = 0), subsequent analyses only included women. The final sample consisted of 140 self-identified women undergraduate students (M age = 20.21, SD = 2.01), recruited from a large urban English-language university in Quebec. The final sample consisted of a group of individuals with a lifetime history of NSSI (n = 56; M age = 20.18, SD = 2.07) and a comparison group of individuals with no history of NSSI (n = 84; M age = 20.24, SD = 1.98).
Upon agreeing to participate, participants were sent a link to the consent form and a battery of online confidential questionnaires. The NSSI group was comprised of participants who reported a history of NSSI on an NSSI screener and met criteria for NSSI based on their self-reported methods of engagement as measured by the Inventory of Statements about Self-Injury (ISAS; described in the Measures section below). An exclusion criteria was applied to NSSI group membership whereby participants that reported on the ISAS solely engaging in hair pulling, pinching, interfering with wound healing (scab picking), or the combination of any of these behaviours exclusively were excluded from further analyses (n = 2), as they do not meet the definition of NSSI put forth by ISSS (2007), as described. Inclusion of these behaviours in previous studies has indicated a higher than expected prevalence rate of NSSI, as these behaviours tend to also be common in the general population (Nock, 2010). Following completion of the online survey, all participants received debriefing information along with community and campus mental health resources and crisis intervention services.
Preliminary Descriptives
Approximately half the sample identified as White (n = 75; 53.57%), 29.29% identified as Asian (n = 41), 7.14% identified as Mixed (n = 10), 2.86% identified as Black (n = 4), 2.14% identified as Latin American/Hispanic (n = 3), 2.14% identified as Middle Eastern, and 0.71% identified as First Nations (n = 1). The majority of participants in the NSSI group (n = 36; 64.71%) reported their first incidence of NSSI occurring before the age of 15 years. Cutting was the most commonly reported method of engagement in NSSI, with forty-five individuals (66.18%) reporting having engaged in cutting, followed by 60.29% reporting scratching, 52.94% reporting self-hitting, 33.82% reporting self-biting, 20.59% reporting burning, 19.12% reporting rubbing skin on rough surfaces, and 11.76% reporting carving and sticking self with needles. The majority of the sample (n = 43; 77.94%) reported engaging in multiple methods of NSSI. Moreover, the mean lifetime frequency of engagement in NSSI was 180.80 (SD = 330.95), and the median was 55. Upon closer examination, 46.43% (n = 26) of participants reported engaging in NSSI 2-50 times in their lifetime, followed by 17.20% (n = 10) reporting 51-100 times, 28.57% (n = 13) reporting 101-500 times, and 12.5% (n = 7) reporting more than 500 times. This heterogeneity in the range of engagement in NSSI is comparable to that observed in previous research (e.g., Saraff & Pepper, 2014).
Measures
Non-Suicidal Self-Injury Screener
Participants responded to “Have you ever engaged in self-injury without wanting to die (e.g., self-cutting, self-hitting, burning, bruising, scratching, etc.)” with either Yes or No.
Non-Suicidal Self-Injury Characteristics
Section 1 of the ISAS (Klonsky & Glenn, 2009) was used as a secondary confirmation of the screener question and to provide a lifetime frequency of 12 different methods of NSSI performed intentionally and without suicidal intent.
Perceived Social Support
The Multidimensional Scale of Perceived Social Support
Social Connectedness
The Social Connectedness Scale Revised (SCS-R; Lee et al., 2001) is a 20-item self-report questionnaire that was used to assess emotional distance of the self from others, for both friends and society (Lee & Robbins, 1995), along with maintaining a sense of closeness (Lee & Robbins, 2000). Items such as “I feel like an outsider” and “I feel disconnected from the world around me” are rated on a 6-point scale ranging from strongly disagree (1) to strongly agree (6). This measure has demonstrated excellent internal reliability (Cronbach’s α = .92) within previous research (Lee et al., 2001). This was also found within the present sample (Cronbach’s α = .95).
Results
Data analytic plan
First, a multivariate analysis of variance (MANOVA) was conducted to examine group differences in perceived social support from family, friends, and significant others. Second, an analysis of variance (ANOVA) was conducted to examine group differences in social connectedness. Effect sizes were interpreted using the generally accepted criteria put forth by Cohen (1988). Third, three separate mediation analyses were conducted by using PROCESS for SPSS (IBM, version 25) and following the recommendations of Hayes (2013). This method of conducting mediation analyses employs 95% bootstrap confidence intervals to determine the significance of the indirect effects of the mediation analyses (Hayes, 2018). This method is encouraged when using small sample sizes, as it estimates the direct and indirect effects of a mediator through data resampling (MacKinnon et al., 2004).
Data cleaning
Results from a Missing Values Analysis determined that less than 5% of the data were missing values; therefore, the data were assumed to be missing completely at random (MCAR) and participants with missing values were removed prior to conducting any analyses (n = 8). Two univariate outliers (+/− 3 SDs) were identified in both the NSSI group and the no-NSSI group, which were then winsorised following the recommendations of Tabachnick and Fidell (2001). Furthermore, no violations of normality were identified.
Group comparisons: Perceived social support and connectedness
To examine hypotheses
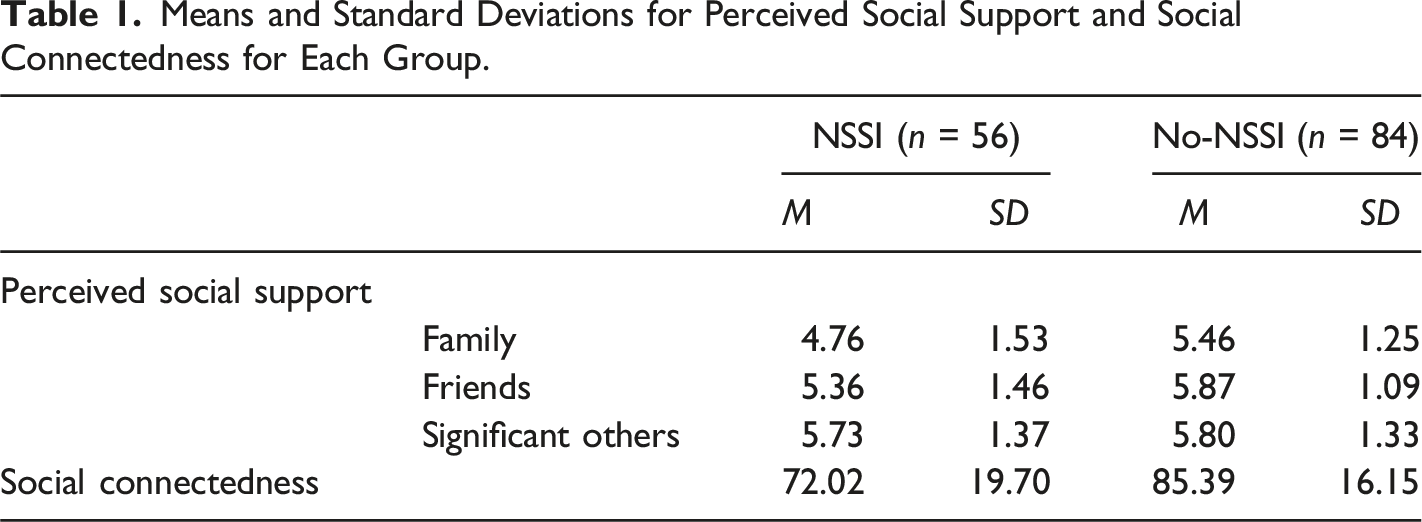
Means and Standard Deviations for Perceived Social Support and Social Connectedness for Each Group.
Mediation analyses
To examine hypotheses (a, b, c). Models depicting the association of perceived social support from (a) family, (b) friends, (c) significant others, NSSI status and the mediating role of social connectedness. * = p < .001.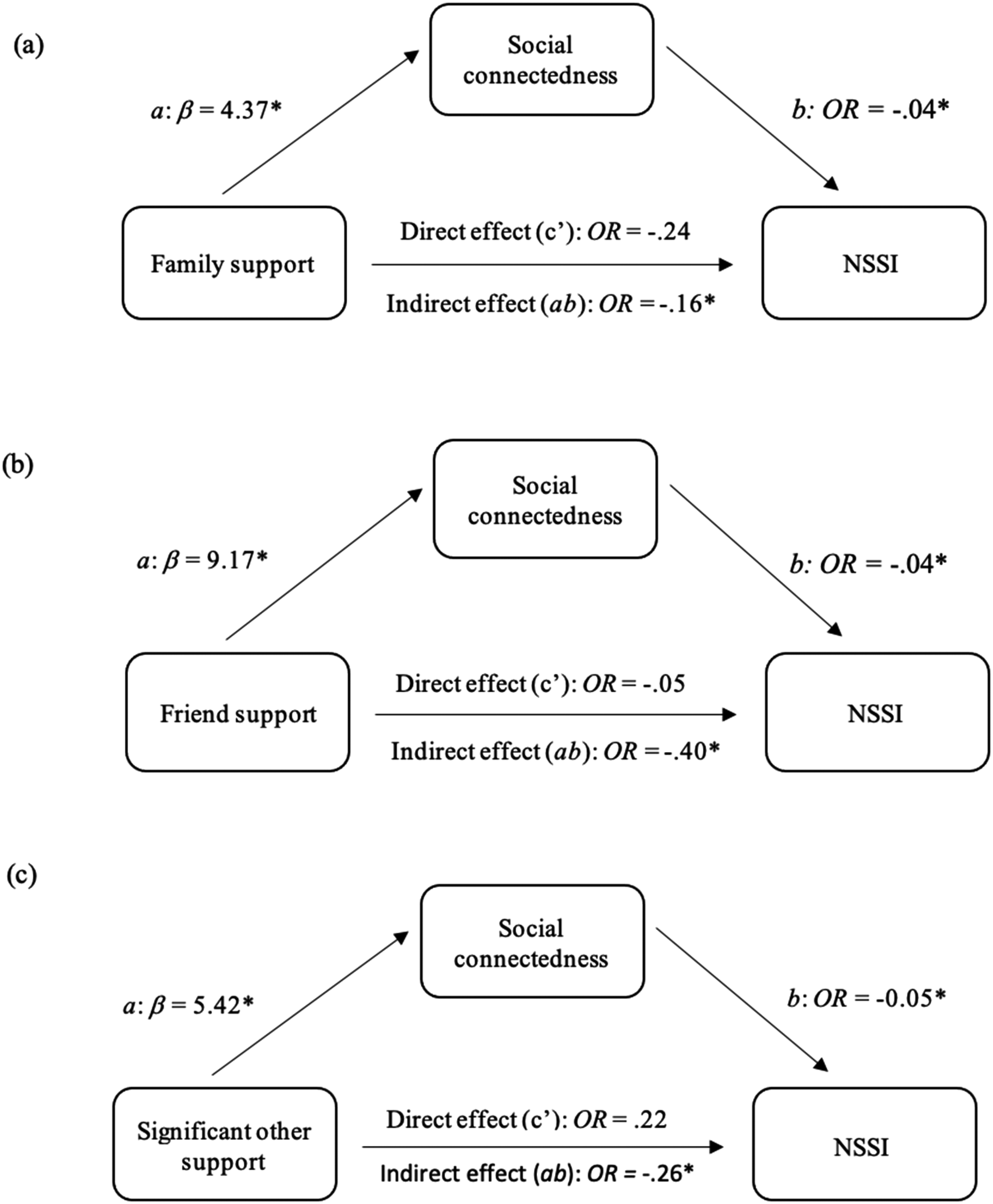
Next, as demonstrated in Figure 1(b), the results suggest that perceived social support from friends was associated with higher social connectedness (path a: b = 9.17, p < .001, 95% CI [7.23, 11.12]). Reports of lower social connectedness were associated with an increased likelihood of NSSI group membership (path b: OR = −.04, p < .001, 95% CI [−.07, −.02]). When controlling for social connectedness, the direct effect of perceived social support from friends on NSSI group membership (path c’: OR = −.05, p = .765, 95% CI [−.30, .41]), was non-significant. An analysis of the mediating role of social connectedness within this model revealed a negative indirect effect (OR = −.40, Boot CI [−.71, −.16]), suggesting a full mediation, and supporting the hypothesis
Lastly, as demonstrated in Figure 1(c), the results suggest that perceived social support from significant others was associated with higher social connectedness (path a: b = 5.42, p < .001, 95% CI [3.25, 7.59]). Reports of lower social connectedness were associated with an increased likelihood of NSSI group membership (path b: OR = −.05, p < .001, 95% CI [−.071, −.03]). When controlling for social connectedness, the direct effect of perceived social support from significant others on NSSI group membership (path c’: OR = .22, p = .149, 95% CI [−.08, .52]), was non-significant. An analysis of the mediating role of social connectedness within this model revealed a negative indirect effect (OR = −.26, Boot CI [−.47, −.12]), suggesting a full mediation, and supporting the hypothesis
Discussion
The present study investigated perceived social support and connectedness as they relate to engagement in NSSI among university students who self-identified as women. Results revealed that women with a history of NSSI perceived their social support to be lower than the comparison group. Interestingly, this study is the first to demonstrate that the relation between women’s perceived social support and NSSI engagement is explained by their reported level of social connectedness. Upon closer examination, the findings indicated that the differences in perceived social support between the groups were due to the NSSI group reporting significantly lower perceived social support from family. The salient finding regarding perceived family support further supports the current knowledge base (e.g., Rotolone & Martin, 2012) that perceived family support appears to be particularly important among young adults who engage in NSSI, beyond other sources of support. This supports the unique importance of the family context for individuals who engage in NSSI that has been found within previous research. e.g., among adolescents, lower family psychological functioning (i.e., communication, conflict resolution) was associated with an increased likelihood of future engagement in NSSI (e.g., Nemati et al., 2020). Similarly, among preadolescents, both low family support and high behavioural control were risk factors for engagement in NSSI (Baetens et al., 2014). While more research is needed, the current study may be further demonstrating the continued importance of the family context in emerging adulthood among individuals who engage in NSSI.
Furthermore, the lack of significant findings for perceived support from friends and significant others is surprising as previous research has document these to also be important for young people engaging in NSSI (e.g., Trepal et al., 2015; Turner et al., 2017). In particular, Kiekens et al. (2017) found that individuals who continued to engage in NSSI as emerging adults compared to those who ceased NSSI, reported less perceived support from their peers. Interestingly, perceived family support only predicted a lifetime history of NSSI and not persistent NSSI engagement among emerging adults (Kiekens et al., 2017). Given that the current study did not assess NSSI recency, the possible importance of perceived social support from friends and significant others for emerging adults who more recently engage in NSSI (or persist to engage in NSSI into this developmental period) may not have been picked up on in the current study. Therefore, perceived family support appears to be an important factor when examining lifetime engagement in NSSI, whereas peer support may emerge as a significant factor when exploring recent and/or persistent NSSI engagement, among emerging adults.
Consistent with the hypothesis, results also revealed that women with a history of NSSI reported lower levels of social connectedness than did those with no history of NSSI. These findings are in line with previous results that have demonstrated that individuals who report engaging in NSSI also report lower levels of social connectedness than those with no history (Rotolone & Martin, 2012). To more closely examine the role of social connectedness in NSSI engagement, the current study investigated whether social connectedness is a mechanism through which perceived social support from different sources influences the likelihood of NSSI engagement. In line with the hypotheses, an indirect effect of perceived social support from each of the supportive sources (i.e., family, friends, significant others) on NSSI engagement was observed through social connectedness. Importantly, this suggests that the relation between perceived social support and NSSI engagement is fully explained by the degree to which women report feeling connected to others. That is, the mere presence of perceiving adequate social support alone was not associated with a decreased likelihood of NSSI engagement. Rather, it was explained by individuals’ sense of connectedness to others that influenced the effect of perceived social support on a decreased likelihood of NSSI engagement.
The current findings support theory of social connectedness in which individuals with higher social connectedness are believed to be more able to connect with those around them, such that they perceive others more positively and are more socially active (Lee et al., 2001). Therefore, the current results may be demonstrating that one’s degree of social connectedness is the mechanism that influences individuals’ positive perception of others, such as their supportive networks, which influences the likelihood of NSSI engagement. Additionally, given that higher social connectedness may lead individuals to be more active socially, this may increase their chances of fostering adequate social support, which is associated with decreased odds of engaging in NSSI. Importantly, previous research has demonstrated how individuals may strengthen their sense of connectedness, and the potential benefits of doing so within clinical settings. For example, Whitlock et al. (2015) found that students reported that talking about their self-injury to those who expressed concern allowed them to feel a greater sense of connection and enabled NSSI cessation. Alternatively, psychological interventions that provide adults with strategies for managing maladaptive cognitions, social avoidance behaviours, and barriers to social contact have been associated with improvements in individuals’ perceived quality of social connections (Zagic et al., 2022).
Although the present study provides new insights, there are limitations that suggest these preliminary results be interpreted with caution. First, the sample size was limited, which limits the reliability of the results. Second, the final sample was constrained to women undergraduate students, with the majority identifying as White, limiting the generalizability of the findings. This is a consistent issue in NSSI research, whereby many studies lack diversity in terms of gender and ethnicity within their samples (Cipriano et al., 2017; Gholamrezaei et al., 2017). Thus, future research should strive to explore the extent to which these demographic variables influence the relation between social connectedness, perceived social support, and NSSI engagement. Third, the present sample may have been subject to sampling bias as a portion of the participants were recruited from a pre-existing database of individuals who wanted to receive research study advertisements, and are therefore more likely to participate in research. Fourth, lifetime history of NSSI, rather than more recent NSSI engagement (e.g., past year) was used in the current study to identify the groups. Therefore, there may be significant variability in the frequencies of engagement in NSSI, leading to a rather heterogenous group of individuals. This appears to be a consistent issue in research due to difficulty recruiting large enough samples to examine this variability more closely. Additionally, the timeframe used to define NSSI in the current study (i.e., lifetime history) differs from that of perceived social support and connectedness which presumably measure one’s current level within each construct. This limits the possibility of making inferences regarding the temporal nature of these constructs. Lastly, due to the cross-sectional design of the study, inferences of causality and directionality cannot be drawn. Additional research is needed to longitudinally examine the relation between perceived social support and social connectedness with a larger sample and more recent (e.g., past year) NSSI engagement.
Despite the limitations, the findings highlight the importance of understanding interpersonal functioning among individuals with lived experience of NSSI. In particular, the results suggest that strategies for fostering family support in clinical settings may be particularly beneficial for those who engage in NSSI. While more research is needed, this study also demonstrated that approaches for strengthening one’s sense of connection may bolster one’s positive perception of their social support, which is related to a lower likelihood of NSSI engagement. Taken together, this preliminary study provides important information for both clinicians and researchers on the apparent role of social connectedness and relevance of understanding the interpersonal context, for those with lived experience of NSSI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.