
Abstract
In trying to better understand why certain individuals self-injure, researchers have proposed high emotional reactivity for negative emotions may influence vulnerabilities and predispose individuals to react to stressful situations in a dysregulated manner, thus engaging in non-suicidal self-injury (NSSI). However, the role of emotional reactivity for positive emotions in those with a history of NSSI is still unclear. Thus, the present study sought to examine group differences in the reactivity of (a) negative and (b) positive emotions in young adults with and without a history of NSSI engagement, and (c) to evaluate whether the reactivity of positive emotions could predict NSSI engagement when controlling for reactivity of negative emotions. The sample consisted of 96 female students who reported engaging in NSSI within the past 2 years (Mage = 20.28 years, SD = 1.65) and an age-matched female comparison group with no NSSI history (Mage = 20.43 years, SD = 1.76). Results from separate MANOVAs indicated individuals with a history of NSSI reported higher negative reactivity across all aspects (emotional intensity, sensitivity, and persistence) than the comparison group, Wilk’s λ = .86, F (3,188) = 10.65, p < .001, partial η2 = .145; however, no significant differences emerged for positive reactivity, Wilk’s λ = .99, F (3,188) = 0.52, p = .669. Moreover, a logistic regression revealed that persistence of negative emotions was the only significant predictor of NSSI, Wald χ2 (1) = 4.54, p = .03. The present results highlight the importance of the persistence of negative emotions for individuals who engage in NSSI. Furthermore, the current study provides the first suggestion of no significant differences in positive emotional reactivity between individuals with and without NSSI; underlining the importance of focusing on negative emotional reactivity in clinical practice as well as using positive emotions to “undo” the effect of negative emotions.
Keywords
Introduction
Non-suicidal self-injury (NSSI) is defined as intentionally inflicting damage to one’s own body, without suicidal intent and for purposes not socially sanctioned (Bentley et al., 2015; International Society for the Study of Self-Injury, 2007; Swannell et al., 2014; Wolff et al., 2019). Although a majority of studies have reported that the first incidence of NSSI occurs between the ages of 12 and 16 (e.g., Andrews et al., 2014; Cipriano et al., 2017; Heath et al., 2008; Muehlenkamp et al., 2012; Ross & Heath`, 2002; Swannell et al., 2014; Tatnell et al., 2014), around a third of individuals begin engaging in self-injury in young adulthood at approximately 18–22 years of age (Hamza & Willoughby, 2014; Kiekens et al., 2019; Klonsky, 2011; Whitlock et al., 2011). In addition, lifetime prevalence rates suggest that between 12% to 35% of young adults have engaged in NSSI at least once in their lives (Brown & Plener, 2017; Gratz et al., 2002; Heath et al., 2008; Whitlock et al., 2006; Zetterqvist et al., 2013).
In trying to better understand why certain individuals engage in NSSI and others do not, researchers have proposed the presence of underlying cognitive and affective vulnerability factors that predispose individuals to engage in this behaviour (e.g., Cohen et al., 2015). For instance, Nock (2009) suggests an integrative model of NSSI combining elements from different research areas to explain the development and maintenance of NSSI. This model proposes that individuals’ risk of engaging in NSSI is increased by genetic (e.g., high emotional reactivity) and environmental factors such as childhood maltreatment and family dynamics. It is believed that beyond certain predispositions, individuals continue to engage in NSSI as it is an effective way of quickly reducing the experience of negative affect (Bresin & Gordon, 2013; Weinberg & Klonsky, 2012). Over time, an individual is more likely to believe that their emotions can only be effectively regulated using this behaviour.
In addition, the experiential avoidance model proposes that NSSI “is a negatively reinforced strategy for reducing or terminating unwanted emotional arousal” (Chapman et al., 2006, p. 372). Thus, those who engage in NSSI are more reactive to their emotions, in that they experience more intense emotions, which they are not necessarily able to effectively regulate (Chapman et al., 2006). According to this model, given a number of risk factors, including high levels of emotional reactivity, individuals may have difficulty regulating their emotions when experiencing a stressful or unpleasant event. In an effort to escape this unpleasant affective state, individuals may choose to engage in NSSI. The reduction of the unpleasant mood negatively reinforces NSSI, thereby creating a vicious cycle between unpleasant affective states and engaging in the behaviour (NSSI). Over time, this association strengthens and NSSI becomes a more frequent response to stressful events.
Emotional reactivity, defined as individual differences in the intensity and temporal nature of behavioural or physiological responses to emotional stimuli, is related to emotion regulation (Calkins, 2004; Chapman et al., 2006; Rothbart et al., 2011). It is believed that emotion reactivity refers to the emotion-response process, where individuals attend to a situation, appraise it as relevant, and experience the activation of an emotion (Evans et al., 2016; Gross & Jazaeri, 2014Gross & Jazaieri, 2014). In the NSSI literature, researchers have focused on emotional reactivity as being composed of three components, including the extent to which the individual experiences emotions in reaction to stimuli (i.e., emotional sensitivity), how strongly or intensely emotions are experienced (i.e., emotional intensity), and the period of time needed before returning to the baseline level of arousal (i.e., emotional persistence; Nock et al., 2008).
Over the past decades, there has been growing evidence to support differences in negative emotional reactivity between individuals who have a history of engaging in NSSI and those who do not. Specifically, individuals with a history of NSSI engagement have been found to be more likely to report greater overall negative emotional reactivity, which include the three facets of sensitivity, intensity, and persistence (e.g., Jenkins & Schmitz, 2012; Nock et al., 2008; Smith et al., 2017). Additionally, other studies have investigated individual facets of negative emotional reactivity and found similar patterns. For example, individuals with a history of NSSI report more negative emotions (i.e., sensitivity; e.g., Baetens et al., 2011; Jenkins & Schmitz, 2012) as well as greater negative emotional intensity (e.g., Anderson & Crowther, 2012; Gratz, 2006; Turner et al., 2012) compared to those who had never engaged in NSSI.
However, to date, most of the research in the field of NSSI has investigated the reactivity of negative emotions and there is a paucity of research on the reactivity of positive emotions and its relationship with NSSI engagement. Positive psychology research has increased awareness of how enhancing positive emotions can be greatly beneficial to coping capacity and well-being (e.g., Pressman et al., 2019). Specifically, the broaden-and-build theory suggests that positive emotions can be conceptualised as being more than the “opposites” of negative emotions by playing an important protective role distinct from that of negative emotions serving to foster resilience (Fredrickson, 2001; Fredrickson & Joiner, 2002, 2018; Waters et al., 2022). It also suggests that positive emotions can contribute to an upward spiral of lifestyle changes whereby positive emotions help contribute to sustained well-being and engagement in wellness behaviours (e.g., Fredrickson, 2013). Thus, for individuals who engage in NSSI, it is possible that difficulties with positive emotional reactivity may be contributing not only to NSSI engagement and therefore warrants further investigation.
However, the majority of research examining positive emotions as it relates to NSSI has been limited to the potential role of positive emotions prior, during, or immediately following the behaviour of NSSI. A recent systematic review by Brown and colleagues (2022) investigated the relationship between the experience of negative and positive emotions and NSSI engagement or thoughts more broadly. A general trend was found whereby negative affect was positively associated with NSSI thoughts while also being higher prior to NSSI engagement and decreasing following NSSI engagement. Yet, findings were much less consistent for positive affect. Positive affect was either inversely or not associated with NSSI thoughts. Meanwhile, other studies examining changes in positive emotions immediately before and following NSSI engagement revealed either a decrease in positive emotions prior to NSSI episodes followed by an increase in positive emotions, an increase in positive emotions prior to NSSI engagement followed by a continued increase, or no relationship. Unfortunately, only five studies in this systematic review examined positive affect so the authors conclude that it may be too early to form definitive conclusions (Brown et al., 2022).
Beyond investigating the experience of emotions immediately prior to, during, or following episodes of NSSI, the direct investigation of positive emotion reactivity (sensitivity, intensity, persistence) remains relatively unexamined and presents mixed findings. In particular, previous research has shown that individuals who engage in NSSI report a lower general tendency to experience positive emotions (e.g., Burke et al., 2018; Hankin & Abela, 2011). Similarly, young adults with a history of NSSI also experienced dampened affective and physiological reactions to positive stimuli compared to those without such a history (e.g., Tatnell et al., 2018). Thus, these studies provide preliminary support for the contention that individuals who engage in NSSI may experience a lower sensitivity for positive emotions relative to those without a history of NSSI. Additionally, the intensity facet of positive emotional reactivity has been found to predict NSSI status, with lower intensity of positive emotions predicting greater risk of NSSI engagement (e.g., Gratz, 2006).
Furthermore, two studies have comprehensively investigated the three facets of both negative and positive emotional reactivity in those with and without a history of NSSI using a positive and negative mood induction. Mettler and colleagues (2021) found that at baseline, those with current NSSI self-reported more difficulties with negative emotional reactivity in comparison to their non-NSSI peers, whereas there were no differences between the groups on the positive emotion reactivity measure. Surprisingly, immediately following this self-report, in response to either the negative or positive mood inductions, no differences were found between the groups in moment-to-moment negative and positive emotion reporting.
In a similar study by Boyes and colleagues (2020), participants with a lifetime history of NSSI engagement self-reported significantly greater negative emotional reactivity and lower self-reported positive emotional reactivity than their non-NSSI peers. Then, during the negative mood induction, when compared to the non-NSSI group, participants who self-injured reported greater sadness at baseline, no differences immediately following the induction, and longer perseverance of sadness over time. However, in the positive mood induction, participants with NSSI consistently reported experiencing lower base levels of amusement across all time points relative to their non-NSSI peers but both groups had a similar pattern of change of positive emotional reactivity. Overall, the mixed findings around the association between positive emotional reactivity and NSSI engagement highlight the fact that more research is needed in this area to better understand how individuals’ dispositional experience of, and response to, negative and positive emotions are associated with NSSI engagement.
Furthermore, it may be important to also consider the influence of gender identity on these relationships. Thus far, there is mixed evidence with respect to gender differences in the reactivity of negative emotions in those who have a history of engaging in NSSI. A study by Baetens et al. (2011) found that female participants reported significantly higher negative affectivity than male participants, who in turn reported significantly higher positive reactivity (Baetens et al., 2011). Another study found that female participants reported significantly higher negative emotional reactivity scores than male participants, and that negative emotional reactivity mediated the relationship between depression and NSSI status for women but not for men (Kleiman et al., 2014). In contrast, Nock et al., (2008) did not find any gender differences in negative emotional reactivity in individuals who reported a history of engaging in NSSI. Clearly further exploration of possible gender differences in negative and positive emotional reactivity is warranted.
Current Study
Overall, the present study aims to investigate the relation between emotional reactivity of negative and positive emotions and individuals’ engagement in NSSI, while taking into account potential gender differences. The objectives of the current study were to examine group differences in the reactivity of (1) negative emotions and (2) positive emotions in university students who report engaging in NSSI in the past 2 years (NSSI group) and a comparison group of students who had not self-injured, and (3) to evaluate whether the reactivity facets of positive emotions (sensitivity, lower intensity, and lower persistence) could predict NSSI engagement when controlling for reactivity facets of negative emotions and gender. Specifically, hypotheses associated with these objectives are as follows. It is hypothesized that university students who engaged in NSSI in the past 2 years would report greater levels across the three components of negative emotional reactivity; sensitivity, intensity and time needed to recover (persistence) from their negative emotions than individuals who have never engaged in NSSI (H1). Secondly, it was hypothesized that students with a history of engaging in NSSI would report lower levels of positive emotional reactivity (sensitivity, lower intensity, and lower persistence) when faced with positive emotions relative to individuals without a history of NSSI (H2). Thirdly, it was hypothesized that lower levels of reactivity to positive emotions would significantly and independently statistically predict history of NSSI engagement when controlling for high levels of negative emotional reactivity (H3).
Method
Participants
Participants were students (N = 220) recruited from a large urban area Canadian university. Following Research Ethics Board (REB) approval, participants were recruited in two ways. First, a research team database was used to contact individuals who had agreed to be contacted about participation in studies of stress and coping and who had also completed an early screening pertaining to their NSSI engagement. Participants were also recruited from an advertisement posted on the university’s online classifieds and social media pages.
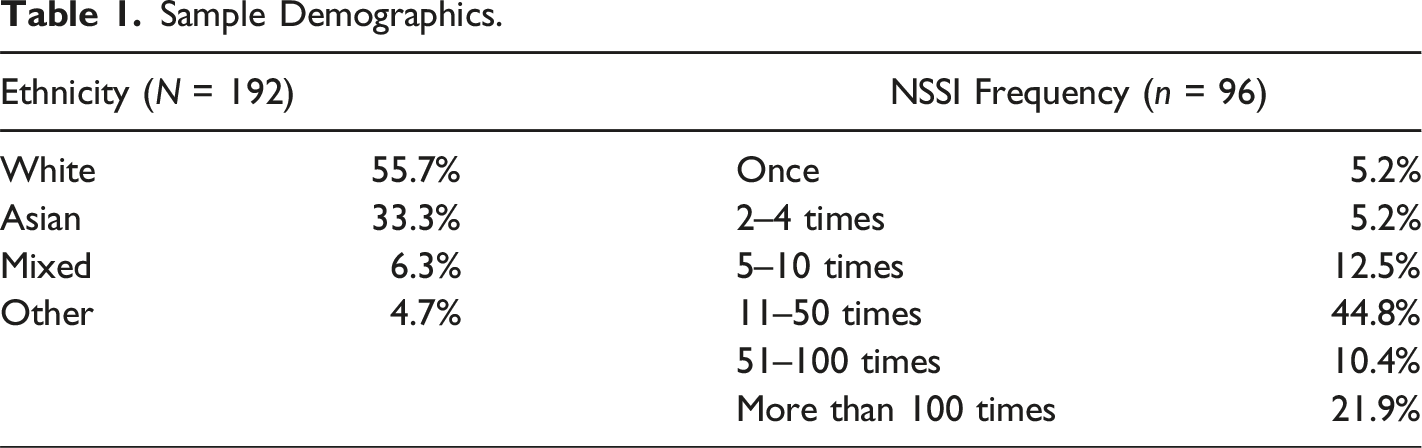
Sample Demographics.
Measures
NSSI Screening Questionnaire
A self-report researcher-designed questionnaire (Stress and Coping Questionnaire) was administered to assess stress and coping in a university sample as well as to provide preliminary screening information for self-injury. Each statement on the questionnaire assesses the use of both healthy (e.g., meditation, talking to a friend) and unhealthy coping (e.g., excessive alcohol intake, NSSI) behaviours in an individual’s lifetime and in the past 12 months. In addition, the questionnaire identifies whether individuals have used the healthy and unhealthy behaviours to cope with stress. NSSI is included as one of the listed behaviours (“physically hurt myself on purpose without wanting to die”). This item was used to provide preliminary information to identify individuals who may be currently engaging in self-injury as well as anyone who may have engaged in such behaviour in the past from the larger sample. If individuals indicated yes, they were asked more detailed questions about their self-injury.
Non-Suicidal self-Injury
The Inventory of Statements about Self-Injury (ISAS; Klonsky & Glenn, 2009) is a self-report measure that assesses various aspects of non-suicidal self-injury (NSSI). The ISAS is broken up into two sections related to the frequency and the functions of NSSI. For the purpose of this study, only information relating to the frequency of NSSI was used. The ISAS has demonstrated excellent internal consistency (Cronbach’s α = .84), concurrent validity, and adequate test-retest reliability (Glenn & Klonsky, 2011; Klonsky & Glenn, 2009) for the reporting of NSSI frequency. This measure was only administered to individuals who indicated on the Stress and Coping Questionnaire that they had ever engaged in NSSI in order to specifically identify individuals who had engaged in NSSI over the past 2 years.
Emotional Reactivity
All participants completed the Emotion Reactivity Scale (ERS; Nock et al., 2008), a 21-item questionnaire developed to assess how individuals experience emotions. In particular, the ERS assesses three areas of the experience of emotions, including: (a) sensitivity (e.g., “even the littlest things make me emotional”), (b) intensity (e.g., “when I experience emotions, I feel them very strongly/intensely”), and (c) persistency (e.g., “when something happens that upsets me, it’s all I can think about it for a long time”). Validation of this measure has demonstrated good internal consistency (Cronbach’s α = .94) and adequate construct validity when compared to other measures (Nock et al., 2008). The ERS is a commonplace scale used in studies measuring emotional intensity in individuals who engage in NSSI. For the purpose of this study, questions that are the positive emotion equivalents for each item were added to the scale (e.g., “when something happens that makes me happy, it’s all I can think about it for a long time.”). In the present study, the internal consistency of the ERS was also good both for negative emotional reactivity (Cronbach’s α: overall = .95; sensitivity = .89; intensity = .89; persistence = .80) and for positive emotional reactivity (Cronbach’s α: overall = .93; sensitivity = .87; intensity = .84; persistence = .77).
Procedure
The study was advertised as a study investigating the emotion regulation of negative and positive emotions. Participants were sent an email invitation briefly describing the study and they were given a link to the online study hosted on LimeSurvey as well as a participant ID. Upon accessing this link, participants viewed an informed consent page at the beginning of the online survey, which stated that all information collected would remain confidential. The participants were also informed that they were free to withdraw from the study at any time without penalty.
The online survey consisted of the battery of questionnaires described in the methods section above. Participants started by completing the Stress and Coping Questionnaire. Individuals who indicated that they had engaged in NSSI in their lifetime were given the ISAS to complete. Those who indicated that the last time they had engaged in NSSI was in the last 2 years (dated from the day they filled out the survey), were included in the sample. All participants were given the ERS to complete. Following completion of the survey, each participant was sent an email which included the necessary debriefing information and received $10 as well a list of resources should they require additional support. The data was then coded and entered into a database, and no identifiable information was available through database access alone.
Results
Prior to running the main analyses and based on best practice guidelines (e.g., Tabachnick & Fidell, 2007), the data were cleaned separately within two groups based on whether participants reported having a history of NSSI engagement over the past 2 years or never having engaged in NSSI (as determined first on the screener and confirmed with the ISAS, as indicated in Procedure above); however, identical data cleaning procedures were used within both groups. Results from a Missing Values Analysis demonstrated less than 5% of missing values; therefore, the data were assumed to be missing completely at random and missing values were imputed using the Expectation Maximisation procedure. Two univariate outliers were identified within the “No NSSI” group and subsequently removed. No multivariate outliers were found. Thus, the final sample consisted of 96 female participants with a history of NSSI engagement over the past 2 years (Mage = 20.28 years; SD = 1.65) along with an age-matched control group of 96 female participants (Mage = 20.43 years; SD = 1.76).
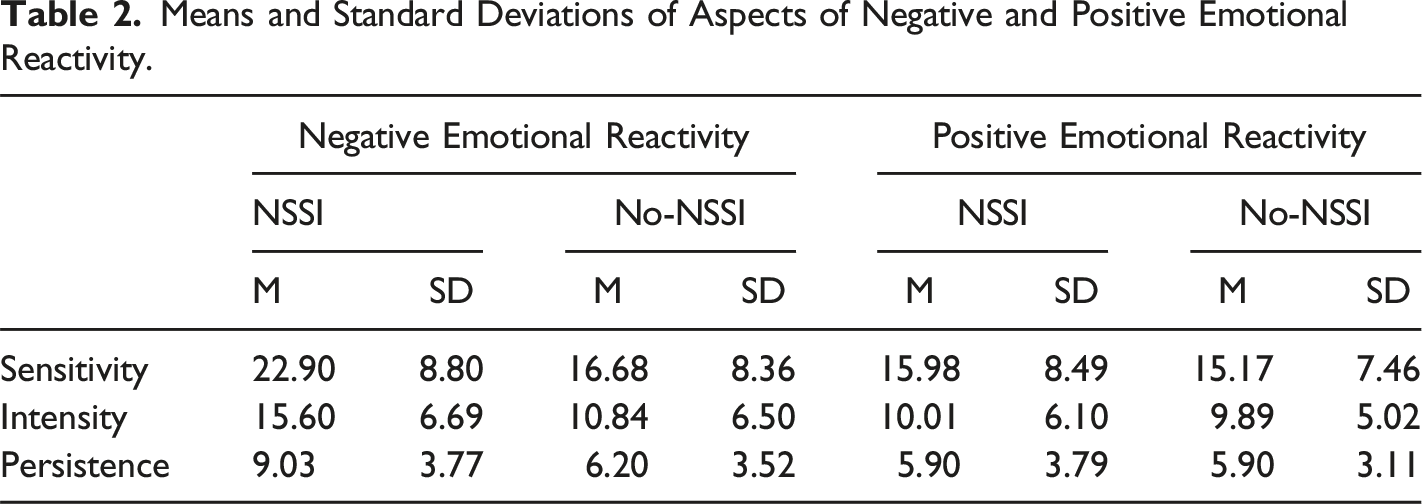
Means and Standard Deviations of Aspects of Negative and Positive Emotional Reactivity.
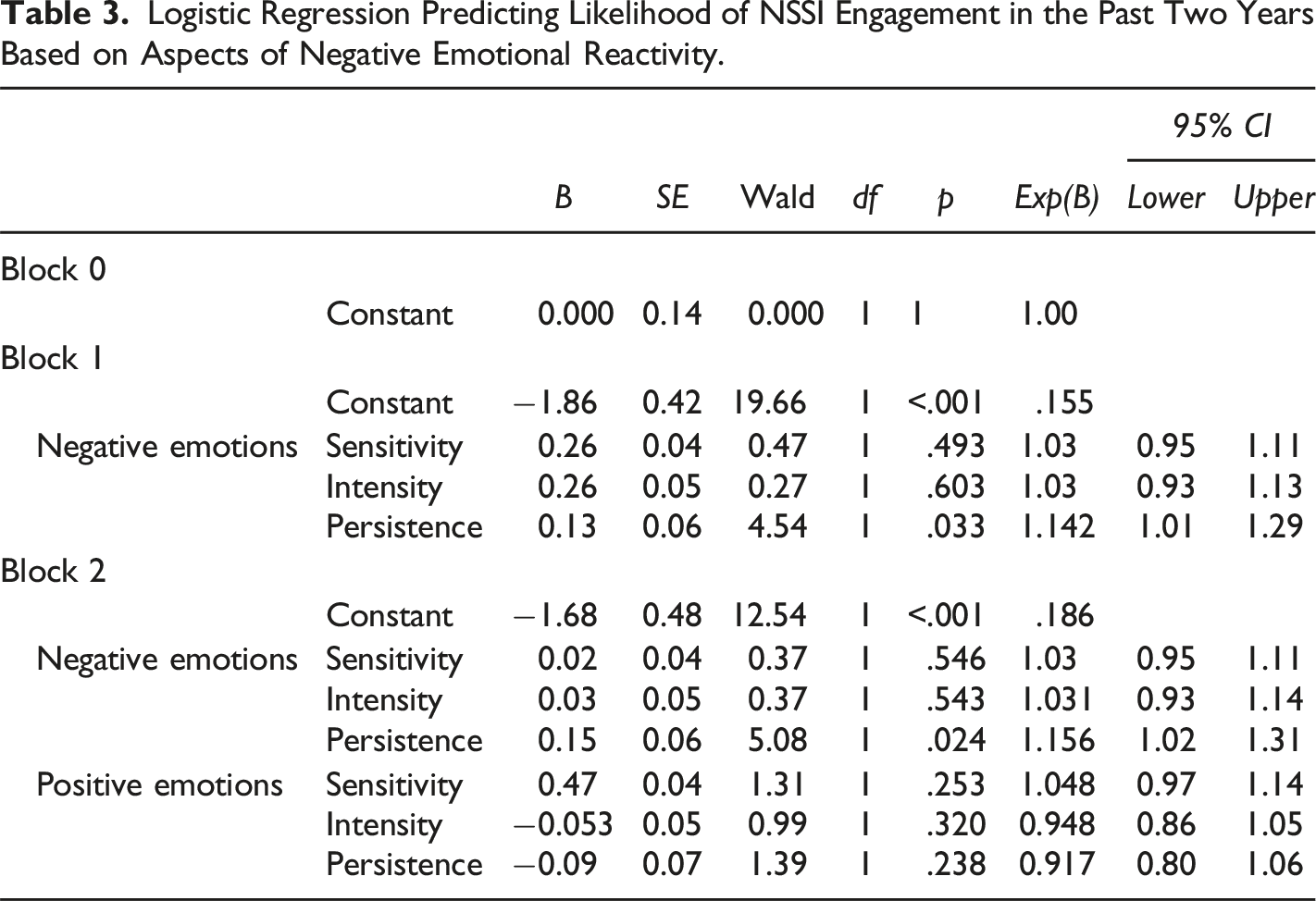
Logistic Regression Predicting Likelihood of NSSI Engagement in the Past Two Years Based on Aspects of Negative Emotional Reactivity.
The second objective was to investigate group differences in the reactivity of positive emotions in young adults with a history of NSSI engagement in the past 2 years as compared to those who have never engaged in NSSI. It was hypothesised that individuals with a history of NSSI engagement in the past 2 years would report lower sensitivity, intensity, and persistence of positive emotions than their no-self injury peers. A one-way MANOVA was conducted for the three aspects of positive emotional reactivity (sensitivity, intensity, and persistence). Both the assumption of equality of covariance and the assumption of homogeneity of variance were met. Contrary to H2, results revealed no significant main effects for the NSSI engagement groups, Wilk’s λ = .99, F (3,188) = 0.52, p = .669.
Finally, the third objective was to evaluate whether the reactivity of positive emotions could predict having a history of NSSI engagement when controlling for reactivity of negative emotions. It was hypothesized that lower levels of reactivity to positive emotions would increase predictability of individuals’ history of NSSI engagement even when controlling for negative emotional reactivity.
Results (see Table 3) revealed that, in Block 1, sensitivity, intensity, and persistence of negative emotions significantly explained 19.1% (Nagelkerke R2) of the variance in NSSI status as an overall model when entered together, χ2 (2) = 29.67, p < .001. Furthermore, a Hosmer-Lemeshow test revealed that the predicted probabilities matched the observed values, χ2 (8) = 5.72, p = .678, and the model successfully predicted 66.7% of cases overall. However, although the overall model was significant, of the two predictor variables, neither sensitivity, Wald χ2 (1) = .47, p = .493, nor intensity, Wald χ2 (1) = .27, p = .603, of negative emotions were statistically significant unique individual predictors of history of NSSI engagement when controlling for the other predictors. However, persistence of negative emotions was a significant predictor of NSSI status, Wald χ2 (1) = 4.54, p = .033. Female participants with higher persistence of negative emotions were 1.14 times more likely to report a history of NSSI engagement than those with lower persistence of negative emotions.
Then, in Block 2, the inclusion of positive emotion reactivity facets (sensitivity, intensity, and persistence) was not a statistically significant contribution to the model, χ2 (3) = 3.28, p = .351, Nagelkerke R2 = .21. Similarly to Model 1, a Hosmer-Lemeshow test revealed that the predicted probabilities matched the observed values, χ2 (8) = 2.91, p = .940. The model successfully predicted a total of 65.1% of all cases.
Discussion
The present study investigated the role of negative and positive emotional reactivity in female university students who engage in NSSI. Specifically, the research objectives were to examine whether female young adults who report having engaged in NSSI over the past 2 years significantly differ from those with no history of NSSI on reported levels of reactivity (sensitivity, reactivity, and persistence) of (a) negative emotions and (b) positive emotions. Furthermore, a third objective was to examine the relative contribution of both negative and positive emotional reactivity (sensitivity, reactivity, and persistence) in the prediction of NSSI engagement over the past 2 years; however, given the findings from the first two objectives, this objective was revised to investigate the relative contribution of the three aspects of negative emotional reactivity in predicting the history of NSSI engagement.
With regard to the relation between negative emotional reactivity and NSSI, it was hypothesized that engagement in NSSI would be related to higher levels of negative emotional reactivity. In support of our first hypothesis, individuals with a history of NSSI and without a history of NSSI significantly differed on all variables of interest with regards to the negative emotional reactivity. More specifically, individuals with a history of engaging in NSSI in the past 2 years reported significantly higher levels of sensitivity, intensity, and persistence (time needed to recover) when experiencing negative emotions compared to individuals who had never engaged in NSSI. These results are congruent with previous findings linking NSSI and negative emotional reactivity (e.g., Evans et al., 2016; Gratz, 2006; Jenkins & Schmitz, 2012; Kleiman et al., 2014; Najmi et al., 2007; Smith et al., 2017). These results also align with the theoretical model put forward by Chapman et al., (2006), which posits that individuals who have higher levels of emotional reactivity will be more likely to engage in NSSI to reduce their experience of negative emotions.
When looking at the role of the reactivity of positive emotions and NSSI, an area requiring further exploration, our hypothesis was not supported. It was expected that individuals with a history of NSSI would report significantly lower levels of sensitivity, intensity, and persistence related to positive emotions. However, no significant differences were reported in the reactivity of positive emotions across all facets of emotional reactivity (sensitivity, intensity, and persistence) between individuals with and without a history of engaging in NSSI.
The current results for emotional intensity are inconsistent with the results of Gratz’s (2006) study, which found that women with a history of engaging in NSSI reported lower levels of emotional intensity for positive emotions. The difference in findings between the present study and Gratz’s (2006) study may be due to differences in methodology. In particular, the measure that Gratz employed to measure emotional reactivity, the Affect Intensity Measure (AIM; Larsen & Diener, 1987), assesses the intensity of negative and positive emotions and does not include persistence or sensitivity. In addition, the participants in the NSSI group from Gratz’s (2006) study had a history of engaging in NSSI at some point in their lifetime, whereas the participants in the NSSI group who participated in the current study had to have engaged in NSSI in the past 2 years. Time could impact the way individuals react and cope with their emotions. In fact, Anderson & Crowther (2012) suggest that individuals who have stopped engaging in NSSI report having different levels of emotional acceptance and impulse control than individuals with more recent NSSI. This difference could impact the way individuals react and cope with their emotions. In sum, further research is needed to clarify the relationship between current and past engagement in NSSI and reactivity of positive emotions.
Finally, when looking at negative or positive emotion reactivity as predictors of NSSI or non-NSSI group membership, a different pattern emerges. It was hypothesized that the three aspects of negative and positive reactivity (sensitivity, intensity, and persistence) would predict NSSI engagement in the past 2 years. The results indicate that some components of reactivity of negative emotions do in fact significantly predict NSSI group membership. Specifically, it was found that the longer that one’s negative emotions last (greater persistence of negative emotions), the more likely an individual is to have a history of NSSI engagement over the past 2 years. These results are in line with the theory of the Experiential Avoidance Model of NSSI (EAM; Chapman et al., 2006), as it is likely that individuals who are experiencing long lasting negative emotions may be more prone to resorting to less healthy ways of regulating their emotions. Interestingly, sensitivity and intensity alone were not found to be predictors of NSSI, although the NSSI and no-NSSI groups were found to differ on these variables. The fact that sensitivity and intensity of negative emotions were not predictors may be due to the fact they were not sufficiently different from one another. Overall, these findings highlight that reactivity to negative emotions, particularly the persistence of negative emotions, may be one of the contributing factors explaining NSSI engagement. While caution is needed in interpreting these findings given the relatively low effect size, this study highlights that further research is needed to better understand how persistence of negative emotions may interact with other contributing factors such as persistence of rumination (e.g., Brown et al., 2022) or hopelessness (e.g. Fox et al., 2015). Nevertheless, this finding is a significant contribution to our understanding of NSSI and has potentially important clinical implications.
In addition to working on individuals’ sensitivity and intensity of negative emotions, it is equally important to target the role of emotional persistence of negative emotions when working with this population. With increased sensitivity, intensity, and persistence of negative emotions, individuals with a history of NSSI are in need of effective means for distress tolerance. The role of distress tolerance in therapy with individuals who have a history of engaging in NSSI has been highlighted in Dialectical Behavioural Therapy (DBT; Linehan, 1993). Numerous studies have demonstrated that participation in DBT has resulted in the reduction of engagement in self-harm in both community and clinical samples (James et al., 2007; Linehan et al., 1991; Verheul et al., 2003). Accordingly, this study provides further empirical support for the use of this modality of therapy with individuals, particularly women, who engage in self-harm.
Furthermore, the findings that positive emotional reactivity is similar in individuals both with and without a history of NSSI may be clinically relevant. In particular, it is possible that the experience of positive emotions can be integrated into the therapeutic setting and “undo” the effects of negative emotions as well as provide these individuals with a wider set of skills to cope with their negative emotions (Garland et al., 2010).
While the current study presents several findings that advance the understanding of emotional reactivity of negative and positive emotions in individuals with a history of engaging in NSSI, the study has several limitations that should be considered. First, although we identify the need to investigate gender differences in NSSI research, the present study is limited to female university students, thus excluding male students and young adults outside the university setting. Secondly, the results of this study were based entirely on self-report information. Future studies may want to use experimental methods to investigate the relationship between emotional reactivity of both negative and positive emotions in individuals with a history of engaging in NSSI. An additional limitation of this study is that it is cross sectional; longitudinal research would be needed to truly predict NSSI engagement over time.
Conclusion
The current findings suggest that the reactivity of positive emotions is comparable across female university students with and without a history of NSSI. However, the reactivity of negative emotions should continue to be the central focus when considering the emotional reactivity of individuals who engage in NSSI. While the role of negative emotional reactivity has already been studied at length, this study confirms these findings and provides further focus on what aspects of negative emotional reactivity may be related to NSSI, particularly the persistence of negative emotions. Thus, pending replication, the results of this study have implications for the clinical treatment of individuals who engage in NSSI, specifically with respect to their tolerance of distress, as the persistence of negative emotions may be very difficult for these individuals to endure.
Furthermore, given the similarities related to the reactivity of positive emotions, across groups, it is possible ones’ positive emotions could serve the purpose of “undoing” negative emotions as suggested by the broaden-and-build theory. However, further research is needed on positive emotional reactivity to better understand its role in contributing to or impacting NSSI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.