
Abstract
The study examined whether caregiver worry of COVID-19 infection and co-existence difficulty differentially predicted child mental health and wellbeing during the lockdown in two culturally different countries that were severely affected by the pandemic: the UK and Turkey. Co-existence difficulty is the hardship experienced by family members living all together in the same house at the same time during the lockdown period. Participants were 1849 caregivers of children between 5- and 12-years old living in the UK (n = 995) and Turkey (n = 854), who completed an electronic survey distributed via social networks during the initial phase of the COVID-19 lockdown (July and August 2020). Caregivers completed a set of questionnaires on child and family wellbeing and on whether the child’s internalizing and externalizing symptoms changed during the lockdown as compared to before. Worry of COVID-19 infection was higher amongst caregivers in the Turkish sample and was associated with higher levels of child internalizing symptoms during the lockdown in the Turkish sample, however there were no statistically significant differences in the size of the impact of worry of infection on the children’s internalizing symptoms between the two countries. Co-existence difficulty independently predicted increase in children’s internalizing and externalizing symptoms during the lockdown in both samples. Families in the UK experienced a higher level of difficulty with co-existence compared to the families living in Turkey but the magnitude of the impact of co-existence difficulty on children’s outcomes between the two samples was not significantly different.The findings suggest that public health strategies should aim to reduce social anxiety and invest in the development of programs aimed at supporting families to overcome the challenges of co-existence during times of public health crisis.
Keywords
Introduction
The outbreak of COVID-19 saw a worldwide implementation of fierce social distancing measures including national lockdown and self-isolation. The United Kingdom (UK) and Turkey were amongst the most seriously affected countries worldwide (Worldometer, 2020). The COVID-19 lockdown has had an unprecedented impact on the psychological wellbeing of children and young people in both countries (Adıbelli & Sümen, 2020; Creswell et al., 2021; Panchal et al., 2021), making the identification of the factors that predict it an important research and policy imperative. Culture can shape emotional and behavioral reactions to the pandemic and its consequences (Burkova et al., 2021). Hence, cross-cultural research can reveal culture-specific factors that predict poor child mental health during the lockdown, and further our understanding of the impact of the pandemic on child wellbeing. However, there is limited cross-cultural research on the impact of the pandemic on children’s outcomes (Fernandez Ruiz, 2021; Maaravi et al., 2021; San et al., 2021). Western European cultures are known to promote individualist values of independence and self-reliance whereas the collectivist values of interdependence, compliance, and inhibition dominate in non-Western European cultures (Green et al., 2005). A body of research suggests that a collectivist mindset (vs. individualistic) could explain variations in the impact of COVID-19 amongst different countries. Individualistic societal values are not supposed to promote the greater good as much as the individual benefit, whereas collectivist values endorse sacrifice to support the common good (Maaravi et al., 2021). On these grounds, a few studies proved empirically that collectivism (vs. individualist) was more strongly associated with adherence to public health guidelines to contain the spread of the virus, because collectivist principles promoted the idea of working cooperatively around the prevention of COVID-19 (e.g., Maaravi et al., 2021; Xiao, 2021). Because children are influenced by families which are nested within wider sociocultural systems of influence (Prime et al., 2020), the cross-cultural examination of caregiver emotional and behavioral reactions to the lockdown can reveal determinants of child mental health and wellbeing that are culture specific. According to Hofstede et al. (2005), the UK and Turkey belong to the individualistic and collectivistic cultures, respectively. Given their different cultural values, caregiver reactions to the stressors of the pandemic and subsequent effects on child outcomes could be different across the two countries. Therefore, the aim of the present study is to compare caregiver response to the COVID-19 pandemic and its association with child mental health and wellbeing during the lockdown in UK and Turkey.
Worry over COVID-19 was an emotional response which while it encouraged the adoption of preventive measures in some countries (Harper et al., 2020; Yıldırım et al., 2021), it was associated with psychological distress in some populations (Fitzpatrick et al., 2020; Kayis et al., 2021; Satici, Gocet-Tekin, et al., 2020). Individuals who reported less tolerance to uncertainty were more likely to report high levels of fear of COVID-19. For instance, fear of COVID-19 mediated the relationship between intolerance of uncertainty and mental wellbeing in a large cross-country level survey of adults in Turkey (Satici et al. 2020b). In another survey of Turkish adults, it was found that intolerance of uncertainty was associated with depression and emotional eating via fear of COVID-19 (Pak et al., 2021). Intolerance of uncertainty refers to the level of uncertainty that can be tolerated by an individual and can increase the perception of an imminent threat which, in turn, impacts negatively on the individuals’ psychological adjustment (Chen & Hong, 2010; Taha et al., 2014). For instance, intolerance of uncertainty was associated with more H1NI (swine flu) related anxiety through great appraisal of threat in a large sample of adults (Taha et al., 2014). In another study, stressful daily hassles were related to more symptoms of anxiety in adults with high levels of intolerance (Chen & Hong, 2010). High levels of intolerance to uncertainty were more strongly associated with increased levels of stress, anxiety and depression in a large sample of adults during the pandemic in Brazil (Ferreira et al., 2021). Additionally, low tolerance endorses more emotional than problem focused responses which are linked to adverse mental health outcomes such as depression and anxiety (Taha et al., 2014). Therefore, during the initial stages of the COVID-19 pandemic, which were characterized by a significant ambiguity about the nature and impact of the COVID-19 illness-related-threat, the emotional reactions to it were more acute in conditions of intolerance of uncertainty. From a cultural perspective, tolerance to uncertainty has been defined as the extent to which the members of a culture feel threatened by ambiguous or unknown situations (Hofstede et al., 2005, p. 206). Hofstede et al., (2005) have shown that there is a tendency for collectivism to be associated with less tolerance to uncertainty resulting in perception of threat being more acute in collectivistic contexts. Considering that Turkey is a primarily collectivist society, it is plausible that caregivers in Turkey were more worried over COVID-19 infection compared to caregivers in the UK. A large survey found that fear of COVID-19 infection was higher in a Turkish sample compared to an Austrian sample of migrant and non-migrant young people (Akkaya-Kalayci et al., 2020). However, at the time that this study is prepared, we are aware of no studies that examined caregiver worry of infection cross-culturally. Additionally, while caregiver worry of COVID-19 infection has had a negative impact on child mental health both in collectivist (Saddik et al., 2021) and individualist societies (Kroon et al., 2022), there seems to be a paucity of studies that compare its impact on child mental health across cultures. It is plausible that cross-cultural differences in caregiver worry of infection have a differential impact on child wellbeing with implications for our understanding of culturally-specific pathways of psychopathology during pandemics.
The lockdown was a public health measure adopted by many countries worldwide to mitigate the spread of the virus which led families to spend extended periods of time together in home confinement. Research to date show that families in several European countries such as Italy, Spain (Orgilés et al., 2020), Belgium (Stassart et al., 2021), and the UK (Morgül et al., 2020) struggled to cope with the forced and prolonged family co-existence. Additionally, in the UK, the families who struggled most were more likely to report that their children’s behavior and emotional state had changed for the worse since the lockdown had started (Morgül et al., 2020, 2022). Because collectivism promotes interdependence in the family unit and strong family ties (Hofstede, 2001), it is plausible that the experience of co-existence during the lockdown amongst families in collectivistic cultures may have not been perceived as challenging as amongst families in individualistic cultures, and as a result, may have not had a significant negative impact on the child’s wellbeing during the lockdown. The cross-cultural examination of difficulty with the forced and prolonged family co-existence and its effect on children’s emotional and behavioral outcomes will help understand better the influence of the lockdown on children’s mental health and wellbeing.
The Present Study
The main aim of the study was to examine cultural variation in the impact of caregiver responses to COVID-19 pandemic related stressors on children’s mental health and wellbeing. To this end, we examined whether caregiver worry of COVID-19 infection and family co-existence difficulty differentially predicted the change in children’s internalizing and externalizing symptoms before and during the initial lockdown in the UK and Turkey.
Our study assessed and controlled for the effects of several individual and contextual variables that could influence caregiver worry of infection and the experience of family co-existence and their association with children’s outcomes during the lockdown. Caregiver and child psychological wellbeing during the pandemic was worse in a context of high risk of infection, poor housing conditions, caregiver and child poor mental health, and parenting stress. Risk of infection has been found to interfere with adult mental health and wellbeing during the pandemic across different countries including Turkey and the UK (Kim et al., 2020; Xin et al., 2020; Yıldırım et al., 2021; Yıldırım & Güler, 2021; 2021; Zhou et al., 2020). Poor housing conditions during the lockdown, such as small apartments with limited views and indoor qualities, were associated with depressive symptoms in adults (Amerio et al., 2020), and lack of outside access (i.e., garden or terrace) (Francisco et al., 2020) and overcrowding (Woessmann et al., 2020) with behavior difficulties and academic performance in children, respectively.
Poor parental mental health was associated with poorer social and emotional wellbeing in children and young people during the lockdown across different countries consistently (Brown et al., 2020; Li & Zhou, 2021; Raw et al., 2021; Saddik et al., 2021; Westrupp et al., 2021). Moreover, children with mental health difficulties were more likely to experience a higher level of psychological difficulties during the lockdown (blinded for review; Asbury et al., 2021; Alghrani & Byrne, 2020). Finally, high parenting stress influences the quality of family relationships (Osborne et al. 2008). Several studies found that caregiver stress with the parenting role was related to a higher level of child social and emotional outcomes during the lockdown and a poorer parent-child relationship (Babore et al., 2021; Brown et al., 2020; Cohodes et al., 2021; Lee et al., 2021; Provenzi et al., 2021; Spinelli et al., 2020).
Looking after young children is challenging as they cannot look after themselves or need a lot of support in their social and academic life compared to adolescents (National Academies of Sciences, 2016). Additionally, at the time that this study was designed, the Opinions and Lifestyle Survey (OLS) in Great Britain in April 2020 reported that mothers of younger children experienced much more difficulty with home-schooling as compared to the mothers of older children (Williams et al., 2020). Therefore, the study focused on primary school children because their caregivers were severely impacted by school-closures, and they were overloaded with extra caring and homeschooling responsibilities often while working with no access to any type of support such as childminders or extended family members. The devastating impact of homeschooling and caring for young children during the lockdown on the mental health of caregivers has been documented (e.g., Vicari et al., 2022). Our intention was to understand the wellbeing of this highly vulnerable group of caregivers and their children.
Methods
Participant Recruitment and Procedures
Between the 14th of July 2020 and the 14th of August 2020, biological/non-biological caregivers (>18 years) of primary school children (5–12 years old) living either in the UK (England, Scotland, Wales, and Northern Ireland) or Turkey were invited to complete a 20-min electronic survey on child and family wellbeing distributed via social networks (e.g., Facebook, Instagram), e-mail, and messaging groups (e.g., Whatsapp). Of the 3408 caregivers (nUK = 1830 and nTR = 1578) who accessed the survey, 1849 between 18 to 61 years old had a fully completed questionnaire. Participants were excluded from the analysis if they did not complete the survey or had a large volume of missing data (>5%; nUK = 835 and nTR = 724). The final sample comprised 995 caregivers living in the UK (Mage = 39.16 years, SD = 5.6) and 854 in Turkey (Mage = 38.25 years, SD = 4.7). Survey development details can be found in (Morgül et al., 2020).
Once the prospective participants clicked on the survey link, they were given information about the nature and purpose of the survey and were invited to participate by giving their consent. Participation was anonymous and participants were informed that they could withdraw at any time without any reason. No compensation and no deception were used. Data were collected and processed in accordance with the General Data Protection Regulation and Data Protection Act 2018, as well as Roehampton University’s Data Protection Policy. The study was granted ethics approval by the University of Roehampton Ethics Committee (Ref: PSYC 20/367).
Measures
Sociodemographic Information and Perceived COVID-19 Infection Risk
The first part of the survey included children’s and families’ sociodemographic characteristics (e.g., participant age, marital status, education level, ethnicity and child age, gender, school type) and questions about their housing conditions (e.g., outdoor access, number of rooms and number of people living-in at home during the lockdown). Caregivers indicated their COVID-19 infection risk on a single multiple-choice question of four options (1 = low risk: I do not know anyone who belongs to a risk group or There are friends/family being at-risk group, but not living with them; 2 = high risk: I belong to an at-risk group or People belonging to an at-risk group live with me).
Caregiver Worry of COVID-19 Infection
Caregivers answered four questions about worry of getting infected (e.g., Have you ever worried about being infected with COVID-19 during the recent coronavirus outbreak period?) using a 5-point rating scale (1 = never thought about it - 5 = worried about it all the time). A total infection worry score was calculated by adding participant responses to the four questions (range: 4–20; Cronbach’s α = .87UK; .91TR).
Family Co-Existence Difficulty
Adapted from Orgilés et al. (2020), caregivers were asked to rate how difficult it was for them to co-exist with all the family members at home (e.g., How hard do you think it was for your family to co-exist during the lockdown?) on a 5-point rating scale (1 = very easy - 5 = very difficult). A higher level of family co-existence difficulty was related to a higher level of child emotional and behavioral difficulties during the lockdown compared to before in families in Italy, Spain and Belgium (Orgilés et al., 2020; Stassart et al., 2021).
Children’s Internalizing and Externalizing Symptoms During the Lockdown as Compared to Before
Caregivers indicated how much they thought their children’s symptoms of emotional and behavioral difficulties changed during the lockdown by rating 23 emotional and behavioral symptom items (e.g., My child is anxious; My child is angry) on a 5-point scale (1 = much less compared to before quarantine; 2 = somewhat less compared to before quarantine; 3 = stayed the same; 4 = somewhat more compared to before quarantine; 5 = much more compared to before quarantine) (Morgül et al., 2020; Orgilés et al., 2020). A total internalizing symptom score (TIS; 5 items; range: 5–25; Cronbach’s α = .88UK; .90TR) and a total externalizing symptom score (TES; 6 items; range: 6–30; Cronbach’s α = .92UK; .89TR) during the lockdown compared to before was calculated by adding up the scores of all the symptom items. Higher ratings indicate higher levels of difficulty during the lockdown than before. Details on the TIS and TES score development can be found in Supplement 1.
Caregiver Mental Health
Caregivers completed the 21-item Depression, Anxiety, and Stress Scale (DASS-21; Lovibond & Lovibond, 1995). It includes three 7-item subscales that measure the emotional states of depression, anxiety, and stress rated on a four-point scale (0 = did not apply to me at all - 3 = applied to me very much, or most of the time). The total score was calculated by adding the subscale scores (range: 0–63). The Turkish version of the DASS-21 has adequate psychometric properties (Yıldırım et al., 2018). The three-factor model explained 52.76% of the total variance, and the individual factors of depression, anxiety and stress explained 18.29%, 16.10% and 18.37% of the total variance, respectively. Additionally, subscale internal reliability was excellent (Cronbach’s α values: Depression = .89, Anxiety = .87, and Stress = .90). Similarly, high levels of internal reliability were detected in our samples (Cronbach’s α = .94UK; .94TR).
Parenting Stress
Caregivers completed the 18-item Parental Stress Scale (PSS; Berry & Jones, 1995). It comprises four subscales that examine parenting stressors (6 items), loss of control (3 items), satisfaction (3 items), and rewards (6 items) rated on a 5-point scale (1 = strongly disagree - 5 = strongly agree). Eight items are reverse scored. A total score is generated by adding the subscale scores (range: 18–90). The Turkish version of the PSS has adequate psychometric properties (Gördesli & Sünbül, 2021). The original four-factor solution explained 43.20% of the total variance, and the individual factors of parental rewards, parental stressors, lack of control, and parental satisfaction explained 14.88%, 12.96%, 9.83%, 5.56%, respectively. The PSS subscales showed good internal reliability (Cronbach’s α values: parental rewards = .76, parental stressors = .72, lack of control = .70, and parental satisfaction = .71). Similarly, internal reliability was good in our samples (Cronbach’s α = .88UK; .83TR).
Child Emotional and Behavioral Difficulties
Caregivers completed the parent-reported version of the 25-item Strengths and Difficulties Questionnaire (SDQ) (Goodman, 2001) developed for children between 4 and 17 years old. It comprises five subscales (emotional symptoms, conduct problems, hyperactivity, peer problems, and pro-social behavior) of five items each rated on 3-point scale (0 = not true - 2 = certainly true). A total difficulty score (range: 0–40) is generated by adding all the subscales, except for the pro-social behavior scale. The SDQ is a psychometrically robust and widely used scale to screen for probable mental disorders in children across the world including Turkey and was found to distinguish cases from non-cases of disorders against the well-established Development and Well-Being Assessment (Husky et al., 2018). Psychometric properties of the Turkish version of the parent SDQ form showed good internal reliability for the total difficulties score (Cronbach’s α = .78) (Husky et al., 2018). In our study, internal reliability of the total scores for each sample was good (Cronbach’s α = .87UK; .78TR).
Translation of Instruments
The Turkish versions of the SDQ, DASS-21 and PSS are publicly available at https://www.sdqinfo.org/py/sdqinfo/b0.py, https://toad.halileksi.net/olcek/depresyon-anksiyete-stres-21-olcegi, and https://toad.halileksi.net/sites/default/files/pdf/parental-stress-scale-toad.pdf, respectively. The remaining instruments were translated into Turkish from the original language (English) by the first author who is a native Turkish speaker and fluent in English, and they were checked for accuracy in meaning and cultural sensitivity by a translator who is a native English speaker and fluent in Turkish. Discrepancies were discussed and resolved by joint agreement of both translators.
Data Analysis
Statistical analyses were performed using the IBM SPSS 26 (Statistical Package for the Social Sciences) and AMOS 18 (Analysis of Moment Structures). Because of missing data on a few internalizing and externalizing symptom-items (≤5% of values were missing across 23 symptom - items), multiple imputation was performed using the Markov Chain Monte Carlo procedure in SPSS (Graham, 2012). Imputation of missing values was performed for symptom-items only. A preliminary screening of the data revealed no issues with multicollinearity, outliers, and normality (Tabachnick et al., 2007). No multicollinearity was detected via variance inflation factor (VIF <5) (Becker et al., 2015). The outliers were tested, and no extreme values were identified, thereby no case was removed from the sample. To check for the assumptions of normality, skewness and kurtosis values were calculated for each of the study variables. Except for the kurtosis and skewness value of outdoor access, which is considered acceptable according to Hair et al. (2010) and Byrne (2010), none of the variables presented extreme skewness and kurtosis values falling outside the proposed threshold of ±2, suggesting a normal distribution for the study variables (Brown, 2006; George & Mallery, 2010).
For comparisons between the two samples, we used one-way analysis of variance (ANOVA) and independent groups t-tests for continuous variables, and Chi-squared tests for categorical variables. Differences were considered statistically significant at p < .05. We ran Pearson correlations to examine the relationship between the study variables in each sample. If the main study variables, worry of infection or co-existence difficulty, were significantly correlated with either the child’s TIS or TES score in either sample, we used post-hoc Fisher’s z-tests (Sheshkin, 2004) to estimate the magnitude of the difference between the two correlations. In this procedure, correlation coefficients were transformed using Fisher’s Z transformations, so that Z has an approximate normal distribution.
We ran multiple regression analysis to examine the contribution of worry of infection and co-existence difficulty to the variance of children’s TIS and TES scores, in the UK and the Turkish sample, respectively, after controlling for the effect of the covariate variables. If worry of infection or co-existence difficulty was significantly predictive of children’s TIS or TES scores in either sample, we ran post-hoc tests to estimate the magnitude of the difference between the two the regression coefficients (β) by including the interaction terms. A new regression equation was performed on the combined samples by adding a dummy variable called Country (UK: 0, Turkey: 1) that denotes the ‘group variable’ as well as the interaction of Country with the study predictors (Clogg et al., 1995). If the interaction term was statistically significant (p < .05), it indicated that the regression coefficient (β) was significantly different across the two samples.
Results
Participant Sociodemographic Characteristics
Between-Country Differences in Study Variables.
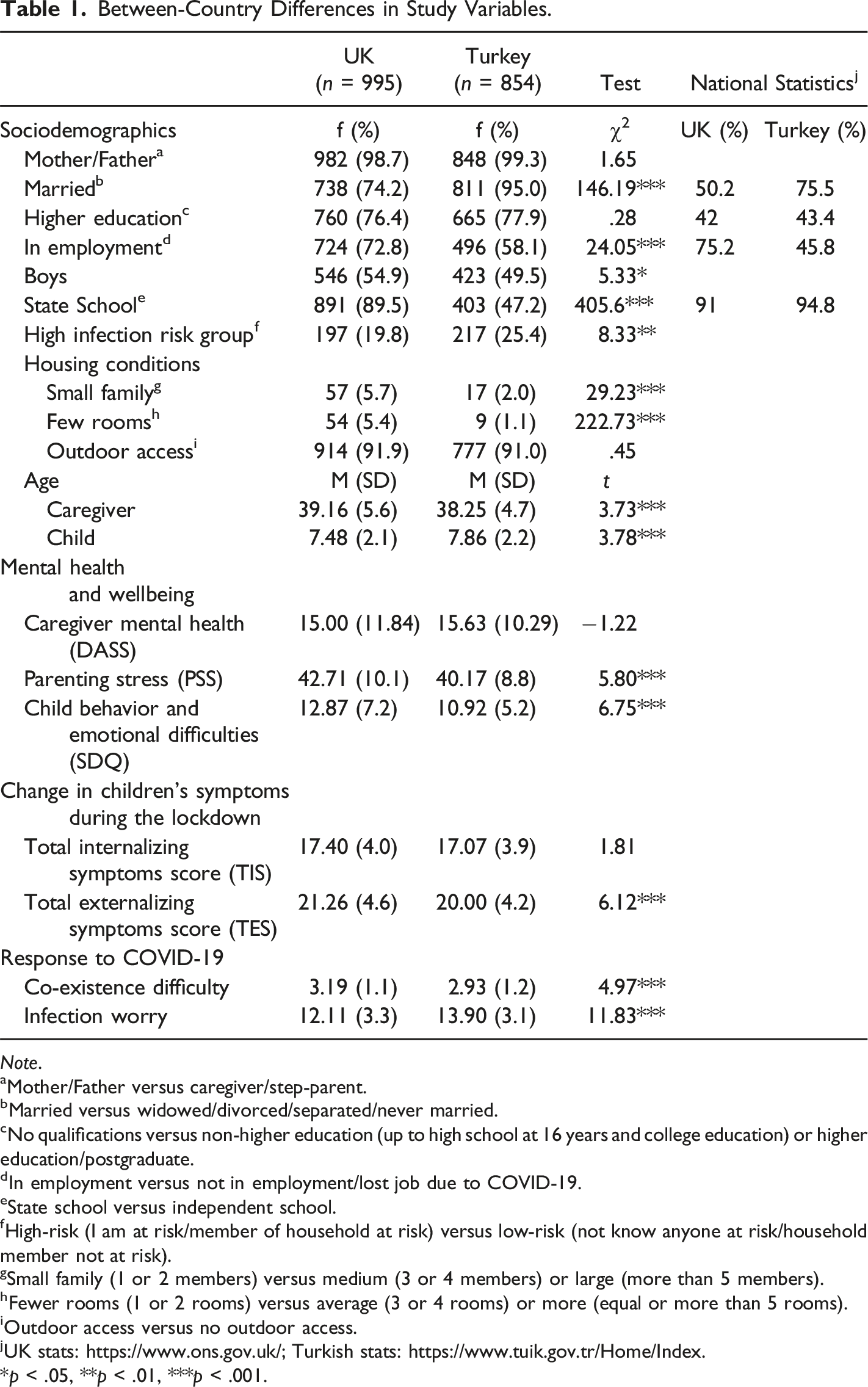
Note. aMother/Father versus caregiver/step-parent.
bMarried versus widowed/divorced/separated/never married.
cNo qualifications versus non-higher education (up to high school at 16 years and college education) or higher education/postgraduate.
dIn employment versus not in employment/lost job due to COVID-19.
eState school versus independent school.
fHigh-risk (I am at risk/member of household at risk) versus low-risk (not know anyone at risk/household member not at risk).
gSmall family (1 or 2 members) versus medium (3 or 4 members) or large (more than 5 members).
hFewer rooms (1 or 2 rooms) versus average (3 or 4 rooms) or more (equal or more than 5 rooms).
iOutdoor access versus no outdoor access.
jUK stats: https://www.ons.gov.uk/; Turkish stats: https://www.tuik.gov.tr/Home/Index.
*p < .05, **p < .01, ***p < .001.
In the UK, non-completers were slightly younger than completers (Mage-nonCOMP = 21.76, SD = 6.33; Mage-COMP = 23.20, SD = 5.64) (F (1,1634) = 21.38, p = .001). Both non-completers and completers were mostly white (nnonCOMP = 402, 76.6%; nCOMP = 749, 67.4%), married (nnonCOMP = 345, 65.7%; nCOMP = 835, 75.2%) working mothers (nnonCOMP = 291, 72.2%; nCOMP = 793, 71.5%) with a university degree (nnonCOMP = 271, 67.2%; nCOMP = 852, 76.8%). Nearly half of the children were boys (nboys-nonCOMP = 209, 52.4%; nboys-COMP = 596, 54.0%). The percentage of belonging to a White ethnic background was statistically significantly higher in non-completers than in completers (x 2 (2, n = 1636) = 15.91, p < .001). The percentage of being married (x 2 (1, n = 1636) = 15.81, p < .001) and having a university or post graduate degree (x 2 (1, n = 1512) = 14.20, p < .001) was significantly higher in the completers compared to the non-completers.
In the Turkish sample, non-completers were slightly older than completers (Mage-nonCOMP = 22.82, SD = 7.62; Mage-COMP = 22.07, SD = 5.00) (F (1,1387) = 3.96, p = .047). Both non-completers and completers were mostly Turkish (nnonCOMP = 255, 92.4%; nCOMP = 991, 89.0% COMP), married (nnonCOMP = 252, 91.3%; nCOMP = 1047, 94.1%) working mothers (nnonCOMP = 115, 51.3%; nCOMP = 617, 55.6%) with a university degree (nnonCOMP = 180, 80.4%; nCOMP = 935, 84.3%). Nearly half of their children were boys (nboys-nonCOMP = 124, 56.1%; nboysCOMP = 552, 50.2%). There was no statistically significant difference in ethnicity, marital status, caregiver education and employment status between the non-completers and completers in the Turkish sample.
Between-Country Differences in Study Variables
Between-country differences are presented in Table 1. Compared to the caregivers in the Turkish sample, caregivers in the UK sample were older, and more likely to have a job, be lone/never married, belong to a small household (1–2 members), and live in a house with fewer rooms.
No significant differences were found in level of education. Compared to children in Turkey, children in the UK were younger, more likely to be boys, and attend state schools. Children in the UK sample were reported to experience more behavior and emotional difficulties than children in the Turkish sample. Additionally, caregivers in the UK sample reported more stress related to their parenting role. Caregivers in the Turkish sample were more likely to belong to a high-risk group for COVID-19 infection and to worry about getting infected, but less likely to have trouble with co-existence than caregivers in the UK sample. The proportion of caregivers who were married and had a higher education in the study samples was higher than in the national population of each country. The Turkish sample had a higher proportion of caregivers in employment and whose children attended private schools than the national population. There were no statistically significant differences between the two samples in the score of children’s TIS during the lockdown, but caregivers in the UK sample were more likely than caregivers in the Turkish sample to report higher levels of TES during the lockdown as compared to before.
Association of Caregiver Worry of COVID-19 Infection and Family Co-existence Difficulty with Children’s Total Internalizing (TIS) and Externalizing Symptoms (TES) Scores During the Lockdown
Correlations Between Study Variables and Change in Children’s Internalizing and Externalizing Symptoms During the Lockdown in the UK and Turkey.
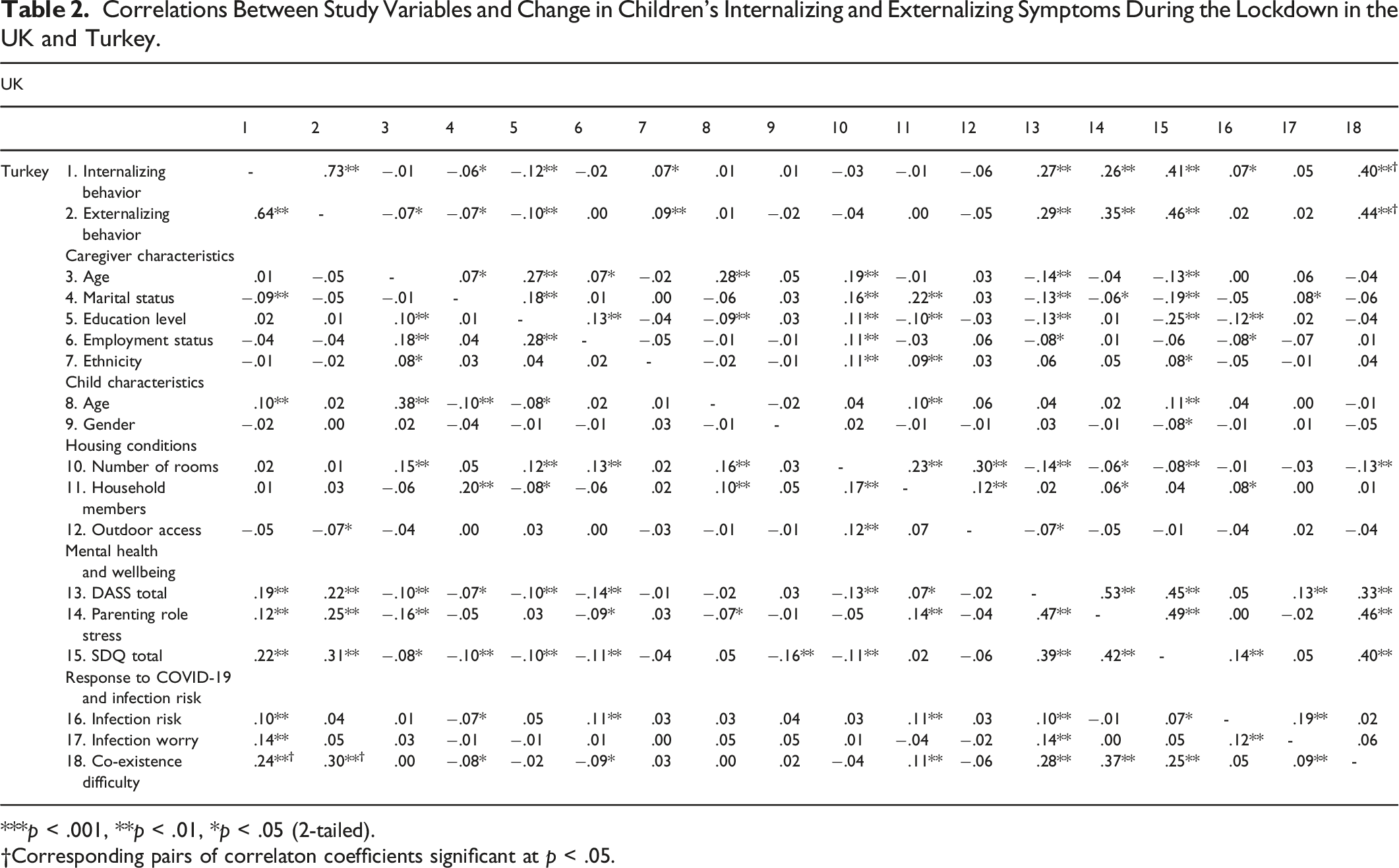
***p < .001, **p < .01, *p < .05 (2-tailed).
†Corresponding pairs of correlaton coefficients significant at p < .05.
Predictors of the Change in Children’s Total Internalizing and Externalizing Symptom Scores During the Lockdown
The study variables that were statistically significantly correlated with either the TIS or TES score in either sample or with either worry of infection or co-existence difficulty in either sample were included in the hierarchical regression analysis (Table 2). A description of the associations between the study variables can be found in Supplement 2. Although gender was not significantly associated with children’s TIS and TES, worry of infection and co-existence difficulty, because the boys in the Turkish sample were significantly fewer than the boys in the UK sample, the analysis controlled for its effect. Although worry of infection was not significantly associated with the TES scores either in the UK or Turkish sample, considering a potential suppressor effect, it was included in the regressions analysis carried out for predicting the TES. We entered the sociodemographic variables including housing conditions in the first step, caregiver mental health and parenting stress in the second step, child mental health in the third step, and caregiver response to COVID-19 variables in the fourth step.
Summary of Regression Analysis of Change in Children’s Internalizing Symptoms Before and During the Lockdown in the UK and Turkey.
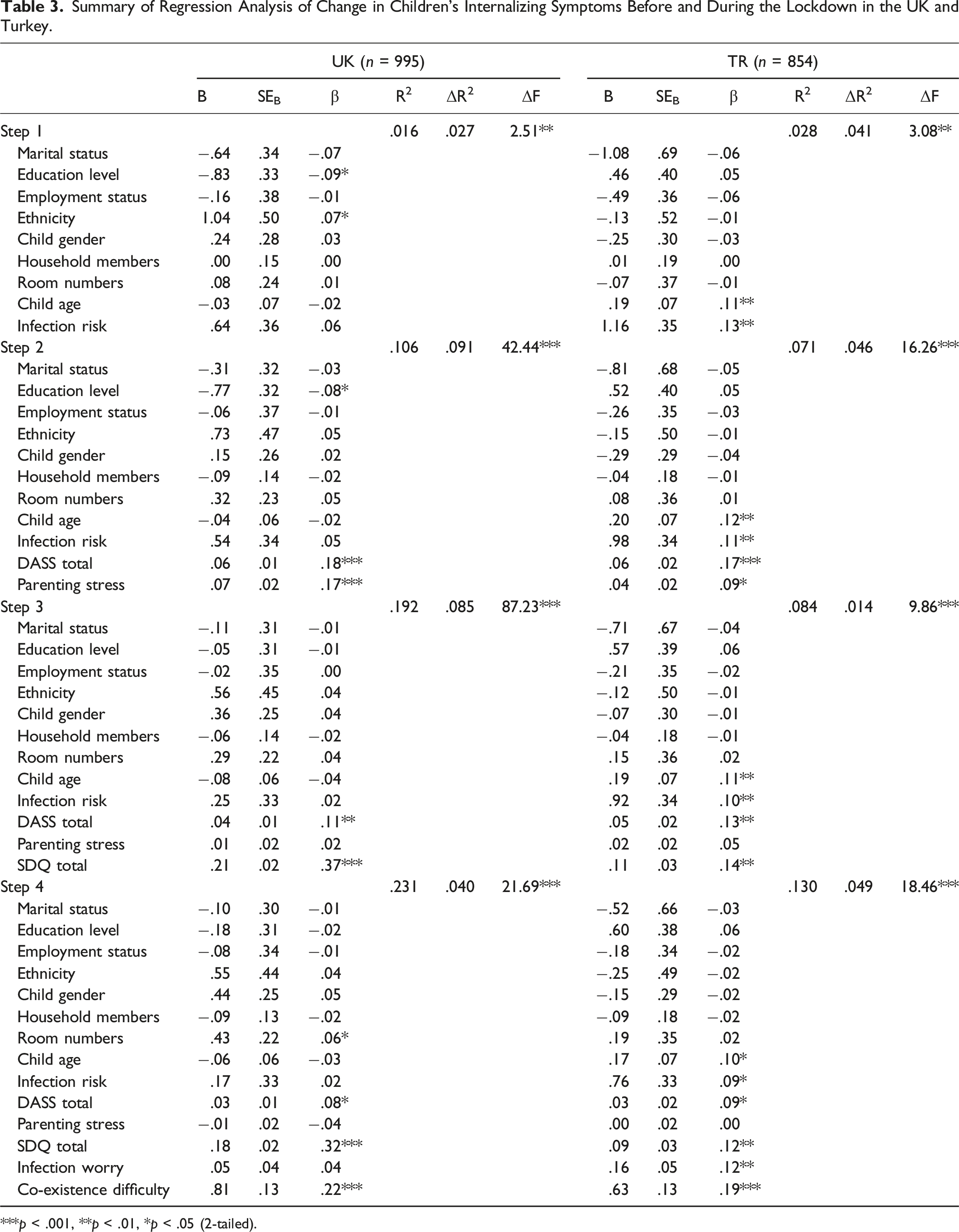
***p < .001, **p < .01, *p < .05 (2-tailed).
Summary of Regression Analysis of Change in Children’s Externalizing Symptoms During the Lockdown in the UK and Turkey.
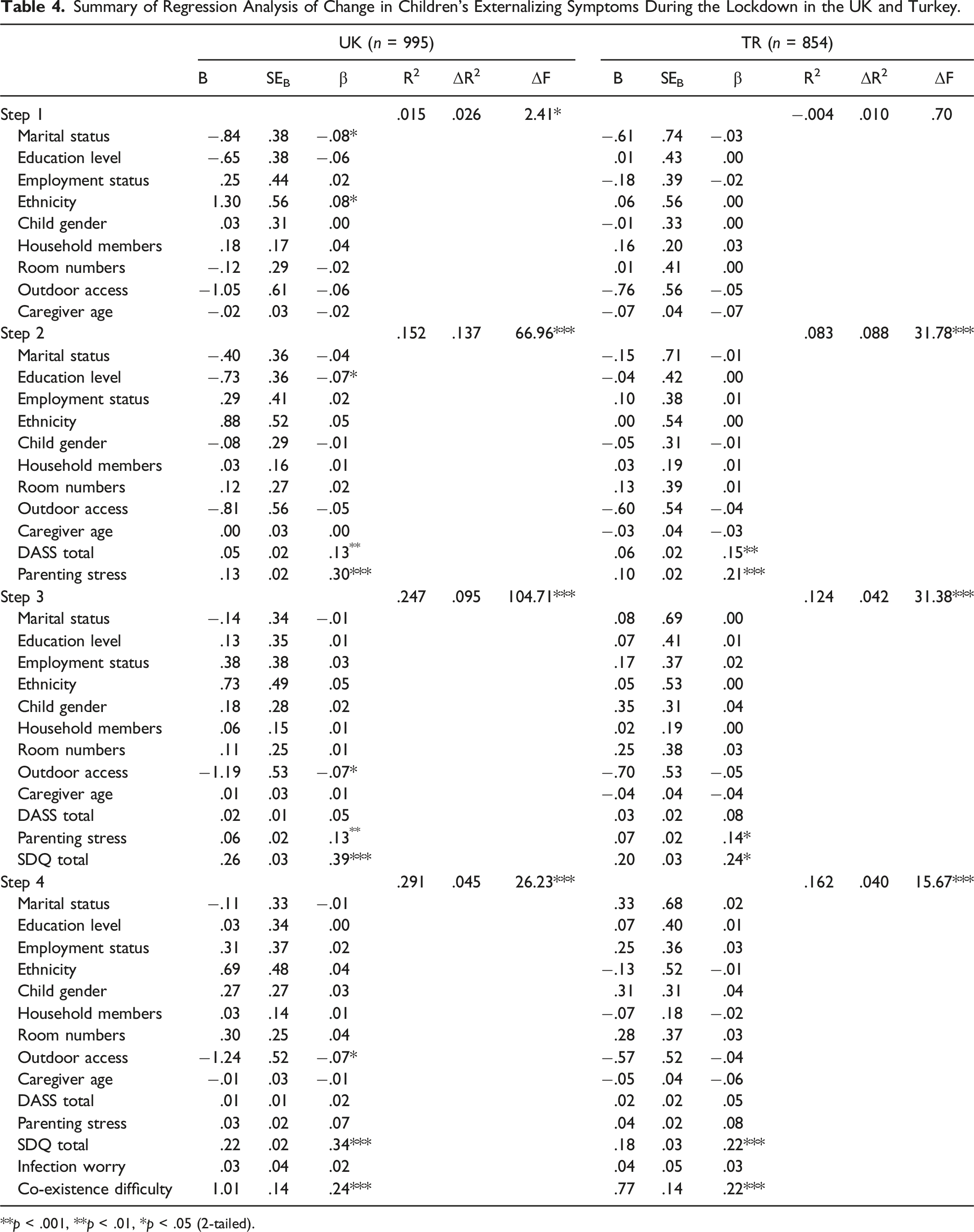
**p < .001, **p < .01, *p < .05 (2-tailed).
Discussion
Our study examined the difference in the impact of worry of infection and family co-existence difficulty on children’s emotional and behavior outcomes during the initial national lockdown in the UK and Turkey. To our knowledge, our study is the first to have contrasted the perception of worry of COVID-19 infection and co-existence difficulty between caregivers in collectivist and individualist oriented countries after controlling for a range of individual and contextual variables including housing conditions, infection risk, and caregiver and child mental health.
Previous research has emphasized the role of fear of COVID-19 infection that has been identified to be an important predictor of psychological outcomes in the Turkish population during the pandemic (e.g., Kayis et al., 2021; Satici et al. 2020a) and revealed differences in the levels of worry of infection experienced by Turkish and European samples of adolescents (Akkaya-Kalayci et al., 2020). Moreover, perception of an imminent illness-related threat, could be more acute in collectivistic contexts because they are less tolerant to uncertainty triggered by unknown events (Hofstede et al., 2005). On these grounds, we speculated that the uncertainty created by the fast spread of the infection may have caused caregivers in Turkey to experience different levels of worry of COVID-19 infection compared to caregivers in the UK, a individualistic society, and that their different experience may have had a differential impact on children’s outcomes between two countries. Worry of infection was higher and uniquely predicted children’s internalizing difficulties in the Turkish sample, however, post hoc analysis showed that the impact of worry of infection on children’s internalizing symptoms did not significantly differ between samples. Our findings did not offer strong evidence for a differential contribution of worry of infection to the outcomes of children in Turkey compared to the UK after controlling for a range of variables, including child and caregiver mental health, parenting stress and infection risk, and suggest that worry of infection differences across countries may not be culturally specific. The higher levels of caregiver worry over COVID-19 infection detected in the Turkish sample could be attributed to lower citizen trust in government and health authorities (Uslaner, 2018). Trust in the authorities’ decisions for the society is critical in crisis management and can significantly influence the public’s reaction to an imminent threat (Xiao, 2021). Another plausible explanation is that caregivers in the Turkish sample reported higher worry of COVID-19 infection because they reported a higher rate of COVID-19 infection risk than the families in the UK sample.
While caregivers in the Turkish sample were more worried over COVID-19 infection compared to the caregivers in the UK sample, they experienced less difficulty with family co-existence, despite reporting a higher number of family membership. The difference could be attributed to the collectivistic orientation of the Turkish families that values interdependence and close-knit family ties (Kusdil and Kagitcibasi, 2000). Because interdependence in the family unit cultivates a sense of belongin and purpose (Hofstede, 2001), spending time with the family during the lockdown may have not influenced families in collectivist societies as dramatically as in individualistic societies. Additionally, because collectivism promotes a strong sense of responsibility for the community and maintenance of social order, it encourages high adherence to prevention measures (Cukur et al., 2004; Germani et al., 2020; Huang et al., 2020; Maaravi et al., 2021). The lockdown was one of the various public health measures that countries used to mitigate the spread of the virus. Families in collectivistic cultures may have perceived the confinement yet another prevention strategy to adhere to and as a result were more tolerant to its impact. However, the findings from a recent longitudinal study of a small sample of primarily white and middle-class families with children between 10 and 13 years old living in Netherlands, a country based on individualistic principles, showed that parents reported positive experiences of the lockdown as a result of more free time and opportunity to spend time with the family (Achterberg et al., 2021). Another plausible explanation is that caregivers in the Turkish sample reported less co-existence difficulty because the children already had had lower rates of externalizing symptoms and mental health difficulties than the children in the UK sample. Nevertheless, family co-existence difficulty uniquely predicted increased levels in internalizing and externalizing symptoms during the lockdown in both samples even after accounting for the effects of several individual and contextual factors. Collectively, our findings are in line with existing research and suggest that the harmful impact of the forced and prolonged family co-existence on children’s social and emotional outcomes during the lockdown may be independent of the cultural context that it emerges in.
Implications
Arguably, efforts to understand the impact of the lockdown on children’s mental health and family wellbeing across the globe should take into account the effects of contextual factors such as caregiver responses to COVID-19 related stressors. Our findings propose that public health strategies should aim to reduce worry and social panic in the face of imminent health crisis. To alleviate worry of infection and uncertainty in the potential outcomes of a pandemic, government and health institutions should propose appropriate psychoeducational resources enlightening the public about the associated emotions (i.e., worry, anxiety, fear). This can support families in the way to normalize their feelings during these challenging times and may help them manage this disease-related worry efficiently. It is recommended that in the event of future public health crisis, governments should impose certain regulations to restrict the use of anxiety-provoking content of pandemic-related messages (e.g., scenes from intensive care units) as they may increase fear and trigger depressive symptoms among some individuals (Pak et al., 2021). For instance, a meta-analysis suggests that the exposure to COVID-19 news and information (e.g., patients on ventilators and their mortality rates) was associated with uncertainty-related responses such as disease concern and some adverse psychological reactions (Chu et al., 2022). Additionally, potential long-term effects of caregiver infection worry on children’s psychological functioning should be examined where the threat was persistent (e.g., several prolonged lockdowns) or where the public health response was poor. Further research should also compare children’s outcomes against children experiencing the lockdown in less threatening environments. Finally, our findings suggest that investing in the development of programs that aim to raise awareness of the challenges involved in living together and ways to overcome them during a public health crisis could be beneficial for families in individualistic and collectivist contexts.
Limitations
The cross-sectional design did not allow to examine the long-term impact of the lockdown in children’s internalizing and externalizing behavior. Changes in children’s symptoms were based only on the perception of the caregiver. Majority of participants were female university graduates. Additionally, half of the Turkish children were primarily attending private schools, which is not representative of the national population. The caregivers in Turkey could have been amongst the most stressed to access the study and therefore the higher levels in worry of COVID-19 infection might not represent the average level of worry in the population. Combined with the finding that the non-completers in the UK were significantly different to the completers in terms of education, employment and marital status, generalization of the findings should be approached with caution. The study did not use any measures to examine collectivism versus individualism, and tolerance of uncertainty. While we cannot argue with certainty that heightened worry of infection in the Turkish sample is the result of cultural factors, the difference should reflect the primary challenges that caregivers had to grapple with. The use of a single-item measure to examine family co-existence difficulty may have not allowed to capture the construct fully. Future studies should consider using multi-item measures to enhance the validity of the assessment of the family co-existence construct. People often access surveys either because they want to voice a concern or because they hope that completing the survey will help them to understand themselves better (Poon et al., 2004). Accordingly, we can be confident that the findings offer an indication of the primary reasons that compelled the caregivers to access the survey in this point in time and within a specific cultural context. Replication studies should include longitudinal design, multi-informant methods of assessing children’s emotional state and behavior and measures that capture cultural orientation.
Supplemental Material
Supplemental Material - Caregiver Worry of Infection and Family Co-existence Difficulty and Association With Change in Children’s Internalizing and Externalizing Symptoms During the Initial COVID-19 Lockdown in the UK and Turkey
Supplemental Material for Caregiver Worry of Infection and Family Co-existence Difficulty and Association With Change in Children’s Internalizing and Externalizing Symptoms During the Initial COVID-19 Lockdown in the UK and Turkey by Evren Morgül, Angeliki Kallitsoglou, and Cecilia A. Essau in Psychological Reports
Supplemental Material
Supplemental Material - Caregiver Worry of Infection and Family Co-existence Difficulty and Association With Change in Children’s Internalizing and Externalizing Symptoms During the Initial COVID-19 Lockdown in the UK and Turkey
Supplemental Material for Caregiver Worry of Infection and Family Co-existence Difficulty and Association With Change in Children’s Internalizing and Externalizing Symptoms During the Initial COVID-19 Lockdown in the UK and Turkey by Evren Morgül, Angeliki Kallitsoglou and Cecilia A. Essau in Psychological Reports
Footnotes
Acknowledgments
The authors would like to thank to the families for their participation in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available from the authors upon reasonable request. Requests to access the datasets should be directed to the corresponding author of the article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.