
Abstract
This paper investigates how positive and negative work-personal life interface constructs are differentially associated with intentions to stay in or leave the profession. The findings help map work-personal life interface constructs on the typology of determinants of intention to stay and intention to leave (disengagers, retainers, criticals, and neutrals). The ordered logistic regression (ologit) modelling of cross-sectional data from a representative sample (n = 601) of midwives in Canada shows that work interference with personal life is a disengager, which has a stronger association with intention to leave than with intention to stay in the profession. Among the work-personal life interface constructs, work enhancement of personal life seems to be the most critical determinant, showing the most substantive association with both intention to stay and intention to leave. This finding suggests that interventions to increase midwives’ intention to stay and decrease their intention to leave should focus on amplifying the enhancing effects of working on midwives’ personal lives. Interventions that aim to reduce work interference with personal life might be more effective in decreasing intention to leave the profession than increasing intention to stay.
Keywords
Introduction
Due to the organizational importance of turnover and its association with various direct and indirect costs (Duffield et al., 2014; Mohammed et al., 2016), employees’ turnover and their intentions to stay in or leave organizations have been investigated by many researchers in the field of occupational and organizational psychology (Laulié & Morgeson, 2021; Ng et al., 2019). According to role theory (Kahn et al., 1964), individuals are engaged in work roles and roles related to their personal lives. Based on this theory, among the factors that have been identified as associated with employees’ intention to stay or leave, those that reflect on employees’ perception of how work and personal life impact one another have particularly been of interest. Research on the interface of work and personal life initially focused on the negative experiences resulting from work interference with personal life (WIPL), also known as work to life conflict and personal life interference with work (PLIW) or life to work conflict. However, over the years, interest in the positive experiences one has as a result of engagement in various work and life roles has expanded through studies on work-enhancement of personal life (WEPL) and personal life enhancement of work (PLEW) (Lapierre et al., 2018; McNall et al., 2010). Research suggests that employees who feel that their work is negatively impacting the other aspects of their lives are more likely to want to leave their jobs (Amstad et al., 2011; Boamah & Laschinger, 2016; Chen et al., 2018; Noor & Maad, 2008) and less likely to want to stay (Aboobaker et al., 2019; Butts et al., 2013). On the other hand, those who feel that work positively influences their lives have a lower intention to leave (Jiang & Shen, 2018; Russo & Buonocore, 2012).
There are, however, several gaps in this literature that this study aims to narrow. First, this study contributes to the literature by focusing on occupational-level intentions. Researchers have often focused on individuals’ intentions towards the organization in which they are employed (Flinkman et al., 2010). In comparison, individuals’ intention to stay in or leave their professions or occupations is less studied (Kossek & Lee, 2017; Li et al., 2019). Occupational-level intentions become especially important in contexts like the healthcare sector, with specific occupational and contextual demands (e.g., on-call and shift work structure and life-and-death situations) that can uniquely influence work-life interface experiences. In these contexts, the decision to leave an organization might be followed by seeking a position in another. However, the decision to leave the profession results in the loss of the individuals’ knowledge and skills from the healthcare sector. Furthermore, it is not uncommon for workers in the healthcare sector (e.g., physicians, midwives) in certain countries and jurisdictions to be considered self-employed or independent contractors (Levitt, 2020; Thiessen et al., 2020), not employees of a specific organization. Studying this topic is particularly important as shortages are anticipated for various healthcare occupations (Haddad et al., 2020; Zimmerman et al., 2002). Therefore, intentions to stay in or leave the profession can significantly affect the availability of services and the health and wellbeing of the public.
Second, this study contributes to knowledge by clearly distinguishing between intention to stay and intention to leave. Despite criticisms towards treating intention to stay and intention to leave as two sides of the same construct (Cho et al., 2009; Nanncarrow et al., 2014; Radford, 2013), it is not uncommon for empirical studies (Ghosh et al., 2013; Hansen et al., 2003; Johari et al., 2012) to use them interchangeably. Meta-analyses and reviews on this topic vary in their approach towards intention to stay and intention to leave. Some reviews treat intention to stay and intention to leave as the same constructs (Chan et al., 2013), while others differentiate between them and report on their determinants separately (Al Zamel et al., 2020). Distinguishing between seemingly similar variables such as customer satisfaction and dissatisfaction (Cadotte & Turgeon, 1988), job satisfaction and dissatisfaction (Herzberg et al., 1959), or health and absence of disease (Larsen, 2021) and their antecedents and consequences has resulted in sizable bodies of literature in their respective fields with extensive practical implications. However, only a handful of empirical studies (Cho et al., 2009; McCarthy et al., 2007; Nanncarrow et al., 2014) have tested the difference between intention to stay and intention to leave and factors associated with them. Cho et al. (2009) propose a typology of determinants of intention to stay and intention to leave where disengagers are variables that influence the intention to leave but not the intention to stay; retainers are those that influence the intention to stay but not the intention to leave, criticals are those that influence both, and neutrals are those that do not influence either intention to stay or intention to leave.
This study’s third and fourth contributions are using a unique sample of healthcare workers in Canada and applying a novel typology of intention to stay and leave determinants. For this investigation, cross-sectional surveys collected from 601 midwives practicing in Canada are used to investigate whether positive and negative constructs at work and personal life interface are differentially associated with midwives’ intention to stay in or leave the midwifery profession. The findings would enable us to map these variables on Cho et al.’s (2009) typology of determinants of intention to stay and intention to leave. We found no studies that explicitly attempted to map positive and negative variables at the interface of work and life on this typology.
Review of the Literature
Based on the theory of planned behaviour (Ajzen, 1985), intentions are good predictors of a person’s behaviour and decisions. Therefore, intention to stay, defined as an individual’s willingness to continue to work in a profession (Tett & Meyer, 1993) and intention to leave, which reflects an individual’s desire to leave a profession in the near future (Flinkman et al., 2008), are used to address the issues of workforce attachment and workforce shortage. The overarching theory guiding this research is the job demands-resources model (Bakker & Demerouti, 2007). This model was originally developed to explain how job demands and resources affect burnout or work engagement. However, the job demands-resources model also explains experiences at the interface of individuals’ work and personal lives (Bakker et al., 2011). This model suggests that individuals’ perceptions of the interface of their work and personal life are shaped based on the demands of time, energy, and emotions for each role and the resources individuals have to allocate to those roles to fulfill those demands. This model has been used to investigate determinants of both intention to stay (Sánchez-Cardona et al., 2021) and intention to leave (Moloney et al., 2018).
The job demands-resources model is extended through strain theory (Goode, 1960) to better explain the negative perceptions at work and personal life interface and expansion theory (Marks, 1977) to reflect on the positive experiences at the interface of work and personal life. Thus, some of the nuances of our model are supported with the use of these other theories to extend our main theoretical framework rooted in the job demands-resources model. The strain theory suggests that individuals have limited time, energy, and emotional resources, and as the demands from one’s job or personal life increase, the pool of resources is depleted. Work interferes with personal life (WIPL) when work demands draw upon the resources required for satisfying engagement with personal life roles, including self-care or roles related to relationships with family and friends. Personal life interferes with work (PLIW) when participating in personal life roles, such as taking care of family members and loved ones, attending social gatherings, or self-care, consumes the resources needed for good performance and engagement with one’s work. The expansion hypothesis (Marks, 1977) argues that individuals’ resources of emotions, time, or energy might be extended because they participate in different work and non-work roles or the positive experiences in one role might improve the quality of life in other roles. Based on this theory, the concept of enhancement (Ruderman et al., 2002) was developed to refer to the positive effects of work and personal life on one another. Work enhancement of personal life (WEPL) happens when one’s non-work roles improve because of their work. Personal life enhancement of work (PLEW) happens when an individual’s work experience or performance is improved because they participate in various non-work roles. In addition to the positive effects of material gains at work on personal life, research has shown various positive effects of work on personal life. For example, being satisfied with one’s job performance is positively associated with performance as a parent (Friedman & Greenhaus, 2000). Furthermore, leadership, time management, goal-setting, and self-direction skills obtained at work can positively affect various personal life roles (Greenhaus & Powell, 2006). On the other hand, self-esteem and confidence developed in the personal life domain (Ruderman et al., 2002), and spousal emotional support are positively linked to career success (Friedman & Greenhaus, 2000).
Regarding the rationale of why WIPL and WEPL might be differentially associated with intention to stay and intention to leave, and therefore map differently on the Cho et al.‘s (2009) typology of determinants of intention to stay and intention to leave, we draw from the salutogenic theory developed by Antonovsky (1979). The salutogenic theory distinguishes between stressors or risk factors (e.g., physical and biomedical challenges, life crises, and conflict) that can cause diseases and generalized resistance resources (e.g., knowledge of coping strategies, cohesion and control, and social support) that can help individuals maintain or improve their health as well as cope with the stressors (Antonovsky, 1979). For the negative side of the interface of work and personal life, previous studies have reported the association between WIPL and PLIW and conditions such as burnout (Brauchli et al., 2011), depression (Beutell Nicholas & Schneer Joy, 2014), mental distress (Lee & Jang, 2017), neck pain and back pain (Baur et al., 2018), cardiovascular problems and digestive problems (Scholarios et al., 2017). WEPL, on the other hand, is positively associated with health, as measured by self-reporting (Ejlertsson et al., 2020). A salutogenic perspective aids in seeing how these factors fit into a job demands-resources model framework; in particular, these findings suggest that WIPL and PLIW can be categorized as stressors and risk factors, while WEPL and PLEW can be considered health-enhancing. It is a natural reaction for individuals to avoid stressors and risk factors while seeking proximity to generalized resistance resources and health-enhancing factors.
The blame for interference or credit for enhancement is often placed on the domain perceived as the origin of the interference or enhancement (Grandey et al., 2005; Lapierre et al., 2008). This perception potentially affects the targets of an individual’s attitudes, intentions, and behaviours. As a result, meta-analysis studies suggest that WIPL and WEPL are more strongly associated with work-related outcomes, while PLIW and WIPL are more strongly associated with personal life-related attitudes (Shockley & Singla, 2011). As the outcomes of this research are work-related, we focus our hypotheses on the differential associations of WIPL and WEPL with the intention to stay in or leave the profession. However, we also test the association of PLIW and PLEW with these outcomes. Findings help to map the positive and negative constructs at the work and personal life interface on Cho et al.’s (2009) typology of determinants of intention to stay and intention to leave and among the disengagers, retainers, criticals, or neutrals (this mapping is further developed in the discussion section). Based on the theoretical foundation provided, when interference occurs, this feedback encourages individuals to avoid stressors; thus, we suggest that individuals’ perception of work as the origin of stress is more strongly related to their intention to abandon that domain. Furthermore, when enhancement occurs, this feedback encourages individuals to seek order, and as such, the perception that work is the origin of health-enhancing factors is more strongly associated with their intention to remain in that domain. Therefore stressors might be more likely to be associated with intention to leave and be categorized as disengagers, while health-enhancing factors might be more likely to be associated with intention to stay and be categorized as retainers. We, therefore, hypothesize that:
H1: Work interference with personal life (WIPL) has a stronger association with the intention to leave than with the intention to stay in a profession.
H2: Work enhancement of personal life (WEPL) has a stronger association with the intention to stay in than with the intention to leave a profession.
Methods
Context
The focus on midwifery in Canada has contextual relevance that is important for several reasons. First, midwives’ intention to stay in or leave their profession is especially important as the World Health Organization (2020) has predicted a severe shortage of midwives in the next decade. Sustainable midwifery care contributes significantly to the health of birthing parents and their newborns (Ten Hoope-Bender et al., 2014) by providing primary care throughout pregnancy, labour, birth and the postpartum period. Furthermore, compared to physician-led care, midwifery care is positively associated with client satisfaction and fewer labour procedures in low-risk pregnancies (Sutcliffe et al., 2012). Among the OECD countries, Canada, in particular, is experiencing a shortage of midwives with the smallest ratio of registered midwives per number of births (OECD Stat, 2019). While there have been efforts in increasing the supply of licensed midwives, the size of the midwifery workforce in Canada is not increasing proportionately (Canadian Institute for Health Information, 2020), suggesting a problem with the retention of midwives. Furthermore, both nationwide (Zeytinoglu et al. (2020) and province-specific (Stoll & Gallagher, 2019) reports have shown a high intention to leave the profession among practicing midwives in Canada. Researchers from Australia (Harvie et al., 2019; Holland & Tham, 2016; Pugh et al., 2013), the United Kingdom (Hunter et al., 2017), and several other countries in Africa, Europe, and Asia (Jarosova et al., 2016; Sidibé et al., 2018) have reported a similar concern. Second, many midwives in Canada (HakemZadeh et al., 2021; Thiessen et al., 2020), similar to midwives in New Zealand (Hildingsson et al., 2016) and the Netherlands (Warmelink et al., 2015b), practice as independent contractors and are considered self-employed. Even when employed by a hospital or private practice, the decision to leave the profession altogether leads to the loss of midwives’ skills and knowledge from the healthcare sector. Therefore, intention to stay in and intention to leave the profession are particularly important for policymakers and health workforce planning in Canada and globally. Third, while there have been some changes to move away from the 24/7 care models (Wilson, 2019), midwives often have to work long hours. Midwives need to be constantly prepared to attend to their clients with no pre-determined schedule when on call. They also deal with stressors related to medical emergencies and the life and well-being of the birthing parents and their newborns (Dahlen & Caplice, 2014). Midwives experience high burnout levels (Stoll & Gallagher, 2019) and compassion fatigue (Leinweber & Rowe, 2010). At the same time, midwifery is a female-dominated profession. While the imbalance in the division of household demands between genders is decreasing, women still face a greater proportion of household demands (Guppy et al., 2019). As a result, midwives are prone to experiencing high levels of both WIPL and PLIW.
On the other hand, working, in general, provides individuals with income, expands their resources, and, therefore, can enhance their personal lives. Moreover, midwifery is a women-centred primary care discipline based on a certain philosophical foundation rooted in feminism (Davison, 2020) that can potentially result in expanding midwives’ resources (e.g., creating a sense of accomplishment and purpose) and lead to the enhancement of non-work roles. The Canadian midwifery model of care is built on principles of professional autonomy, engaging in a “non-authoritarian and supportive partnership with clients,” and recognizing the right of birthing parents to make informed choices about their care, including about their choice of birthplace (Canadian Association of Midwives, 2015). Because of these professional principles, Hawke (2021) writes that not only are “midwives … often at the forefront of political campaigns for women’s empowerment, overtly advocating for women’s rights and reproductive justice” (p. e.92), but that their day-to-day activities are “acts of everyday rebellion” (p. e.93).
Sample and Procedure
In 2018, we targeted all registered midwives in Canada through an online survey. According to the Canadian Association of Midwives (2018), there were 1690 registered midwives in Canada when this study was conducted. Therefore, a sample all-units data collection method was appropriate for this small population (Salant et al., 1994). The survey was pilot-tested at several Canadian midwifery conferences and was modified based on the comments received. The survey was distributed online and through the listservs of the Canadian Association of Midwives (CAM), the Canadian Midwifery Regulators Council (CMRC), and the provincial and territorial regulatory bodies. The project website, which included a link to the survey, was printed on bookmarks shared with midwives at various midwifery conferences. The study was also advertised through a social media webpage developed for this study on Facebook.
Midwives had the option to complete either the English or the French version of the survey. The study information page disclosed to midwives that the findings would be published in academic journals, presented at conferences, and shared with various stakeholders, including policymakers, to improve midwives’ working conditions. An added incentive was also offered through the option of entering a draw for one of three $50 e-gift cards. We received 720 surveys from registered midwives across Canada and omitted the records that did not answer the items related to the dependent and independent variables included in this paper. Our final sample size was 601, which exceeds the recommended sample size of 322, required to maintain a given level of precision (e.g., with a margin of error of .05, a 95% confidence level and a true population proportion of .5) for a population size of around 2000 (Krejcie & Morgan, 1970).
Our survey collected demographic and human capital characteristics of age, marital status, tenure, prior career, and education completed prior to midwifery-specific education. We further controlled for these characteristics in our analysis. The rationale for the inclusion of these control variables is that previous studies (Chiang & Chang, 2012; Liu et al., 2012), in a comparable female-dominated professional context (nursing), have shown that individuals who are younger, married, and have less experience are more likely to have high intentions to leave their professions. These findings might be due to various reasons, including the social norms of having to disproportionately perform a majority of family-related responsibilities and having less experience to handle various job stressors. Furthermore, there are studies (Flinkman et al., 2013; Troesch & Bauer, 2019) that suggest having completed another professional training or being involved in another career prior to one’s current occupation are associated with lower intention to leave the profession probably due to factors such as having higher general self-efficacy and different perceptions of professional challenges. Age was measured as three categorical variables: ages 23–34, 35–44 (reference group in regressions), and 45 plus (equal 1 for the respective category and 0 otherwise). The marital status variable was categorized as married or living with a partner/common-law (equal to 1) and otherwise (=0, including single, widowed, divorced/separated, and other). The number of years of tenure as a midwife was measured with six binary variables. These variables were as follows (coded equal 1 for the respective category and 0 otherwise): Less than a year, 1–3 years, 4–5 years, 6–10 years (reference category in the regressions), 11–20 years, and 20 plus years. The previous career indicator was collected with the following question: ‘Prior to becoming a midwife, did you have another career?‘, where yes = 1 and no = 0. The question for education (i.e., what post-secondary education did you complete in addition to your midwifery training) was coded as university degree (=1) (e.g., an undergraduate degree (B.A, B.Sc.), some graduate studies (no degree), and a graduate degree (Master’s, Ph.D.)) and otherwise (=0) (e.g., none, college diploma, and some undergraduate studies (no degree)).
Demographic and Human Capital Characteristics of the Respondents.
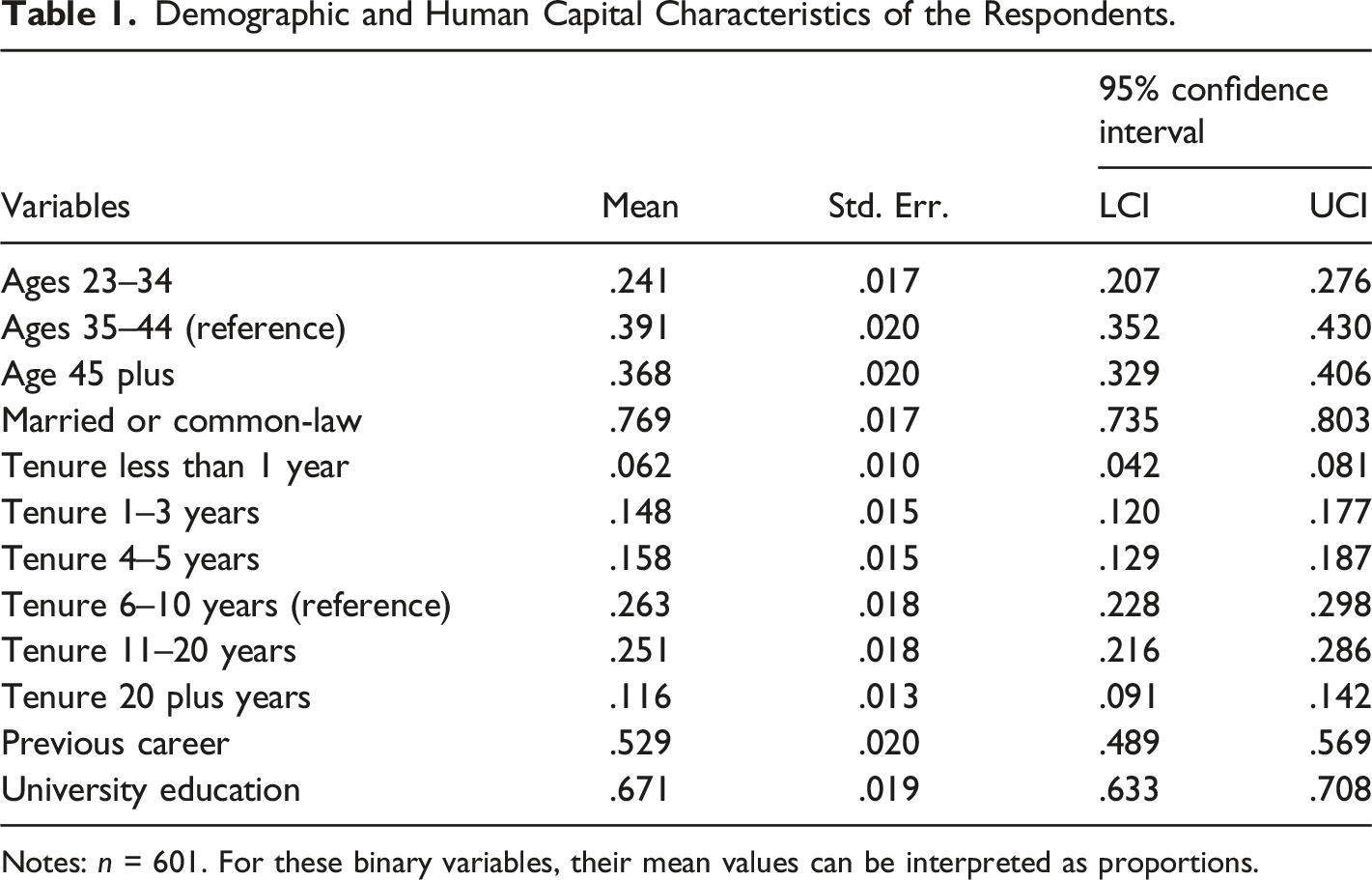
Notes: n = 601. For these binary variables, their mean values can be interpreted as proportions.
Measures
Intention to stay in the profession was measured through a scale developed by Lyons (1971). The wording of the items was slightly modified to match the context. The items included ‘If I were completely free to choose, I would prefer to keep working as a midwife; I would like to stay in this profession for a long time; If I had to quit work for a while (for example, because of personal/family reasons), I would return to this profession.’ Respondents selected their agreement level with each item on a five-point Likert scale from 1 = strongly disagree to 5 = strongly agree. The intention to stay in the profession variable was calculated as the sum of the responses to all three items. The Cronbach α for intention to stay was relatively high at α = .894 (see Table 1 for descriptive statistics). For the intention to stay in the profession single-item measure, the question ‘I would like to stay in this profession for a long time’ was used with the five-point Likert scale. Intention to leave the profession was measured using one item suggested by Fimian et al. (1988): ‘I am seriously considering leaving the midwifery profession in the near future.’ The same approach had been used to measure intention to leave in the context of nursing and midwifery by others (Borkowski et al., 2007).
For capturing midwives’ WIPL, PLIW, WEPL, and PLEW, we used an abridged version of Fisher et al. (2009, p. 444) scales. Items were identified using the Fisher et al. (2009) criteria, such as the exploratory factor analysis (output available upon request) and content analysis of the items. The wordings of the items used were slightly modified in consultation with midwives during the pilot stage to better reflect the context of the study. Others have utilized the Fisher et al. (2009) scales to capture both positive and negative constructs at work and personal life interface (Baumeler et al., 2018; Hirschi et al., 2019). Some of the items included in the survey were: ‘My personal life suffers because of working as a midwife’ (WIPL) (M = 4.06, SD = .82) (see Table 1); ‘My personal life drains me of energy for work’ (PLIW) (M = 2.02, SD = .72); ‘My work gives me the energy to pursue personal activities’ (WEPL) (M = 3.51, SD = .85); ‘My personal life gives me energy for my work’ (PLEW) (M = 2.66, SD = .96). Midwives were asked to select their level of agreement with each statement based on a Likert scale from 1 = strongly disagree to 5 = strongly agree. After removing one item from the PLIW subscale to improve reliability, the Cronbach’s α for the independent variable scales of WIPL, PLIW, WEPL, and PLEW indicated relatively high internal reliability (α = .94, .79, .79, and .75, respectively, see Table 1 diagonal).
Analysis
The analyses include univariate descriptive means, standard deviations, bivariate correlations, and multivariate regressions. The regression Models 1a, 1b, and 2 (a,b) were run separately with the dependent variables intention to stay 3-item scale, intention to stay 1-item measure, and intention to leave 1-item measure, respectively. Models 1a and 2a were run using ordinary least squares, while models 1b and 2b use ordinal logit. The ordered logistic regression (ologit) modelling is an appropriate technique when the variable response categories are ordinal in nature (e.g., five-point scale). Thus, the ologit does not assume a continuous measure, and as such, it accounts for nuanced differences across the categorical scale (e.g., the ologit generates a set of cut-points).
Further, the ologit coefficients can be transformed into odds ratios (e.g., Odds Ratio= OR = exp (β), where the odds ratios compare the probability of events for two groups). The regressions enable a test of our main hypotheses (i.e., the comparison of coefficients in models 1b and 2b). The main purpose for model 1b is to enable an appropriate assessment of the hypotheses by comparing the coefficients with model 2b, where both models 1b and 2b have single-item dependent variables and ordered logistic regression is used, thereby permitting a comparison across similar analyses. For the review of the regression analyses, only models 1a (and 2b) will be commented upon in detail as the results are substantively similar to models 1b (and 2a).
The cross-sectional data enable the investigation of associations and not causal relationships. In the regression analysis, standardized β coefficients are presented. The use of standardized coefficients implies the results can be interpreted in the context of standard deviation units; for example, a one-unit change in an independent variable (i.e., a one standard deviation change) implies that the β represents the change in the dependent variable in standard deviation units. Concerning the independent variables in the model, the correlation matrix’s coefficients suggest that we do not have any multicollinearity concerns (e.g., none of the independent variable correlations are greater than r = .59, see Table 1). For all of the statistical analyses, Stata SE was used.
Results
Means, Standard Deviations, Correlations, and Scale Reliabilities.
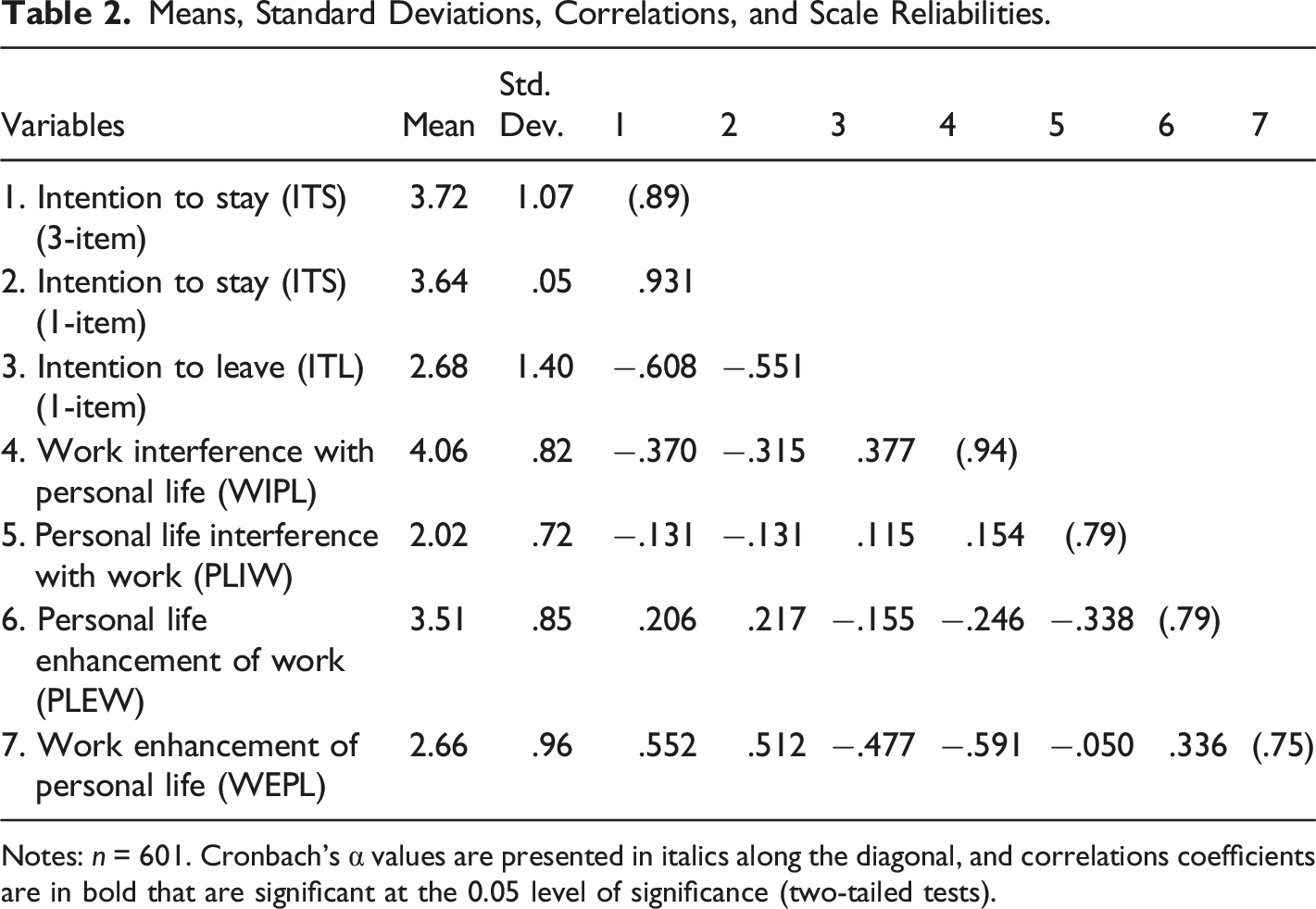
Notes: n = 601. Cronbach’s α values are presented in italics along the diagonal, and correlations coefficients are in bold that are significant at the 0.05 level of significance (two-tailed tests).
Single-item measures have been used to measure both the intention to stay and intention to leave concepts. As a result, in terms of discriminant validity, only the distinctiveness of the constructs can be accessed (using correlation coefficients), and not the degree to which measured constructs are capturing what they are supposed to measure and not another construct, because multi-item measures were not used (i.e., if multi-item measures were used then a confirmatory factor analysis could be used to assess discriminant validity with a focus on cross-loadings). Thus, correlation coefficients become the most appropriate empirical analysis to assess the distinctiveness of these single-item measures. Commonly, correlations are used with a cut-off threshold to assess the distinctiveness of the constructs. An absolute threshold would imply that any correlation less than 1 (or near) implies a difference, while prior literature has identified .85 as a cut-off that balances Type I and Type II errors with the acknowledgement that .9 or greater indicates a similarity of constructs problem and .8 a lack of a problem (Rönkkö & Cho, 2020). The intention to stay 3-item and 1-item measure correlations with the 1-item measure of intention to leave reported above are substantively below these thresholds.
Intention to Stay and Intention to Leave Regression Models.
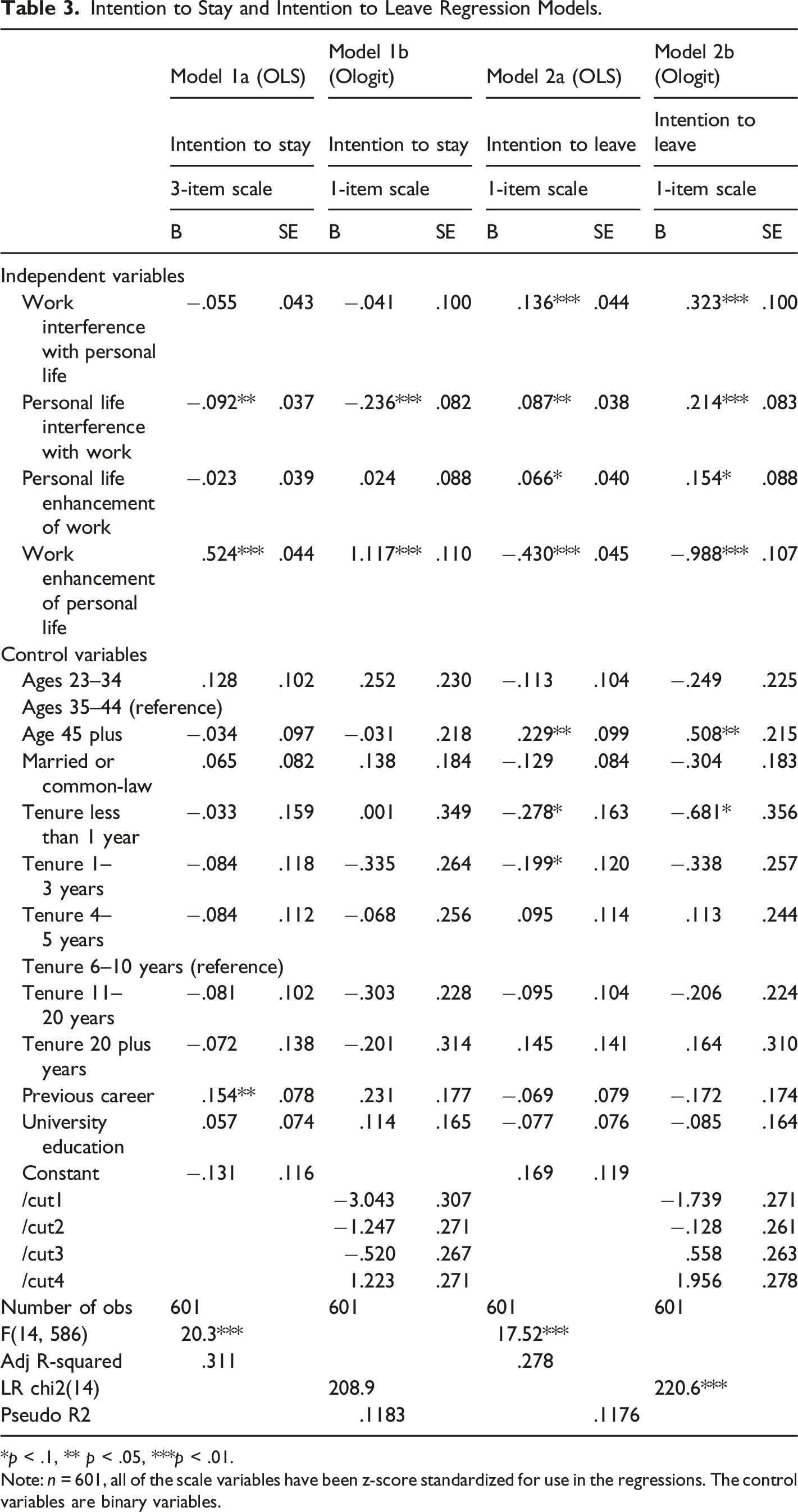
*p < .1, ** p < .05, ***p < .01.
Note: n = 601, all of the scale variables have been z-score standardized for use in the regressions. The control variables are binary variables.
For the intention to stay model 1a, there are three statistically significant variables PLIW (β = −.09, p = .013), WEPL (β = .52, p < .001), and previous career (β = .15, p = .048); while for the intention to leave model 2b, the four main independent variables (WIPL (β = .32, p = .001), PLIW (β = .21, p = .010), PLEW (β = .15, p = .079), and WEPL (β = .99, p = .000)) are statistically significant, in addition to age 45 plus, married/common-law status, and tenure less than 1 year. It is interesting to note that for both models (1a and 2b), the variable WEPL has the most substantive coefficients increasing the intention to stay by .52 standard deviations and decreasing the intention to leave by −.99 (Odds Ratio = exp (-.99) = .37), respectively.
Concerning the hypotheses, H1 was supported at the 5% level of significance (work interference with personal life (WIPL) has a stronger association with the intention to leave the profession than to stay), using a chi2 test, comparing models 1b and 2b, and adjusting for the direction of the coefficient (chi2 (1) = 6.59, p = .0102). For Hypothesis 2, even though the model 1b WEPL coefficient was greater in magnitude than model 2b, it was not statistically significantly greater at the 5% level of significance (chi2 (1) = 1.15, p = .2831), indicating no support for work enhancement of personal life (WEPL) having a stronger association with the intention to stay than to leave.
Discussion
This study attempted to show that different work and personal life interface constructs might be differentially associated with intention to stay in or leave a profession. Evidence on the effect of a factor on the separate concepts of intention to stay and intention to leave can aid stakeholders in developing human resource management policies and practices that support workers within occupations where retention is essential for avoiding shortages. Thus, as noted in the introduction of this article, the contribution to the literature is four-fold: (1) a focus on occupational level intentions; (2) conceptual distinction between intention to stay and intention to leave; (3) a unique sample of midwife healthcare workers in Canada; and (4) the application of a novel typology of intention determinants.
We focused on midwives as they top the list of scarce health care professionals globally (World Health Organization, 2020) and also in Canada (OECD Stat, 2019). Therefore, understanding midwives’ intention to stay in or leave the profession is critical to developing effective interventions for managing Canada’s health workforce. Informed by the job demands-resources (JDR) model (Bakker & Demerouti, 2007) (with extensions informed by role strain theory (Goode, 1960) and expansion theory (Marks, 1977)) and the salutogenic theory (Antonovsky, 1979), and through online surveys, we captured midwives’ both negative (work interference with personal life and personal life interference with work) and positive (work enhancement of personal life and personal life enhancement of work) experiences at the interface of work and personal life. Studying these constructs is particularly important in the context of midwifery as a female-dominated and women-centred profession.
We suggested that interference constructs can be categorized as stressors and enhancement constructs as generalized resistance resources based on the job demands-resources model (Bakker & Demerouti, 2007) and the salutogenic theory (Antonovsky, 1979). We then hypothesized that the extent to which one considers their profession a source of stress and a risk factor (i.e., factors to be avoided) has a stronger association with their intention to leave their profession than their intention to stay in their profession. This hypothesis was supported based on our data and analysis, suggesting that interventions focused on reducing midwives’ work interference with their personal lives might be more effective in reducing their intention to leave rather than increasing their intention to stay in the profession. We also hypothesized that the extent to which one perceives their profession as a source of energy and enhancing their lives (i.e., factors to be sought after) has a stronger association with their intention to stay in their profession than with their intention to leave their profession. This hypothesis, however, was not supported. Our analysis demonstrated that work enhancement of personal life has the most substantive coefficient value compared to the other constructs studied at the interface of work and personal life, with both intentions to stay in and leave.
Similar to all studies, this study has several limitations. First, the data used for this study are cross-sectional, implying that the results are associative and not causal. Second, the study focuses on a single occupation in Canada which provides insight into understanding outcomes for this occupation but may not be generalizable to other occupations and jurisdictions. Third, the outcomes of focus were intention to stay and leave, which are work-related outcomes, and as such personal life-related outcomes were not collected, preventing a more comprehensive exploration of outcomes. Given these limitations, future research can address these issues by collecting longitudinal data, expanding the target population focus, and/or expanding the topic area focus to personal life outcomes.
Our overarching contribution to the work-life interface and turnover literature is providing evidence for the differential relationships between work-life interface constructs and intention to stay or intention to leave. We demonstrated that work interference with personal life has a significantly stronger association with intention to leave the profession than with intention to stay. This contribution is also made in the context of expanding the application of the salutogenic theory by arguing that at the interface of work and personal life, health-enhancing factors are more strongly associated with someone’s intention to stay. In contrast, risk factors and stressors are more strongly associated with someone’s intention to leave. While only the hypothesis related to a risk factor was supported, this opens an interesting avenue for future research using the salutogenic theory.
It is not uncommon for investigations of the interface of work and personal life to focus solely on the negative experiences of work interference with personal life and personal life interference with work. However, our study demonstrated that work enhancement of personal life, which is among the positive experiences at the work and personal life interface, is a critical determinant of intention to stay and intention to leave as it showed a stronger association with both intention to leave and intention to stay compared to the negative experiences. Therefore, studies that only include the negative work-life interface experiences in terms of their association with work or personal life domain outcomes paint an incomplete picture. Research on what factors increase the personal life-enhancing capacity of work and how they can influence attitudes, behaviours, and emotions can be particularly insightful. Further research can identify this profession’s personal life-enhancing capacities, such as midwifery, which is a calling for some and an important part of their identity (Bloxsome et al., 2020).
As noted in the introduction, this study contributes to our understanding of how to map the positive and negative sides of the interface of work and personal life on Cho et al.‘s (2009) typology of determinants of intention to stay and intention to leave. The findings show that among the work-personal life interface constructs, work enhancement of personal life of midwives has the strongest association with both intention to stay in and intention to leave the midwifery profession. This substantiveness finding (in contrast to no support for H2) suggests that work enhancement of personal life is the most critical among the work personal life interface constructs according to Cho et al.‘s (2009) typology, where critical was defined as a factor that impacts both intention to stay and leave outcomes. However, work interference with personal life has a stronger association with midwives’ intention to leave the profession than their intention to stay, and as such, this factor would be classified as a disengager (i.e., a factor that influences intention to leave but not stay) (Cho et al., 2009, p. 375). As we face a global shortage of midwives, it is critically important to design and implement effective interventions to reduce the risk of turnover and increase midwives’ retention in their profession. As such, factors that act as retainers (i.e., impact intention to stay but not intention to leave) should be emphasized in HR practices, while neutrals (i.e., factors that neither impact intention to stay or leave) should be identified so that efforts are not wasted or in vain.
One of the practical implications of this study is that for influencing both intention to stay in or leave the profession, potentially the most effective interventions are those that can increase the enhancing effects of work on personal life. For those healthcare providers employed by clinics, hospitals, or other organizations, policies such as wellness programs or healthcare coverage that extend benefits to employees’ families can help increase work enhancement of personal life (Russo & Buonocore, 2012). However, there are limited suggestions on work-personal life-enhancing interventions from research or professional bodies for midwives, particularly when they are independent contractors or self-employed. Increasing one’s monetary compensation, billed through insurance plans, is an intervention that decreases work interference with personal life by increasing one’s earning power so that with fewer work hours, or fewer caseloads for some midwives, one can still meet earnings goals. However, better pay can also enhance one’s personal life by expanding financial resources that enable individuals to allocate them based on their needs (Grawitch et al., 2010). For example, midwives would be able to hire help for childcare, household chores, and other personal life-related demands with more expendable income. It should be noted that in 2020, the Human Rights Tribunal of Ontario ordered a retroactive pay adjustment for midwives as well as “compensation for injury to dignity, feelings, and self-respect” due to decades-long effects of gender discrimination on midwives’ compensation (Association of Ontario Midwives v. Ontario (Health and Long-Term Care), 2020). The decision identified midwives as “sex-segregated workers.” It concluded that the methods of determining midwives’ compensation should include a gender analysis where the overlaps in the scope of practice of midwives and historically male professions of family physicians and obstetricians should be taken into consideration (Association of Ontario Midwives v. Ontario (Health and Long-Term Care), 2020).
Research also suggests that increasing the intrinsic satisfaction from performing the job itself is positively associated with work enhancement of personal life (Baral & Bhargava, 2010). While the relationship between intrinsic job satisfaction and work enhancement of personal life was not empirically tested in this paper, research (Warmelink et al., 2015a) recommends that enabling midwives to focus on the rewarding aspects of their profession, such as direct interaction with clients and collaboration with supportive co-workers rather than on administrative and non-client related tasks, can help with this regard.
For preventing midwives from wanting to leave the profession, interventions for decreasing the interference of work with the personal lives of midwives can be helpful. These interventions can include allocating days off each week, implementation of policies that restrict consecutive hours of contact with clients (Fereday & Oster, 2010), and sharing the caseload of clients among a team of midwives or between midwives and other primary care providers in the community (Malott et al., 2012; Wilson, 2019).
Footnotes
Acknowledgments
We would like to thank all Canadian midwives who completed our surveys and shared their experiences and knowledge with us. We would also like to thank the research advisory committee of this project (Natalie Beauchamp, Briar Hill Midwives; Barbara Borland, College of Midwives of Ontario; Ivy Bourgeault, University of Ottawa; Naomi Brooks, Rankin Inlet Birthing Centre; Eby Heller, Canadian Association of Midwives; Karyn Kaufman, McMaster University; Melissa Langlais, IWK Community Midwives; Lorna McRae, Access Midwifery; Caroline Paquet, Université du Québec à Trois-Rivières; Kris Robinson, Canadian Midwifery Regulators Council; Kellie Thiessen, University of Manitoba; Rhea Wilson, Burlington & Area Midwives Inc.) for sharing their expertise and knowledge. Furthermore, we would like to thank Jennifer Plenderleith, the research coordinator of our project, for her contributions to survey preparation, ethics approval applications, data collection, and data management.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the Canadian Institutes of Health Research (CIHR) (Funding Reference Number: MOP – 142286). CIHR had no role in the conceptualization, execution, or writing of this study.
Authors’ Contributions
Conceptualized and original draft preparation: [Farimah HakemZadeh and James Chowhan]; Project conceptualization, survey design and funding acquisition: [Isik Zeytinoglu, Elena Neiterman, Farimah HakemZadeh, Johanna Geraci, and Derek Lobb]; Leadership and research activity planning and execution: [Isik Zeytinoglu and Derek Lobb]. Assistance in research activity planning and execution: [Farimah HakemZadeh, Elena Neiterman, and Johanna Geraci]; Data analysis and interpretation of results: [James Chowhan and Farimah HakemZadeh]. All authors contributed to revisions of various earlier drafts and read and approved the final manuscript.
Data Availability
The dataset this paper uses is the original data collected and owned by Drs. Zeytinoglu, HakemZadeh, Neiterman and Lobb. This data can be made available after the owners have completed using it for their submissions (journal articles and other media outputs).
Code Availability
The statistical analysis code and output that this paper is based on can be available for review, from the corresponding author, upon request.
Ethics Approval

| Site | REB Protocol # | Renewal Date |
| McMaster University | 1737 | 19-Apr-20 |
| University of Waterloo | ORE #: 21613 | 17-Aug-20 |
| York University | 2019-353 | 03-Oct-20 |
Inform Consent
Respondents provided consent prior to completing the online survey. They had the opportunity to review the letter of information and to voluntarily agree or not agree to their participation in the study. Responses from those who answered yes to the following question were included in the data and analysis:
Having read the above, I understand that by clicking the “YES” button below, I agree to take part in this study under the terms and conditions outlined in the accompanying letter of information. (Yes, I agree to participate or No, I do not agree to participate)