
Abstract
Little is known about abortion and contraception policy in prisons in Canada. The aim of this study was to determine policies governing access to abortion and contraception in prisons in Canada. Between 2022 and 2023, we sent freedom of information requests to each province and territory and to the federal government of Canada, requesting any information with respect to policies governing abortion and contraception in prisons and jails. Our review identified only one outdated policy pertaining to abortion access, and no policies governing hormonal contraception. The lack of proactive policy to assert access to commonly required services threatens reproductive autonomy.
Introduction
Women and gender diverse people are the fastest growing population in prisons in Canada, with the population increasing to 39% between 2013 and 2018 (Malakieh, 2019). However, institutions of incarceration are often ill-equipped to address gendered needs, including health services. In Canada, most prisoners are in custody in provincial/territorial facilities (Paynter et al., 2020), where the majority are held in pretrial detention. Most incarcerated women are of reproductive age, and Indigenous people, Black people, 2SLGTBQIA + people, people with disabilities, and other marginalized groups experience disproportionately high rates of incarceration.
There is evidence people in prison have higher rates of fertility than the general public, and approximately 4% may be pregnant on admission to custody (Liauw et al., 2016). Challenges experienced by pregnant people in prison include the stress of surveillance, unhygienic environments, inadequate nutrition, lack of access to over-the-counter medications and vitamins, and poor access to prenatal care (Carter Ramirez et al., 2020a). Liauw et al. (2016) found people in prison have much higher rates of lifetime experience of abortion (57%) compared to the general public (approximately 33%, Norman, 2012). Incarcerated people report delays and denial of reproductive care (Liauw et al., 2021; Paynter et al., 2023) and barriers to health information (Liauw et al., 2021). Having experienced incarceration before or during pregnancy is associated with preterm birth and babies of low birth weight and small for gestational age (Carter Ramirez et al., 2020b). Further, limited access to health care and health information prevents incarcerated people from making informed reproductive health choices.
Our recent scoping review of international research addressing contraception and abortion among people in prison (Paynter et al., 2022) found barriers to care include lack of onsite access to options, experience of contraceptive coercion by health care professionals, out-of-pocket financial costs, and periods in custody that caused disruptions to medical coverage and insurance status. US researchers have found rates of abortion vary considerably between jurisdictions, indicative of unequal access based on where an incarcerated person is located (Kirstein et al., 2023; Sufrin et al., 2021).
In Canada, abortion services were completely decriminalized in 1988 and are publicly funded with few exceptions. There are no limitations in criminal law with respect to gestational duration, mandatory waiting times, or parental consent requirements for abortion. Self-referral for care is available in all provinces and territories. In 2015, Health Canada first approved mifepristone for medication abortion, and it became available in 2017 as a publicly funded service with primary care providers including family doctors and nurse practitioners authorized to prescribe (Dunn & Brooks, 2018). Uptake of medication abortion among the general population has been swift, with procedural abortion falling from 96% of care in 2016 to 66% of care in 2019 (Renner et al., 2022). The introduction of mifepristone also prompted significant growth in the abortion provider workforce: the number of abortion providers rose four-fold from 2019 to 2021 (Dunn et al., 2022; Renner et al., 2023; Schummers et al., 2022). With respect to contraception, the contraceptive implant was approved by Health Canada in 2020, improving options for long-activating reversible contraception (Lao & Connolly, 2020). In Spring 2023, British Columbia became the first province to provide universal public funding for contraception (Government of British Columbia, 2023).
Despite decriminalization, recent drug approvals, self-referral and public funding, and barriers to abortion and contraception persist. Patients lack information about options, face difficulties navigating services, and encounter stigma and shame. The procedures and policies in prison settings may exacerbate these challenges. For instance, our team determined the geographic isolation of Canada's prison can force prisoners to travel up to 700 km for a procedural abortion (Paynter & Heggie, 2023). Judgmental attitudes and stigma among prison staff and health care providers may result in health care underutilization and poor health (Kouyoumdjian et al., 2016). Prisoners experience frequent violations of privacy and confidentiality when they seek health services, which may be particularly discouraging in the context of seeking stigmatized sexual and reproductive health services (Paynter et al., 2022; Pont et al., 2012).
Policy Environment
At international, federal, and provincial/territorial levels, there are laws and standards for the treatment of prisoners which can be interpreted as supportive of prisoner access to abortion and contraception while in custody. According to the World Health Organization List of Essential Medicines (2023), the “list of minimum medicine needs for a basic health-care system, listing the most efficacious, safe and cost-effective medicines for priority conditions,” includes oral, injectable, implantable, and intravaginal hormonal contraceptives, interuterine devices, and mifepristone-misoprostol for medication abortion. The United Nations Minimum Standards for the Treatment of Women Prisoners (2011), known as the Bangkok Rules, stipulates: “Gender-specific health-care services at least equivalent to those available in the community shall be provided to women prisoners.”
Section 86 of the federal Corrections and Conditional Release Act (1992) specifies that Correctional Service Canada will provide “essential health care” and “reasonable access to nonessential health care” and that this care “shall conform to professionally accepted standards.” The CRC drug formulary, a list of medications approved for use by federal prisoners, includes oral, injectable, implantable, and intravaginal hormonal contraceptives, interuterine devices, and mifepristone-misoprostol for medication abortion. Section 76 of the CCRA, “Programs for female offenders,” specifies that the CSC “shall (a) provide programs designed particularly to address the needs of female offenders and (b) consult regularly about programs for female offenders with (i) appropriate women's groups and (ii) other appropriate persons and groups with expertise on, and experience in working with, female offenders.” Furthermore, the CCRA states: “Correctional policies, programs, and practices [will] respect gender, ethnic, cultural, religious, and linguistic differences, sexual orientation, and gender identity.”
Within provincial/territorial corrections legislation, there is variable acknowledgment of gendered needs. Gender, female, women, and woman do not appear at all in the PEI Correctional Services Act, the NB Corrections Act. The Nova Scotia Corrections Act includes gender-specific instructions with respect to the strip searching of female prisoners and that female prisoners be incarcerated in separate accommodations. Both the Newfoundland and Labrador Corrections Act state that “policies, programs, and practices will respect age, gender, sexual orientation, ethnic, cultural, religious, and linguistic differences and will be responsive to the particular needs of women,” that, “a superintendent, of a correctional facility that houses female inmates, must have the knowledge, experience, skill, and education necessary to appreciate and understand the unique challenges and needs faced by the female inmates,” and finally, that “the director shall coordinate and encourage wherever possible … specific programming and services to … provide for the particular needs of female offenders.”
There may be regulations within correctional services that are also supportive of access to contraception and abortion. For example, the NS Correctional Health Services Patient and Family Guide states: “Please note on your health request form if you have specific concerns or requests related to trans, gender diverse, or women's health. For example, a request to be seen by a health care provider of a specific sex or gender.”
Although common, pregnancy prevention and termination are highly stigmatized services. Without specific policies addressing pregnancy prevention and termination for women and gender diverse prisoners, prison staff, health care providers, and prisoners themselves may not be aware of their rights to care.
Method
From late Fall 2022 to early Spring 2023, in collaboration with a pro bono lawyer and law student, we conducted Access to Information and Privacy (ATIP) and Freedom of Information and Protection of Privacy (FOIPOP) requests to the federal government and all the provincial and territorial governments in Canada to determine what prison policies existed with respect to pregnancy prevention and termination. The request stipulated: I request any and all information regarding Correctional Services Canada policies governing pregnancy (including childbirth), pregnancy prevention (i.e., contraceptives including implants, intrauterine devices, condoms, oral contraceptives, patches, rings, etc.), and pregnancy termination (i.e., abortion). Furthermore, I request any and all information concerning the kinds of contraception and abortion medications approved for prescription and use within Canadian correctional facilities, as well as information regarding the volume of contraception prescriptions and abortions provided to people in Canadian correctional facilities, by year, for the past ten years.
Responses from each department were extracted and entered verbatim into an Excel spreadsheet. Data was organized by ministry or department (health or justice), by type of content (policy, letter, drug formulary, and other), and whether it addressed abortion, contraception, or another aspect of pregnancy.
As two jurisdictions sent their entire drug formularies as documentation, we decided to also review the contents of the formulary in each jurisdiction. These are all available publicly online. We extracted whether mifepristone-misoprostol (medication abortion) is mentioned as well as the appearance of emergency contraception, contraceptive ring, pills, injection, implant, and hormonal intrauterine device (IUD). While inclusion does not mean it would be readily available to prisoners, exclusion is indicative of a clear barrier to access.
Results
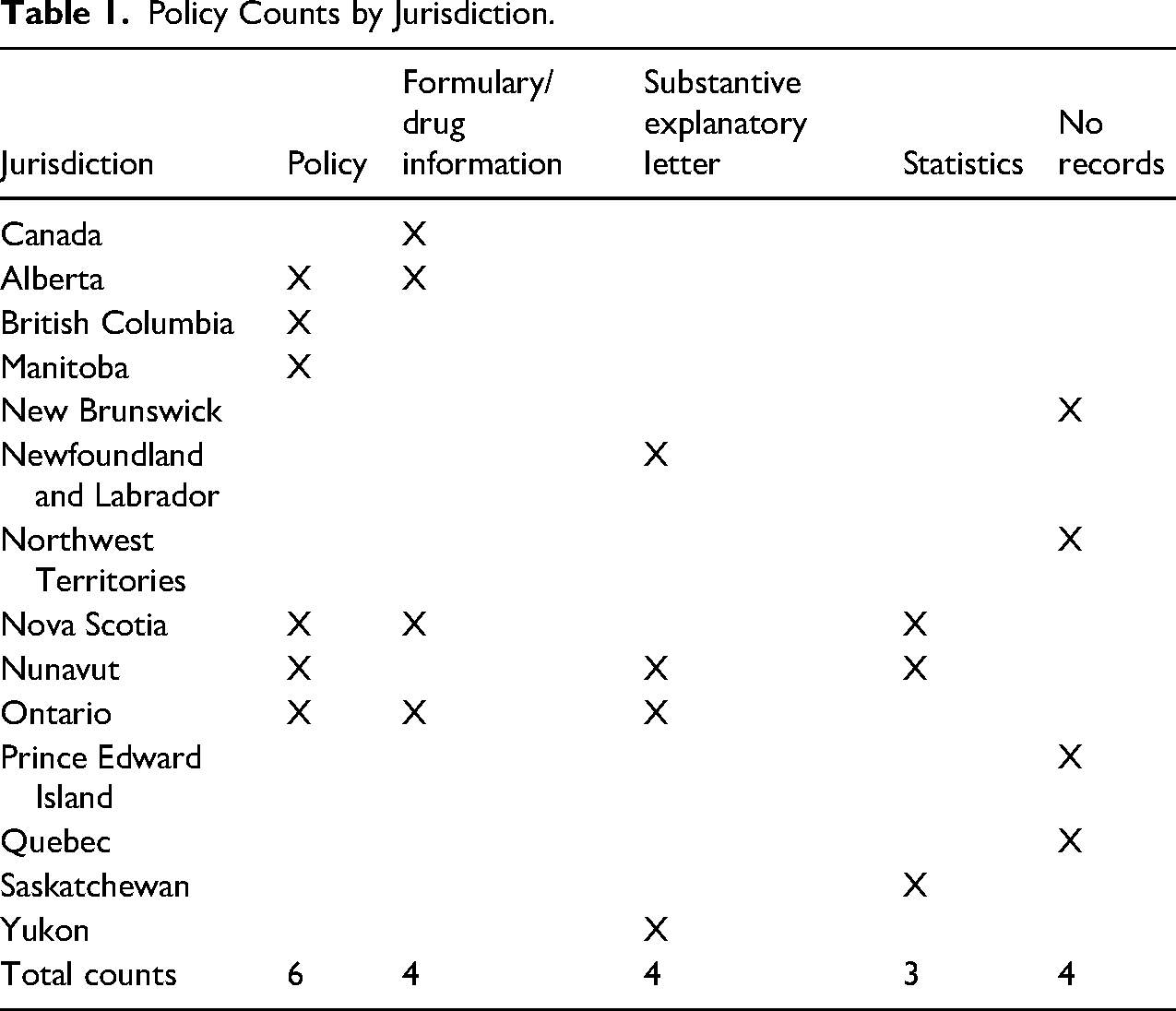
Of the 14 jurisdictions we contacted, four responded that they had nothing to provide: New Brunswick, the Northwest Territories, Prince Edward Island, and Quebec. The provincial health authority of Newfoundland and Labrador and the territorial justice department in the Yukon provided letters explaining their practices and procedures with respect to abortion and contraception, although a policy was not available. Explanatory information was also provided by Nunavut and Ontario in their letters. Six jurisdictions sent policy documents on various topics: two provincial health departments (Alberta and Nova Scotia), three provincial justice departments (British Columbia, Manitoba, and Ontario), and one territorial justice department (Nunavut). As will be discussed, these did not necessarily address our questions pertaining to abortion and contraception. We received drug formularies or information about approved or prescribed medications from the federal Correctional Services of Canada, Ontario, Alberta, and Nova Scotia. Two jurisdictions sent information about the number of contraception prescriptions and/or abortions from 2013 to 2023 (Nunavut and Nova Scotia; see Table 1 and Figure 1).
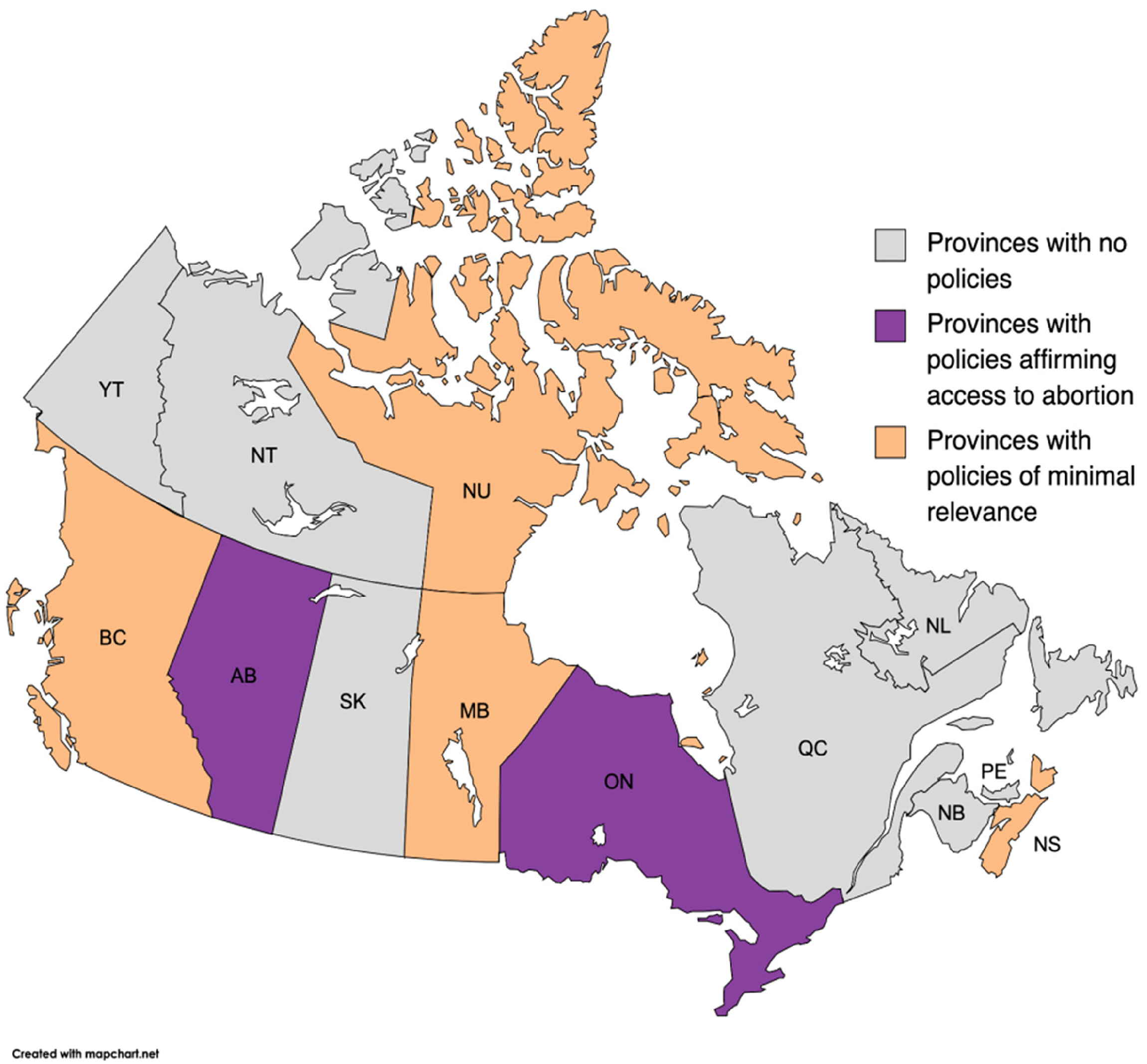
Map of policy availability by jurisdiction.
Policy Counts by Jurisdiction.
In addition, we received information pertaining to the Mother-Child Program at Alouette Correctional Centre for Women in British Columbia, about Communicable Diseases in Manitoba; a Contraceptive Learning module from Nova Scotia Health, the British Columbia business plan to transfer responsibility for correctional health services from a private contractor to the provincial, and a Canadian HIV/AIDS Legal Network publication regarding HIV and hepatitis C prevention for prisoners in Canada.
Policies Addressing Abortion
Alberta
Two provinces sent us policies addressing abortion. Alberta Health Services “Termination of Pregnancy policy PS-92,” dated 2017, applies province-wide and is not specific to prisoners. Its stated objective is “to provide a policy for the safe performance of surgical and medical termination of pregnancy and to provide direction concerning respectful care of patients (women) who seek pregnancy termination.” It states: The decision to terminate is the patient's and the degree of involvement of her family is for her alone to decide. During this difficult time, health care professionals will strive to provide care that is reflective of compassion and dignity and acknowledges the diversity of opinions concerning pregnancy termination. Support for patients making a decision about ending a pregnancy will be based upon assessment of the wishes and needs of the patient. Due recognition should be given to personal, cultural, racial, ethnic and religious differences and sensitivities regarding this decision, but this recognition must not extend to avoiding any of the provisions of this policy, nor to any action in contravention of Canadian Law. Diagnosis of pregnancy and appropriate management should be determined early because the risks and complications of termination of pregnancy are lowest in early pregnancy. There should be timely access to the provision of termination of pregnancy services. The safety and effectiveness of surgical and medical termination of pregnancy procedures are affected by the fetal gestational age. Termination of pregnancy should, in general, occur prior to 21 weeks and zero (0) days gestational age… Pregnancies greater than 21 weeks and zero (0) days of gestation require additional consideration and action … [and] will be offered and provided in circumstances where at least one of the criteria below are met.
Section 3.1 of the policy specifies: “For hospitals and accredited non-hospital surgical facilities under the jurisdiction of Alberta Health Services, only physicians who have appropriate privileges shall perform termination of pregnancy.” Section 6.3 continues: “The termination of pregnancy procedure must only be performed in an acute care hospital and by a physician.”
With respect to belief-based denial of care, the policy stipulates care providers “should treat the patient with respect, compassion, dignity, and fairness. Physicians providing care for patients choosing termination of pregnancy, their personal moral and religious beliefs notwithstanding, shall at all times act in the best interest of their patient,” and “No health professional who provides direct patient care shall be compelled to participate in pregnancy termination … this exclusion does not apply to necessary participation in the care of patients suffering emergent post-procedure maternal complications” (Section 4.2–4.3).
Ontario
Ontario is the only jurisdiction with a policy specifically addressing abortion in the context of incarceration. The Ontario Ministry of Correctional Services Health Care Services Policy and Procedures “HCS 01 22 02: Health Care Services for Women” (1999), under the subsection “Elective Surgical Interruption of Pregnancy” states: “Decisions relating to female inmates who wish to terminate their pregnancy are regulated by provincial and federal law.” The policy continues: “A female inmate wishing to terminate her pregnancy while incarcerated shall be referred to the institution physician. The physician shall counsel the patient and discuss the options at length. Referral for further assessment shall be made as indicated,” and “Confidentiality of health care counseling and interventions shall be maintained at all times.”
There is a section addressing continuation of pregnancy against medical advice: If the institution physician or community specialist believes the continuation of a pregnancy would likely endanger the health or life of the inmate, this will be discussed with the inmate, options provided, and arrangements made after obtaining informed, signed consent. Should the woman refuse to accept the recommendation to terminate the pregnancy, the senior medical consultant shall be advised and all such communication shall be documented in the health file… The health care file shall reflect the counseling provided to each inmate considering an abortion, as well as any other medically and legally required steps taken by staff.
With respect to belief-based denial of care, the policy explains: “Where an employee's religious beliefs are in conflict with facilitating an abortion, such beliefs shall be taken into consideration. Where the health care of the inmate necessitates abortion, the employee may be compelled to facilitate the treatment in the course of his/her duties.”
With respect to location, the policy states: “Should surgery be indicated, regular procedures for the arrangement of a medical temporary absence shall be followed. Abortions shall not be performed in any ministry [of corrections] facility.” It continues: “An inmate may request access to abortion services from a private abortion clinic. Payment for the procedure shall be assumed by the inmate.” And finally: “Where possible, unescorted medical temporary absence should be considered to facilitate access to private clinics. Where an unescorted medical temporary absence is not feasible, the health care staff shall consult the senior medical consultant.”
Policies Addressing Pregnancy
British Columbia
British Columbia Corrections provided their policy “9.24 Pregnant Inmates (Revised May 15). The policy begins: “BC Corrections recognizes the special bond between mother and child” and goes on to describe how the department supports access to prenatal care, arrangements for delivery, and how a “release plan for the infant” will be assessed by the Ministry of Children and Family Development (child welfare). There is no mention of spontaneous or therapeutic abortion care, postpartum contraception, or pregnancy prevention more generally.
Manitoba
Manitoba Community Safety Division provided their Pregnant Inmates Policy (May 2021). It states that pregnant inmates are provided with specialized counseling and prenatal care, and every effort is made to ensure they deliver in hospital. This policy also recognizes “the special bond between mother and child.” Notably, the policy indicates that pregnant prisoners are not to be shackled and are to be “front-cuffed.” There is no mention of spontaneous or therapeutic abortion care, postpartum contraception, or pregnancy prevention more generally.
Nunavut
The Nunavut Women's Correctional Centre Standing Orders Chapter 9.0 Admission and Discharge includes the text: “Upon admission offenders shall be assessed for the presence of health issues requiring nursing care or referral to a physician including pregnancy.” In their response letter (February 13, 2023), Nunavut indicated they did not otherwise have a specific policy pertaining to “pregnancy, family planning, or termination.”
Policies Regarding Contraception
Nova Scotia
No jurisdiction provided a policy pertaining specifically to hormonal contraception for people in prison. Nova Scotia Health provided two provincial policies that authorize registered nurses and licensed practical nurses to provide emergency contraception in emergency rooms and nonurgent community clinics if they have been assessed as competent to do so. Nova Scotia Health also included their Contraception Learning Module (2014), which reads: “RNs may provide one package of oral contraceptives when assessed competent” (p. 3).
Letters
In their response letter, Newfoundland and Labrador's Department of Health indicated: “They prescribe contraceptives as per any community provider. If it is requested by an individual, they prescribe it. They therefore would not have any policies governing that as it is basic, standard practice.” Who constitutes “they” was not specified but is assumed to be institutional prescribers.
The Nunavut Department of Justice response letter by Valerie Inukpuk RN stated: “If they want access to birth control they have the same options as women who are not incarcerated as there are no corrections restrictions on forms or types of family planning” and explained that contraception is covered by the Nunavut Land Claims agreements and the department of corrections (February 13, 2023). Further, in their letter, they explained that while no prescriptions were initiated in custody, existing prescriptions were maintained (February 13, 2023).
The Yukon response letter stated: “If the client chooses to have an abortion—their right to choose is of upmost value to the facility. We offer medical abortions (Medication) depending on the gestation or referral for surgical intervention if needed.” It also included the text: “There is no record of any women inmates having given birth while sentenced or remanded to Whitehorse Correctional Centre. As such, there is no set policy or protocol that deals with such an event in Yukon.”
Ontario's response letter stated that conjugal visits are not available in any of their facilities.
Formularies and Drug Information
We received information about drug coverage from four jurisdictions, including the drug formulary from Correctional Services Canada and Ontario. We then decided to compare the formularies in each of the jurisdictions with respect to what was included as medication abortion and hormonal contraception options. While the inclusion on a formulary does not guarantee access for prisoners, the complete exclusion of a product constitutes a barrier. New Brunswick and Nova Scotia were the only jurisdictions covering all options for modes of hormonal contraception and medication abortion administration, and Alberta was the most restrictive (see Table 2).
Drug Formularies by Jurisdiction.
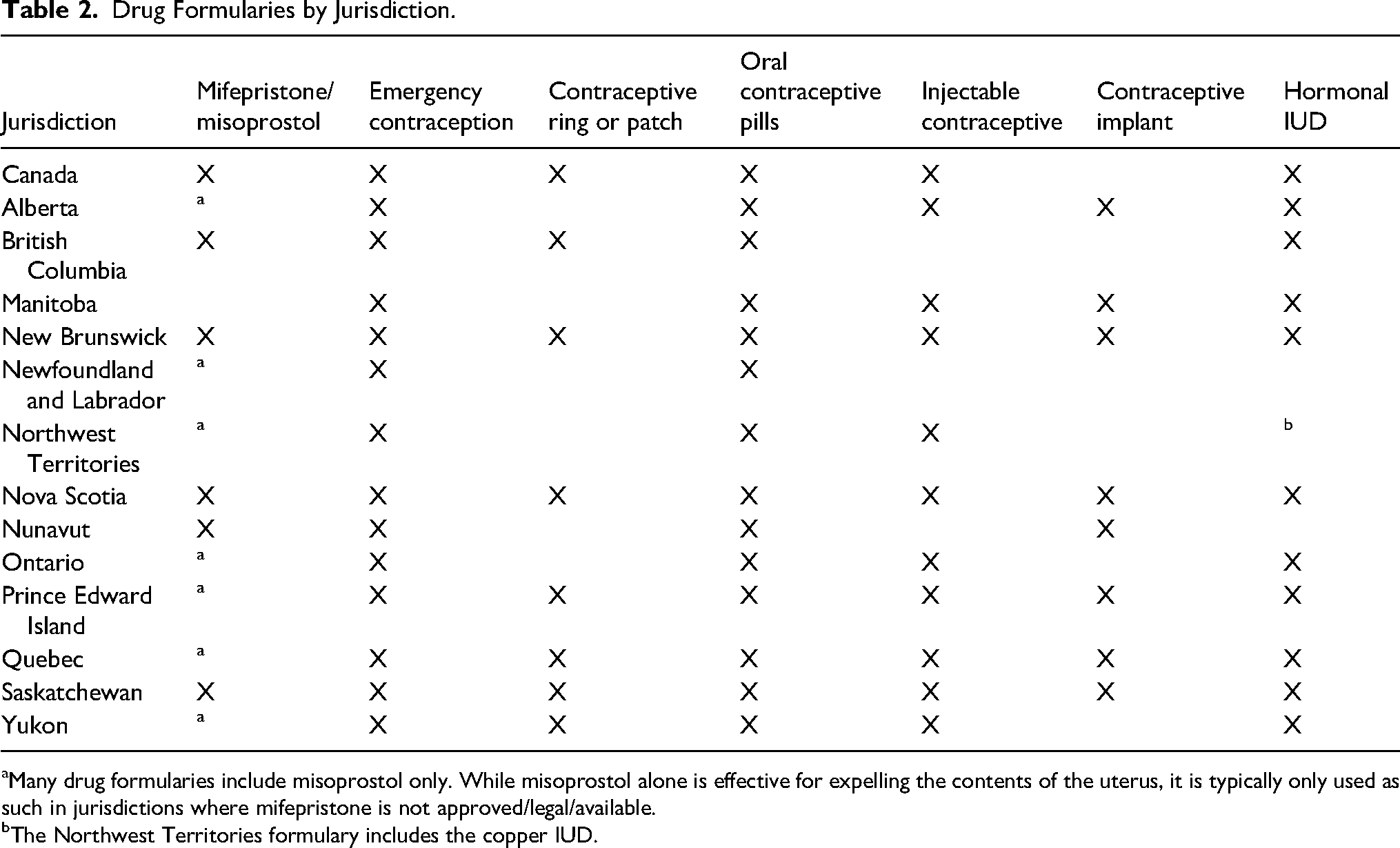
Many drug formularies include misoprostol only. While misoprostol alone is effective for expelling the contents of the uterus, it is typically only used as such in jurisdictions where mifepristone is not approved/legal/available.
The Northwest Territories formulary includes the copper IUD.
Statistics
Abortion
Nunavut indicated that from 2013 to 2023, 127 women were admitted to custody, of whom 10 (8%) were pregnant. During that 10-year period, one person gave birth while in custody, and two experienced spontaneous abortion. None obtained a therapeutic abortion. The Saskatchewan Department of Health indicated that patients had been transferred from correctional facilities to hospitals providing procedural abortion care in each of 2012–2013, 2015–2016, 2016–2017, 2018–2019, and 2019–2020. Exact numbers per year were too small (<5) to be reported.
Contraception
Nunavut indicated that from 2013 to 2023, over which time 127 women had been admitted to custody, the prison issued 10 contraception prescriptions: seven prescriptions for Depo Provera, two for oral contraceptive pills, and one for an intrauterine device. Nova Scotia provided counts of contraception prescriptions from 2013–2014 to 2022–2023, averaging from fewer than five (and hence not reportable) to 18 per year. They did not indicate the total number of prison admissions during this period; however, the unit for women at the Central Nova Scotia Correctional Facility has a capacity for 48 people at a time (Paynter, Bagg & Heggie, 2020; Nova Scotia, 2021). During COVID-19, admissions to custody in Nova Scotia fell drastically, and during each of 2020, 2021, and 2022, there were fewer than five contraception prescriptions. Nova Scotia also indicated that emergency contraception was prescribed to fewer than five clients in total over the 10-year period.
In their response letters, Correctional Services Canada, Alberta, Manitoba, Ontario, and Yukon specifically stated that they do not collect information on the number of prescriptions provided in their facilities.
Discussion
This policy review found a single, significantly outdated policy pertaining to abortion access for people in prisons and no policy governing hormonal contraception in prison. Only two jurisdictions provided counts of abortion obtained by people in prison over the past 10 years, in one (Nunavut), the count was zero; in the other (Saskatchewan), although yearly counts were too low to report, there were instances in each of 5 years. Only two jurisdictions provided counts of hormonal contraception prescriptions. While only a few jurisdictions sent us formularies, when we compared publicly available information regarding formulary inclusions, we found what was included varied considerably. Simply put, this review indicates there are significant differences in reproductive rights protections and health services access depending on where a person is incarcerated. The affirmations for access to gender-specific health care made in the Bangkok Rules are not asserted through correctional policies.
There are no criminal laws governing abortion in Canada, and in all provinces and territories, both procedural and medication abortions are available through self-referral. Nurse practitioners are authorized to provide abortion through medication and, in some settings (e.g., parts of Ontario), midwives may do so under medical directives.
Although not particular to prison contexts, the province-wide abortion policy sent by Alberta is notable for its emphasis on compassion, timely access, and duty to care. It does, however, place emphasis on the gestational duration of 21 weeks as a type of turning point. There is nothing in Canadian law that creates a 21-week limitation. Further, the sole reference to physicians excludes nurse practitioners, who are authorized to prescribe medication abortion across Alberta. We inquired as to the status of this policy and were informed it is currently under review (Personal communication, Alberta Health Services, November 8, 2023).
The very old (1999) Ontario corrections policy pertaining to terminations also affirms duty to provide care, to maintain confidentiality, and that the choice to terminate is the patient's. The insistence that abortions are not “performed” in a correctional facility brings into question how a mifepristone medication abortion would be handled. Although many procedural abortion sites in Ontario are publicly funded, privately owned freestanding clinics unaffiliated with hospitals (Paynter & Heggie, 2023), the policy stipulates prisoners would have to pay to use private facilities. Most interestingly, the policy encourages the use of unescorted temporary absences to allow incarcerated patients to visit the abortion clinic. The use of unescorted temporary absences is, nowadays, very uncommon.
In some ways, the lack of any policy in 12 of the 14 responding jurisdictions is unsurprising and perhaps unalarming: in Canada, abortion is a health service, and there is an argument to be made that unique policies are not required for each individual health service a prisoner may seek to access. However, it must be acknowledged that abortion care is highly stigmatized, and seeking care remains complex and shrouded in secrecy. Although medication abortion is now almost as commonly sought as procedural abortion in Canada (CIHI, 2021), it was only approved 8 years ago and remains poorly understood (Sethi & Park, 2023). Researchers have found over 50% of incarcerated women in Canada have inadequate health literacy (Donelle & Hall, 2016). Lack of access to the Internet and to community health services and support networks prevent incarcerated women from learning about important reproductive health developments. US research has found correctional officers are also underinformed about reproductive services (Pendleton et al., 2020). The logistics of arranging procedural abortion services external to the institution would be daunting, possibly including separate appointments for ultrasound, blood work and the procedure, and significant travel accompanied by at least two correctional officers or sheriffs at all times. But how medication abortion could work in a prison context is questionable. In a federal prison environment, most sentenced prisoners in general population stay in “cottages” with individual, private rooms; it is harder to accept the acceptability of managing abortion in a provincial jail, where prisoners are under constant surveillance and face considerable limitations in access to hygiene products, water, pain relief, and support. Proactive policy and procedures to support seeking services would be valuable.
A lack of policy affirming the right to abortion, in a context where rights to privacy, bodily autonomy, and confidentiality are routinely denied, is a deterrent. Policies like those in BC and Manitoba that immediately associate pregnancy with “a special bond between mother and child” also inherently communicate a lack of access to termination options. Similarly, while several jurisdictions assert prisoners can just request contraceptive prescriptions like any other medication, and no policy is therefore needed, without an affirmative policy, prisoners may feel discouraged from doing so. Furthermore, our comparison of formularies found significant variation in what each jurisdiction includes.
Ontario's letter referred to a policy against conjugal visits. Denying the right to conjugal visits is a surprising response to our query about access to abortion and hormonal contraception. Furthermore, contraception products are useful for menstruation management/amenorrhea for pain relief, anemia prevention, and gender-affirming care, all of which may be highly desired in a carceral context.
The dearth of information about reproductive health in institutions of incarceration in Canada prevents understanding of how incarceration affects the fertility, health in pregnancy and postpartum, and neonatal outcomes of people in prisons and their infants. It is unacceptable for most jurisdictions to simply not collect this information.
Limitations
This policy review is inherently limited to the documents that were returned to us by the jurisdictions. While we aimed for comprehensiveness in the language of our queries, important documents may not have been included.
Conclusion
No jurisdiction in Canada has an up-to-date policy affirming access to either abortion or hormonal contraception. Women are the fastest-growing population in institutions of incarceration in Canada, and lack of proactive policy to assert access to commonly required services and products may create barriers. Such a policy is needed, as is basic data about pregnancy frequency and outcomes among incarcerated people. This policy would support institutions to meet the minimum standards set forth in the Bangkok Rules. Further research is required to understand prisoner experiences of seeking abortion and contraception while incarcerated in federal and provincial/territorial institutions and correctional staff and prison health professionals’ knowledge of abortion methods and pathways to care.
Footnotes
Acknowledgement
The authors would like to thank Susannah Mackenzie-Freeman and Jaime Burnet for their assistance in conducting and submitting information requests.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.