
Abstract
Reproductive coercion (RC) broadly encompasses behaviors that interfere with a person’s reproductive choices, including control over contraception, pregnancy, and pregnancy outcomes, and can pose considerable health risks. However, its full impact on health remains insufficiently understood. This scoping review systematically examined empirical literature on the health consequences of RC published between 2010 and 2024. Following JBI methodology and Preferred Reporting Items of Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR) guidelines, we searched five databases (MEDLINE, CINAHL, Embase, PsycINFO, and Scopus) for peer-reviewed studies reporting on RC and associated health outcomes. Sixty-two studies across 18 countries met inclusion criteria, the majority from high-income settings, revealing adverse effects on reproductive, sexual, and mental health. Most studies focused on pregnancy coercion and contraceptive sabotage perpetrated by male partners. RC was consistently associated with adverse mental health outcomes, including post-traumatic stress disorder, anxiety, and depression. Studies associated RC with an increased risk of unintended pregnancy and sexually transmitted infections. Contraceptive use patterns varied: some studies reported reduced uptake among those experiencing RC, while others described increased use of covert long-acting methods and emergency contraception as protective strategies. Few studies examined physical health outcomes or healthcare utilization following RC. Evidence gaps remain regarding the health consequences of other RC behaviors, including coerced continuation or termination of pregnancy and forced contraception, as well as from low- and middle-income contexts. Clarifying the health consequences linked to current or past experiences of different RC behaviors may support healthcare providers in recognizing and responding to RC, to promote reproductive autonomy and improve health outcomes for RC victim-survivors.
Keywords
Background
Reproductive coercion (RC), situated at the nexus of gender-based violence and sexual and reproductive health (SRH), is a form of abuse that interferes with autonomous reproductive decision-making and negatively impacts overall health and well-being (Grace & Anderson, 2018; Tarzia & Hegarty, 2021). It involves behaviors that restrict or control a person’s reproductive choices, often enacted by intimate partners or family members (Rowlands & Walker, 2019). These behaviors may include pressuring someone to become pregnant, interfering with contraception, or coercing them into continuing or ending a pregnancy. Researchers have commonly examined RC in the context of male intimate partners who use pressure and coercion tactics to cause pregnancy, including sabotaging contraception (Miller et al., 2010). Tarzia & Hegarty (2021) refer to such interpersonal forms of RC as reproductive coercion and abuse.
While most scholarship has conceptualized RC as an interpersonal issue, there has long been discussion about whether it should be understood more broadly to include structural dimensions like policies and practices enacted by institutions and systems that impact reproductive autonomy (Grace & Anderson, 2018; Grace & Fleming, 2016; Tarzia & Hegarty, 2021). More recently, researchers and organizations have explicitly applied RC terminology to structural determinants such as racism, restrictive abortion legislation, and health system policies (Coleman et al., 2023; Graham et al., 2023; Marie Stopes Australia, 2020; Warling et al., 2023), framing these practices within a broader definition of reproductive violence (Laverty & de Vos, 2021). In this review, we adopt an inclusive definition of RC that acknowledges both its interpersonal and structural forms, but recognize them as distinct yet interconnected domains. We consider structural forms of RC where policies, practices, or institutional actions were explicitly described in the evidence by researchers as coercively shaping a person’s reproductive choices, rather than as broader impacts on reproductive autonomy (Upadhyay et al., 2014).
A substantial body of evidence shows that people who experience violence face a significantly higher risk of unintended pregnancies and adverse reproductive health outcomes (Coker, 2007; Moore et al., 2010). Perpetrators of violence often use pregnancy as a means of control (Bacchus et al., 2006), and researchers widely recognize RC as a major contributor to unintended pregnancies (Grace & Anderson, 2018). RC frequently co-occurs with intimate partner violence (IPV) and can lead to long-term adverse physical, mental, sexual, and reproductive health consequences (Grace & Miller, 2023; McCauley et al., 2014; Northridge et al., 2017). However, the diverse ways in which RC manifests across populations, and hidden dynamics within relationships, can obscure its health impacts, making it difficult for healthcare providers to identify and support those affected (Wellington et al., 2021).
Researchers have found that individuals experiencing IPV often access healthcare services more frequently than those who do not, seeking care for injuries and other health-related concerns (Campbell, 2002; Potter et al., 2021). Similarly, individuals experiencing RC are more likely to seek healthcare, particularly for contraception, pregnancy, and abortion-related care (Zachor et al., 2018). This places healthcare providers in a unique position to identify and support those at risk of or experiencing RC. Yet many providers struggle to recognize RC because of its concealed nature, and they often lack the training, support, and resources needed to respond appropriately (Wellington et al., 2021).
Clarifying the health consequences linked to current or past experiences of RC could guide healthcare providers in recognizing and responding to RC. While previous systematic reviews have investigated how pregnancy coercion and contraceptive sabotage are associated with unintended pregnancies (Grace & Anderson, 2018; Grace & Fleming, 2016; Moulton et al., 2021), recent commentaries have only offered broad overviews of RC’s health impacts (Grace & Miller, 2023; Tarzia & Hegarty, 2021). To date, no comprehensive review has mapped the full range of health consequences stemming from the varied and complex behaviors that comprise RC. To address this gap, this study conducted a scoping review to examine evidence on the health consequences of experiencing RC. The lack of consensus on RC definition and measurement posed challenges for applying the stringent inclusion and appraisal criteria required for systematic reviews or meta-analyses (Munn et al., 2018), making a scoping review the most appropriate methodology to map and synthesize the breadth of available evidence on RC health consequences that can inform future research and intervention strategies in healthcare settings.
Methods
This scoping review followed the JBI Methodology for scoping reviews (Peters et al., 2020) and adheres to the Preferred Reporting Items of Systematic Reviews and Meta-Analyses extension for scoping reviews (PRISMA-ScR; Tricco et al., 2018). We published the review protocol to minimize duplication and enhance transparency in the review process (Saldanha et al., 2023). This paper addresses one of the research questions outlined in the protocol: What are the health consequences of experiencing RC?
Eligibility Criteria
The eligibility criteria included original, peer-reviewed articles published in English between January 1, 2010, and June 2, 2024. The year 2010 was selected as it marks the first formal use of the term “reproductive coercion” in academic literature (Miller et al., 2010). We applied no restrictions regarding participant age, gender, country, study context, perpetrator identity, or study design. A broad definition of RC-guided inclusion, encompassing any behavior described in the literature as interfering with a person’s reproductive decision-making. We excluded studies that (a) focused solely on the scientific or biological aspects of reproduction, (b) comprised gray literature, conference abstracts, commentaries, dissertations, book chapters, editorials, or protocols, or (c) discussed sexual coercion and violence without addressing reproductive impacts. A comprehensive justification for the eligibility criteria appears in the published protocol (Saldanha et al., 2023).
Search Strategy
The search strategy used adjacency operators and Boolean logic to link terms related to reproduction with those related to coercion and violence. The detailed search strategy is available in the published protocol. We conducted searches across five databases: Ovid MEDLINE, Embase, Scopus, CINAHL, and PsycINFO. A research librarian supported a pilot search in December 2022. We ran the full search on January 23, 2023, and again on June 2, 2024.
Study Selection
We imported all identified studies into COVIDENCE software, subsequently removing duplicate studies. Two reviewers (SS and DL) independently screened titles, abstracts, and full-text articles for inclusion. A third reviewer (JRB) resolved any conflicts. Due to the high volume of studies retrieved, a forward citation search was not conducted.
Data Extraction and Synthesis
The authors developed a data extraction tool for this review; this tool is available in the published protocol (Saldanha et al., 2023). After piloting the tool on a subset of 12 articles, 1 reviewer (SS) extracted the data and held regular meetings with the research team (JRB, MM, DM) to verify the process and discuss emerging findings. Extracted data included (a) study characteristics (title, author(s), year of publication, aim, methodology, and context), (b) victim-survivor sample characteristics (age, gender, and inclusion criteria), (c) RC victimization characteristics (behaviors, perpetrators, and measurement tool used), and (d) main findings related to health consequences (non-significant and significant quantitative results with p-values <.05 and 95% confidence intervals, qualitative themes and interpretations). We conducted a qualitative content analysis (Hsieh & Shannon, 2005) and present the results in narrative and tabular formats. We extracted text describing the impact of RC on any health-related outcome from each article. Using an inductive, iterative approach, the first author (SS) synthesized data segments and accompanying codes and, with input from the research team, developed categories of RC-related health consequences (Hsieh & Shannon, 2005).
Results
Selection of Evidence Sources
The database search identified 1,554 articles. After removing duplicates, the screening process assessed 782 titles and abstracts. Of these, 166 full-text articles underwent eligibility assessment based on the inclusion criteria, resulting in including 62 studies. Figure 1 presents the PRISMA flow diagram, which outlines the number of studies included at each stage of the selection process.
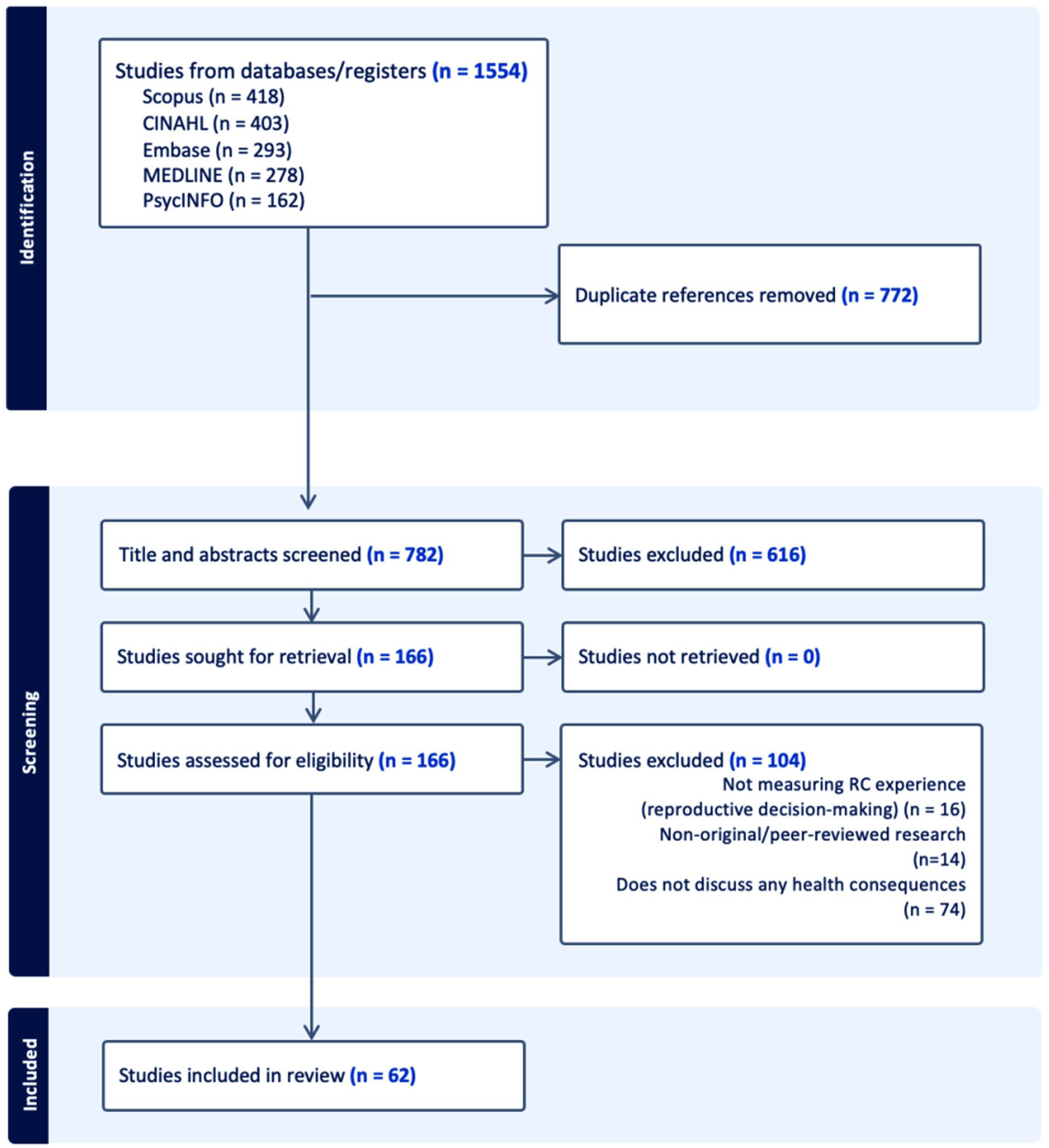
PRISMA flowchart for included studies.
Article Characteristics
We identified 62 eligible studies, conducted across 18 countries. The United States of America (USA) was the most frequent country of publication (n = 38), followed by Australia (n = 5) and Ethiopia (n = 4). Most studies used a quantitative cross-sectional design (n = 52), followed by qualitative interviews (n = 11). We identified many studies published between 2020 and 2024 (n = 39). Study settings varied, with SRH services (n = 25) and community-based contexts (n = 25) being the most common. Across the 62 included studies, the vast majority of participants were described as women or female, most often of reproductive age (15–49 years), with only 3 studies explicitly reporting gender identity of participants (Grace et al., 2022b; Lévesque et al., 2021; Swan et al., 2022). Only four studies included participants who were men/male: three quantitative studies (Hayes & Kopp, 2020; Swan et al., 2022; Wright et al., 2018) and one qualitative study (Thomas et al., 2024). Quantitative studies controlled for gender/sex in analyses, while the qualitative study presented findings where participants’ gender was apparent through quotes. Overall, the evidence on RC health consequences presented in this review largely reflects women’s experiences of RC. Supplemental Appendix A provides detailed descriptions of each study’s characteristics. Table 1 presents the frequency and percentage of study characteristics.
Characteristics of Evidence Sources.
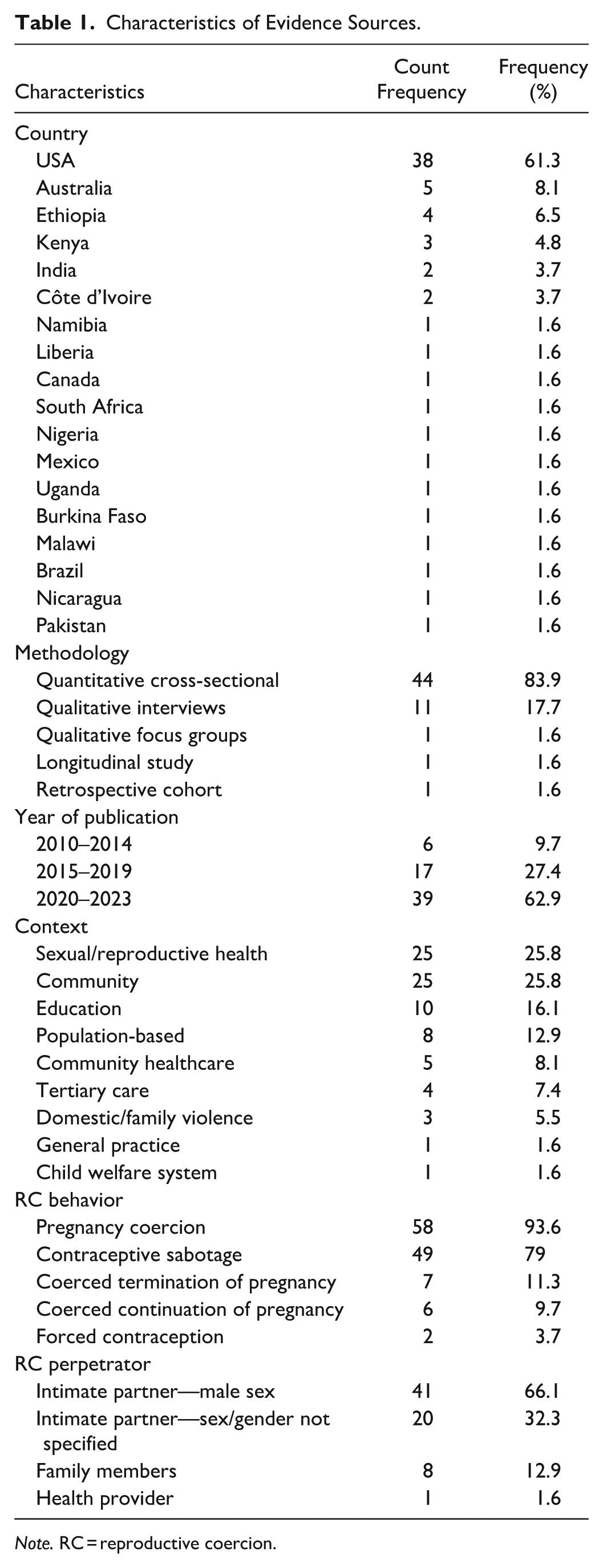
Note. RC = reproductive coercion.
RC Behaviors
Most studies examined the health consequences of pregnancy coercion (n = 58) and contraceptive sabotage (n = 49). Pregnancy coercion included threats, violence, or forced sex aimed at causing pregnancy; this also included instances of contraceptive sabotage where studies measured pregnancy intent. Contraceptive sabotage referred to interference with contraception in the absence of clear intent to cause pregnancy. Fewer studies explored the health consequences of coerced continuation of pregnancy (n = 6) or coerced termination of pregnancy (n = 7). Only two studies (3.7%) investigated the health impacts of forced contraception, including forced sterilization.
RC Perpetrators
Most studies identified intimate partners as the primary perpetrators of RC. Specifically, 41 studies referenced male partners, while 20 did not specify partner sex and/or gender. A smaller number of studies identified family members (n = 8) and healthcare providers (n = 1) as perpetrators.
Summary of RC Health Consequences
The health consequences of RC victimization spanned five key domains: (a) reproductive health, (b) sexual health, (c) mental health, (d) physical health, and (e) healthcare utilization. Supplemental Appendix B provides a comprehensive overview of the health consequences reported across the included studies.
Reproductive Health
Studies reported reduced general contraceptive use among individuals experiencing RC, based on quantitative evidence (John & Edmeades, 2018; Katz et al., 2017; Kraft et al., 2021; Rosenfeld et al., 2018; Silverman et al., 2019; Tomar et al., 2020; Wollum et al., 2023; Wood et al., 2022a) and qualitative findings (Buchanan & Humphreys, 2021; Uysal et al., 2022). However, several quantitative studies did not find a significant association between RC and contraceptive use, including Katz and Sutherland (2020), Marques et al. (2024), Northridge et al. (2017), Perry et al. (2020), Sutherland et al. (2015), Thiel de Bocanegra et al. (2010), Wood et al. (2023b, 2023c), and Wright et al. (2018).
Two quantitative studies observed a negative association between RC and oral contraceptive use (Cheng et al., 2021; Tomar et al., 2020), while others found no association with condom use (Cheng et al., 2021; Grace et al., 2022b; Hill et al., 2019; Northridge et al., 2017; Sutherland et al., 2015; Tomar et al., 2020). Conversely, quantitative studies associated RC with increased use of emergency contraception (Bagwell-Gray et al., 2021; Kazmerski et al., 2015), injectables (Skracic et al., 2021; Sutherland et al., 2015), implants (McCloskey et al., 2020; Skracic et al., 2021), and intrauterine devices (McCloskey et al., 2020; Skracic et al., 2021). RC was associated with covert contraceptive use in quantitative studies (Bagwell-Gray et al., 2021; Wood et al., 2023b, 2023c), with qualitative studies also describing covert contraception as a safety strategy in response to experiencing pregnancy coercion/contraceptive sabotage (Brenner et al., 2021; Grace et al., 2020, 2022a; Thiel de Bocanegra et al., 2010; Thomas et al., 2024; Wood et al., 2023c). Two quantitative studies found that RC was associated with reporting female sterilization (Cheng et al., 2021; Skracic et al., 2021). Most studies found no association between RC and use of other contraceptive methods such as the ring, patch, or withdrawal (Grace et al., 2022b; Northridge et al., 2017; Skracic et al., 2021; Sutherland et al., 2015).
Studies identified associations between RC and both ever experiencing pregnancy (Grace et al., 2022b; PettyJohn et al., 2021; Sutherland et al., 2015) and current or recent pregnancies (Grace et al., 2022a; Rosenbaum & DiClemente, 2020; Rosenfeld et al., 2018). Researchers consistently reported unintended pregnancy as the most robust reproductive health outcome of RC, supported by both quantitative (Ghayur et al., 2023; Holliday et al., 2017; Jones et al., 2016; Miller et al., 2010; Miller et al., 2014; Skracic et al., 2021; Wood et al., 2023a; Zemlak et al., 2024) and qualitative studies (Buchanan & Humphreys, 2021; Thiel de Bocanegra et al., 2010; Uysal et al., 2022; Wood et al., 2023b). A few studies found no significant association (Perry et al., 2020; Rosenfeld et al., 2018; Samankasikorn et al., 2019), suggesting that an unintended pregnancy may not always equate to a coerced pregnancy. One study associated RC with having had a miscarriage (Cheng et al., 2021), though findings varied (Grace et al., 2022a). Others reported positive associations with abortion (Cheng et al., 2021; Ghayur et al., 2023; Grace et al., 2022a; McCloskey et al., 2020; Sutherland et al., 2015), with several qualitative studies documenting covert abortion as a safety strategy in response to RC (Bagwell-Gray et al., 2021; Grace et al., 2022a; Thomas et al., 2024). One qualitative study connected pregnancy coercion driven by son preference with multiple closely spaced pregnancies (Puri et al., 2011). Fay and Yee (2020) found a positive association between experiencing RC and low birth weight neonates, but no association with preterm birth or stillbirth.
Sexual Health
Quantitative studies consistently identified a significant association between RC and increased risk of sexually transmitted infections (STIs; Grace et al., 2022b; Jones et al., 2016; Kraft et al., 2021; McCloskey et al., 2020; Northridge et al., 2017). Two studies directly attributed this risk to non-consensual condom removal (Lévesque et al., 2021; Willie et al., 2021). Other studies associated RC to reduced sexual desire (Lévesque et al., 2021), heightened sexual anxiety and depression (Sheeran et al., 2025), and decreased sexual assertiveness (Sheeran et al., 2025), although this study found no significant effect on sexual satisfaction (Sheeran et al., 2025). One study examining human immunodeficiency virus risk found higher acceptability of pre-exposure prophylaxis among women who reported experiencing contraceptive sabotage by a male partner (Willie et al., 2017).
Mental Health
Price et al. (2022) documented a significant association between RC and poorer overall mental health, with qualitative accounts describing emotional outcomes of experiencing RC such as self-blame, guilt, and diminished self-worth (Brenner et al., 2021; Buchanan & Humphreys, 2021; Puri et al., 2011). Several studies reported increased anxiety (Fay & Yee, 2020; Sheeran et al., 2025; Steinberg et al., 2016; Tarzia et al., 2018), stress (Sheeran et al., 2025; Steinberg et al., 2016), psychological distress (Willie & Callands, 2018), and reduced life satisfaction (Sheeran et al., 2025) among those experiencing RC. Qualitative findings reinforced these mental health outcomes (Bakare & Gentz, 2020; Lévesque et al., 2021). Post-traumatic stress disorder (PTSD) consistently appeared as one of the most prevalent mental health consequence of RC, with multiple quantitative studies reporting significant associations (Alexander et al., 2021; Anderson et al., 2017; Grace et al., 2022c; Jiwatram-Negrón et al., 2022; McCauley et al., 2014; Sheeran et al., 2025; Tarzia et al., 2018; Zemlak et al., 2024). Depression was also frequently associated with RC (Alexander et al., 2021; Grace et al., 2022d; Kraft et al., 2021; Sheeran et al., 2025; Zemlak et al., 2024), though a few studies found no significant association (Anderson et al., 2017; Grace et al., 2022c; Tarzia et al., 2018). Studies further associated RC with higher rates of alcohol and drug misuse (Muñoz et al., 2023; PettyJohn et al., 2021; Rosenbaum & DiClemente, 2020), though some results remained inconclusive. One study examined suicidal behavior but found no significant association with RC (Jiwatram-Negrón et al., 2022).
Physical Health
Few studies investigated the physical health consequences of experiencing RC. Hayes & Kopp (2020) found no association between RC and self-reported physical health. One study identified a significant association between RC and anemia (Fay & Yee, 2020). Puri et al. (2011) qualitatively noted the physical gynecologic harm of undergoing multiple forced abortions, though the study provided little detail beyond noting physical trauma. Bakare and Gentz (2020) reported qualitative evidence on the impact of forced sterilization on weight changes, abdominal pain, and back pain.
Healthcare Utilization
Several studies reported a higher number of health visits among individuals experiencing RC (Cheng et al., 2021; Grace et al., 2022b, 2022d), and qualitative accounts attributed this to symptoms resulting from forced sterilization (Bakare & Gentz, 2020). However, not all studies found an association between experiencing RC and increased healthcare utilization (Fay & Yee, 2020; Hill et al., 2019). RC was also associated with delayed initiation of antenatal or prenatal care, with women experiencing RC more likely to have their first healthcare contact after 12 weeks of gestation (Price et al., 2022), and qualitative findings describing avoidance or missed appointments because of partner interference or fear (Buchanan & Humphreys, 2021). However, Wood et al., 2022b did not find an association between RC and completion of antenatal and postnatal care. Several studies reported increased use of SRH services among individuals experiencing RC. These included higher rates of STI testing (Grace et al., 2022b; Kazmerski et al., 2015), pregnancy testing and options counseling (Ghayur et al., 2023; Kazmerski et al., 2015; Lévesque et al., 2021), and abortion services (Upadhyay et al., 2014). However, other studies found no significant associations between RC and access to mental health services, contraceptive counseling, general health consultations (Cheng et al., 2021; Grace et al., 2022b, 2022d; Hill et al., 2019), or screening services, such as mammography and cervical cytology (Marques et al., 2024).
Discussion
This review comprehensively synthesizes the health consequences of experiencing RC across five key domains: reproductive, sexual, mental, physical health, and healthcare utilization. It extends evidence from previous systematic reviews that primarily identified associations between RC and unintended pregnancy or covert contraceptive use (Grace & Anderson, 2018; Grace & Fleming, 2016; Moulton et al., 2021), by mapping a broader range of health outcomes linked to five distinct RC behaviors. Most studies focused on pregnancy coercion and contraceptive sabotage, consistently associating these behaviors with adverse reproductive, sexual, and mental health outcomes. In contrast, few studies examined physical health impacts or healthcare utilization as a result of experiencing RC, revealing important gaps in the evidence base. Table 2 summarizes the key findings and their implications for research, practice, and policy.
Summary of Critical Findings and Associated Implications for Research, Practice, and Policy.
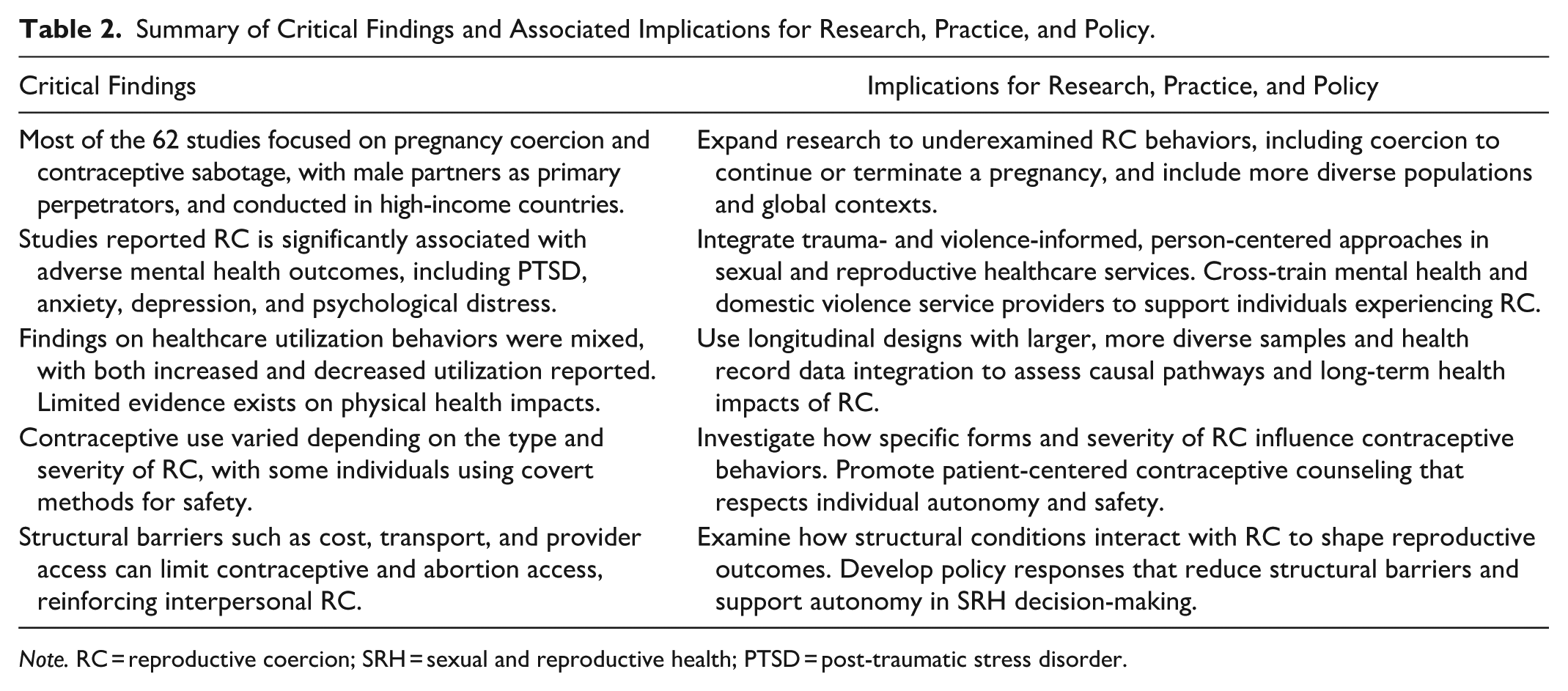
Note. RC = reproductive coercion; SRH = sexual and reproductive health; PTSD = post-traumatic stress disorder.
Health consequences of coercion to continue or terminate a pregnancy, and of forced contraception, remain underexplored. Although some studies have addressed these behaviors, they are often not fully captured within broader conceptualizations of RC. For example, the Turnaway Study demonstrated that denying individuals abortion and forcing them to carry unwanted pregnancies led to greater psychological harm such as heightened anxiety and low self-esteem (Biggs et al., 2017), as well as increased risks of complications like eclampsia and postpartum hemorrhage (Gerdts et al., 2016). Yet few studies in this review examined the broader psychological or reproductive health outcomes associated with coerced continuation or termination of pregnancy, or with forced contraception, indicating a critical gap in the evidence base.
Findings from this review show that the impact of RC on contraceptive use is mixed and varies by both the type of contraception and the nature of coercive behaviors. Some studies reported reduced contraceptive use, particularly oral contraceptives, while others found increased use of covert methods like injectables or intrauterine devices. These varying patterns may reflect the form RC takes; for example, verbal pressure (e.g., being told not to use contraception) may interfere with contraceptive choices differently than physical interference (e.g., flushing pills) (Skracic et al., 2021). However, few studies have examined how the severity or form of RC impacts contraceptive choices, limiting practical guidance for healthcare providers. Recognizing how different forms of RC shape contraceptive decision-making is essential for providing patient-centered contraceptive care. Healthcare providers must offer flexible, non-judgmental support and ensure access to a full range of contraceptive options, including support for starting, stopping, switching methods, or choosing non-use or traditional methods, based on individual needs, safety, and autonomy.
The varied findings on the impact of RC on contraceptive use are further complicated by differences in how contraceptive use is measured across studies. Many studies relied on self-reported contraceptive use without accounting for whether use is consistent, voluntary, or effective. In some cases, a person’s desire or intention to use contraception may not align with their actual use (Boydell & Galavotti, 2022), often reflecting RC and the influence of others. In addition, most studies assume a link between contraceptive use and pregnancy intention (Boydell & Galavotti, 2022), but individuals may use contraception for reasons unrelated to pregnancy, and their pregnancy preferences may not always align with their contraceptive behavior (Samari et al., 2020). Future RC measurement tools should account for the possibility that pregnancy and contraceptive intentions may diverge, and that reported contraceptive use does not always reflect true reproductive autonomy (Holt et al., 2023).
This review affirms the association between RC and unintended pregnancies, while also highlighting that coerced pregnancies do not always equate to unintended pregnancies. Pregnancy intentions may shift over time due to changing motivations within both violent and nonviolent relationships (Carter et al., 2013; Rocca et al., 2019). Future studies should clearly differentiate between pregnancy intention and coercion. In some cases, an existing pregnancy may reduce an abusive partner’s need to exert RC (Grace et al., 2022a). Additionally, some individuals may describe RC without identifying a partner’s clear desire for pregnancy (Katz et al., 2017). Exploring partner perspectives on RC and pregnancy intentions could provide deeper insight (Tarzia & McKenzie, 2024). Reproductive counseling in healthcare settings could consider the influence of significant others on decision-making.
Our findings, which identify the association of RC with negative mental health outcomes such as PTSD, depression, and anxiety, demonstrate a clear need to integrate mental health and SRH care for individuals reporting RC. Future studies should examine in more detail co-occurring mental health outcomes associated with RC (Jiwatram-Negrón et al., 2022). Trauma- and violence-informed care remains essential in recognizing RC, creating safe spaces for disclosure, and ensuring appropriate, safe responses (Wathen & Mantler, 2022). Such care must prioritize patient-centered support and non-directive care to ensure informed decision-making (Anderson et al., 2017). Cross-training mental health professionals and domestic violence workers may improve support for those experiencing RC and associated mental health risks (Jiwatram-Negrón et al., 2022).
Most studies included in this review were conducted in high-income countries, particularly the USA, highlighting a need for more research in diverse global contexts. As RC evidence from low- and middle-income countries grows, future research could conduct comparative analyses of health consequences by region and country, allowing for more nuanced insights into how RC operates in diverse social, political, and health system contexts. Additionally, majority were cross-sectional in design, limiting the ability to draw causal inferences. Future research should prioritize longitudinal and prospective cohort studies, as well as the use of health record data, to better capture the temporal relationship between RC and health outcomes (Fay & Yee, 2020). RC research to date has also focused primarily on cisgender women in heterosexual relationships with male intimate partners as perpetrators, overlooking the broader range of perpetrator identities and diverse population experiences. Expanding this focus to include different gender identities, relationship dynamics, and cultural contexts is essential for a more comprehensive understanding of RC. In addition, most evidence identified in the review was collected from SRH settings. However, in some countries, contraception and pregnancy tests are widely available over the counter (Grace et al., 2022b; Hill et al., 2019), which may help explain the absence of significant associations between RC and healthcare utilization. Further investigation is needed in settings like pharmacies to better understand how RC influences healthcare utilization.
Finally, most studies in this review focused on interpersonal forms of RC, with limited attention to structural or institutional barriers that also restrict contraceptive access (Engelbert Bain et al., 2021). Some researchers suggest treating structural and interpersonal RC as separate but related factors (Tarzia & Hegarty, 2021). Yet women who wish to use long-acting reversible contraception as a safety strategy can have costs or lack of provider access obstruct their use (DiCenzo et al., 2023). These barriers may reinforce partner interference or limit resistance strategies. In addition, restrictive political climates surrounding reproductive rights, such as the overturning of Roe v. Wade in the USA, have implications for health complications due to forced pregnancies and reduced access to safe abortion, disproportionately impacting marginalized populations (Keegan et al., 2023). Further research should examine how structural conditions interact with interpersonal RC in shaping access to contraception, pregnancy, and abortion care.
Limitations
This scoping review did not include a critical appraisal of the quality of included studies, which limits the ability to offer definitive conclusions or recommendations for policy and practice. Beyond variation in RC measurement and definition across studies, the predominance of cross-sectional designs, reliance on retrospective self-report in most studies, and potential recall or publication bias may also have contributed to variability and mixed findings across studies. Most studies also originated from the USA, restricting the generalizability of findings to low- and middle-income contexts. Limiting the review to English-language, peer-reviewed studies published since 2010 may have excluded relevant insights available in gray literature, earlier publications, or research published in other languages. Some studies may have overstated the health consequences of contraceptive sabotage by inferring pregnancy intent without directly measuring or reporting it. Our search strategy did not capture broader reproductive autonomy literature, which, while relevant to reproductive decision-making, was not explicitly described using RC terminology; future research could examine structural threats to reproductive autonomy and their intersections with interpersonal RC in shaping health outcomes. We also reported findings as presented in the included studies; however, many included did not explicitly differentiate RC from overlapping forms of IPV or sexual violence, which is an important consideration that future systematic reviews or meta-analyses could address. Healthcare provider coercion in reproductive contexts, including obstetric/gynecologic violence, is often not labeled as RC. Our review, therefore, may not capture the full extent of this issue, though we included available evidence given the growing use of the term RC to encompass coercion enacted by health providers.
Conclusion
This review demonstrates the significant health consequences of experiencing RC, with most evidence centered on pregnancy coercion and contraceptive sabotage. To build a more complete understanding, future research should explore underexamined forms of RC, such as coercion to continue or terminate a pregnancy, and broaden geographic scope beyond high-income countries. Greater attention is needed to how the type and severity of RC behaviors influence contraceptive choices, and how structural barriers such as cost and access interact with partner interference. Differentiating between unintended and coerced pregnancies and incorporating partner perspectives on pregnancy intent will strengthen conceptual clarity of RC. Healthcare responses must integrate trauma- and violence-informed and person-centered approaches to SRH that holistically address the intersection of psychological and physical health. Expanding research to diverse healthcare and community settings and employing longitudinal research methods will support stronger evidence and more effective interventions.
Supplemental Material
sj-docx-1-tva-10.1177_15248380251383931 – Supplemental material for Reproductive Coercion and Associated Health Consequences: A Scoping Review
Supplemental material, sj-docx-1-tva-10.1177_15248380251383931 for Reproductive Coercion and Associated Health Consequences: A Scoping Review by Susan Saldanha, Jessica R. Botfield, Desireé LaGrappe, Maryam Moradi and Danielle Mazza in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-2-tva-10.1177_15248380251383931 – Supplemental material for Reproductive Coercion and Associated Health Consequences: A Scoping Review
Supplemental material, sj-docx-2-tva-10.1177_15248380251383931 for Reproductive Coercion and Associated Health Consequences: A Scoping Review by Susan Saldanha, Jessica R. Botfield, Desireé LaGrappe, Maryam Moradi and Danielle Mazza in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
None.
Data Availability
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an International Tuition Scholarship and a Graduate Research Scholarship from the Faculty of Medicine, Nursing and Health Sciences, Monash University (Grant no: N/A).
Ethical Considerations
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.