
Abstract
Non-institutional political participation (NiPP) is rising in Southern Europe. However, how the relationship between health and NiPP is conditioned by age and education remains underexplored. To address this gap, this study analyses data from 8944 participants in the European Social Survey (wave 10) across Portugal, Spain, Italy, and Greece. Results showed that as subjective general health (SGH) increases, the likelihood of NiPP decreases. Both age and education moderated this relationship. For younger individuals and those with higher education, increased SGH led to reduced NiPP. Conversely, for older individuals and those with lower education, the decline in NiPP participation was less pronounced as SGH increased. Future research should examine specific forms of participation and specific health conditions, as well whether age and education continue to moderate NiPP involvement.
Exploring the Role of Health, Age, and Education in Non-Institutional Political Participation
The exercise of citizenship can manifest itself in different ways (Dalton, 2008). The most common is through voting (Denny and Doyle, 2007; Goerres, 2007; Kriesi, 2008; Mattila et al., 2013; Pacheco and Fletcher, 2015), which may be called an institutional, traditional, or conventional form of political participation. However, this type of participation has been losing ground to other forms of manifestation (Klingemann and Fuchs, 1995; Stolle and Hooghe, 2011). The emergence of social movements, protests and demonstrations, and online petitions—known as non-institutional forms of political participation (NiPP)—have gained relevance as an important channel for people to express their anger and discontent with government policies (Kriesi, 2008; Norris, 2001; Norris et al., 2005), particularly among young people (Marien et al., 2010; Mattila, 2020; Stolle and Hooghe, 2011).
Health status has been regarded as a strong predictor for NiPP (Christensen et al., 2019; Couture and Breux, 2017; Kirbiš et al., 2023; Mattila, 2020; Söderlund and Rapeli, 2015). In contrast, traditional forms of political participation associate poorer health with lower levels of political efficacy (Denny and Doyle, 2007), interest, and participation (Söderlund and Rapeli, 2015). Several studies show that people with health issues tend to participate more in NiPP (Christensen et al., 2019; Couture and Breux, 2017; Kirbiš et al., 2023; Mattila, 2020; Söderlund and Rapeli, 2015). Moreover, other individual factors, such as age and education, are also associated with NiPP. Age is a strong predictor of health (Couture and Breux, 2017; Kirbiš et al., 2023). Older generations are more susceptible to chronic diseases, which may limit their capacity to participate, while younger individuals are more likely to recover fully and be mobilized into action (Franceschi et al., 2018). This suggests a potential relationship between age and NiPP, with younger individuals more likely to engage in NiPP (Couture and Breux, 2017; Kirbiš et al., 2023). Most differences in individual-level participation stem from socioeconomic status (SES), which is strongly linked to higher levels of education (Verba et al., 1995). SES resources enhance citizens’ knowledge and skills, thereby increasing the likelihood of political engagement (Kirbiš et al., 2017). Regarding education, research indicates that the more educated a person is, the more likely they are to participate in NiPP (Ejrnæs, 2017). While Verba and Norman (1972) established that middle-class individuals are more politically active, recent studies have emphasized the role of health in motivating political action (Kirbiš et al., 2023; Mattila et al., 2018).
Health inequalities have been widely explained through theories emphasizing the social determinants of health, the social gradient, and the notion of fundamental causes (Link and Phelan, 1995; Marmot, 2005). These perspectives stress that education, income, and social status provide access to “flexible resources” that can be mobilized to maintain or improve health, thereby reproducing inequalities across contexts and over the course of life. The life course approach further shows that health disadvantages accumulate over time, while the double disadvantage framework highlights how intersecting vulnerabilities (e.g. poor health combined with low education) exacerbate exclusion. When applied to non-institutional political participation (NiPP), these perspectives intersect with the Civic Voluntarism Model (Verba et al., 1995), which posits that the lack of personal resources such as education (alongside with social network embeddedness and psychological involvement in politics) may hinder participation (Kirbiš et al., 2023). In this sense, health is not only a condition affecting individual capacity to engage, but also a stratifying factor that interacts with education and age to shape access to participatory resources.
We situate our theoretical framework within both traditions—health inequality theories and the Civic Voluntarism Model (CVM)—strengthening the conceptual framework (Figure 1) by linking individual health conditions to broader social structures and conditions (low/high levels of education) to explain NiPP. Therefore, we propose to analyze the moderating effects of age and education in the relationship between subjective general health (SGH) and NiPP, in Southern Europe countries (SEC).
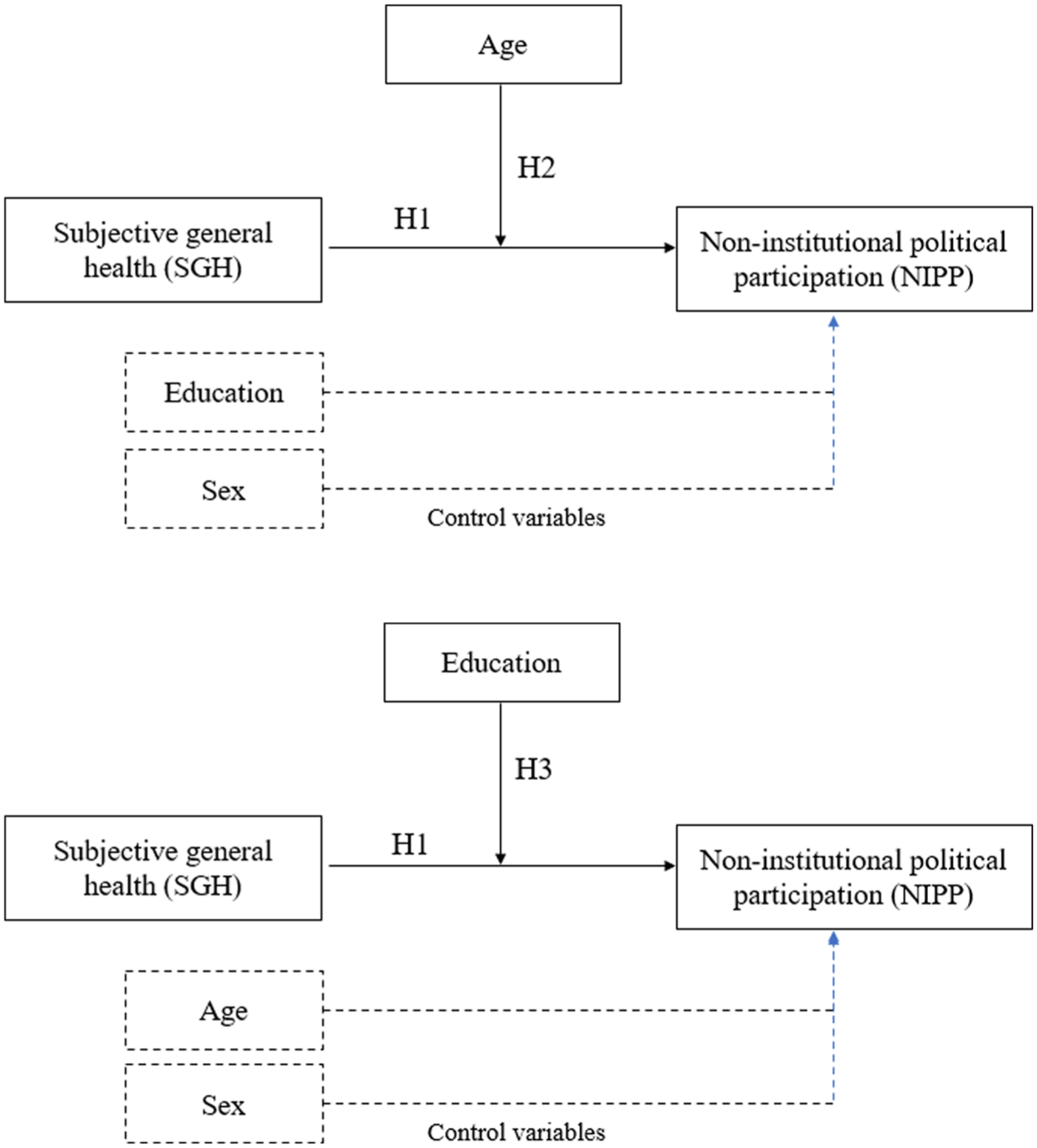
Conceptual Model.
Southern Europe usually appears as a theoretical framework for studies on welfare (Esping and Anderson, 1990 and Ferrara, 1996), but in recent years it has gained traction in political participation studies due to a gradual rise in NiPP across Southern Europe, particularly in Portugal and Spain. In Portugal, for example, both volunteering and participation in demonstrations remain below the European average (Serra-Silva and Oliveira, 2022), however, petition signing has grown in Portugal (Serra-Silva and Oliveira, 2022), while demonstrations have become more frequent in Spain.
Comparative research using European Social Survey (ESS) rounds 3 to 7 (2002–2014) confirms that Portugal and Spain display distinct mobilization patterns when compared with Central and Eastern Europe, suggesting a regional trajectory of increasing NiPP (Campos Lima and Artiles, 2018). In the study of Goroshit (2016), analyzing data from ESS round 5, there was clear evidence of an uprising in NiPP in Spain (55.9%), Greece (27.3%) and Portugal (10.9%). This trend is particularly visible among young people. Analyses of ESS rounds 8 and 9 show that, following the economic crisis, political mobilization among youth in Portugal, Spain, Italy, and Greece has expanded, notably through digital channels, signaling structural shifts in participation (Lisi et al., 2021). More recent ESS round 10 data corroborate these dynamics: Spain reports the highest NiPP levels (petition signing, online political content, boycotting, volunteering), followed by Greece, with Italy and Portugal at lower but growing levels.
When comparing to northern European countries, such as Denmark and Sweden, literature evidence that volunteering in non-profit organizations is widespread, while in Southern Europe, citizen mobilization tends to occur through unions and associations (Serra-Silva and Oliveira, 2022). Some authors argue that Nordic citizens often express dissatisfaction through NiPP, whereas this culture has been historically weaker in Southern Europe (Anderson and Hoff, 2001; Von Erlac, 2001).
Evidence on self-assessed general health (SGH) is more nuanced. On the one hand, SGH tends to be slightly worse in Portugal and Spain than the European average for young people, with a higher proportion of individuals reporting their health as “fair” but not as much as Sweden or Finland (Eurostat, 2025). On the other hand, SEC consistently record fewer healthy life years compared to Northern and Central Europe, reflecting a higher prevalence of functional limitations and chronic conditions. This pattern suggests that, despite greater longevity, the quality of health across the life course is relatively poorer in Southern Europe (OECD, 2023). Such evidence reinforces the relevance of a regional focus, as it enables examination of how health interacts with sociodemographic variables such as age and education in shaping NiPP.
Overall, NiPP in Southern Europe has increased, particularly among younger cohorts, driven by economic crises and digitalization. These evolving dynamics make SEC a region worthy of studying and investigating the relationship between SGH and NiPP, while accounting for key sociodemographic moderators.
Relationship between SGH and NiPP
Health is a significant factor in political participation (Carpenter, 2012; Christensen et al., 2019; Goerres, 2007; Mattila, 2020; Mattila and Papagiorgiou, 2017 ; Pacheco and Fletcher, 2015; Shore et al., 2019; Söderlund and Rapeli, 2015; Stockemer and Rapp, 2019). As Carpenter (2012, p. 303) observes, “health and illness shape who we are politically.” Poor health often shifts an individual’s focus from political to personal matters (Söderlund and Rapeli, 2015). In traditional political participation, poor health reduces the likelihood of voting (Brown et al., 2020; Couture and Breux, 2017; Denny and Doyle, 2007; Mattila et al., 2013; Pacheco and Fletcher, 2015; Söderlund and Rapeli, 2015) and decreases psychological engagement with politics (Gidengil and Wass, 2024).
By contrast, the relationship between health and NiPP appears to follow a different pattern. Individuals in poor health often turn to more accessible forms of activism, such as contacting public officials or attending demonstrations (Söderlund and Rapeli, 2015), particularly among younger cohorts (Christensen et al., 2019; Couture and Breux, 2017; Kirbiš et al., 2023; Söderlund and Rapeli, 2015; Stolle and Hooghe, 2011). Evidence also suggests that people with disabilities are more likely to participate in demonstrations or to contact politicians directly (Mattila and Papagiorgiou, 2017). Likewise, a Canadian cross-sectional study found that individuals reporting poor mental health were more likely to sign online petitions (Couture and Breux, 2017). Supporting this trend, Nordic research shows that in Finland and Denmark young people in poor health are highly engaged in signing initiatives (Christensen et al., 2019).
Theoretical perspectives on health inequalities help to explain these dynamics. Classical approaches emphasize that health inequalities stem not only from individual factors (such as behavior or genetics) (Correia et al., 2024) but, more fundamentally, from social and structural conditions including income, education, housing, employment, and public policy (Marmot, 2005). The social gradient perspective underscores that socioeconomic status (SES) represents a “fundamental cause” of health outcomes because it provides access to flexible resources such as knowledge and social networks (Link and Phelan, 1995). SES is also central to the CVM, where it constitutes a key component of personal resources that facilitate political participation (Kirbiš et al., 2017; Verba et al., 1995). Given this context, the study proposes the following hypothesis:
Hypothesis 1: SGH is negatively related to NiPP.
Age and Education as Moderators
Although poor health negatively impacts traditional political participation, particularly among older individuals (Mattila et al., 2013), younger people tend to participate more in NiPP despite reporting lower levels of health (Christensen et al., 2019; Couture and Breux, 2017; Söderlund and Rapeli, 2015; Stolle and Hooghe, 2011). The literature suggests that younger individuals with poor health have a higher propensity to engage in various forms of NiPP (Kirbiš et al., 2023). For example, young people with poorer health have a higher propensity to sign citizens’ initiatives (Christensen et al., 2019; Söderlund and Rapeli, 2015), to wearing a campaign badge/sticker, contacting public officials and taking part in a lawful demonstration (Söderlund and Rapeli, 2015), or to participate more in non-profit organization (Curtis et al., 1992) which are forms of NiPP. Kirbiš, Mattila, and Rapeli (2023) interpret this evidence in the fact young people have more to lose than older people, meaning young people “have more years left than older people, so they feel more motivated to participate because they have more at stake” (Kirbiš et al., 2023: 219). However, it should be considered that participation in NiPP depends on the specific health issues young people have. For instance, the type of health issues that young people face, many times, is different from older generations. Older generations are susceptible to a range of chronic diseases which can manifest in an incapacity to political participation (Sonnicksen, 2016) while younger generations are more likely to suffer from temporary diseases which can be more likely to participate in NiPP (Couture and Breux, 2017; Schur et al., 2015) and have fewer other relevant resources such as social networks, integration and civic skills (Kirbiš et al., 2023). So, although voting is more frequent to older generations because they feel a subjective norm to vote (Goerres, 2007), studies have shown that NiPP are keener to younger generations (Christensen et al., 2019; Marien et al., 2010; Norris, 2002; Stolle and Hooghe, 2011; Zukin et al., 2006). The “new citizens” are less likely to just put their vote into the ballot box, but to actively participate in politics and be active through the various ways of doing politics. Why do people with poorer health, especially young people, turn to NiPP? In the literature, there are two main factors pointed out. One is that young people who feel less healthy can easily support initiatives from home (Christensen et al., 2019) and young people are the ones with more familiarity with new technologies and higher education (Skocpol, 2004). This generation is more familiar with the variety of instruments for participating in non-institutional forms (e.g. Internet) which enables, even in poorer health conditions, to actively participate in political actions. Another reason is highlighted by Mattila (2020), following Stoker (2006), which suggested that it had to be related with distrust in the political system. People who have a high political trust in the system (institutions, etc.) tend to decrease their participation in non-institutional forms and, on the other hand, people who have a reduced trust in the political system tend to participate more in non-institutional forms (Mattila, 2020). Since people with poorer health feel discredited by the conventional forms of politics, they turn to non-institutional forms to make their voice heard (Mattila, 2020). Thus, it is hypothesized as follows (Figure 1):
Hypothesis 2: Age moderates the relationship between SGH and NiPP, such that the association is stronger for younger individuals than for older ones.
Similarly, education is a strong predictor of (Chen et al., 2023; NiPP Ejrnæs, 2016). Higher education levels enhance civic skills and access to resources, increasing participation in NiPP (Stolle and Hooghe, 2011; Verba et al., 1995). Education not only improves political knowledge and cognitive skills but is also strongly associated with socioeconomic status (SES), which contributes to social stratification in emerging forms of political participation (Slavina, 2021; Stolle and Hooghe, 2011; Verba et al., 1995).
While the literature provides robust evidence of education as a predictor of NiPP, it may also operate as a moderator of the relationship between health and participation. Poor health often reduces individuals’ ability to engage in conventional political activities such as voting, attending meetings, or maintaining sustained political involvement (Mattila et al., 2013; Söderlund and Rapeli, 2015). However, higher levels of education can mitigate these negative effects by equipping individuals with civic skills, political knowledge, and access to resources that enable them to remain politically active despite health limitations (Burden et al., 2017; Verba et al., 1995). Empirical evidence suggests that individuals with higher education are better positioned to adapt their modes of participation when health constraints arise. For example, those with advanced educational backgrounds are more likely to substitute resource-intensive activities (e.g. attending demonstrations) with less physically demanding but equally effective forms of engagement, such as signing petitions or participating in digital activism (Marien et al., 2010; Stolle and Hooghe, 2011). Education therefore acts as a buffering factor, reducing the extent to which poor health excludes individuals from public life. From a theoretical standpoint, this dynamic aligns with the Civic Voluntarism Model (Verba et al., 1995), which posits those personal resources—particularly civic skills and knowledge, strongly associated with educational attainment—enhance the likelihood of participation. Education not only increases the repertoire of available participatory strategies but also fosters resilience against the demobilizing effects of poor health. Consequently, the interaction between health and education reflects a broader stratification mechanism, whereby those with fewer educational resources are more vulnerable to political disengagement when facing health problems, while highly educated individuals maintain higher levels of participation (Ejrnæs, 2016). Given this, the study proposes the following:
Hypothesis 3: Education moderates the relationship between SGH and NiPP, such that the association is stronger for individuals with higher education.
Method
Data Source
Data were retrieved from the European Social Survey (wave 10) of the year 2020. The European Social Survey is an academically driven cross-national survey that has been conducted every 2 years across Europe and Israel since 2001. The survey measures the attitudes, beliefs and behavior of European people. The inquiry for this data panel was applied between 2018 and 2019 (https://www.europeansocialsurvey.org/, accessed on 28 June 2023).
Participants
The sample included 8994 participants (53.5% were female) from four southern European countries: Portugal, Spain, Greece, and Italy. Participants were aged between 15 and 90 years (M = 51.1, SD = 18.0) and the years of schooling ranged from 0 to 50 (M = 12.2, SD = 5.2). The characterization of each country can be found in Table A1 (cf. Supplementary Material).
Measures
Dependent Variable: NiPP
The dependent variable, NiPP, was derived from eight yes/no items assessing various forms of NiPP considering the previous 12 months. The eight items of NiPP included worn or displayed campaign badge/sticker; volunteered for not-for-profit or charitable organization; donated to or participated in political party or pressure group; taken part in public demonstration; boycotted certain products; posted or shared anything about politics online; signed petition; contacted politician or government official. Before creating a composite measure, a multiple correspondence analysis (MCA) was conducted to examine whether the items could be meaningfully summarized in a single dimension. The first dimension accounted for 33.9% of the total variance, supporting the use of a unidimensional scale. Reliability was satisfactory (ω = 0.73) (Hayes and Coutts, 2020). Consistent with previous research that emphasizes capturing engagement in NiPP broadly rather than distinguishing between specific acts (Christensen et al., 2019; Marien et al., 2010), it was created a summated scale reflecting the number of activities in which respondents had participated. Given the positive skew of this new variable, it was transformed into a dummy variable (0 = no NiPP and 1 = at least one form of NiPP).
Independent Variable: SGH
SGH is a valid measure of self-rated health status (DeSalvo et al., 2006), making it suitable for use as a self-reported health variable in the ESS. In this measure, individuals evaluate their own perception of their health status. SGH was assessed using a 5-point Likert-type scale, ranging from 1 (very good) to 5 (very poor). Reverse coding was applied so that higher scores corresponded to a better perception of health.
Moderators: Age and Education
Age and education were examined as individual-level factors moderating the relationship between SGH and NiPP. Age was operationalized as a continuous variable measured in years, and education was assessed by the total number of years of schooling completed.
Control Variables: Sex, Age and Education
Since education is closely related to age—with newer generations typically having higher levels of education due to the considerable expansion of educational opportunities in the late twentieth century (Skocpol, 2004)—these two variables are correlated. This trend is particularly evident in Southern European countries, where younger generations have benefited from widespread access to education in recent decades (Capucha et al., 2016). Consequently, in our analysis, when age is the moderator, education will be controlled, and vice versa.
Sex was also included as a control variable since it is one of the most standard control variables in political participation research (Inglehart and Norris, 2003; Marien et al., 2010; Stockemer and Rapp, 2019; Verba et al., 1995). Many studies and national surveys consistently include this variable because differences in participation between men and women are well documented. We coded the sex variable as a dummy variable (0 = female, 1 = male).
Data Analysis
Descriptive statistics, including percentages, means, standard-deviation and bivariate correlations, were first calculated for all the study variables. Then, a logistic regression analysis was conducted to test Hypothesis 1, focusing on the main effect between SGH and NiPP. This analysis included the two moderators age and education as control variables, and also the variable sex. Finally, to test Hypotheses 2 and 3 two moderation models were estimated using the PROCESS macro for SPSS version 4.2 (Hayes, 2022), given that NiPP was measured as a binary variable. Each model incorporated one moderator—either age or years of schooling—in the relationship between SGH and NiPP (see Figure 1). Age and years of schooling were treated as covariates when not used as moderators, and sex was included as a control variable in both models. Predicted probabilities from the logistic regression models were used to plot the interaction effects in Figures 2 and 3. The parametric estimates were validated with bootstrapping (5000 bootstrap samples) to ensure the robustness of the results. Statistical significance was set at p < 0.05.
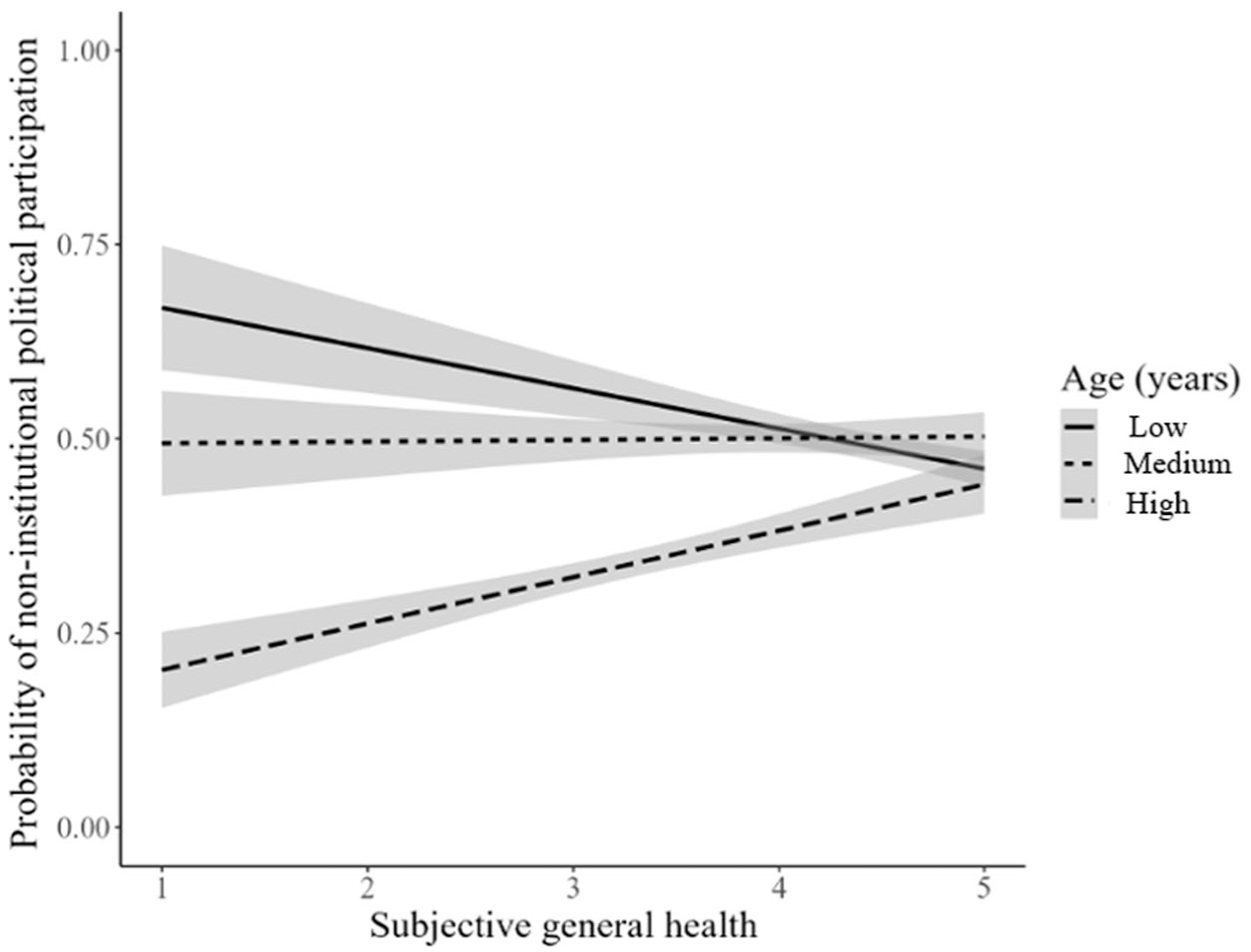
The Moderating Effect of Age on the Relationship between Subjective General Health (SGH) and Non-institutional Political Participation (NiPP).
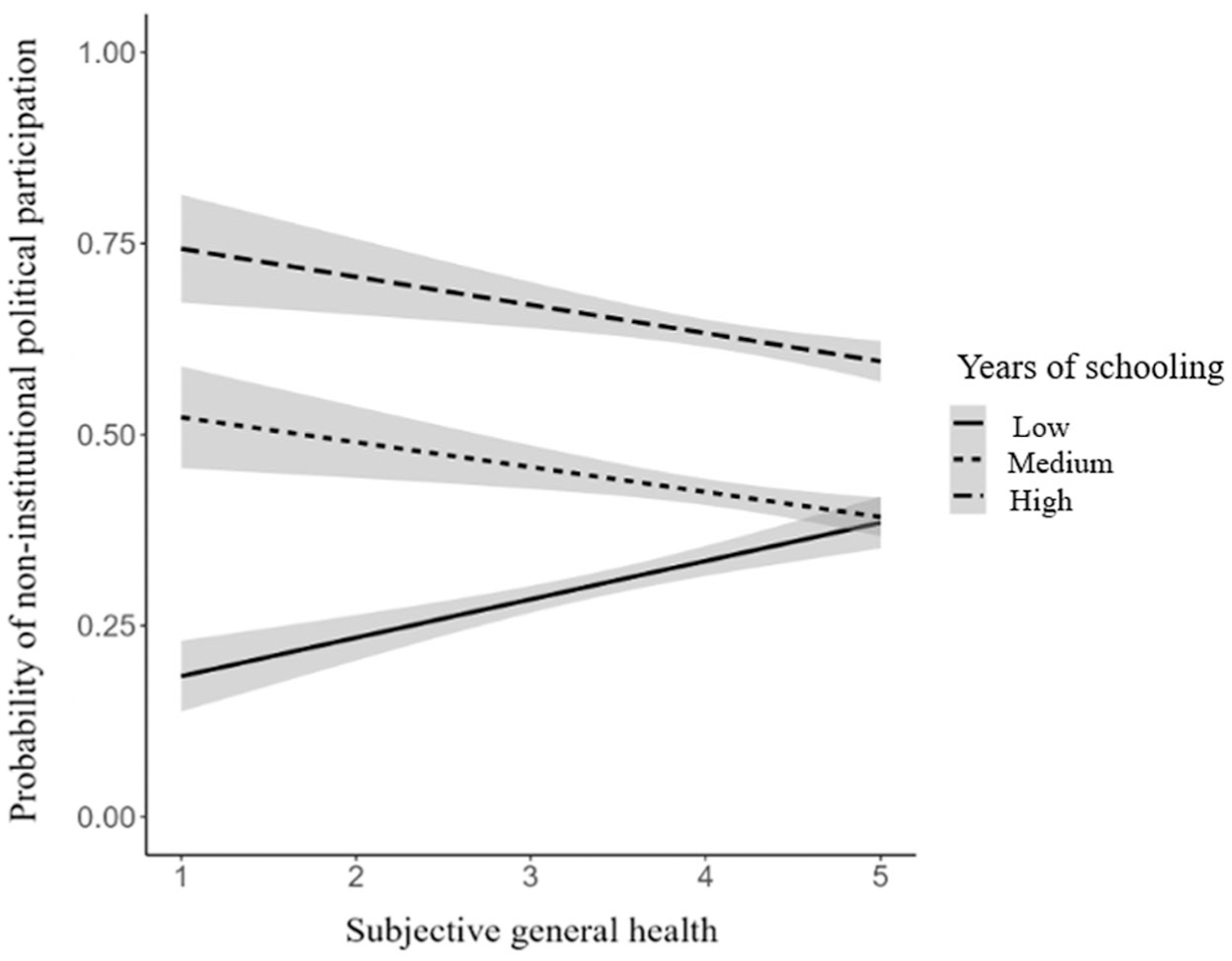
The Moderating Effect of Education on the Relationship between Subjective General Health (SGH) and Non-institutional Political Participation (NiPP).
Results
Table 1 presents the means and standard deviations of the study variables. All zero order correlations were significant, ranging from small to large effects (Cohen, 1992).
Descriptive Statistics for the Study Variables.
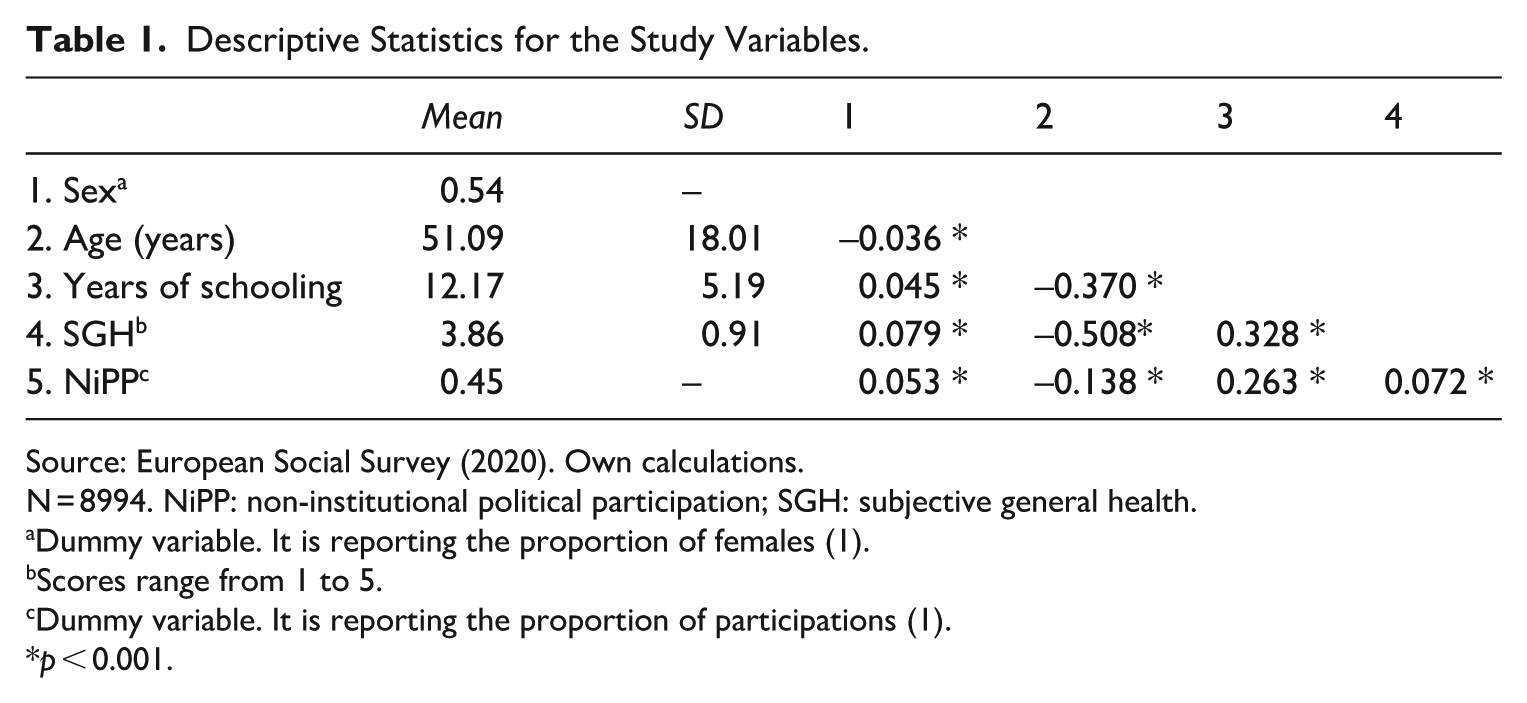
Source: European Social Survey (2020). Own calculations.
N = 8994. NiPP: non-institutional political participation; SGH: subjective general health.
Dummy variable. It is reporting the proportion of females (1).
Scores range from 1 to 5.
Dummy variable. It is reporting the proportion of participations (1).
p < 0.001.
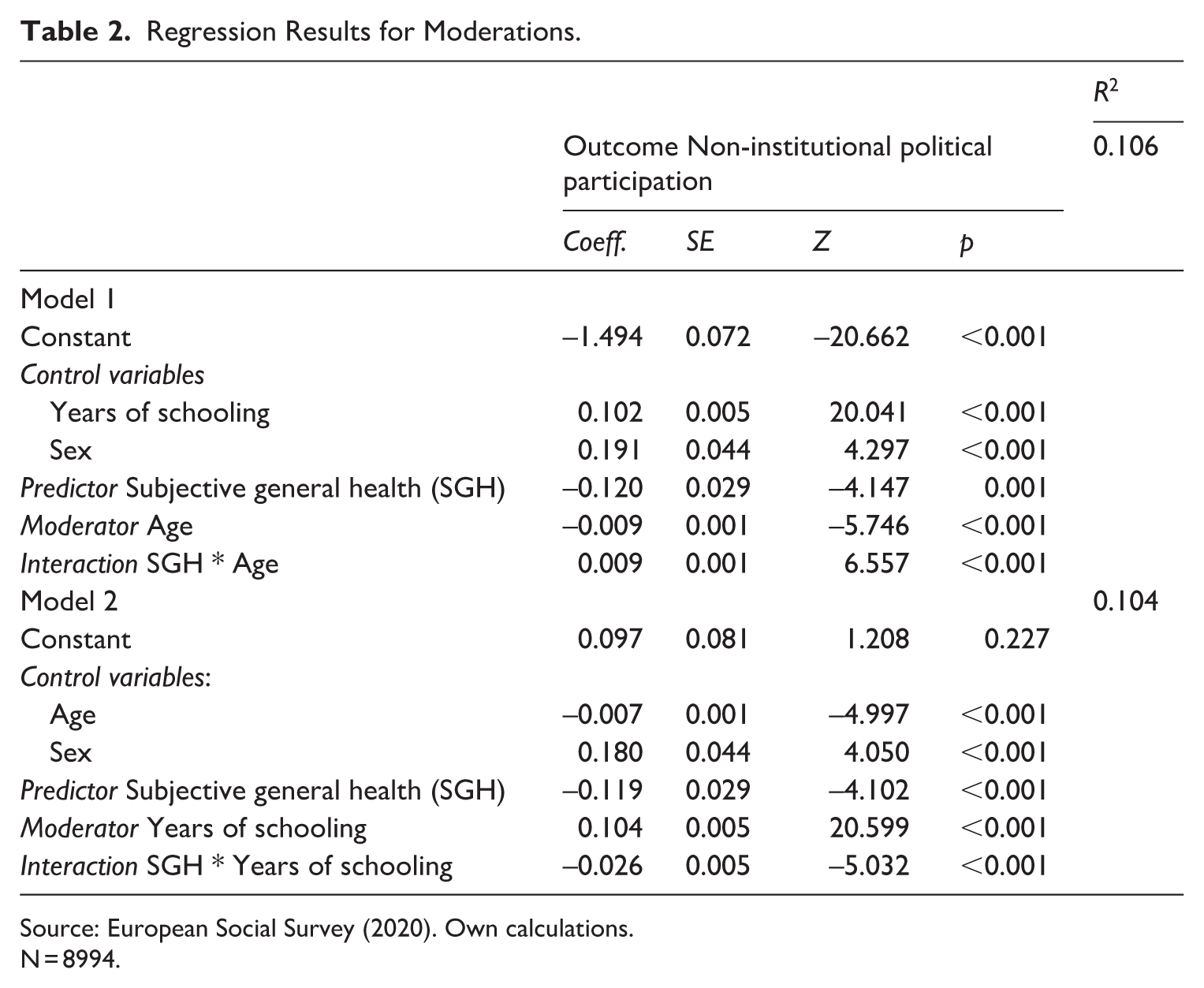
The first research hypothesis, which examined the relationship between SGH and NiPP, was addressed first. A significant association was found between them (B = –0.125, Wald = 21.312, p < 0.001). The effect size was Part R2 = 0.011, which, according to Cohen’s guidelines (2016) is considered small. The two variables were negatively associated, indicated that as the perception of health increased, the probability of participation in NiPP decreased. Thus, Hypothesis 1 was supported. Table 2 presents the results of testing two moderation effects: age moderating the relationship between SGH and NiPP (Hypothesis 2), and education moderating the same relationship (Hypothesis 3). The interaction for both models was significant (B = 0.009, Z = 6.557, p < 0.001, and B = –0.026, Z = –5.032, p < 0.001, respectively). The effect sizes for the moderators were small, with Part R2 = 0.015 for age and Part R2 = 0.013 for education. To interpret the moderation effects of age and education, simple slopes were plotted at low (1 SD below the mean) and high (1 SD above the mean) levels. As shown in Figure 2, for younger individuals, the relationship between SGH and NiPP was negative and significant (simple slope = –0.311, Z = –7.269, p < 0.001, Figure 2). However, for older individuals, this relationship was positive, but not significant (simple slope = 0.069, Z = 1.845, p = 0.069). These results supported for Hypothesis 2. Regarding the moderating effect of education, for individuals with fewer years of schooling, the relationship between SGH and NiPP was positive and not significant (simple slope = 0.044, Z = 1.029, p = 0.304, Figure 3). However, for those with more years of schooling, the relationship between SGH and NiPP was negative and significant (simple slope = –0.247, Z = –6.307, p < 0.001). As proposed by Hypothesis 2, the association between SGH and NiPP, such that association is stronger for those with higher education, further supporting this hypothesis.
Regression Results for Moderations.
Source: European Social Survey (2020). Own calculations.
N = 8994.
Discussion
This study focused on NiPP in southern European countries, examining how age and education moderate the relationship between SGH and NiPP in these countries. The results highlight the role of individual factors, such as age and education, in shaping this relationship. A significant moderating effect was observed for both factors, underscoring the importance of considering these variables when exploring the link between SGH and NiPP, especially in the context of the increasing trend of NiPP across Europe, particularly in southern countries. Although significant, the effect sizes were small. Nevertheless, the results indicate that younger people with poorer SGH tend to engage more in NiPP. Existing literature supports the notion that younger individuals with poorer health are more likely to engage in NiPP (Chen et al., 2023; Christensen et al., 2019; Couture and Breux, 2017; Söderlund and Rapeli, 2015). Younger people generally have greater access to the Internet and are more familiar with new technologies (Skocpol, 2004). In addition, they are at a stage in life where health issues are often temporary and have a lesser impact compared to older generations, who are more likely to suffer from chronic conditions and have a reduced capacity for full recovery (Couture and Breux, 2017; Franceschi et al., 2018). This relative resilience may make younger individuals more inclined to participate in non-institutional political activities, even when their health is compromised. For instance, they can easily engage in activities such as signing citizens’ initiatives or participating in online forums and demonstrations from the comfort of their homes (Christensen et al., 2019; Marien et al., 2010; Söderlund and Rapeli, 2015). In contrast, older adults, who are less familiar with new technologies and tend to have more disabling diseases, may find that illness has a closer association with reduced ability to participate in such activities.
Our findings reveal that the relationship between SGH and NiPP is moderated by education. For individuals with more years of schooling, the relationship between SGH and NiPP differs from those with fewer years of schooling. Among individuals with lower levels of education, better self-perceived health significantly increases the likelihood of engaging in NiPP. However, for those with more years of schooling, the perception of health is inversely related to NiPP participation. Despite the small effect size, the results align with the literature on NiPP, which suggests that education plays a role in the social stratification of emerging forms of political participation (Slavina, 2021; Stolle and Hooghe, 2011). Education reduces the negative impact of health on NiPP when it comes to donating money (Burden et al., 2017). Activities such as signing petitions, boycotting, and donating money are more accessible to individuals with higher incomes, which are often associated with higher levels of education (Slavina, 2021), as it is suggested by the key component of personal resources—socioeconomic status (Kirbiš et al., 2017; Verba et al., 1995)—in the CVM theoretical model. Furthermore, actions like posting political news online or signing petitions, which require Internet access, may exclude those without sufficient digital literacy (Marien et al., 2010; Skocpol, 2004; Stolle and Hooghe, 2011). Participation in boycotts, demonstrations, and volunteering also demands a certain level of knowledge and information that may be less accessible to those with lower levels of education (Marien et al., 2010; Stolle and Hooghe, 2011; Stolle et al., 2005). It is important to note that younger individuals are more likely to have higher levels of education, largely due to the expansion of higher education (Skocpol, 2004), which has been particularly relevant in southern European countries in the past decades (Capucha et al., 2016). The interplay between age, education, and NiPP is particularly relevant in these countries, where the expansion of universities and the democratization of education occurred more recently. Consequently, individuals who benefited from these educational advancements are likely to be more engaged in NiPP. Overall, these findings contribute to understanding how education and age influence individuals’ participation in NiPP, which is rising in southern European countries.
Recognizing these small but meaningful effects has important implications for policymakers, who should implement integrated policy approaches that address both health (e.g. integrating health and civic education into school curricula, creating civic education programs, or community mobilization efforts targeting underrepresented groups) and education (e.g. expanding lifelong learning opportunities for adults). These two factors serve as foundational pillars of democratic participation. Therefore, this study can contribute to a broader audience in political science and international relations, as the findings underscore that health constitutes an important dimension of inequality influencing democratic participation and inclusion, issues central to the study of politics and governance. The participation of citizens with lower education and poorer health in noninstitutional political activities is crucial for ensuring a more comprehensive representation of societal interests, leading to more responsive and accountable governance. When these groups are excluded from NiPP, their voices are absent from policy debates, weakening democratic resilience.
Limitations and Future Work
This study has several limitations, which also highlight opportunities for future research. First, NiPP was analyzed by combining multiple forms of participation into a single scale. While MCA indicated that these items could be meaningfully summarized in one dimension, this approach treats all acts as equivalent and does not capture variation in the intensity or type of participation. Certain predictors may influence specific forms of NiPP differently (Pacheco and Fletcher, 2015; Söderlund and Rapeli, 2015). For instance, participating in a demonstration or attending a party meeting may be more demanding, particularly for individuals in poor health, whereas wearing a campaign badge, boycotting products, or signing petitions presents fewer barriers. Future research should explore these different modes of political participation separately and consider cluster analyses to identify participation profiles based on health perception, age, and education. By categorizing individuals as participants or non-participants, differences across engagement types and levels are masked, which may attenuate associations with explanatory variables. Our goal was to capture broad engagement in NiPP (Christensen et al., 2019; Marien et al., 2010), but future studies could analyze specific acts individually (Slavina, 2021) or adopt alternative scaling strategies to account for heterogeneity and intensity of participation. Although statistically significant, effect sizes in our study were small. Nevertheless, these findings are consistent with prior research on NiPP, which also reports modest associations with individual-level factors (Christensen et al., 2019; Marien et al., 2010; Söderlund and Rapeli, 2015), reflecting the broader reality that complex social phenomena are shaped by multiple factors, often with small individual effects (Götz et al., 2022).
Another limitation is the cross-sectional nature of the data, which precludes causal inference. However, the study’s aim was to examine the moderating role of individual factors such as age and education in the relationship between NiPP and self-rated general health (SGH), which was successfully achieved. Future research could benefit from longitudinal designs to explore causal mechanisms and better understand how health and sociodemographic factors interact over time to shape patterns of NiPP.
Supplemental Material
sj-docx-1-psx-10.1177_00323217251401087 – Supplemental material for Subjective General Health and Non-institutional Political Participation: Do Age and Education Matter?
Supplemental material, sj-docx-1-psx-10.1177_00323217251401087 for Subjective General Health and Non-institutional Political Participation: Do Age and Education Matter? by Bruno Miguel Oliveira, Tiago Delgado Ribeiro and Helena Carvalho in Political Studies
Footnotes
Data Availability Statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The data used in this study were obtained from the European Social Survey (ESS), which adheres to strict ethical guidelines and procedures. The ESS has received ethical approval from the relevant national and institutional review boards in each participating country. As this study involves secondary data analysis, no additional ethical approval was required.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Tiago D. Ribeiro is supported by a grant from the Portuguese Foundation for Science and Technology (reference number 2023.03976.BD).
Supplemental Material
Additional Supplementary Information may be found with the online version of this article.
Table A1. Descriptive Statistics per Country.
Table A2. Self-Reported Non-institutional Political Participation in the Southern European Countries.
Table A3. Self-Reported General Health in the Southern European Countries.
Author Biographies
![]() .
.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.