
Abstract
Research on work-related trauma in criminal justice has focused on front-line officers, overlooking personnel such as analysts, secondary investigators, call takers, and forensic specialists, who are indirectly exposed to trauma. This systematic review synthesized 62 studies. Findings identified that supporting personnel face distress comparable to front-line staff, commonly experiencing Secondary Traumatic Stress, PTSD, and burnout. Risk factors included gender and low organizational support, while workplace social support and positive coping strategies, mitigated adverse outcomes. Negative coping strategies, including avoidance, exacerbated distress. Criminal justice settings need to recognize risk, foster effective coping mechanisms, and implement early interventions for supporting personnel.
Keywords
Law enforcement is widely regarded as one of the most stressful, high-strain professions (Cartwright and Roach, 2021; Duran et al., 2019; Gershon et al., 2009). Personnel are routinely exposed to potentially traumatic situations, including violent incidents and crime scenes, which threaten not only their physical health but also their psychological wellbeing (Gershon et al., 2009; Noblet et al., 2009). Consequently, law enforcement professionals are at elevated risk of cardiovascular conditions, substance misuse, suicide, and psychological disorders. For example, police personnel are approximately twice as likely (20%) to develop post-traumatic stress disorder (PTSD) compared to the general population (7–9%) (Carleton et al., 2018; Ménard and Arter, 2014; Syed et al., 2020).
Most research to date has focused on frontline officers, highlighting risks of PTSD, burnout, and other psychological disorders (Brewin et al., 2022; Duran et al., 2019; Ugwa and Idemudia, 2025). By contrast, non-public-facing roles, referred to in this review as secondary investigators and analysts (SIAs), have received comparatively less attention than front-line roles, despite a growing body of research. SIAs include crime analysts, intelligence officers, digital forensic examiners, investigative advisors, and forensic case reviewers. These professionals are indirectly exposed to traumatic experiences through repeated engagement with distressing material, including forensic evidence, investigative reports, and graphic digital media. Exposure occurs through multiple modalities—visual (e.g., reading crime reports), auditory (e.g., listening to call recordings), and audio-visual (e.g., reviewing videos in digital evidence)—and can elicit emotional and cognitive responses similar to those experienced by frontline officers (Duran and Woodhams, 2023). Although they are not directly exposed to traumatic experiences, cumulative and repeated exposure may still place SIAs at risk of psychological distress.
Indirect exposure can lead to secondary trauma (also called vicarious trauma, second-hand trauma, or indirect trauma), defined as emotional distress arising from engagement with individuals affected by primary trauma or trauma-related material (Baird and Jenkins, 2003; Figley, 1983). Secondary trauma can disrupt an individual’s sense of self, professional identity, and core beliefs regarding safety, trust, esteem, intimacy, and control (Saakvitne et al., 1996). It is increasingly recognized as a manifestation of secondary traumatic stress (STS) within the broader PTSD framework (American Psychiatric Association. (2022)), with symptoms mirroring PTSD, including hyperarousal, intrusive recollections, emotional numbing, avoidance behaviors, and burnout (Figley, 1995).
Despite growing recognition of secondary trauma, most reviews focus on frontline officers, often overlooking SIAs (Greinacher et al., 2019; Sherwood et al., 2019; Ugwu and Idemudia, 2025). When SIAs are included, they are frequently grouped with frontline staff, which can obscure distinctions in exposure type, role-specific stressors, and psychological outcomes (Cartwright and Roach, 2022; Foley et al., 2022; Ko and Memon, 2023). Such grouping risks underestimating the unique challenges associated with indirect exposure to trauma and limits our understanding of the factors that influence vulnerability and resilience. Evidence from the National Police Wellbeing Survey highlights role-specific differences in wellbeing, underscoring the importance of considering job responsibilities, exposure type, and individual characteristics when assessing psychological impact (Cartwright and Roach, 2021; Oscar Kilo, 2019). Foley et al. (2022) specifically recommended focusing on homogeneous populations to better understand how different roles affect trauma-related outcomes.
Given these gaps, this review aims to systematically synthesize literature on SIAs who are indirectly exposed to the traumatic experiences of others. The review has two core objectives: 1. To identify the types of psychological distress experienced by SIAs. 2. To examine potential risk and protective factors influencing these mental health outcomes.
By focusing exclusively on SIAs, this review seeks to illuminate the unique impact of indirect exposure to distressing material in non-public-facing roles, providing critical insight to guide organizational policy, targeted interventions, and future research. To date, no systematic review has addressed this population in isolation, and this review aims to fill this important gap.
Methods
The systematic literature review was conducted following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA; Haddaway et al., 2022) guidelines to identify all published studies investigating psychological distress experienced by SIAs who are indirectly exposed to trauma of others at work.
Search strategy
An electronic search strategy was collaboratively developed by the authors and a subject librarian to perform a forward search in bibliographic databases. The search terms used included: “secondary trauma*” OR “second hand trauma*” OR “indirect trauma*” OR “vicarious trauma*” OR “work related trauma*” AND “mental ill health*” OR “mental illness*” OR “psychological distress*” OR “wellbeing*” AND “police*” OR “law enforcement*” OR “secondary investigators” OR “analysts” OR “criminal justice*”.
Six electronic databases were searched: ProQuest Central, SCOPUS, OVID (including PsycINFO and MEDLINE), Web of Science, PubMed, and EBSCO/CINAHL, capturing studies published from 1926 to January 2026. Advanced searches used Boolean operators, truncation, and quotation marks to capture studies across three domains: secondary trauma, psychological distress, and SIAs. A manual secondary search of reference lists from eligible articles was conducted to identify additional relevant studies.
PEO framework
The search strategy was guided by the PEO (Population, Exposure, Outcome) framework, which is commonly used in reviews examining associations between exposures and outcomes. In this review, the population comprised law enforcement professionals working as SIAs, the exposure related to indirect contact with traumatic experiences of other people, and the outcomes included psychological distress, risk and protective factors associated with secondary trauma. This ensured the review remained focused on the types of distress experienced by SIAs and the factors influencing mental health.
Eligibility criteria
Inclusion criteria
Studies were included if they: (a) Involved law enforcement, police, or criminal justice professionals whose daily roles include indirect exposure to the trauma of others (e.g., analysts, investigative advisors, call takers, forensic examiners); (b) Reported empirical research on secondary, vicarious, or work-related trauma; and (c) Examined mental ill-health, psychological distress, or wellbeing.
Exclusion criteria
Studies were excluded if they: (a) Were not published in English; (b) Were reviews, editorials, commentaries, or other non-empirical publications; (c) Were not journal articles or theses; or (d) Included mixed samples of frontline and supporting personnel without separate analyses for SIAs
Data extraction
Full texts of eligible articles were reviewed by the first author, with data extracted using a standardized form including: author, year, target population and sample size, country, study design, risk and protective factors, and psychological distress outcomes. Selection based on inclusion and exclusion criteria was discussed collaboratively by both authors. A manual secondary search of reference lists was conducted to identify additional studies. Both authors reviewed all selected articles to ensure consensus for final inclusion.
Results
The search strategy yielded 11,087 results from six databases (see Figure 1). Of these, 11,051 records were removed because 432 were duplicates; 50 were not in English or were not journal articles or theses; 8622 focused on sectors outside law enforcement; 1859 did not focus on secondary trauma, 85 had front-line only samples and four were reviews (Cartwright and Roach, 2022; Foley et al., 2022; Key, 2021; Ko and Memon, 2023). Thirty-six papers were initially included in the review. The reference lists of these papers were examined, sourcing an additional 26 relevant papers. Therefore, a total of 62 papers were included in the final review. PRISMA flow chart.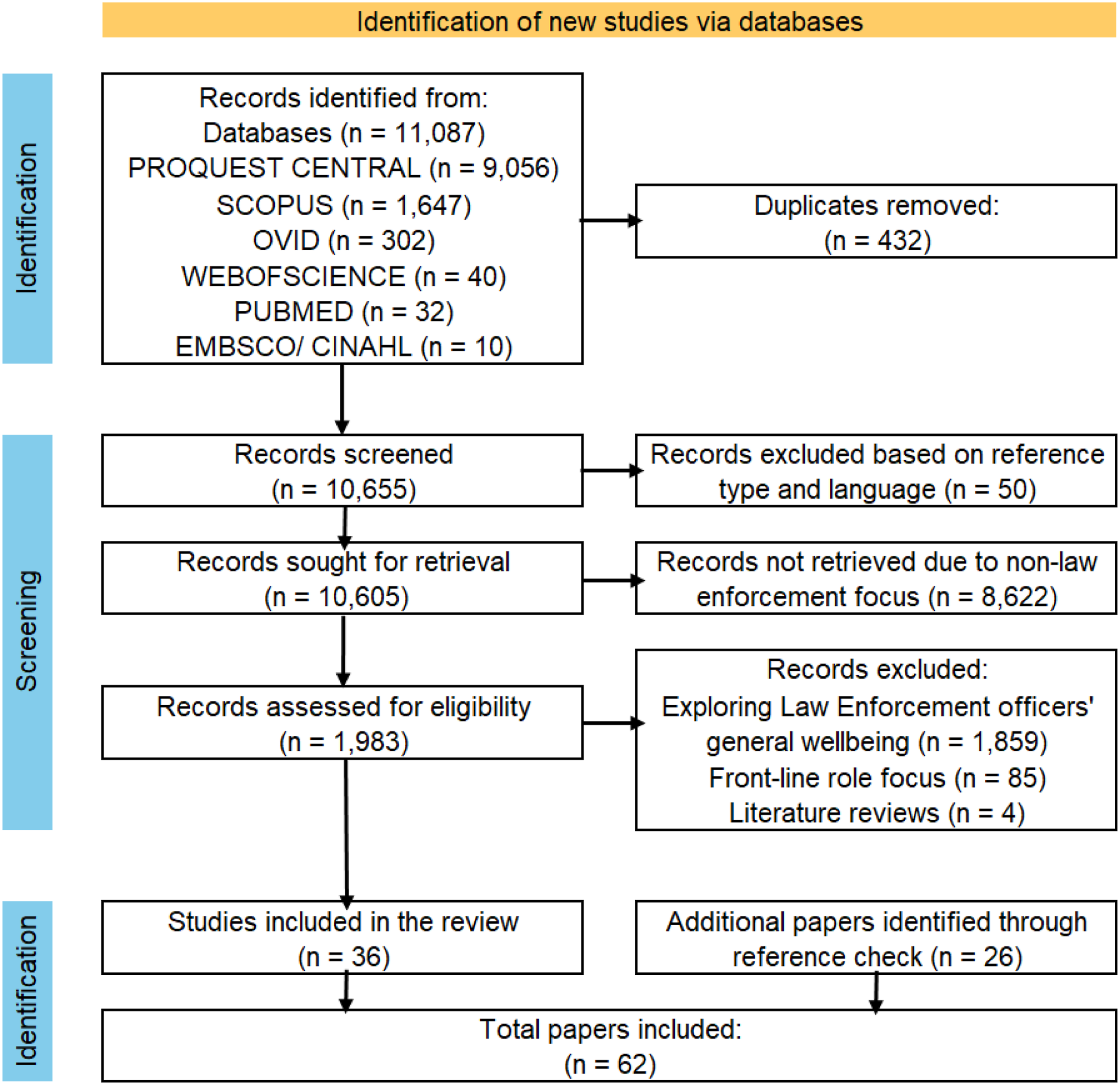
Study characteristics
Papers included in the Systematic Review.
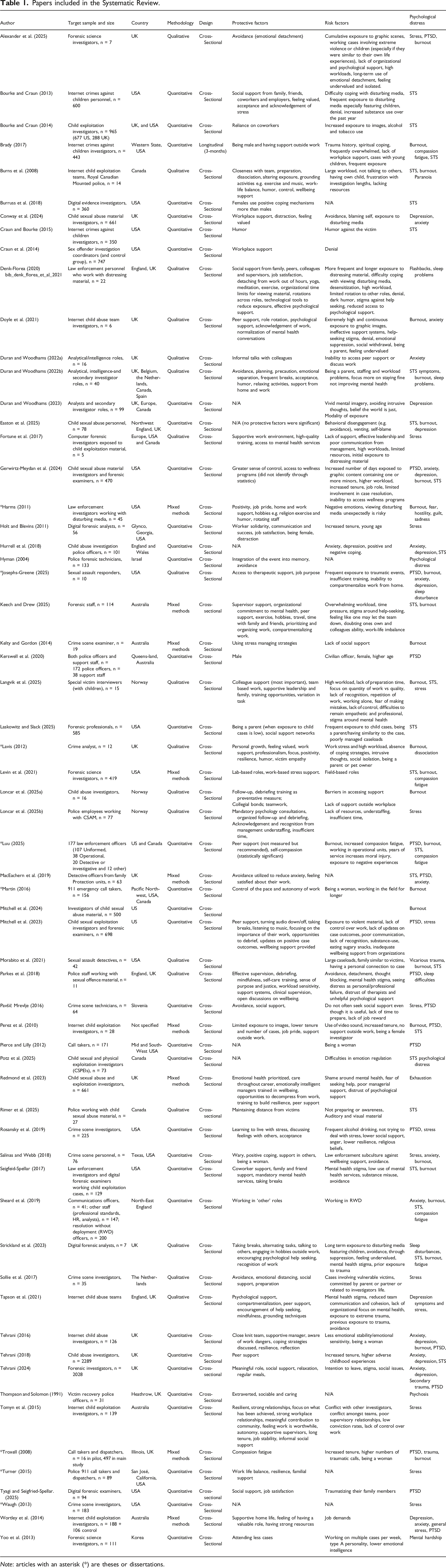
Note: articles with an asterisk (*) are theses or dissertations.
Psychological distress
Table 1 shows that psychological distress was commonly reported among SIAs exposed to traumatic experiences of other people. Only four studies found no link between indirect exposure and psychological distress (Craun et al., 2014; Thompson and Solomon, 1991; Tomyn, 2015; Waugh, 2013). Six primary mental health outcomes emerged: STS, PTSD, anxiety, depression, sleep disturbances, and burnout (see Figure 2). Psychological distress theme.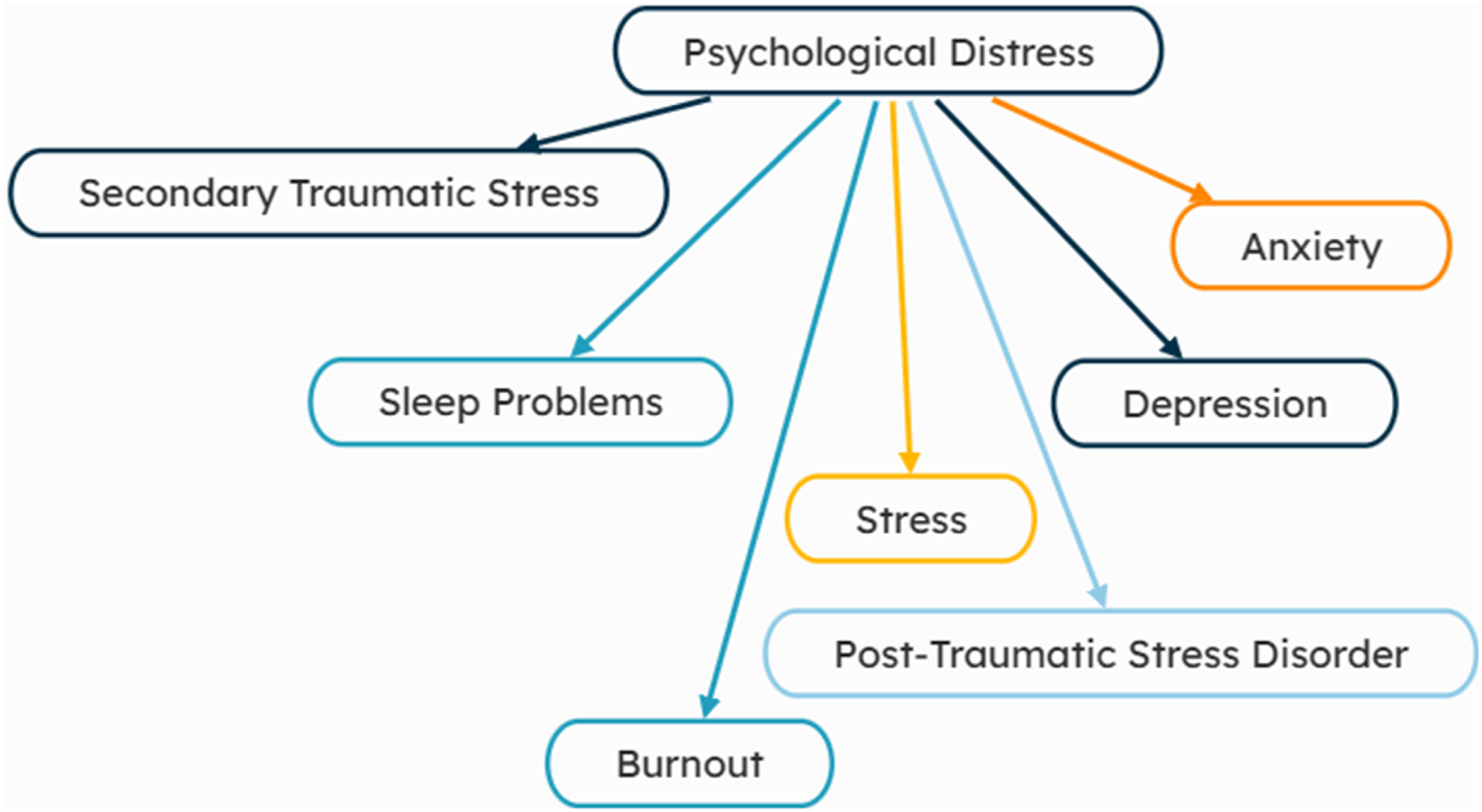
Secondary traumatic Stress (STS)
STS was reported in 25 studies (see Table 1: Bourke and Craun, 2013, 2014; Brady, 2017; Burns et al., 2008; Burruss et al., 2018; Craun and Bourke, 2014; Duran and Woodhams, 2022b; Easton et al., 2025; Gerwirtz-Meydan et al., 2024; Hurrell, 2018; Keech and Drew, 2025; Langvik et al., 2025; Laskowitz and Slack, 2025; Levin et al., 2021; Luu, 2025; MacEachern et al., 2019; Morabito et al., 2021; Perez et al., 2010; Potz et al., 2025; Rimer et al., 2025; Seigfeid-Spellar, 2017; Sheard et al., 2019; Strickland et al., 2023; Tehrani, 2018, 2024). Brady (2017) found that one in four professionals in internet child exploitation roles exhibited high STS, while MacEachern et al. (2019) reported over half of child abuse investigators experienced STS, with 11% at high-to-severe levels. Craun and Bourke (2015) noted that STS symptoms generally remained stable unless combined with risk factors, whereas some populations showed low or negligible STS (Harms, 2011; Hyman, 2004; Martin, 2016; Tehrani, 2018).
PTSD
Twenty-two studies linked PTSD to indirect exposure to trauma, particularly in child exploitation roles (see Table 1: Alexander et al., 2025; Bourke and Craun, 2014; Burns et al., 2008; Denk-Florea, 2020; Gerwirtz-Meydan et al., 2024; Josephs-Greene, 2025; Kerswell et al., 2020; Luu, 2025; MacEachern et al., 2019; Mitchell et al., 2023; Parkes et al., 2018; Pavšič Mrevlje, 2016; Perez et al., 2010; Pierce and Lilly, 2012; Rosansky et al., 2019; Strickland et al., 2023; Tehrani, 2016, 2024; Troxell, 2008; Tyagi and Seigfried-Spellar, 2025; Wortley et al., 2014; Yoo et al., 2013). Reported symptoms included denial (Bourke and Craun, 2014) and flashbacks (Burns et al., 2008; Denk-Florea, 2020; Strickland et al., 2023), with 3.5–17% of professionals experiencing clinically significant PTSD (Pavšič Mrevlje, 2016; Pierce and Lilly, 2012; Rosansky et al., 2019). One-third of child exploitation professionals reported intrusive thoughts (MacEachern et al., 2019). Kerswell et al. (2020) found higher PTSD in civilian support staff (13% clinically significant) than frontline officers, though Wortley et al. (2014) and Yoo et al. (2013) reported similar or lower prevalence among LE professionals compared to frontline staff.
Burnout
Twenty-two studies reported burnout among SIAs (See Table 1: Alexander et al., 2025; Bourke and Craun, 2014; Brady, 2017; Doyle et al., 2020; Duran and Woodhams, 2022b; Easton et al., 2025; Gerwirtz-Meydan et al., 2024; Harms, 2011; Josephs-Greene, 2025; Keech and Drew, 2025; Kelty and Gordon, 2014; Langvik et al., 2025; Lavis, 2012; Loncar et al., 2025a; Luu, 2025; Martin, 2016; Mitchell et al., 2024; Perez et al., 2010; Seigfeid-Spellar, 2017; Sheard et al., 2019; Strickland et al., 2023; Troxell, 2008). SIAs experienced significant burnout, with one in four feeling “miserable” and “cynical” (Duran and Woodhams, 2022b). Overall, burnout levels ranged from low to moderate (Brady, 2017; Harms, 2011; Perez et al., 2010). High prevalence was reported among internet child exploitation investigators (Brady, 2017; Perez et al., 2010), with concomitant STS. Police call handlers reported higher compassion fatigue, though some studies indicated lower burnout compared to frontline officers (Sheard et al., 2019; Troxell, 2008).
Anxiety
Eighteen studies reported anxiety following exposure to distressing material (See Table 1: Burns et al., 2008; Conway et al., 2024; Denk-Florea, 2020; Doyle et al., 2020; Duran and Woodhams., 2022a, 2022b; Gerwirtz-Meydan et al., 2024; Harms, 2011; Hurrell, 2018; Josephs-Greene, 2025; MacEachern et al., 2019; Salinas and Webb, 2018; Sheard et al., 2019; Strickland et al., 2023; Tehrani, 2016, 2018, 2024; Wortley et al., 2014). LE professionals experienced fear (Harms, 2011; Pierce and Lilly, 2012), paranoia (Burns et al., 2008; Denk-Florea, 2020; Strickland et al., 2023), and trust issues (Duran and Woodhams, 2022b; Tehrani, 2016, 2024). Burns et al. (2008) found heightened paranoia and protectiveness in internet child exploitation staff, while Harms (2011) attributed anxiety to disturbing media exposure. Higher anxiety and stress were reported compared to the general population, with police call handlers experiencing more distress (Duran and Woodhams, 2022b; MacEachern et al., 2019; Sheard et al., 2019).
Stress
Fifteen papers reported stress among SIAs (see Table 1). Child abuse investigators most commonly experienced stress (Fortune, 2017; Holt and Blevins, 2011; Langvik, 2025; Loncar, 2025b; Mitchell, 2023; Tapson, 2021; Tomyn, 2015), followed by crime scene and forensic investigators (Alexander, 2025; Pavšič Mrevlje, 2016; Rosansky, 2019; Salinas and Webb, 2018; Sollie, 2017; Waugh, 2013) and call takers (Turner, 2015). Stress often exceeded coping abilities and, if unmanaged, could lead to STS or burnout (Alexander, 2025; Holt and Blevins, 2011; Loncar, 2025b; Rosansky, 2019; Sollie, 2017). Some studies highlighted resilience, with protective factors mediating stress (Fortune, 2017; Mitchell, 2023; Turner, 2015). Internet child exploitation investigators displayed particularly strong coping (Tomyn, 2015). Other studies reported low stress (Salinas and Webb, 2018) or no link between stress and trauma exposure (Mitchell, 2023; Waugh, 2013).
Depression
Thirteen studies identified depression and related symptoms such as isolation, mood fluctuations, anger, and sadness (See Table 1: Burns et al., 2008; Conway et al., 2024; Duran and Woodhams, 2022a, 2022b, 2023; Easton et al., 2025; Harms, 2011; Hurrell, 2018; Josephs-Greene, 2025; Tapson et al., 2021; Tehrani, 2016, 2018; Wortley et al., 2014), particularly in child exploitation and abuse roles. Depression was linked to STS (Hurrell, 2018) and exposure to traumatic material (Duran and Woodhams, 2022a, 2022b, 2023; Harms, 2011). For instance, 25% of professionals reported feeling miserable and unable to trust others (Duran and Woodhams, 2022b), with 52% reporting moderate and 37% severe depression (Duran and Woodhams, 2023). Some professionals reported no emotional impact (Duran and Woodhams, 2022b; Harms, 2011).
Sleep problems
Twelve studies reported sleep disturbances (See Table 1: Burns et al., 2008; Denk-Florea, 2020; Duran and Woodhams, 2022b; Harms, 2011; Josephs-Greene, 2025; MacEachern et al., 2019; Parkes et al., 2018; Perez et al., 2010; Pierce and Lilly, 2012; Strickland et al., 2023; Tehrani, 2016; Yoo et al., 2013), including nightmares and difficulty sleeping. Disturbed sleep affected 50% of professionals (Duran and Woodhams, 2022b), and 26% of staff exposed to traumatic media reported high exhaustion (Harms, 2011). Forensic investigators often devalued sleep due to workload (Yoo et al., 2013). Links between sleep problems and other psychological symptoms were not formally examined.
Risk factors
A series of factors which increase the likelihood of experiencing psychological distress because of secondary trauma were identified; these can be split into individual and job-related risk factors.
Individual risk factors
Several individual risk factors have been identified in the literature as contributing to psychological distress, including demographic, personality, cognitive, and negative coping mechanisms. (Figure 3)
Demographic factors
Research on age as a risk factor for STS shows conflicting findings. Holt and Blevins (2011) suggest younger professionals may be at higher risk, whereas Kerswell et al. (2020) indicate older professionals could be more vulnerable. Gender-related risk factors also show inconsistencies. Some studies suggest being male increases risk (Harms, 2011; Salinas and Webb, 2018), while others indicate females may be more susceptible to STS and psychological distress (Kerswell et al., 2020; Martin, 2016; Perez et al., 2010; Pierce and Lilly, 2012; Tehrani, 2016; Troxell, 2008). Tenure also shows mixed effects; shorter tenure may increase risk (Yoo et al., 2013), while longer tenure may heighten vulnerability, potentially due to growing responsibilities (Gerwirtz-Meydan et al., 2024; Holt and Blevins, 2011; Luu, 2025; Martin, 2016; Perez et al., 2010; Tehrani, 2018; Troxell, 2008).
Personality factors
Personality traits influence susceptibility to STS and psychological distress (Duran and Woodhams, 2023; Thompson and Solomon, 1991; Yoo et al., 2013). Type A personalities, characterized by high stress and work-driven behavior, are more likely to experience distress (Yoo et al., 2013). Extraversion has been associated with mental stability (Thompson and Solomon, 1991), whereas the potential vulnerability of introverted individuals requires further research. Mental illness history may increase psychological distress risk (Brady, 2017; Sollie et al., 2017; Strickland et al., 2023; Yoo et al., 2013), though evidence relating to past trauma is mixed – some studies found no clear link to STS (Hurrell, 2018; Tehrani, 2018).
Cognitive factors
Cognitive processes, including intrusive thoughts and vivid mental imagery, contribute to psychological distress (Duran and Woodhams, 2023; Lavis, 2012). Intrusive thoughts, such as involuntarily replaying traumatic events, can heighten STS risk (Duran and Woodhams, 2023; Lavis, 2012). Vivid mental imagery may increase vulnerability to STS and depression, particularly when distressing memories are replayed in detail (Duran and Woodhams, 2023). Research on mental imagery is limited, and comparisons across studies are scarce.
Negative coping mechanisms
Negative coping mechanisms provide temporary relief but often exacerbate long-term distress. Substance use, particularly alcohol and tobacco, was commonly employed to manage stress, though it carried harmful consequences over time (Bourke and Craun, 2013, 2014; Burruss et al., 2018; Mitchell et al., 2023; Pierce and Lilly, 2012; Rosansky et al., 2019; Seigfeid-Spellar, 2017). Humor was sometimes used to avoid engagement with traumatic material, but it could inadvertently increase STS (Craun and Bourke, 2015; Denk-Florea, 2020).
Avoidance—including dissociation, denial, and precautionary behaviors—was the most frequently reported negative strategy (Alexander et al., 2025; Bourke and Craun, 2013, 2014; Burns et al., 2008; Conway et al., 2024; Craun et al., 2014; Denk-Florea, 2020; Doyle et al., 2020; Duran and Woodhams, 2022b, 2023; Easton et al., 2025; Harms, 2011; Holt and Blevins, 2011; Hyman, 2004; Lavis, 2012; MacEachern et al., 2019; Morabito et al., 2021; Parkes et al., 2018; Pavšič Mrevlje, 2016; Pierce and Lilly, 2012; Salinas and Webb, 2018; Seigfeid-Spellar, 2017; Sollie et al., 2017; Strickland et al., 2023; Tapson et al., 2021). While avoidance temporarily reduced anxiety, it suppressed trauma processing, increased hypervigilance, and often heightened long-term distress and burnout. Some SIAs also suppressed intrusive thoughts, which can increase psychological distress (Duran and Woodhams, 2023). Certain roles, such as crime scene professionals, relied heavily on avoidance and rarely engaged in positive coping strategies, further increasing psychological strain (Salinas and Webb, 2018).
Job-related risk factors
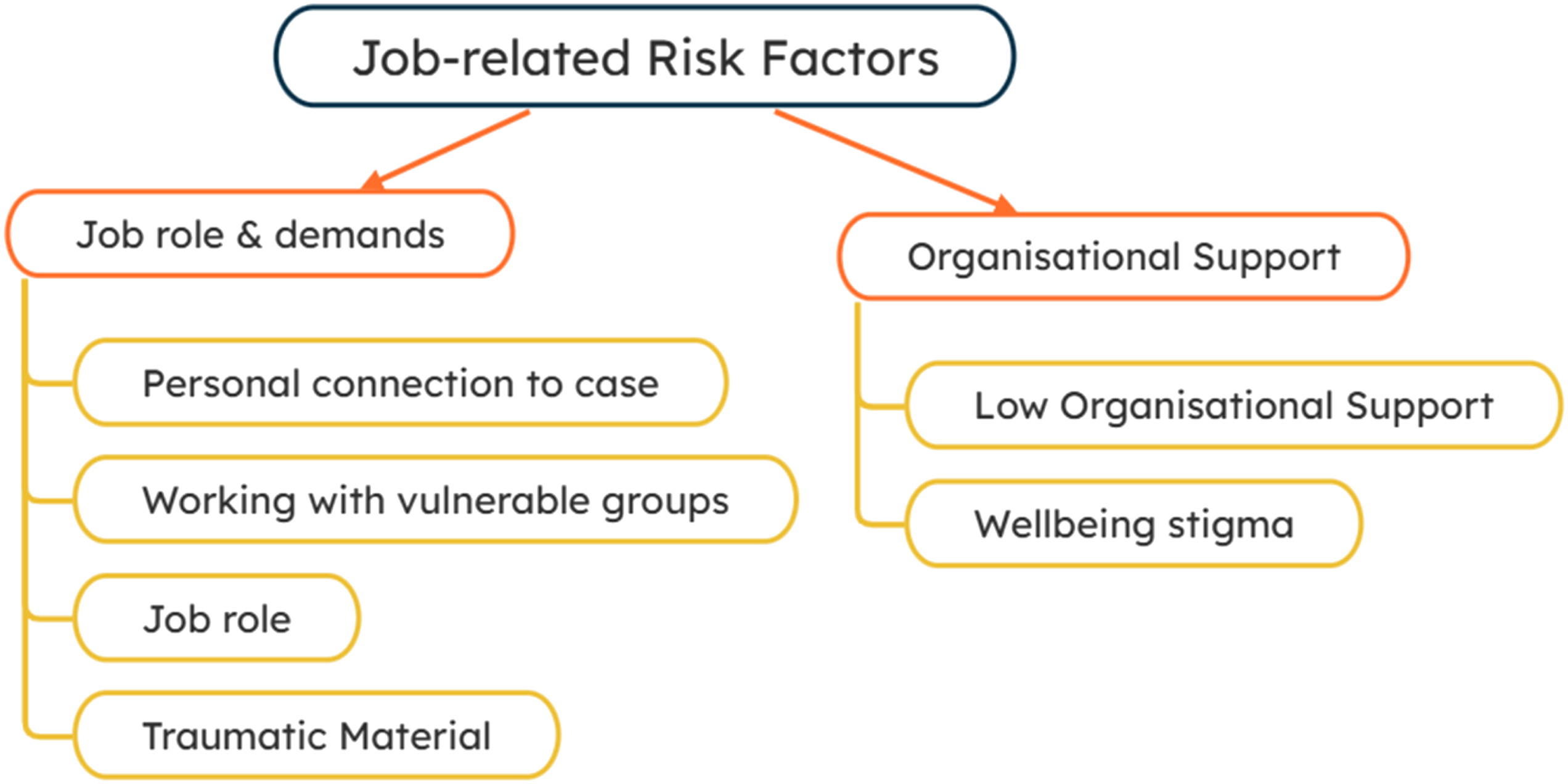
Job-related factors contributing to psychological distress can be broadly grouped into job role and demands, and organizational support factors. (Figure 4)
Job role and demands
Although psychological distress resulting from secondary trauma is widely discussed, only a few studies explicitly identify job role as a risk factor (Gerwirtz-Meydan et al., 2024; Kerswell et al., 2020; Levin, 2021; Luu, 2025; Sheard et al., 2019; Tehrani, 2018; Waugh, 2013; Wortley et al., 2014). Civilian staff in law enforcement and forensic roles tend to report higher levels of stress and STS (Kerswell et al., 2020; Sheard et al., 2019). Roles involving child exploitation further elevate the risk of psychological distress (Bourke and Craun, 2013; Tehrani, 2018; Wortley et al., 2014).
Having a personal connection or related life experiences to victims is another important risk factor (Alexander et al., 2025; Burns et al., 2008; Doyle et al., 2020; Duran and Woodhams, 2022b; Laskowitz and Slack, 2025; Lavis, 2012; Morabito et al., 2021; Sollie et al., 2017). SIAs in such situations may experience heightened anxiety and adopt avoidance strategies to cope (Duran and Woodhams, 2022b; Morabito et al., 2021). Detectives and forensic professionals with family or age-related similarities to victims report increased STS and psychological distress (Doyle et al., 2020; Laskowitz and Slack, 2025; Morabito et al., 2021), worrying their loved ones may become a victim or they may retraumatize their family members (Tyagi and Seigfried-Spellar, 2025)
Working with highly vulnerable populations, such as children, infants, and the elderly, also increases vulnerability to psychological distress (Alexander et al., 2025; Bourke and Craun, 2013; Brady, 2017; Doyle et al., 2020; Gerwirtz-Meydan et al., 2024; Sollie et al., 2017). These cases often involve complex emotional and ethical demands that intensify stress.
Exposure to traumatic material, including graphic images and disturbing case details, is a well-established risk factor (Alexander et al., 2025; Bourke and Craun, 2013, 2014; Brady, 2017; Burns et al., 2008; Conway et al., 2024; Denk-Florea, 2020; Doyle et al., 2020; Gerwirtz-Meydan et al., 2024; Hurrell, 2018; Josephs-Greene, 2025; Kelty and Gordon, 2014; Mitchell et al., 2023; Morabito et al., 2021; Strickland et al., 2023; Tapson et al., 2021; Troxell, 2008; Wortley et al., 2014; Yoo et al., 2013). Increased volume and intensity of exposure are linked to higher STS, particularly among child exploitation workers (Alexander et al., 2025; Burns et al., 2008; Denk-Florea, 2020; Doyle et al., 2020; Hurrell, 2018; Strickland et al., 2023; Tapson et al., 2021). Similarly, call takers and crime scene examiners are more susceptible to burnout due to high caseloads (Kelty and Gordon, 2014; Troxell, 2008). Greater exposure is associated with elevated anxiety, stress, depression, and PTSD (Wortley et al., 2014; Yoo et al., 2013). However, a study of computer-based forensic investigators found initial exposure to distressing material was associated with stress, but that exposure over time did not have a negative effect (Fortune et al., 2017).
Organizational support factors
Low organizational support is one of the most frequently cited risk factors for psychological distress (Alexander et al., 2025; Brady, 2017; Burns et al., 2008; Denk-Florea, 2020; Doyle et al., 2020; Duran and Woodhams, 2022a, 2022b; Fortune et al., 2017; Gerwirtz-Meydan et al., 2024; Harms, 2011; Josephs-Greene, 2025; Keech and Drew, 2025; Kelty and Gordon, 2014; Langvik et al., 2025; Laskowitz and Slack, 2025; Lavis, 2012; Loncar et al., 2025b; Mitchell et al., 2023; Morabito et al., 2021; Redmond et al., 2023; Rosansky et al., 2019; Strickland et al., 2023; Tapson et al., 2021; Tehrani, 2024; Tomyn et al., 2015; Wortley et al., 2014). Factors such as insufficient resources, high workloads, deadline pressures, inability to control work, inadequate staffing, and lack of recognition contribute to stress and STS. Low organizational support can also manifest as poor peer support, ineffective leadership, team conflict, and professional isolation (Doyle et al., 2020; Fortune et al., 2017; Redmond et al., 2023; Tapson et al., 2021; Tomyn et al., 2015).
A subculture against accessing wellbeing support has been observed in law enforcement (Salinas and Webb, 2018). This may prevent professionals from addressing stress and prioritizing their mental health, leading them to focus on “staying fine” rather than seeking help (Denk-Florea, 2020; Doyle et al., 2020; Duran and Woodhams, 2022b; Gerwirtz-Meydan et al., 2024; Keech and Drew, 2025; Langvik et al., 2025; Loncar et al., 2025a; Parkes et al., 2018; Redmond et al., 2023; Rosansky et al., 2019; Seigfeid-Spellar, 2017; Strickland et al., 2023; Tapson et al., 2021; Tehrani, 2024).
Protective factors
Protective factors are those that reduce the likelihood of psychological distress among SIAs exposed to indirect trauma. These factors can be grouped into individual characteristics, social support, work-related strategies, and adaptive coping mechanisms, see Figure 5. Individual risk factors. Job-related risk factors. Protective factors.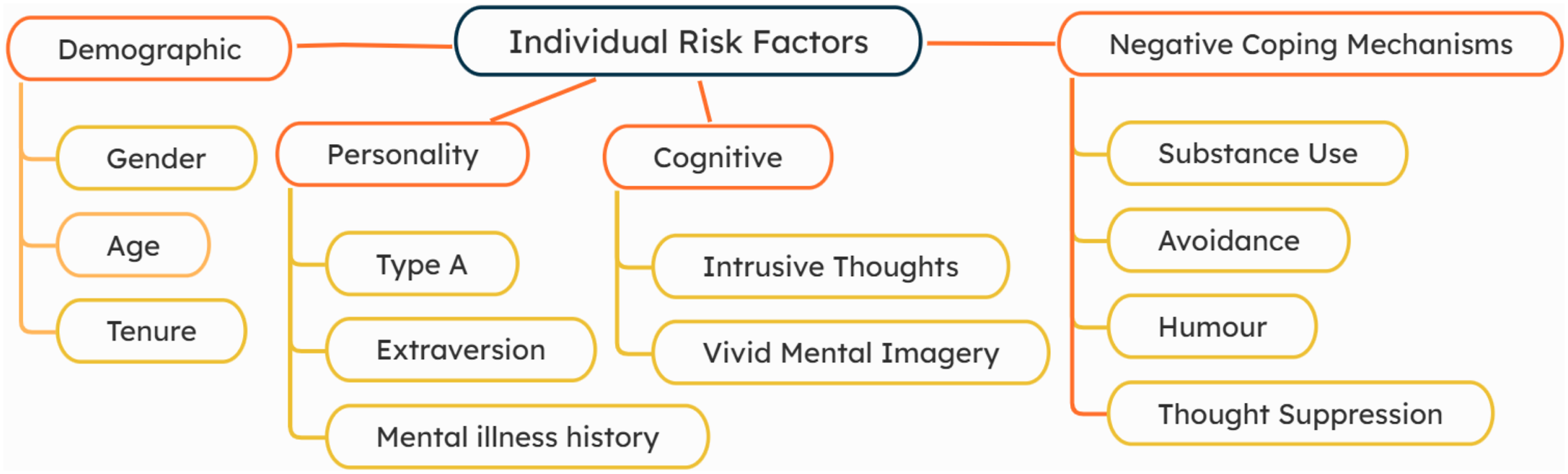
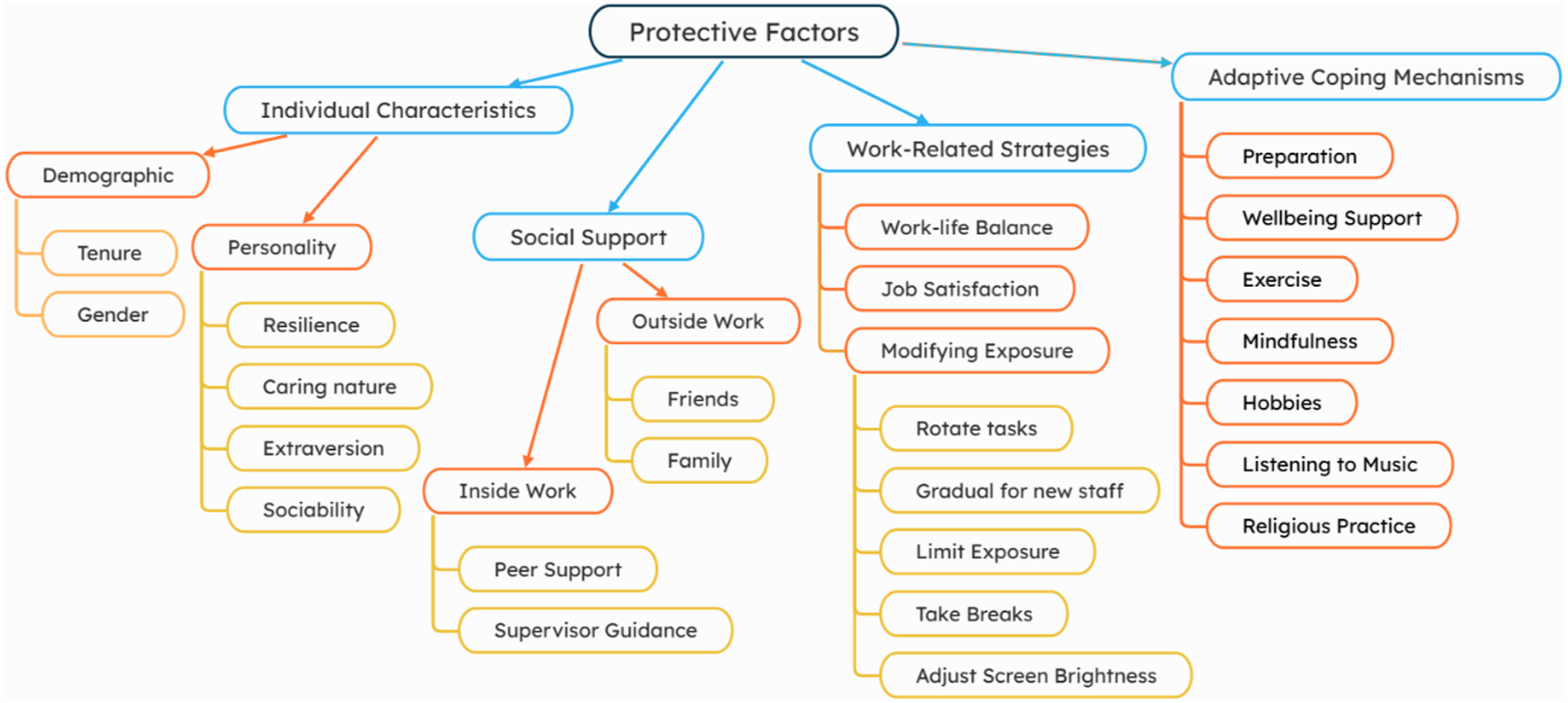
Individual characteristics
Certain demographic and personality factors appear to be protective. Being male was associated with lower STS, although the reasons remain unclear (Bourke and Craun, 2014; Brady, 2017). Protective personality traits, such as extroversion, sociability, resilience, and caring nature, enhance coping with workplace stress (Thompson and Solomon, 1991; Tomyn et al., 2015). One study found longer tenures are protective, potentially because of increased job stability (Tomyn et al., 2015), but length of tenure was also associated with risk.
Social support
Social support is consistently identified as protective, both within and outside the workplace. Workplace support included supervisory guidance, peer conversations, worker solidarity, and close-knit teams, particularly in high-risk roles such as internet child exploitation (Bourke and Craun, 2013; Burns et al., 2008; Conway et al., 2024; Craun et al., 2014; Denk-Florea, 2020; Doyle et al., 2020; Duran and Woodhams, 2022a, 2022b; Harms, 2011; Holt and Blevins, 2011; Keech and Drew, 2025; Langvik et al., 2025; Lavis, 2012; Luu, 2025; Parkes et al., 2018; Redmond et al., 2023; Seigfeid-Spellar, 2017; Strickland et al., 2023; Tapson et al., 2021; Tehrani, 2016, 2024; Tomyn et al., 2015; Tyagi and Seigfried-Spellar, 2025). Support from family and friends outside of work also protected against STS (Bourke and Craun, 2013; Brady, 2017; Denk-Florea, 2020; Duran and Woodhams, 2022b; Langvik et al., 2025; Perez et al., 2010; Seigfeid-Spellar, 2017; Turner, 2015; Wortley et al., 2014). Notably, some studies reported that SIAs did not always utilize available workplace support despite recognizing its benefits (Burns et al., 2008; Pavšič Mrevlje, 2016).
Work-related strategies
Maintaining a work-life balance helped reduce stress, decompress from work and improve life satisfaction (Burns et al., 2008; Denk-Florea, 2020; Keech and Drew, 2025; Redmond et al., 2023; Strickland et al., 2023; Turner, 2015). Other strategies involved modifying exposure to distressing content, e.g. by limiting exposure, taking breaks, adjusting screen brightness, rotating tasks, or gradually introducing new staff. Such practices reduced symptoms of STS and supported coping (Burns et al., 2008; Denk-Florea, 2020; Doyle et al., 2020; Duran and Woodhams, 2023; Harms, 2011; Mitchell et al., 2023; Perez et al., 2010; Rimer et al., 2025; Seigfeid-Spellar, 2017; Troxell, 2008; Yoo et al., 2013).
Job satisfaction also served as a protective factor. Feeling valued, motivated, and that one’s work was meaningful reduced risk (Bourke and Craun, 2013; Conway et al., 2024; Denk-Florea, 2020; Doyle et al., 2020; Harms, 2011; Holt and Blevins, 2011; Josephs-Greene, 2025; Lavis, 2012; Loncar et al., 2025b; MacEachern et al., 2019; Mitchell et al., 2023; Parkes et al., 2018; Pavšič Mrevlje, 2010; Perez et al., 2010; Strickland et al., 2023; Tehrani, 2024; Tomyn et al., 2015; Tyagi and Seigfried-Spellar, 2025; Wortley et al., 2014). SIAs often do not hear about the outcomes of the cases they are working on but have reported that positive case updates are important to their job satisfaction (Mitchell et al., 2023).
Adaptive coping mechanisms
Adaptive coping mechanisms facilitate processing of traumatic material, promote resilience, and support wellbeing. Protective strategies reported by SIAs included mental and physical preparation (Burns et al., 2008; Duran and Woodhams, 2022b), accessing wellbeing support and debriefing (Burns et al., 2008; Denk-Florea, 2020; Doyle et al., 2020; Fortune et al., 2017; Gerwirtz-Meydan et al., 2024; Josephs-Greene, 2025; Keech and Drew, 2025; Loncar et al., 2025a, 2025b; Mitchell et al., 2023; Redmond et al., 2023; Seigfeid-Spellar, 2017; Strickland et al., 2023; Tapson et al., 2021), exercise (Burns et al., 2008; Denk-Florea, 2020; Harms, 2011; Keech and Drew, 2025), mindfulness and relaxation activities promoting optimism, reflection, and acceptance (Bourke and Craun, 2013; Duran and Woodhams, 2022b; Parkes et al., 2018; Rosansky et al., 2019; Salinas and Webb, 2018; Tapson et al., 2021; Tehrani, 2016, 2024), hobbies (Harms, 2011; Keech and Drew, 2025; Strickland et al., 2023), listening to music (Burns et al., 2008; Mitchell et al., 2023), and religious practices, although some studies linked these to higher STS (Brady, 2017; Harms, 2011; Rosansky et al., 2019). Despite these benefits, accessing psychological support was often limited by a law enforcement subculture that discouraged help-seeking (Salinas and Webb, 2018).
Discussion
This discussion synthesizes evidence to address the review’s core objectives: to identify the types of psychological distress experienced by SIAs exposed to distressing material and to examine risk and protective factors influencing mental health outcomes in this population. Consistent with most studies, SIAs experience a range of mental health difficulties, most commonly STS, PTSD, anxiety, depression, sleep disturbances, and burnout. STS was particularly prevalent among analysts working with child exploitation material. Although levels were generally stable over time, high workload, frequent exposure, and low organizational support exacerbated symptoms (Craun et al., 2014; Duran and Woodhams, 2023). Some evidence indicated higher PTSD prevalence in SIAs compared to other law enforcement personnel (Kerswell et al., 2020), suggesting that indirect exposure alone can produce clinically significant distress. Anxiety and depression manifested as heightened fear, social withdrawal, and paranoia, while sleep disturbances—including nightmares and insomnia—further compounded distress (Duran and Woodhams, 2022b; Yoo et al., 2013). Burnout and compassion fatigue were also prevalent, particularly among child exploitation investigators and call handlers (Sheard et al., 2019), indicating that sustained exposure to distressing material—even without direct interaction with victims—can lead to emotional exhaustion and reduced occupational functioning.
Risk factors for psychological distress
A range of individual and job-related risk factors were identified as contributors to psychological distress among SIAs. Individual factors such as gender and age were inconsistently associated with distress. Some studies suggested males were at higher risk, while others indicated females were more vulnerable (Harms, 2011; Kerswell et al., 2020). This inconsistency suggests that individual characteristics interact with organizational and contextual variables rather than serving as stable predictors. Cognitive factors, including mental imagery, were largely underexplored (Duran and Woodhams, 2023), highlighting an important gap for future research.
Job-related factors were more consistently associated with distress. These included job roles, frequent exposure to distressing material, engagement with cases resembling personal experiences, work with vulnerable victims, stigma surrounding mental health, and, most prominently, low organizational support. High workloads, deadline pressures, and inadequate staffing further exacerbated psychological distress. The robustness of these findings underscores the central role of organizational factors in shaping SIAs’ mental health.
Furthermore, maladaptive coping strategies—including avoidance, emotional suppression, substance misuse, and humor—were also commonly reported. Avoidance emerged as the most prevalent maladaptive strategy (Salinas and Webb, 2018) and is consistent with both Ehlers and Clark (2000) and Woodhams and Duran (2024) models, which posit that avoidance impedes trauma processing and perpetuates psychological distress. Findings suggest coping strategies function as mechanisms through which both risk and protective factors influence mental health outcomes, underscoring the importance of interventions that promote adaptive coping while reducing reliance on avoidance.
Protective factors and resilience
Several protective factors help mitigate the impact of indirect trauma exposure among SIAs. Social and peer support was most consistently identified (Burns et al., 2008; Craun et al., 2014; Harms, 2011), though its accessibility was often limited by workplace stigma and culture. Individual characteristics, such as personality traits and gender, were occasionally reported as protective, but the evidence was limited and inconsistent (Bourke and Craun, 2014; Brady, 2017; Tomyn et al., 2015).
Adaptive coping strategies also contributed to resilience. These included seeking social support, gradual exposure or mental preparation, physical exercise, relaxation, hobbies, listening to music, optimism, and religious practices. Social support via peers was the most frequently reported protective factor, but its effectiveness was often constrained by organizational culture.
Several protective factors, particularly modifiable organizational factors—such as opportunities for collegial interaction and support for work–life balance—offer practical avenues for intervention. These findings suggest that workplace-based strategies can play a crucial role in fostering resilience and reducing the psychological impact of indirect trauma.
Implications for policy and practice
The evidence points to clear targets for organizational intervention. Low organizational support, workload pressures, and stigma are robust predictors of distress, indicating the need for systemic solutions. Practical strategies include manageable workloads, adequate staffing, role clarity, and recognition of analytical work.
Peer support, while protective, is often underutilized due to cultural and structural barriers. Organizations should implement structured support mechanisms, such as reflective supervision, peer mentoring, and psychologically informed leadership, to normalize help-seeking and enhance accessibility.
Given the prevalence of maladaptive coping, training programs should emphasize adaptive coping strategies, including emotional regulation, gradual exposure, and trauma-processing techniques. Embedding such programs in professional development can mitigate cumulative stress (Duran and Woodhams, 2022).
Finally, modifiable workplace factors—such as fostering collegial interaction and supporting work–life balance—offer tangible targets for intervention. Together, these measures indicate that safeguarding SIAs’ mental health requires organizational commitment, rather than relying solely on individual resilience.
Strengths and limitations of the review
This review is the first to synthesize evidence exclusively on law enforcement professionals working as SIAs, enabling a more nuanced understanding of how indirect exposure to traumatic material affects individuals in non-public-facing roles. A key strength lies in the rigorous methodology, including comprehensive searches across six databases and supplementary manual searches.
However, several limitations should be acknowledged. Variability in how studies defined law enforcement personnel may have limited comparability, and the range of professional roles included across studies may also introduce heterogeneity. For example, roles such as victim interviewers, call takers, and digital analysts may experience different types, modalities, and intensities of exposure to traumatic material, ranging from direct interaction with victims to secondary exposure through digital or recorded content. As a result, experiences of exposure may not be directly comparable across occupational groups, which should be considered when interpreting the findings of this review. Additionally, the exclusion of non-English publications and grey literature may have resulted in the omission of relevant findings. Despite these limitations, the review provides a robust foundation for understanding psychological distress and resilience among SIAs.
Conclusion
Indirect exposure to traumatic material is sufficient to produce substantial psychological distress among SIAs. While individual risk factors remain inconsistent, organizational factors—including low support, high workload, and stigma—consistently influence outcomes. Protective factors, particularly social support, alongside adaptive coping strategies, offer actionable avenues for intervention. Future research should focus on longitudinal, cross-cultural studies, and evaluate organizational and coping-focused interventions to safeguard the wellbeing and occupational effectiveness of SIAs exposed to secondary trauma.
Footnotes
Author note
*Please note: the research was conducted at the University of Birmingham, but the first author has moved to a new institution since completing this research. Cullen’s current affiliation is: Centre for Regional Economic and Social Research, Sheffield Hallam University, Sheffield, S1 2LX
Ethical considerations
This systematic review does not require ethical approval.
Author contributions
Both authors collaboratively decided the aims and search criteria. NC searched the databases, filtering articles via the inclusion and exclusion criteria. Relevance of articles was checked by FD. Full text of relevant articles was read by NC to populate ![]() and identify themes. These themes were collaboratively confirmed. NC drafted the report, tables and figures which were then reviewed and added to by FD. Both authors were involved in all stages of the report creation.
and identify themes. These themes were collaboratively confirmed. NC drafted the report, tables and figures which were then reviewed and added to by FD. Both authors were involved in all stages of the report creation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Not applicable as this is a systematic review, no original datasets were generated or analyzed
*Included in the review.