
Abstract
The mental health and wellness (MHW) of police officers is a global concern. Although many individual-level programs have been implemented in recent years to help officers cope with traumatic events, these initiatives overlook the structural-level conditions that frame how MHW is perceived in police organizations. Drawing on police culture and social identity theory, this paper argues that progress requires attention to three areas: restructuring expectations surrounding MHW in policing, redefining perceptions of officers with MHW concerns, and realigning leadership practices to prioritize organizational MHW.
Introduction
On July 31, 2018, Ontario Provincial Police (OPP) Sergeant Sylvain Routhier took his life after a battle with post-traumatic stress disorder (PTSD) (Routhier, 2021). According to a posthumous memoir written by his wife, Sylvain had been employed as a police officer for 14 years and was described as someone who demonstrated what a remarkably successful career in policing could look like. He was beloved by his family, colleagues, and the members of the communities where he lived, volunteered, and worked. Sylvain maintained a strong passion for being a police officer, even as he began to struggle with the emotional and psychological tolls his profession invoked. He had taken the initiative to seek help from family members and mental health professionals, but kept the weight of his suffering concealed from others and, most notably, from his fellow police officers. By the end of 2018, an additional seven actively employed police officers and one retired police officer died by suicide in Ontario, Canada, raising concern that the policing profession was entering a mental health and wellness crisis (Ministry of the Solicitor General, 2024).
Canada is not unique in dealing with this issue, as the mental health and wellness of police officers has become an increasing concern across a variety of diverse locales, including Great Britain, Ireland, and the United States of America (Krishnan et al., 2022). In turn, the need to provide police officers with education, training, policies, and interventions pertaining to their mental health and wellness has become both recognized and advocated for (Cohen et al., 2019; Grupe, 2023; Schuster and Ross, 2019). Police organizations have begun to implement various measures to enhance the mental health and wellness of their employees, examples of which include resilience training (Janssens et al., 2021; Van Der Meulen et al., 2018b), emotional intelligence and mental strength training (Blumberg et al., 2019; Van Der Meulen et al., 2018a), mindfulness (Cohen et al., 2019; Papazoglou and Andersen, 2014), trauma-informed practice (Blumberg et al., 2020; Lathan et al., 2019), and self-check techniques (Blumberg et al., 2020; Cohen et al., 2019; Schuster and Ross, 2019). Despite these efforts, police officers remain hesitant to utilize these resources for fear of the stigma that has been pervasively associated with frontline responders seeking and accessing help for concerns related to mental health and wellness (Bikos, 2021; Bullock and Garland, 2018; Edwards and Kotera, 2020; Karaffa and Koch, 2016).
The culture that underscores policing has routinely been posited as the predominant source of police officers’ reticence to use mental health and wellness resources due to its emphasis on bravery, resilience, and strength (Bikos, 2021; Bullock and Garland, 2018; Grupe, 2023; Karaffa and Koch, 2016). Admitting to struggling with mental health and wellness may be perceived as incongruent with a cultural climate where police officers are expected to exercise a high degree of management over their emotions at all times (Bikos, 2021; Grupe, 2023; Jackson and Theroux, 2023). Research on the mental health and wellness of police officers has consequently illuminated the need to reframe how police culture shapes such issues (Bell and Eski, 2016; Bikos, 2021; Cohen et al., 2019).
While scholars have offered theoretically sound explanations for why mental health and wellness remain a taboo topic in policing, few have attempted to draw on theory to guide how this issue might be addressed or improved (e.g., Bullock and Garland, 2020; Ricciardelli et al., 2021). To begin to address this gap in the literature, we first briefly explore the state of police officer mental health and wellness. Next, we discuss police culture and social identity theory to set the stage for our argument. The goal of this paper, then, is to demonstrate how combining police culture and social identity theory can offer a meso-level theoretical framework for creating an institutional atmosphere that is supportive of police officer mental health and wellness through three key strategies: (1) restructuring expectations surrounding mental health and wellness paradigms in policing; (2) redefining perceptions of police officers who experience mental health and wellness concerns; and (3) realigning leadership practices to prioritize organizational mental health and wellness. Although our argument is theoretical and in need of further empirical evidence, we highlight that if a cultural shift can occur, the stigma surrounding mental health and wellness may be reduced, motivating police officers to seek out and utilize available resources while mitigating feelings of alienation or unacceptance for doing so. These changes may help police organizations address the current disconnect that exists between what is perceived to be the “ideal” police officer, founded on the notion of mental toughness, and the realities of what a career in policing truly entails, which is that experiencing mental health injuries is not only normal but to be expected.
Police officer mental health and wellness
Stress within the working environment of police officers is frequently divided into two categories: operational and organizational stressors (Cohen et al., 2019; Duran et al., 2019; Ricciardelli et al., 2021; Tuckey et al., 2012). Operational stressors pertain to stressful events that are directly related to the day-to-day context of police work and, depending on the situation, can be dependent on the rank, role, or unit in which an officer works (Duran et al., 2019; Ricciardelli et al., 2021; Tuckey et al., 2012). Examples of operational stressors include arresting suspects, being verbally and physically harassed or assaulted, delivering death notices, employing use of force, feeling unable to help someone in a trying situation, ordeals with external branches of the judicial system, and/or receiving criticism from the media (Duran et al., 2019; Ricciardelli et al., 2021; Tuckey et al., 2012). Organizational stressors concern the bureaucratic elements of police work and can encompass the expectations, norms, and politics within the policing profession (Duran et al., 2019; Ricciardelli et al., 2021; Tuckey et al., 2012). Examples of organizational stressors include a lack of support from management or colleagues, a sense of inequality within the police organization, perceptions of favouritism, bullying, insufficient equipment or resources, policy changes, and the culture of policing itself (Duran et al., 2019; Gavin and Porter, 2025a; Ricciardelli et al., 2021; Tuckey et al., 2012).
Responses to operational and organizational stressors can be either acute or chronic (Cohen et al., 2019; Stinchcomb, 2004; Waters and Ussery, 2007). Acute stress generally develops in response to major events that have an instantaneous or unexpected onset and are usually short in duration (Cohen et al., 2019; Stinchcomb, 2004; Waters and Ussery, 2007). Chronic stress typically results from cumulative exposure to routine or mundane stressors over a prolonged period (Cohen et al., 2019; Stinchcomb, 2004; Waters and Ussery, 2007). When left unaddressed or untreated, these stressors place police officers at an elevated likelihood for the development of various mental health and wellness concerns, including anxiety, depression, posttraumatic stress, alcohol and/or substance use, and suicide (Bullock and Garland, 2018; Edwards and Kotera, 2020; Velazquez and Hernandez, 2019).
As noted previously, police organizations have responded to the proliferation of mental health and wellness concerns with a wealth of programs, but despite these measures,. statistics routinely illustrate that the problem only appears to be worsening over time (Dubord and Corley, 2026; Kamkar et al., 2020). For example, in Canada, over the last 15 years, sick leave has increased 184% in the Royal Canadian Mounted Police (RCMP) (Marfo, 2025). Comparatively, in the United Kingdom, there were over 17,000 police officers off work for various mental health reasons between 2024 and 2025, up 22% from the previous year (Ford, 2025). These figures insinuate that individual-level programs have not had the intended effect of improving the mental health and wellness of police officers, highlighting the need for more structural-level changes that directly challenge the cultural landscape of police organizations (Dubord and Corley, 2026).
Police culture
Police culture can be defined as a compilation of shared attitudes, beliefs, and values that dictate the norms and expectations of policing (Campeau, 2019; Cenk Demirkol and Nalla, 2020; Loftus, 2010; Paoline, 2003). In this sense, police culture functions as an internal resource that helps to guide police officers in performing daily activities such as maintaining an acceptable work ethic, interacting with colleagues and members of the public, navigating the hierarchical system of the police organization, completing tasks proficiently and promptly, as well as engaging with community agencies both inside and outside of the criminal justice system (Campeau, 2019; Cenk Demirkol and Nalla, 2020; Loftus, 2010; Paoline, 2003). Police culture is often operationalized using a myriad of conventional traits, including authoritarianism, bravery, conservativism, cynicism, hypervigilance, loyalty, machismo, pragmatism, secrecy, suspicion, as well as a mission-oriented focus and a propensity for danger (Campeau, 2019; Cenk Demirkol and Nalla, 2020; Loftus, 2010; Paoline, 2003).
Police organizations will commonly refine elements of police culture to fit the context of their work environment, which often differ considerably from one another with respect to their size, geographical location, sociodemographic composition, crime index, as well as their institutional leadership and management (Cordner, 2016; Ricciardelli et al., 2021; Van Maanen, 1973). These differences may be further extended by the idiosyncratic styles of policing that exist across organizations, which are moulded by the governmental bodies that oversee them (Cordner, 2016). Police officers are also likely to have anomalous interpretations of police culture that are dependent on their work experience, unit, and rank (Cenk Demirkol and Nalla, 2020; Cordner, 2016; Reiner, 2010; Terrill et al., 2003). Police chiefs, captains, lieutenants, sergeants, instructors, and frontline officers differ in terms of the expectations they are held to, the roles they fulfill, and the duties that they must complete (Cenk Demirkol and Nalla, 2020; Cordner, 2016; Reiner, 2010; Terrill et al., 2003). Regardless of these differences, it is undeniable that police culture fosters a sense of unity among police officers, deeply rooted in their shared experiences and interpretations of the world (Cenk Demirkol and Nalla, 2020; Kurtz and Upton, 2018; Ricciardelli et al., 2021; Sklansky, 2007).
Police culture plays an important role in determining what work events are classified as traumatic versus which are trivialized (Waters and Ussery, 2007). Irrespective of the situations that police officers find themselves in, there is a ubiquitous understanding that the expression of stress-related emotion is largely inappropriate (Bell and Eski, 2016; Bikos, 2021; Edwards and Kotera, 2020; Waters and Ussery, 2007). Displays of emotion, such as crying, being unable to concentrate, or the loss of situational control, are generally equated to being a form of weakness and subsequently portray police officers engaging in such acts as being inept or untrustworthy (Bell and Eski, 2016; Bikos, 2021; Edwards and Kotera, 2020; Karaffa and Koch, 2016; Soomro and Yanos, 2019). Police officers experiencing emotional distress may feel a sense of shame for being unable to align with the stoicism and toughness that is demanded by their organization (Bikos, 2021; Bullock and Garland, 2018; Edwards and Kotera, 2020).
Police officers known to be struggling with their mental health and wellness can experience stigmatization internally and/or structurally (Bikos, 2021; Bullock and Garland, 2018; Karaffa and Koch, 2016; Soomro and Yanos, 2019). Internal stigma pertains to how an individual perceives themselves through the lens of others around them; when these perceptions are aversive, the individual in question may devalue themselves and worry about exclusion, loss of image, and isolation from others (Bikos, 2021; Karaffa and Koch, 2016; Soomro and Yanos, 2019). Structural stigma consists of the ways institutional attitudes, policies, and procedures perpetuate negative stereotypes; when these typecasts are disparaging, individuals may be subject to discrimination and loss of status (Bikos, 2021; Karaffa and Koch, 2016; Soomro and Yanos, 2019). Through these processes of stigmatization, police officers experiencing poor mental health and wellness are likely to construe their identity as a police officer as being spoiled through internalizing perceptions of uselessness or lameness that run counterintuitive to professional expectations of utility and optimal performance (Bullock and Garland, 2018). To this end, there is a need to move beyond police culture literature alone and draw on elements of social identity theory to examine how police officers perceive themselves within this cultural environment to gain a more robust understanding of mental health and wellness within police organizations.
Social identity theory
Social identity theory (Tajfel, 1974, 1982; Tajfel and Turner, 1979) elucidates how intergroup relations across social structures, situations, and networks play an integral role in the formation and maintenance of an individual’s sense of identity (Davis et al., 2019; Hogg 2016; Hornsey, 2008; Sim et al., 2014). This shared identity can shape the way that individuals think, feel, and behave within the context of a distinctive social group; it provides directives and evaluations of who they are, sets forth beliefs that group members are expected to espouse, and draws attention to how their group differs from others (Davis et al., 2019; Hogg, 2016; Huddy, 2001; Stets and Burke, 2000). Social identity theory comprises three primary facets: self-categorization, identity salience, and self-enhancement (Hogg, 2016; Huddy, 2001; Stets and Burke, 2000; Terry et al., 1999; Welbourne et al., 2017).
Individuals are reflexive in that they can conceive of themselves as objects that can be classified or named in relation to specific features, known as prototypes, through a process called self-categorization (Hogg, 2016; Huddy, 2001; Stets and Burke, 2000; Welbourne et al., 2017). When an individual identifies with a particular group, they are likely to perceive themselves as similar to the prototypical group member (Davis et al., 2019; Hogg, 2016; Huddy, 2001; Welbourne et al., 2017). In addition, they quickly learn how to differentiate themselves from other social groups, forming ethnocentric categories of “us” (the in-group) and “them” (the out-group) (Hogg, 2016; Huddy, 2001; Stets and Burke, 2000; Tajfel, 1982).
As a social identity becomes more prominent, it begins to reshape how an individual views themselves (Hornsey, 2008; Sim et al., 2014; Stets and Burke, 2000; Terry et al., 1999). This notion of identity salience can explain how an individual becomes more prone to act in line with the behavioural norms of their social groups, even if these dispositions might be inconsistent with elements of their self-identity (Sim et al., 2014; Terry et al., 1999). When a social group identity is salient, the members within it will view themselves less as individuals and more as exemplars of the group prototype, moving away from identifying as an “I” or “me” and toward identifying as an “us” or ”we” (Davis et al., 2019; Haslam, 2013; Hornsey, 2008; Sim et al., 2014; Tajfel, 1974; Terry et al., 1999).
The social groups that an individual views themselves as a member of exist in contrast to other social groups, each having more or less power, relevance, and status (Hogg, 2016; Stets and Burke, 2000; Tajfel, 1982). Social identities, therefore, seek to build and preserve a positive association with the categories that one identifies with, configuring a basis for self-enhancement (Hogg et al., 1995; Stets and Burke, 2000; Tajfel, 1982). Group members learn to view their actions and behaviours as in-group stereotypical and normative, while viewing those of non-group members as out-group stereotypical and possibly competitive or discriminatory (Hogg et al., 1995; Stets and Burke, 2000).
Social identity theory is adept at illustrating how individuals develop a collective sense of self within the context of the profession they work within, given that organizations are made up of social actors that come together in pursuit of self-selected shared interests, motives, and goals (Arshad et al., 2022; Ashforth and Mael, 1989; Hogg and Terry, 2000; Welbourne et al., 2017). Social identities in organizations can become salient through symbolic and cultural properties, such as physical settings, rhetoric, stories, and traditions, which cultivate a claim to uniqueness relative to other professions (Ashforth and Mael, 1989). Organizations that have a strong social identity among their employees have been shown to elicit beneficial outcomes such as increased organizational commitment, low rates of turnover, augmented organizational citizenship behaviour (e.g., altruism, courtesy, virtuousness), as well as greater employee satisfaction and work performance (Ashforth and Mael, 1989; He and Brown, 2013; Hogg and Terry, 2000; Welbourne et al., 2017).
Possessing a strong sense of social identity maintains the possibility of invoking both positive and negative outcomes for police officers (Bullock and Garland, 2018). On the one hand, group membership may instill a feeling of community, effectuate a sense of identity validation, and facilitate social support (Bullock and Garland, 2020; Hogg and Terry, 2000; Welbourne et al., 2017). On the other hand, group membership can instill a fear of rejection and create prejudice that is directed toward individuals who do not exhibit group characteristics (Bullock and Garland, 2020; Haslam, 2013; Hogg and Terry, 2000).
Social identity theory has been found relevant to explaining several phenomena in policing. For instance, Murphy et al. (2018) utilized social identity theory to examine police bias and public cooperation, whereas Chan et al. (2025) examined procedural justice and legitimacy in policing. In addition, Stubbs and Tong (2025) applied social identity theory to whistleblowing in police organizations, while Charman and Tyson (2023) analyzed voluntary resignation among police officers. As we develop further in the next section, social identity theory can also be linked with police culture to develop a meso-level theoretical understanding of police officer mental health and wellness that moves beyond individual-level program responses (Ashforth and Mael, 1989; Welbourne et al., 2017).
Towards a meso-level theoretical framework
Police organizations continue to provide police officers with individual-level knowledge, tools, and resources for mental health and wellness management. Unfortunately, as discussed earlier in this paper, it is doubtful that police officers will engage with these measures if the cultural stigma surrounding mental health and wellness continues to prevail (Bikos, 2021; Bullock and Garland, 2018; Cohen et al., 2019; Jackson and Theroux, 2023). Although the decision to utilize mental health and wellness resources ultimately rests at the discretion of each police officer, the motivation to do so is likely to be influenced by how this matter is perceived within the police organization. In other words, because police officers are part of a collective culture, it is imperative to account for their social ecology in order to determine how to build a structural-level system where mental health and wellness concerns are accepted and normalized (Bikos, 2021; Stets and Burke, 2000; Suarez et al., 2023).
Drawing on police culture and social identity theory, the remainder of this section outlines a meso-level theoretical framework for creating an institutional atmosphere that supports police officers who might be struggling with their mental health and wellness. Insights from police culture and social identity theory render an understanding of how group membership can proactively shape police officers’ perceptions of mental health and wellness. This theorizing proposes that progress may be accomplished through three overarching techniques: (1) restructuring expectations surrounding mental health and wellness paradigms in policing; (2) redefining perceptions of police officers with mental health and wellness concerns; and (3) realigning leadership practices to prioritize organizational mental health and wellness. By highlighting these three potential areas of change, we hope to lay the groundwork for further empirical work in each of these areas.
Restructuring expectations surrounding mental health and wellness paradigms in policing
Around the world, police organizations consist of established prototypes that set forth an array of expectations for group membership, such as what group members ought to look like and how they are to conduct themselves and their business (Davis et al., 2019; Huddy, 2001; Sim et al., 2014; Tajfel, 1982). Police officers use these prototypes as markers to verify their identity; in essence, the more similar they are to the prototype, the better they perceive their ability to fit into the social world they inhabit (Bikos, 2021; Huddy, 2001). Put simply, when police officers are able to verify their identity, they are likely to feel positive about themselves and their role within the organization (Davis et al., 2019; Stets and Burke, 2000). Conversely, when police officers are unable to verify their identity or are in conflict with established identity expectations, they are likely to feel negative about themselves and their role within the organization (Davis et al., 2019; Stets and Burke, 2000).
Empirical research on mental health and wellness upholds that the existing prototype requires police officers to exhibit somewhat of a superhuman persona where they invariably stand tall, act courageously, and demonstrate resilience (Bullock and Garland, 2018; Deschênes et al., 2018; Velazquez and Hernandez, 2019; Waters and Ussery, 2007). Central to this prototype are characteristics entrenched in traditional connotations of masculinity, such as assertiveness, brazenness, emotional control, endurance, over-commitment to the organization, and self-reliance (Bell and Eski, 2016; Bikos, 2021; Papazoglou and McQuerrey-Tuttle, 2018; Velazquez and Hernandez, 2019). These features, in conjunction with police culture, have consequently generated the expectation that good or competent police officers are those who maintain a calm and composed demeanour and do not require assistance to contend or cope with the stressors that they encounter (Bell and Eski, 2016; Bikos, 2021; Tuckey et al., 2012; Velazquez and Hernandez, 2019). Although there is a certain degree of necessity and utility in the ability to distance oneself from their feelings in the line of duty, an over-emphasis on emotional suppression presents the potential to create an organizational setting where police officers become apprehensive to acknowledge symptoms of mental health and wellness concerns for fear of deviating from the status quo (Bullock and Garland, 2018; Soomro and Yanos, 2019; Tuckey et al., 2012; Velazquez and Hernandez, 2019). In turn, police officers may feel as though their only option is to suffer in silence as they worry that confiding in colleagues runs the risk of diminishing their social identity by appearing to be incompetent (Edwards and Kotera, 2020; Ricciardelli et al., 2021; Soomro and Yanos, 2019; Velazquez and Hernandez, 2019).
This research indicates that the mental health and wellness of police officers could be improved if the prototype that surrounds this issue could be restructured. It has been theorized that there may be important gains made in police officer mental health and wellness by embedding these mental health and wellness principles directly into the ethos of policing, intrinsically constructing a work environment where police officers feel empowered, protected, and respected to take care of themselves and each other (Cohen et al., 2019; Jackson and Theroux, 2023). As Gavin and Porter (2025b) found, police officers in Ireland were reluctant to engage in mental health and wellness initiatives for reasons such as concerns about career implications and the perceived stigma around seeking help. Thus, the cultural undertones of a police organization play a pivotal role in pushing police officers either toward or away from accessing mental health and wellness resources, hereby illustrating the need to drive home the idea that these problems are to be expected and that asking for help is a sign of strength and not weakness (Cohen et al., 2019; Edwards and Kotera, 2020; Jackson and Theroux, 2023).
Reconceptualizing the mental health and wellness prototype using police culture.
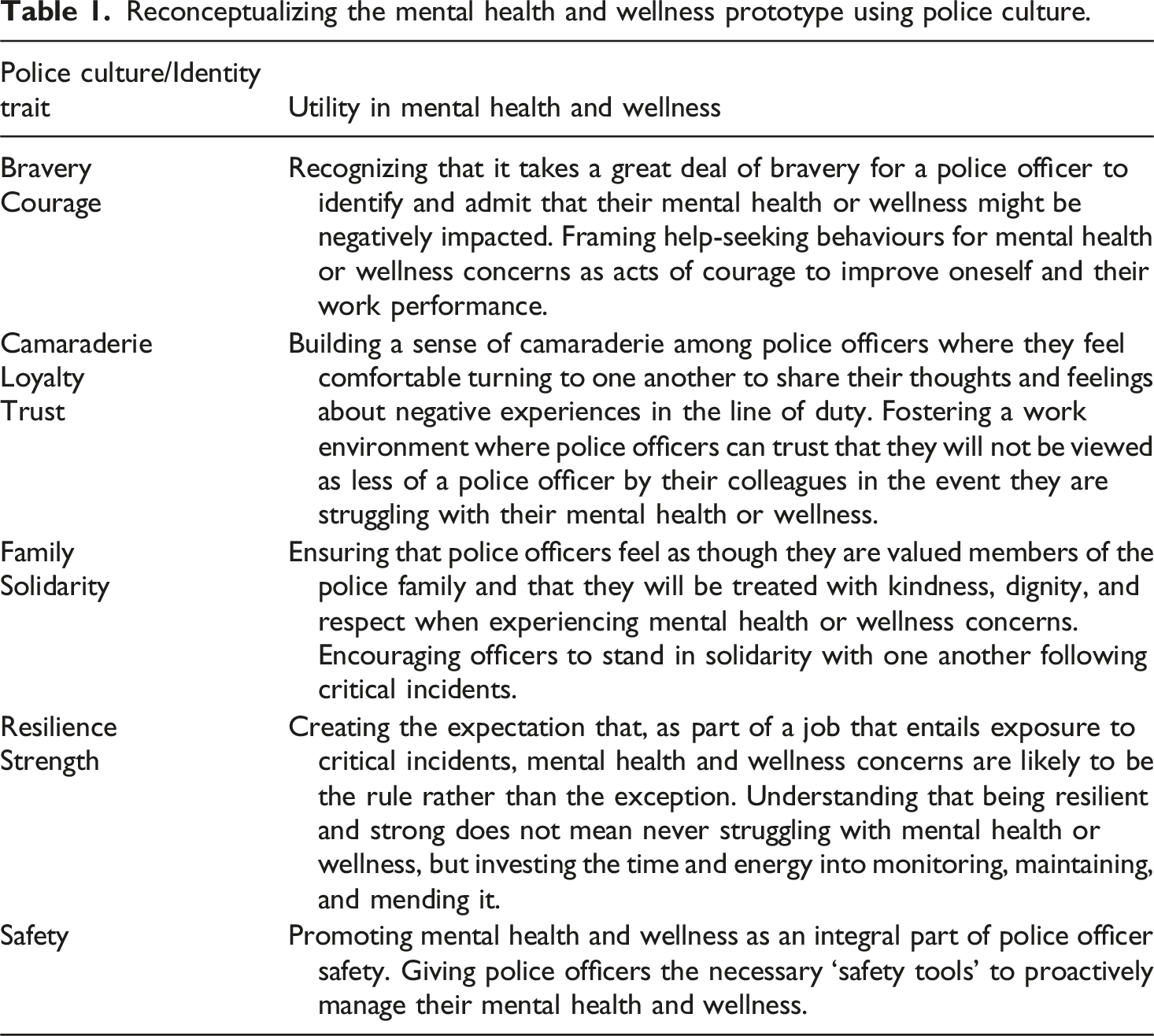
Police culture has also been recognized as being a coping resource in and of itself that assists officers in dealing with the adversities, hazards, and strains of the policing profession (Chan, 1996; Paoline, 2003; Terpstra and Schaap, 2013). To this end, police culture may be able to act as “a stage for tolerance towards mental health [and wellness concerns], instead of being a domain of stigmatization” (Bell and Eski, 2016: 98; Loftus, 2010). There is also a burgeoning body of evidence which suggests that cultural attitudes toward mental health and wellness could be in the initial phases of changing for the better in policing (Bell and Eski, 2016; Bikos, 2021; Edwards and Kotera, 2020).
Redefining perceptions of police officers with mental health and wellness concerns
Police organizations are made up of an assemblage of social groups (e.g., civilians, sworn members, specialized units, leadership) that intersect and impinge upon one another; each of which contains a different level of inclusiveness based on the extent to which they resemble group prototypes (Ashforth and Mael, 1989; Charman, 2017; Haslam, 2013; Hogg and Terry, 2000; Hornsey, 2008; Tajfel, 1982).). Police officers use their group membership(s) as a method of social comparison that concurrently seeks to protect and bolster the influence of their group as well as enhance self-esteem (Hogg, 2016; Huddy, 2001; Martiny and Rubin, 2013). As such, police officers who belong to groups that emulate prototypical norms tend to be viewed favourably and possess a higher social standing (the in-group), whereas those in groups that do not endorse prototypical norms may be regarded critically and occupy a lower social standing (the out-group) (Charman, 2017; Hogg, 2016; Hogg and Terry, 2000; Huddy, 2001; Martiny and Rubin, 2013).
Turning the focal point to mental health and wellness, empirical research proposes that there are two conventional social groups in police organizations: police officers with and without mental health and wellness concerns (Bell and Eski, 2016; Bullock and Garland, 2018; Edwards and Kotera, 2020). These categorizations have come to exist as a by-product of the perception that police officers who are struggling with their mental health and wellness are failing to meet prototypical ideals, effectively becoming a marginalized community within the police organization (Bell and Eski, 2016; Bullock and Garland, 2018; Edwards and Kotera, 2020; Ricciardelli et al., 2021). In this respect, mental health and wellness concerns act as a marker of separation that differentiates police officers who are viewed as being impervious to the pressures of police work (thereby representing the in-group) from police officers who are unable to cope with the pressures of police work (henceforth becoming the out-group) (Bell and Eski, 2016; Bullock and Garland, 2018; Edwards and Kotera, 2020; Karaffa and Koch, 2016).
Ironically, it has been noted that, for the most part, police officers begin their careers in a relatively good state of well-being and develop a host of mental health and wellness concerns due to their occupational experiences (Gavin and Porter, 2025a; Porter and Gavin, 2025; Rose and Unnithan, 2015; Waters and Ussery, 2007). Yet, in a concerted effort to retain their place in the in-group, police officers may inadvertently engage in behaviours that are consistent with pluralistic ignorance, which is known to occur when individuals in a group internally reject a belief or feeling while believing that other group members internally accept it (Grupe, 2023; Karaffa and Koch, 2016). Police officers may, therefore, underestimate the prevalence and normalcy of mental health and wellness concerns and feel as though it is a personal shortcoming to struggle with processing traumatic or stressful calls for service (Bell and Eski, 2016; Grupe, 2023; Karaffa and Koch, 2016). Moreover, police officers might falsely perceive themselves as being an anomaly from their colleagues if they wish to seek out or utilize available mental health and wellness resources (Bell and Eski, 2016; Grupe, 2023; Karaffa and Koch, 2016).
It is widely documented that one of the most instrumental assets for police officers in managing their mental health and wellness is the opportunity to rely on their colleagues for assistance, compassion, and guidance (Deschênes et al., 2018; Duran et al., 2019; Ricciardelli et al., 2021; Schuster and Ross, 2019). Peer support is especially invaluable considering that police officers are often reluctant to discuss their mental health and wellness concerns with individuals external to the police organization either because they do not want to worry their family and friends or due to the inability of outsiders such as general practitioners, psychotherapists, or psychiatrists to comprehend or relate to policing (Bell and Eski, 2016; Duran et al., 2019; Papazoglou and McQuerrey Tuttle, 2018; Waters and Ussery, 2007).
This research suggests that improving the mental health and wellness of police officers might require a redefinition of the in- and out-groups that revolve around this phenomenon. To impart this change and alter in- and out-groups, it would be beneficial to rely upon the doctrine of police storytelling (Cockcroft, 2007; Van Hulst, 2013). Stories are a key component of identity formation in policing as they not only retell past events but also provide direction on future scenarios for police officers (Van Hulst, 2013; Waddington, 1999). Thus, stories can serve as a metaphorical “repair shop” in policing that is filled with anecdotes, fellowship, and tools that are shared amongst police officers (Van Hulst, 2013; Waddington, 1999).
Police officers can use storytelling as a platform to normalize mental health and wellness concerns by sharing their personal experiences with their peers, beginning with the event(s) that they believe contributed to the development of stress, the signs and symptoms that indicated they needed to seek help, the recovery process, and how they navigated their return back to work (Cohen et al., 2019). This presents an opportunity to change the narrative surrounding mental health and wellness from one that instructs police officers to grit their teeth and endure it to one that coaches them to take the necessary time to access the appropriate measures and work through it. In doing so, police organizations can help generate a close bond between colleagues who understand and empathize with one another over mental health and wellness concerns, constructively building a more accessible space for police officers to lean into support from their peers (Ricciardelli et al., 2021). This change could help shift the in-group away from being viewed as police officers who are impervious to the pressures of police work to one that acknowledges that all police officers at one time or another will likely struggle with their mental health and wellness and subsequently require some form of assistance or support.
Realigning leadership practices to prioritize organizational mental health and wellness
Police organizations are structured in compliance with a chain of command system where those at the top are tasked with setting the agenda, beliefs, goals, and values of the institution (Arshad et al., 2022; Hogg et al., 2005, 2012). Police officers subsequently look to individuals in leadership positions for cues on how to form and understand their identity (Arshad et al., 2022; Hogg et al., 2005, 2012). Police leaders occupy a quintessential role as “identity entrepreneurs” who maintain the authority to construct and reconstruct perceptions of group prototypes as well as delineate, consolidate, and modify what constitutes the in- and out-groups (Arshad et al., 2022; Hogg et al., 2012). In this regard, police leaders act as a prototypical model of what it means to be a member of the organization, either as it currently stands or as a representation of what they aspire for it to be (Hogg et al., 2012; Steffens et al., 2021).
Empirical research asserts that individuals in leadership positions are largely responsible for determining how mental health and wellness is interpreted by the members of their organization based on the viewpoints that they exemplify (Bullock and Garland, 2020; Cohen et al., 2019; Edwards, 2023; Violanti, 2021). Police leaders who exhibit a supportive demeanour toward self-care maintain the potential to create a work environment where police officers feel supported in seeking help for mental health and wellness concerns, which can increase organizational commitment and morale, elevate work performance, and improve quality of life (Arshad et al., 2022; Bullock and Garland, 2020; Edwards, 2023; Shim et al., 2015; Violanti, 2021). Alternatively, police leaders who approach self-care with a negative outlook run the risk of creating a work environment that stigmatizes police officers for seeking help for mental health and wellness concerns, which can lead to absenteeism and turnover within the organization (Bikos, 2021; Edwards, 2023; Violanti, 2021).
This research conveys that the mental health and wellness of police officers could be improved if police leaders emphasized the importance of this matter by making it a salient feature of police organizations. It has been argued that support from individuals in leadership positions is perhaps one of the most influential building blocks in challenging the existing norms, perceptions, and structures that surround police officer mental health and wellness (Cohen et al., 2019; Tam-Seto and Thompson, 2023; Violanti, 2021). When police leaders demonstrate buy-in for the mental health and wellness education curricula, training programs, and resources that are offered through their organization, they send a progressive message about this issue that trickles down throughout the ranks, setting the precedent for how these concerns are to be understood and responded to (Bikos, 2021; Bullock and Garland, 2020; Edwards, 2023).
To empower police leaders to prioritize the mental health and wellness of the individuals within their organization, it would be beneficial to look toward the canons of transformational leadership, which is centred upon the notion that leaders ought to focus on priorities such as developing and selling a vision, inspiring and motivating employees, acknowledging and valuing the members within their organization, as well as facilitating open and participatory communication across personnel and ranks (Cohen et al., 2019; Shim et al., 2015; Silvestri, 2007). Police leaders operating under a transformational approach to leadership are invested not only in the success of the organization itself but also in the well-being of their employees, creating a climate of care and trust as well as generating a sense of belonging and oneness within the institution (Arshad et al., 2022; Cohen et al., 2019; Shim et al., 2015; Silvestri, 2007). Accordingly, transformational leadership has been cited as a key tactic in altering the trajectory of police culture and practice due to the social dynamics that exist between leaders and employees in unison with the contextual factors that characterize the profession (Cohen et al., 2019; Shim et al., 2015; Silvestri, 2007).
Police leaders can set an example by guiding with courage and compassion when it comes to helping police officers plan for and respond to mental health and wellness concerns, moving beyond organizational branding that often results in the implementation of education curriculums, training programs, and resources for the purpose of implementing a “quick fix” (Bikos, 2021; Edwards, 2023; Tam-Seto and Thompson, 2023; Violanti, 2021). Although police leaders cannot circumvent the sources of stress and trauma that police officers face in the line of duty, they do possess the ability to formulate a work environment that acts as a buffer against these circumstances (Randall and Buys, 2013).
Given this, to effect positive change, police leaders must be willing to learn about what the members of their organization identify as being detrimental to their mental health and wellness, be receptive to findings from empirical research, conduct consultations with experts inside and outside of the organization, invite employees to participate in the development of preventative or rehabilitative measures, offer nonjudgmental support and information about resources that have been put in place, and encourage individuals to come forward and seek help early on (Cohen et al., 2019; Randall and Buys, 2013; Violanti, 2021). Together, these strategies may enable police leaders to make it clear that the mental health and wellness of police officers is of paramount importance, as well as demonstrate that they endorse the initiatives they introduce.
Conclusion and future research directions
Throughout this paper, we have argued that fusing police culture and social identity theory can offer a meso-level theoretical framework to reconceptualize how the mental health and wellness of police officers is understood and perceived. This approach is predicated upon three interrelated strategies: (1) restructuring expectations surrounding mental health and wellness paradigms in policing, (2) redefining perceptions of police officers with mental health and wellness concerns, and (3) realigning leadership practices to prioritize organizational mental health and wellness. These techniques are indeed only a starting point in attempting to highlight some areas in need of attention in what is inherently a complex and longstanding issue. While more research is needed to test the validity of our proposed theoretical framework, it could be implemented in tandem with the variety of mental health and wellness efforts and programs noted above. This theoretical framework provides police organizations with an apparatus to work toward crafting an identity as an institution that prioritizes mental health and wellness and that stands in solidarity with their police officers.
Forthcoming studies should continue to uncover police officers’ perceptions of the culture that underpins their respective organizations and how it shapes attitudes and beliefs surrounding mental health and wellness, the utility of social support among police officers experiencing mental health and wellness concerns, and the impact of organizational leadership on attitudes toward mental health and wellness. These findings can shed light on important considerations, such as whether the core ideologies of police culture have changed in relation to the contemporary state of policing, and help to determine if police organizations and/or police officers are becoming more tolerant of mental health and wellness. Additional research is needed to explore police officers’ perspectives on the mental health and wellness education, training, and resources that they receive during their careers. This data can help police organizations understand what police officers find helpful and unhelpful, as well as identify what could be improved or what is missing altogether. In order to paint the most comprehensive picture of the mental health and wellness of police officers, research ought to be conducted that considers the nexus between police culture, identity, and the education, training, and resources that are available.
Footnotes
Acknowledgements
Special thanks to Dr Tyler Frederick and Dr Jennifer Lavoie for providing thoughtful commentary on previous versions of this publication.
Ethical considerations
Ethical approval was not required for the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work of the first author was funded in part by the Ontario Graduate Scholarship (OGS) Program.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.