
Abstract
Police officers are routinely exposed to stressors which can negatively impact their mental health. This paper presents findings from an anonymous online survey undertaken by 98 members of An Garda Siochána (the Irish police force). It considers Irish police officer perceptions of mental health support and the barriers they face to accessing and engaging with mental health support. Barriers to engaging with support included the impact of stigma, the potential negative impact on career progression, a lack of trust in the support services and a general lack of resources.
Introduction
The Irish police force, or An Garda Siochána (‘Guardians of the peace’), was established in 1922. It is made up of approximately 14,000 officers, approximately 12,000 of which are rank-and-file. Unlike many other police forces, An Garda Siochána are committed to a uniform national community policing style which manifests itself in a predominantly unarmed and less aggressive approach to policing (Marsh, 2022). An Garda Siochána shares key similarities with other Anglo-American policing models. It has a bottom-heavy structure, with most officers at the entry level engaged in random patrols, crime investigation, and responding to public requests. Officers receive brief, batch-based training in formal school and field settings and are widely dispersed, often operating with minimal supervision. Their decision-making, sometimes referred to as ‘discretion’, only comes into play after an incident has been legally defined. The authority of police officers remains rooted in common law (Manning, 2012), as well as in the unarmed nature of the force. In 1922, the first Commissioner of An Garda Síochána, Michael Staines, stated, “The Garda Síochána will succeed not by force of arms or numbers, but on their moral authority as servants of the people”, and this holds true to the present day.
Research into the operation of An Garda Siochána has generally been focussed on the organisations history, and Manning (2012) has noted that primary sources on the Garda are historical and descriptive (Allen, 1999; Brady, 1974; Breathnach, 1974; McNiffe, 1997), socio-legal and analytic (Mulqueen, 2010; Walsh, 1998) or based on interviews with retired officers (Conway, 2010) (see Manning 2012, 355). Historically there has been a lack of research into the mental health of police officers in Ireland (when compared with other jurisdictions), but research undertaken in recent years has found there to be widespread frustration among frontline officers, a supervision vacuum, a growing feeling disillusionment, burnout and poor levels of mental health (Fallon, 2018; Garda Representative Association, 2023; Gavin and Porter, 2024; Gibbons, 2024; PwC, 2018).
The unique nature of police work sees police officers exposed to a wide range of occupational stressors which are often categorised as operational and organisational stressors (Gavin and Porter, 2024; Gibbons, 2024; Porter and Gavin, 2024). Operational stressors are usually associated with police exposure to social traumas such as poverty, violence, and addiction, as well as being forced to deal with potentially life-threatening situations on a near-daily basis (Rooney and McNicholas, 2020). These situations can include witnessing, or being subjected to traumatic events, witnessing, or experiencing acts of violence, crime involving children, responding to events with mass casualties, and dealing with sexual offences (Brewin et al., 2020; Gavin and Porter, 2024; Miller et al., 2022). Police officers can also be exposed to vicarious trauma, for instance, in cases where they are notifying families of a death, witnessing graphic images, or dealing with distressing emergency calls (Kirschman et al., 2014). Organisational stressors are more commonly associated with the administrative side of police work. Police officers face stress due to the nature of shift work, long hours, poor pay, a lack of support from senior managers, excessive and unfair workloads, increased amounts of administration, and the impact of austerity on police numbers (Gavin and Porter, 2024; Porter and Gavin, 2024). This all amounts to a police service being asked to do more with less (Solar and Smith, 2022).
Exposure to the above stressors can negatively impact on the mental health of police officers and can lead to the development of a range of mental health problems including Post-Traumatic Stress Disorder (PTSD) and Complex-PTSD (CPTSD) (Brewin et al., 2020; Gavin and Porter, 2024; Porter and Gavin, 2024; Stevelink et al., 2020), depression, anxiety (Jetelina et al., 2020; Stevelink et al., 2020), burnout, drug and alcohol addiction (Irizar et al., 2021), self-harming, and even suicide (Hem et al., 2001; McCafferty et al., 1992). The prevalence of PTSD and depression amongst police officers is over twice that of the general population (Kessler et al., 2005; Syed et al., 2020) and this is linked with absenteeism (Cartwright and Roach, 2020), aggression (Rajaratnam et al., 2011), and suicide (Hem et al., 2001). To help cope with such stressors some police officers have been found to engage in hazardous or harmful drinking or drug taking, and when compared to those without a mental health problem, police employees with depression, anxiety, or PTSD, were twice as likely to be harmful drinkers (Ballenger et al., 2011; Brough et al., 2016; Davey et al., 2000, 2001; Irizar et al., 2021; Lindsay and Shelley, 2009; Syed et al., 2020). Consequently, support for the mental health of police officers is of vital importance. This help can come in various forms.
Critical Incident Stress Management (CISM) has been increasingly adopted by police forces worldwide as a comprehensive crisis intervention program (Everly and Mitchell, 1997). It aims to reduce acute psychological distress from violent incidents and prevent long-term posttraumatic effects. Research has shown that those who engage with CISM can develop a range of strategies that work to mitigate psychological distress and promote mental wellbeing (Everly et al., 2002). Employee Assistance Programmes (EAPS) are a crucial resource for police departments to support their officers and address mental health. They are programs which are funded by the employer in question and operate in both the public and private sector. Police EAPs are often under-utilised by police officers (Asen and Colon, 1995; Donnelly et al., 2015; Newell et al., 2022) and this is often due to officer mistrust of either the institution, the programme or both (Quick, 2023). Many police officers see EAP’s as organisational lip service or box ticking which are designed to serve the organisational interest rather than interests of individual police officers (Goldstein, 2006).
Peer-support programs offer police officers a confidential space to share experiences with colleagues who best understand their challenges. These programs foster a culture where seeking help is encouraged and reduce the stigma around mental health, promoting a sense of community and support within the force (Milliard, 2020). Research demonstrates that some police officers feel that such programmes are ill-equipped to meet their support needs and can be both inconsistent and unreliable (Fallon, 2018). As with EAP’s, many police officers view peer-support programmes as tokenistic, and this must call their value into question (Rooney and McNicholas, 2020). TRiM (Trauma Risk Management) is a peer-group-based system that was first developed in the Royal Marines (Frappell-Cooke et al., 2010). It has been adopted by several UK-based police forces to provide “a structured process for assessing personnel’s risk of developing psychological distress following exposure to potentially traumatic events” (Watson and Andrews, 2018, 350). By utilising a peer-led approach, TRiM aims to encourage a more open recognition of trauma-related distress within the police. As it is peer-led the process can develop camaraderie as fellow police officers may have shared similar experiences relating to traumatic exposure. TRiM may help to ameliorate some of the negative effects of traumatic exposure (Hunt et al., 2013) and police officers who used TRiM reported less stigma, less PTSD symptoms and fewer barriers to help seeking than those who did not use it (Watson and Andrews, 2018).
Police officers are often reluctant to seek help for their mental health. Police culture, and the stigma associated with mental health, plays a significant role in this failure to seek help (Newell et al. (2022); Watson and Andrews (2018)). Stigma involves reducing someone in our minds, “from a whole and usual person to a tainted, discounted one”, whereby we view the person has having a failing, shortcoming or handicap (Goffman, 1963, 12). It is an attribute that is deeply discrediting. This can also be internalised, and internal stigma plays a role in influencing individual reactions to stress. Thus, it has a significant role in the way a person responds to psychological distress (Stuart, 2017). The stigma associated with mental health results in police officers being fearful that seeking help for their mental health may be perceived as a sign of cowardice or weakness (Edwards and Kotera, 2021; Miller, 1995; Newell et al., 2022; Watson and Andrews, 2018). This conflicts with a police culture focussed on machismo and masculinity, resilience, hardiness and psychological capital, all of which demands police officers are tough and brave and in control of their emotions (Bell and Eski, 2016; Crowe et al., 2022; Edwards and Kotera, 2021; Janssens et al., 2021; Papazoglou, 2013; Reiner, 2010).
Concerns over confidentiality have also been highlighted as a barrier to police officers seeking mental health support (Fallon, 2018; Kerrisk et al., 2021; Newell et al., 2022). Officers may also resist disclosing their mental ill health for fear of negative reactions from colleagues (Bullock and Garland 2018; Karaffa and Koch, 2016; Kerrisk et al., 2021). Police officers are likely to view accessing mental health services in a negative light, whereby they are more concerned with the potential damage that it may do to their career as opposed to the potential positive change in their mental health (Porter and Lee, 2023). Such a culture may thus encourage a ‘tough it out’ mentality, making it challenging for officers to cope with these experiences (Porter and Lee, 2023). Not seeking help may exacerbate an existing condition and research has shown that police officers who actively avoided seeking help for their mental health, later reported higher levels of declining mental health (Soomro and Yanos, 2018).
Method
Ethical approval was obtained from the ethics committee at the Univeristy of the West of England (UWE) Bristol. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all participants who were included in the study.
This research involved a series of qualitative and quantitative questions examining the mental health of police officers throughout the Republic of Ireland. The study was based on the premise that the mental health police officers was a problematic issue, and that serving members would welcome to opportunity to discuss this.
On 12 September 2023, a call for participants was placed on the social media accounts (i.e. Twitter /X and LinkedIn) of both authors. The survey remained open until 12 December 2023. Those who were interested in learning more about the research were invited to click on the survey link taking them to an online information sheet which outlined the core objectives of the study. Those who wished to participate provided fully informed consent and were invited to answer a series of questions relating to mental health and policing.
Participants were asked several demographic questions regarding age, gender, and length of service in the police. The questions used to inform this qualitative analysis were “How does your organisation support mental health?” and “What do you feel are the main barriers to accessing mental health support in your organisation?” Open-ended questions are widely used in qualitative research and exploratory studies, allowing respondents to freely express their thoughts. They provide researchers with deeper insights, capturing diverse perspectives that may be personal, unexpected, or overlooked in survey design, ultimately enriching the data collected (Albudaiwi, 2017).
The authors adopted an inductive approach to this research. This allowed them to identify pertinent issues related to mental health and policing at the outset. Inductive reasoning is open-ended and exploratory, especially at the beginning of the research process, and its use involves the researcher inferring the implication of their findings for the theory that prompted its use (Bryman, 2016; Given, 2008).
Qualitative data were analysed through thematic analysis (Braun and Clarke, 2006). Thematic analysis was used as it is both flexible and accessible and generally suitable for analysing nearly all types of qualitative data (Finch and Fafinski, 2012). This was carried out by both researchers, as coding with another researcher and comparing analytic observations can lead to enriched coding (Braun and Clarke, 2021). The process involved a superficial reading of the data for familiarisation. During this phase, we independently recorded our reflections, acknowledging that each rereading could yield new interpretative insights. Emerging themes were identified based on the initial notes and were preliminarily discussed. Subsequently, we collaboratively developed subthemes, refining terminology and establishing shared meanings.
Comparison between demographics (gender & age) of our sample (n = 98) and those of An Garda Siochána.
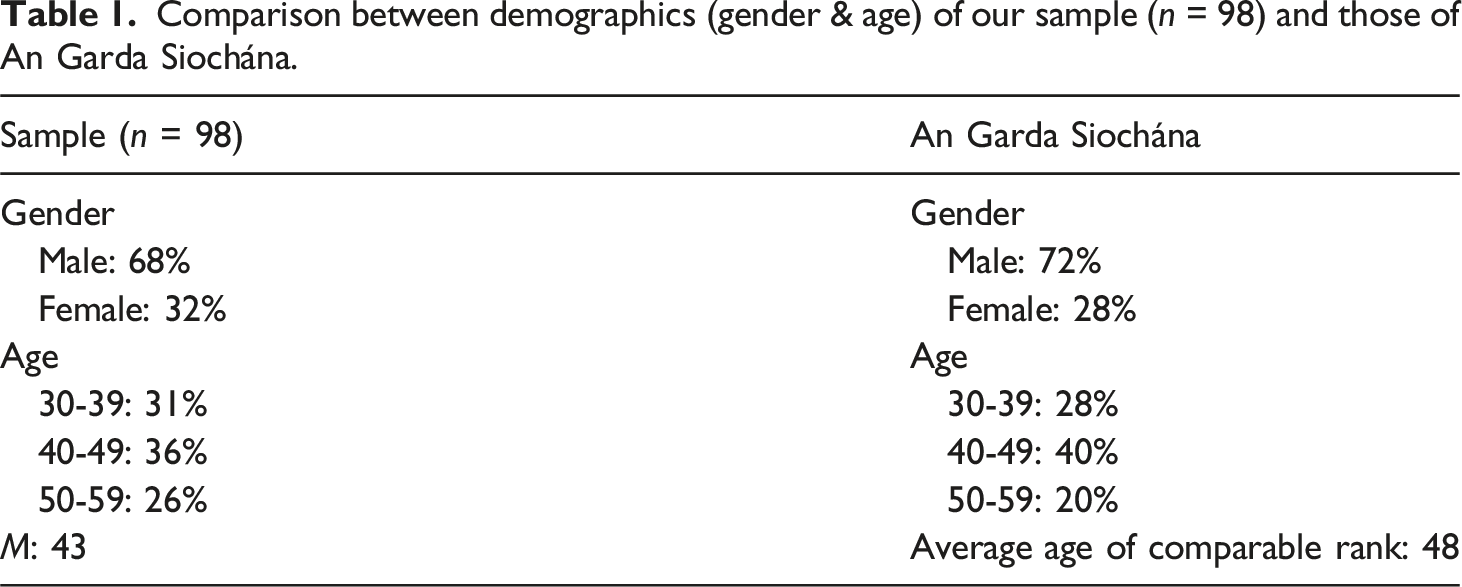
While the sample size is representative of the demographics of An Garda Siochana, the authors are aware that the sample size represents less than 1% of the overall organisation. We also aware that this study does not capture the full picture relating to mental health in Irish policing. However, the rich narratives that were obtained from participants are reflective of other studies which have been undertaken into An Garda Siochána with much larger sample sizes which considered cultural issues within the organisation and how police culture has impacted on the mental health of members of An Garda Siochána (Fallon, 2018; PwC, 2018) and, therefore, this study does go some way to helping understand some of the main issues relating to mental health and policing in Ireland. In order to fully capture the multi-faceted and nuanced issues related to this topic, wider and more in-depth studies are needed.
Support for mental health
In response to the question How does your organisation support mental health?” a significant number of participants referred to support being available through a mobile phone app, as well as counselling and welfare services which are made available through an Employee Assistance Programme. This suggests that at the very least, there is an awareness of the support options available. Regarding the availability of counselling, participants were very aware of how many sessions could be availed of, with several noting that up to six counselling sessions could be undertaken, and that this can be extended to 12 on request. One participant noted that ‘mental health support is readily available through the Employee Assistance Service’ (Detective Inspector, Male, 25 years of service), while another wrote that ‘If someone needs help there are welfare officers and there are well-advertised counselling services available to any member’ (Detective Sergeant, Male, 32 years of service). Some participants felt confident of being able to access services if required, and while they felt that there were no real barriers to accessing services, a greater culture of openness was needed when discussing mental health within the organisation: No real barriers but it is not something that is openly talked about enough (Garda, Male, 4 years of service).
No barriers. Should be encouraged more by management (Garda, Male, 17
years of service).
Several participants were positive about the development of mental health services and the supports that were available. Several stated that mental health support within An Garda Síochána was now better than it has been for over 30 years and that senior leadership within the organisation was responsible for this. One wrote that ‘Our current Commissioner has placed mental health and wellbeing in his top priorities for the entire police force and he has delivered on that with a Wellness Policy, wellness days and support services, an APP and many more initiatives. It is now at the best I have seen it in 31 years’ (Chief Superintendent, Male, 31 years of service), while another felt that the provision of mental health services ‘has improved a lot since I joined the job 34 years ago when this topic would have been frowned upon’ (Detective Sergeant, Female, 34 years of service).
Another participant wrote ‘It is improving as the concept is being addressed and embraced at last. Wellness programmes, the KOPS (Keeping Our People Safe) app, the ASSIST suicide prevention programme and now the expansion of the professional supervision programme is benefiting’ (Detective Superintendent, Male, 39 years of service).
Barriers to seeking mental health support
Thematic analysis of responses to the question “What do you feel are the main barriers to accessing mental health support in your organisation?” found there to be several barriers to accessing mental health support. These were: the stigma associated with seeking mental health support, the potential negative impact on career progression, a lack of trust in the services offered, a lack of trust in management, a lack of time to engage with mental health support services and a lack of resources devoted to such services.
Participants highlighted the impact that stigma can have when it comes to seeking help for one’s mental health. One noted that ‘there is a stigma around mental health issues and as a consequence members bottle up what is causing their stress’ (Garda, Male, 40 years of service) while another felt that ‘there is a stigma if member goes sick with stress or mental health issues’ (Garda, Male, 7 years of service). One participant claimed that there was an ‘expectation to be available all the time’ (Female, Superintendent, 30 years of service). This comment reinforces research which contends that police culture presents with a 'tough it out' mentality when it comes to mental health. This mentality was highlighted by another participant who felt that mental health was ‘a taboo subject due to the nature of the job, a sense of ‘that’s what you signed up for so get on with it’ due to years of this being the norm’ (Garda, Female, 16 years of service). This attitude was reiterated by other participants. One wrote that ‘Welfare is brushed under the carpet. A ‘get up and get on with it’ mentality is very much voiced’ (Garda, Male, 6 years of service) while another claimed that ‘we are expected to suck it up (or worse, bottle it up) and get on with things’ (Detective Garda, Male, 17 years of service).
It appears that those who cannot 'tough it out' end up being stigmatised within the organisation. One participant felt that main problem with stigma, and with the 'tough it out' mentality in policing, was that both came from their colleagues. They wrote ‘Admitting an issue to my peers would arise suspicions that I would be windy and flaky in an incident. Have to show strength and courage in front of them’ (Garda, Male, 22 years of service). Another participant felt that ‘It has always been seen as a weakness for members to be seen to struggle with their mental health, so there is a stigma still if someone is needing to use services’ (Garda, Female, 14 years of service). One participant noted that ‘If you access it (mental health support) you have a mark on you’ (Garda. Male, 27 years of service). Others were conscious that this ‘mark’ or ‘spoiled identity’ (Bullock and Garland 2018; Goffman, 1963) may have a detrimental impact on the career of a police officer, and many participants cited fears over career progression as a barrier to seeking mental health support. This was especially true for those who worked in specialist units, for examaple where firearms are required, with one participant writing that, ‘it would hold you back in your career and would call into question your ability to operate in a firearms unit’ (Garda, Male, 15 years of service). Participants claimed that if a person sought help for their mental health, this would stay on their record. It would be seen as a weakness and would negatively impact on their career progression. One participant noted that ‘One’s career would come to a dead end if one was being treated for a mental health issue’ (Garda, Female, 13 years of service) while another commented that ‘Nobody wants to be the person that asked for help for fear of it affecting their career negatively’ (Sergeant, Male, 18 years of service).
Participants also expressed a lack of trust in the services that were available. While peer support schemes were highlighted by several participants, some felt that peer schemes were untrustworthy due to a lack of training and confidentiality. The peer support scheme was described as not being fit for purpose as there was a lack of trained professionals to help those who were struggling. One felt that those providing counselling ‘had no experience of working related trauma’ (Garda, Male, 23 years of service) while others criticised the lack of options available, the lack of access to ongoing support and the availability and quality of the services. Confidentiality was cited as a concern by several participants who felt that ‘your struggles are fodder for workplace gossip’ (Garda, Female, 16 years of service). Trust was found to be lacking in the ability of senior management to deal with mental health concerns. One participant claimed that ‘some managers are nervous about the subject of mental health’ (Garda, Male, 18 years of service) while another stated that ‘Management aren’t qualified in how to deal with mental health issues’ (Detective Garda, Male, 17 years of service). Participants also claimed that senior management were not interested in dealing with the mental health concerns of rank-and-file officers, and that they ‘care more about their end of the month reports and key performance indicators than the welfare of the members on the frontline every day and night’ (Garda, Male, 5 years of service). This was reinforced by another participant who claimed that management ‘have no interest in anyone being unavailable due to stress or mental health issues’ (Detective Garda, Male, 17 years of service).
Practical barriers to accessing services were also highlighted, especially the lack of time available and the lack of resources dedicated to mental health support. Participants believed support should be made available during the working day and that it should not take up time outside of work. One participant wrote that it ‘all has to be done on your own time and you will have to travel at least an hour to obtain same. Getting an appointment can take some time’ (Garda, Female, 33 years of service) while another cited ‘Getting time off or having to go to mental health support on days off’ (Garda, Male, 4 years of service) as a barrier to accessing support. Participants were also of the view that mental health support is under-resourced. One felt that An Garda Síochána ‘always go for the broken and cheaper option’ (Detective Garda, Male, 15 years of service) while several wrote that the organisation simply does not want to invest the money into dealing with mental health concerns. Participants felt that An Garda Síochána should look to emulate other police forces ‘with good working strategies…we seem to never follow a model that works’ (Detective Garda, Male, 15 years of service).
Many felt that the organisation is paying lip-service to mental health issues and that the support available is merely a tokenistic, box-ticking exercise. Some of the comments which reflected this include the following: It pays lip-service to welfare issues, but its approach is a box-ticking exercise (Garda, Female, 16 years of service).
It has a token counselling service in place for anyone looking for it, but our own management have little to no regard for the mental health of their staff (Detective Garda, Male, 17
years of service).
One participant described the welfare officer system as ‘terrible and very dependent on the individual officer…When I reference people to her it is with the caveat that she will probably not call back’ (Garda, Male, 26 years of service).
Discussion
The findings in this paper demonstrate that members of An Garda Síochána are at the very least aware of the ways in which An Garda Síochána supports the mental health of its members and several participants referred to ways in which mental health support is accessible. These findings are positive, and given that many initiatives to support mental health only came on stream in the third and fourth quarters of 2021 as part of the An Garda Síochána Health and Wellbeing Strategy 2021-2023 (An Garda Siochana, 2021), it is encouraging to see that so many are already aware of their existence. Several long serving members felt that mental health support was stronger now than ever before in An Garda Síochána. Again, this is a positive finding, but it must be tempered by noting that until quite recently there was very little in the way of mental health support provided, so there was, as one participant noted ‘a low starting base level’ (Garda, Male, 27 years of service).
Police culture needs to be considered as a significant barrier to help seeking, as well as means by which poor mental health in reinforced within the police force. The general tenets of police culture are a sense of mission (action/cynicism/pessimism), suspicion of the public, isolation from the public /solidarity with colleagues, a conservative outlook, machismo or bravado, institutional racism and pragmatism (Reiner, 2010). While many of these facets of police culture are focussed on how the police engage with the public, many can be understood in the context of barriers to help seeking. For example, if a police officer is unable to demonstrate a degree of machismo and bravado and feels as though they must open up to colleagues about their mental health, this may see them being labelled as weak which may raise issues related to pessimism and suspicion. While police officers are generally considered to be cynical and suspicious of the public, this cynicism and suspicion could be redirected towards a colleague who speaks openly about their mental health. It may also result in other officers becoming cynical or pessimistic about working with someone who is open about their mental health. It might also result in breaking bonds of solidarity which may have been forged with colleagues, and consequently the individual in question may become isolated from their colleagues though stigmatization.
Participants were also critical of the mental health support services offered, with many claiming that it was more of an optical exercise so An Garda Síochána can demonstrate that they are supporting the mental health of its members. This is reflective of research which has found there to be a culture of box-ticking and lip-service when it comes to dealing with mental health concerns in An Garda Síochána (Kerrisk et al., 2021). Many felt that management within An Garda Síochána do not care about the mental health of its members, and that efforts of management in this area were tokenistic. Again, this is reflective previous research in this area (Fallon, 2018; Kerrisk et al., 2021).
Participants listed a variety of barriers to accessing mental health support. A wide range of participants, irrespective of age, gender or length of service, highlighted the impact that stigma has on seeking mental health support. This confirms findings from previous research which has examined the mental health of the police in Ireland, and in other jurisdictions, which demonstrates that stigma is closely associated with police culture, regardless of jurisdiction (Clifton and Hancock, 2025; Drew and Martin, 2021; Fallon, 2018; Kerrisk et al., 2021; Milliard, 2020; Newell et al., 2022; Watson and Andrews, 2018). This has resulted in a situation whereby many members of An Garda Síochána will not simply speak about their mental health for fear of being labelled as weak or unreliable, or as one participant stated, being viewed as ‘windy or flaky’. Many members of An Garda Síochána seem to be simply getting on with their job and reinforcing a ‘tough it out' mentality, whereby they do not talk about, or seek support for their mental health. This is worrying, as unresolved mental health problems with police officers can result in the development of maladaptive coping behaviours such as drug taking and hazardous drinking (Ballenger et al., 2011; Brough et al., 2016; Davey et al., 2000, 2001; Irizar et al., 2021; Lindsay and Shelley, 2009; Syed et al., 2020).
Participants were also very aware of the potential negative impact that seeking mental health support could have on their career and cited this as a barrier to seeking mental health support. This is closely linked to the stigma that can be attached to seeking mental health support and has been highlighted in related research (Burns and Buchanan, 2020). Participants were conscious that seeking mental health support could leave a ‘mark’ on their character. This was especially true for those who worked in specialist units where firearms are required and is consistent with research which found that police officers were often reluctant to come forward due to fears over being labelled and having their firearm removed (Milliard, 2020). Milliard (2020) highlighted the promotion process itself as a source of stress and anxiety. This was not specifically highlighted by participants in this research, but nepotism in the promotions process has been highlighted in other research into An Garda Síochána (Fallon, 2018; Gavin and Porter, 2024; PwC, 2018).
A lack of trust in the mental health support services offered and a lack of trust in management were also highlighted as barriers to engaging with mental health support. Confidentiality is important to help avoid the stigma that may come from colleagues being aware of the condition of your mental health. A lack of confidentiality will see fewer people engaging with the available services or confiding in their line managers. This will also reinforce the ‘tough it out' mentality whereby people do not speak about their mental health, and this could potentially turn into a vicious cycle. A lack of trust and confidentiality was highlighted by Kerrisk et al. (2021) who suggested that the use of mental health services could increase if police officers believed that they were engaging with a truly confidential service.
Further barriers to accessing mental health support were a lack of time to engage with mental health support services and a lack of resources devoted to such services. Participants were critical of having to seek mental health support outside of working hours. Several commented on having to attend court or fill in for others who may be on sick leave on their days off, which nullifies any chance they may have of switching off from work. Shift work and the long hours worked by police officers can be detrimental to their personal lives, and having to use personal time to engage with mental health services is likely to put additional strain on the personal lives of police officers (Newell et al., 2022). The availability of a mobile app for such services might provide police officers with a better opportunity to engage with mental health services, as they can scroll through the options on their phone at their own convenience and when they have more time to really think about what they need. Several participants commented on the availability of such an app for mental health support. Since its launch in November 2021 (An Garda Síochána, 2021) there have been over 170,000 page views, and the most commonly viewed pages were ‘Useful Contacts’ and ‘Common Concerns’. Over 14,600 members of An Garda Síochána have registered with the app (An Garda Síochána, 2023 no). This shows that investment is taking place in mental health support and that members are aware of and are using the services (An Garda Siochana, 2023).
Participants were, however, critical of the overall level of resource devoted to mental health and many felt that despite recent investment and initiatives, more was needed to support the mental health of members of An Garda Síochána. One participant noted that while the organisation ‘has introduced programmes and initiatives as mentioned above which are good. However, due to lack of resources, lack of time, being overworked, burned out, lack of leaders to drive direction this all takes its toll on people' (Detective Sergeant, Female, 34 years of service). Some felt that the organisation should be more proactive when it comes to supporting the mental health of its members, rather than having a system where people need to self-refer for help. Several participants felt that counselling and support should be made mandatory for those who have experienced a traumatic incident. This could help to remove the stigma associated with seeking mental health support after experiencing a traumatic incident as well as removing the fear associated with the potential negative impact on one’s career if mental health support sessions were mandatory.
Conclusion
This paper has examined the barriers to engaging with mental health support for members of An Garda Síochána in Ireland. The main barriers we found to exist were stigma, the potential negative impact that it may have on career progression, a lack of trust in the services offered and in management, a lack of time to engage with mental health support services and a lack of resources devoted to such services. Our findings generally confirm findings in similar international research and this suggests that barriers to seeking and engaging with mental health support are deeply ingrained in policing culture. Participants in our research were generally aware of the mental health supports which are available for members of An Garda Síochána. Those participants who were long serving members were encouraged by recent developments and initiatives.
Others, however, were critical of the level of support available and felt that more needs to be done to support the mental health of members of An Garda Síochána into the future. Additional support needs to be accompanied by a cultural shift that does not stigmatise help seeking. Until this happens, members of An Garda Síochána will continue to avoid seek help for their mental health. As long as the policing culture encourages the idea that seeking help is a sign of weakness, then police officers will not seek help for issues which may be damaging their mental health. This will result in their mental health deteriorating and the issue becomes cyclical. Many participants cited issues related to police culture and the impact of stigma as being significant barriers to help seeking. Several participants were of the view that a process of mandatory mental health counselling in the aftermath of a traumatic incident could help alleviate the fear of seeking help for member of An Garda Síochána. Making such sessions mandatory might help cut though some of the cultural impacts, especially the stigma, which is often associated with help seeking, for those who are suffering from poor mental health.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.