
Abstract
Existing evidence suggests exposure to police activity negatively impacts the mental health of the policed. But research on whether, and why, police activity is correlated with the prevalence of mental health challenges among individuals and in specific areas remains piecemeal. We conducted a Rapid Evidence Assessment (REA) of the literature examining the association between policing and mental health, with a focus on investigating whether people in poor mental health are more likely to interact with police, whether police activity is higher in areas where people face more mental health challenges, and the reasons for these interactions. A total of 31 studies exploring the scale and reach of police encounters involving individuals dealing with mental health issues were included. The evidence suggests a pattern of heightened policing activity in specific geographic areas where individuals contend with elevated mental health challenges, and police spend more time dealing with individuals with mental health issues compared to the general population. These interactions occur for a wide variety of reasons, and people with mental health conditions encounter the police as victims, offenders, people in need and in other roles. Implications and directions for future research are discussed.
Keywords
Introduction
In recent years, the intersection between mental health challenges and police activities has emerged as an area of significant concern. Globally, societies are witnessing an increasing prevalence of mental health issues, a trend that has significant implications for public safety and policing (MPS, 2018). Mental health disorders, ranging from common conditions like anxiety and depression to more severe forms like schizophrenia and bipolar disorder, not only affect the wellbeing of individuals but also pose unique challenges to policing (Home Office, 2023a). The role of police officers has traditionally been centred around maintaining law and order, but they are increasingly finding themselves on the front lines of mental health crisis response (HMICFRS, 2018; Kane et al., 2020). This shift has raised important questions about the adequacy of police training, the resources available for handling such situations, and the impact of these encounters on both police officers and those with mental health conditions (Home Office, 2023a). In many communities, police are now often the first point of contact for individuals experiencing mental health crises (HMICFRS, 2018; Kane et al., 2020). This frequent interaction raises concerns about the potential for higher levels of police activity in areas where mental health challenges are more prevalent, which may have implications for all those living there.
There is, moreover, strong emerging evidence of a negative impact of police activity on the mental health of the policed (Jindal et al., 2022; McLeod et al., 2020), further underlining the importance of exploring the correlation between higher police activity and the prevalence of mental health challenges among certain individuals and in specific areas. This is for several reasons. First, if certain groups or communities with higher mental health needs also experience more police interactions this raises questions of fairness and equity, similar to those, for example, that lead to some ethnic minority communities feeling ‘over-policed and under-protected’. Second, identifying areas with a higher prevalence of mental health challenges and increased police activity can inform proactive measures to prevent adverse outcomes, and enable development of targeted interventions and support systems to address both mental health needs and the nature and consequences of interactions with the police. Third, this examination might provide insights into the dynamics of public safety and policing practice. It could help to determine whether police are being called upon to address mental health crises, or whether their presence may be contributing to mental distress in specific communities. If it is established that police spend more time in areas with mental health challenges, it might aid in determining whether resources should be redirected towards mental health services and community support rather than increased policing in these areas. This could also advocate for policy changes that promote alternative responses, such as crisis intervention teams or mental health professionals, to de-escalate situations and support individuals in distress. Finally, exploring the relationship between police and mental health might encourage greater collaboration between police, mental health professionals, and community organisations to ensure that individuals in need receive appropriate care and support rather than punitive measures.
This article presents the findings from a rapid evidence assessment (REA) that takes stock of the empirical evidence surrounding the patterns and trends in police activity specifically related to mental health issues. We systematically searched the literature with the following question in mind: Are people in poor mental health more likely to interact with police, and is police activity higher in areas where people face more mental health challenges? Given the limited research on this topic, our scope for this review was broad. We searched for and included in the REA any papers that assessed the relationship between a measure of policing and a measure of mental health, even if this analysis was not the central point of the paper.
The main objective of this article is to provide a narrative summary of the empirical research linking police activity to people who face, and to areas where people face, more mental health challenges, and to provide guidance for future research and inquiry. We proceed with a discussion of policing mental health. We then detail the search strategy for this REA, discuss the findings from the review and provide directions for future research.
Policing mental health
Police activity is disproportionately directed towards people on the margins of society. Many categories of people are especially likely to become the objects of police attention (Singleton et al., 1998), but the focus of this paper will be on people experiencing poor mental health who interact with police, as victims, witnesses, offenders, or for other reasons. Police are the ‘service of last resort’ and have always been involved with people in various forms of mental health crisis. But austerity-driven cuts to health and other services have in many cases left them as a service of first resort, the only agency available to respond to calls for help from people in various forms of distress. Research has shown that individuals with mental illnesses are more likely to come into contact with police due to a variety of factors, including inadequate access to mental health services, which can lead to a reliance on police during crises (Kesic, 2013; Ogloff et al., 2013; Puntis et al., 2018). Additionally, symptoms of mental illness can sometimes result in behaviours that attract police attention, such as public disturbances or behaviours perceived as threatening (Rueve and Welton, 2008). Moreover, studies show certain geographic areas - particularly crime hotspots - tend to also have high concentrations of mental health-related incidents. White and Goldberg (2018) and Weisburd and White (2019) highlight the overlap between areas of concentrated crime and mental health crises, suggesting that police are drawn to these environments due to the convergence of social, economic, and mental health-related issues. These factors help explain why police agencies may disproportionately engage with individuals experiencing mental health issues.
Current estimates suggest that there has been an increase in mental health-related demand on police services, with officers now spending anywhere from 5% to as much as 40% of their time responding to people with mental health problems (HMICFRS, 2018; Kane et al., 2020) 1 (it is highly likely that this extends to people with other health problems, too; Bradford, 2017). People with mental health problems are overrepresented in the criminal justice system (CJS) and feature disproportionately at all levels of the criminal justice pathway, from arrest to prison, and then release back into the community (Charette et al., 2014; Fazel et al., 2016). Having a mental health problem also increases the likelihood of recidivism soon after discharge and subsequent re-entry to the criminal justice system (Chang et al., 2015).
In response to this problem, there is increasing interest among criminal justice and mental health agencies in the UK in developing initiatives to improve relationships between police and people with mental health problems, reduce unnecessary arrests, reduce the use of inappropriate detentions under the mental health act section 136, and ultimately reduce the criminalization of those with mental health problems (Abramson, 1972; Lamb et al., 2002; Teplin, 1984; Torrey et al., 2010).
Naturally, different nations adopt diverse strategies when policing individuals with mental illnesses. For example, in the United States, Crisis Intervention Teams (CIT) are widely used, focusing on training officers to respond to mental health crises with de-escalation techniques and partnering with mental health professionals (Compton et al., 2014). In addition to CITs, the United Kingdom has implemented street triage models, where mental health professionals directly accompany police officers during such incidents (Puntis et al., 2018). Other countries, such as Australia (Ogloff et al., 2013) and Canada (Cotton and Coleman, 2010), also emphasise collaborative approaches between police and mental health services, but with variations in the level of integration and involvement of mental health professionals. Moreover, co-occurring disorders, such as the presence of both mental illness and substance use disorders, significantly impact how individuals interact with the criminal justice system. Literature consistently shows that individuals with co-occurring disorders face unique challenges, and both policing and treatment strategies must be adapted to address these complexities (Drake et al., 2001). Police interactions with people experiencing co-occurring disorders often require a nuanced approach due to the compounded nature of these conditions. For instance, research has shown that individuals with co-occurring disorders are more likely to be involved in repeated police interactions due to the overlapping symptoms of substance abuse and mental health crises, which can complicate the policing response (Abram and Teplin, 1991). Treatment options also differ, as integrated care models that address both mental health and substance use simultaneously have been found to be more effective than separate treatments (Mueser et al., 2003).
Such efforts are more important than ever considering the growing evidence of negative effects of policing on the mental health of the policed, and the emerging evidence that suggests that police activity exacerbates the mental health problems they face (Jindal et al., 2022; McLeod et al., 2020). For example, systematic reviews by McLeod et al. (2020) and Jindal et al. (2022) revealed a significant correlation between police encounters and adverse mental health outcomes in Black Americans, particularly youths. McLeod et al. (2019) found that experiences ranging from arrests to witnessing police actions were linked to issues like depression, PTSD, and anxiety. Jindal et al. (2022) extended these findings to Black youth, showing a connection between police interactions and various negative outcomes, including mental health issues, risky behaviours, and increased fear and hopelessness. Both reviews collectively underscore the profound impact of police encounters on the mental wellbeing of Black communities, especially the younger population.
Although there is therefore an increasing focus on the complex interplay between policing practices and mental health, this REA represents the first attempt to conduct a comprehensive review of evidence on the patterns of police activity among specific populations and within areas grappling with mental health challenges. Despite growing attention on the complex relationship between policing practices and mental health, there has to date been no review of the evidence exploring how police activity is patterned among certain populations and within specific regions facing mental health challenges, nor of the reasons why police come into contact with people with mental health issues.
Rapid evidence assessment
This article presents the findings from an REA of the empirical evidence on the patterning of police activity. An REA is no substitute for a systematic review or meta-analysis. Although an REA shares many of the same features as a systematic review (e.g. transparent search criteria, strict inclusion/exclusion criteria), it is not as extensive or exhaustive as a systematic review and there is more room for bias. For example, REAs can be carried out within a much shorter timeframe and there is less focus on the overall quality of the source material. Further, unlike a meta-analysis, it is not possible to draw conclusions about overall effect sizes from REAs. However, an REA allows for the inclusion of a broader diversity of sources compared to a systematic review or meta-analysis, enhancing the comprehensiveness of the evidence base.
The aim of this article is to take stock of the evidence base and to provide a narrative summary of the findings from which a systematic review and meta- analysis could follow. The main research questions guiding this REA are (1) are people in poor mental health more likely to interact with police; (2) is police activity higher in areas where people face more mental health challenges; and (3) for what reasons do police encounter people with mental health challenges, and where do they do so?
Method
Search terms for rapid evidence assessment.

Records identified through the database searches were then sifted to identify relevant studies. In selecting the studies, the following inclusion criteria were used: a. The study must report the findings of a quantitative or a qualitative empirical research project exploring the relationship between police activity and community mental health; b. Be available in English; c. Have been published from the year 2000 onwards.
EPPI-Reviewer six software
3
was used for all information management. Studies were first screened on title and abstract to remove any that were ineligible, based on the above inclusion criteria. Full-text screening was then conducted, and the inclusion criteria were again applied to exclude ineligible studies. The exclusion process was therefore conducted in two stages, as depicted in Figure 1. At the screening stage, papers were excluded if they did not meet basic eligibility criteria, which were defined as follows: studies had to be published in English, published after the year 2000, and related to policing and community mental health. Studies that did not fit these criteria were removed from further consideration. At the second stage of the review, additional papers were excluded based on more detailed criteria. This included papers where the full text was not available (such as theses unavailable for access) or where duplicate results had been published in journal articles. Papers were also excluded based on the nature of the evidence provided. Specifically, we excluded studies that did not measure or explore the relationship between policing and mental health, those that focused primarily on police training for mental health issues, or those that discussed police encounters in mental health contexts without exploring broader community interactions. Furthermore, papers focusing on perceptions of mental health service provision by police, commentaries, policy documents, magazine articles, or studies primarily examining the impact of policing on mental health were excluded. Rapid evidence assessment screening process.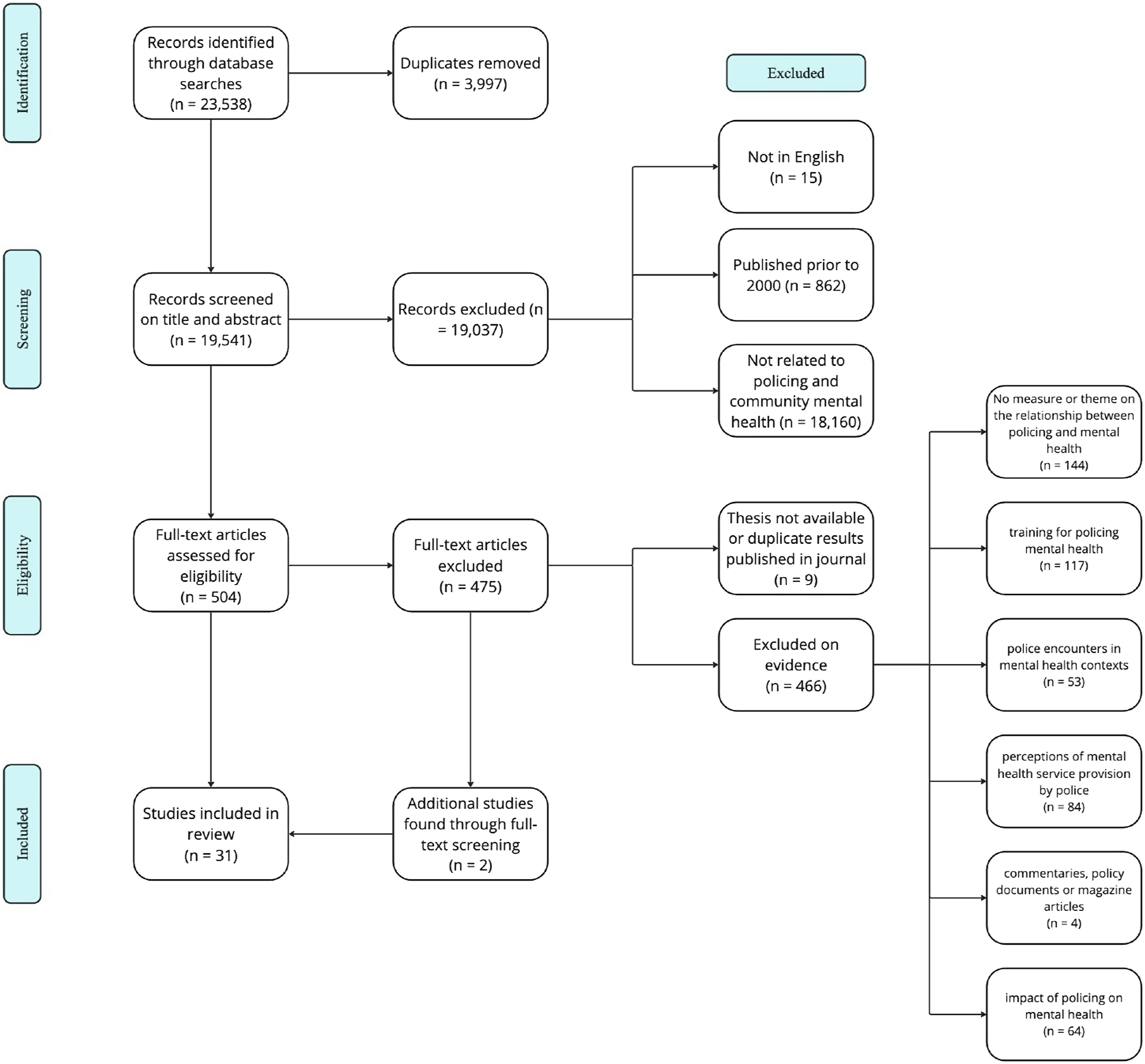
During the full-text screening, each study’s reference list was also screened to identify any relevant studies that did not appear in the database search. These studies were then screened, and the inclusion criteria applied. The screening process and final studies included are shown in Figure 1. Data extraction was then conducted on the studies included in the review (N = 31). Data extraction codes encompassed several key coding categories, including: (1) General information, documenting research type, participant demographics, and geographical context; (2) Aim and research design, detailing the study’s objectives and methodology; (3) Policing and mental health measures, noting the specific assessments used; (4) Analytical approach, describing the methodologies and techniques applied; (5) Findings on the policing-mental health relationship, highlighting insights into how police activities relate to mental health.
Results
A total of 31 studies (27 quantitative; four mixed methods) were included in this REA – see the Supplement Appendix for descriptive information about each, along with a summary of the main findings related to the research question. The full list of references for studies included in this REA is also available in the supplementary materials. In what follows, we explore the evidence concerning the prevalence of police activity in regions characterised by elevated mental health challenges, the likelihood of individuals in poor mental health to interact with police, and the reasons for and locations of police encounters with individuals facing mental health challenges.
The studies include data from 99,622 participants, 1,368,632 police contacts, events or incidents, and 4,332,100 calls for service: a total of 5,800,344 data points. Participants were aged 12-82 years old (where specified), including both male and female, Black and White, participants. The studies were predominantly from Canada (N = 12, 38%) and the United States (N = 8, 25%), with others coming from Australia (N = 3, 9%), New Zealand (N = 3, 9%), and the UK (N = 3, 9%). The reviews (N = 3, 9%) reported on data from the UK, USA, Australia, Canada, and New Zealand.
Study methods
Among the research studies analysed, seventeen (56%) adopted a cross-sectional research design, while four (13%) employed a descriptive research approach to record and interpret information about policing activity to capture a detailed snapshot of specific characteristics at a particular point in time. One study (3%) utilised a combination of both descriptive and cross-sectional methodologies. One (3%) study adopted a longitudinal research design, while five (16%) engaged in spatial analysis. Additionally, three (9%) of the studies conducted systematic reviews. The majority of the studies primarily focused on the examination of data routinely gathered by police and criminal justice agencies; and focused predominately on the frequency of interactions between individuals with mental disorders and the police, police involvement in them accessing mental health services, and the prevalence of calls for service related to individuals with mental disorders. Further details on the methodologies of the included studies are available in the Supplement Appendix.
Cross-sectional
The cross-sectional studies primarily investigated the link between police engagement and mental health, specifically examining the frequency and nature of police interactions (e.g. arrest rates and calls for service) with individuals experiencing mental health issues versus those without (Anstis and Thomas, 2022; Barfield, 2013; Bowden et al., 2022; Charette et al., 2014; Compton et al., 2023; Crocker et al., 2015; Koziarksi et al., 2022). They evaluated the impact of mental health on police behaviour in diverse settings, including cases of homelessness (Kouyoumdjian et al., 2019) and neighbourhood characteristics (Krishan et al., 2014), and investigated the geographical distribution of mental health-related police calls (e.g., as in Richter, 2010). Additionally, these studies explored factors predicting mental health apprehensions, with a focus on the influence of police contact (Shore and Lavoie, 2019). A variety of control variables were incorporated, covering aspects such as homelessness, a lack of social support, unemployment, substance abuse, and personality disorders, to account for key socio-demographic and other pertinent influences.
Descriptive
The descriptive studies employed various research methods. Key methodologies included: Leveraging police and custody records to extract quantitative data on demographic details, incident specifics, and mental health assessments, thereby identifying patterns and distributions within large datasets (O'Brien et al., 2011; Oluboku, 2019); Applying qualitative techniques to gather subjective information on individuals’ mental health and experiences with police, enriching the dataset with personal accounts and assessments (Oluboku, 2019); Utilising standardised forms (e.g. incident reports) to systematically collect detailed information on police encounters, specifically focusing on interactions with individuals with intellectual or developmental disabilities, to facilitate nuanced comparisons and analyses (Watson et al., 2022); Combining statistical data analysis with thematic content analysis of qualitative data sources, such as interviews and observational notes, to explore the context and detailed nuances of police involvement in mental health cases from multiple perspectives (Bendelow et al., 2019; Liegghio et al., 2017).
Longitudinal
The study by Dean et al. (2021) explored the connection between early childhood emotional/behavioural issues and later police encounters in a cohort of Australian children, tracked from school start in 2009 until age 13. It analysed teacher-rated developmental and behavioural assessments, focusing on how these early vulnerabilities might predict later police contact as persons of interest, survivors, or witnesses, while adjusting for socio-economic and cultural backgrounds to ensure reliable results.
Spatial analysis
These studies (Hodgkinson and Andresen, 2019; Huey et al., 2021; Koziarski, 2021, 2022; Vaughan et al., 2019) employed spatial analyses on police call data to explore the geographical patterns and concentrations of mental health-related incidents. Through techniques like Kernel Density Estimation and spatial autocorrelation tests, the research aimed to visualise and quantify how these incidents are distributed across different urban areas, identifying clusters and the extent of their concentration. Analyses ranged from exploratory visualisations of call concentrations to comparisons between mental health-related calls and other types of police interactions, offering insights into the spatial dynamics of mental health issues in policing within specific cities.
Systematic reviews
The systematic reviews investigated various aspects related to mental health and police interactions, encompassing both qualitative and quantitative analyses as appropriate to the research focus. Clugston and colleagues (2023) focused on the prevalence and characteristics of mental disorder and suicidality in police negotiation events, employing a qualitative synthesis to categorize findings thematically. Hallett et al. (2021) investigated the dynamics of Taser use on individuals in mental distress, combining qualitative and quantitative approaches for an integrative review, and also conducted a meta-analysis to ascertain prevalence rates of Taser use in such contexts. Livingston (2016) exclusively used quantitative studies to examine the rates of police arrests among individuals with mental disorders, the role of police in pathways to mental health care, and the frequency of police calls involving persons with mental disorders, applying statistical analyses to explore differences across study variables.
The scale and reach of police encounters with individuals dealing with mental health issues
This next section provides a narrative summary of the findings from the REA, specifically focusing on the scale and reach of police encounters with individuals dealing with mental health issues. There is substantial evidence supporting the idea that police activity is higher both in areas where people face more mental health challenges and among individuals who themselves face these challenges; and these findings relate to the reasons police encounter people with mental health challenges. This narrative unfolds through three key dimensions: heightened police engagement in regions marked by mental health challenges, recurrent encounters between police and individuals grappling with mental health issues, and a notable disproportionality in policing practices towards those with mental health concerns.
Higher police activity in areas with mental health challenges
Studies indicate that police activity is more prevalent in areas where people face mental health challenges. Often, specific locations are identified as ‘hot spots’ where police respond to mental health-related incidents.
Three studies conducted in Canada pinpointed precise locations where police activities related to mental health issues occurred. In Koziarski’s (2021) research, data spanning 6 years of calls for service in a small Canadian city were analysed, revealing a significant concentration of calls related to Persons with Prevalent Mental Illness (PwPMI) in specific spatial units. Notably, there were two PwPMI call hot spots. The first, larger area was situated within the downtown core where there is a concentration of numerous social services and public health units. The second, smaller area was situated in the north-east corner of the city at the local hospital. Hodgkinson and Andresen’s (2019) study analysed hot spots of police service calls in another Canadian city, revealing differences between mental health-related call types. The kernel density map of the city revealed three hot spots: one to the east (a homeless shelter), one to the north (a motel used for short-term housing), and one to the west (a cluster of low-income residences for known offenders). Total mental health calls had a single hot spot at the homeless shelter, which aligned with expectations due to the connection between mental health issues and homelessness. Known mental health and attempted suicide had two hot spots (homeless shelter and residential cluster), while disturbance and drunkenness had one (homeless shelter), contributing to the overall hot spot for total mental health. In another urban Canadian setting, Vaughan et al. (2019), used a spatial point pattern test and kernel density estimation to compare the spatial distributions of calls for service involving emotionally disturbed persons (EDP) to all other police contacts. Findings indicated that there were significant variations among these two calls-for-service, with EDP calls clustering in just a few specific places. To understand this better, the authors looked at certain places that might attract EDP incidents. The sole hospital within the city was contained within the identified hotspot areas. It was also observed that a large proportion of public health units (80%), private and public substance use and/or addiction services (73%), pharmacies (69%), and walk-in clinics (67%) were located within these concentrated areas. Similarly, more than half of the alcohol points-of-sale (56%) and criminal justice services (55%) were located in the identified areas.
Current research therefore indicates a potential link between locations frequented by individuals facing mental health challenges and the clustering of police activity, operationalised as mental health-related calls for police service (Hallett et al., 2021; Hodgkinson and Andresen, 2019; Koziarski, 2021; Vaughan et al., 2019). The use of Tasers in mental health crises, however, does not seem to be limited to specific settings. A third of the studies (n = 10) included by Hallett et al. (2021) systematic review identified the physical environments within which Tasers were deployed, particularly in relation to use on those experiencing mental distress. Narrative synthesis of those results revealed that the use of Tasers in mental health crises occur in various settings, including public places, private residences, and healthcare facilities.
Frequent interactions between police and individuals with mental health issues
Available data confirms that police frequently interact with individuals with mental health issues and the police. This includes arrests, police involvement in their pathway to mental health care, and police dispatches and encounters involving people with mental health issues. Livingston’s (2016) comprehensive analysis of 85 studies found that one in four people with mental disorders had a history of police arrest 4 . Additionally, one in 10 individuals had police involved in their pathway to mental health care in some way 5 , and approximately one in 100 police dispatches and encounters involved people with mental disorders 6 .
Several individual studies underscored the significant frequency of interactions between individuals with mental health issues and the police. Liegghio et al. (2017) study focused on children and youth accessing mental health services, revealing that approximately one in six of them had police involvement when seeking help. This often occurred due to the need for support at home for distressed children or concerns about their behaviour in the community. Koziarski et al. (2022) research highlighted the involvement of people with mental illness in calls for police service. People with mental illness were involved in a substantial 11% of these calls. Logistic regression models showed that people with mental illness were more likely to be involved in certain types of calls compared to others. In Hodgkinson and Andresen’s (2019) analysis of hot spots of police calls for service in a Canadian city, ‘Total Mental Health-related’, a subcategory of known mental health calls, attempted suicide, disturbance, and drunkenness, ranked as third most common (14% of all calls for service).
Moreover, Durbin et al. (2010) study, which analysed trends in police contacts related to mental illness, suicide-related contacts, and mental health apprehensions, emphasized the increasing frequency of police encounters with individuals experiencing mental illness. Linsley and colleagues (2007) found that 20% (41 individuals) of the cases studied who died by suicide had police interactions in the 3 months prior to their death, either as crime victims or alleged offenders. Remarkably, as many of these individuals had police contact in those 3 months as had seen a mental health professional in the year before their suicide. This indicates that interactions with the police are relatively common among those who later die by suicide, with nearly 25% of suicide cases in the study having engaged with the criminal justice system in the 3 months preceding their death.
Police interactions with individuals with mental health issues are shaped by the nature of calls received and the time spent handling these situations, often involving vulnerable groups such as youth and ethnic minorities, with issues including substance abuse and self-harm (Shore and Lavoie, 2019). These calls cover a wide range of scenarios, from wellness checks to situations involving victims, complainants, or suspects with mental health issues (Huey et al., 2021). There is a trend towards increased collaboration with mental health agencies, preferring options like home or healthcare facility transportation over detention. Despite many incidents being resolved without formal action, they still consume significant police resources (Hendy et al., 2022; Shore and Lavoie, 2019; Watson et al., 2022; Yang et al., 2018). When formal action is needed, such as transporting individuals to hospitals during mental health emergencies, the challenges for police escalate, highlighting the complex dynamics and resource demands of these interactions (Bendelow et al., 2019; Clugston et al., 2023; Yang et al., 2018).
Police spend more time dealing with individuals with mental health issues
Studies highlight that police spend more time dealing with individuals with mental health issues when comparing police engagement with individuals with mental health challenges against those without such conditions. This disproportionality is evident in various aspects of police activity, including police contact, arrests, charges, the use of force, and Taser usage.
There appears to be a higher prevalence of Taser usage during mental health emergencies. For example, Hallett et al., 2021 research highlighted the relatively common use of Tasers in mental health crises, with individuals experiencing mental distress subjected to a higher prevalence of Taser usage compared to the general population. Specifically, of all recorded usage in the 31 studies reviewed, overall prevalence of Taser use on individuals experiencing mental distress was 28%. Moreover, O'Brien and colleague’s (2011) study on Taser deployment showed that Tasers were more likely to be discharged during mental health emergencies than during criminal arrests, raising concerns about their disproportionate use on individuals with mental illness 7 .
There also appears to be increased police contact among children with emotional or behavioural problems. Dean et al. (2021) study focused on young children and their contact with the police in relation to emotional or behavioural problems identified by teachers. Findings indicate that emerging emotional or behavioural problems and developmental vulnerabilities in young children are linked to an increased risk of police contact. Specifically, children who were identified by their teachers as having emotional or behavioural problems at school entry had a significantly higher incidence rate of police contact for any reason. In fact, the incidence rate of police contact was twice as high for children with these problems compared to those without such problems.
Studies pointed to increased arrests for persons with serious mental illness, and greater use of force against individuals with mental illnesses, co-occurring disorders, and substance abuse disorders. Barfield’s (2013) findings indicated that persons with serious mental illness are more prone to arrests, seemingly due to higher rates of substance abuse. Specifically, substance abuse significantly predicted arrests among those with serious mental illness. Crocker and colleagues (2015) found that persons with mental illness were more likely than those without mental illness to be in contact with police as suspected offenders, to have a greater number of offences, to reoffend more quickly, and to be formally charged for a suspected offence. Moreover, Kesic et al. (2013) study found that the police were more likely to use or threaten to use weapons, like pepper spray, on people who seemed to have mental health issues. This was the case even if the person’s behaviour was not necessarily aggressive. Morabito’s et al. (2017) study indicated that individuals with mental illnesses, co-occurring disorders, and substance abuse disorders, as compared to their non-disordered peers, are more likely to face the use of force and be perceived as resistant by police.
Individuals experiencing homelessness are also subject to a higher likelihood of police interaction, with minor offenses more likely to result in arrests when involving individuals with mental illness. Kouyoumdjian and colleague’s (2019) longitudinal study encompassed 547 adults grappling with mental illness who found themselves homeless at the outset. Participants were randomised into either an intervention group, receiving scattered-site housing with rent supplements and varying levels of mental health services, or a control group that continued with standard community services. In the year preceding randomisation, a substantial 56% of participants had interactions with police. These interactions persisted in Study Years 1 and 2, albeit with a slight decline, to 52% and 43%, respectively. Examining specific incidents across the 3 years, 41% of the 518 occurrences pertained to victimisation, 46% were linked to mental health assessments, and 22% centred around instances of suicidal behaviour. Of particular note, the odds of encountering any form of police interaction within the past 90 days were markedly elevated among the unhoused, with a 47% higher likelihood for those experiencing homelessness compared to those who were stably housed. Charette and colleague’s (2014) study showed that police interventions involving individuals with mental illness often related to less severe offences. However, minor offences involving individuals with mental illness were more likely to result in arrests compared to those involving individuals without mental illness. Compton and colleagues (2023) reported similar findings. Most arrests involving people with serious mental illnesses were for misdemeanours, specifically class A misdemeanours, and this class comprised a larger proportion of arrests for those with the indicator than of arrests for those without it. Bowden and colleague’s (2022) study revealed that while young individuals with autism were not disproportionately represented within the criminal justice system, notable disparities were evident in the nature of offences committed and the rates of incarceration among those charged with offenses. Specifically, young adults with autism exhibited lower rates of police contact, yet when such contact occurred, they were more frequently confronted with severe charges.
Discussion
While academic interest in the relationship between policing practices and mental health has been growing, this REA marks the first effort to systematically review and analyse evidence concerning the patterns of police activity within specific populations and regions facing mental health challenges, and the reasons why police encounter people with mental health issues, vis and vis other populations and other types of areas.
Overall, the evidence suggests that police activity is higher amongst people who face, and in areas where people face, more mental health challenges. There appears to be a discernible increase in police involvement in areas characterised by prevalent mental health issues. This heightened engagement is marked by frequent interactions between police and individuals struggling with mental health conditions. These interactions occur for a wide variety of reasons, and people with mental health conditions encounter the police as victims, offenders, people in need and in other roles. Additionally, there seems to be a significant imbalance in the way policing practices are applied to those with mental health concerns, indicating an unequal focus in these encounters.
Our findings are particularly concerning in light of emerging patterns of police activity and the growing body of evidence indicating a detrimental impact of such activity on the mental health of those policed (Jindal et al., 2022; McLeod et al., 2020). The findings of this REA not only fill a significant gap in academic research but also draw attention to the urgent need for a deeper understanding of these complex dynamics.
Specifically, we identified two key findings: heightened police activity in areas with greater mental health challenges, and a higher frequency of interactions between police and individuals with mental health issues (compared with those without such issues; i.e. they are more likely to have police contact than population proportions would suggest). These findings have implications for policy, practice, and community engagement. The increased police activity in areas with more prevalent mental health issues signals the need for specialised police training and interventions to ensure sensitive responses to mental health crises. The frequent interactions between police and individuals with mental health challenges highlight the necessity for re-evaluating policing strategies, equipping officers with the skills to engage empathetically and effectively in these situations.
Furthermore, police spending more time dealing with individuals with mental health issues raises concerns about equity and fairness, pointing to the need for policy reforms that address biases and systemic issues within policing practices. To address these challenges, effective collaboration between mental health services, social services, and police forces is crucial, particularly in areas with heightened police activity. This collaboration should aim to foster supportive and non-criminalising interactions, while also addressing the existing gaps in access to mental health services that contribute to this over-policing.
Limitations and future research
While our REA provides valuable insights into the relationship between mental health challenges and police interactions, it has of course a number of limitations.
The findings regarding the frequency of interactions between police and individuals facing mental health issues, as well as the heightened policing of these individuals, are supported by a broad base of evidence, including 18 cross-sectional studies, four descriptive studies, 1 study employing both methodologies, 1 longitudinal study, and three systematic reviews with meta-analyses. This breadth of evidence allows us to assert with a reasonable degree of confidence that (a) police frequently encounter individuals with mental health issues and (b) the police spend more time dealing with these individuals, compared to the general population. However, it is important to acknowledge the limitations inherent in these findings, particularly the heavy reliance on cross-sectional studies. While these studies provide valuable snapshots, they limit our ability to infer causality. The need for more longitudinal and experimental studies remains critical to further explore the causal pathways that lead to heightened police engagement with individuals experiencing mental health challenges.
The idea that police activity is concentrated in areas with a higher prevalence of mental health challenges is less robustly supported, as this finding is based on a smaller subset of five studies. These studies, including contributions by Vaughan et al. (2019), Hodgkinson and Andresen (2019), and Koziarski (2021), use methodologies such as Kernel Density Estimation (KDE) to suggest an association between geographic areas and mental health-related police calls. While these findings provide important initial insights, they call for more rigorous research methods to better understand this relationship. Koziarski (2021), for instance, advocates for more advanced research approaches to explore how location impacts the frequency and nature of police interactions with individuals facing mental health issues. Indeed, it is unsurprising that individuals with mental health issues frequently encounter the police. However, the specific reasons behind these interactions remain less understood.
Additionally, it is important to consider the limitations of the review method itself. While REAs are efficient, they may introduce bias due to their limited scope and time constraints. As such, the findings of this review should be interpreted with caution. Future research is encouraged to undertake a systematic review for more comprehensive insights and, if possible, a meta-analysis to empirically strengthen the understanding of the link between police activity and areas with high mental health challenges, offering a more detailed and quantifiable analysis of this complex relationship.
Conclusion
This REA represents the first comprehensive effort to examine and synthesise the empirical evidence on the relationship between police activity and mental health challenges among individuals and within communities. Our findings indicate with a reasonable degree of certainty that police frequently interact with individuals facing mental health issues, and that there is a tendency for heightened police attention towards these individuals compared to the general population. However, the assertion that police activity is more intense in areas with higher prevalence of mental health challenges requires further empirical validation. Additional research is needed to better understand and substantiate the idea police interactions with individuals experiencing mental health issues are geographically clustered. Such research would not only clarify the specific factors driving these interactions but also assess whether these findings are generalisable across different regions, cultures, and policing policies. Establishing the broader applicability of these findings is essential for informing effective interventions and policies that can be adapted to diverse contexts.
Supplemental Material
Supplemental Material - Policing and mental health: A rapid evidence assessment of the patterning of police activity
Supplemental Material for Policing and mental health: A rapid evidence assessment of the patterning of police activity by Arabella Kyprianides and Ben Bradford in The Police Journal.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the Economic and Social Research Council ES/X003434/1.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.