
Abstract
To guide the prevention of policing in persons experiencing homelessness and mental illness, we examined police interactions in this population by combining data from At Home/Chez Soi and Montreal police databases (N= 454). We explored the types, initiators, locations, and mental health/judicial outcomes of interactions over four years, identifying sub-groups using latent class analysis and then comparing sociodemographic and psychosocial variables between groups. Four groups emerged: few, mainly as a suspect, diverse, and frequent and diverse interactions. The characteristics of participants with more suspect interactions are described. Grouping suggested the policing of behaviors associated with homelessness and underreporting of victimization.
Long-Form Abstract
Police services have become highly involved in interventions with vulnerable populations over the years, notably with persons experiencing homelessness and mental illness. In order to best allocate resources for preventive interventions with this population, we aimed to examine patterns of police interactions in people experiencing both homelessness and mental illness and their associated psychosocial correlates. Combining data from the At Home/Chez Soi study and Montreal police databases (N = 454), we explored the types, initiators, locations, and mental health or judicial outcomes of police interactions in this population over a 4-year period. Further, we used latent class analysis to identify groups characterised by the frequency of contacts and distinguishing interactions as a suspect, victim, or person in crisis. We compared sociodemographic and psychosocial variables between emerging groups. Sixty-two percent of participants had at least one interaction, most often as suspects. Four groups emerged: few interactions, interactions mainly as a suspect, diverse interactions, and frequent and diverse interactions. Participants with more suspect interactions were more likely to be younger men with a substance use disorder, poorer community functioning, and no past stable employment. Grouping of interaction patterns suggested the policing of behaviors associated with homelessness and underreporting of victimization. We discuss policy and service delivery implications.
Introduction
Homelessness is increasingly recognized as a public health issue as people who are homeless or unstably housed have higher rates of emergency-service use, physical and mental health problems, and premature mortality (Fazel et al., 2014; Sleet and Francescutti, 2021). Amongst the homeless population in high-income countries, 76.2% live with at least one mental disorder such as alcohol or drug-abuse disorders, major depression, or schizophrenia spectrum disorder (Gutwinski et al., 2021). According to recent Canadian data, people who have experienced unsheltered homelessness (i.e., having lived in a homeless shelter, a makeshift shelter, or in outdoor spaces) and hidden homelessness (‘couch-surfing’ - temporarily staying with friends, family, or others) are three times more likely to report fair or poor mental health than those who have experienced neither (28% vs 9%) (Uppal, 2022).
In addition to significant healthcare needs, people who experience both homelessness and mental illness have a high lifetime prevalence of arrests, convictions, and incarcerations (Roy et al., 2014). Disproportionate criminal justice involvement (CJI) in this group is partly attributed to the “criminalization of homelessness”, that is the penalization of behaviors associated with homelessness including loitering, trespassing, and survival-driven behaviors (i.e., panhandling, sex work, theft, etc.) (Chesnay et al., 2013; Robinson, 2017). Furthermore, people with a mental illness are reportedly twice as likely as those without a disorder to be arrested for similar offenses (Charette et al., 2014). The paucity of community mental health alternatives to institutionalization are thought to contribute to this judicialization of mental illness, with police services increasingly responding to mental health crises (Marcus and Stergiopoulos, 2022; Roesch and Goossens, 2022). People with a mental illness, and in particular women and people experiencing concomitant homelessness, are also more likely to be victims of crimes than the general population, creating additional contact with police services (Desmarais et al., 2014; Gutwinski et al., 2021; Marr et al., 2023). Police interactions among homeless persons with mental illness may have numerous deleterious effects such as further CJI, fragmented health care, trauma, and re-victimization. People with a mental illness also report positive experiences where police facilitated transfers to health services during a crisis or responded to victimization (Brink et al., 2011; Livingston et al., 2014).
A recent Canadian study examined encounters between police and people experiencing mental illness and homelessness (Kouyoumdjian et al., 2019). Among people with a mental illness, the odds of any police interaction within a 3-month window were 47% higher for homeless than stably housed people (Kouyoumdjian et al., 2019). Interactions included incidents of victimization, mental health crises, threatened or attempted suicide, and suspicion of offending. Some Canadian research has also employed multilevel modelling specifically to identify predictors of criminal convictions in this population (Parpouchi et al., 2021). Moreover, the predictors of specific CJI trajectories (i.e., “Multiple Disturbances” and “Non-violent Frequent User”), have also been studied in this population (Roy, Crocker, Nicholls, Latimer & Isaak, 2016b). However, the current literature does not reflect the characteristics of more common policing interactions – such as contact for noncriminal and criminal reasons, crisis calls, or ticketing – which precede arrest and may be partly influenced by different individual factors (Parpouchi et al., 2021). In addition to identifying such risk factors and thus early-intervention targets for all persons experiencing homeless and mental illness, distinguishing between patterns of police interactions could help delineate sub-groups of persons with particular risks, needs, and opportunities for the prevention of CJI.
In the present study, we thus aimed to retrospectively: (1) describe the nature and outcome of police interactions with people experiencing homelessness and mental illness; (2) model heterogeneity and identify patterns of interactions as a suspect, victim, or person in crisis; and (3) identify the psychosocial correlates associated with such patterns.
Methods
This study examined participants from the Canadian At Home/Chez Soi randomized controlled trial (RCT) of Housing First (Goering et al., 2011), recruited between 2009 and 2011 in Montreal. Eligibility criteria for the trial included being absolutely homeless or precariously housed, at least 18 years old, and having a diagnosis of mental illness, with or without a substance use disorder. Mental illness was defined as a psychotic disorder, mood disorder with psychotic features, major depressive episode, manic or hypomanic episode, panic disorder or posttraumatic stress disorder, as evaluated using the DSM-IV criteria on the Mini International Neuropsychiatric Interview (Lecrubier et al., 1997). Additional details on the trial, including descriptions for scales included in this study, are available through the registered protocol (Goering et al., 2011). The present study was approved by the appropriate institutional research ethics board, including additional approval for the use of administrative police data. All participants provided signed informed consent for interviews and data access.
Participants
While 469 participants were recruited in Montreal, 454 were included in the present analyses; one participant did not consent to administrative justice data collection, two participants’ police files were irretrievable, and 12 participants passed away over the study period.
Variables of interest
Statistical analyses
Using latent class analysis (LCA) in Mplus version 8, we identified groups which presented similar patterns of police interactions (i.e., statistical classes), based on frequency of interactions per subject and three indicator variables computed from the 4-year sum of interactions as suspect, victim, and person in crisis (Winsorized at the 99th percentile). We tested the plausibility of two-to six-class solutions, accounting for sufficient sample sizes, interpretability of resulting groups, and avoiding nonconvergence (Nylund-Gibson et al., 2023). The best solution was selected based on theoretical interpretation (i.e., so that groups are qualitatively and quantitatively distinct), parsimony (fewer groups preferred) and the following fit indices: the Bayesian Information Criterion (lowest is preferred), entropy (>0.80), and the bootstrapped likelihood ratio test (Nylund et al., 2007). We then assigned individuals to groups that were most consistent with their own patterns of interactions based on their maximum posterior probability estimate and bivariate analyses (chi-square analyses and analyses of variance) (Bolck et al., 2004; Heron et al., 2015; Vermunt, 2017). Sociodemographic analyses were conducted in R software v.2022.07.02 + 576. For all analyses, significance level was set at p < .05.
Results
Sample description
Sociodemographic and clinical characteristics of the sample.
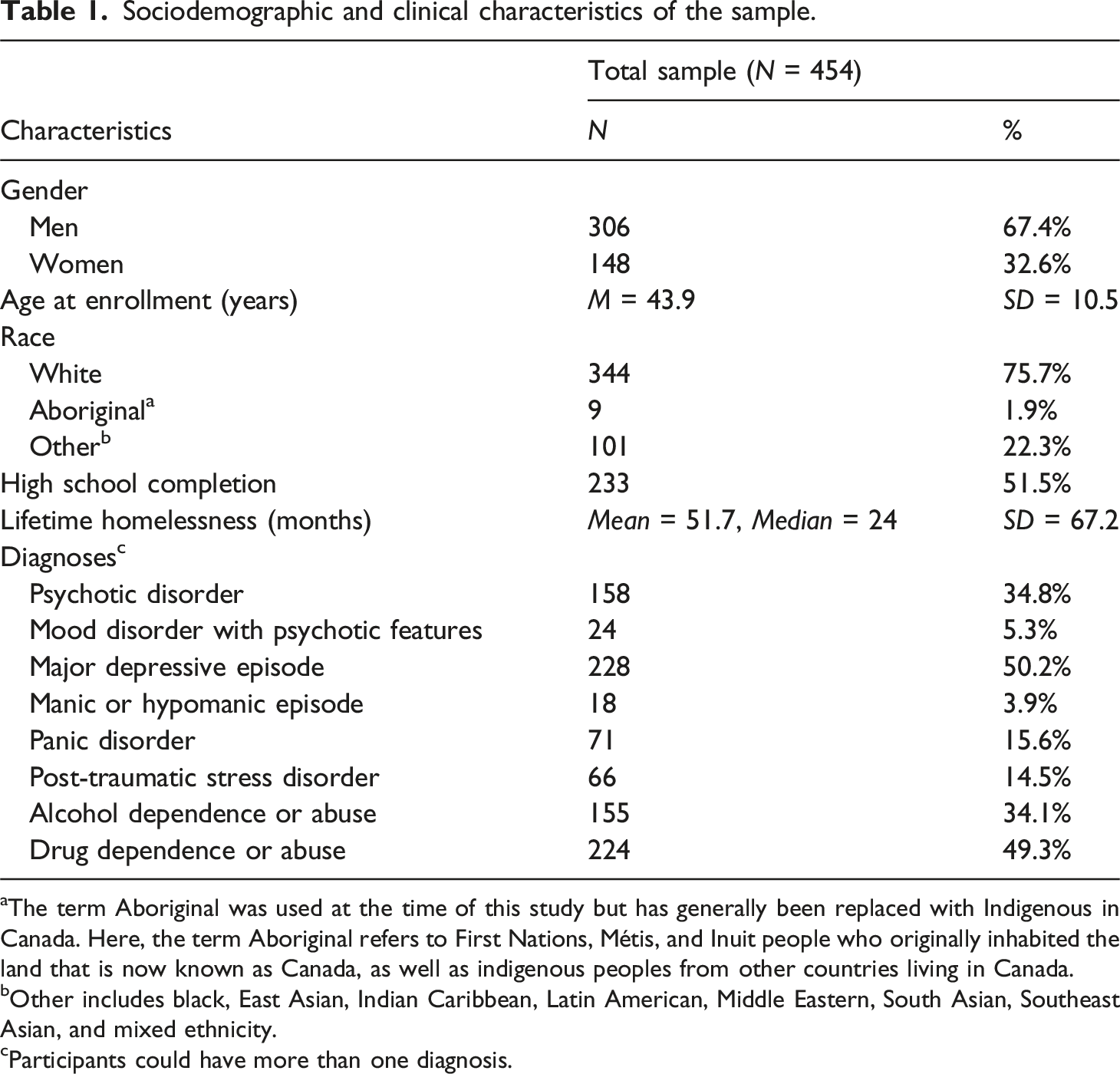
aThe term Aboriginal was used at the time of this study but has generally been replaced with Indigenous in Canada. Here, the term Aboriginal refers to First Nations, Métis, and Inuit people who originally inhabited the land that is now known as Canada, as well as indigenous peoples from other countries living in Canada.
bOther includes black, East Asian, Indian Caribbean, Latin American, Middle Eastern, South Asian, Southeast Asian, and mixed ethnicity.
cParticipants could have more than one diagnosis.
Types of policing interactions
Over the 4-year period of the study, 284 (62.6%) participants had at least one police-reported interaction, cumulating 1190 police interactions as suspects (77.5%; M = 2.6/person), 170 as victims (11.1%; M = 0.4/person), and 176 as a person in crisis (11.5%; M = 0.4/person). Of people with at least one interaction, 50% had at least one contact as a suspect, 23.6% as a victim, and 18.9% as a person in crisis. Participants without any police interactions were significantly older, identified more often as women, reported higher levels of high school completion, had experienced homelessness for shorter durations, and were less likely to have a diagnosis of psychotic disorder, alcohol abuse, or substance abuse (p < .01).
Type and characteristics of police interactions.
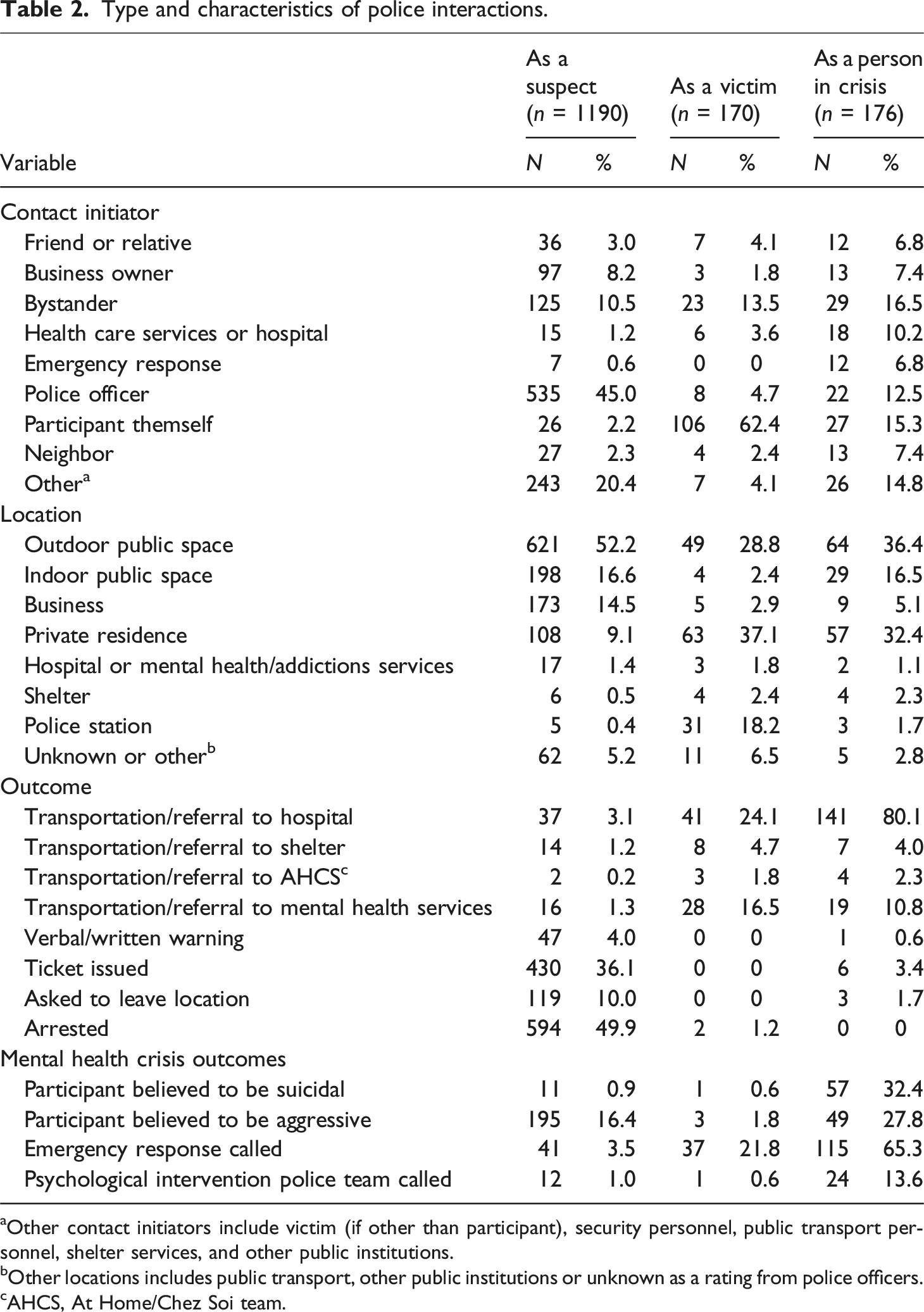
aOther contact initiators include victim (if other than participant), security personnel, public transport personnel, shelter services, and other public institutions.
bOther locations includes public transport, other public institutions or unknown as a rating from police officers.
cAHCS, At Home/Chez Soi team.
Groups of policing interactions
Latent-class analysis model fit statistics.
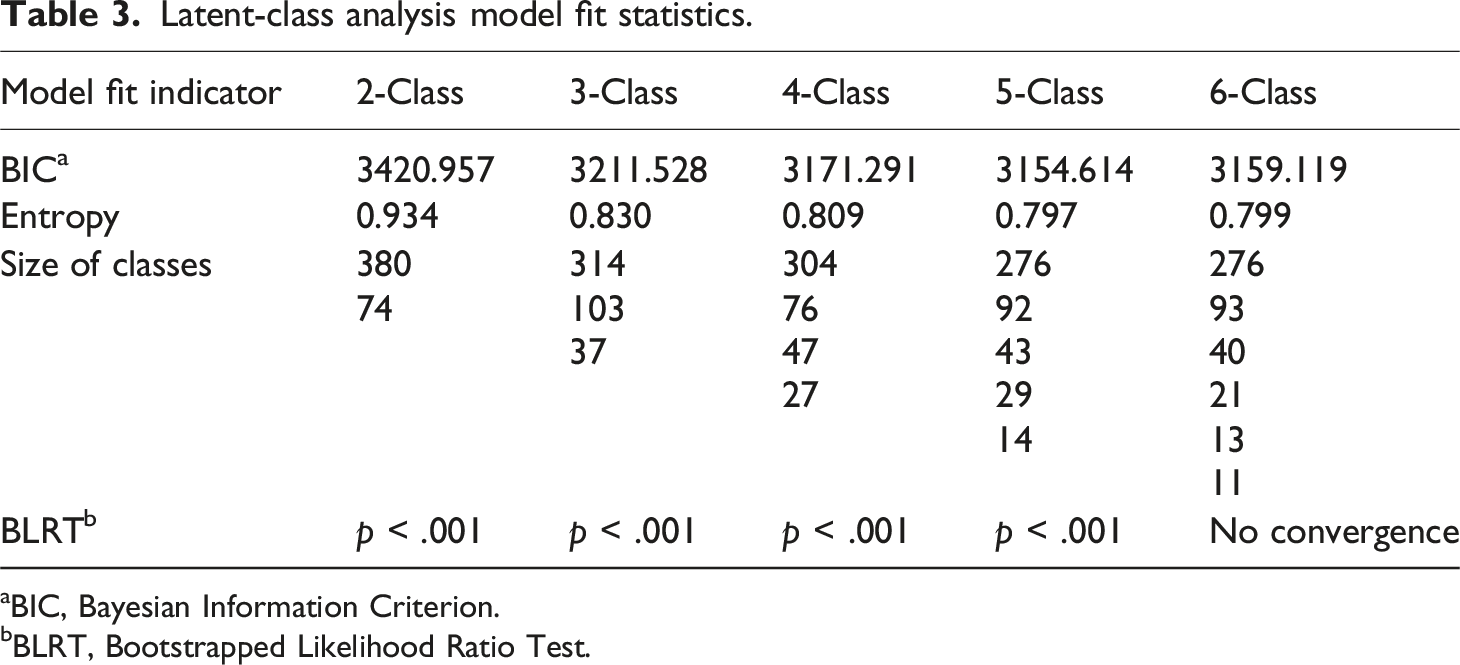
aBIC, Bayesian Information Criterion.
bBLRT, Bootstrapped Likelihood Ratio Test.
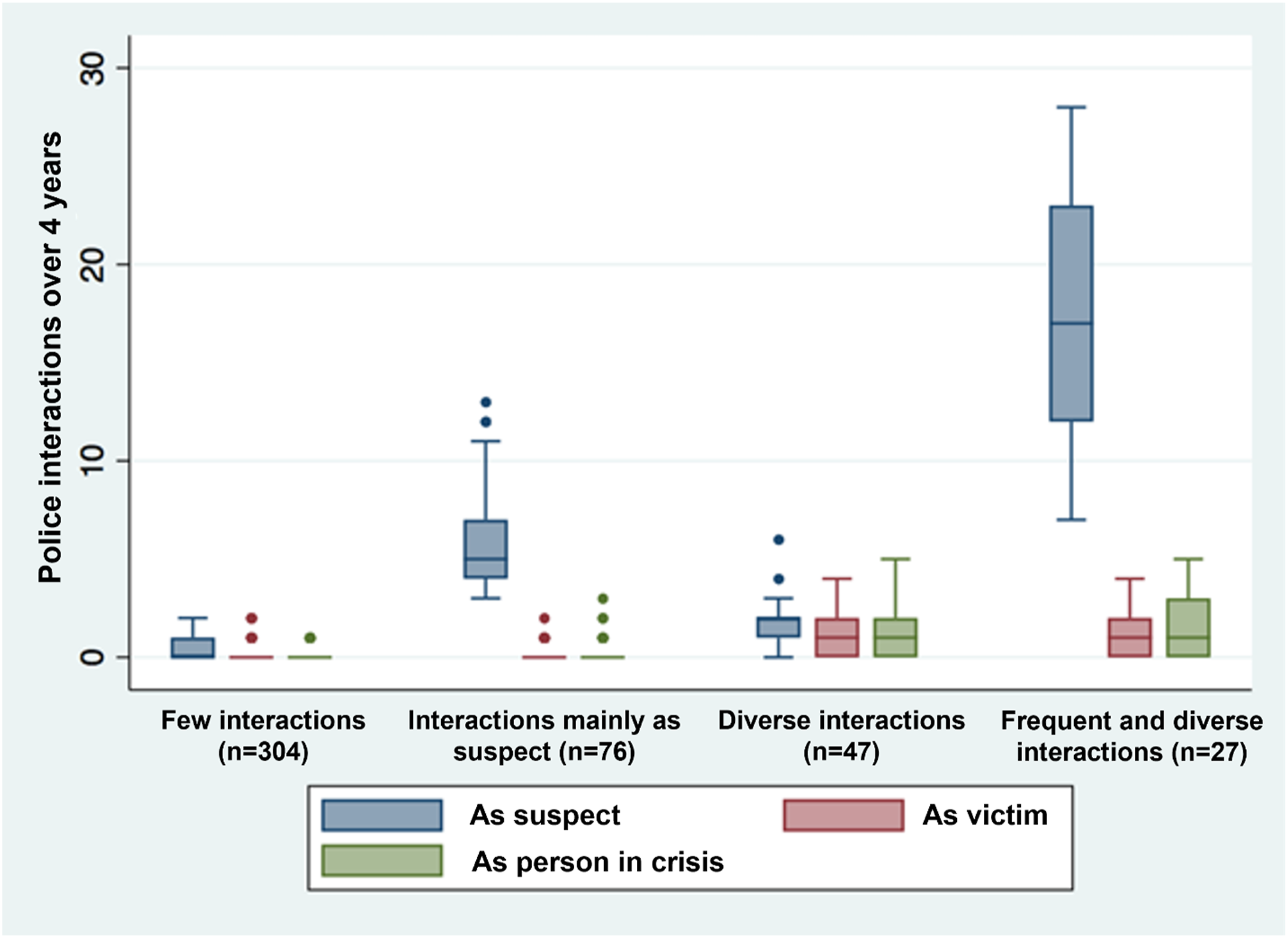
Police interactions by group and status of participants. Note. Box plot displaying the number of each type of police interaction over the 4-year follow-up per class. Boxes represent the interquartile range (IQR), and dots represent outliers (beyond 1.5 × IQR).
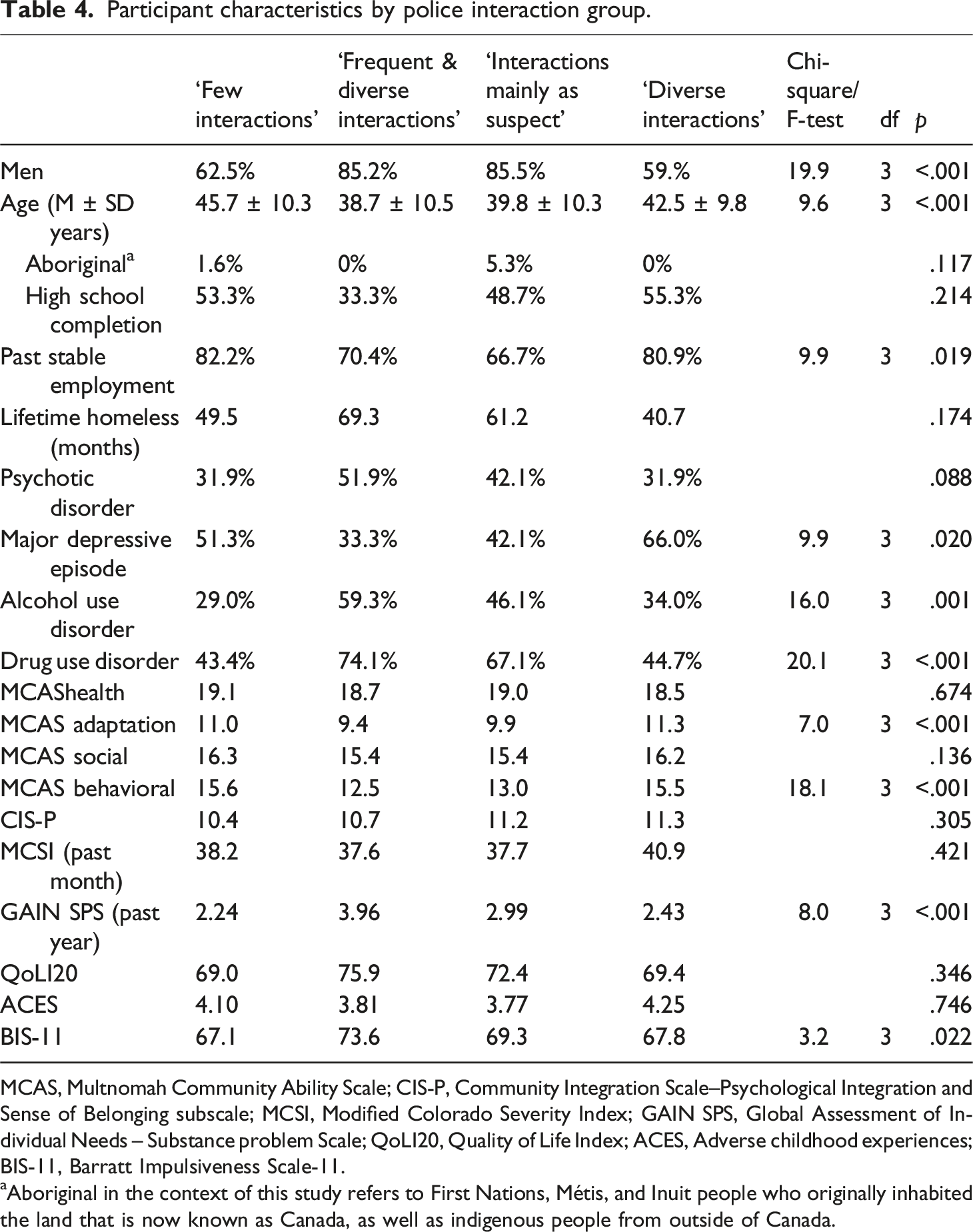
Participant characteristics by police interaction group.
MCAS, Multnomah Community Ability Scale; CIS-P, Community Integration Scale–Psychological Integration and Sense of Belonging subscale; MCSI, Modified Colorado Severity Index; GAIN SPS, Global Assessment of Individual Needs – Substance problem Scale; QoLI20, Quality of Life Index; ACES, Adverse childhood experiences; BIS-11, Barratt Impulsiveness Scale-11.
aAboriginal in the context of this study refers to First Nations, Métis, and Inuit people who originally inhabited the land that is now known as Canada, as well as indigenous people from outside of Canada.
Discussion
Two thirds of people experiencing both homelessness and mental illness in Montreal also experienced police interactions over the 4-year period, comparable to yearly rates reported in Toronto’s At Home/Chez soi cohort which also used administrative data (55.8% in the year prior to the trial and 43%–52% post-trial) (Kouyoumdjian et al., 2019). Participants were most often considered suspects and ultimately arrested in about half of instances. Despite these macro-level trends, interactions showed heterogeneous patterns, especially regarding who initiated contacts and in which location. Modeling police interactions using LCA shed light on four overarching groups, characterized by the nature (i.e., as a suspect, a victim, or a person in crisis) and frequency of interactions.
For suspect-dominant groups (i.e., “interactions mainly as suspect” and “frequent and diverse interactions”), significant correlates included younger age, male gender, substance use disorders, greater severity of substance use problems, and greater impulsivity. In line with the interpretation that suspect interactions lead to more arrests and would be the contacts to lead to CJI, these findings replicate most commonly identified predictors of CJI in this population (Luong et al., 2021; Parpouchi et al., 2021; Roy, Crocker, Nicholls, Latimer, Gozdzik, et al., 2016a; Roy et al., 2014). Present findings therefore further underscore the need to target substance abuse as a criminogenic factor (Luong et al., 2021). Moreover, most suspect interactions resulted in arrests, tickets, or the individual being asked to leave the premises. The vast majority did not involve an aggressive participant. Moreover, 45% of suspect-interactions were initiated by police. Though it was not possible to ascertain exact reasons for individual tickets or arrests, when taken together these results lend support to the criminalization of homeless hypothesis. That is, similarly to previous studies (Kouyoumdjian et al., 2019; Roy, Crocker, Nicholls, Latimer, Gozdzik, et al., 2016a), participants might have been subjected to policing for situations which would be better addressed through psychosocial support, such as breaching parole or probation conditions, using or carrying drugs, committing survival offenses, or disrupting the peace.
Participants in the “diverse interactions” class showed the highest rate of major depressive episodes. This class was characterized by the most interactions as a victim or person in crisis and by non-male respondents. An association has been previously reported between PTSD or violent victimization and subsequent depressive symptoms in women experiencing homelessness and mental illness specifically (Tinland et al., 2018). With regards to psychotic diagnoses, neither having a psychotic disorder nor the severity of symptoms in the past month were significantly different between groups. This is somewhat in line with Parpouchi et al.’s (2021) multilevel modelling of criminal convictions in the Vancouver At Home/Chez Soi cohort, which found no independent association between this harder CJI outcome and individual severe mental disorders.
Most calls related to victimization were initiated by participants themselves while calls for people in crises were evenly distributed across types of initiators. Crisis calls did in fact end in a hospital transfer and/or call to emergency response teams rather than escalating CJI. While only 21% and 24% of interactions as victims resulted in hospital and emergency response help, data did not allow to determine whether these interactions would have required further care. An important finding from the present study is the low rate of victimization reported (23.6%) as compared to other At Home/Chez soi cohorts. For example, 41% of police encounters were related to victimization in the Toronto cohort (Kouyoumdjian et al., 2019) and self-reported national data showed 51% of participants were victimized in the 6 months prior to the trial Roy, Crocker, Nicholls, Latimer, Gozdzik, et al., 2016a). The low prevalence in this study suggests victimization was underreported to authorities. This may be related to mistrust towards police because of previous encounters (especially where individuals have been handcuffed or report being assaulted by an officer) (Krameddine and Silverstone, 2016; Watson et al., 2008; Zakrison et al., 2004), as well as hidden victimization given the low number of interactions reported by bystanders. Of note, both groups characterized by victimization also included high rates of suspect interactions, replicating the well-documented correlation between victimization and CJI in this population (Roy, Crocker, Nicholls, Latimer & Isaak, 2016b; Roy et al., 2014).
Findings from this study hold important implications for reducing barriers to help seeking in people experiencing homelessness and mental illness. Previous research shows that procedural safety determines perceptions of both law enforcement and health and social services in this population, with labelling as vulnerable versus deviant being a key moderator (Roy et al., 2020). While crisis intervention teams and training involving police have aimed to reduce stigmatising attitudes in first responders and improve subsequent CJI and health outcomes, there is mixed-evidence as to their success (Marcus and Stergiopoulos, 2022; Rogers et al., 2019). In contrast, non-police crisis intervention teams show promising results for engaging users with services and reducing CJI (Marcus and Stergiopoulos, 2022). There is a need for further experimental evaluations of these teams (Marcus and Stergiopoulos, 2022), notably to ensure service planning is informed by users’ perspectives and past trauma experiences (Hopper et al., 2010; Spolum et al., 2023). Ultimately, alternative crisis response teams will only be effective in a wider health and social services system which provides timely and continuous access to integrated mental health care (Roesch and Goossens, 2022; Xanthopoulou et al., 2022).
The sensitivity of administrative data on policing compared to self-reports represents a strength of this study. This method enabled an investigation of the heterogeneity in police interactions over a significant period of time, as well as pointed to potential blind-spots in reporting victimization. Nevertheless, interpretation was limited by lack of consistency across reports as to why participants were ticketed or arrested. While previous At Home/Chez Soi analyses have shown good agreement between self-reported and administrative data with respect to court appearances (Lemieux et al., 2017), it is probable that some interactions between police and participants may not have been captured in police reports. Such interactions may include victimization (which was likely underreported in this study) or access to mental health or crisis services not coordinated by police. Second, in accordance with our objectives to model patterns of interactions cross-sectionally, causal mechanisms or confounders were not investigated. Third, we did not investigate the effect of the housing intervention, as it has been reported elsewhere to have no effect on CJI (Kouyoumdjian et al., 2019; Leclair et al., 2019; Luong et al., 2021) or arrests (Aubry et al., 2016; Stergiopoulos et al., 2015). Therefore, while the present study spanned from 2 years prior to 2 years after the trial, the housing intervention is not expected to have had a differential effect than control conditions on police reported outcomes in the present study. Fourth, because the trial selected for absolutely homeless or precariously housed persons from various community services, the sample in this study is less generalizable to persons experiencing hidden homelessness. Finally, there is a need to replicate findings over time, as the implementation of new civilian and police-driven interventions in this population may affect results. Future research should also consider the independent effects of prediction variables longitudinally, notably to model the effects of mental health treatment and social support interventions on CJI.
In conclusion, results from this study add to the evidence base on the frequent interaction of police and people experiencing homelessness and mental illness in Canada, especially as suspects. Results suggest this population may face unnecessary policing related to the behaviors associated with homelessness and underreported victimization. Addressing criminogenic risk factors as well as reducing barriers to help seeking should be prioritized in future evidenced-based policy development and service models for risk management (Leclair et al., 2019).
Footnotes
Acknowledgements
M.L and M.C.L acknowledge financial support from the Canadian Institutes of Health Research (CIHR) in the form of Vanier Canada Graduate Scholarships. L.R and T.N each acknowledge their CIHR Foundation Grants. We thank Stéfanie Brière with the Montreal Police Service for her expertise and contribution throughout the data extraction process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported through a Health Canada contribution to the Mental Health Commission of Canada and by a grant from the CIHR (MOP 136958). This research was undertaken in part, thanks to the funding form the Canada Research Chairs program to A.G.C.