
Abstract
Implementation of trauma-informed policing is developing at pace; however, evidence of impact is limited. This study examines the impact of trauma-informed practice (TIP) training (trainees, n = 358) across two police forces in England. 316 trainees completed a pre- and post-training survey measuring attitudes/knowledge relating to TIPs (229 matched for paired analyses). Compared to pre-training, post-training participants were significantly more likely to agree with statements relating to trauma-informed knowledge/attitudes (effect sizes: medium-large). The study suggests positive impacts of training. Further evaluation is required to determine wider impacts for police forces and partners, those encountering the criminal justice system, and the wider community.
Background
Over the past few decades, preventing and responding to the impacts of Adverse Childhood Experiences (ACEs) has become a key priority across countries, services, and communities (Bellis et al., 2023a). ACEs refer to experiences during childhood that can lead to stress or trauma, such as physical, sexual or emotional abuse and neglect, exposure to violence in the household or community, or other household or community stressors such as parental alcohol and other drug use, or incarceration or poor mental health of a household member (Bellis et al., 2023a). There is strong evidence to suggest that ACEs and associated trauma can have impacts on health and well-being and other outcomes across the life course. A meta-analysis of studies examining associations between ACEs and health and well-being in adulthood, shows that compared to those who experienced no ACEs, those who suffered four or more ACEs were significantly more likely to experience poor mental health, use illicit drugs or report problematic drug or alcohol use, be a victim or perpetrator of violence, and attempt suicide (Hughes et al., 2017). Evidence also suggests that ACEs can increase the risk of engagement with the criminal justice system (Bellis et al., 2016; Brodie et al., 2023; Ford et al., 2019; McCoy et al., 2023). For example, studies across England and Wales estimate that compared to those experiencing no ACEs, those with four or more ACEs are 11 to 20 times more likely to have been incarcerated at some point in their lifetime (Bellis et al., 2014, 2016). Further, studies of those engaged in the criminal or youth justice system suggest much higher levels of exposure to ACEs, compared to the general population. In Wales, a study of a male adult offender population found that 80% reported at least one ACE, and nearly half had four or more ACEs (Ford et al., 2019), figures much higher than the Welsh population (47% and 14% respectively; Bellis et al., 2016). Further, those with four or more ACEs were four times more likely to have ever served a sentence in a young offender institution than those with no ACEs (Ford et al., 2019). Another study of children and young people (aged 10-18) engaged in a youth justice service in England found that 91.5% had experienced at least one ACE, and 55.1% had experienced four or more ACEs (McCoy et al., 2023), compared to 47.9% and 9.0% of adults across England (Bellis et al., 2014). Recent evidence from England and Wales has also shown that there are increased risks of engagement with the criminal justice system in adulthood for those who had experienced only one ACE compared to those who experienced no ACEs (Bellis et al., 2023b).
Whilst evidence suggests that exposure to ACEs can increase risks of engagement with criminal justice (and other) services across the life course, evidence also suggests that a high proportion of police demand focuses on responding to and supporting those with complex needs. For example, a systematic review has estimated that one in 100 police dispatches and encounters involve people with mental disorders (Livingston, 2016), and in England and Wales, over 80% of all police calls are estimated to involve supporting those who are vulnerable and/or have complex social needs, typically for non-criminal incidents (College of Policing, 2015). Further, the small proportion of the population with complex needs can often place a disproportionately high demand on police and multi-agency services (Bellis et al., 2023a; College of Policing, 2015; Livingston, 2016). Engagement with the criminal justice system by this vulnerable group may be a consequence of health or social issues (e.g., substance use), which, if not addressed, may perpetuate a cycle of repeated contact with services, and further criminal justice and health and social issues (Bellis et al., 2023a; Ford et al., 2019; Hughes et al., 2017; Quigg et al., 2023). Globally, there is growing attention on the role of policing in strengthening their role in a whole system multi-agency approach to addressing complex issues that cross criminal justice and public health agendas, such as ACEs and trauma, violence, alcohol and other drug use, and mental health (Quigg et al., 2023).
Across various countries, police forces and partners at local and national levels are advocating for and developing and implementing ACE and/or trauma-informed approaches across police and other public services (Blue et al., 2020; Brodie et al., 2022; Hardcastle et al., 2021; Lathan et al., 2019; Olson et al., 2022; Quigg et al., 2023). Trauma-informed approaches to policing involve an overarching model of policing with vulnerable individuals, with guiding principles which promote understanding of the impacts of trauma on individuals’ wellbeing and behaviour. Trauma-informed policing emphasises the need, when working with individuals impacted by trauma, to prioritise safety, choice and empowerment, establishing trust, and to be considerate of underlying cultural factors and the role these may play when interacting with individuals (Bellis et al., 2023a; DeCandia and Guarino, 2015). Understanding these principles is critical for those working with traumatised individuals, with these principles acting as a guide to, wherever possible and safe to do so, move away from policing methods which are more likely to re-traumatise or trigger individuals. For example, evidence from people in the UK with lived experience of trauma and ACEs, who have had multiple encounters with police, has indicated that these encounters, especially if they use overly forceful or hands-on methods of policing, can exacerbate symptoms of trauma, therefore reducing their trust in police services (Borysik and Corry-Roake, 2021). Improved understanding of trauma-informed policing may help to move police staff and officers towards approaches (e.g. open and honest communication, and allowing time to understand the underlying causes of behaviour), which may support more positive outcomes with vulnerable individuals. As such, increasing understandings of ACEs and trauma-informed practice has the potential to support police officers and staff in identifying and responding to vulnerable people (whether victims, perpetrators or witnesses) more effectively, improving opportunities for early intervention, and preventing further criminal justice or other health and social issues (Bateson et al., 2020).
Over recent years, approaches to developing ACE and/or trauma informed police forces have started to emerge across the United Kingdom. Often, these include awareness raising training for police officers and staff on ACEs and/or trauma-informed practices. However, there is little evidence on the impact of such training (Youth Endowment Fund, 2023). A few recent studies evaluating ACE/trauma-informed training for police officers suggest that training sessions can increase trainees’ understanding of vulnerability and ACEs and improve their confidence to work utilising ACE or trauma-informed approaches (Glendinning et al., 2020; Hardcastle et al., 2021). This study aims to add to this limited but emerging evidence base by examining the impact of two ACE/trauma-informed practice training programmes delivered across two police forces in England (funded separately via two Violence Reduction Units). Specifically, the study aims to examine: • The associated impact of ACE/trauma-informed practice training on police officers and staff’s attitudes and knowledge in relation to trauma-informed practices. • If the impacts of the training programmes are mediated by how the training programme is implemented, and sociodemographic factors.
Methods
The ACE/trauma-informed practice training programmes
Police force areas
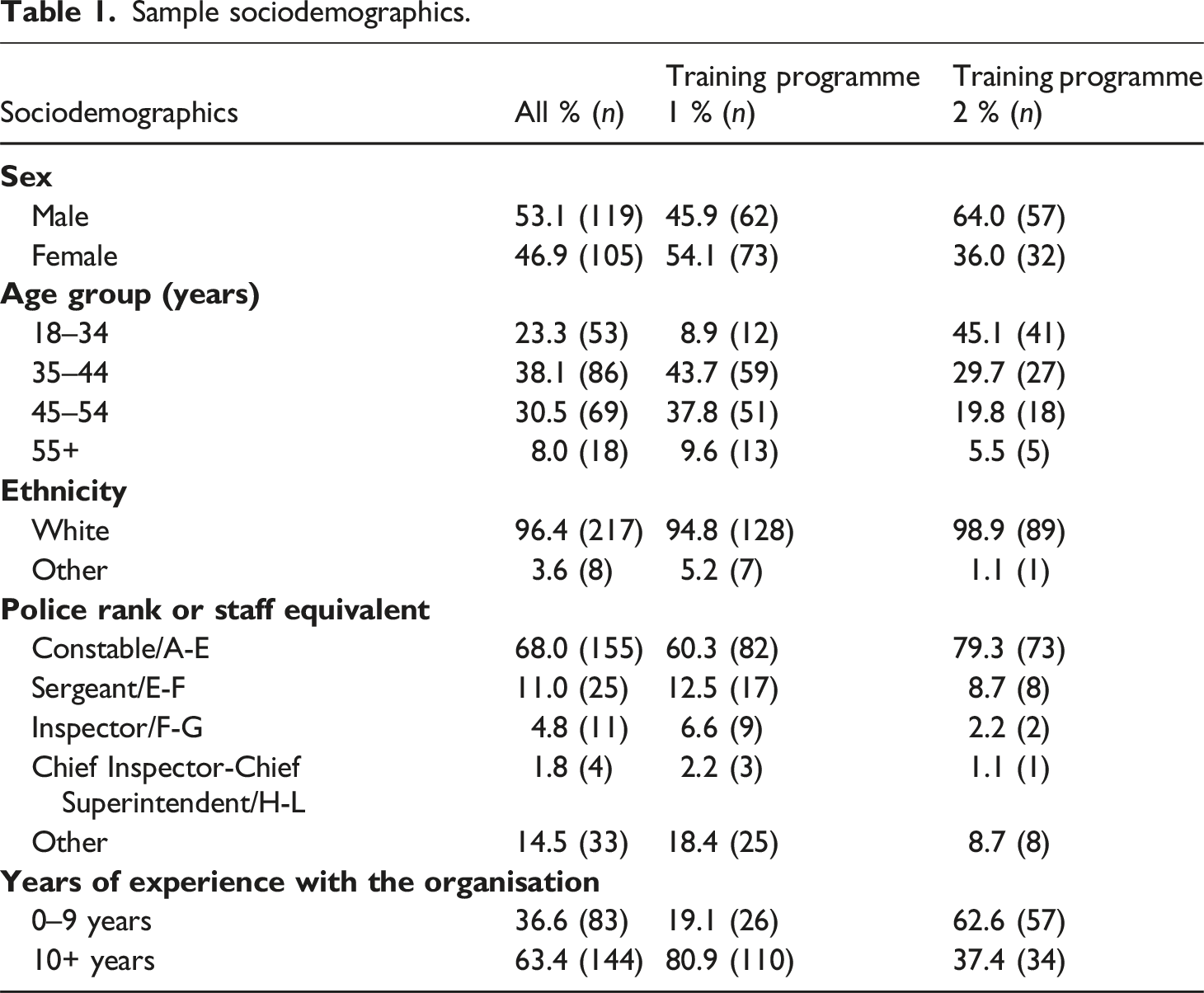
Training programme 1 was delivered in a police force (with around 4000 police officers) in a predominantly urban area in Northwest England. Training programme 2 was delivered in a police force (with around 3300 police officers) in a predominantly rural area in Southeast England.
Training programme 1
Partners from a Violence Reduction Unit in England commissioned a series of ACE/trauma-informed practice training sessions for police officers and staff to improve knowledge and understanding of ACEs and trauma-informed practices. Ten three-and-a-half-hour sessions were implemented, with training content delivered in-person by formal lecture (using PowerPoint slides) and video aides covering an overview of trauma and ACEs, the impacts of trauma on offending behaviours and health and well-being, how trauma may present, and some of the principles and benefits of trauma-informed policing. The training also included a reflective practice session where trainees could discuss in groups, some of the key aspects of trauma-informed policing, and how they can develop their practice to be more trauma-informed. Each session was delivered by a public health practitioner with expertise in ACEs/trauma-informed practices, with a senior police officer also providing a short introduction to the training purpose and the force’s priorities around prevention and trauma-informed practices.
Training programme 2
Partners from another Violence Reduction Unit in England commissioned the implementation of training sessions for police officers and staff to improve knowledge and understanding of ACEs and trauma-informed practices. Eleven three-hour sessions were implemented with training content delivered online by informal lecture (using PowerPoint slides) and video aides covering an overview of trauma and ACEs, the impacts of trauma on the brain and how this links to offending behaviours, how trauma may present, and the benefits and practical considerations for trauma-informed policing. The training session had regular opportunities for interaction between the trainee group and the trainer with concepts related back to ground level policing. Each session was delivered by a practitioner from an organisation with expertise in ACEs/trauma-informed practices. The organisation focusses on supporting multi-agency partners to develop, implement and enhance trauma-informed practices, and had been commissioned to support the police force to enhance their trauma-informed practices, including delivery of training and wider staff and organisational support.
Study design, participant recruitment and sample
A pre- and post-test study design was implemented across the two training sites. Prior to each training session, the trainer provided trainees with a verbal description of the study and access to a participant information sheet inviting them to take part in the study (information sheets were shared electronically for trainees completing surveys online). Trainees who consented to take part were invited to self-complete a pre- and post-training survey, either paper-based (training programme 1) or online (training programme 2). In total, 170 police officers/staff attended training programme 1, and of these 136 (80.0%) completed both a pre- and post-training survey. For training programme 2, 188 police officers/staff attended, and of these 180 (95.7%) took part in pre- and/or post-training surveys; here only 51.7% (n = 93) completed both the pre- and post-training survey. To assess pre-to-post-training changes at an individual, as well as a sample level, survey participants were asked to include their initials and day and month of birth. This allowed for individuals’ pre- and post-survey responses to be anonymously linked. Pre- and post-training surveys measured relevant sociodemographics, and participant’s attitudes, and knowledge relating to trauma-informed policing approaches. Ethical approval was obtained from Liverpool John Moores University.
Measures
Sociodemographics
Included age (18-24; 25-34; 35-44; 45-54; 55-64; 65+ years), sex (Female; Male), ethnicity (any White ethnic background; any other non-White ethnic background), police rank/staff level equivalent (Constable/A-E; Sergeant/E-F; Inspector/F-G; Chief Inspector/H-I; Chief Superintendent/L; Other), and time (years) spent working for the organisation.
Survey for Trauma-Informed Systems Change (STISC)
To assess changes from pre-to-post-training, two out of five subscales of the STISC (Moreland Capuia et al., 2022) were implemented in both pre- and post-training surveys for: trauma-informed knowledge and attitudes (23-items); and system-wide trauma-informed knowledge and attitudes (6-items). The STISC is a recently developed tool for the measurement of trauma-informed care and services and is designed to be implemented with practitioners across any field/industry (Moreland Capuia et al., 2022). The trauma-informed knowledge and attitudes subscale examines understanding of brain physiology and biology in relation to ACEs, the impacts that trauma and ACEs can have on individuals, and awareness of trauma-informed practices (see Supplemental tables 1-3). The system-wide trauma-informed knowledge and attitudes subscale examines trainees’ attitudes towards the importance of trauma-informed practices for their work/organisation (see Supplemental table 4). For each subscale, participants indicated on a five-point scale how much they agreed with each statement (1 – strongly disagree; 5 – strongly agree). Scores were totalled for each subscale, with higher scores indicating more trauma-informed knowledge, attitudes, and practices. The other three subscales of the STISC included: safety and acceptance at work (7-items); training, support, interaction, and environment (20-items); and awareness of cultural background at work (3-items). However, it was seen that items on these subscales would not reasonably be expected to be impacted by a training session alone, and required longer-term system change, as such these subscales were only implemented in pre-training surveys. In training programme 2 the wording of some items was adapted to use language which was more culturally and locally relevant (see footnotes in Supplemental tables).
Analyses
Only participants with matched pre- and post-training data were included in analyses (n = 229). Paired-sample t-tests were used to explore whether significant changes were observed across the items included in the two STISC subscales utilised and the overall score for each subscale, for trainees attending either of the training programmes. Effect sizes (d) were calculated as post-hoc tests for the measurement scores, and the magnitude of effects were determined using Cohen’s categorisation of effect sizes (small, 0.20; medium, 0.50; large, 0.80). ANCOVA models were used to examine any differences in post-training subscale scores by the training programme that was implemented, whilst controlling for pre-training subscale scores, sex, age, and years of experience working for the organisation.
Results
Trainee characteristics
Sample sociodemographics.
Individual level trauma-informed knowledge and attitudes
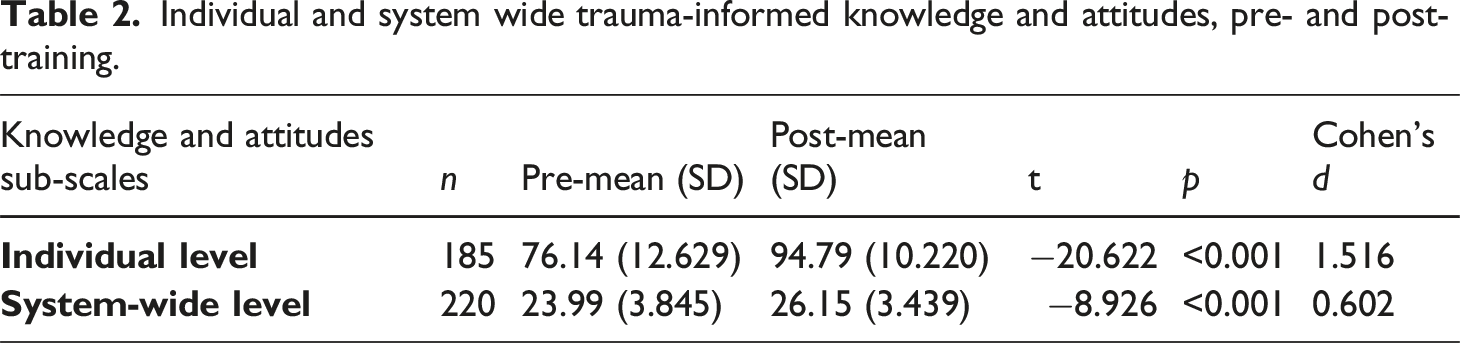
For pre-training, the mean combined score for individual-level trauma-informed knowledge and attitudes was 76.1. Compared to pre-training, post-training scores for trauma-informed knowledge and attitudes improved for all knowledge and attitude items (see Supplemental tables S1-3), with a significant increase in the combined mean score (post-mean = 94.79; p < .001; large effect size [d = 1.516]; Table 1), indicating improvements in individual level trauma-informed knowledge and attitudes.
System-wide trauma-informed knowledge and attitudes
Individual and system wide trauma-informed knowledge and attitudes, pre- and post-training.
Pre-to-post-training changes and trainee characteristics
In multivariate analyses, while controlling for pre-training scores on the individual-level trauma-informed knowledge and attitudes subscale, and sex, age, and years of experience with the organisation, there was no significant difference by training programme in mean post-training individual-level trauma-informed knowledge and attitudes subscale scores (training programme 1, mean = 95.28; training programme 2, mean = 94.64; F (1,175) = 1.365, p = .244).
In multivariate analyses, while controlling for pre-training scores on the system-wide trauma-informed knowledge and attitudes subscale, and sex, age, and years of experience with the organisation, there was a significant difference by training programme on post-training system-wide trauma-informed knowledge and attitudes subscale scores (training programme 1, mean = 27.15; training programme 2, mean = 24.85; F (1,210) = 9.302; p = .003).
Discussion
This study provides evidence to suggest that ACE/trauma-informed practice training sessions for police officers and staff can significantly improve trainees’ individual-level trauma-informed knowledge and attitudes with a large effect size, including improving trainees’ understanding of brain physiology and biology in relation to ACEs, the impacts that trauma and ACEs can have on individuals, and awareness of trauma-informed practices. ACEs/trauma-informed training sessions can also significantly improve trainees’ system-wide trauma-informed knowledge and attitudes with medium effect size, including trainees’ attitudes towards the importance of trauma-informed practices. Further, it suggests that there may be elements of the delivery of training sessions, or the system within which training is being implemented (e.g. police force/community area) which support improved outcomes in trainees’ system-wide trauma-informed knowledge and attitudes.
In the United Kingdom (UK), approaches to develop ACE or trauma-informed approaches across communities, organisations and systems is starting to emerge with pace (Bellis et al., 2023a; Quigg et al., 2023). Research has highlighted that police officers and staff acknowledge the importance of addressing vulnerability and trauma to protect those most at risk (Barton et al., 2019; Gillespie-Smith et al., 2020). However, evidence also suggests that they can lack the knowledge and skills to adequately identify and support vulnerable and traumatised individuals. ACE and trauma-informed training is therefore an important element of improving the knowledge, attitudes, and skills of police officers and staff who work with individuals affected by trauma. Drawing on two different, yet similar ACE/trauma-informed practice training for police implemented via two Violence Reduction Units, this study adds to the emerging evidence base suggesting that such training can have positive impacts on police officers and staff’s attitudes and knowledge (Youth Endowment Fund, 2023). This is an important initial step in improving the overall capacity of the police workforce to work in a more safe and productive manner with individuals affected by trauma.
Such changes in knowledge and attitudes may not only support police to implement trauma-informed practices more effectively, but also help improve ground-level buy-in to changing the wider policing (and multi-agency) system to work in more trauma-informed ways. However, while training sessions to enhance awareness of trauma and its impacts can lead to positive knowledge and attitude changes (as shown by this and other studies), moving towards trauma-informed practice operationally at the ground-level in policing may require longer-term and wider investment (Goodall, 2022). Improving ground-level trauma-informed practices, whilst positively influenced by training, will require workforce development and system-level changes to organisational practice. This includes addressing key barriers at individual-level and systemic cultural barriers that potentially limit individuals’ (and the systems) capacity to work in trauma-informed and/or preventative ways (Goodall, 2022; Quigg et al., 2023). Barriers can include a lack of strategic management of workforce support; workload pressures and staff turnover; competing priorities across organisations; and a culture of crime fighting in the police (Barton et al., 2019; Gillespie-Smith et al., 2020; Quigg et al., 2023). Further, police officers/staff may have experienced ACEs/trauma personally, and a lack of support for individuals’ own experiences of trauma, experiences of vicarious trauma, and high levels of burnout and stress, can be barriers and are often experienced by police who work with individuals affected by trauma (Barton et al., 2019; Cartwright and Roach, 2022; Foley and Massey, 2021; Ludwig and Reid, 2021). Supporting staff’s own health and wellbeing has been identified as one key element of moving towards a more trauma-informed workforce and requires longer-term commitment in terms of improving wellbeing resources for police officers and staff, and of improving leadership buy-in to make police officer and staff wellbeing a force priority (BristolSomerset, 2021). Such system wide approaches are developing across some police forces in England and Wales (e.g. Hampshire and Isle of Wight [Hampshire Police and Crime Commissioner, 2021]; South Wales [Glendinning et al., 2020]); However, further evaluations are required to determine the impacts of trauma-informed approaches across police forces, on officers and staff, those engaged in the criminal justice system, the wider community, and on the overall success of multi-agency approaches to protect people from harm.
Through examining two training programmes with similar objectives but delivered using different methods across two varying police forces (one urban/one rural), this study adds context around the impact of varying training programme implementation approaches. Critically, it suggests that both online and in-person approaches can be effective in positively impacting on police officer and staff’s knowledge and attitudes at the individual level. Whilst all outcomes from this study where significant in a positive direction, the study did however find differences in the level of impact for system-wide trauma-informed knowledge and attitudes between training programme types, which requires further investigation. Such differences may be due to differences in the delivery of training sessions or the system within which training was implemented (e.g. police force/community area). For example, training that is delivered in-person, and is adapted to be culturally and locally relevant, with time allocated for trainees to interact and reflect on their own practices may support more positive outcomes. There may also be other underlying factors that influence how beneficial training sessions may be, such as leadership buy-in and promotion of trauma-informed working, overall levels of staffing, levels of staff wellbeing and burnout, trainees personal experience of ACEs/trauma, and recency of previous trauma-informed training sessions. These training-level and force-level factors should come into consideration when deciding how best to implement trauma-informed training sessions.
The current research is the first to utilise the Survey for Trauma-Informed Systems Change tool (STISC; Moreland-Capuia et al., 2022) in evaluating the impacts of ACEs/trauma-informed training on police officers and staff trauma-informed knowledge and attitudes. This study suggests that the STISC tool provides a feasible and acceptable way to assess police officer and staff trauma-informed knowledge and attitudes using a matched-pair pre and post-survey study design. However, there are certain items in the tool that may need to be adapted based on cultural and local language to ensure that participants have a consistent understanding of the meaning of individual items. For example, the item ‘I understand trauma stewardship’ had relatively low levels of agreement at pre and post-survey implementation in training session 1. This may be due to the language of ‘trauma stewardship’ not being commonly utilised in UK police forces. As such adapting this item to include the definition of trauma stewardship (‘I understand trauma stewardship (i.e. acknowledging and understanding others’ trauma and suffering without taking it on as our own)’ may have been beneficial in using this tool in the UK. In training session 2, a higher proportion agreed with this statement at pre and post-survey implementation, potentially indicating that trainees had a better understanding of what is meant by this item. Further, the current study did not utilise all subscales within the STISC tool as it was seen that other subscales related to organisational practices and cultural factors would not have been impacted by the training in the short-term. Future work evaluating longer-term organisational and system-level trauma-informed changes to police forces may wish to utilise the full STISC tool.
The findings within this study should be considered recognising its limitations. While this study utilises matched-pair analyses of pre- and post-training surveys, a more robust study design than using unmatched analyses; participants were only drawn from two UK police forces and the sample size is relatively low, meaning that the sample is unlikely to be representative across police forces. Nonetheless, this study adds to a limited evidence base on the impact of ACEs/trauma-informed practice training on police officer and staff trauma-informed knowledge and attitudes (Youth Endowment Fund, 2023). Additionally, the findings within this study show significant positive changes with medium-large effect sizes, meaning that even with organisational differences between UK (and international) police forces in trauma-informed knowledge and attitudes, ACEs/trauma-informed training will still likely have positive impacts on police officer and staff trauma-informed knowledge and attitudes. In multivariate analyses, there may have been differences in underlying force-level factors which impact upon how effective training sessions may be (e.g., leadership buy-in to trauma-informed working; type of area – rural/urban). However, such factors were not measured by surveys and as such were not factored into analyses. Future research may wish to analyse force-level factors and the impacts this has both on trauma-informed working and on the impacts of trauma-informed training sessions.
Supplemental Material
Supplemental Material - The impact of adverse childhood experience and trauma-informed practice training for police in two regions in the United Kingdom
Supplemental Material for The impact of adverse childhood experience and trauma-informed practice training for police in two regions in the United Kingdom by Zara Quigg, Charley Wilson, Ellie McCoy and Nadia Butler in The Police Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.