
Abstract
Policing is considered a highly stressful role, and police officers are at risk of mental health issues during their service. This is an area which has gained increasing attention in recent years, but further research, using validated measures, is needed to help identify other factors that are important and ensure further development as well as evidence-based, bespoke intervention. The current study sought to explore the general prevalence of stress, depression and anxiety in a UK sample of police officers, to examine whether length of service moderates the effects of stress, depression and anxiety, and whether certain personality traits protect against these. A self-report questionnaire was completed by 177 serving UK police officers from 10 different regions. Results revealed clinical levels of anxiety and depression, and comorbid presentations of major depression and anxiety, at rates significantly higher than reported in the general population. Results indicated officers are most at risk of experiencing stress during the first 15 years of their service, and that officers’ stress was organisational rather than trauma related. Additionally, officers higher in traits of extraversion and lower in neuroticism reported lower anxiety. The results of these findings are discussed, and suggestions have been made based on the current findings.
Introduction
The Police Federation Leavers Survey 2017–2018 reported low morale (52.5%), the impact the job had on their psychological health (43.3%) and stress of the job (40%), as major influences on their decision to leave policing. The highest proportion of leavers (64.5%) also reported they would never consider returning. Respondents were asked what would make them reconsider their decision to leave. The third highest response (26.5%) was improved welfare provisions (Wellington, 2018). Thus, after retirement due to age or length of service, the major reasons for leaving the police service were related to wellbeing and mental health of the officers.
There is a wealth of research which indicates that police employees are at substantial risk to their mental and physical health (Clements et al., 2021), specifically stress-related illnesses such as heart disease (Ramey et al., 2009), PTSD (Robinson et al., 1997), anxiety and depression (Gershon et al., 2008), and suicide (Violanti and Aron, 1994). Serving Officers are exposed to many different types of stress: organisational, operational, external and personal (Dempsey and Forst, 2013). The most impactive of these are operational stressors, for example, witnessing life changing events (Violanti and Aron, 1994). Abdollahi (2002) suggested the role an officer carries out plays a significant part in the levels of stress perceived by an individual. For example, those with exposure to violent or traumatic events, such as officers on patrol, would report higher levels of perceived stress than colleagues who work in the training department. Whereas Habersaat et al. (2015) explored the relationship between risk and welfare in serving police officers, hypothesising that subjection to distressing events such as severe violence would link to risk and differ across departments. However, they found no difference between departments and suggested this could be due to personality attributes, or other protective factors. There is some suggestion that personality traits may guard against the effects of stress. For example, research indicates police employees possess higher levels of conscientiousness and lower levels of neuroticism (Detrick and Chibnall, 2013), and these traits can correlate with decreased stress levels (Garbarino et al., 2014) and increased tolerance to working shifts (Natvik et al., 2011).
Several studies suggest length of service may play a role in response to stress, although results are inconsistent. A recent study by Burnett et al. (2019) investigating the effects of compassion fatigue and stress in a large single UK police force, who reported length of service as a significant predictor of stress. In contrast, Evans et al. (1992) reported officers with 12 years’ service or more described less anxiety than colleagues with fewer years of service, suggesting officers with more years of service may have developed coping strategies which assist them when faced with stressful situations.
A further variable to consider is gender differences, with female officers reporting higher perceived stress than males (Thompson et al., 2005; Schaufeli and Enzmann, 1998; Berg et al., 2005; Acquadro et al., 2015). Factors such as gender discrimination from fellow officers and superiors, or perception of a lack of adequate support, could also raise the levels of stress in female officers (Morash and Haarr, 1995; Haarr, 1997; Wexler and Logan, 1983; Shelley et al., 2011). In contrast, Burnett et al. (2019) reported male officers experienced greater levels of burnout and stress than their female colleagues, suggesting male officers are more susceptible to mental health issues. Similarly, Habersaat et al. (2015) reported female officers presented with more emotion orientated coping, there was a significant effect of sex on depression symptoms and absence data demonstrated that female police officers (54.79%) were more likely to take leave for psychological and mental ill health reasons, compared to males (45.29%). The impact of the role may also vary according to gender. For example, Kurtz (2008) reported stress was significantly associated to making violent arrests for female officers but not male officers, while association to a victim or offender was a significant stressor for men but not for female officers. Furthermore, Bartal et al. (1992) reported female officers experienced significantly more stress than their male colleagues when faced with incidents relating to tragedy or danger.
There is also a great risk of experiencing trauma within policing and this can often be experienced as a part of routine duties (Violanti et al., 2017) as well as through exposure to extreme unpredictable events (Regehr et al., 2019). The negative psychological effects of trauma exposure have been heavily researched, with a recent study employing validated measures of PTSD with over 16,000 UK police employees from different ranks and roles (University of Cambridge & Police Care UK, 2019). The findings indicated that 20% of officers, who had experienced trauma, could be diagnosed with PTSD. Research such as this is extremely beneficial in expanding knowledge, but it has been argued that focussing on more acute negative psychological health and wellbeing effects of working within the field of policing is important as without this the full extent of the potential impacts is not known (Cartwright and Roach, 2020). Indeed, these authors determined from absence data that, of the complaints related to mental health issues, 56% were due to stress, 37% anxiety and depression and 7% other issues. Therefore, suggesting that common mental health issues such as anxiety and depression are prevalent within police personnel. A limitation of this research however was that it only used absence data and the authors highlighted the need for the use of standardised tools to measure mental ill health and stress of police employees.
The police service has also undergone huge reductions in funding. In the UK, approximately 17,000 uniform and CID officers have been lost (Burnham, 2015). In contrast, the National Office for Office for National Statistics (2018) shows a rise in crime. In 2015, the Police Federation of England and Wales (PFEW) conducted a focus group which provided evidence that suggested these staff reductions may be negatively impacting officers’ individual wellbeing (Elliott-Davies et al., 2016). From this, the PFEW carried out a demand, capacity and welfare survey in 2016, on each individual force across the country to assess the impact of job demands and capacity to meet these, as well as welfare (Elliott-Davies and Houdmont, 2016). A wide range of organisational stressors were included, with 66% of officers stating their workload was too high (compared to 46% of UK Armed Forces personnel); 67% stating they were unable to meet all the conflicting demands placed on them; 85% stating there weren’t enough officers in their team/unit to manage demand; and 53% stating they were never or rarely able to take their full break. 80% of respondents acknowledged that within the previous 12 months they had experienced feelings of stress, low mood, anxiety or other mental health and wellbeing difficulties, with 92% indicating work had caused their psychological difficulties or made them worse. A second survey was carried out in 2018, with over 18,000 completions, 43.9% of respondents indicated they found their job very or extremely stressful (up from 38.6% in 2016) with the authors highlighting this is almost three times higher than the Health and Safety Executive found in the general population in 2010 (15%) (Elliott-Davies, 2019). This survey is now biennial with the intention being to inspire positive change within the whole police service, by gathering evidence that can influence this. The 2020 findings continue to indicate concerns regarding psychological health and wellbeing, with 33% of respondents (from 12, 471 viable responses) reporting they find their job very or extremely stressful (Elliott-Davies, 2021). Additionally, academics recently reviewed UK Police Employee absences using Freedom of Information Act data, from 57% of UK police personnel (Cartwright and Roach, 2020). The findings indicated that absence rates due to psychological ill health, trauma and stress had almost doubled over the past 10 years from 4.72% in 2008 to 8.82% in 2018. Whilst these figures are concerning, it has been suggested that higher stress-related absences may be suggesting that attitudes are changing, indicating individuals have more accepting attitudes towards mental health and wellbeing in policing and may feel more comfortable coming forward for help and support (Cartwright and Roach, 2020).
These research studies are enormously beneficial in providing officers the opportunity to express their views and provide data to determine the challenges they face, around several areas including health and wellbeing. The trend over the three PFEW surveys and almost doubling of absence rates due to psychological ill health, trauma and stress highlighted by Cartwright and Roach (2020) is indicative of work-related stress, anxiety and depression for many, but this cannot be concluded due to non-clinical questions being used. Occupational stress has frequently been researched and given the high figures reported, is important to continually assess. Additionally, however, anxiety and depression are the most common mental health problems experienced and can be caused or aggravated by work-related issues (HSE, 2022) and are therefore also important to specifically assess, using validated measures. According to NICE (2022), generalised anxiety disorder (GAD) is characterised as reporting chronic, excessive worry which is not related to specific circumstances and symptoms of physiological arousal such as insomnia, muscle tension and restlessness and depression is characterised by persistent low mood and/or loss of pleasure in the majority of activities and several associated cognitive, physical, emotional and behavioural symptoms. A recent study of over 40,000 UK police officers and staff found 9.8% reported probable depression, 8.5% reported probable anxiety and 3.9% probable PTSD (Stevelink et al., 2020). These findings highlighted the importance of continued health monitoring, particularly for those who are heavy drinkers, recently exposed to traumatic incidents and police staff.
In recent years, attention has been paid and progress made in providing bespoke support for emergency workers and specifically police personnel, demonstrating positive organisational change in this area. In 2015, the mental health charity MIND carried out a survey of emergency services personnel in England with the aim of better understanding their experiences of mental health problems. Of the responses, 1194 were from the police service, with 91% reporting that whilst working for the police service, they have experienced stress, low mood or poor mental health and 61% reported they had personal experience of mental health problems, which was the highest of all the emergency services surveyed. Additionally, 37.78% said that work was the main cause of their poor mental health, and this was much higher than the general population, where only 15% attributed this to work (MIND, 2015). Following this survey, MIND set up a Blue Light programme, with the aim of tackling stigma and providing support for emergency services personnel, which continues to grow today. Additionally, the National Police Wellbeing Service (NPWS) was introduced in 2019 by the College of Policing and they in conjunction with Public Health England have launched the Oscar Kilo initiative, which is an evidence-based, police sector specific service, that provides resources and information regarding wellbeing and hosts the Blue Light Wellbeing Framework. These initiatives represent positive developments in police personnel mental health and wellbeing, yet more research is needed to ensure further development, evidence-based intervention design is possible and to determine what additional factors are important. Literature to date is inconsistent in terms of the role of gender, length of service, personality, and operational stressors on stress and mental health in police officers, but consistent in reporting of high levels of stress, anxiety, depression and related mental health presentations across police officers as a whole. Identifying individual factors, utilising validated measures of common mental health disorders is important to ensure further progress. The present study aims to explore rates of stress, anxiety and depression in UK police nationally, employing validated measures and examining other possible relevant factors including length of service, gender, personality and job role (e.g. frontline police versus office-based).
The current study has the following hypotheses:
As length of service increases, prevalence of mental health problems will decrease (i.e. lower stress, anxiety and depression).
There will be sex differences in the level of reported stress, anxiety and depression.
Uniformed officers will report higher levels of stress, anxiety or depression than those in other roles.
Stress, anxiety and depression will predict satisfaction with life.
Conscientiousness, extraversion and neuroticism will predict levels of stress.
Length of service will moderate the relationships between predictor variables and outcomes on mental health measures.
Method
Participants
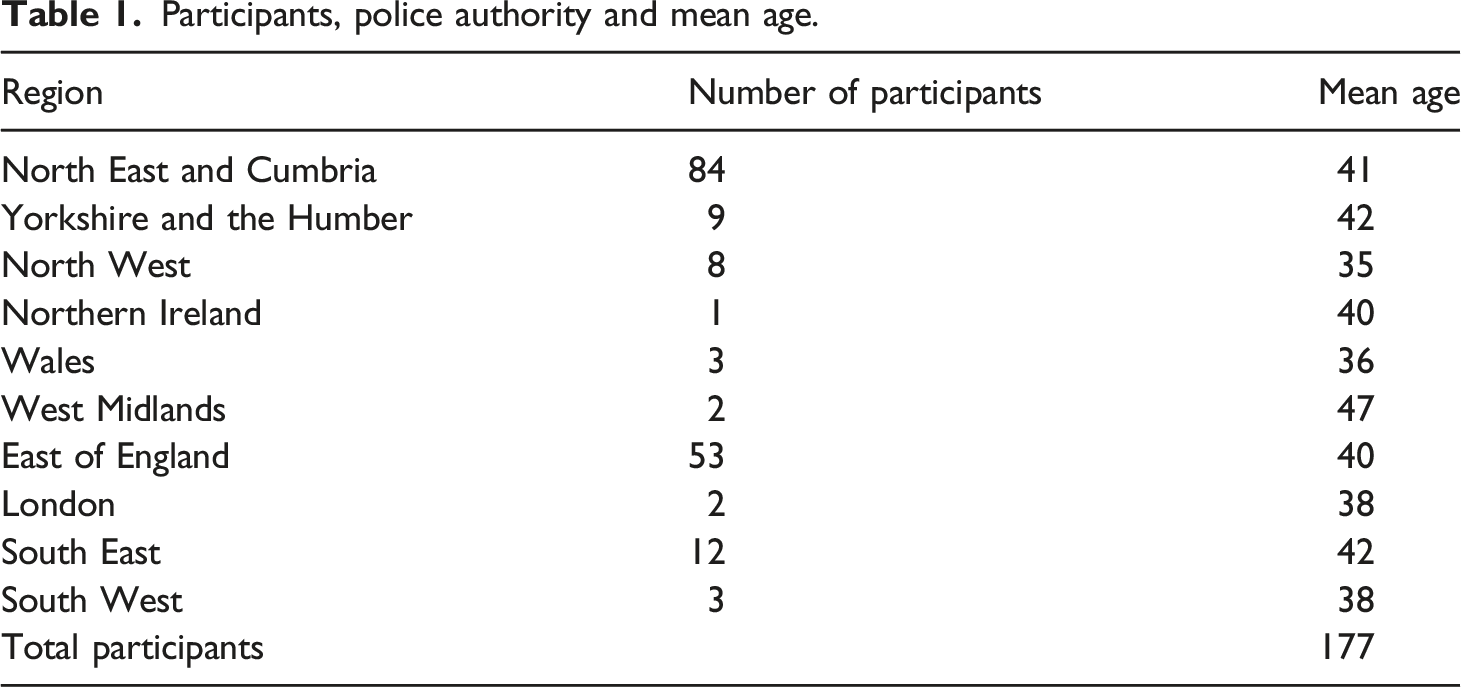
Participants, police authority and mean age.
Materials
Participants were asked to complete an online questionnaire. This consisted of demographic information, (age, gender, department and shift work) and five validated scales.
(1) Operational Police Stress Questionnaire (OPSQ) (MacCreary and Thompson, 2006). This is a twenty-item, validated measure, which identifies the most common stressors for police officers. Cronbach’s alpha revealed the questionnaire to have excellent reliability ⍺ = 0.94.
(2) Generalised Anxiety Disorder questionnaire (GAD-7) (Spitzer et al., 2006). This is a seven-item, self-report questionnaire, devised to briefly screen for generalised anxiety disorder. Cronbach’s alpha revealed the questionnaire to have excellent reliability ⍺ = 0.91.
(3) Patient Health Questionnaire-9 (PHQ-9) (Kroenke et al., 2001), is a nine-item questionnaire, with the items constructed directly from the diagnostic criteria for major depressive disorder contained within the DSM-IV. Cronbach’s alpha showed the PHQ-9 to have good reliability ⍺ =0 .89. Both the GAD-7 and PHQ-9 have been validated in primary care and the general population (Lowe et al., 2008).
The scoring used for both the PHQ-9 and GAD-7 are in line with NHS Primary Trusts, such as that of Devon Partnership: https://www.dpt.nhs.uk/search?q=phq+-+7+gad
(4) Satisfaction With Life Scale (SWLS) (Diener et al., 1985). This five-item questionnaire assesses a participant’s life satisfaction component of subjective wellbeing. Cronbach’s alpha revealed the questionnaire had a good level of reliability ⍺ = 0.87, and good internal consistency (Cronbach’s alpha ranging from 0.79 to 89).
(5) Big Five Inventory-10 (BFI-10) (Rammstedt and John, 2007). This instrument is a 10-item scale used to measure extraversion, agreeableness, emotional stability, conscientiousness and openness personality traits. Reliability analyses were not performed due to the limited number of items for each trait.
Procedure
Ethical approval was granted by the Psychology Department’s ethics committee at Northumbria University, prior to data collection. Participants were presented with information about the study. It was explained that confidentiality would be assured, and participation was voluntary. Participants were also given instructions regarding how to withdraw their information should they wish to do so later and asked to provide informed consent to participate. Participants then completed the questionnaire online using Qualtrics and it was available for 7 weeks.
Treatment of data
The data was analysed using SPSS, with several statistical approaches employed to appropriately explore each hypothesis. Descriptive statistics were firstly utilised to compare anxiety, depression and comorbidity scores to general population norm groups and published clinical criteria. An independent t-test was also utilised to explore differences between the sample and general population in anxiety and descriptive statistics reviewed for most prominent stressors. For each of the hypotheses, the following inferential techniques were employed: hypotheses 1,4 and 6, correlations; hypothesis 2, independent t-tests; hypothesis 3, one-way ANOVAs; hypothesis 5, multiple regression and moderation analyses for hypothesis 6.
Results
In order to explore rates of stress, anxiety and depression within the sample, the study focused on the results from the PHQ-9 and GAD-7, as these are the two measures that specifically assess presentation of clinical levels of depression and anxiety disorder. These will be addressed in turn.
Depression and anxiety
In order to directly compare findings to the general population, the depression results were compared with Martin et al.'s. (2006) representative general population results from 2066 subjects aged 14–93 years. They defined clinical levels of ‘Major Depression’ and ‘Other Depressive Disorder’ in their population, with rates of 3.8% Major Depression, and 5.4% Other Depressive Disorder. Using the same methodology, the present study identified 24.3% of the sample as meeting criteria for Major Depression, six times higher than the general population, with 6.0% of the present sample as meeting criteria for Other Depressive Disorder, in line with the general population. It was not possible to compare the sample means for significance of difference, because the Martin et al. paper does not provide the means or standard deviation for the total PHQ-9 scores.
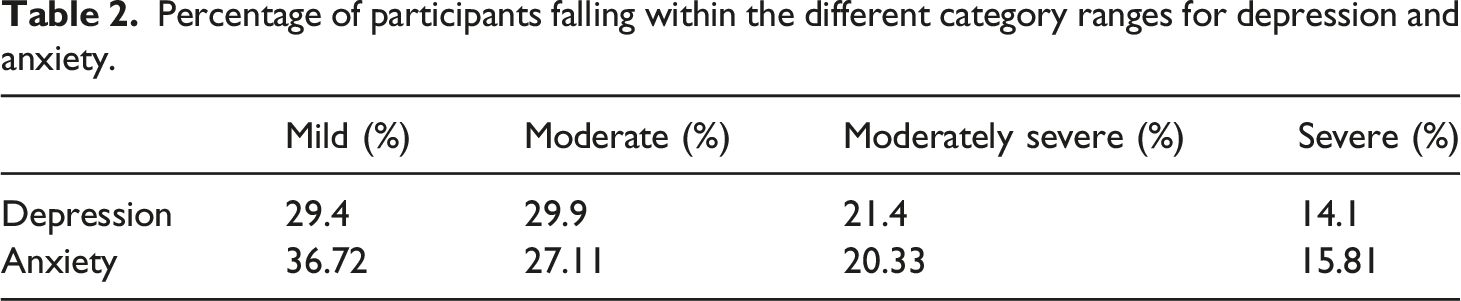
The anxiety results were compared with Lowe et al. (2008) who provided normative general population data from 5033 participants aged 14–92. Analysis was aligned with Lowe et al. to identify participants as ‘yellow flag’ and ‘red flag’ for clinical levels of anxiety disorder. General population rates from Lowe et al. identified 9.68% of their sample as ‘yellow flag’ and 13.85% of their sample as ‘red flag’. The present study identified 24.3% of the present police sample as ‘yellow flag’ for anxiety disorder, and 19.21% as ‘red flag’ for anxiety disorder. A t-test on the means was conducted to explore difference in GAD-7 total scores between the present sample and the general population sample reported in Lowe et al. Assuming non-paired samples, and unequal variance, t = −13.43, p < .001, indicating significantly higher overall anxiety levels in the present sample.
Percentage of participants falling within the different category ranges for depression and anxiety.
Depression and anxiety comorbidity
To further explore the impact of depression and anxiety within the present UK police sample, results from the PHQ-9 and GAD-7 were cross-referenced to identify the number of respondents who met criteria for both Major Depression or Other Depression plus Yellow Flag or Red Flag Anxiety disorder. There was no overlap between Other Depression and Yellow or Red Flag anxiety, with 0 respondents who met criteria for Other Depression also meeting criteria for anxiety as defined.
In contrast, there was substantial overlap between Major Depression and both levels of anxiety. 34.89% of the Yellow Flag sample also met criteria for Major Depression (8.47% of the total sample). 82.36% of the Red Flag sample also met criteria for Major Depression (15.82% of the total sample). See Figure 1. Proportion of comorbid major depression with yellow flag and red flag anxiety.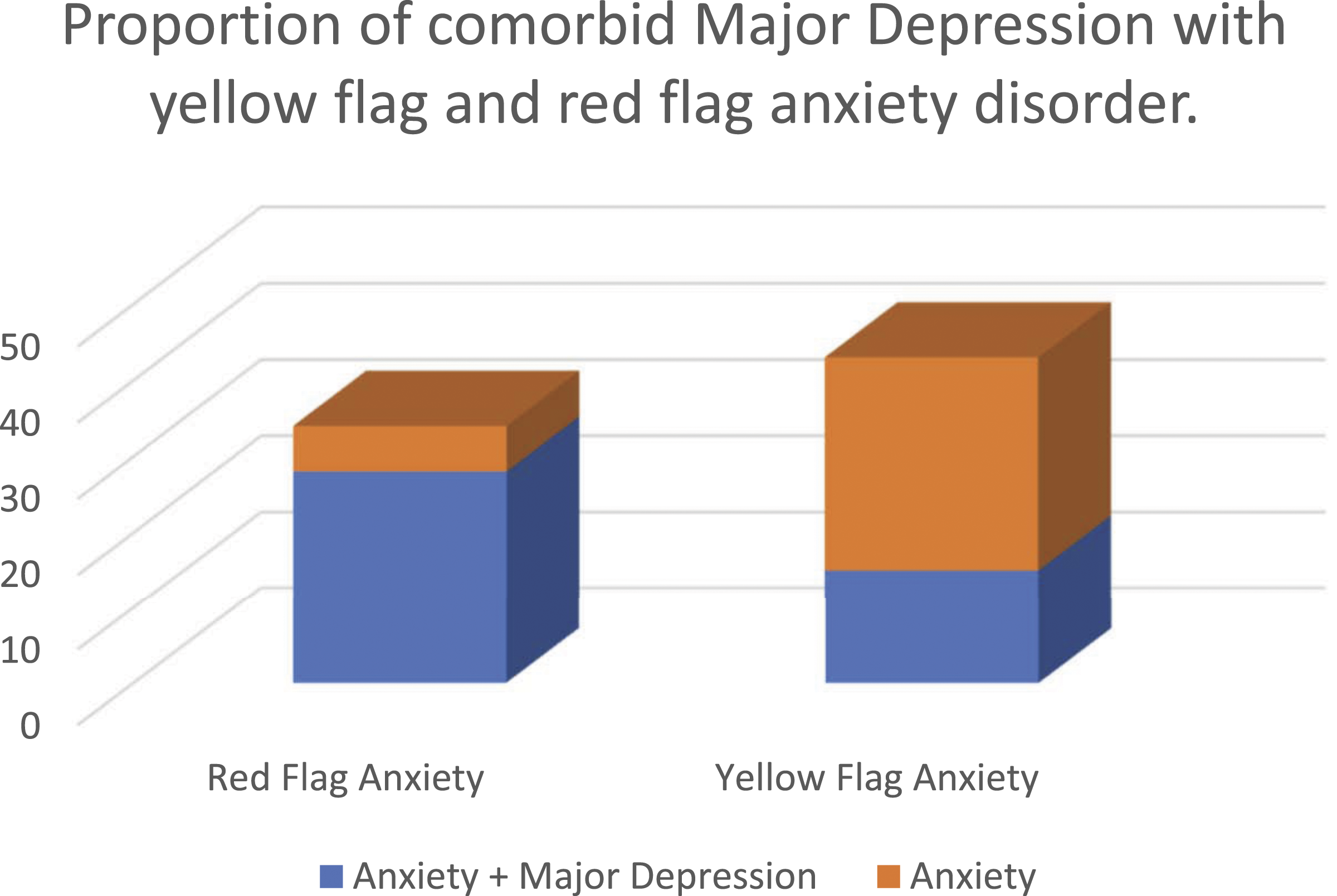
Stress
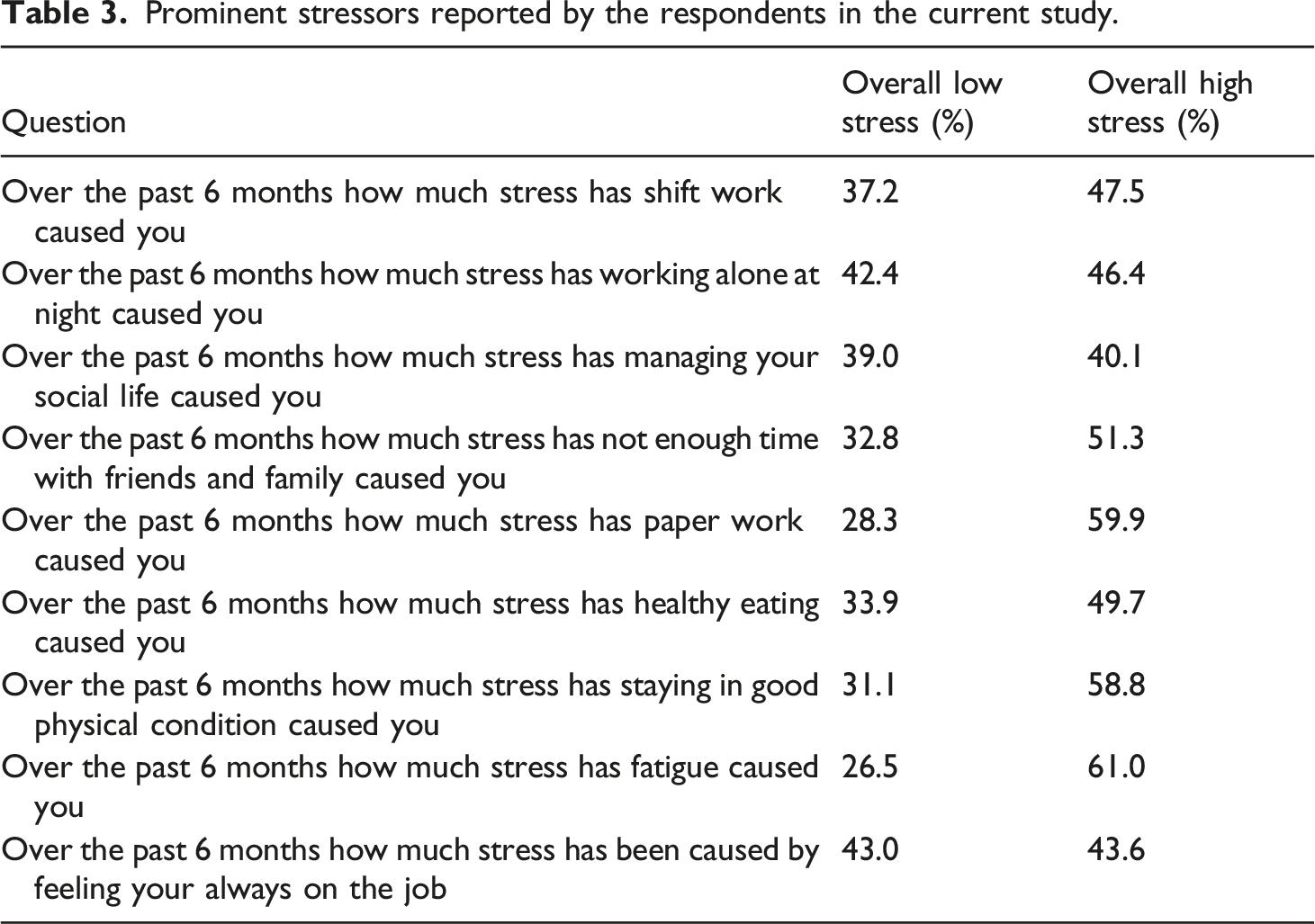
Prominent stressors reported by the respondents in the current study.
Correlations between length of service, PHQ-9, GAD-7 and OPSQ.
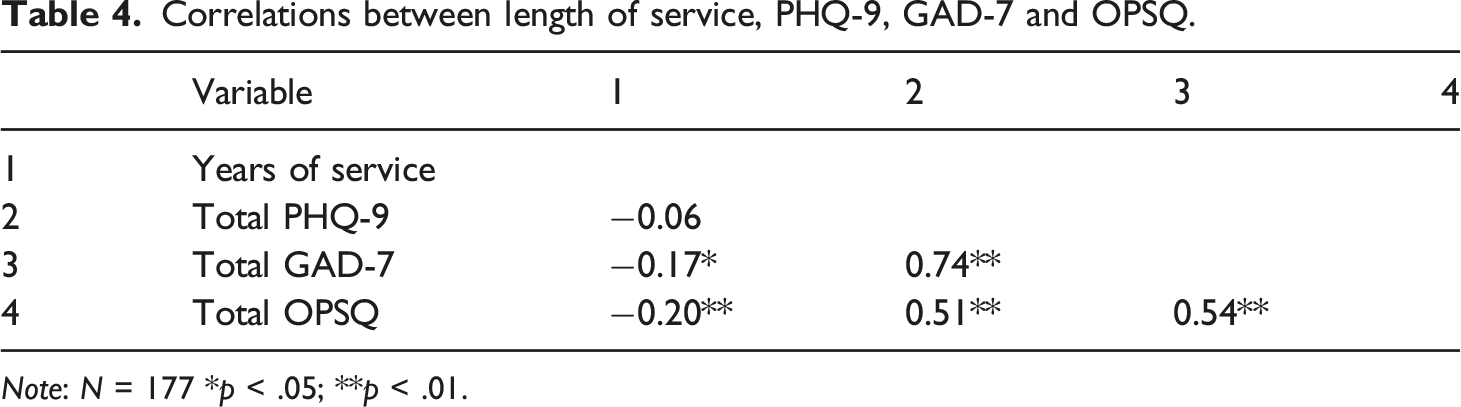
Note: N = 177 *p < .05; **p < .01.
To explore H2, participant data was analysed using independent t-tests to compare stress, anxiety and depression scores in males and females. There were no significant differences on any measure: OPSQ - Males (M = 75.14, SD = 27.70), Females (M = 73.99, SD = 28.73); (t = .268 df = 175, p = .79); PHQ-9 - Males (M = 9.43, SD = 5.90), Females (M = 9.60, SD = 6.30); (t = −0.165, df = 175, p = .87); GAD-7 - Males (M 8.83, SD = 5.80), Females (M = 9.0, SD = 6.04); (t = −0.178, df = 175, p = .86).
H3 was examined using one-way ANOVA. There was a significant difference between uniformed officers and plain-clothed officers on the OPSQ: F (1175) = 4.90, p = .03. There was no significant difference between uniformed and plain-clothed officers on the GAD-7 (p = .21) nor PHQ-9 (p = .50).
Correlations between SWL, PHQ-9, GAD-7 and OPSQ.
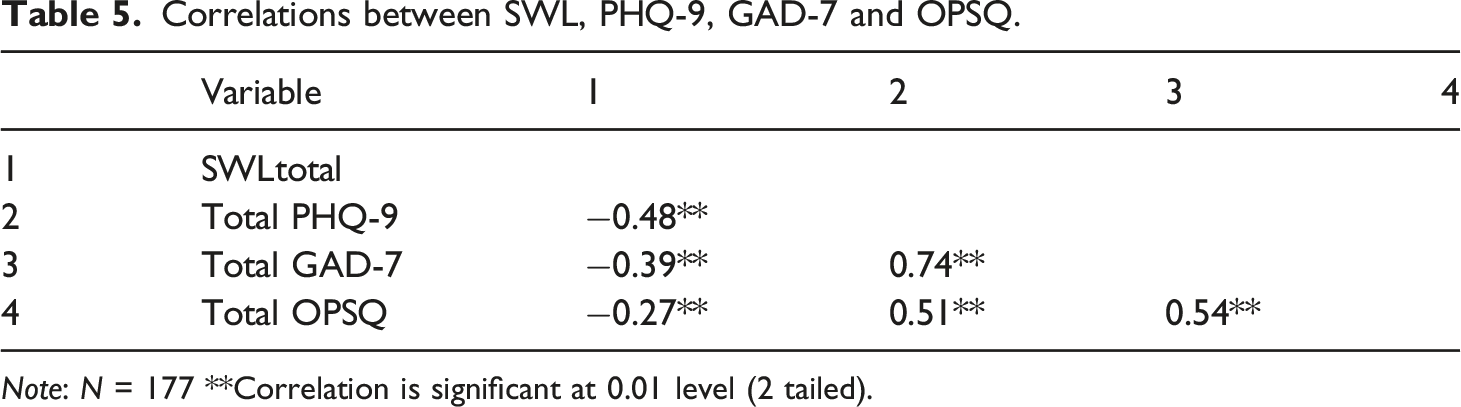
Note: N = 177 **Correlation is significant at 0.01 level (2 tailed).
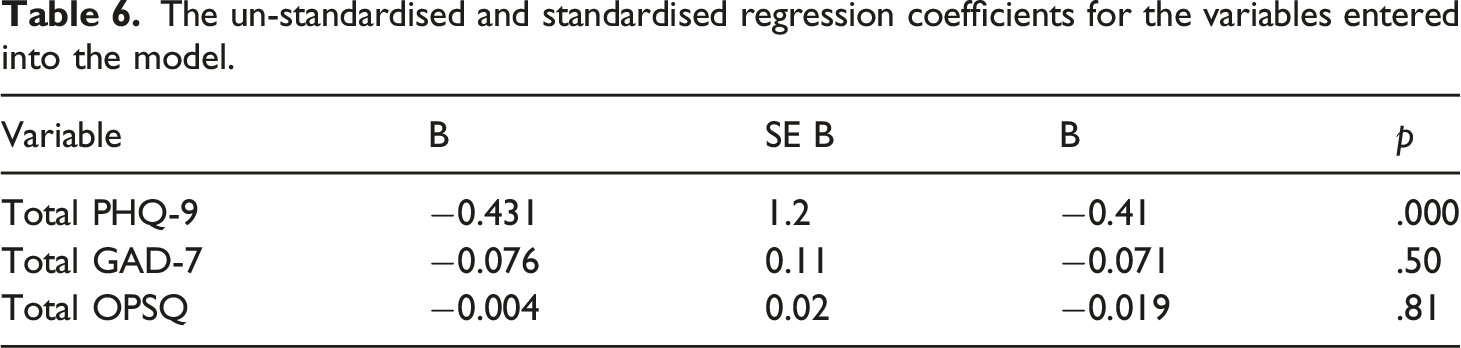
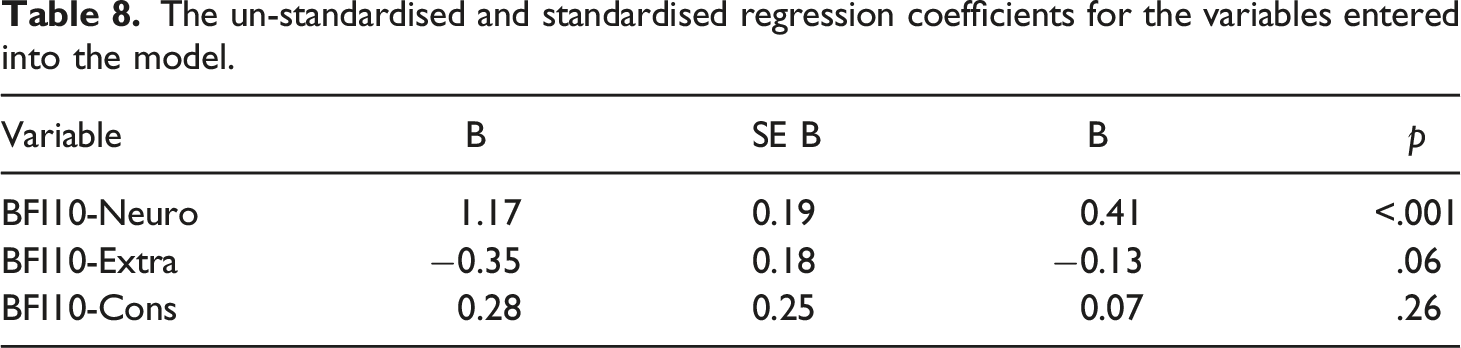
The un-standardised and standardised regression coefficients for the variables entered into the model.
Correlations between conscientiousness, extraversion and neuroticism and GAD-7 scores.
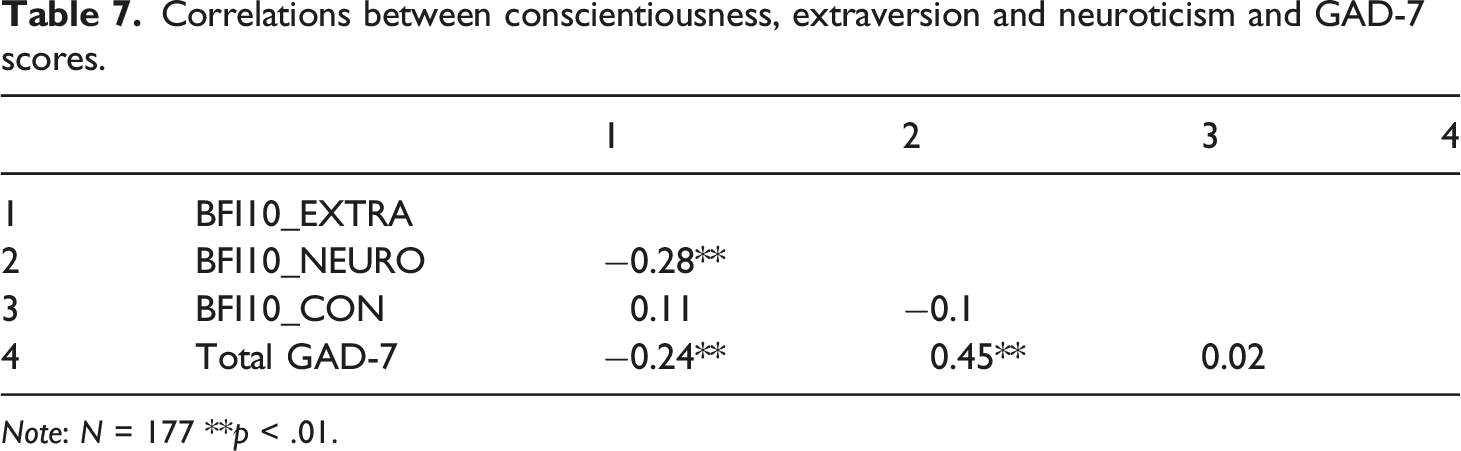
Note: N = 177 **p < .01.
The un-standardised and standardised regression coefficients for the variables entered into the model.
To explore H6, the first moderation examined SWL, GAD-7 and length of service. The data was checked for missing data and accuracy, no missing data was identified, and the data was verified as accurate by obtaining descriptive frequencies. Linear regression analysis was carried out to check the data for outliers and to check there were no homogeneity or homoscedastic problems. The outcome variable was the GAD-7 and predictor variables were total scores on SWL scale, and length of service. Assumptions were verified by examining the histogram, linearity and scatter plot which revealed normality of the data. The values for Mahalanobis, Cook’s and Leaverage were all computed which resulted in three outliers being identified and removed from the model. Multicollinearity was checked by running correlational analysis on the predictor variables total scores from years of service and the SWL Scale, this revealed the predictor variables were not correlated (r = 0.033, N = 174, p = .66).
Moderation analysis was carried out using (Hayes, 2012) plug in for SPSS Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modelling. The results revealed the overall model: F (3170) = 16.45, p < 0.001, R2 = 0.23 was significant and accounted for 23% of the variance. SWL was a significant negative predictor: b = −0.41, t (170) = −5.83, p <. 001. That is, for every 1 unit increase in satisfaction of life there is a −0.41 decrease in anxiety. Length of service was not a significant predictor b = −0.08, t (170) = −1.79, p = .07 and the Interaction between all three variables in the model was not significant b = −0.01, t (170) = −1.38, p = .16.
The second moderation explored whether years of service moderated SWL and OPSQ. Linear regression analysis was carried out to check the data for outliers and to check there were no homogeneity or homoscedastic problems. The values for Mahalanobis, Cook’s and Leaverage were all computed, which resulted in two outliers being identified and removed from the model. Multicollinearity was checked by running correlational analysis on the predictor variables, length of service and satisfaction with life, they were not correlated (r = 0.30, N = 175, p = .69).
The results revealed the overall moderation model was significant: F (3171) = 8.96, p < .001, R 2 = 0.12 accounting for 12% of the variance. SWL and length of service were both significant negative predictors within the model. Satisfaction with Life b = −1.19, t (171) = −3.39, p < .001. For every one unit increase in SWL, there is a −1.19 decrease in OPSQ. Length of service b = −0.49, t (171) = −2.01, p = .04. For everyone unit increase in years of service the result is a −0.49 decrease in OPSQ. The overall interaction model was also statistically negatively significant: Interaction b = −0.09, t (171) = −2.22, p = .02.
The analysis revealed no relationship between SWL and length of service prior to serving 15 years: (SWL) b = −0.50, t (171) = −1.02, p = .30. At 15 years of service (average) (SWL) b = −1.19, t (171) = −3.39, p < .001. Thus, by 15 years of service every additional year gives a decrease of −1.19 on levels of stress. At higher years of service, (SWL) b = −1.88, t (171) = −4.29, p < .001. Thus, for more years of service above the mean (of 15 years) stress as measured by the OPSQ decreases by −1.88 (See Figure 2). Moderation effect of years of service on the total scores gained on the satisfaction with life and operational police stress questionnaire scales.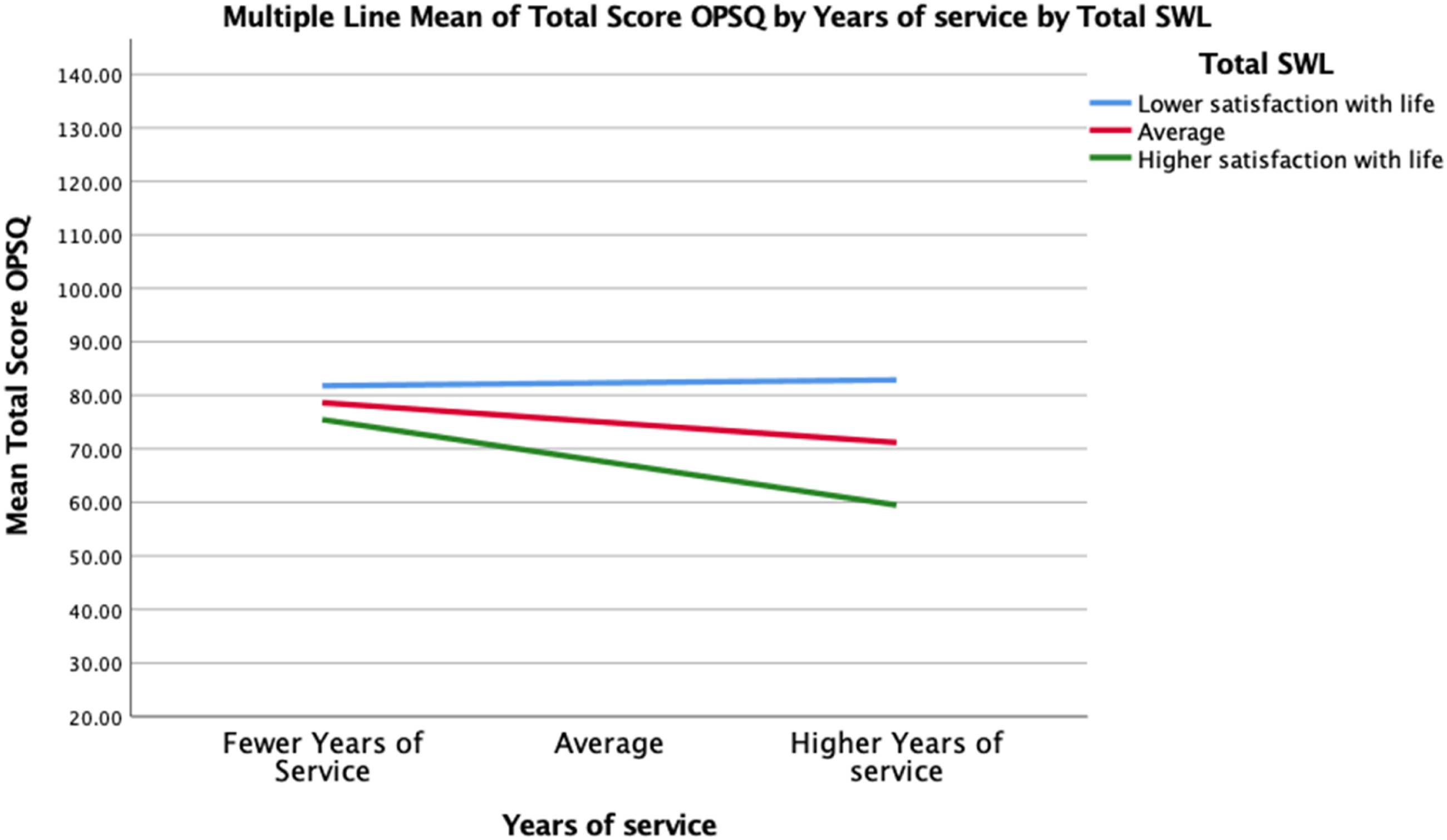
Having served at least 15 years, years of service and stress are significantly related t (171) = −1.97, p = .05, b = −0.81. As years of service increase, SWL increases and OPSQ decreases, with the longest serving officers (32 years) showing a decrease on the OPSQ of −2.72 per year (b = −2.72, t (171) = −3.72, p < .001).
To test the hypothesis that years of service moderated SWL and depression as measured by the PHQ-9, linear regression analysis was carried out to check the data for outliers and that there was no homogeneity or homoscedasticity. The values for Mahalanobis, Cook’s and Leaverage were all computed, which resulted in two outliers being identified and removed from the model. Multicollinearity was checked by running correlational analysis on the predictor variable’s years of service and satisfaction with life. This revealed the predictor variables were not correlated (r = 0.30, N = 175, p = .69). The results revealed the overall moderation model was significant. Overall model: F (3171) = 19.77, p < .001, R 2 = 0.26–26% of the variance is due to the interaction of the variables in the model.
SWL was significant within the moderation model: SWL b = −0.47, t (171) = −7.40, p < .001. For every one unit increase in SWL, there is a reduction of −0.47 on the PHQ-9. However, length of service was not significant within the model: Length of Service: b = −0.02, t (171) = −0.38, p = .70. The overall interaction model was not significant - Interaction: b = −0.02, t (171) = −1.62, p = .10.
Moderation analysis was also conducted to explore the interaction between neuroticism, years of service and GAD-7. Linear regression analysis was carried out to check the data for outliers and to check there was no homogeneity or homoscedasticity. The values for Mahalanobis, Cook’s and Leaverage were all computed, which resulted in two outliers being identified and removed from the model. Multicollinearity was checked by running correlational analysis on the predictor variable’s length of service and neuroticism, indicating the variables were not correlated (r = 0.00, N = 175, p = .99). Results revealed the overall moderation model was significant. Overall model: F(3171) = 25.67, p < .001, R 2 = 0.24. This accounts for 24% of the variance in the model.
Neuroticism was a significant predictor of anxiety - Neuroticism: b = 1.30, t (171) = 6.84, p < .001. For every 1 unit increase in neuroticism, there is a 1.30 increase in Anxiety. Length of service was also significant: b = −0.11, t (171) = −2.27, p = .02. For every 1 unit increase in years of service, there is t a −0.11 decrease in anxiety. However, the interaction between all three variables was not significant, Interaction: b = 0.01, t (171) = .61, p = .53.
Discussion
The present study explored rates of stress, anxiety and depression within a UK sample of 177 serving officers. Results indicate rates of Major Depressive Disorder in the present police sample 6 times that reported in the general population. Furthermore, 24.3% of the present sample met criteria for ‘yellow flag’ anxiety disorder, and 19.21% ‘red flag’ for anxiety disorder, significantly higher than reported general population rates. Depression and anxiety comorbidity was then examined. One third of the respondents who reported yellow flag anxiety levels also reported comorbid major depression levels, and 82.36% of the respondents who reported major depression also reported comorbid red flag anxiety levels. There is a lack of research that has explored the existence of comorbid presentations of anxiety and depression in a sample of serving police officers, using validated measures and this study helps to begin bridging the gap.
One of the main reasons why officers resign from the police is mental health (e.g. Wellington, 2018). The present results indicate a substantial level of anxiety and depression in police officers, and a link between depression and both yellow and red flag anxiety. Monitoring of anxiety levels would be recommended, with supportive strategies being put in place when officers score on or near to the yellow flag level on the GAD-7 to reduce the risk of reaching the red flag level, which was strongly associated with comorbid major depression. This may help reduce health risks associated with high levels of depression and anxiety as identified by Ramey et al. (2009), Robinson et al. (1997) and Gershon et al. (2008). Future research may wish to explore whether the relationship found in the current study is supported in larger samples, and whether providing early intervention methods to those scoring at or just below ‘yellow flag’ helps reduce clinical levels of depression. The findings in this study could go some way to explaining why the suicide rate amongst officers is three times that of the normal population (Miller, 2005).
It was hypothesised uniformed officers would report greater feeling of stress, anxiety and depression than their plain-clothed colleagues. Results indicated uniformed officers are more likely to experience higher feelings of stress, but not of anxiety or depression. The largest stressors identified were fatigue, paperwork, not enough time with friends and family, shift work and (lack of) healthy eating. This suggests the main stressors experienced by officers in the UK are organisational, rather than trauma related, in contrast with findings from the US (e.g. Abdollahi, 2002), and consistent with findings around shift work and stress (Ma et al., 2015). In contrast with previous research, no differences between genders were discovered. However, rates of stress, anxiety and depression were generally high in our sample, which may have impacted on results and requires further exploration.
In terms of personality, results indicated that respondents with higher levels of neuroticism reported higher levels of anxiety, and respondents with higher levels of extraversion reported lower levels of anxiety. There was no correlation between conscientiousness and anxiety. Multiple linear regression identified that neuroticism was a significant predictor of anxiety. Results therefore support the findings of Detrick and Chibnall (2013) and Habersaat et al. (2015), and suggest consideration could be given to screening personnel with a personality measure, to identify those who score higher on the extraversion scale and lower on the neuroticism scale, as these traits may provide protective factors against anxiety and then and would allow for bespoke development and intervention to be employed for individuals.
Looking at the potential impact of length of service, analysis suggested the more years of service an officer has the lower their presentation of operational stress, but with no significance prior to serving 15 years, which supports the findings of Evans et al. (1992) who found officers with 12 years or more service reported significantly less stress. Similarly, the significant negative correlation between length of service and GAD-7 suggests as length of service increases less anxiety is reported, or conversely those who experience less anxiety serve longer. Additionally, research has demonstrated that individuals who experience higher levels of anxiety do not perform as well when faced with ego-threatening tasks, and individuals who experience higher levels of anxiety when faced with demanding events perform less well than those who experience reduced levels of anxiety. Collectively, these findings suggest that screening for anxiety and offering bespoke intervention, both proactively and following high levels, is of upmost importance to improve personnel mental health, support performance and reduce attrition.
There was no relationship between length of service and depression, which is interesting given depression levels were six times that of the general population. However, many who were depressed had comorbid anxiety, and results indicated heightened stress and anxiety does link to depression and lower satisfaction with life. Present results revealed a significant negative correlation between the OPSQ, GAD-7, PHQ-9 and SWLS indicating that as stress and mental health difficulties rise satisfaction with life reduces, and conversely satisfaction with life increases, stress and mental health difficulties reduce. Multiple regression revealed the PHQ-9 was a significant predictor, indicating depression plays a significant role in satisfaction with life. Working on ways to enhance satisfaction with life could therefore be a preventative measure in the management or treatment of depression in police officers.
Limitations
Whilst the present study has identified a number of significant findings around mental health in the police there are a number of limitations. For example, respondents were not asked to identify whether they were plain-clothed or uniformed. Rather, this differentiation was made through personal knowledge from the researcher of the various departments in which participants were based. This may have resulted in some officers being wrongly coded. A second limitation was the use of self-report questionnaires, and the possibility of responder bias. It may that those who were feeling the pressure of their role, or were feeling stressed, depressed or anxious, were the participants who responded, leading to the high rates reported here. Conversely, there may be a stigma attached to reporting mental health issues and this may have limited the number of responders. Whilst the current study had enough respondents for statistical power, some forces were more represented than others; thus, there is a need for caution around assuming generalisability of results. Finally, the current study did not examine coping strategies employed by respondents, and therefore is limited in the conclusions that can be drawn around protective factors and therefore warrant further research.
Summary and contribution
The current results highlight significant levels of stress, anxiety and depression in serving police officers, utilising validated measures and identifies high risk for comorbid clinical anxiety and major depression. Thus, demonstrating this is an important area for screening, intervention and further research. The most significant stressors reported were organisational issues such as fatigue, paperwork, need to stay in physical condition, not enough time with friends and family, lack of healthy eating, and shift work. Addressing these organisational stressors may therefore reduce mental health difficulties within the police and are factors that require further investigation. Results also supported literature indicating that longer-serving officers, or those with higher extraversion and lower neuroticism personality traits, may be at reduced risk for anxiety or stress. It is possible that officers with particular personality traits are more likely to remain in the job, due to higher levels of resilience to work-related stress and is an area for future research and development within forces. This research highlights the need for routine screening within police personnel for anxiety and depression and the use of personality tools for development. These methods would also provide evidence that can be used to aid the design of bespoke intervention for individuals. It is hoped that research investigating individual differences will endure, to ensure the evidence base continues to grow. It is this evidence that can further strengthen initiatives such as the Blue Light programme and the National Police Wellbieng Service, in ultimately supporting forces to build world-class wellbeing support for all police personnel and improve the lives of those who serve and protect society.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.