
Abstract
The aim of the present study was to examine if work effort is associated with burnout among police officers and if job rewards and healthoriented leadership can mitigate the potential adverse effects of high work effort on officers’ mental health. Data were collected in a German police department (n = 573). The results indicated that high work effort was associated with higher levels of burnout while job rewards and health-oriented leadership were associated with lower levels of burnout. Additionally, health-oriented leadership buffered the effects of work effort on police officers’ burnout levels while job rewards showed no buffering effect. The results emphasize the importance of leadership for health promotion in policing.
Keywords
Introduction
The job of police officers is regarded as especially stressful and demanding, since it is characterized by various operational and occupational stressors like confrontation with violence, negative citizen encounters or shift work (Berg et al ., 2006; Biggam et al ., 1997). Especially, organizational factors like excessive administrative tasks or inconsistent leadership styles are identified as stressors by police officers (Biggam et al ., 1997; Newman and Rucker-Reed, 2004; Shane, 2010). At the same time, there are significant stressors related to police operations that commonly refer to the nature of police work. Particularly, the investigation of homicide is associated with cognitive and emotional stress among police personnel, like intrusive thoughts, disrupted sleep patterns and low mood (Roach et al ., 2017). Furthermore, a recent survey in the UK found that nearly 90% of 16,857 police officers had been exposed to a work related traumatic event and almost one in five experienced post-traumatic stress symptoms subsequently (Police Care UK, 2019). Prolonged exposure to work stress is associated with a variety of adverse health outcomes and police officers show elevated risks for cardiovascular disease and higher rates psychological distress compared to other working populations (e.g., Violanti et al ., 2006). A syndrome that is triggered by high job demands and chronic work stress is burnout, which is considered as a serious health threat to police officers (Santa Maria et al ., 2018; Stearns and Moore, 1993). It refers to a state of emotional exhaustion, accompanied by feelings of ineffectiveness and cynicism about the value of one’s work (Maslach et al ., 2001). High levels of burnout among police officers in turn are associated with a more positive attitude toward violence and a more frequent use of violence during officers’ duty (Kop et al ., 1999) as well as with work-family conflicts (Mikkelsen and Burke, 2004) and spouse violence (Johnson et al ., 2005). On an organizational level, burnout plays a mediating role in the relationship between job demands and counterproductive work behaviors of police officers (Smoktunowicz et al ., 2015) and is associated with job dissatisfaction and desires to leave the job (Pines and Keinan, 2005). Furthermore, burnout is a risk factor for developing depression (Hakanen et al ., 2008), which is associated with at-work performance deficits (Lerner and Henke, 2008) and an increased risk for police officers to develop metabolic syndromes (Hartley et al ., 2012).
While high work demands and work stress is associated with serious health impairments among police officers, the availability of job resources constitutes a protective factor against job-related burnout (e.g., Schaufeli and Bakker, 2004) and is capable to mitigate the negative impact of work demands on police officers’ mental health (Santa Maria et al ., 2018). Due to the highly stressful nature of police work and its negative consequences for police officers’ health, their social environment and the organization as a whole, the identification of job resources that are protective against job-related strain appears to be of particular importance in this occupational group. The aim of the current study was to examine the link between work effort and burnout among police officers and if job rewards and health-oriented leadership can mitigate the potential adverse effect of high work effort on officers’ mental health.
Effort-reward imbalance in police work
According to the effort-reward imbalance (ERI) model by Siegrist (1996), the availability of rewards in the work context is of key importance for employee health. The model is based on principles of social reciprocity and claims that an imbalance due to high effort and low reward at work generates strong negative emotions and stress responses among employees, increasing their risk of long-term adverse health effects. Effort refers to the demands and requirements related to the job and includes heavy workload, time pressure and being interrupted at work. Rewards that counterbalance effort are money, esteem, status consistency and career opportunities. Additionally, the ERI-model asserts that persons who are overcommitted to work, i.e. who react with excessive engagement to demanding situations at work and have a strong desire of being in control, have a heightened susceptibility to stress responses due to effort-reward imbalances (Siegrist and Li, 2016).
Many studies support the basic assumption of the ERI-model that an imbalance in terms of high effort and low rewards elicits sustained stress responses in employees and leads to psychological strain. Above all, the strongest evidence exist for the link between effort-reward imbalance and depressive symptoms among employees (Siegrist, 2017). According to Siegrist (2017), the relative risk of depression is elevated by about 80 percent among employees who experience stress due to high efforts spent and low rewards received. Furthermore, empirical evidence points to a link between an effort-reward imbalance and increased burnout levels among employees across different occupational groups (Bakker et al ., 2000; Klein et al ., 2010; Unterbrink et al ., 2007; Williams et al ., 2018).
If employees have little choice with regard to alternative workplaces, the prolonged imbalance between high effort and low reward is a serious risk factor for health problems in working populations (Siegrist, 2012). Since the employment sector of police work is rather specific and does not offer a large number of alternative career opportunities, police officers may be especially prone to adverse health effects due to high effort and low rewards. A recent study examined the association between ERI and burnout among police officers (Violanti et al ., 2018). Results indicated that an increased ERI among police officers is associated with increased levels of the burnout dimensions emotional exhaustion and cynicism. ERI was also found to be related to the subjective likelihood of health-related early retirement of police officers (Georg et al ., 2019). The results of further studies indicate that police officers who experience ERI have a nearly eight times higher risk to suffer from depression (Garbarino et al ., 2013) and show greater psychological distress (Janzen et al ., 2007). Thus, there is preliminary evidence that police officers who are exposed to high effort and limited rewards are at risk for developing significant health problems.
The role of leadership for the health of police officers
There is growing evidence that leadership is an important job resource in occupational health. Reviews on leadership styles across different occupations show that leaders play a crucial role with regard to health and well-being as well as to negative health outcomes like the experience of stress and burnout among employees (Kuoppala et al ., 2008; Montano et al ., 2017; Skakon et al ., 2010).
To date there are only a few studies examining the leadership-health link in the context of policing. Results of a recent study on German police officers indicated that a positive leadership climate was associated with reduced levels of emotional exhaustion, the core dimension of burnout (Engel et al ., 2018). Furthermore, a positive leadership climate also buffered the negative impact of high work effort on the experience of emotional exhaustion in this study. Another study on the effects of leadership on positive psychological states among officers indicated a strong relationship between leaders showing genuine concern for others’ well-being and increased self-confidence, a sense of fulfillment for the job and self-esteem among officers (Dobby et al ., 2004). Russell (2014) examined whether transformational leadership moderates the relationship of stress and burnout among police officers. Transformational leadership refers to leaders motivating employees to transcend self-interest for the benefit of the organization through charisma, inspiration, intellectual stimulation, and individual consideration (Bass, 2010). Results indicated that the experience of stress exacerbates burnout levels among officers and that transformational leadership attenuated this relationship. However, the buffering effect of transformational leadership was weaker under highly stressful conditions. A further study found that transformational leadership was related to increased psychosocial well-being of police officers, indicated by better self-esteem, more perceived social support at work, and less romantic partner conflict (Can et al ., 2017).
Transformational leadership and other existing leadership conceptions are measures of general leadership behavior which do not explicitly address health-related actions of leaders and do not take motivational or cognitive aspects of leadership into account. To address this gap, the concept of Health-oriented Leadership (HoL) was developed by Franke and Felfe (2011). The conceptualization of HoL focuses explicitly on health-related aspects of leadership and also attends to the leaders’ values and awareness toward employee health besides behavioral aspects. Health behavior in the HoL concept refers to creating healthy working conditions, providing information on health and safety issues as well as enabling and encouraging employees to engage in healthy behavior at work. Health awareness refers to a leader’s attention and sensitivity to health issues of employees and health impairing work conditions. A leader who scores high on health awareness is more likely to properly evaluate employees’ stress levels and to recognize signs of strain at an early stage. The value of health aspect addresses the leaders’ interest in health-related topics in the work context and the importance leaders attach to health in general. In the daily work routine it translates into the leaders’ sense of responsibility for employee health and their concerns about health issues of their staff members. The HoL concept also addresses the active role of employees in the leadership-health link by investigating the role of the employees’ own health-related behaviors, awareness and values in this process. The HoL concept also addresses the active role of employees in the leadership-health link by investigating the role of the employees’ own health-related behaviors, awareness and values in this process. According to Franke and Felfe (2011) a major advantage of the HoL concept is that it provides health-specific practical implications for the health promotion of employees.
In a longitudinal test-of-concept-study health-oriented leadership was positively related to employee health and negatively related to irritation, health complaints and work-family conflicts (Franke et al ., 2014). Importantly, health oriented leadership explained a unique variance in the health outcomes beyond transformational leadership. Moreover, the relationship between a health-oriented leadership style and health outcomes was mediated by the employees own health behavior at work. Thus, employees who perceived the leadership style of their direct supervisor as health-oriented were more likely engaging in health promoting behaviors at work resulting in fewer health complaints. Recently, the concept of HoL was applied to the context of police work for the first time (Santa Maria et al ., 2019). Results indicated that a health-oriented leadership style was associated with more well-being and lower levels of burnout, depression and physical complaints among police officers. The officers’ own health-behaviors only partially mediated the relationship between leadership and well-being while they did not mediate the relationship between leadership and adverse health outcomes. Thus, the results emphasize the importance leadership for the health of police officers beyond their own health behaviors in the work context.
The present study
The present study focuses on the association of work effort and police officers’ burnout levels and examines the potential protective role of job rewards and leadership in this process. While the ERI model claims that the availability of rewards is crucial in order to reduce adverse health effects due to high efforts at work, leadership plays a minor role in the operationalization of the reward dimension in the ERI-model. Thus, the aim of the current study is to enhance the ERI model by examining the potential beneficial role of leadership for police officers’ health. We focus on the value and awareness dimension of health-oriented leadership since organizational and operational demands like high-risk operations, confrontation with violence, staff shortage or shift work may significantly reduce the potential of police leaders to engage in actual health-oriented behavior in the daily working routine. We assume that the amount to which police officers perceive leaders as being aware of job-related health risks (health awareness) and attach importance to their health and well-being (value of health) are important factors for mitigating stress-related adverse health effects in this occupational group.
In accordance with the ERI model we hypothesize that work effort is positively, and job rewards are negatively related to symptoms of burnout among police officers. Also in line with the postulations of the ERI model, we expect that the relationship between work effort and burnout is weaker for officers enjoying high job rewards, i.e. we expect that job rewards buffer the health impairing effect of work effort. With regard to the potential health promoting role of leadership, we hypothesize that besides rewards also health-oriented leadership is associated with reduced burnout levels and is capable of buffering the adverse impact of work effort on officers’ burnout levels (see Figure 1).
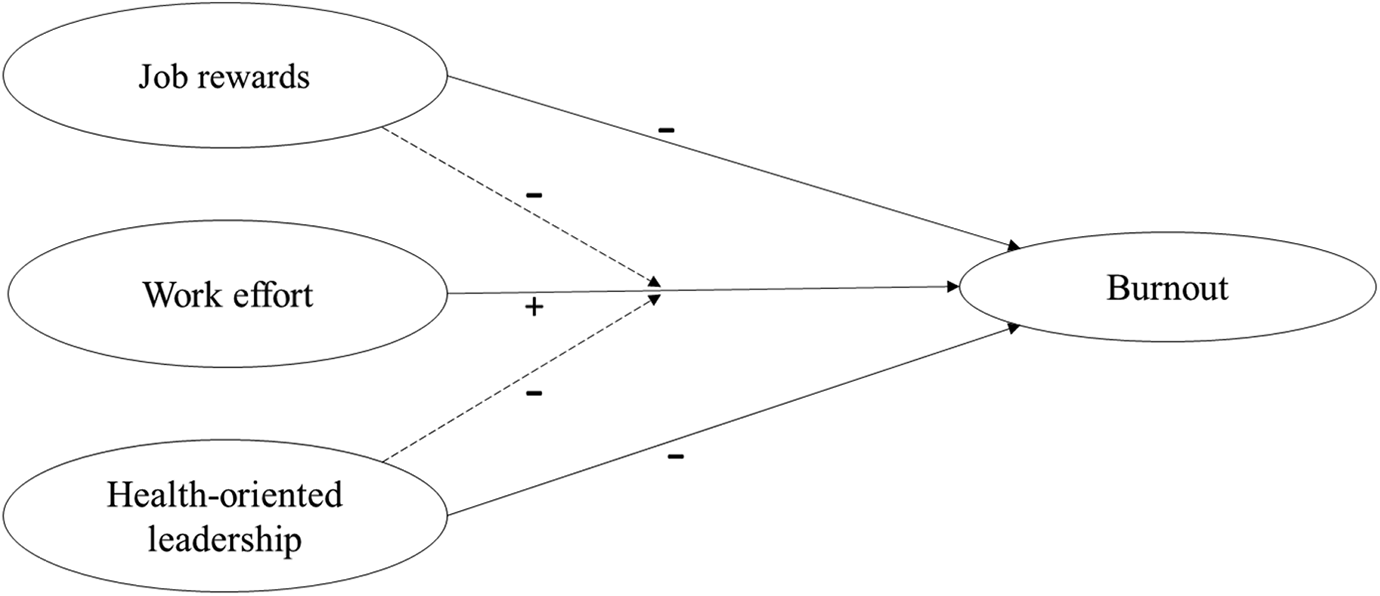
Model including the hypothesized relationships between health-oriented leadership, work effort, job rewards and burnout. The interaction paths are indicated by a dashed line.
Method
Participants and procedure
Data of the present study were obtained via an online survey in an urban police department in Germany. All 1787 members of the department received an invitation to participate in the survey via their working e-mail address. Police officers out of the office received a paper pencil version of the questionnaire at their home addresses. Participants were informed that participation was voluntary and that all data were kept confidential. In total, 573 police officers completed the survey, resulting in a response rate of 32%. Regular citizen encounters were part of the work routine for 87% of the police officers in the present sample. Furthermore, 60% of the officers were participating in police operations and 25% had leadership roles in the department. The vast majority of the police officers in the present sample were working full time (91%). The mean age of the sample was 42.5 years (SD = 9.8), 70% were male and 30% were female. The average years of service of the participating officers was 21.1 years (SD = 11.2). The study was approved by the ethics committee of the research institute as well as by the personnel board of the police department.
Measures
Data analysis
Descriptive statistics with regard to characteristics of the study sample, outcome variables (means, standard deviations) and reliability measures were obtained using SPSS 24. For testing the hypotheses we conducted structural equation modeling (SEM) with Mplus version 7.4 (Muthén and Muthén, 2014). As recommended by Schermelleh-Engel et al . (2003), the fit of the models was assessed by the Chi-Square goodness-of-fit statistic, Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), the Tucker Lewis Index (TLI) and Standardized Root Mean Square Residual (SRMR). For the RMSEA a cutoff value close to .06, for the SRMR a cutoff value close to .08 indicates a good fit. For the CFI and the TLI values of .90 are acceptable and values close to .95 indicate a good fit of the hypothesized model to the data (Hu and Bentler, 1999).
The measurement model was specified and tested first, in order to identify and address potential issues regarding the model fit before the full structural model was tested (Herting and Costner, 2000). In order to test the hypotheses, a model with work effort, job rewards and health-oriented leadership as exogenous variables and burnout as an endogenous variable was specified in a first step. In a next step, two interaction terms (job rewards x work effort/ health-oriented leadership x work effort) were added to the model in order to test the respective buffering hypotheses. Thus, in order to test the combined effect of work effort and job rewards an interaction term (work effort x job rewards) rather than the commonly used ERI ratio term was utilized in the present study, as recommended by Van Vegchel et al . (2005).
For all model estimations Robust Maximum Likelihood (MLR) was used.
Results
Means, standard deviations, intercorrelations and reliability coefficients (Cronbach’s alpha) of the study variables are presented in Table 1. The internal consistencies (Cronbach’s alpha) of all scales except for work effort exceed the value of .70, indicating good reliability. Cronbach’s alpha for the work effort scale was .67, indicating acceptable reliability. All correlations between the variables were significant (p < .05).
Means, standard deviations, correlations between the study variables and internal consistencies (Cronbach’s Alpha).
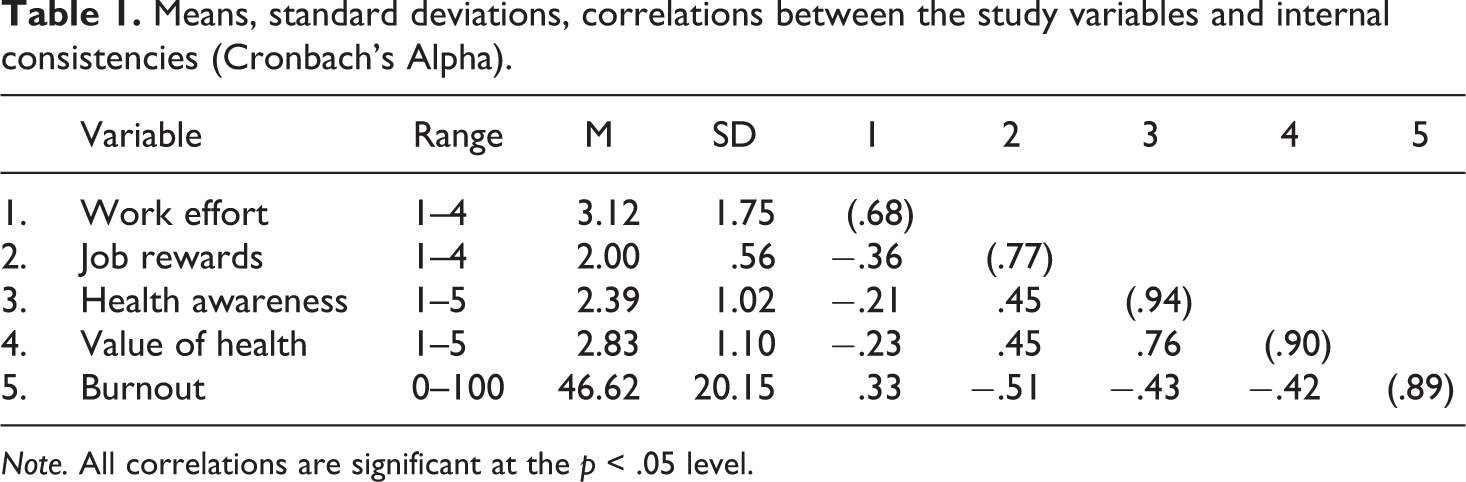
Note. All correlations are significant at the p < .05 level.
The measurement model of the exogenous (work effort, job reward, health-oriented leadership) and endogenous variables (burnout) showed that the model fits the data adequately (χ2 [244, N = 573] = 820.125, p < .001, CFI = .92, TLI = .91).
The model of the hypothesized relationships between health-oriented leadership, work effort, job rewards and burnout was tested using SEM (see Figure 2). The hypothesized model showed a reasonable fit with the data, indicated by the following goodness-of-fit measures: χ2 [244, N = 573] = 810.125, p < .001, RMSEA = .06, SRMR = .05, CFI = .92 and TLI = .91. Since the χ2 test is sensitive to sample size, a significant χ2 test is common for large samples (Hu and Bentler, 1999). In line with our hypotheses, work effort was positively (ß = .16, p < .01) and job rewards were negatively related to burnout (ß = −.37, p < .01), confirming the basic postulations of the ERI-model. As expected, health-oriented leadership was also negatively related to burnout (ß = −.24, p < .01; Figure 2).
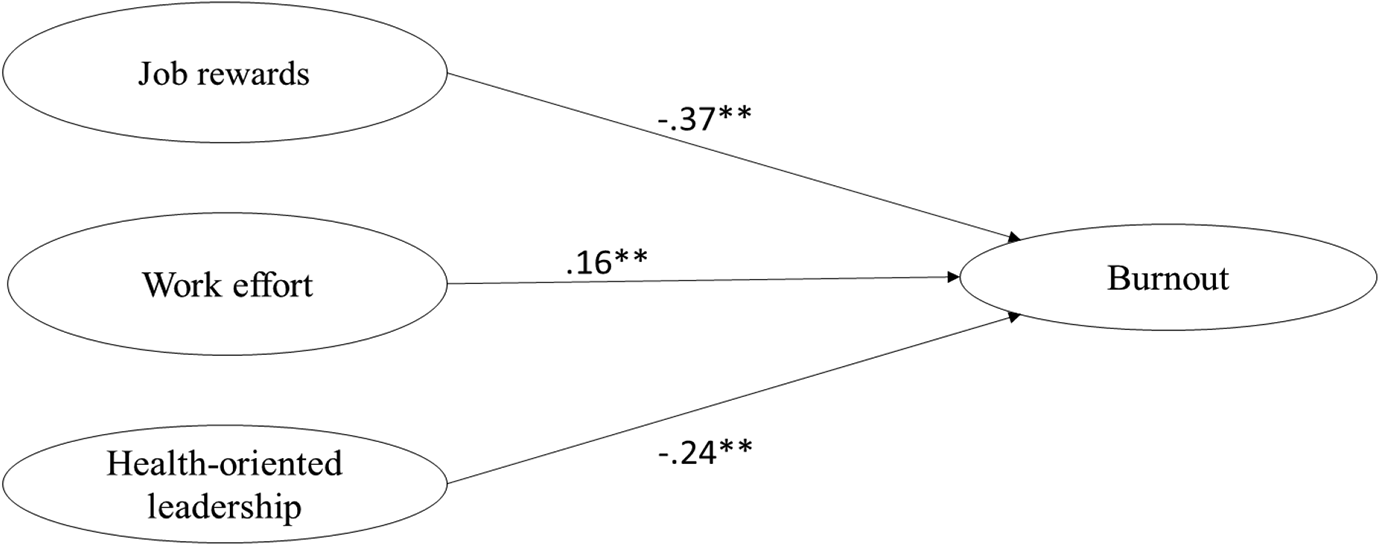
Standardized path coefficients for the hypothesized relationships between job rewards, work effort, health-oriented leadership and burnout. *p < .05. **p < .001.
In order to test whether job rewards and health-oriented leadership buffer the adverse impact of work effort on mental health, a second model with the respective interaction terms was specified and tested. Since the goodness-of-fit measures (RMSEA, SRMR, TLI, CFI) are not assessable for interaction terms, the comparison of the second model with the first model was obtained by the Akaike information criterion (AIC) and the z test of the interaction terms. The AIC of the second model including the interaction terms (AIC = 56676.50) was smaller than in the first model (AIC = 56677.05), indicating that it fitted the data better (Schreiber et al ., 2006). The interaction term with health-oriented leadership was significant (ß = −.18, p < .05). However, the interaction term with job rewards was not significant (ß = .09, p = .26). Thus, an adjusted model without the non-significant interaction term was specified and tested (see Figure 3), resulting in a better fit of the model to the data (AIC = 56673.63). In the adjusted model the interaction term for health-orientated leadership was still significant, confirming the buffering effect of HoL on the relationship between work effort and burnout (ß = −.11, p < .05).
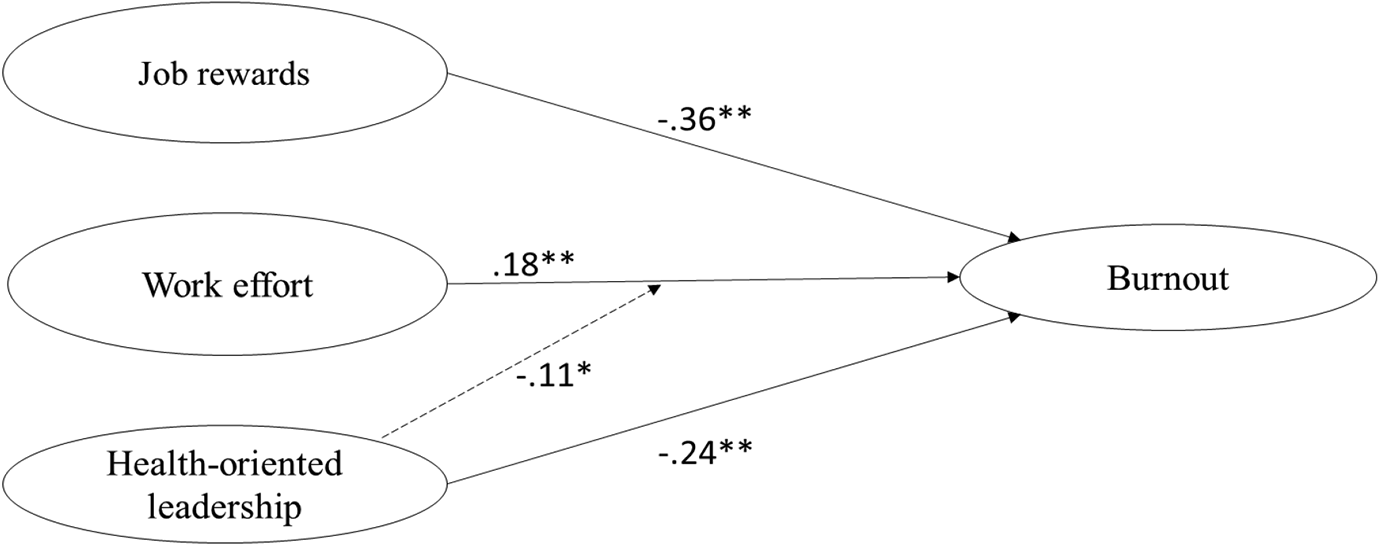
Standardized path coefficients for the adjusted model including the significant interaction term (Work effort x Health-oriented leadership). *p < .05. **p < .001
Discussion
The aim of the present study was to examine the relationship between work effort and burnout among police officers and to identify protective factors against work-related psychological strain in the context of police work. While job rewards are regarded as an important resource that counteract health issues due to high demands at work in the well-established ERI model, the current study aimed to enhance the model by focusing also on the potential health promoting impact of health-oriented leadership in this process.
In sum, the results confirmed our central assumptions regarding the importance of leadership for police officers’ health, while the hypotheses regarding the postulations of the ERI model were only partially supported. In line with the ERI model, work effort was associated with increased burnout levels while job rewards were associated with reduced burnout levels. However, only health-oriented leadership but not job rewards mitigated the health impairing effects of high work effort, pointing to the prominent role of leadership for health promotion in policing.
The result that work effort was associated with higher levels of burnout is in line with results of previous studies indicating that high work effort is linked to emotional exhaustion, the central component of the burnout syndrome (Hall et al ., 2010; Willis et al ., 2008). Furthermore, the finding of this study corresponds also to the results reported by Santa Maria et al . (2018) after which workload is linked to emotional exhaustion and subsequent depressive symptoms among police officers. Thus, our results contribute to the empirical evidence that high work effort constitutes a significant risk factor for adverse mental health effects among police officers.
As expected, job rewards were negatively related to the experience of job-related burnout, supporting the basic assumption of the ERI model that the availability of rewards in the working context constitutes a protective factor against work-related strain (Siegrist, 2017). However, job rewards did not buffer the adverse effects of work effort on officers’ burnout levels in the present sample. This finding contradicts the assumption that the relationship between work effort and job-related strain is weaker for employees who perceive their work as rewarding. In the present study job rewards were assessed as a global measure without differentiating the three distinct reward systems (esteem rewards, financial rewards, security rewards). Thus, a possible explanation for the non-significant interaction effect is that potential effects of job rewards may have been averaged. While Siegrist and Peter (1996) advocate the use of reward as a global measure, van Vegchel et al . (2005) suggest that the reward structures should be examined independently since different rewards may have different effects on the outcome measures. For example, high work effort had the most adverse effects on employee health when esteem rewards were low, while low financial rewards did not have a strong effect on health outcomes (van Vegchel et al ., 2005). Thus, instead of one global measure of job rewards, future research should examine the specific effects of the reward dimensions on health outcomes of police officers separately. Another possible explanation for the missing buffering effect might be that there are other more important job resources in the occupational field of policing which alleviate the adverse effects of high work effort. For example, a study using the job demands-resources model (JD-R) found that social support by colleagues, shared values and a positive leadership climate were important job resources that buffered the adverse effects of high job demands on emotional exhaustion among police officers (Santa Maria et al ., 2018). Police officers’ work values were also identified as a protective factor against burnout and were positively related to work engagement in a recent study by Basinka and Daderman (2019). Thus, it may be advisable to use broader models like the JD-R model in future research to allow the integration of various job resources relevant to policing.
The finding that a health-oriented leadership style was associated with reduced levels of burnout among police officers in the present sample is consistent with existing studies on the leadership-health link showing that health-oriented leadership is associated with reduced physical and psychological health problems in the general working population (Franke et al ., 2014) and among police officers (Santa Maria et al ., 2018).
Furthermore, our results indicate that health-oriented leadership style was even capable of buffering the health-impairing effects of high work effort. That is, officers who perceive that their direct supervisor cares for their health and is aware of their current stress level have a reduced risk for job-related burnout. The potential of leadership to mitigate the adverse effects of job demands on mental health of police officers was also found in a previous study in which a positive leadership climate buffered the negative impact of high work effort on emotional exhaustion among police officers (Engel et al ., 2018). Moreover, our results regarding health-oriented leadership are all the more remarkable as not behavioral aspects but the leaders’ health awareness and their value for health mitigated the adverse effects of high work effort. Police officers who perceive that their supervisor attaches importance to health issues and recognizes when and why someone is stressed, may feel better cared for and taken more seriously. Thus, HoL may reflect a leader’s appreciation and recognition for individuals which had been shown to be positively associated with employee well-being in stressful work situations (Gilbert and Kelloway, 2018; Stocker et al ., 2018). Leaders’ health awareness and value of health may be especially important beyond behavioral aspects in the context of policing, since the potential of actual health-oriented leadership behavior, like protecting employees from physical strain at the workplace, is often restricted due to the challenging nature of police work as a high risk occupation (Dantzer, 1987). The everyday routine police officers face especially in stressful urban environments often implies the risk of physical and psychological harm. Furthermore, organizational factors like staff shortage or shift work may also hinder police leaders in health-oriented behavior, even if they do care and attach importance to the health of their subordinates. Since appreciation and recognition may be an important underlying mechanism in the leadership health link, future research should examine their role within the theoretical framework of health-oriented leadership. For example, it could tested whether appreciation and recognition moderate the relationship between leadership and beneficial health outcomes among employees.
Limitations and future directions
Despite its strength in providing knowledge about preventive factors against job-related burnout among police officers, the present study has some limitations that should be noted. First, all analyses were based on cross-sectional data which does not allow conclusions about the temporality and causality of the observed effects. Longitudinal studies are needed in order to assess causal influences of job rewards and leadership on health outcomes of police officers. However, the concept of health-oriented leadership (Franke et al ., 2014) and the ERI model (Tsutsumi and Kawakami, 2004; van Vegchel et al ., 2005) were both empirically validated in longitudinal studies. Thus, previous studies support the hypothesized directions of the relationships between work effort, job rewards, leadership and burnout tested in the present study. Second, all data in the present study were obtained by self-report measures. This increases the risk of common method variance which may cause an overestimation of the strength of the observed relationships. This potential problem could be addressed by using objective rather than solely subjective measures. For example, the number of operations of police officers could be taken into account as a proxy for work effort. Third, even though we obtained a satisfactory overall response rate of 32%, there is the risk that results may be biased by nonparticipation. On the one hand studies have shown that responders are slightly healthier than non-responders in large population based health surveys. On the other hand those studies have also shown that the impact of these differences on prevalence rates was rather small, resulting in relatively unbiased results even for studies with only moderate response rates (Sogaard et al ., 2004; Vink et al ., 2004).
Practical implications
The results of the present study show that high work effort has adverse consequences for mental health of police officers. There are several job demands that are inherent to policing and can hardly be changed. Still, it is nonetheless vitally important to reduce police officers’ work effort whenever possible in order to prevent work-related health impairments. The aspects of work effort assessed in the present study, like working overtime or under high time pressure, represent organizational stressors which had repeatedly been identified as the greatest source of police stress (Shane, 2010; Violanti and Aron, 1995). Staff shortage is a major problem related to high workload and time pressure in the daily work routine of police officers. Hiring more staff may not only prevent job-related strain in police officers but is also advisable from an economic point of view since staff savings may result in even higher costs due to higher rates of sickness absence and associated costs for the health-care system in the long run. The results of the present study provide further empirical support for the necessity to reduce workload and staff shortages in order prevent health problems among police personnel and to sustain police officers’ long term working-capacities.
Besides reducing work effort, leadership appears to be of particular importance for the objective to promote police officers’ health. Thus, police leaders have a special responsibility not only for performance aspects but also with regard to protecting the health of their subordinates. This is even true, when leaders’ capabilities to engage in health-promoting behavior is restricted because of job demands in policing which can hardly be changed. First, our results implicate that the awareness of police leaders for signs of stress and strain among officers should be promoted during leadership development. For example, Chapin et al . (2008) describe a specific training program for police leaders to recognize and address stress symptoms among their personnel. Police leaders are educated in physical, emotional and social effects of stress and how to assess signs of stress experienced by officers in their unit. Besides focusing on stress management strategies, the training program provides a specific tool for rewarding officers who take action to manage their own stress, support a coworker in difficult times or challenge the social climate that discourages and stigmatizes help seeking in the department.
In order to reduce stigmata and create a working atmosphere wherein help seeking is encouraged the value leaders attach to health issues of subordinates is an important prerequisite. When a police leader expresses that he or she cares for the health of their subordinate officers and signals that it is nothing to be ashamed of to feel stressed and emotionally strained at times, it is more likely that they seek social support and take positive action to manage their stress. Thus, a health-oriented attitude that is characterized by valuing the health of subordinate officers should be promoted as well during police leadership development in order to prevent that officers postpone help seeking until job-related problems may force disciplinary action and mental health problems become chronic.
Taken together, the findings of the present study provide further evidence that police leaders play a key role for creating a healthy working environment and for reducing job-related mental health issues among police officers. A greater incorporation of health-orientated aspects of leadership in the education of police leaders is likely to have a beneficial impact on police officers’ health and may support them to cope better with the daily hazards of a highly demanding job.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Berlin Police, Germany. The funding source supported the collection of the data by addressing potential participants. The Berlin Police had no further involvement with regard to study design, analysis or interpretation of the data, writing process or submission of the article.