
Abstract
Introduction
Hand preference is the tendency to be more skilled and comfortable using one hand instead of the other for tasks. Twin studies have shown that genetic effects account for around 25% of the variance in hand preference, with the remaining attributed to non-shared environmental influences (Cuellar-Partida et al., 2021; De Kovel et al., 2019; Medland et al., 2009; Ocklenburg et al., 2025). While hand preference starts to emerge prenatally, at 10–12 weeks (Hepper, 2013), it does not get fully established until the early primary school years (around 6 years of age; Scharoun & Bryden, 2015). Most of the population is right-handed, around 10.6% are left-handed, and 9.3% are mixed-handed (i.e., showing inconsistent hand preference for tasks), including the ambidextrous (Papadatou-Pastou et al., 2020). Ambidextrous individuals (those using both hands equally well) are a very small group; estimated prevalence is 1–3% (Cuellar-Partida et al., 2021). Being left-handed or mixed-handed is seen more frequently in males than females (Cuellar-Partida et al., 2021; Papadatou-Pastou et al., 2020).
To date, hand preference has been predominantly studied in the context of motor skills and cognition. However, there is also evidence for a link with psychological and neurological conditions, including eating disorders (EDs) (Christman et al., 2007; Niederhofer, 2007). EDs are complex psychiatric disorders characterised by disturbances in eating behaviours, body image, and weight regulation. They are also highly comorbid with other psychiatric conditions (Arcelus et al., 2011), with some studies suggesting that as high as 70% of ED patients have another psychiatric illness (Momen et al., 2022). However, the association between hand preference and EDs has only been explored in small adult samples. To our knowledge, there is no research into the association between hand preference and ED symptoms in the general adolescent population. We carried out this study to fill this gap.
Hand Preference and Eating Disorder (ED) Risk
Hand preference is related to brain lateralization, with the left-handed being typically less lateralized than their right-handed counterparts. For example, 96% of right-handers and 73% of left-handers are left-hemisphere dominant for language (McManus, 2009; Sha et al., 2021), in turn suggesting some cognitive differences between the left and the right-handed (Badzakova-Trajkov et al., 2010; Uher & Treasure, 2005). However, research has shown that both the direction of hand preference and its degree (the consistency of hand use for specific functions) are important factors in lateralisation. Right-handers are generally more consistent in degree than left-handers, as well as more lateralized, with potential less interaction across hemispheres, although it is the mixed-handed and the ambidextrous who likely show the greatest interhemispheric interaction (McManus, 2019). However, it is not known whether less lateralization in left-handers is a result of development and adjustment, given the world is ‘made’ for right-handers, or cultural factors pressuring right-hand use (Papadatou-Pastou et al., 2020).
Their cause notwithstanding, differences in brain lateralization may be related to ED risk. For example, in anorexia nervosa patients, decreases in parietal lobe activity linked to bodily awareness were consistent across both hemispheres (Titova et al., 2013), tentatively suggesting less lateralization in anorexia nervosa. These differences may also contribute to differences in perceptual biases related to body image, observed deficits in EDs. For example, if the right hemisphere (the dominant hemisphere in the left-handed) plays a key role in body-image representation (since it is dominant for visual processing), then damage to it may be directly linked to ED psychopathology. This has indeed been evidenced by ED remissions following removal of lesions in the right frontal and temporal lobes (Uher & Treasure, 2005).
Nonetheless, research into the direct association between hand preference and EDs is limited. Christman et al. (2007) examined the link between handedness and both accuracy of perceived body-size and ED symptomology in 185 undergraduate students. They found that stronger right-hand use was associated with larger discrepancies between perceived and actual BMI (particularly in females). They also suggested that strong right-hand use may be associated with increased ED psychopathology, although their findings cannot generalise across the range of hand preference, since their just three strong left-hand users were removed from the analysis. Interestingly, a small-scale study of 18 ED patients and 18 controls found that right-hand use was less represented among ED patients (14%) than controls (58%). However, statistical assumptions were not met for analysis and the hand-preference questionnaire used considered eight functional tasks, with hand-representation differing by task (Niederhofer, 2007). Together these two studies suggest that both non-right-hand preference and strong degree of right-hand preference may be related to elevated ED risk.
Methods
Sample
We used data from the Millennium Cohort Study (MCS) a longitudinal survey of children born in the UK between September 2000 and January 2002 (https://cls.ucl.ac.uk/cls-studies/millennium-cohort-study/). The MCS utilised a stratified clustered sampling method to ensure representation of the UK population. There have been eight sweeps (waves) of data collection to date. In MCS, data on hand preference (N = 11,361) and ED symptoms were first collected at sweep 6, age 14.
Measures
Hand Preference
At the age 14 sweep, participants were asked to indicate which hand they write with best, with options being right-hand (RH), left-hand (LH) or either hand.
ED Symptoms
At the same sweep, they were asked four questions indexing degree of: exercising with the intention to lose weight; dietary restriction with the intention to lose weight; current intention to lose weight, and weight dissatisfaction. The questions align with clinical features of EDs as defined by DSM-5 (APA, 2022) and used in assessment of EDs. Although these four items were not derived from a single validated ED measure, they are aligned with well-known, heavily-used and validated measures, including the Eating Disorder Examination (EDE) and EDE-Questionnaire (EDE-Q). The EDE and EDE-Q have demonstrated good validity and reliability across studies and have been shown to discriminate between individuals with EDs and non-clinical controls (Cooper et al., 1989; Fairburn & Beglin, 1994). Importantly, the three EDE/EDE-Q subscales most relevant here (those assessing weight concern, shape concern, and eating concern) consistently show high internal consistency in adolescent and adult samples (Friborg et al., 2013). Another self-report instrument, studied with ED patients and related to the measure of weight dissatisfaction used in MCS, is the Body Shape Questionnaire (BSQ; Cooper et al., 1987) which measures body image symptoms and can identify persons with excessive concerns about weight or shape (Rosen et al., 1996).
Confounders
Variables associated with 'exposure' and outcome included sex; ethnicity (UK census groups of White, Black, Indian, Pakistani/Bangladeshi, Mixed, or Other, recoded to white vs not); family income (equivalised household income quintiles, recoded to bottom quintile vs not); and concurrent pubertal status (skin changes) and weight (UK90 reference). The MCS ‘stratum’ was also controlled to account for the MCS sample design.
Statistical Analysis
Each ED symptom was coded 1 (present) or 0 (not present). A total ED risk measure where participants were scored 1 if they had all four ED symptoms was also created. For writing-hand preference, as the proportion of either-hand use participants was too small for reliable analysis (N = 145/1.3%), we ran analyses where the left-hand use group both included the either-hand use group (i.e., ‘non-right-handers’) and excluded them (i.e., ‘left-handers’). As there was no difference in results with that group excluded, we excluded them throughout, and in all analyses the right-hand use group was coded 1 and the left-hand use group 0. Logistic regression models were fitted to examine the relationship, after confounder adjustment, between writing-hand preference and each ED symptom as well as total ED risk. Assumptions and model fit index were examined for each model fitted.
Results
As expected, most participants were right-handed (87% reported they write best with their right hand, 12% with their left, and 1.3% with either hand; Table S1). About 65% were healthy weight, but 60% were dissatisfied with their weight and 60% reported engaging in exercise to lose weight. Dietary behaviours were less prevalent, with 45% reporting dietary restriction to lose weight and 42% reporting an intention to lose weight. About 20% were at ED risk (showing all four ED symptoms). Writing-hand preference (right-hand vs left-hand) was not related to any ED symptom or total ED risk at the bivariate level (Tables S2–S6).
Logistic Regression Results for Risk of Weight Dissatisfaction
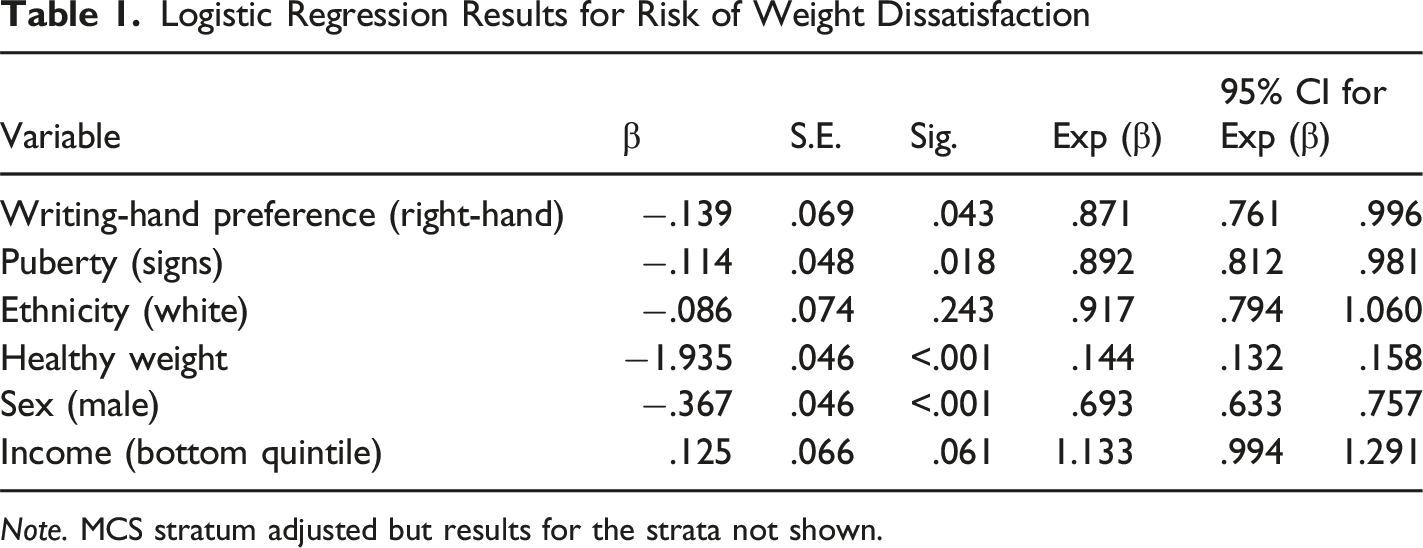
Note. MCS stratum adjusted but results for the strata not shown.
Discussion
Our hypothesis that in the general UK population there would be differences in risk of ED in adolescence by writing-hand preference was not supported as writing-hand preference was not related to total ED risk. However, compared to right-handed, left-handed adolescents were more likely to report weight dissatisfaction after adjustment for confounders. That is, although there were no differences by writing-hand preference in exercising to lose weight, engaging in dietary restriction to lose weight, or intending to lose weight, the left-handed group was at increased risk of weight dissatisfaction. These findings are important as they may suggest potential differences in brain organization in left-handers that relate to body perception (Uher & Treasure, 2005). We note, however, that the size of the effect of writing-hand preference was small, but also very specific as it was not related to any ED symptom even at the bivariate level.
We speculate that left-handed adolescents may be more likely to be dissatisfied because of an ‘over-processing’ or hyper-fixation of body image due to right hemisphere dominance. It is important to be reminded, however, that this difference emerged only after adjusting for confounders. As expected, the strongest and more consistent predictors of all ED symptoms were female sex and being of unhealthy weight, with minority ethnic and advanced pubertal status also significant for most ED symptoms. Weight dissatisfaction, in particular, was strongly related to unhealthy weight and female sex. Together these findings suggest that sex and weight are likely strong suppressors of the effect of writing-hand preference on weight dissatisfaction. They also mean that, to be of use in an ED risk assessment in adolescence, information on writing-hand preference must be considered alongside that on sex and weight status.
In terms of future directions, we urge researchers to consider the role of degree of hand preference too, as degree (i.e., strong vs. mixed) is potentially as important as its direction when considering psychological differences (Niebauer, 2004). We must almost acknowledge that mental health symptoms, not accounted for in the study, might play a role in the relationship between hand preference and weight dissatisfaction. There are some additional study limitations. Firstly, as the study was observational and cross-sectional in design, causality cannot be inferred. Secondly, the measures used, including the single item on writing-hand preference, were collected at age 14. Therefore, we could not determine the exact onset of ED symptoms or account for different developmental trajectories of writing-hand preference. Thirdly, our hand preference measure was a crude measure of writing-hand preference. For example, it did not capture whether the preferred writing hand was also used for other functions. Handedness is a complex construct, as individuals’ ability to use their non-dominant hand varies (Corey et al., 2001). Our study could not capture this complexity since children were only administered a single-item question (asking them with which hand they write best) in adolescence instead of a validated questionnaire (e.g., the Edinburgh Handedness Inventory; Oldfield, 1971). According to past literature, single-item measures may not be capturing the complexity of mixed-handedness accurately, leading to misclassification and inconsistency (De Kovel et al., 2019). However, the distribution of hand preference in our sample is broadly in line with what has been reported (Papadatou-Pastou et al., 2020), which reassures. Still, the very small number in our sample of those using either hand to write precluded a more granular analysis of atypical writing-hand preference by ED risk. Future research should address these limitations.
Supplemental Material
Supplemental Material - Writing Hand Preference and Eating Disorder Symptoms in Adolescence: Findings From a UK Birth Cohort Study
Supplemental Material for Writing Hand Preference and Eating Disorder Symptoms in Adolescence: Findings From a UK Birth Cohort Study by Esther Eldridge-Mrotzek and Eirini Flouri in Perceptual and Motor Skills.
Footnotes
Acknowledgements
We would like to thank the MCS families who made this work possible.
Ethical Considerations
Consent to Participate
Parental consent was obtained for all data used in this study. The cohort children themselves provided assent at age 11 and consent at age 14.
Author Contributions
Eirini Flouri: Supervision, Project administration, Writing - review & editing; Esther Eldridge-Mrotzek: Conceptualization, Writing - original draft, Visualization, Writing - review & editing; Methodology, Data Curation, Investigation, Formal Analysis.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.