
Abstract
The Global Physical Activity Questionnaire (GPAQ) has been used often to assess physical activity (PA) patterns. However, the European Portuguese version of this instrument has not been validated. We aimed to validate the self-administered GPAQ, version 2, (GPAQv2) for Portuguese adults. We included 32 participants in a pilot study of a Portuguese adaptation of the test and 108 participants in an assessment of their PA patterns and sedentary behavior (SB) through the GPAQv2. For its validation, we compared the GPAQv2 to the International PA Questionnaire-Long Form (IPAQ-LF) (concurrent validity) and the ActiGraph wGT3X-BT accelerometer (criterion validity). We evaluated PA and SB at baseline and after seven consecutive days. Test-retest reliability with the Kappa test (k) and the Intraclass Correlation Coefficient (ICC) ranged from strong to almost perfect (k: 0.864–0.976) and from moderate to excellent (ICC: 0.56–0.994), respectively. Concurrent validity, assessed by Spearman’s Correlation Coefficient, was moderate to substantial (rho: 0.471–0.680), and there was fair to substantial criterion validity (rho: 0.226–0.672). Bland-Altman plots showed that the GPAQv2 overestimated vigorous and moderate to vigorous PA and underestimated moderate PA. The largest difference values were related to SB, since the GPAQv2 underestimated sitting time. In sum, we found the GPAQv2 to have acceptable validity and reliability for assessing PA and SB patterns, and we recommend its use for Portuguese adults.
Introduction
Regular physical activity (PA) is a fundamental component of a salutogenic lifestyle, due to its multiple proven benefits in promoting health (Bull et al., 2009; WHO, 2020b) and preventing such chronic diseases as cardiovascular disease (Kyu et al., 2016; Tucker et al., 2022), type 2 diabetes (Fletcher et al., 2018), cancer (D’Ascenzi et al., 2021; Matthews et al., 2020) and other health outcomes (Angulo et al., 2020; Dipietro et al., 2019), including mental health (Barnes, 2015; Sawan et al., 2023). The World Health Organization (WHO) guidelines recommend that adults (18–64 years old) practice at least 150–300 minutes of moderate-intensity aerobic PA (MPA) or at least 75–150 minutes of vigorous-intensity aerobic PA (VPA) or an equivalent combination of moderate and vigorous-intensity PA (MVPA) each week to maintain or improve overall health and reduce the risk of or even prevent chronic disease (WHO, 2020b). However, over the last few decades there has been an exponential increase in physical inactivity levels in contemporary society (Nikitara et al., 2021), leading to an increasingly sedentary lifestyle (Stamatakis et al., 2019). Furthermore, physical inactivity is currently considered the fourth risk factor for global mortality (WHO, 2010).
Monitoring population PA levels is only possible if there are reliable and valid PA assessment instruments (Armstrong & Bull, 2006). Subjective self-report methods, namely questionnaires, are among the most often used instruments in epidemiological studies (Sember et al., 2020), with the advantage of suitability for large samples of people and with low associated costs (Strath et al., 2013). Nevertheless, self-administered PA questionnaires can be cognitively difficult for respondents to complete (Janz, 2006), may induce social desirability bias (Strath et al., 2013), may use unfamiliar terms for gauging PA intensities (e.g.; moderate and vigorous), and may over or under-estimate patterns of PA (Sallis, 2010). To overcome these problems, accelerometers have been broadly used as an objective method of assessing the criterion validity of PA questionnaires (Sember et al., 2020; Skender et al., 2016).
Several PA questionnaires have been validated and frequently used (Strath et al., 2013) in different countries for public health monitoring and epidemiology research, including the International Physical Activity Questionnaire (IPAQ), with its long and short forms (IPAQ-LF; IPAQ-SF) (Craig et al., 2003). While the IPAQ-LF was created to assess PA domains, it has been criticized as too long and complex; the shorter IPAQ-SF focuses on PA generally, rather than specifying its various sub-domains (Armstrong & Bull, 2006; Craig et al., 2003). The gap between the long and short forms of the IPAQ prompted the development of another reliable, valid and standardized questionnaire, taking into account cultural context, socioeconomic and/or literacy levels of respondents, and country-specific types of PA (Armstrong & Bull, 2006; Bull et al., 2009; Sember et al., 2020). The WHO prepared the Global Physical Activity Questionnaire (GPAQ) as part of their STEPwise approach to surveilling risk factors for chronic diseases. The IPAQ improved upon the long and short versions of the IPAQ, since the GPAQ evaluates PA in multiple domains (work, moving between places and leisure activities) and includes an assessment of sedentary behavior (SB) (Armstrong & Bull, 2006; WHO, 2005, 2022). Though the GPAQ, version 2, (GPAQv2) has been applied in over 100 countries (WHO, 2020a) and widely used (Mengesha et al., 2019; Whiting et al., 2021; WHO, 2011), there has been no translation and validation of it for the European Portuguese population. In this study, we aimed to validate and analyze the psychometric properties of the GPAQv2 for the Portuguese adult population, by comparing it to both an objective (accelerometry) and subjective (IPAQ-LF) method.
Method
Study Design
This was a cross-sectional, observational, and prospective study, consisting of two phases: a qualitative phase in which we translated and adapted the GPAQv2, and a pre-test and quantitative phase in which we tested the translated/adapted instrument’s reliability and validity in a sample of Portuguese adults. In this second stage, we evaluated the PA level of all participants through two administrations of the GPAQv2 at two time points (M1 and M2), separated by seven consecutive days. We also compared the GPAQv2 Portuguese version with the respondents’ completion of the IPAQ-LF and with ActiGraph wGT3X-BT accelerometer values. These two different correlates served as measures of concurrent and criterion validity, respectively.
Ethical Considerations
This study was authorized by the WHO, and the research protocol was approved, on 22 April 2022, by our local Ethics Committee (N.° 61/22). All participants were informed about the purpose of the study and provided written informed consent for the pilot test and qualitative and quantitative phases in person.
Sample Size
We conducted a power analysis (G*Power 3.1.9.7) to estimate a required sample size based on a previous study (Ács et al., 2020), in which investigators adapted and validated the GPAQv2 (by self-administration) for an apparently healthy Hungarian population and compared it with accelerometry and the IPAQ-LF. We assumed a Pearson’s linear correlation coefficient of 0.48 for our findings and assumed a statistical power of 80% and a statistical significance level of 5%. The minimum necessary number of individuals for the quantitative phase was 108 individuals, ensuring equal distribution between sexes.
Participants
We first recruited a sample of 118 adults from the local Faculty of Medicine between May 2022 and September 2022. Inclusion criteria were: (a) age between 18 and 60 years old, (b) both females and males, (c) Portuguese nationality and resident in mainland Portugal, (d) availability to participate in the two assessment time points, (e) able to read and understand Portuguese, and (f) willingness to sign informed consent. Exclusion criteria were: (a) any physical or cognitive deficits that would interfere with engaging in activities of daily living; (b) being pregnant; and (c) being an athlete (defined as individuals who were simultaneously training in sports to improve their performance, actively participating in sports competitions, and registered in a local, regional or national sport federation with sport training and competition as their major activity or focus of personal interest to which they devoted several hours on all of most days, exceeding the time they allocated to other types of professional or league activities (Araújo & Scharhag, 2016). While all recruited participants met these inclusion/exclusion criteria, our final sample contained 108 participants, due to some missing data as explained below (Supplemental Material 1).
Procedures
Qualitative Phase
We conducted the instrument translation phase of this research by following WHO recommendations (WHO, 2005). Two qualified professionals translated the original questionnaire from English to European Portuguese, and a PA expert performed a back-translation into English. Subsequently, two PA expert analyzed all versions created and any discrepancies between the translations were discussed and a consensus was reached unanimously. The new version of the GPAQv2 received a final revision from a European Portuguese language teacher.
We performed a pilot test on this finalized new version of the GPAQv2, by self-administration, in a sample of 32 participants, homogeneously distributed by sex and age groups (18–60 years old). These respondents reported no difficulties understanding the questions, with average ratings of 4.75 in the 5-points on a Likert scale.
Quantitative Phase
We explained the study protocol to participants and obtained their written informed consent, and we then asked them to complete both the GPAQv2 and IPAQ-LF digitally (via a link provided) and to wear an accelerometer for seven consecutive days. We collected their sociodemographic and anthropometric data through the provided link. At the end of the evaluation week, all participants were once again asked to complete both questionnaires and return the accelerometers to the research team. Participants received short message service reminders on the days they were scheduled to complete the questionnaires. A report of the results obtained was sent to each participant as a strategy for promoting PA and health literacy.
Physical Activity Outcome Measures
Global Physical Activity Questionnaire, Version 2 (GPAQv2)
The GPAQv2 consists of 16 questions that assess adults’ PA levels during a typical week. The questionnaire assesses three PA domains: (a) work, (b) travel to and from places. and (c) recreational activities and sedentary behavior (SB). The duration and frequency of PA and SB were evaluated in all domains in minutes/day. We used the GPAQ Analysis Guide (WHO, 2012) for scoring responses. We calculated the total MPA, VPA, MVPA and SB in minutes/week, and we converted the SB into hours/day, as this scale for this variable is easier to perceive and interpret for most people. Previous studies have also validated the GPAQv2 in other countries (Herrman et al., 2013; Keating et al., 2019).
International Physical Activity Questionnaire (IPAQ-LF)
We used the self-administered IPAQ-LF Portuguese version (Campaniço, 2016) as a subjective method of testing the concurrent validity of the GPAQv2. This questionnaire contains 31 questions and was designed to assess PA in a usual week in the following domains: work, commuting/transportation between locations, household chores, general maintenance and family care, leisure activities and SB. Consistent with the organization of the GPAQv2, MPA, VPA, MVPA and SB were calculated in minutes/week, and SB in hours/day. The data was cleaned and processed according to the guidelines outlined in the IPAQ-LF manual (International Physical Activity Questionnaire group, 2004). The IPAQ is one of the most used questionnaires for assessing PA and several studies have already examined its validity and reliability. (Cerin et al., 2012; Cleland et al., 2018; Ryan et al., 2018; Van Holle et al., 2015).
ActiGraph wGT3X-BT
We measured PA objectively with triaxial ActiGraph wGT3X-BT (AG; ActiGraph, Pensacola, FL, USA) accelerometers. All participants were instructed to wear the accelerometer around their right hip (via an elastic belt) in the extension of the mid-axillary line to the iliac crest. Participants were instructed to wear the accelerometer throughout the day, except during water-related activities and during their sleep. The accelerometers were set to a frequency of 100 Hz, storing all information in 10 second epochs. At least three valid days, including one weekend day, with a minimum of 600 minutes of utilization, were required for a participant’s accelerometer data to be included in subsequent data analysis. Accelerometer activation, downloading, and data processing were carried out using ActiLife Software version 6.13.4 (ActiGraph, Pensacola, FL, USA). Calculation of average time spent by participants in different types of PA intensity was carried out. We used the cut-off points by Troiano (Troiano et al., 2008) to distinguish PA intensity: sedentary (0–99 counts/min); light (100–2019 counts/min); moderate (2020–5998 counts/min) and vigorous (5999 counts/min). All variables were converted to time (minutes) per valid day.
Statistical Analysis
Our exploratory data analysis included the calculation of absolute frequencies and percentages for categorical variables; and we used means or Ms (and standard deviations or SDs) and medians (and interquartile ranges or IQRs as descriptors for numerical variables. We tested the normality of data distributions of continuous quantitative variables with the Kolmogorov-Smirnov test. Differences in the mean values of sociodemographic data between females and males were tested with the Student-t test for two independent samples or the Mann-Whitney U test for non-parametric data, as appropriate. We used the chi-square test for homogeneity for qualitative variables, or the Fisher’s Exact test or the Fisher-Freeman-Halton test when the chi-square test could not be applied. We tested the reliability of categorical and continuous variables with the Cohen’s Kappa coefficient (k) and Intraclass Correlation Coefficients test (ICC) - Model: Mixed two-factor; Type: Absolute agreement, respectively. The reliability ratings for k values were defined as: none (0–0.20), minimal (0.21–0.39), weak (0.40–0.59), moderate (0.60–0.79), strong (0.80–0.90) and almost perfect (>0.90) (McHugh, 2012). The ICC was categorized as: poor (<0.50), moderate (0.50–0.75), good (0.75–0.90) and excellent (>0.90) (Koo & Li, 2016). A reliability value of ≥0.70 was considered acceptable (Nunnally & Bernstein, 1994). Concurrent validity between questionnaires (GPAQv2 vs. IPAQ-LF) and criterion validity between GPAQv2-accelerometer were determined for all participants using the Spearman Correlation Coefficient (rho) with the following criteria: 0–0.2 = poor; 0.21–0.40 = fair; 0.41–0.60 = moderate; 0.61–0.80 substantial and 0.81–1.0 = near perfect (Bull et al., 2009). Agreement between the GPAQv2 and the accelerometer was assessed using Bland-Altman graphs, with the respective limits of agreement (Mean ±1.96 × SD) at 95% (Bland & Altman, 1986). We performed all statistical analyses with the Statistical Package for Social Science (SPSS), version 28. We set statistical significance at 5% (p < .05).
Results
Participant Characteristics
Participant Characteristics.
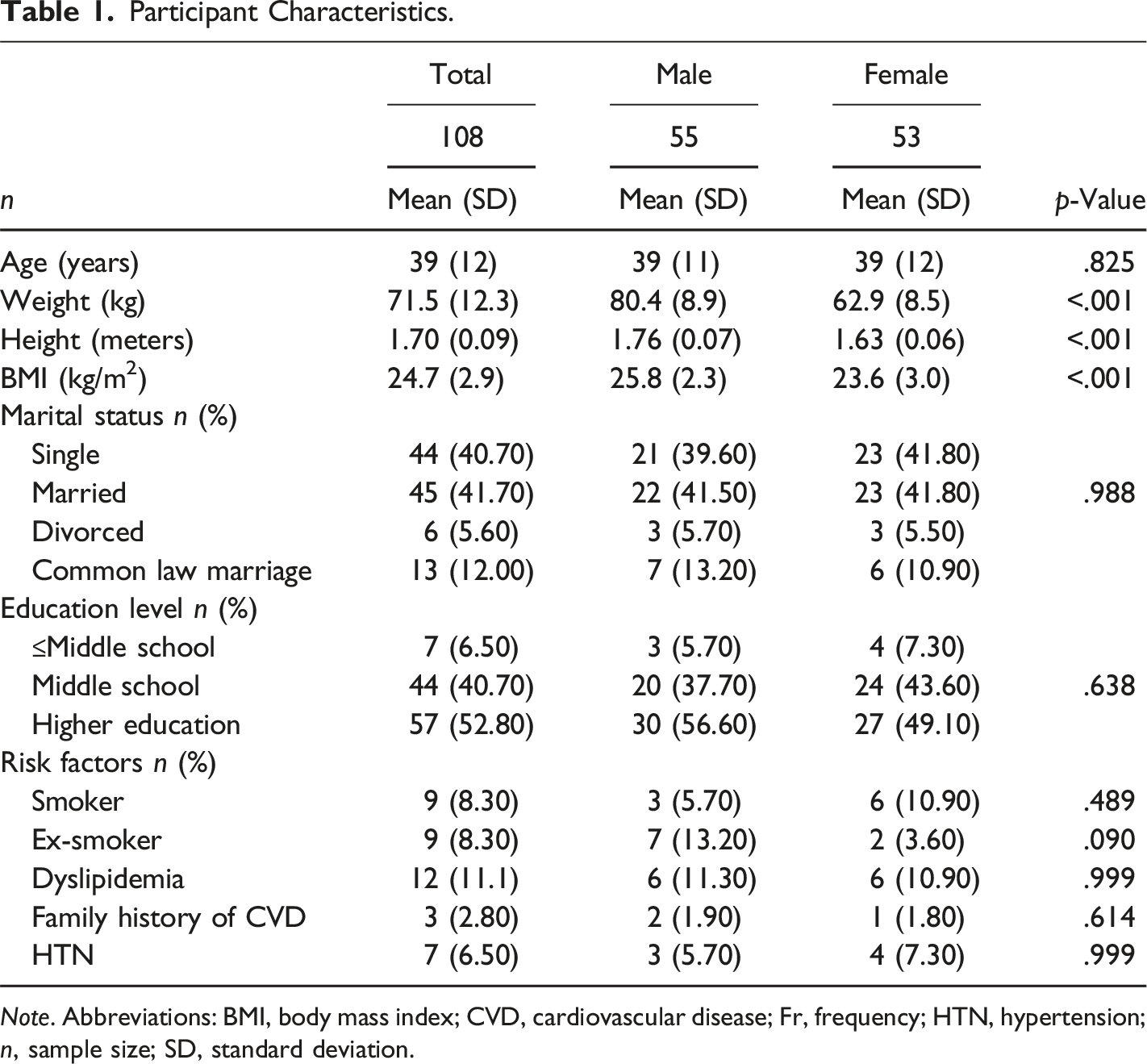
Note. Abbreviations: BMI, body mass index; CVD, cardiovascular disease; Fr, frequency; HTN, hypertension; n, sample size; SD, standard deviation.
Pattern of Physical Activity of the Sample According to Accelerometry, GPAQv2 and IPAQ-LF.
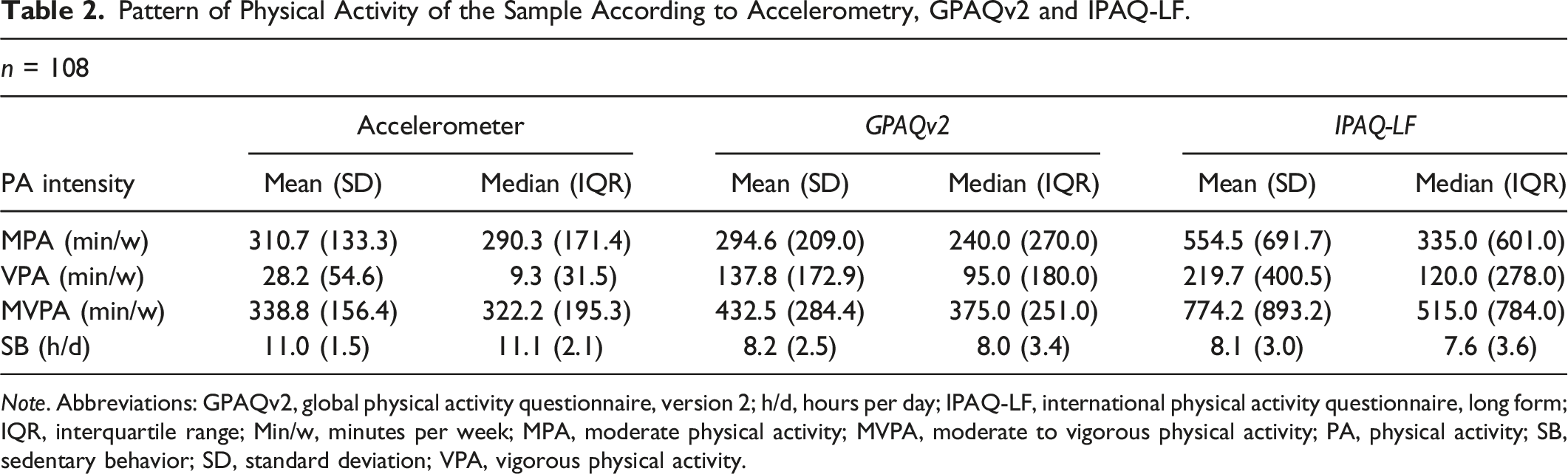
Note. Abbreviations: GPAQv2, global physical activity questionnaire, version 2; h/d, hours per day; IPAQ-LF, international physical activity questionnaire, long form; IQR, interquartile range; Min/w, minutes per week; MPA, moderate physical activity; MVPA, moderate to vigorous physical activity; PA, physical activity; SB, sedentary behavior; SD, standard deviation; VPA, vigorous physical activity.
Reliability
Test-Retest Results for the Kappa Reliability Value.
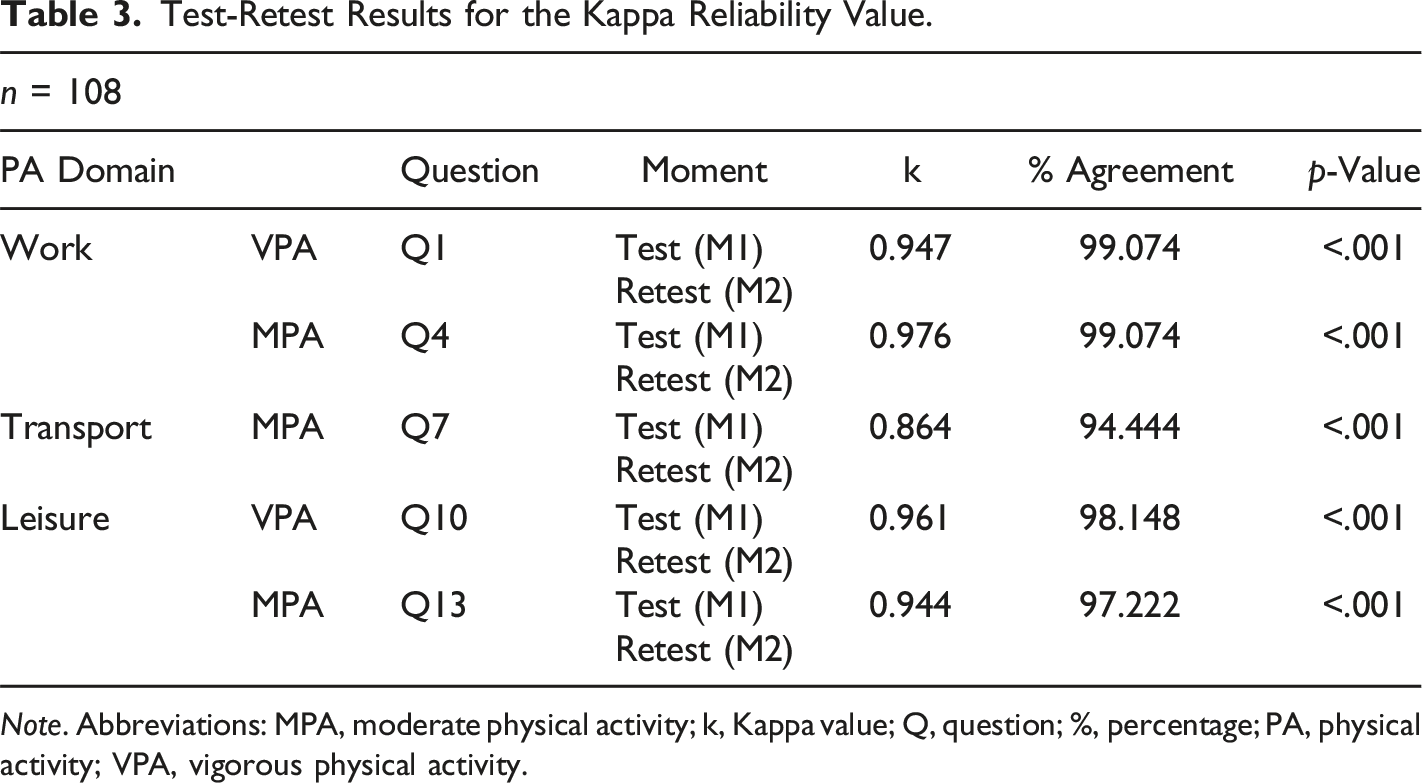
Note. Abbreviations: MPA, moderate physical activity; k, Kappa value; Q, question; %, percentage; PA, physical activity; VPA, vigorous physical activity.
Test-Retest Reliability Analysis with Intraclass Correlation Coefficients (ICCs).
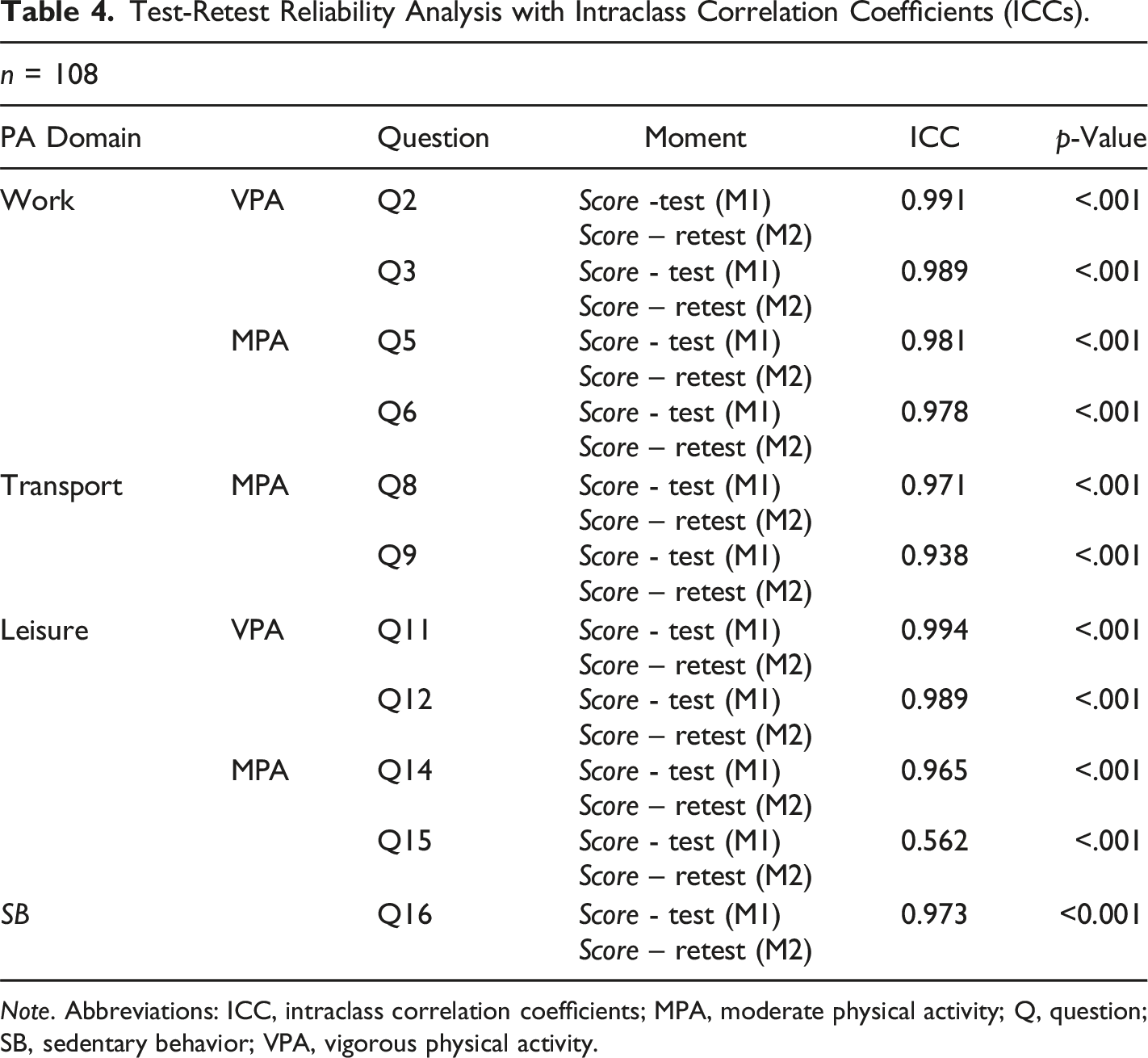
Note. Abbreviations: ICC, intraclass correlation coefficients; MPA, moderate physical activity; Q, question; SB, sedentary behavior; VPA, vigorous physical activity.
Concurrent and Criterion Validity
The criterion validity of the GPAQv2 was assessed against the accelerometer, while concurrent validity was tested against the IPAQ-LF (Supplemental Material 2). We found statistically significant differences for all PA levels and SB when comparing the results obtained from the three assessment instruments. The correlations between GPAQv2 and the accelerometer were positive and ranged from fair to substantial. The weakest association was verified for the SB, whereas the highest was for the MVPA. Comparing the GPAQv2 and IPAQ-LF, we found moderate to substantially positive correlations, where the highest association corresponded to MPA and the lowest to the SB.
Bland-Altman Analysis
Bland-Altman plots were used to measure the agreement between PA activity intensities assessed by GPAQv2 and the accelerometer records (Figures 1A–D). We observed significant bias between the two assessment instruments for all PA levels intensity and SB. Several outliers were identified, 6 for MPA, 8 VPA, 5 MVPA and 5 SB, with these data points falling outside the limits of agreement. For MPA, the mean bias between the two instruments was 16.05 minutes/week, with the range of variation from −327.91 to 295.80. This suggests that the GPAQv2 underestimated PA for this level of intensity. For VPA, the mean bias was 109.67 minutes/week, with a range of variation from −204.14 to 423.48, suggesting a tendency towards overestimation of GPAQv2 compared to the accelerometer. As for MVPA, the mean bias was 93.62 min/w, with a range of variation from −347.18 to 534.42. The greatest mean difference was observed for SB which was 172.67 min/w (−468.74; 123.41) or 2.88 h/d (−7.81; 2.06). These results confirm the GPAQv2’s tendency to underestimate this level of activity. Bland-Altman Plots of the Criterion Validity of the Global Physical Activity Questionnaire, Version 2.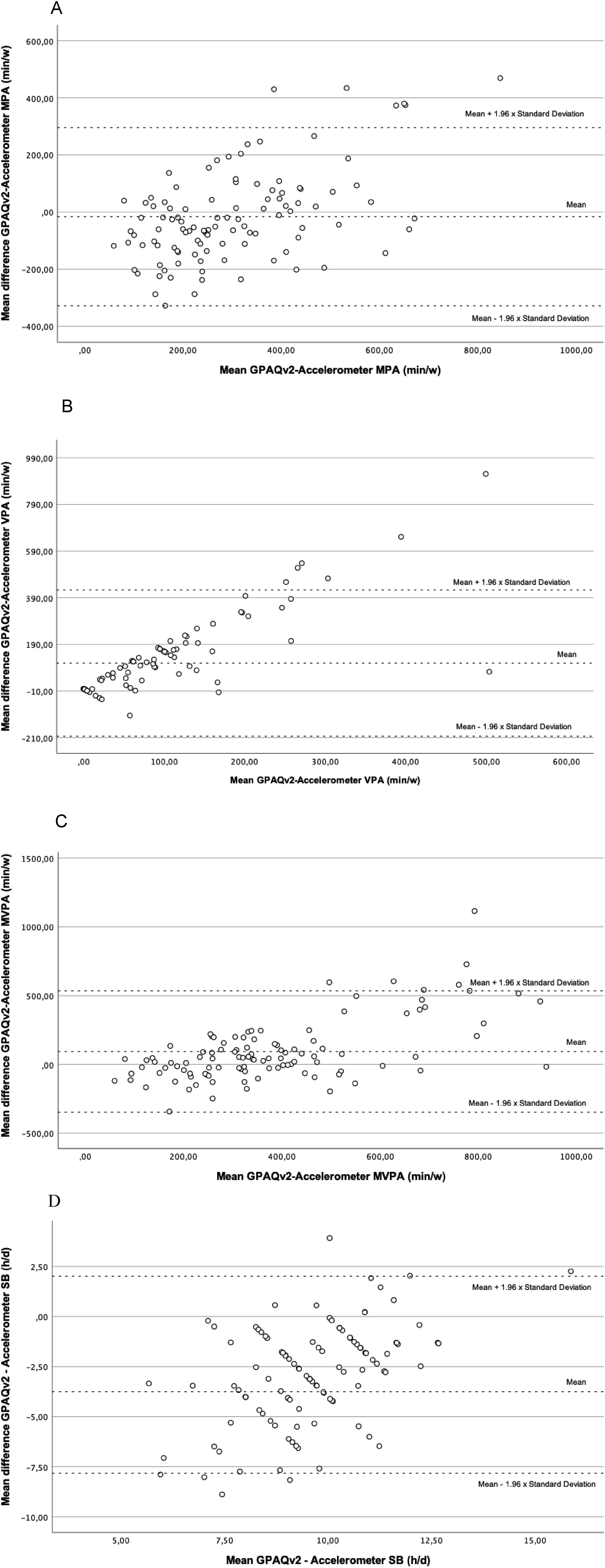
Discussion
In this study, we examined the reliability and validity of the self-administered GPAQv2 for assessing PA in Portuguese adults by comparing it with an accelerometer (objective method) and the self-administered IPAQ-LF (subjective method). The GPAQv2 showed acceptable and statistically significant reliability on test-retest correlations one week apart, with correlation values ranging from strong to almost perfect for k values, and moderate to excellent for the ICC. These values are consistent with those from other studies in different countries (Bull et al., 2009; Keating et al., 2019). For instance, Ács et al. (2020) reported an ICC: 0.899–0.987 in the adult Hungarian population, while Bull et al. (2009) found k values ranging from 0.67 to 0.73 across nine countries, with higher values in Shanghai. Rivière et al. (2018) reported poor to good reliability (ICC = 0.37–0.94; k = 0.50–0.62) in a French version of the GPAQ and Lee et al. (2020) found k values ranging from 0.30–0.67 and rho between 0.47–0.70, in Korea. Reliability results across studies may have oscillated due to several factors, including the wide age range of our target population (e.g., 15–79 years old) (Keating et al., 2019), cultural and socioeconomic differences between developed and developing countries (Bull et al., 2009; Keating et al., 2019), and variations in the participants’ education and health levels (Alkahtani, 2016; Bull et al., 2009; Mumu et al., 2017). In our study, 52.80% of the participants were highly educated. Similar findings were reported by Lee et al. (2011), who found that participants with higher education were less likely to overestimate their PA levels on the IPAQ-SF. We found the reliability of self-reported VPA to be highest for the work and leisure domains, likely because of the routine nature of work activities facilitated recall when completing the GPAQv2 (Adıgüzel et al., 2021). VPA in leisure activities, was also more reliably reported, as this intensity level is typically achieved through easier to recall structured recreational exercises (Chu et al., 2015; Meh et al., 2021). In contrast, activities such as moving between places or practicing MPA in daily life may be more challenging to accurately report (Chu et al., 2015).
Our concurrent validity findings showed moderate to substantial correlations between GPAQ-IPAQ PA intensity scores, closer to Revière et al. (2018) results (rho: 0.410–0.860) than Herrman et al. (2013) (rho: 0.260–0.630). These differences in results may be due to variations in the IPAQ form used (Rivière et al., 2018). The short form (IPAQ-SF), used in some studies, lacks the ability to differentiate PA by domains, whereas the IPAQ-LF and GPAQv2 assess PA by domains, which may facilitate participants’ recall (Armstrong & Bull, 2006; Meh et al., 2021). However, the IPAQ-LF has been criticized for being too long (Armstrong & Bull, 2006), potentially leading to PA overestimation. This highlights the importance of using the same questionnaire when comparing PA data across populations (Rivière et al., 2018). SB showed the strongest association between questionnaires, consistent with Bull et al. (2009) findings (rho = 0.650, p < .01) and Adıgüzel et al. (2021) findings (rho = 0.940, p < .001). A possible explanation for these similarities is that SB is similarly approached in both questionnaires (Adıgüzel et al., 2021). However, the single SB question in subjective PA assessments (GPAQv2 and IPAQ-SF) can lead to underestimation with these instruments (Meh et al., 2021), suggesting that the IPAQ-LF, with its two SB questions, distinguishing between weekdays and weekends may be favored for SB (Craig et al., 2003).
Our criterion validity findings showed that accelerometer-assessed sedentary time was significantly higher than self-reported SB in the GPAQv2. This is consistent with previous findings (Ács et al., 2020; Cleland et al., 2014; Lee et al., 2020; Meh et al., 2021). We found a significant correlation (rho = 0.226, p = .019) between these measures, falling within the range identified in a recent systematic review (rho: 0.007–0.47) (Keating et al., 2019), but our values were higher than that those reported by Cleland et al. (2014) (rho = 0.187, p = .135) (2014), Lee et al. (2020) (rho = 0.18, p < .01) (2020) and Ács et al. (2020) (rho = −0.007, p = .936). However, Meh et al. (2021) obtained a higher correlation (rho = 0.400, p £0.01), using a different brand of accelerometers.
In our Bland-Altman analysis, the agreement between the GPAQv2 and accelerometer data was consistent with findings from other studies (Ács et al., 2020; Keating et al., 2019). Ács et al. (2020) reported an overestimation for the VPA (212.75 minutes/week) and MVPA (104.93 minutes/week) and underestimated SB time measured by an accelerometer (6336.79 minutes/week), while Meh et al. (2021) overestimated MVPA (M = 64, SD = 143 minutes) and underestimated SB time by an average of 151 minutes/day (SD = 172 or about 2.5 hours/day), a value similar to our data with a Portuguese population (M = 172.67, SD = 151.06 minutes/day or 2.88 hours/day). Discrepancies may be due to differences in measurement methods, as the GPAQv2 only assesses PA lasting at least 10 consecutive minutes, while accelerometers measure all movement (Rivière et al., 2018). Study design factors, such as the particular week of accelerometer use, could also contribute to variability (Keating et al., 2019). Finally, individual differences in PA literacy and subjective interpretation of bodily sensations during PA could affect accuracy between measures, particularly for MVPA (Canning et al., 2014; Meh et al., 2021). The mean difference in reported PA obtained and represented in the Bland-Altman graphs confirmed an PA overestimation tendency of the subjective self-report methods (especially for VPA) and SB underestimation by these methods (Keating et al., 2019), compared with objective methods (Colley, 2018). Our study has several strengths. The GPAQv2 demonstrated acceptable reliability with correlation values ranging from strong to almost perfect for k values, and moderate to excellent for the ICC. Furthermore, the self-administered GPAQv2 allows for ease of use and widespread application without the need for trained interviewers. Our use of a sample with a high proportion of highly educated participants provided insights into how education levels can influence the accuracy of PA self-reports. Additionally, we adhered to the WHO’s standardized recommendations for validating the GPAQv2, adapting the example images to portray PA types (Bull et al., 2009) in the Portuguese cultural context.
Limitations and Directions for Future Research
This study is not without limitations. We opted for the self-administered version of the GPAQv2, noting that similar results have been obtained by these two methods in at least one prior study (Chu et al., 2015). Still, the original questionnaire was designed for use by a trained interviewer. Our participant sample was a convenience sample, and most participants were physically active, which may not be representative of the Portuguese population; latest reports concluded that 45% of adults in Portugal are physically inactive (OECD & WHO, 2023). The choice of our threshold upper age limit of 60 years of age was justified by a previous study (Wanner et al., 2017) that warned of a need for cautiously interpreting PA for people over 60 years old, due to low correlations of self-reported and actual PA found for this sub-group. However, our choice limits generalization of these data to older individuals. Another limitation presented was our lack of control over the environment when the questionnaire was completed, since environmental factors can influence the ability to respond and concentrate. Similarly, we did not consider the average completion time (Vilelas, 2020), which may be useful for future time management in applying the GPAQv2. As for PA assessment methodology the accelerometer is not effective in evaluating certain activities such as cycling, swimming, lifting weights, or movements performed mostly with the upper limbs (Warren et al., 2010), including some domestic tasks (Hoos et al., 2012). Finally, the criterion of “10 consecutive minutes” present in the GPAQv2 may have been a barrier in self-reported PA assessment, as the accelerometer always evaluated continuously rather than within this time interval. Troiano et al. (2020) considered removing this rule and one recent study accounted for every minute of PA (WHO, 2020b). Future investigators might update the GPAQv2, since the WHO mentioned that it would be subject to revision for possible adjustments and such adjustments have now been recommended (WHO, 2020b) regarding removing the rule of counting PA in intervals of 10 consecutive minutes. Additionally, we recommend including reports of muscle strengthening activities in the GPAQv2, as these activities are not present in any question (Meh et al., 2021), despite multiple health benefits associated with this practice. It would be interesting to validate the GPAQv2 in more countries and different cultural contexts, and future researchers might apply hetero-administration, through an interview. In this sense, our study validated another PA assessment instrument, which could positively contribute to the monitoring of public health in Portugal (or in portuguese-speaking countries) where physical inactivity has a high prevalence of 45% (OECD & WHO, 2023). Its application could enable the characterization of the PA levels across diferent domains within populations, consequently leading to the development of health promotion policies and PA programs.
Conclusion
In this study, we provide valuable evidence on the psychometric properties of the GPAQv2 in the Portuguese cultural context. Our results demonstrate acceptable reliability, moderate to substantial concurrent validity with the IPAQ-LF, and reasonable to substantial criterion validity with accelerometry. However, self-reported PA levels were higher for VPA and MVPA and lower for MPA and SB compared to accelerometry. Our validation and test-retest reliability data enables the use of GPAQv2 among Portuguese adults to study PA within the WHO’s STEPwise approach for the surveillance of chronic disease risk factors.
Supplemental Material
Supplemental Material - Reliability and Validity of the Global Physical Activity Questionnaire (GPAQ) for Portuguese Adults
Supplemental Material for Reliability and Validity of the Global Physical Activity Questionnaire (GPAQ) for Portuguese Adults by Mariana Ribeiro, Elisabete Fernandes, Mariana Borges, Madalena Pires, Xavier Melo, Fausto J. Pinto, Ana Abreu, and Rita Pinto in Perceptual and Motor Skills.
Footnotes
Acknowledgments
We would like to express our gratitude to the WHO for authorizing the translation process of the GPAQv2, and to all participants who contributed for this study. Special thanks go to Maria Isabel Barbosa, José Manuel Fiuza and Sérgio Carvalho for their support during the translation and cultural adaptation process of the GPAQv2.
Author Contributions
MR participated in the concept and design of the study, contributed to data collection and data statistical analysis, and drafting of the manuscript. EF contributed to data analysis and interpretation of results. MLP and MB participated in the design of the study and data collection. AA, FJP and XM participated in the design of the study and drafting of the manuscript. RP participated in the concept and design of the study, supervision and contributed to data collection. All authors contributed to the manuscript writing. All authors have read and approved the final version of the manuscript and agree with the order of presentation of the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.