
Abstract
Keywords
Background
Palliative care provides a comprehensive, patient-centered approach for individuals facing severe, chronic, or advanced illnesses where curative treatment is no longer viable (World Health Organization, 2020). The primary goal shifts from disease recovery to symptom relief and quality of life (QoL) enhancement for both patients and their families (Ferrell & Coyle, 2019). According to the World Health Organization, over 56.8 million people globally require palliative care annually, with 25.7 million in their final year of life. However, 78% of these patients reside in low- and middle-income countries, where access to integrated palliative services remains critically limited (World Health Organization, 2021).
Beyond managing physical symptoms, palliative care also addresses the psychological, emotional, and social dimensions of illness, recognizing the profound emotional burden experienced by both patients and their informal caregivers, such as family members or close friends (Nysaeter et al., 2024). Throughout this study, the term “caregiver” will be used exclusively to refer to these informal, unpaid care providers. The transition to palliative care represents a psychologically critical phase, as patients confront disease progression and caregivers assume increasing responsibilities. This shift is often accompanied by heightened emotional distress, which significantly impacts psychological well-being and adaptive coping in both patients and caregivers (Martí-García et al., 2023). While interdisciplinary support plays a crucial role, individual psychological factors—such as resilience, self-efficacy, and emotional expression—are essential in shaping the adaptation process (Cheng et al., 2023).
Resilience has been identified as a key protective factor in managing stress and promoting emotional adjustment. Research suggests that patients with higher resilience levels exhibit better pain management and greater psychological adaptability (Ristevska-Dimitrievska et al., 2015; Sihvola et al., 2023). For caregivers, resilience buffers against burnout and emotional exhaustion, thereby sustaining their ability to provide long-term care (Talamona, 2023; Yu et al., 2018). Similarly, self-efficacy—the belief in one’s ability to handle challenges—has been associated with lower stress levels and increased caregiver satisfaction, reducing helplessness and emotional strain (Fadei et al., 2024; Merluzzi et al., 2021). Emotional expression further modulates these processes, as greater expressivity is linked to better psychological well-being in both patients and caregivers (Haun et al., 2022). Conversely, difficulties in emotional communication are associated with increased distress and maladaptive coping (Cherry et al., 2017; Huda et al., 2022; Safavi et al., 2023). Caregivers with lower emotional expressivity frequently experience higher stress levels and diminished well-being, which may, in turn, impact the QoL of the patient (Eraslan et al., 2022; Ochoa et al., 2020).
Despite the well-documented importance of these psychological dimensions, several key knowledge gaps remain. While previous research has explored the role of resilience in caregivers, few studies have examined the bidirectional impact of resilience and self-efficacy between patients and caregivers (Li & Loke, 2013; Martí-García et al., 2023). Additionally, although gender differences in coping, emotional regulation, and grief processing have been well documented (Blum et al., 2024; Narayanan et al., 2025; Ullrich et al., 2019; Wong et al., 2013) it remains unclear how these differences specifically influence emotional expression and psychological adaptation within the palliative care context, particularly regarding resilience and self-efficacy in both patients and family caregivers.
Addressing these research gaps, the present study investigates the relationship between resilience and self-efficacy in palliative care patients and their caregivers, assessing how these psychological factors contribute to well-being and QoL during the transition to palliative care. Furthermore, the study examines gender differences in emotional expression and their impact on coping mechanisms. Additionally, we explore how different patient-caregiver relationships (e.g., spouses vs. parent-child) shape psychological adaptation.
This study explicitly examines the following research questions: (1) Is a higher level of resilience associated with reduced psychological distress among patients in palliative care? (2) How do resilience and self-efficacy interact in shaping psychological distress and caregiving burden among family caregivers? (3) Does resilience mediate the relationship between self-efficacy and caregiving burden in caregivers? (4) Are there gender differences in emotional expression among patients receiving palliative care? (5) Does the type of patient-caregiver relationship influence psychological distress and adaptation?
By identifying key psychological intervention targets, this research aims to enhance tailored support strategies, ultimately reducing distress and improving adaptation in palliative care settings.
Methods
Study Design
This cross-sectional observational study was conducted at Fondazione Policlinico Universitario A. Gemelli IRCCS, a tertiary care center specializing in oncology and palliative care. Data collection took place between June 2022 and October 2024.
Participants
A total of 160 patients receiving palliative care and 123 caregivers were recruited from the Specialized Palliative Care Unit utilizing a consecutive sampling approach. This non-probabilistic technique is widely employed in clinical research, as it systematically includes all eligible individuals who meet predefined inclusion criteria during the recruitment period, thereby minimizing selection bias in real-world settings (Etikan et al., 2016; Hulley et al., 2013). Considering the exploratory nature of this study and its primary objective, a formal sample size calculation was not conducted.
Inclusion criteria required that patients be ≥ 18 years old, diagnosed with a life-limiting condition requiring palliative care, not undergoing active curative treatment, and capable of providing informed consent. Primary caregivers were eligible if they were informal caregivers of an enrolled patient, ≥18 years old, and willing to participate.
Exclusion criteria for both groups included: severe psychological distress, significant cognitive impairment, or physical limitations preventing questionnaire completion. All participants provided written informed consent, and no cases were excluded due to missing data.
Procedure
Recruitment was conducted utilizing a consecutive sampling strategy to mitigate selection bias. Notably, some caregivers participated independently from their respective patients, thereby facilitating a more comprehensive data collection on caregiving burden and self-efficacy. Participants were provided with a detailed explanation of the study and signed an informed consent form. The assessment was conducted utilizing paper-based questionnaires, administered in person to both patients and caregivers. Patients completed the questionnaire either during their hospital stay (prior to transfer to hospice or discharge) or during scheduled outpatient appointments at the palliative care service. Similarly, caregivers were approached either during their relative’s hospitalization or during outpatient visits, and completed the questionnaire on-site under researcher supervision. The assessment comprised a total of 70 items, systematically organized according to standardized instruments. Likert-scale response formats were employed, ranging from 5 to 7 points depending on the specific measure used. Participation in the assessment was entirely voluntary, with participants retaining the right to withdraw at any point during the process. Data collection was anonymous, fully coded without personal identifiers, and securely stored on an institutional server accessible only to authorized research personnel. The estimated time to complete the questionnaire was approximately 30 minutes.
The study was conducted in accordance with the Declaration of Helsinki and received ethical approval from the relevant institutional Ethics Committee (Approval ID: 4776, Protocol No. 0012759/22, 12/04/2022).
Measures
Demographic Measures
Demographic and clinical data were collected for both patients and caregivers, including gender, age, marital status, education level, occupation, relationship with the patient, and patient disease status (first diagnosis vs. relapse). These variables were assessed to account for their potential impact on psychological adaptation.
Psychological Measures
Psychological adaptation was assessed using previously validated Italian versions of standardized psychometric instruments. No new instrument was developed for this study. All selected measures have demonstrated good validity and reliability in prior research, including within Italian populations (Allegranti et al., 1993; Callegari et al., 2016; Costantini et al., 2016; Sibilia et al., 1997).The General Self-Efficacy Scale (GSE) (Schwarzer & Jerusalem, 1995) is a 10-item Likert scale measuring confidence in one’s ability to handle challenging situations. The Integrated Palliative Care Outcome Scale (IPOS) (Bausewein et al., 2011) is a 17-item Likert scale designed to evaluate physical symptoms, emotional distress, and overall well-being in palliative care. The Toronto Alexithymia Scale (TAS-20) (Taylor et al., 1992) consists of 20 items assessing difficulty in identifying and expressing emotions, structured into three subscales: difficulty identifying feelings, difficulty describing feelings, and externally oriented thinking. The Resilience Scale-14 (RS-14) (Allegranti et al., 1993) includes 14 items measuring resilience-related factors such as perseverance, self-efficacy, and emotional regulation. The Caregiver Inventory (CGI-I) (Callegari et al., 2016) is a 9-item scale evaluating self-efficacy in caregiving tasks.
Data Analysis
All statistical analyses were conducted using Jamovi (version 2024), with significance set at p ≤ .005. Descriptive statistics were used to summarize demographic and psychological characteristics. Pearson’s correlation coefficients were calculated to assess associations between resilience, self-efficacy, psychological distress, and caregiving burden. Independent t-tests were performed to examine gender differences in emotional processing using the Toronto Alexithymia Scale (TAS-20). One-way ANOVAs were conducted to evaluate variations in resilience (Resilience Scale-14, RS-14) across categorical variables, including caregiver-patient relationship and employment status. Multiple linear regression models were used to identify predictors of psychological distress (IPOS) in patients and caregiving burden (CGI-I) in caregivers. Potential confounders such as age, gender, and caregiver-patient relationship were adjusted for in multivariate models. A mediation analysis was conducted to examine whether resilience mediated the relationship between self-efficacy and caregiving burden, using a bootstrapping approach with 5000 iterations. Mediation effects were considered significant if the 95% confidence interval did not include zero.
Bias and Methodological Considerations
To minimize selection bias, a consecutive sampling method was used, ensuring that all eligible patients and caregivers available during the study period were included. Measurement bias was reduced by employing validated psychometric instruments. To control for potential confounding effects, multivariate regression analyses adjusted for key variables such as age, gender, and caregiver-patient relationship.
Results
Descriptive Statistics
Demographic and Characteristics of Patients and Caregivers.
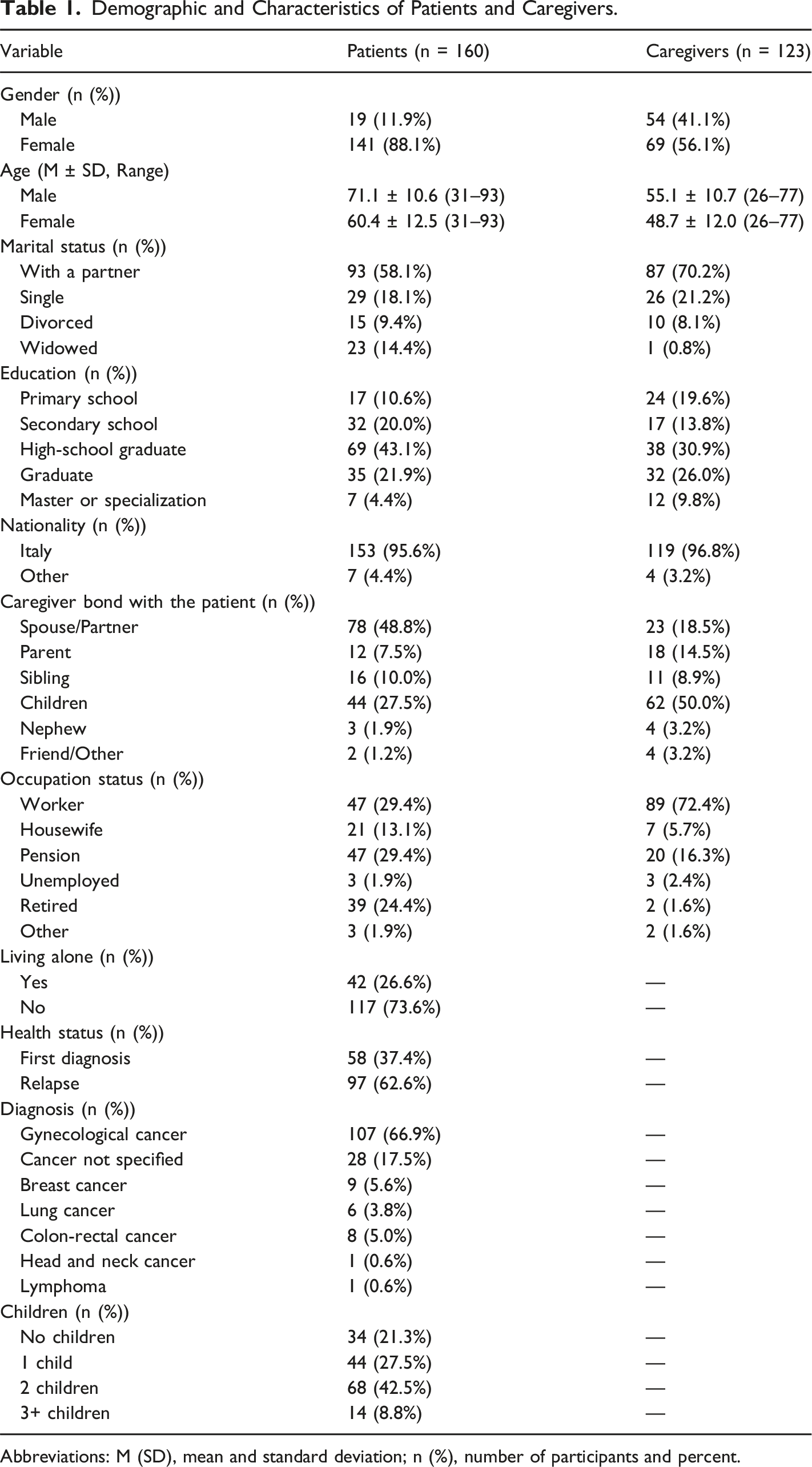
Abbreviations: M (SD), mean and standard deviation; n (%), number of participants and percent.
Descriptive Statistics of Psychological Scales.
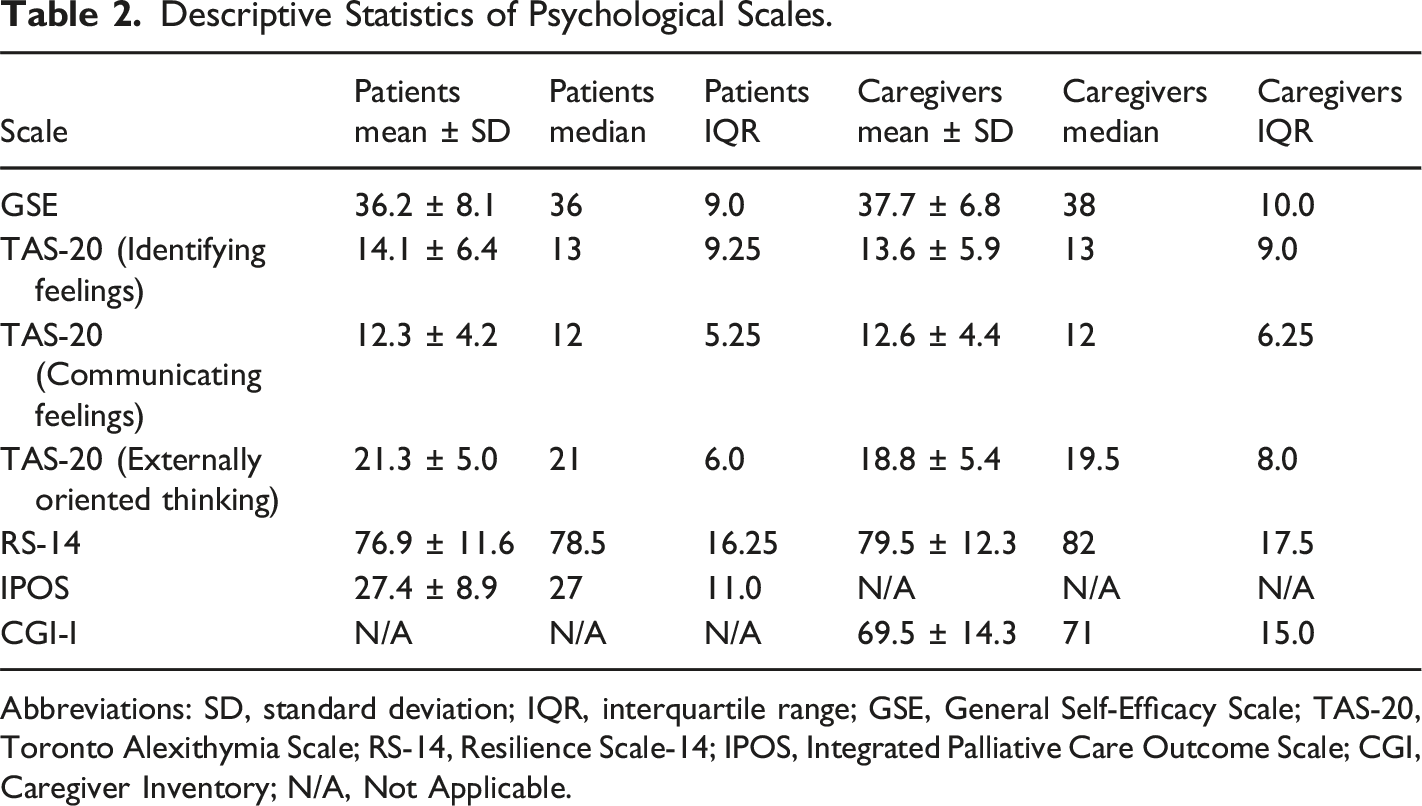
Abbreviations: SD, standard deviation; IQR, interquartile range; GSE, General Self-Efficacy Scale; TAS-20, Toronto Alexithymia Scale; RS-14, Resilience Scale-14; IPOS, Integrated Palliative Care Outcome Scale; CGI, Caregiver Inventory; N/A, Not Applicable.
Patient Outcomes
Correlations and Group Differences
Comprehensive Summary of all Patient Outcome Analyses.
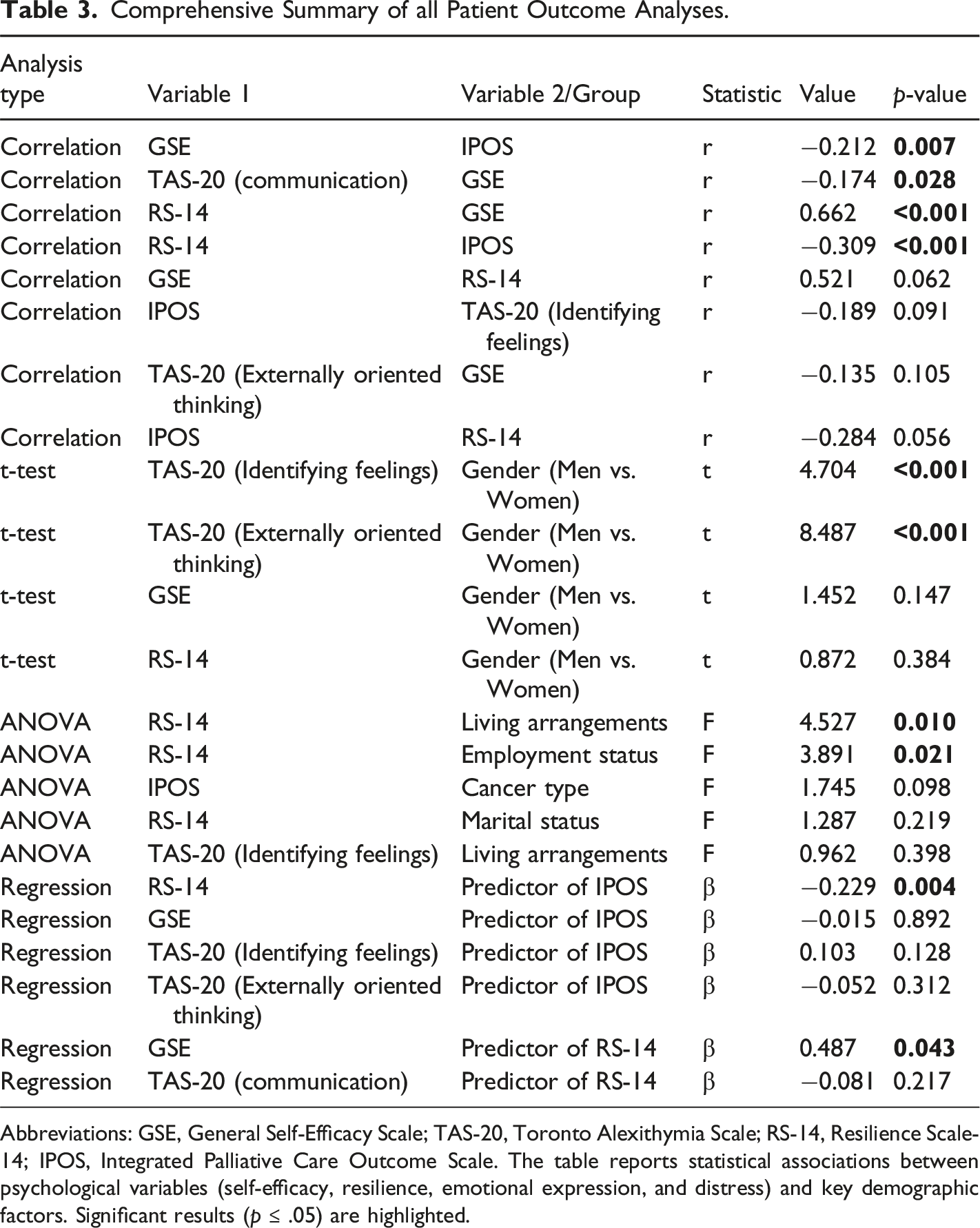
Abbreviations: GSE, General Self-Efficacy Scale; TAS-20, Toronto Alexithymia Scale; RS-14, Resilience Scale-14; IPOS, Integrated Palliative Care Outcome Scale. The table reports statistical associations between psychological variables (self-efficacy, resilience, emotional expression, and distress) and key demographic factors. Significant results (p ≤ .05) are highlighted.
Gender Differences in Emotional Expression
An independent t-test revealed significant gender differences in emotional processing. Male patients exhibited greater difficulty in identifying emotions (TAS-20, M = 20.3) compared to female patients (M = 13.3) (t = 4.704; p < .001). Additionally, men scored significantly higher on externally oriented thinking (TAS-20, M = 28.8 vs. M = 20.3) (t = 8.487; p < .001), suggesting a reduced tendency to engage in emotional elaboration.
Group Differences in Resilience
A one-way ANOVA indicated that resilience (RS-14) significantly varied based on living arrangements (F = 4.527, p = .010). Patients living with their parents had the highest resilience scores (M = 89.2), whereas those in assisted living or non-family households exhibited the lowest scores (M = 66.5). Employment status also influenced resilience (F = 3.891, p = .021), with retired individuals reporting the highest resilience levels (M = 78.2) and unemployed patients demonstrating lower scores (M = 70.3). A full summary of resilience differences is provided in Table 3.
Predictors of Psychological Distress
A multiple linear regression analysis examined psychological factors influencing distress (IPOS) in patients. The overall model significantly predicted distress (F (2,157) = 8.274; p = .004), explaining 9.5% of the variance (R 2 = 0.095). Higher resilience (RS-14) emerged as a significant predictor of lower distress (β = −0.229, p = .004), whereas self-efficacy (GSE) did not significantly predict distress levels (β = −0.015, p = .892). A comprehensive overview of patient outcomes is provided in Table 3.
Impact of Caregiver Type on Psychological Distress
A linear regression model assessed whether caregiver type, patient age, and gender influenced psychological distress (IPOS). Caregiver type was negatively associated with distress (β = −0.731; p = .066), though this result did not reach statistical significance. Patient age was not a significant predictor (β = 0.028; p = .646). Gender exhibited a trend toward significance (β = 3.721; p = .098), suggesting potential gender differences in distress levels.
Caregiver Outcomes
Correlations and Group Differences
Comprehensive Summary of all Caregiver Outcome Analyses.
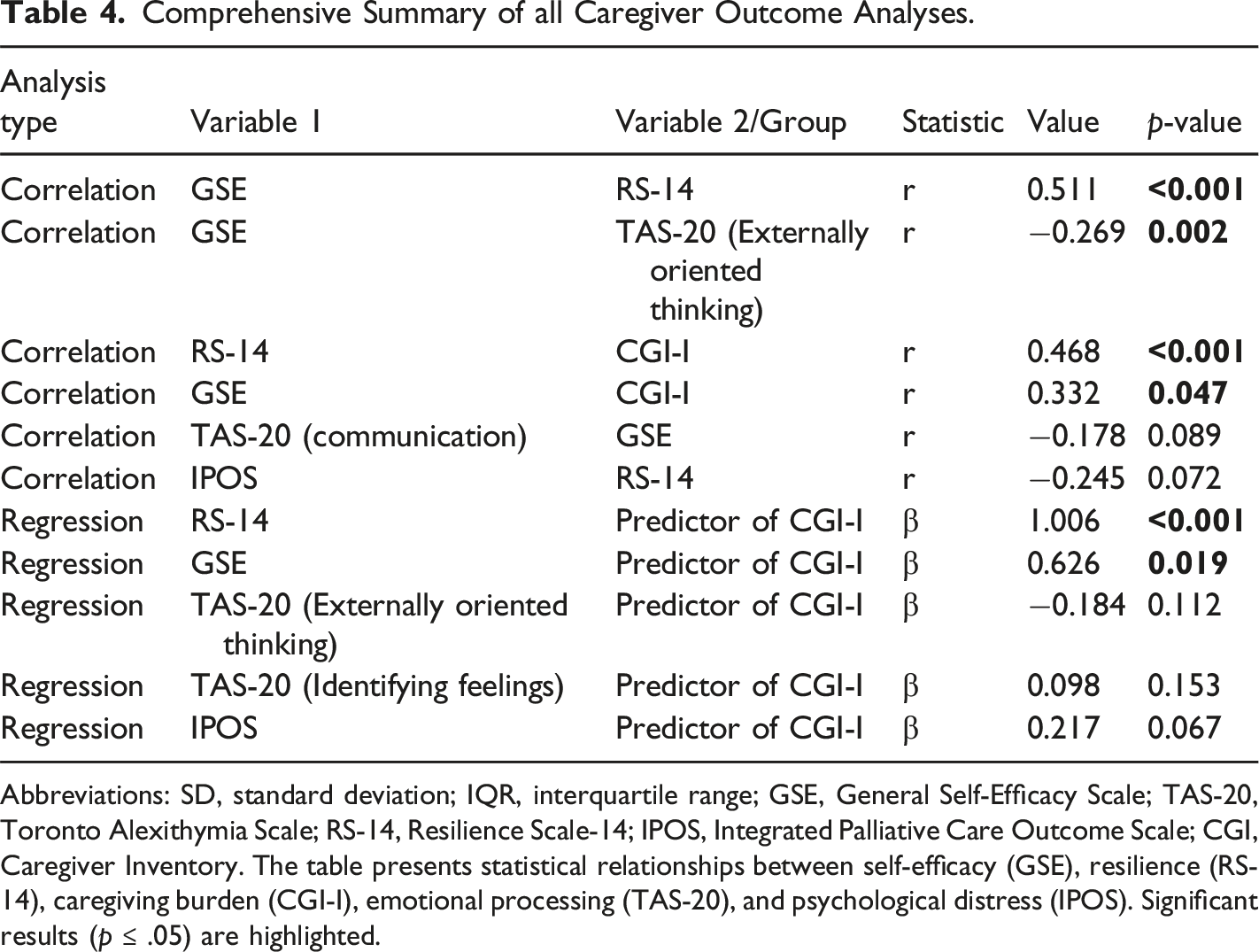
Abbreviations: SD, standard deviation; IQR, interquartile range; GSE, General Self-Efficacy Scale; TAS-20, Toronto Alexithymia Scale; RS-14, Resilience Scale-14; IPOS, Integrated Palliative Care Outcome Scale; CGI, Caregiver Inventory. The table presents statistical relationships between self-efficacy (GSE), resilience (RS-14), caregiving burden (CGI-I), emotional processing (TAS-20), and psychological distress (IPOS). Significant results (p ≤ .05) are highlighted.
Predictors of Caregiving Burden
A multiple linear regression analysis examined the role of resilience and self-efficacy in predicting caregiving burden (CGI-I). The model was highly significant (F(2,121) = 47.64; p < .001), explaining 44.1% of the variance (R 2 = 0.441). Contrary to expectations, resilience was positively correlated with caregiving burden (β = 1.006; p < .001), suggesting that while resilience may be beneficial, it does not necessarily alleviate the stress associated with caregiving. Additionally, higher self-efficacy was associated with greater caregiving burden (β = 0.626; p = .019), indicating that caregivers with a stronger belief in their capabilities might take on increased responsibilities, thereby intensifying their perceived burden. A detailed analysis is presented in Table 4.
Mediation Analysis: the Role of Resilience in the Relationship Between Self-Efficacy and Caregiving Burden
Mediation Analysis: Resilience as a Mediator Between Self-Efficacy and Caregiving Burden.
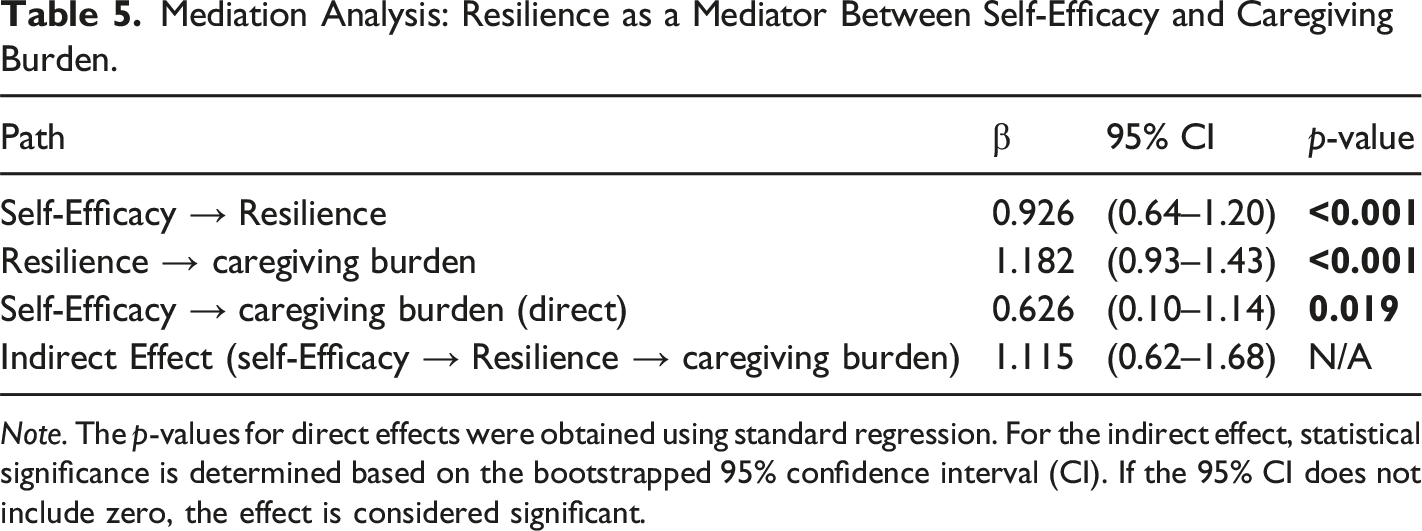
Note. The p-values for direct effects were obtained using standard regression. For the indirect effect, statistical significance is determined based on the bootstrapped 95% confidence interval (CI). If the 95% CI does not include zero, the effect is considered significant.
Discussion
This study explored the interplay among resilience, self-efficacy, psychological distress, and caregiving burden within the context of palliative care patients and their caregivers. Additionally, it examined gender differences in emotional processing and the role of the patient-caregiver relationship in psychological adaptation. Together, these findings provide valuable insights into the psychosocial mechanisms that shape the experiences of both patients and caregivers, offering a foundation for targeted clinical interventions.
A key finding of this study is the strong positive correlation between self-efficacy and resilience in both patients and caregivers, aligning with prior research (Chen et al., 2022). While self-efficacy contributes to psychological adaptability, it did not independently predict lower distress levels in patients. This suggests that additional psychological resources —particularly resilience— are necessary to mitigate distress effectively (Er & Erkan, 2023; Rodríguez-Prat et al., 2022). Conversely, resilience demonstrated a more direct protective effect against psychological distress, highlighting the need for interventions that specifically enhance resilience rather than focusing solely on self-efficacy.
Among caregivers, resilience exhibited a paradoxical association with increased caregiving burden. Although typically considered a buffer against stress, our findings showed that higher resilience was linked to greater perceived caregiving burden. Mediation analysis indicated that self-efficacy fosters resilience, which, in turn, correlates with a heightened caregiving burden. This suggests that resilient caregivers may assume more responsibility or emotional involvement, potentially intensifying their strain over time (Krug et al., 2016; Ullrich et al., 2024). These findings highlight the need to complement resilience-building programs with practical workload management strategies. Structured interventions focused on boundary-setting, stress regulation, and self-care could support caregivers in sustaining their resilience without leading to emotional exhaustion or burnout (Roth et al., 2015).
In addition to these intrapersonal factors, gender emerged as a relevant variable in emotional processing, particularly among male patients. Men exhibited greater difficulty in identifying and expressing emotions, as well as a higher tendency toward externally oriented thinking (Mendia et al., 2024). These characteristics may reduce their capacity to engage in adaptive coping strategies, increasing their vulnerability to psychological distress (Blum et al., 2024). Furthermore, difficulties in emotional expression may limit their ability to seek psychological support, further exacerbating their distress over time.
Given these patterns, interventions aimed at enhancing emotional awareness and structured communication skills could be particularly beneficial for male patients (Momenimovahed et al., 2021; Ozonder Unal & Ordu, 2023). Since men may be less inclined to seek traditional psychological support, tailored approaches should focus on improving emotional literacy through structured and accessible methods.
Contrary to expectations, the type of patient-caregiver relationship did not exhibit a statistically significant impact on psychological outcomes, including self-efficacy, resilience, distress, or burden. Although a trend suggested that caregiver type might influence patient distress, this effect was not statistically significant. These findings challenge the assumption that familial caregivers, particularly spouses, experience greater emotional strain compared to non-familial caregivers (Soto-Rubio et al., 2022).
Although no significant effect was detected, the observed trend underscores the potential for further investigation with larger sample sizes. It is plausible that variations in emotional closeness and caregiving dynamics, rather than the specific caregiver role, may influence psychological adaptation and distress levels. Future research should explore whether specific caregiving relationships, such as spousal or parent-child roles, impose distinct emotional and practical burdens that affect psychological well-being (Choi et al., 2024; Tan et al., 2021).
The strong association between resilience and lower psychological distress suggests that resilience-focused interventions, such as structured training programs and emotional regulation therapies, may be more effective than those centered solely on self-efficacy (Yu et al., 2023). Enhancing resilience through psychological interventions could provide both patients and caregivers with essential coping mechanisms to navigate the psychological challenges of palliative care. However, given the relationship between resilience and caregiving burden, interventions should be carefully structured to promote resilience while preventing excessive emotional strain. Caregiver support programs should integrate stress management techniques, structured caregiving responsibilities, and peer-support networks to mitigate the risk of burnout (Riffin et al., 2020). Encouraging self-care and establishing clear boundaries within caregiving roles could further enhance the effectiveness of these interventions.
In parallel with the need to support caregiver resilience, it is also crucial to consider gender-based differences in emotional processing.
Additionally, recognizing gender differences in emotional processing is crucial for optimizing psychological support in palliative care settings. Male patients, who often struggle with identifying and expressing emotions, may benefit from structured emotional literacy programs that facilitate self-expression and adaptive coping strategies (Dev et al., 2024). On the other hand, female patients, who tend to experience heightened emotional awareness, may require interventions that help manage emotional over-engagement and distress tolerance. A gender-sensitive approach in clinical practice could improve psychological well-being by tailoring interventions to the specific emotional and coping needs of different patient populations. By addressing these aspects, palliative care teams can develop more effective, evidence-based psychosocial interventions that enhance psychological adaptation, improve care experiences, and ultimately promote overall quality of life for both patients and caregivers.
Limitations and Future Directions
This study has certain limitations that should be acknowledged. The cross-sectional design prevents causal inferences regarding the relationships between resilience, self-efficacy, distress, and caregiving burden, making it difficult to determine how these psychological factors evolve over time. Future longitudinal studies could provide deeper insights into the long-term impact of resilience-enhancing interventions. Moreover, the sample predominantly included female patients with gynecological cancer, which may limit generalizability to other palliative care populations.
Expanding research to a more diverse range of diagnoses and demographic backgrounds would strengthen the applicability of these findings. Furthermore, unexamined factors such as caregiving duration and patient condition severity may influence psychological adaptation. Future studies should explore how these variables interact with resilience and self-efficacy to refine intervention strategies.
Conclusion
This study provides a comprehensive analysis of the interplay among resilience, self-efficacy, psychological distress, and caregiving burden in the palliative care context. While resilience emerged as a protective factor for patients, its paradoxical association with increased burden among caregivers underscores the complexity of their psychological adaptation. These findings emphasize the need for tailored interventions that enhance resilience while preventing emotional exhaustion in caregivers.
Additionally, the identification of gender disparities in emotional processing highlights the importance of implementing gender-sensitive psychological interventions to optimize coping strategies. Addressing these differences could lead to more effective and personalized psychosocial support for patients navigating palliative care.
From a clinical perspective, integrating resilience-building programs, structured caregiver support, and gender-specific psychological therapies may significantly improve overall quality of life. By applying these evidence-based approaches, palliative care teams can foster psychological resilience, reduce distress, and promote holistic well-being for both patients and caregivers.
Footnotes
Authors Note
This work is dedicated to the memory of Professor Giovanni Scambia, whose unwavering commitment to research, clinical excellence, and compassionate care has left an indelible mark on all of us. His visionary leadership and tireless dedication to advancing palliative care continue to inspire our work and guide our mission. We are deeply grateful for the privilege of having walked this path with him.
Acknowledgments
We sincerely thank the patients, caregivers, and all physicians and nurses of the Palliative Care Unit for their invaluable support and participation in this study.
Author Contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
The study adhered to the Declaration of Helsinki and received approval from the Ethical Committee of Fondazione Policlinico Universitario A. Gemelli IRCCS (Approval ID: 4776, Protocol N° 0012759/22, 12/04/2022). Written informed consent was obtained from all participants, who were enrolled voluntarily with the right to withdraw at any time. Data were fully anonymized, coded without personal identifiers, and securely stored on an institutional server accessible only to authorized researchers.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.