
Abstract
Programs providing end-of-life education require a standardized tool to identify knowledge gaps and evaluate programming. The aims of this mixed methods study was to examine the perceived clinical utility of the Death Literacy Index (DLI) in the Canadian context. An online survey and focus groups captured quantitative and qualitative data from end-of-life care stakeholders. The survey included the DLI and a measure of clinical utility. Participants rated the DLI positively on a 5-point Likert scale: acceptability (4.3), relevance (3.9), and usefulness (4.1). Qualitative findings supported these ratings and highlighted areas for improvement, including simpler language and more inclusive cultural and spiritual content. Ratings for usefulness reflected the index’s potential for initiating end-of-life discussions and program evaluation, though participants noted it may need more specificity to capture nuanced understandings of death literacy. Overall, the findings suggest the DLI requires further refinement and validation to enhance its applicability in the Canadian context.
Keywords
Introduction
Most Canadians prefer receiving end-of-life care at home, supported by home care and their families, to manage care in the community (Taylor & Quesnel-Vallée, 2017; Wilson et al., 2013). Discussions about death and end-of-life care are often avoided, resulting in fear and a lack of preparedness when it happens (Kastenbaum & Moreman, 2018; Rizvi et al., 2020). Increasing the public’s awareness and understanding of death, dying and end of life is essential for supporting individuals, families, and communities. Further, it can empower Canadians to make informed decisions, access resources, and receive the support they need within their communities to fulfill their final wishes. This knowledge is referred to as “death literacy” and is defined as “a set of knowledge and skills that make it possible to gain access to, understand, and act upon end-of-life and death care options” (Noonan et al., 2016, p. 32).
A better understanding of death literacy levels and knowledge gaps within communities, including among groups with specific needs, is essential for developing public health approaches to palliative care and community engagement. One such approach is the development of Compassionate Communities, which are initiatives that aim to build more resilient and supportive communities, with the hope of fostering greater comfort and capability in addressing issues related to death and dying (Abel et al., 2011). However, research on initiatives like Compassionate Communities is limited. Standardized evaluation tools could provide crucial information to inform interventions and community organizations, such as Compassionate Communities (Leonard et al., 2020; Noonan et al., 2016).
One such tool developed by researchers in Australia is the Death Literacy Index (DLI) (Leonard et al., 2022). This 29-item tool covers four dimensions of death literacy: factual knowledge, practical knowledge, experiential knowledge, and community knowledge (see Figure 1). Factual knowledge refers to an understanding of death-related policies, services, and planning. Practical knowledge involves hands-on skills gained by providing care and engaging in conversations about death and dying. Experiential knowledge is an awareness of one’s personal growth from death, dying, and end-of-life experiences. Community knowledge includes being aware of community support groups and community care. The DLI and its subscales, including experiential knowledge, practical knowledge (including hands-on support and talking support subscales), community knowledge (including community support groups and accessing help subscales), and factual knowledge.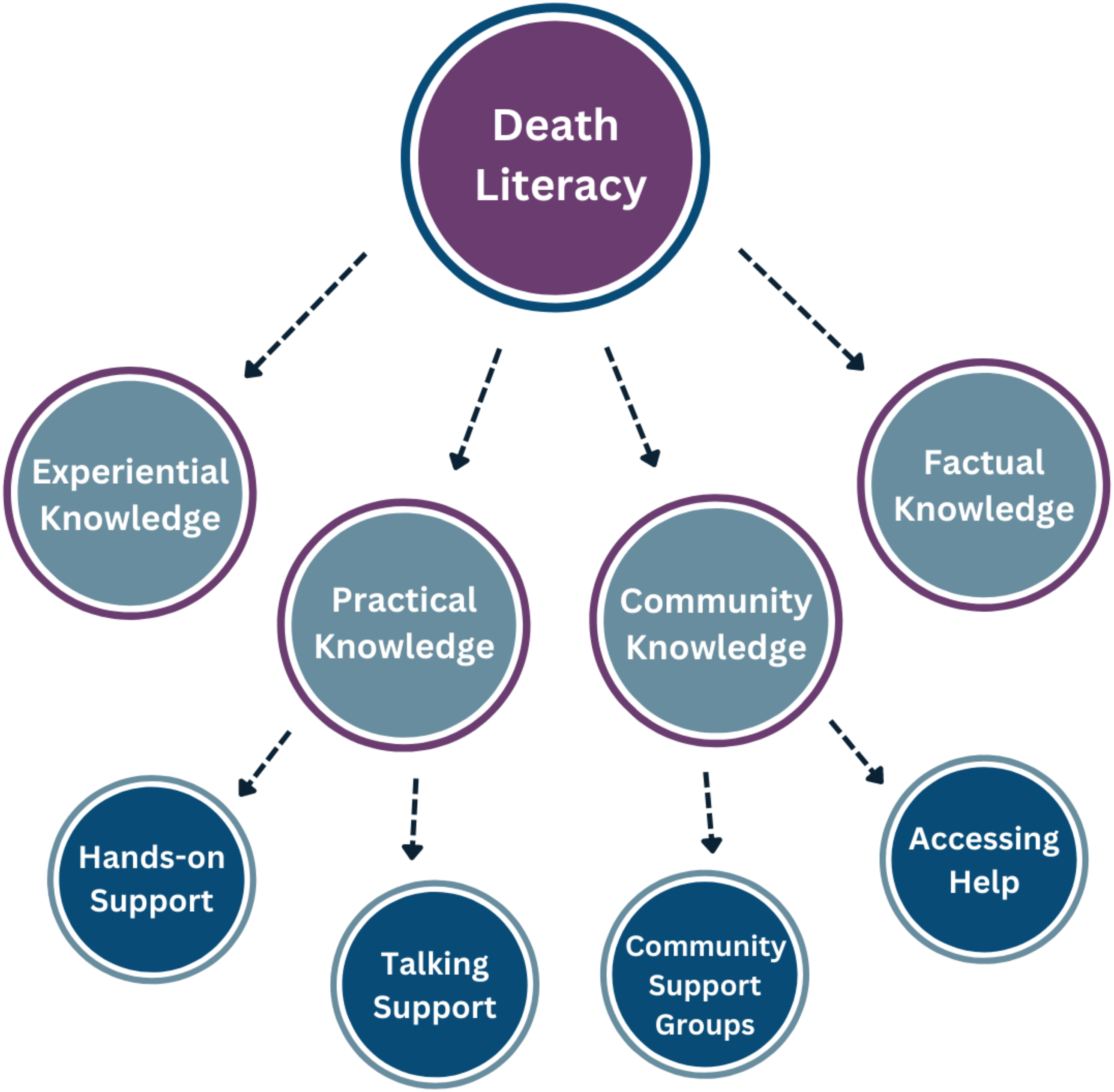
The index has shown significant construct validity when tested on the general Australian population and is predicted to be generalizable internationally (Leonard et al., 2022; Noonan et al., 2024). To date, the UK, Sweden, China, and Turkey have found the index to be valid and reliable in their respective contexts (Che et al., 2023; Graham-Wisener et al., 2022; Johansson et al., 2023; Semerci et al., 2022). While the validity is essential in ensuring the index measures what it intends to, another broader and important consideration is its clinical utility. This refers to the perceived usefulness, value, and applicability of a test, treatment, tool, or practice in real-world settings (Moorthie & Harris, 2021). Studies examining the DLI in various international contexts have indirectly explored aspects of clinical utility, which has prompted contextual adaptations to reflect the unique cultural and social needs of populations (Che et al., 2023; Graham-Wisener et al., 2022; Johansson et al., 2023; Semerci et al., 2022). The utility of the index is stated in establishing benchmark levels of death literacy, informing public health initiatives, and improving understanding of death literacy (Graham-Wisner et al., 2022; Noonan et al., 2024; Van Dinther et al., 2025).
To date, studies have not directly examined the clinical utility of the DLI, nor has the index been validated for use within the Canadian context. Based on Darzins and colleagues’ (2016) clinical utility criteria (Darzins et al., 2016), our objectives were to evaluate the perceived acceptability, content relevance and coverage, and overall usefulness of the DLI from the perspective of Canadian stakeholders with knowledge and experience in end-of-life care. Findings from our study will lay the groundwork for subsequent testing, adaptation, and broader validation efforts.
Methods
Study Design
We used a mixed-methods sequential explanatory design, which comprised two components: a cross-sectional online survey and focus groups to capture more detailed qualitative data from stakeholders with knowledge of death, dying, and end-of-life care. We completed the online survey first to inform the focus groups.
Component 1: Online Survey
We administered the online survey through SurveyMonkey. The survey featured three main sections: demographic questions, the DLI, and a clinical utility measure.
Demographic Questions
We collected demographic data from participants to describe our sample. Questions included age, gender identity, ethnocultural background, first language, and stakeholder role.
DLI
The DLI is a 29-item scale that includes four subscales. The subscales measure Factual knowledge (7 items), Practical knowledge (two subscales: Talking support, Hands-on care; 8 items total), Experiential knowledge (5 items), and Community knowledge (two subscales: Accessing help, Support groups; 9 items total). Each item on the four subscales is scored on a 5-point Likert scale. The practical knowledge subscales ask respondents to rate the difficulty or ease of tasks from 1 (“not at all able”) to 5 (“very able”). The Experiential knowledge and Factual knowledge subscales ask respondents how much each of the statements sound like them. Experiential knowledge is rated from 1 (“very untrue of me”) to 5 (“very true of me”) and Factual knowledge from 1 (“very untrue of me”) to 5 (“very true of me”). The two subscales within the Community knowledge subscale asks respondents to rate their level of agreement with the provided statements, which pertain to their knowledge of supportive individuals and groups in their community. This subscale is rated from 1 (“Strongly disagree”) to 5 (“strongly agree”). Mean scores are calculated for each of the four subscales by summing the items and then dividing by the number of items in the subscale. The means scores are then converted to a score between zero and 10, with higher scores representing higher levels of death literacy. We changed item 20 to “funeral home staff” “from” cemetery staff “to better reflect the Canadian context and their contributions in supporting people at the end of life and into bereavement.
Clinical Utility Measure
We developed a measure based on Darzins and colleagues’ (2016) clinical utility criteria to evaluate the clinical utility of the index. This measure focused specifically on acceptability, content relevance and coverage, and usefulness (Darzins et al., 2016). Acceptability refers to how well a tool is received by those for whom it is intended. It includes the time and effort required to complete it, language usage, and the appropriateness and accessibility of the content. Content relevance refers to how well the items within a tool correspond to central aspects of the subject of interest and coverage, or the extent to which important aspects are captured. In terms of the index, content relevance and coverage of death literacy. As death, dying, and EOL care are likely to be influenced by sociocultural factors (Koenig & Gates-Williams, 1995), we included the relevance of the content to diverse populations in our evaluation. A tool’s usefulness gauges the value of the information in terms of practical application and potential contributions to address the issue. For the index, this is the perceived value of the tool for evaluating and improving death literacy in Canada. We aimed to evaluate acceptability (6 items), content relevance and coverage (8 items), and usefulness (5 items) of the index. Our measure included a total of 19 items. Respondents rated on a 5-point scale, the extent to which they agreed or disagreed with each statement, from 1 “completely disagree” to 5 “completely agree”. We summed and divided the scores for each of the three clinical utility criteria by the number of items within each criterion. Higher scores indicate stronger agreement. We provided participants with space to submit answers to open-ended questions for more detailed feedback.
Sampling and Sample
We reasoned that, given the preliminary nature of the study, a first step in evaluating the clinical utility of the index was investigating opinions of Canadian stakeholders with relevant experience and knowledge of end-of-life matters. We sought perspectives of various stakeholders, including those living with a life-limiting illness, their family members, health and social care professionals, trainees, volunteers, and community organizations. Stakeholders had to be English speaking, and 18 years and over to be eligible to take part in the survey. Our sampling strategy was purposeful but one of convenience.
Recruitment, Survey Distribution, and Data Collection
We obtained research ethics approval from our affiliated organizations. To improve survey response rates, a recognized strategy was used that emphasized the relevance of the research, outlined the expectations of participants, minimized participant burden by limiting the length of the survey, and repeated contact reminders (Dillman et al., 2009). We distributed a recruitment email and flyer outlining the study through our professional networks. We carefully selected stakeholders with a broad range of perspectives. Our networks included a volunteer community organization that has volunteers with diverse experiences and backgrounds, a national palliative care nursing organization, and medical students from an Ontario university. Participants were encouraged to share the link with other stakeholders using a snowball sampling approach. Completion of the survey implied informed consent for our study. Respondents were given the option to enter a draw for one of three $50 gift cards as a gesture of appreciation following survey completion. We invited participants to an online focus group (component 2) to further discuss their perspectives.
Component 2: Online Focus Groups
Online focus groups were conducted to elucidate participants’ perspectives and insights. The sample comprised survey respondents who expressed an interest in taking part in the focus groups. Of the fourteen respondents who expressed an interest, eleven participated in one of two focus groups. We obtained verbal informed consent prior to the start of the focus groups. We developed open-ended questions based on the clinical utility criteria and informed by responses to the online survey (component 1), but with flexibility for participants to discuss matters that were important to them. Each focus group was conducted and recorded using a password-protected and encrypted Zoom account. Each focus group lasted approximately 1.5 hours and was facilitated by three members of the research team.
Plan of Analysis
After scoring of the measures, we calculated descriptive statistics for fixed response options to the online survey in terms of frequencies, means, and ranges using IBM SPSS version 29. Our primary aim was to examine responses on the clinical utility measure, but we also calculated the index scores to describe the level of death literacy in our sample. Cronbach’s alphas were calculated for the index subscales. We converted scores to percentages to make interpretation easier. We analyzed qualitative data from the open-ended short-answer responses to the online survey and the focus groups using qualitative content analysis. Coding was guided by, but not limited to, the clinical utility criteria using a deductive and inductive approach and organized into categories and subcategories. We conducted data triangulation in our analysis by integrating data from the two components of the study, enabling us to compare and contrast our findings on the clinical utility of the index.
Results
Characteristics of the Online survey respondents and Main Study Variables.
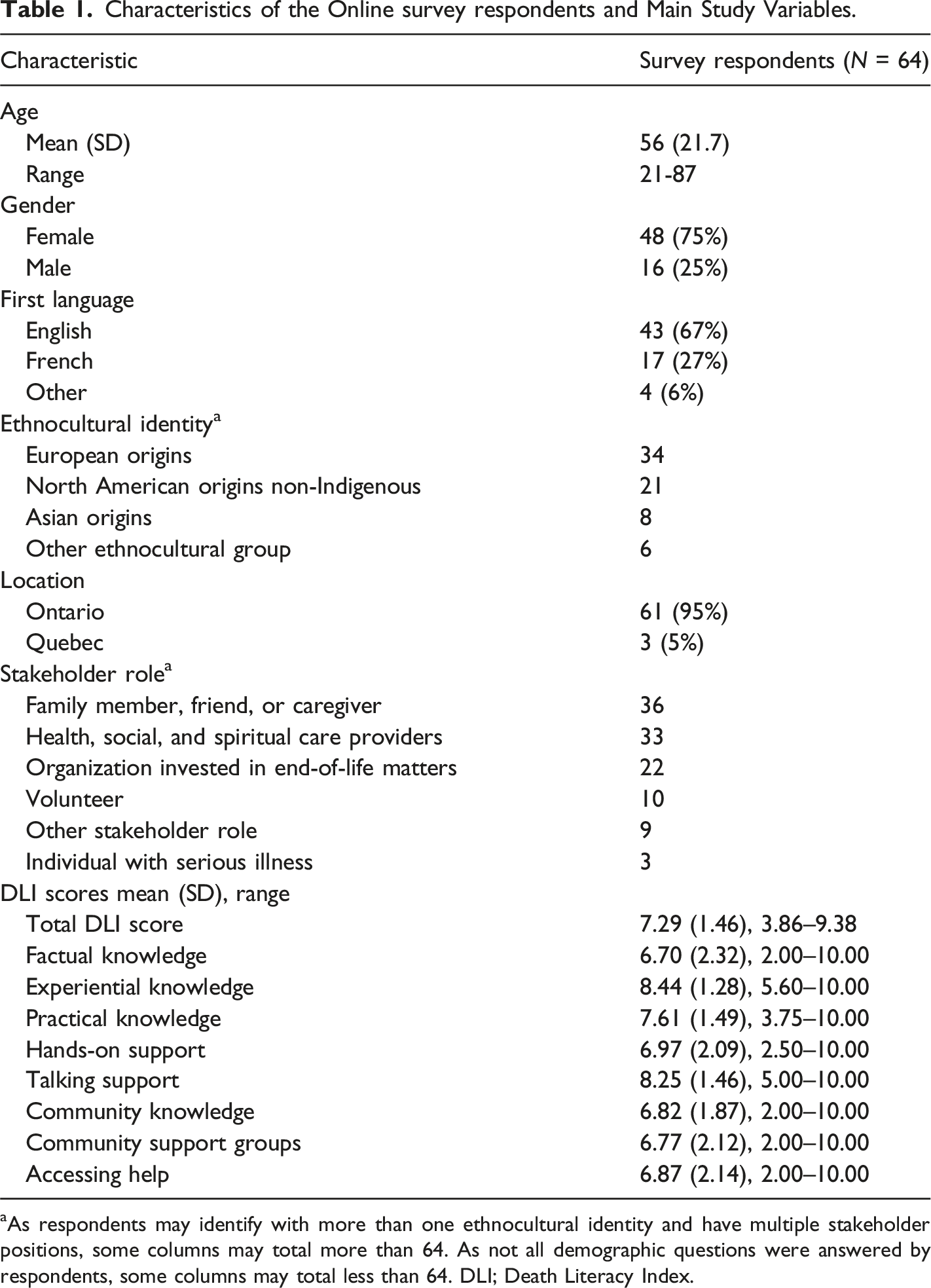
aAs respondents may identify with more than one ethnocultural identity and have multiple stakeholder positions, some columns may total more than 64. As not all demographic questions were answered by respondents, some columns may total less than 64. DLI; Death Literacy Index.
The focus groups comprised eleven of the survey respondents, with six females and five males. Eight out of eleven were over 60 and three being under 60. They were mostly English speakers (9/11) and of European descent (7/11). In describing our sample, we calculated their levels of death literacy (Table 1). The mean score for the entire index was 7.29. The highest-scored items included those from the Talking Support subscale, as well as the Experiential knowledge subscale. Lowest-scoring items originated from Accessing help, Hands-on care, and Factual knowledge subscales and pertained to the respondent’s ability to access culturally appropriate support, administer injections, and their knowledge of the law regarding dying at home. Cronbach’s alphas for subscales ranged from 0.755 to 0.933, indicating internal consistency.
Clinical Utility of the DLI
Frequency and Percentages of Agreement and Disagreement on the Clinical Utility Measure.
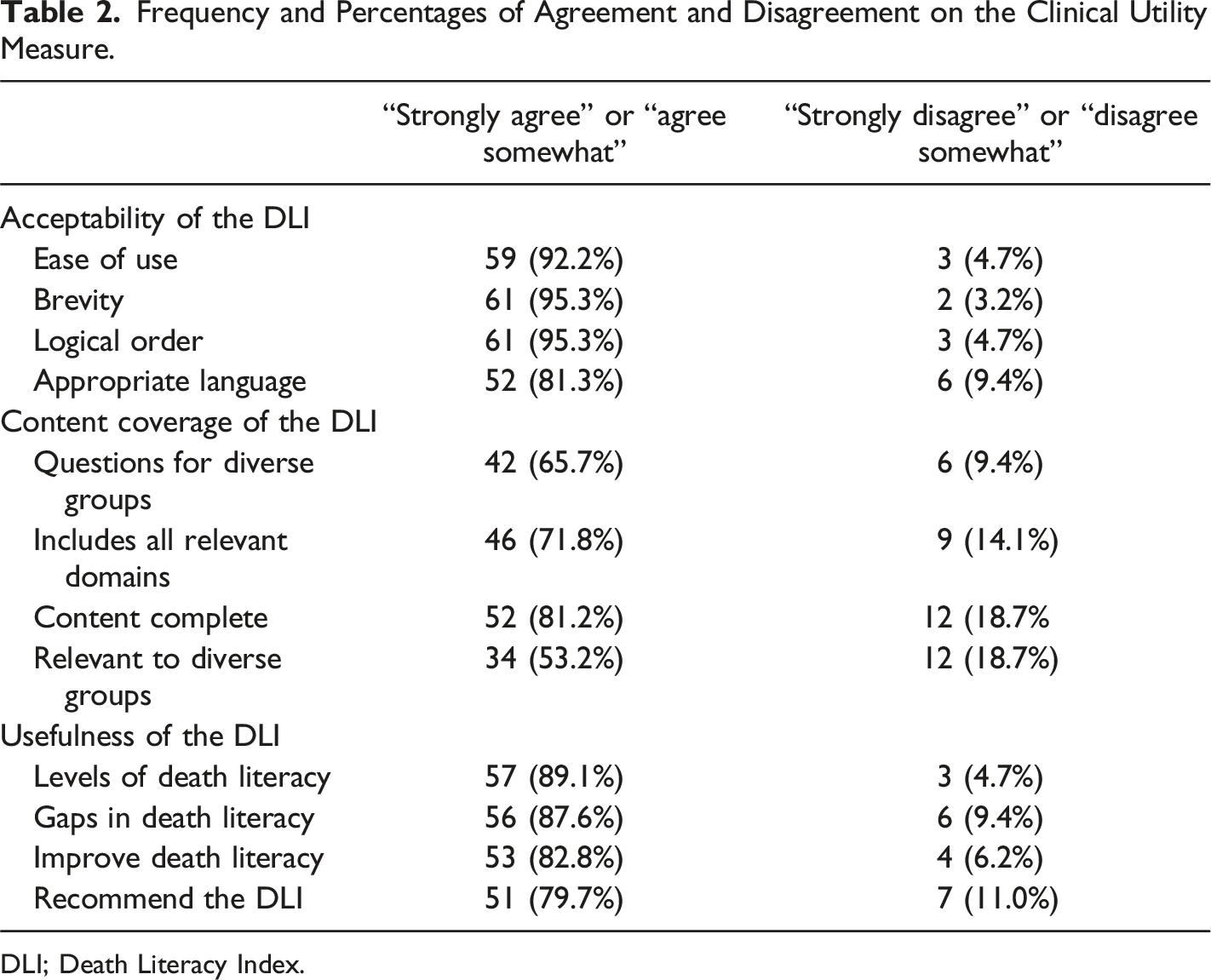
DLI; Death Literacy Index.
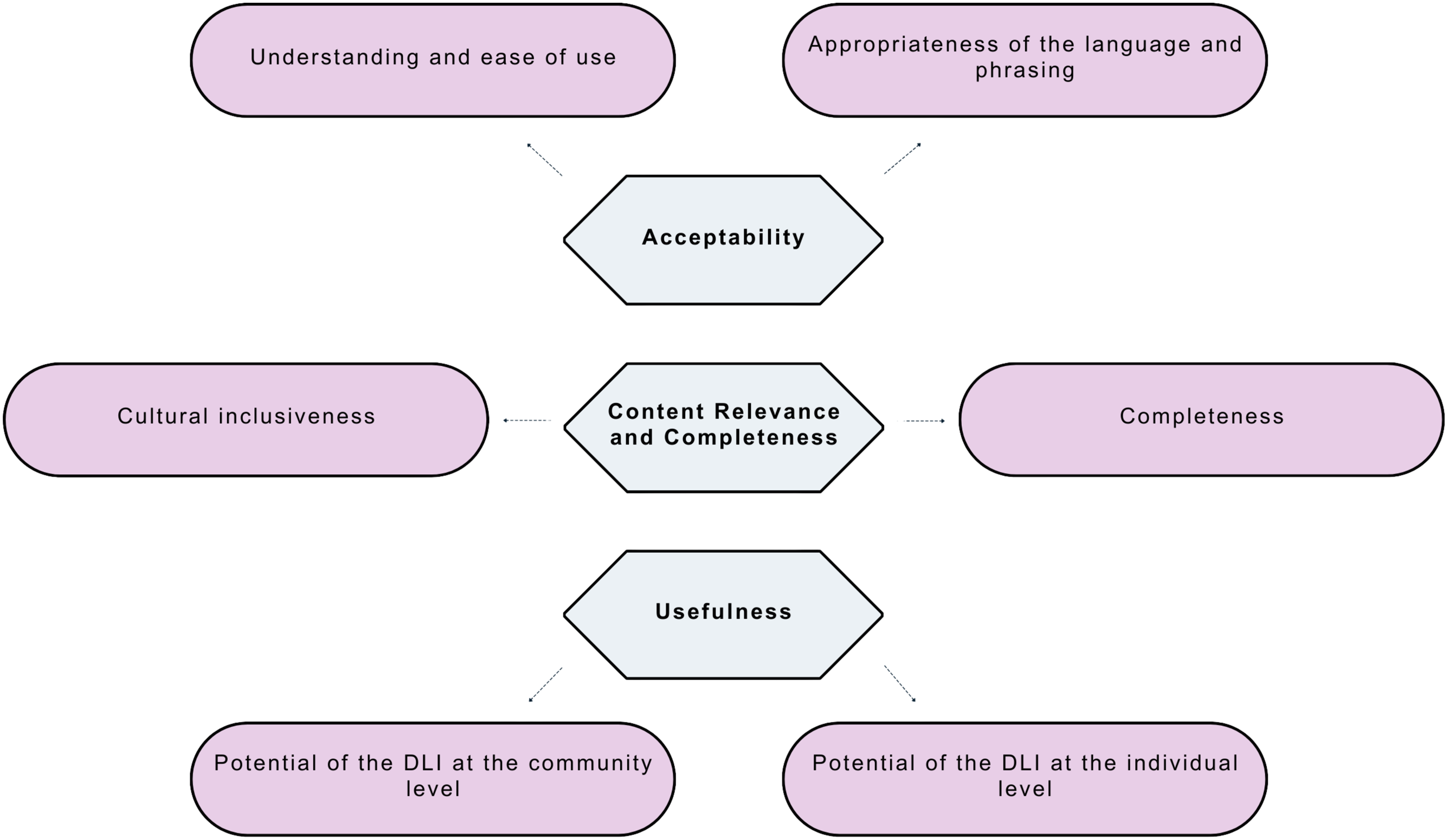
The three categories and subcategories from the qualitative data and quantitive data. The three categories are acceptability, content relevance and coverage, and usefulness. Acceptability has two subcategories: ease of use and format, and language and comprehension. Content relevance and coverage has two subcategories: content relevance and completeness and inclusivity. Usefulness has two subcategories: Reflections and conversations about death and dying, and assessment and evaluation.
Acceptability
Acceptability encompassed how well respondents received the tool, and opinions on time required to complete it, accessibility and appropriateness of content, and the language used. On average, scores on acceptability were higher than scores for the other clinical utility criteria (mean: 4.3, SD: 0.71, range: 4) (see table 2). We divided the category acceptability into two subcategories: ease of use and format, and language and comprehension.
Ease of Use and Format
As shown in Table 2, most respondents found the index easy to use, brief, logical in its order of items, and generally appropriate language usage. It took only 4 minutes and 4 seconds to complete on average (range of 1 minutes, 3 seconds to 18 minutes, 53 seconds). The qualitative data, where participants commented on how simple and clear the tool was to complete, supported these conclusions. The index’s brevity made it more acceptable because it required less effort to complete, though there was recognition that the index did contain “some pretty tough questions.” Participants also liked the structure of the tool: “I really like the four domains and the kind of structure that it gave, the series of questions it made.”
Language and Comprehension
The focus of this subcategory was the appropriateness of the language and terminology used in the index, including the response options and accessibility of the language to people from varied educational and cultural backgrounds within Canada. Responses concerning language and accessibility were generally positive: as shown in Table 2, 81.3% of survey respondents agreed that language was appropriate. Although reasonably high, this was just over 10.9% lower than respondents’ average score for “ease of use”, which was scored at 92.2%. Looking at the qualitative responses, there were concerns about the index’s reading level and accessible terminology. As one survey respondent remarked, “Some with different linguistic or cultural backgrounds may need an explanation of some terms, such as life-threatening illness.” This finding was identified in both the survey and focus groups, where participants felt there should be more background information for items in the tool, definitions, and simpler language. Question 19 on the Factual knowledge subscale asks if the respondent has “sufficient understanding of illness trajectories” to make treatment decisions. Participants felt that respondents might not fully understand the term “illness trajectories.” Participants also identified that some terms may need modification to better reflect the Canadian context. For example, the term “GP (general practitioner)” might be replaced by “family physician” or “nurse practitioner.” Moreover, participants believed the term “talking support” within the prompt for this subscale was unclear, and the wording of questions in the subscale was somewhat confusing. A significant area of debate in the focus groups concerned the appropriateness of the tool’s name. While some in the focus groups approved of the term “death” in the title and felt it represented the index, several respondents to the survey and focus group participants held the opinion that “death” should not be in the title. Added to this, some thought the name of the index was ambiguous. “The title is not understandable and too sophisticated for most. When I first heard the term [Death Literacy Index], I thought someone wanted to know what I had read about dying and death! … It should be simple: “What do you know about dying and death?”
Content Relevance and Coverage
The criteria with the lowest scores were the clinical utility measures of content relevance and coverage (mean: 3.9, SD: 0.87, range: 3.1) (see table 2). The content relevance of the index can be understood as: Are the items currently in the tool important to death literacy?, while coverage can be understood as: Are there aspects of death literacy that are missing but should be covered?. Given the overlap between content relevance and coverage, these criteria were combined into one subcategory. Further, as participants commented on the relevance and inclusivity of the index content for diverse cultural groups in Canada, the subcategory inclusivity was created.
Content Relevance and Completeness
Of all three categories, content relevance and completeness had the fewest number of participants indicating agreement with items on the clinical utility measure. The specific question within this category with the lowest agreement (53.2%), was the tool’s relevance to diverse groups. Though participants agreed (81.2%), that the content of the death literacy was, mostly, complete. Survey respondents and focus group participants identified areas missing from the index. They felt the Factual knowledge subscale was missing crucial questions on advance care planning, power of attorney (POA), wills, and other death, dying, and end-of-life-related documents. As the index was developed outside of Canada, knowledge of legalized medical assistance in dying (MAiD) as an end-of-life care option was missing, but thought to be a necessary consideration when evaluating Canadians’ death literacy levels. Further reflecting the Canadian context and the limited availability of family physicians, focus group participants recommended including “health care providers” on the Practical knowledge subscale instead of solely focusing on physicians, recognizing that not all Canadians have a family doctor. Acknowledging the importance of spirituality and spiritual care as an essential component of palliative and end-of-life care, participants also expressed the need for a dedicated section to assess spiritual care.
Another sizeable area of discussion related to the Practical knowledge subscale. Skills and knowledge related to the tasks and how to perform them (e.g., feeding, washing, and giving injections) as a measure of death literacy. Participants felt the skills required likely ranged depending on what level of care was required. Of note, they distinguished between knowledge and level of comfort in performing these tasks. One participant discussed his experience of caring for his mother at the end of life: “The comfort, versus the knowledge of doing hands-on care, are two different questions to me. The knowledge of how to do it, or feeling comfortable in doing it … But when it came to being able to feed her? That would have been difficult for me to do it; also bathing her or administrating injections, but lifting and moving her was an easy thing to do because I was strong enough to do it. And it was somehow different than if I had to dress her.”
Inclusivity
Though the content covered major areas relevant to death literacy, participants felt the broad focus of some items in the index was “not in depth enough to provide knowledge about culturally diverse communities.” There were also suggestions provided on how to improve inclusivity: “Potentially including information on specific rituals and views regarding death in different cultures could make the survey more comprehensive.” Another respondent echoed this, while also noting the importance of considering how LGBTQ2 + understand and navigate death and dying: “Cultural attitudes toward death differ - you might need more research into reaching racialized and LGBTQ2+ communities”. The feeling that the tool was not in depth enough for different groups overlapped with comments on the lack of content on spiritual care as a focus group member expressed: “it [DLI] needs more questions regarding spiritual beliefs as these are often linked to diverse groups or community knowledge.”
Usefulness
The category of usefulness had high levels of agreement, with 89.1% of survey respondents agreeing that the tool was useful in measuring levels of death literacy. The mean score of usefulness of the index was 4.1 (SD: 0.81, range: 4) (see Table 2 for agreement statistics).
Reflections and Conversations About Death and Dying
Participants appreciated the role the index could play in promoting reflection and discussion on end-of-life matters. They felt it could help people become more comfortable discussing death and dying with others. Also, for reflecting on their own beliefs and wishes as they relate to matters on life and death. “Even by asking the questions, it’s such an opportunity, like you just have no idea the ripple effect of even having just asked that question, how it can make a change, or get people thinking or future discussions.”
The potential of the index was exemplified in a quote from a medical student: “I think that this is a pretty important index to give to people throughout their lifetime, and I’d like people to have more conversations about it so that they don’t feel blindsided if someone were to be going through end of life, so they can mentally prepare for that before it happens.”
Given the potential of the index, one suggestion posed by focus group participants was to add a resource guide or appendix to the index within communities, so people could improve their death literacy and access the resources available to them. Relating to this quote on improving death literacy, 83% of participants showed agreement that the index has potential to improve death literacy. Another participant noted that the tool could be an impetus for discussion at the broader community level: “I think it would be a great conversation starter for [death cafés], because the whole purpose of death cafés is to get people more comfortable with talking about death.”
Assessment and Evaluation
There was some uncertainty regarding the usefulness of the tool in terms of an assessment of levels of death literacy. That is, what could be done with the information gathered from the tool, and how the knowledge gap in death, dying and end of life could be reduced based on the findings. There was concern that the information sought in the index was too general and was not useful for capturing diversity in experience and knowledge of death and dying. As one focus group member stated, “The questions are pretty broad so the information back wouldn’t have the nuances that give a clear picture of the level of knowledge.” Despite this, survey respondents and focus group participants agreed the index had potential. They suggested the index could be a baseline assessment of death literacy within community programs and as an evaluation tool to determine the effectiveness of programs. “I feel that the survey [DLI] is a good baseline data collection point to see at a basic level what respondents understand and have experience with related to death and dying. I feel it does not capture everything and would likely require a follow up evaluation (interview, focus group, etc.) to enrich that baseline data.”
Several participants suggested its use as a benchmarking tool for organizations: Compassionate Communities, faith communities, pastoral outreach teams, and churches. Also, as a tool for understanding training needs within organizations: “From an organizational perspective, I think it [DLI] would be a very interesting tool which would yield information, which would guide staff development and training in terms of how we understand death literacy. I see from an organizational perspective, it being very useful.”
Overall, 80% of participants agreed they would recommend the index as a measure of death literacy.
Discussion
Based on our examination of the perceived clinical utility of the DLI in the Canadian context, participants felt the DLI was acceptable but identified potential areas for improvement. Key suggestions included enhancing clarity and simplifying the language to make it more accessible. Participants also emphasized the need to improve the cultural and spiritual relevance of the index by including items that reflect Canada’s diverse population, as well as questions to better reflect matters related to death and dying within the Canadian social and legislative landscape. In terms of the usefulness of the DLI, participants were positive, identifying the potential of the index in efforts toward increasing death literacy by encouraging reflection on death and dying, and as a benchmarking tool for organizations to evaluate and enhance end-of-life programming. However, they also noted that, while the index provides a broad measure of death literacy, it may lack the sensitivity to capture contextual and cultural nuances, potentially limiting its overall usefulness.
As contextual factors shape clinical utility, it is not unexpected that terminology in the Australian-developed DLI requires modification for a specific population. Our finding regarding acceptability in terms of language and comprehension echo those found in other studies and have prompted the development of a revised full version of the DLI (DLI-R) and a shortened nine item version (DLI-9) (Noonan et al., 2024). Revisions were made to item and scale phrasing, as well as word choices, to improve clarity and accessibility. For example, items on the Talking support scale that participants in our study found unclear, were modified in the DLI-R (Noonan et al., 2024). Similarly, complex terminology such as “illness trajectories” was rephrased to “how illnesses progress to make decisions” (Noonan et al., 2024). One previously unreported observation regarding acceptability was the index’s title. Participants were divided on the use of the word “death” in the title. Some felt “death” in the title accurately reflected the tool’s content, while others felt discomfort, possible reflecting unease with matters concerning death and dying not uncommon within societies (Kastenbaum & Moreman, 2018).
While changes to terminology are relatively straightforward, cultural variations are more challenging to address. Validation studies support the structure and substructures of the DLI, adding to its cross-cultural generalizability (Noonan et al., 2024), but also draw attention to the importance of cultural and contextual factors, critical to content relevance and coverage. This has the has led to changes to the index in the UK, China, Sweden and Turkey, to better reflect their contexts (Che et al., 2023; Graham-Wisener et al., 2022; Johansson et al., 2023; Semerci et al., 2022). In China, for example, the index was changed to align with cultural taboos and practices (Che et al., 2023). Similar to the UK study by (Graham-Wisener et al., 2022), we replaced the term “cemetery staff” used in the original DLI and DLI-R with “funeral staff” to better reflect their roles. Interestingly, China’s index valuation includes both funeral and cemetery staff, reflecting the cultural practice of keeping cremated remains in shrines (Che et al., 2023). Given Canada’s multicultural population, including Indigenous Peoples (Berry, 2013; Srikanth, 2012), participants in our study questioned whether the index adequately reflects diverse understandings of death, which had a bearing on their perception of the index’s content relevance and ultimately its usefulness. Of note, was attention to spiritual aspects of death and dying, which participants felt were central to many people’s experiences of death and an integral part of an assessment of death literacy.
While we found the DLI captured many key elements of death literacy and was well-received, participants identified opportunities to enhance its relevance within the Canadian context. For example, it currently does not reflect Canada’s legal landscape around end-of-life care, including medical assistance in dying (MAiD), which shapes public understanding and experience (Government of Canada, 2024). To better align with the increasing importance of advance care planning within Canada (Canadian Hospice Palliative Care Association, 2020), participants also recommended enhancing the index by including knowledge of pertinent Canadian death-related documents. Further, modifications were to ensure the index fit with the structures that support Canadians with death, dying, and end-of-life care. In Canada, the shortage of family physicians (general practitioners; GPs) have created challenges with access and expanded the scope of practice for nurse practitioners (Canadian Institute for Health Information, 2023). Our findings suggest that “health professional” is a more suitable term than focusing solely on physicians. Accordingly, the DLI-R Talking Support subscale has changed its emphasis from GPs to “health professional” to address this concern (Noonan et al., 2024). Overall, these insights point to the index’s strong foundation and its potential for further refinement to enhance its cultural and contextual fit in Canada.
The index is a measure of knowledge and skills, and, as such, there is a focus on performing tasks such as bathing and feeding another person within the Hands-on support subscale. Participants emphasized the importance of supporting those providing care. An important distinction identified in our study, reflecting the relational nature of caring for someone, is between knowing what to do (“know how”) and having the physical ability, emotional and psychological comfort, and willingness to perform the task. While a care recipient’s level of functioning helps determine the intensity of care required, the caregiver’s own capacity is also a factor. Bathing a person with significant functional limitations is more demanding and requires greater skill than assisting someone with minimal needs to wash. For some caregivers, their own health may limit their ability to provide some types of hands-on support (Taylor & Quesnel-Vallée, 2017). While the relationship between the care recipient and caregiver, its nature, and social and cultural norms can influence caregiving (Berry, 2013). Based on participants’ feedback, a suggested revision would be to ask how comfortable a respondent is performing a particular task.
In evaluating the usefulness of the index, participants identified the potential of the DLI to determine levels of death literacy. Benchmarking levels of death literacy demonstrate the usefulness of the index for tracking changes within and across communities and over time (Noonan et al., 2024). For the stakeholders who took part in our study, the potential of the DLI lies in its ability to identify gaps in death literacy to inform educational and supportive interventions and to evaluate programs. However, research in this area is more limited. A recent mixed-methods study using the DLI and interviews with unpaid carers of palliative care patients in South Australia revealed how carers learn, talk, and share information about death and dying (Van Dinther et al., 2025). Comparing the carers’ lived experiences with levels of death literacy offered insights into factors influencing levels of death literacy and how this knowledge may or may not translate into action (Van Dinther et al., 2025). More research is required to fully evaluate the DLI as a tool for program development and evaluation.
Limitations
As a preliminary step in examining the clinical utility of the DLI in Canada, we sought the views of stakeholders with expertise in death, dying, and end-of-life care. Our sample was one of convenience and not intended to represent the Canadian population. As a result, levels of death literacy were higher than those observed in general population studies (Johansson et al., 2023). While we did not encounter ceiling effects, this remains a consideration when using the index with specific groups like our sample, such as healthcare professionals or those involved in palliative care (Noonan et al., 2024). Our findings provide valuable insights into the index’s potential and aspects that may require refinement, but we recognize our sample was small and lacked cultural and linguistic diversity. To fully assess the index’s clinical utility, further research is required with a larger and more representative sample.
Conclusion
Overall, we found the DLI has potential for use in Canada but requires modifications, further testing, and validation to enhance its clinical utility. Adapting the index to the Canadian context will support a better understanding of the public’s knowledge and needs; information that is essential for strengthening death literacy across Canada’s diverse communities.
Supplemental Material
Supplemental Material - Clinical Utility of the Death Literacy Index in Canada: A Mixed-Methods Study
Supplemental Material for Clinical Utility of the Death Literacy Index in Canada: A Mixed-Methods Study by Charmaine Holland, Christine J. McPherson, Nick Busing and Paul Hébert in OMEGA - Journal of Death and Dying
Footnotes
Acknowledgements
We would like to thank Compassionate Ottawa for their efforts in spearheading this work to explore the usefulness of the Death Literacy Index in Canada. Their drive to support our communities through living, dying, and grief truly strengthens our capability to care for each other in times of need. Many thanks to Claire Maultsaid for her contribution to assisting with conducting focus groups and qualitative analysis. We would also like to thank our community members and colleagues who provided valuable input and guidance throughout the study.
Charmaine Holland would like to acknowledge her grandmother, whose love and wisdom have profoundly shaped her life and whose passing in 2023 deepened her commitment to death literacy and compassionate end-of-life care. She is also grateful to her mentor and friend, the late Dr. Ronald Bayne, MD/CM, FRCPC (1923–2021), Canada’s pioneering geriatrician and an advocate for initiating conversations around death and dying. She further thanks Dr. Claudius Che, MD, CCFP, and Dr. Richard Safranyos, MD, FRCPC, whose early mentorship and compassionate care towards patients have shaped her core values and advocacy interests.
Author Contributions
All authors of this article contributed to the design and conduction of this study. The study survey, clinical utility evaluation tool, and focus group question guide were created with effort from all authors. The first draft of the manuscript was written by Charmaine Holland; Christine McPherson assisted with writing the results and discussion; and all authors commented on and/or edited previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We gratefully acknowledge the Medical Student Summer Research Program, offered by the Faculty of Medicine at the University of Ottawa, for providing a bursary that supported part of this research.
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Bruyère Research Institute and the University of Ottawa research ethics boards, reference number M16-22–021, and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Data Availability Statement
Availability of the online survey data is available on request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.