
Abstract
The aim of the study was to examine the predictive roles of socio-demographic variables (age, gender, caregiver relationship to the patient, and living arrangements), cancer-related variables (time passed since diagnosis, cancer stage), psychological factors (receiving psychological help after diagnosis, current need for support), resilience, transformative power of suffering, and hope on mental health continuum (MHC) of caregivers of cancer patients. The sample consisted of 119 caregivers (92 females and 27 males) of early-stage cancer patients diagnosed within the past five years without metastasis. Data were collected using the Demographic Information Form, Mental Health Continuum Scale-Short Form (MHCS-SF), Brief Resilience Scale (BRS), Transformative Power of Suffering Scale (TPSS), and Dispositional Hope Scale (DHS). Pearson Correlation, and Hierarchical Regression Analysis were conducted. The results indicated that being the spouse of the patient was a negative predictor of MHC (p < .05), while not reporting a need for psychological help and living separately from the patient were positive predictors (p < .05). Additionally, resilience, the transformative power of suffering, and hope significantly predicted MHC (p < .01). On the other hand, age, gender, caregiver role (child or parent), cancer stage, treatment duration, and whether the caregiver received psychological help, did not significantly predict MHC (p > .05).
Introduction
Cancer is one of the most common and serious chronic diseases in the world that threatens human health (Sung et al., 2021). Death rate because of cancer increased 10 million people in 2019 from 6 million people in 1990 (Global Burden of Disease, 2020). World Health Organization [WHO] (2020) statistics indicated that in 112 of 180 countries in the world, cancer was the primary or secondary cause of death of people younger than 70. In Türkiye, the statistics revealed that every 221 people in 1000 people got cancer diagnoses in 2016 (Turkish Public Health Institution-TPHI, 2018). Although diagnosis and death rates were increasing in recent years, survival rates were also rising with new treatment techniques, early interventions, and new medical developments (Miller et al., 2019).
Cancer has both physical effects such as swelling, fatigue (Harris et al., 2014), shortness of breath, fever, (Gensheimer & Loo, 2017), eating problems, constipation; and psychological effects such as depression, anxiety, distress (Grov et al., 2005; Park et al., 2013) on patients. Hinz et al.’s (2010) study found that more than half of the patients suffered from at least one of the two psychological issues which were depression and anxiety. Moreover, some patients were dealing with post-traumatic stress disorder (PTSD), sleeping disturbances, death anxiety, and low level of psychological well-being (Grov et al., 2005; Rhee et al., 2008).
Cancer was seen a familial disease due to the reason that it affects both patient and family system during the diagnosis, treatment and after treatment process (Opsomer et al., 2020, 2022). Families get through this process as difficult as the patients due to the reason that this type of serious disease threatens the whole system financially, socially, and psychologically (Lauzier et al., 2005). Similar to patients, distress, depression, anxiety are some of the effects that were shown in caregivers, and some of these effects such as distress could be permanent (Ell et al., 1988; Given & Given, 1992; Pitceathly & Maguire, 2003). Stenberg et al.’s (2010) review study revealed that over 55% of the problems caregivers underwent pertained to cancer diagnosis and the accompanying mood changes, panicking, sense of loss, and feelings of distress, fear, anxiety, depression, helplessness, and loss of meaning. Caregivers’ most visible response to all these feelings were found as suppression in Schmid-Büchi, Halfens, Dassen and van den Borne’s study (2008).
Cancer has a crucial impact on the mental health of patients’ caregivers. Mental health continuum (MHC) is an umbrella term that covers emotional well-being, psychological well-being, and social well-being (Keyes, 2002). Caregiving brings new roles and responsibilities in people’s life, and all these changes make people feel stuck, vulnerable, and desperate (Kim et al., 2006). At the end, their life satisfaction decreases (Kim et al., 2012) and the development of anxiety and depression might be sometimes permanent (Stenberg et al., 2010) due to the reason that caregiving requires working approximately 8.8 hours per day with the responsibility of emotional support, caring other family members, medical assistance that can be very overwhelming (Kim & Spillers, 2010).
To deal with all these, personal resources such as resilience and hope were required to keep moving. Resilience means having the ability to move on after a challenging life event (Masten, 2001). In other way, to get through a devastating life event, people adapt that challenging event (Limonero et al., 2015; Palacio et al., 2018). In caregiving process, resilience took different roles such as being mediator how to deal with disease and adaptation to disease as well as a protective role in taking the burden off the caregiver, that is, when caregivers’ resilience level is high, the pain caused by caregiving decreases (Palacio et al., 2018) and being supportive to coping strategies (Dionne-Odom et al., 2021). Moreover, studies indicated that resilience positively affects caregivers’ mental and physical health and it increased life satisfaction by showing a protective role toward developing psychological disorders such as anxiety or depression (Goldzweig et al., 2013; Palacio et al., 2018; Steptoe et al., 2009).
According to Carel and Kidd (2019), challenging life events have the power to transform people’s desires, life perceptions or values. Transformative power of suffering (TPS) was described as the positive transformation that a person went through being stronger after a devastating life event (Joshanloo, 2014). Besides negative impacts of cancer on caregivers, it also has positive effects on caregivers such as improved self-esteem, finding meaning in life, and a stronger tendency to live a purposeful life (Andrykowski & Hunt, 1993; Bower et al., 2005; Ness et al., 2005). These concepts were mostly associated with post-traumatic growth (Cormio et al., 2014; Pirl, 2004). The pain that was a result of a trauma, has influence on perception of life or finding more meaning in life (Tedeschi & Calhoun, 1996). Although studies on TPS were limited in the literature (Carel & Kidd, 2019), there was some research related to post-traumatic growth (Joseph & Linley, 2008; Palacio et al., 2018; Tedeschi & Calhoun, 2004). Some dimensions of post-traumatic growth were parallel with the definition of TPS such as responsibilities (new roles, new responsibilities related with the hospital, illness and patient) (Kim et al., 2006), coping skills (Friedman et al., 1988), and hope (Carver et al., 1993). To be more specific, additional new roles and responsibilities that come from the treatment process have the potential to change caregivers’ perspective about life. These changes could enhance caregivers’ psychological resources and help them to find new meanings in life (Kim et al., 2006). Another study found that partner caregivers’ post traumatic growth levels were higher after the treatment process (Manne et al., 2004) based on the idea that the treatment process is a turmoil meaning that it affects both negatively or positively. Since the cancer treatment process is a rough trot for both patients and caregivers in terms of mental health, the process has the potential itself to transform pain into a powerful weapon to fight with the disease. At this point, TPS can show up on the stage with its positive roots. It is important to check this concept with caregivers because the appearing studies for caregivers are about depression and anxiety. For example, Schulz and Beach’s (1999) study showed that non-caregivers’ mortality risk rate 39% less than caregivers while Brown et al.’ (2009) disclaimed the opposite which indicated that dealing with such a kind of disease in a lifetime raises people’s adaptation skills and reduces mortality. This example is one of the bases for the idea that TPS levels of caregivers have an effect on their mental health.
Hope which influences people’s resilience, mental health, life perspective etc. (Rutter, 2012) was described as expecting one person’s aims to be met (Snyder et al., 1996). This definition involves two dimensions which were engaging actions to achieve that aim and having potential for drawing alternative ways (Snyder et al., 1996). When the subject was cancer, hope had gained different meanings throughout different research. For example, Duggleby et al. (2007) came out with a new concept called “hanging on to hope” after a study related with terminally ill patients’ caregivers and this study described hope as being positive, being unique, and living in the moment. Despite hope was a concept that focused on the future rather than the present (Duggleby et al., 2007), in that study, hope was worked as a present subject. With caregivers, studies mostly investigated the role of hope as a resource to deal with the disease in the process by supporting psychological and spiritual well-being of the families (Borneman et al., 2002; Holtslander et al., 2005). Another study indicated that hope never ends during the process independently from the stage or treatment duration (Bergqvist & Strang, 2019).
This study was conducted to investigate the role of resilience, TPS and hope on MHC of cancer patients’ relatives. To know whether resilience, TPS and hope were related with MHC or not could help the literature to find new ways to reduce negative effects of cancer process on families’ mental health and support their psychological resources.
Method
Research Design
Cross-sectional research design was used in this study. In a cross-sectional study, data obtained at a certain time from an existing population related to the research question are examined. It was described as taking a “snapshot” of a group of individuals. There isn’t a prospective or retrospective follow-up (Carlson & Morrison, 2009).
Sample
Population of the study consisted of individuals who had a parent, partner, or child with a cancer diagnosis. Participants who were older than 18 years old, whose patients were at the first three stages of cancer within the past two years, when they got prognosis, and their cancer did not metastasize, and in the active treatment process were included to the study. On the other hand, if the patients were at the four or terminal stage, cancer metastasized, or treatment process completed were excluded from the study. Convenient and snowball samplings which are non-probability sampling methods were used to collect data. In a convenience sampling method, researchers reach out to people who are available, fast reachable, and easy to reach. Snowball sampling method is used in working a population who is difficult to reach (Karasar, 2011).
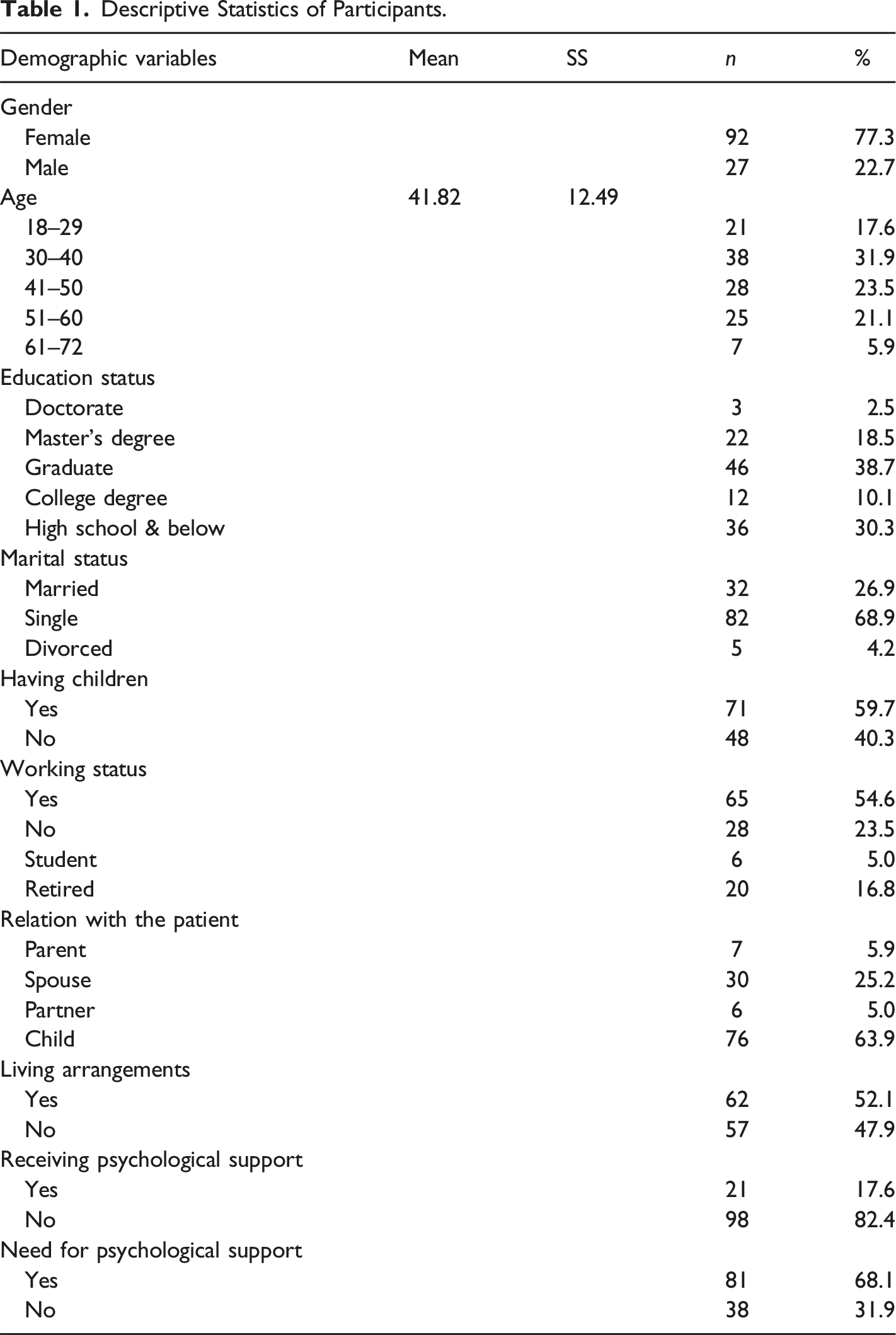
Descriptive Statistics of Participants.
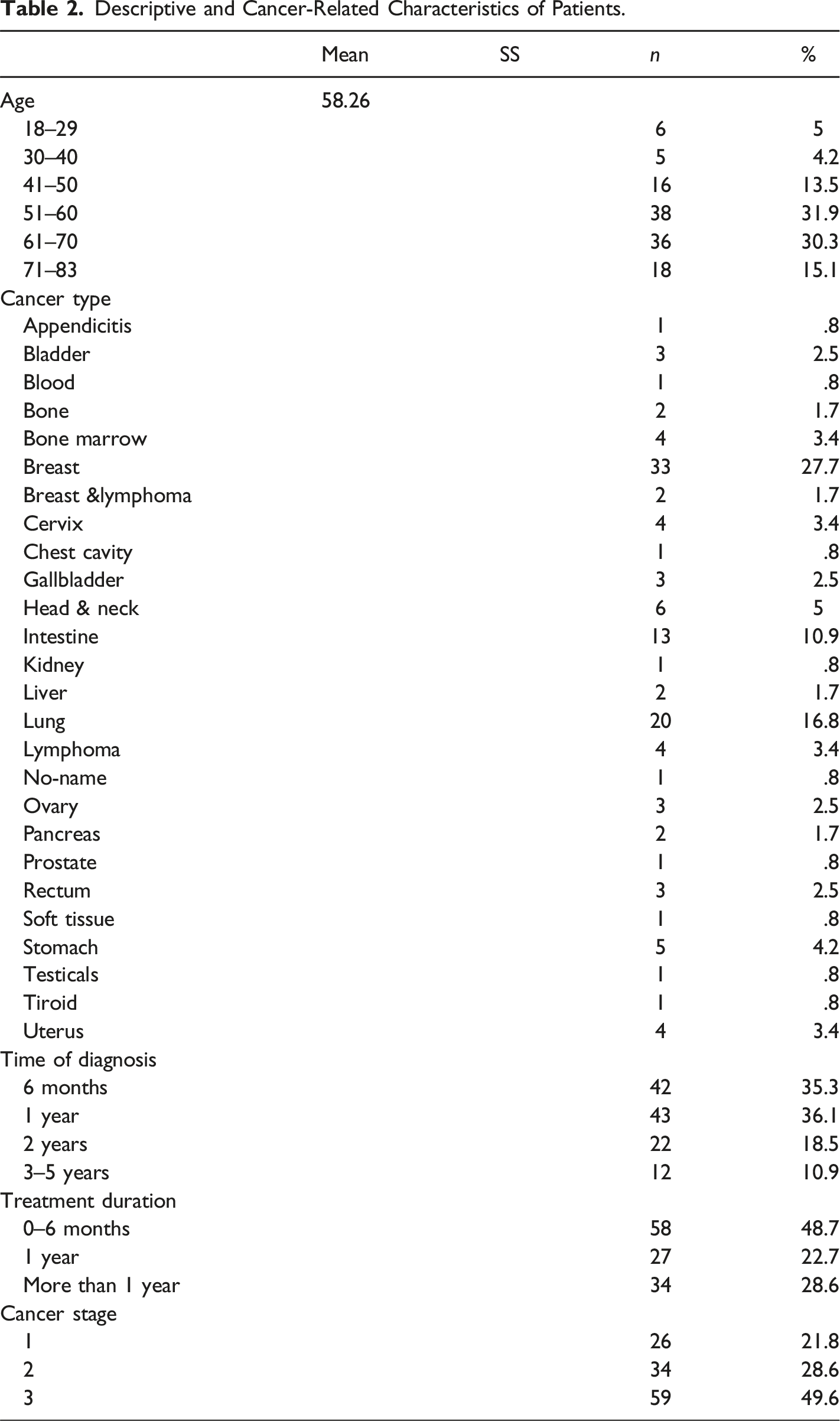
Descriptive and Cancer-Related Characteristics of Patients.
Measures
Demographic Information Form, Mental Health Continuum Scale-Short Form (MHCS-SF), The Brief Resilience Scale (BRS), Transformative Power of Suffering Scale (TPSS) and Dispositional Hope Scale (DHS) were filled out respectively in the current study.
Demographic Information Form (DIF)
DIF which was developed by the research was consisted of fifteen questions about age, gender, educational background, marital status, children, job information, cancer patients’ diagnosis history, any psychological help after diagnosis, and need for psychological help
Mental Health Continuum Scale-Short Form (MHCS-SF)
The MHCS- SF was developed by Keyes et al. (2008) to assess well-being. Turkish adaptation of the scale was made by Demirci and Akin (2015). The scale consists of 14 items and 3 subscales and it is a 6-points Likert type scale ranging from “never” (0) to “every day” (5). First three items measure emotional well-being, items 4-8 measures social well-being while the last six items measure psychological well-being. There was no reverse item in the scale. The points were added to each other, and the total score refers to the mental health continuum. The lowest score of the scale was “0” while the highest score of the scale was “70”. Marking one of the first three items, and six of the last eleven items as “almost every day” (4) or “every day (5)” means flourishing while marking three of the first three items and six of last three items “almost never,” and “never” indicates languishing. The rest of the results except flourishing and languishing was accepted in the normal range in terms of mental health continuum (Keyes et al., 2008). The Cronbach’s alpha value of the scale was calculated as .93 in this study while it was .90 in the Demirci and Akin work (2015).
The Brief Resilience Scale (BRS)
The BRS was developed by Smith et al. (2008), and Turkish adaptation of the scale was made by Dogan (2015). The BRS is a 5-point Likert scale with one factor and 6 items ranging from “strongly disagree” (1) to “strongly agree” (5). Three items (2, 4, and 6) coded reversely. The lowest score of the scale was “6” while the highest score of the scale was “36.” The higher scores mean a high level of resilience whereas lower scores indicate low level of resilience. The Cronbach’s alpha value of BRS was found as .74 in this study. However, in Doğan’s study (2015), it was calculated as .83.
Transformative Power of Suffering Scale (TPSS)
TPSS is a 7-Likert type scale which was developed by Joshanloo (2014) to assess people’s beliefs and their potential of being open to what life brings after a challenging event in a positive way. TPSS consists of one factor and 5 items. There is no reverse item. Scores can change between “5” to “35” and higher scores indicate that a person has a high level of beliefs about the transformative power of suffering. The Turkish adaptation of the scale was made by Dincer et al. (2015). TPSS was a reliable scale with its Cronbach’s alpha value which was .84 both in this study and in the adaptation study.
Dispositional Hope Scale (DHS)
DHS was developed by Synder et al. (1991) to check continuous hope levels of individuals older than fifteen years old. Agency (items 2, 9, 10, and 12) and pathway (items 1, 4, 6, and 8) are two subscales of the scale. DHS consists of 12 items and there is one item for past, two items for present, and one item for future: in total four items for both sub-scales. Four items that are irrelative with the hope were not counted while calculating total score. The total score of eight items indicates hope score, and the lowest score of the scale was “8” while the highest score of the scale was “64” (Lopez et al., 2000). Higher scores indicate high levels of hope while lower scores indicate low levels of hope. Turkish validity and reliability study was made by Tarhan and Bacanlı (2015). The Cronbach alpha value was calculated as .75 in this study while it was calculated as .83 in adaptation study (Tarhan & Bacanlı, 2015).
Data Collection Procedure
Ethical principles of the Helsinki Declaration were followed during the study. Ethical approval was taken from the Scientific Research and Publication Ethics Board of Bahcesehir University (Number: E-20021704-604.02.02-56176) on 4/4/2023 (see Online Appendix I). Data was gathered both online and in person. Questionnaires were put on the google forms and links were shared by researcher’s social media accounts such as Facebook, Instagram, WhatsApp, and X. Furthermore, first, the researcher visited hospitals that gave permission for the study and got in contact with the patient’s caregivers and requested to take part in the study. Filling the scales took approximately 20 minutes. Data was collected between February and December in 2023. In the survey kit, an informed consent form (ICF) was the initial document and participants had to fill. ICF provided information about the purpose of the study, confidentiality, possible outcomes, and importance of giving an honest response. Personal information of the participant such as name, gender, age, educational and marital status were not received.
Data Analysis
SPSS 25 program was used to run statistical analysis of this study. Descriptive statistics were used to determine socio-demographic characteristics of data. Hierarchical regression (HR) analyses were conducted to investigate the predictive role of socio-demographic variables (age, gender, caregivers of patient, and living conditions with the patient), cancer-related variables (time passed since diagnosis, stage of cancer), psychological conditions (receiving help after diagnosis, needing psychological support), resilience, transformative power of suffering, and hope (agency and pathways) on mental health continuum in caregivers of cancer patients. The correlation among study variables was examined through Pearson Product Moment Correlation Coefficient Analysis.
Findings
Preliminary Analysis of the Study
Correlation Results of Mental Health Continuum, Resilience, Transformative Power of Suffering, and Hope.
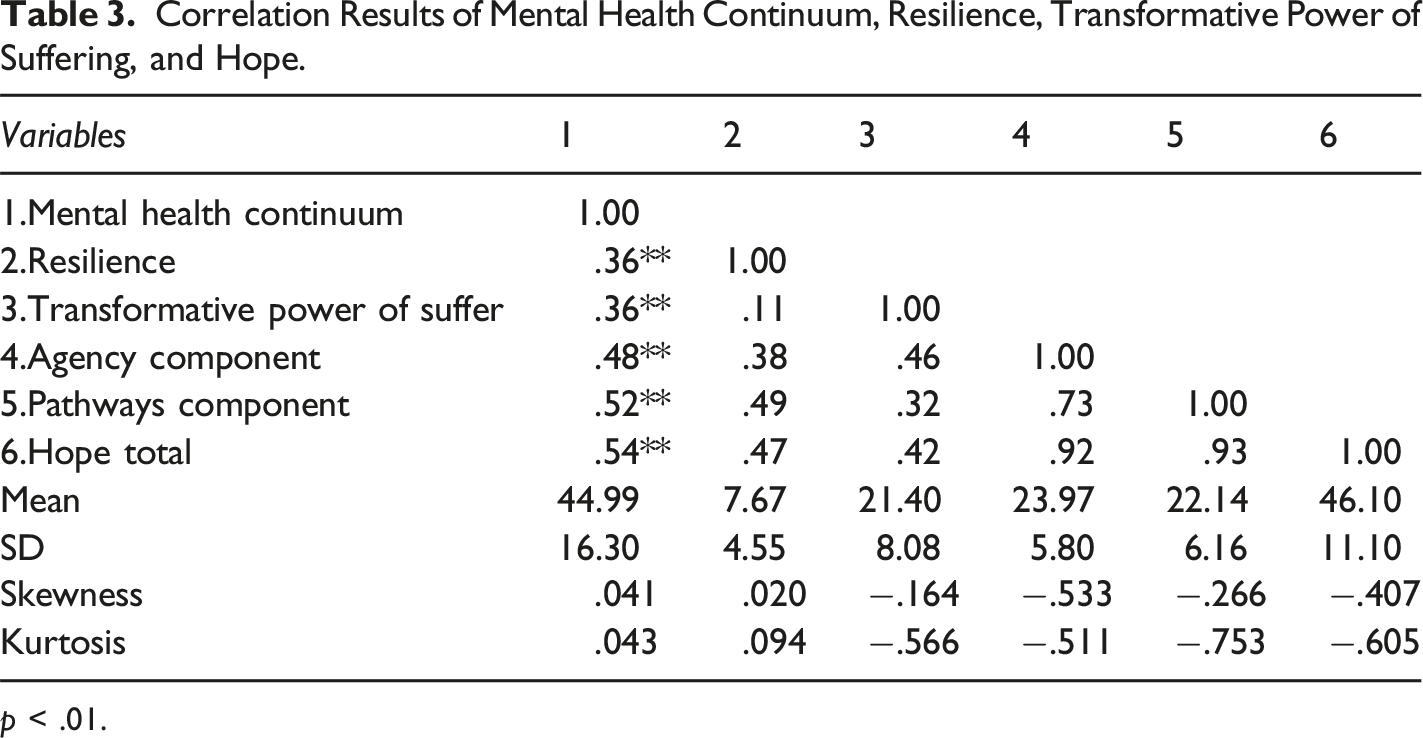
p < .01.
Hierarchical Regression Analysis
Hierarchical Regression Analysis Results for Mental Health Continuum of Caregivers of Cancer Patient (n = 119).
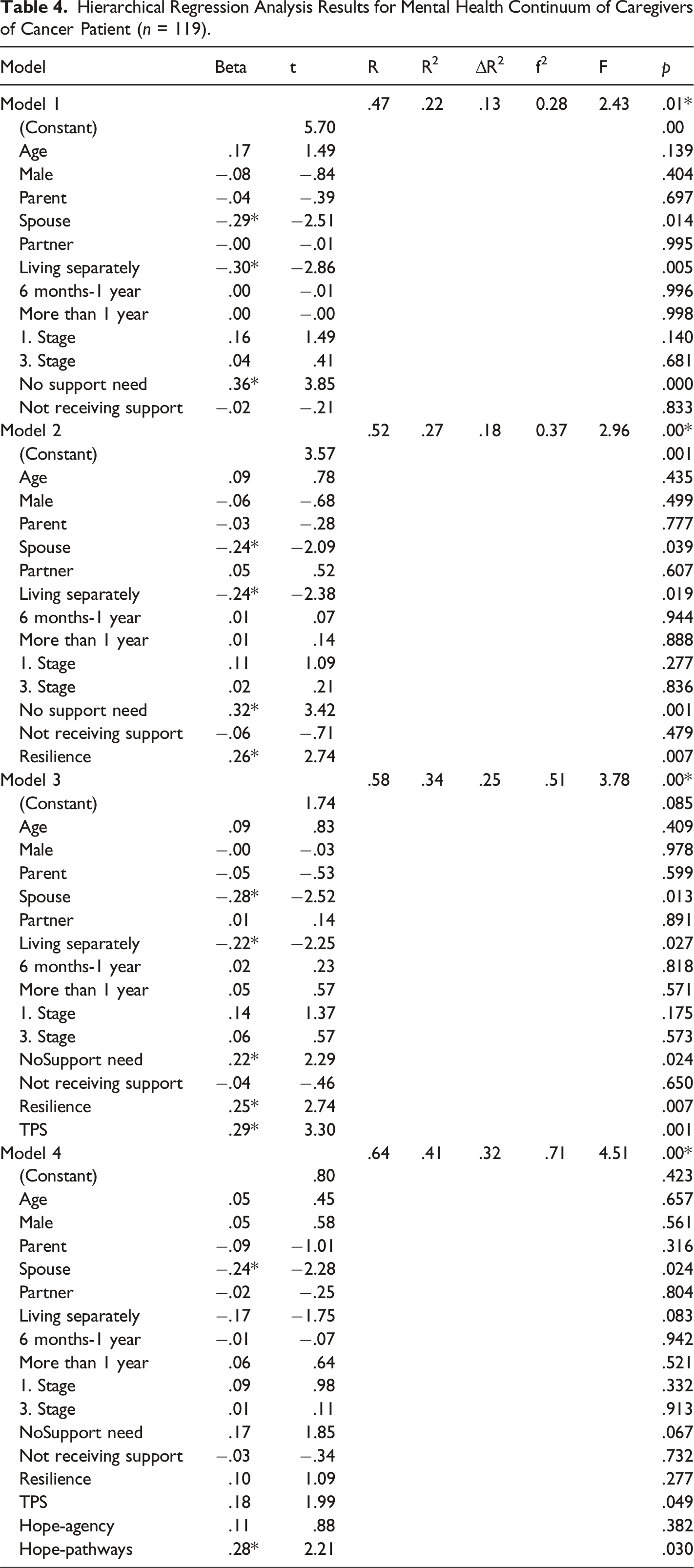
The results of the hierarchical analysis results indicated that being spouse of the patient (β = −.29; t = −2.51; p < .01), living separately with the patient (β = −.30; t = −2.86; p < .01) negatively, not reporting any need for psychological help (β = 36; t = 3.85; p < .01) positively predicts mental health continuum in the first model whereas the rest of the variables; age, gender, being child, receiving psychological support before, cancer stage, treatment duration didn’t predict mental health continuum. Socio-demographic variables, cancer-related variables, and psychological conditions explain 22% of the variance in mental health continuum significantly in the first model (R 2 = .22, F (12, 106) = 2.43, p > .01). The effect size was medium (f2 = 0.28).
In the second model, being spouse of the patient (β = −.24; t = −2.09; p < .01) negatively, living separately with the patient (β = −.24; t = −2.38; p < .01) negatively, not reporting any need for psychological help (β = 32; t = 3.42; p < .01) positively, and resilience (β = 26; t = −2.74; p < .01) positively, predicted mental health continuum. However, age, gender, being child, partner or parent of the patient, receiving psychological support before, cancer stage, treatment duration didn’t predict mental health continuum. Resilience with the socio-demographic variables, cancer-related variables, and psychological conditions explained 27% of the variance in mental health continuum in the second model (R 2 = .27, F (1, 105) = 7.53, p > .01). The contribution of resilience to the model was 5% (Change in R 2 = .05). The effect size was between medium and large (f2 = 0.37).
Being spouse of the patient (β = −.28; t = −2.52; p < .01), living separate houses (β = −.22; t = −2.25; p < .01), need for psychological support (β = .22; t = 2.29; p < .01), and resilience (β = 25; t = 2.74; p < .01) continued to predict mental health continuum in the third model as well as transformative power of suffering (β = .29; t = 3.30; p < .01). On the other hand, age, gender, being child, partner, or parent of the patient, receiving psychological support before, cancer stage, treatment duration didn’t predict mental health continuum. Previous variables and transformative power of suffering explained 34% of variance in mental health continuum in the third model (R 2 = .34, F (1, 104) = 10.87, p > .01). Contribution of transformative power of suffering on the model was about 7% (Change in R 2 = .07). The effect size was large (f2 = 0.51).
Lastly, in the fourth model, it was yielded that being spouse of the patient (β = −.24; t = −2.28; p < .01), and dispositional hope (β = −.28; t = −2.21; p < .01), predicted mental health continuum while resilience, transformative power of suffering, living separately, need for psychological support, and resilience did not predict mental health continuum. In addition, age, gender, being child, partner, or parent of the patient, receiving psychological support before, cancer stage, treatment duration didn’t predict mental health continuum. Being the spouse of the patient and pathway component of hope explains 41% of the variance in mental health continuum in the last model (R 2 = .41, F (2, 102) = 6.67, p > .01). Hope’s addition to the change was 7% (Change in R 2 = .07). The effect size was large (f2 = 0.71).
Discussion
The predictive role of resilience, transformative power of suffering and hope on the mental health continuum of cancer patients’ caregivers was investigated in the current study. In the first step, relations between sociodemographic variables (age, gender, caregiver relationship of patient, and living arrangements), cancer-related variables (time passed since diagnosis, cancer stage), psychological conditions (receiving psychological help after diagnosis, need for psychological support) and mental health continuum were analyzed and interpreted. The results indicated that age and MHC were not found correlated and age did not predict MHC in caregivers. Contrary to the findings of the current study, Lee et al. (2013) found that younger people deal with the process being more stressfully while older people are better able to manage it (Kim & Spillers, 2010). They suggested that since younger caregivers have more stress sources such as work, financial situation, different active roles in life etc. in their lives, they are in the riskier group in terms of distress during the caregiving process. The dominant age group of this study was 30–40 (n = 38, M = 41.82). In this study, MHC of caregivers was not related to age because the dominant group may be using the work, and different roles as a protective factor to keep moving rather than a distress source. This difference may be the result of cultural difference also due to the reason that Lee et al.’s study (2013) was conducted in China which is a very different community compared to Turkish culture. Responsibility of the same age could be different in two cultures.
Being the spouse of the patient predicted MHC negatively. Although Deimling et al. (1989) claimed that adult children’s psychological burden symptoms are similar to spouses, in this study, being the patient’s child did not predict MHC, while being a spouse did. On the other hand, in this study the dominant group was the adult children of the patients who were actively working, having their own families and responsibilities which might be seen as a protective factor against caregiving process negative outcomes. Moreover, it was claimed in a study suggesting that when parents were during the treatment process, their optimism level was high while their stress level was low (Compas et al., 1996). In addition, being a spouse brought additional roles and responsibilities that made life more difficult while the treatment process comes with a new set of skills such as decision making, keeping their lives (Hilton et al., 2000) and spouses became lonely during the caregiving process. At this point being a spouse negatively predicted MHC according to the results.
Although the living conditions were not found correlated with MHC, living separately with the patient during the treatment process positively predicted MHC in this study. When the caregivers live separately from the patient, the frequency of seeing patients in pain decreases which might be a protective factor for caregivers’ mental health. Deimling et al. (1989) emphasized that when children of the patient lived with the patient, their caregiver burden level was not different from their spouses and according to their study, living with the patient affected the psychological burden of caregivers. In Turkey, children mostly live with their parents if they are not married and whether they are married or not they live together with their parents if parents get diagnosed with a life- threatening disease. Hence, living separately positively predicted MHC in the Turkish sample.
A positive significant correlation between not reporting a need for psychological help and MHC was found. According to the reply to the demographic information form, most of the caregivers responded that they did not receive any psychological support before (n = 98), however the majority of them reported that they needed psychological support (n = 81). This result might be explained by characteristics of Turkish culture which showed that Turkish people still have prejudices toward receiving or needing psychological help. Despite realizing that they need psychological help, they prefer to receive support from other sources such as neighbors, friends and family according to the oncology unit observations.
A significant positive correlation between resilience and MHC was found in this study. In addition, resilience positively predicted MHC of caregivers showing that when resilience level was high, MHC level of caregivers was high, too. In Türkiye, caregivers reported that they feel less depressed, and their quality-of-life scores were higher compared to the patients (Gozum & Akcay, 2005). In correspondence with this, resilience could prevent caregiver burden (Uzar-Ozcetin & Dursun, 2020). This study also supported these claims by showing that caregivers’ MHC scores were higher while their general sense of their mental health was positive. This result might be the result of the power of social systems in Türkiye due to the reason that caregivers’ resilience was frequently supported by the community of the caregivers which might be related with environmental factors in resilience.
Together with the resilience, TPS also positively predicted MHC in this study. Concept of TPS was related to gaining new positive skills (Tedeschi & Calhoun, 1996). Being a caregiver makes people more resilient, adaptive (Kim et al., 2006). In correspondence with these previous studies, TPS positively predicted MHC in cancer patients’ caregivers. Participants’ TPS level was relatively high as well as their MHC and resilience level.
A significant positive correlation between hope and MHC was found. In addition, one of the components of hope which was the pathways component took a predictive role on MHC with another variable which was being the spouse of the patient. Spouses of the patients’ hope levels were high in terms of trying to find a solution to be better, and this helped them to maintain their MHC. This result was separately handled from age, gender, being the child of the patient, receiving psychological help before, cancer stage, living with the patient, treatment duration, reporting any need for psychological help, resilience, and transformative power of suffering. Being spouse of the patient and pathways component of hope in terms of mental health continuum of caregivers were the most explanative outcome.
The results of the current study revealed that gender, between being parent, being spouse and being child of the patient, living condition, time of diagnosis, cancer stage, receiving psychological help before and MHC were not correlated with each other, and gender did not predict MHC in cancer patients’ caregivers.
Limitations & Suggestions
To conclude, this study had some limitations such as participants’ mental state due to the reason that they were caregivers, and their emotional reactions were open to changes during the process. Also, responses were taken by self-report questionnaires which means that answers were based on participants’ own thoughts and emotions. During the data collection process, some candidates reacted negatively to the study, some of them were upset that only the first three stage patients were involved. Gender inequality was another limitation due to the reason that male participants were lower compared to the female ones. Although this study consisted of partners, spouses, parents and children of patients, the dominant part of the participants were children of the patients so to understand the other relatives’ parts, more research must be done. This study involved women and adult children’s caregivers, meaning that representatives of the sample may be controversial. Family roles, responsibilities of treatment in terms of caregiving process changes due to gender and age such as financial problems, domestic works etc. Gender and type of relatedness inequality in this study, pose a challenge for generalizability of the results. For instance, resilience and hope levels could change among men and women due to gender differences as well as type of relatedness. A mother and a child could react differently toward a parent or a child’s disease. On the other hand, women’s role as caregivers is mostly similar around the world and this study gave a clue about how women reacted as caregivers in the cancer treatment process. In addition, adult children’s roles and reactions are also common when the subject is cancer because responsibilities and requirements are similar.
Studying resilience, hope, and the transformative power of suffering is essential within the framework of the mental health continuum, particularly for mental health professionals working with caregivers of cancer patients. Group intervention programs can be developed and implemented to enhance caregivers’ levels of resilience and hope. Following these interventions, experimental studies can be designed to evaluate their effectiveness. Enhancing the resilience and hope of spousal caregivers—by supporting the transformative power of suffering—may be especially impactful, given the predictive role that being the spouse of a cancer patient plays in positioning individuals along the mental health continuum.
In future studies, different related terms such as quality of life, decision making processes can be investigated with TPS which was a new concept in the field. Sisters, brothers and friends should be added to the target group to understand different kinds of relations in the cancer process. Different groups can be studied in more equal classifications in future studies.
Supplemental Material
Supplemental Material - Mental Health Continuum of Cancer Patient’s Caregivers: Resilience, Transformative Power of Suffering, and Hope
Supplemental Material for Mental Health Continuum of Cancer Patient’s Caregivers: Resilience, Transformative Power of Suffering, and Hope by Elif Yağmur Bursalıoğlu Erdem, and Berna Güloğlu in OMEGA - Journal of Death and Dying
Supplemental Material
Supplemental Material - Mental Health Continuum of Cancer Patient’s Caregivers: Resilience, Transformative Power of Suffering, and Hope
Supplemental Material for Mental Health Continuum of Cancer Patient’s Caregivers: Resilience, Transformative Power of Suffering, and Hope by Elif Yağmur Bursalıoğlu Erdem, and Berna Güloğlu in OMEGA - Journal of Death and Dying
Footnotes
Author note
This study is a master thesis which was conducted by the first author under the supervision of the second author.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study is a master thesis which was conducted by the first writer under the consultancy of the second writer. The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, [Bursalıoğlu-Erdem, E. Y.], upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.