
Abstract
Background
Bereavement is universal, whilst grief is a natural response to loss, it can have detrimental effects on physical and mental well-being. Bereavement support is not widely available, and workplaces could play a key role in providing consistent, equitable support.
Aim
We explored the views of employers and employees on bereavement training in the workplace.
Findings
Findings were organised into four themes: unique challenges faced by employees and employers after bereavement; gap in training; need for tiered, bespoke training; requirement for policy change. Bereavement training in the workplace was seen as beneficial.
Conclusions
This study addresses a crucial gap in bereavement support by exploring grief training in the workplace. Policy recommendations include: in-house and external support and paid leave as standard.
Keywords
Introduction
Bereavement is universal and therefore it has previously been debated whether grief itself should be recognised as a disease (Stroebe, 2015). Whilst it is widely accepted that grief is a natural response to loss, it is associated with detrimental effects on both physical (Stroebe et al., 2007) and mental well-being, resulting in high levels of healthcare consultations and increased mortality rates (Harrop et al., 2020a, 2020b; Lundorff et al., 2017; Stroebe et al., 2007; Torrens-Burton et al., 2022).
Aoun et al. (2017) proposed a three-tiered model to describe populations risk of poor outcomes following a bereavement. They estimated that 60% of people are at low risk of prolonged grief disorder, 30% moderate risk and 10% high risk. An increased risk of prolonged or complicated grief is associated with personal and relational factors. Lack of meaningful social relationships is an independent social determinant of poor physical and mental health and is particularly relevant in bereavement. Those who are bereaved and lack social support are at high risk for complicated grief and poor mental health including risk of suicide (Pitman et al., 2020). Certain specific social characteristics are associated with increased risk of isolation and prolonged grief, such as those experiencing loss of a spouse/partner (Bristowe et al., 2024) with loss of a same-sex partner associated with an even greater risk of complicated grief (Timmins et al., 2022; Valenti et al., 2023). The model proposed by Aoun et al. (2017) fits with the model adopted by the National Institute for Health and Care Excellence (NICE) which describes three levels of support (National Institute for Health and Care Excellence, 2004). This describes the key role workplaces play in level one support.
Bereavement service provision has been largely based on the estimations of Aoun et al. (2017). It is assumed that those within the low risk group will deal with their grief utilising only the support of family and friends, those in the moderate risk group may need non-specialist bereavement support (e.g. support provided in primary care), whilst those at high risk of prolonged/complicated grief will require specialist professional input (Penny & Relf, 2017).
For those needing specialist bereavement support, current services fall short and vary widely depending on geographical location, despite recent calls for more uniform provision (Harrop et al., 2021; Torrens-Burton et al., 2022; Wakefield et al., 2020; Harrop et al., 2020). As such, provision is inequitable with the most vulnerable societal groups missing out (Bristowe et al., 2018; Selman et al., 2023). The majority of specialist services that are available, are provided by voluntary community sector organisations that do not receive statutory funding and are reliant on charitable giving. The future of these services is often precarious, particularly in the wake of the pandemic and subsequent cost of living crises (Mayland et al., 2020; Selman et al., 2023). Sustainability of current specialist services looks unlikely let alone expansion in response to the current demand (Selman, 2021; Selman et al., 2023a, 2023).
In view of the inadequacy and instability of specialist bereavement support services, contemporary literature advocates for alternative support strategies. These aim to adopt a public health approach, improving grief literacy amongst the general population. Grief literacy describes a multidimensional capacity to “access, process and use knowledge regarding the experience of loss” (Breen et al., 2020). There is recognition that increasing this may facilitate appropriate bereavement support in turn enabling society to function more effectively. By increasing individuals’ ability to cope after the death of a loved one, they are better able to return to their societal roles. Compassionate Communities (Compassionate Communities, 2021), Grief festivals (Selman et al., 2023a) and the development of supportive workplaces are public health initiatives gaining traction (Aoun et al., 2017; Compassionate Communities, 2021; Harrop et al., 2021). The former proposes that bereavement support should be better embedded into communities and that strengthening community action in this area should incorporate neighbourhoods, educational institutions, places of worship and workplaces (Abel et al., 2023). Bereavement has a significant socio-economic impact, with 5% of the working population on bereavement related leave at any time and bereaved employees returning to work functioning at a reduced level (Stephen et al., 2015). Workplaces having the tools to better support employees experiencing bereavement may reduce this socio-economic impact.
The Chartered Institute of Personnel and Development (CIPD) recently launched its new guidance for employers on compassionate and comprehensive bereavement support. This states employers should have clear bereavement policies that outline: • The provision of “in-house” basic support that; trains and empowers managers to support employees, provides workplace support including counselling, occupational health and employee assistance programmes (Selman et al., 2023). • A proactive approach to identifying those in need of specialist bereavement care and clear guidance on how this should be accessed (CIPD, 2021). • Clear bereavement policies outlining leave entitlement.
Jack’s Law, introduced on the 6th April 2020, legislates for two weeks parental bereavement leave and pay. No such legislation exists for other bereavements (CIPD, 2021). Leave is offered at the discretion of employers. Unpaid leave alone may be offered, however costs associated with preceding ill health and funerals often preclude its use. Employees frequently continue to work with detrimental effects on their performance and longer-term health (ACAS, 2018; Wales, 2021). CIPD, Cruse Bereavement Care, Bereavement UK and Affinity Coaching have called the government to create a new legal right to leave and pay, for all those experiencing a bereavement of a close family member or dependent. In addition, as bereavement impacts on employers so significantly, could it be in their best interests to consider contributing to bereavement support as part of a health promotion response? (CIPD, 2021).
Aim: To explore the views of employers and employees on whether bereavement training should be offered in the workplace; if so, to whom; and, concomitantly, whether associated policy change is required.
Materials and Methods
Setting
In Newcastle, St Oswald’s is an independent hospice with 145 clinical-staff, 15 adult-inpatient beds, 6 children’s-inpatient-beds, outpatients, lymphoedema and regional specialist bereavement services. In 2021 the bereavement service started providing training for employers and employees in both public and private sector organisations. This unique enterprise aimed to create both compassionate employers and public facing organisations by teaching individuals what people experience when a loved one dies, how it affects their life, how support can be provided and why this is important. To date 343 participants from 105 regional and national organisations from different employment sectors have been trained including; voluntary community sector organisations; health-service providers (clinical and non-clinical); independent businesses; higher education institutes; and local authorities. The virtual environment is used to keep venue costs down and reduce travel time.
Recruitment and Sampling
All those who received bereavement training from St Oswald’s Hospice were asked for expressions of interest for participation in this research study. All interested participants were eligible for inclusion. Purposive sampling in relation to professional sector representation was used. Recruitment continued until data adequacy was achieved (when no new themes or codes were emerging from the data) and representatives from all sectors were included.
Data Collection
RT conducted in-depth qualitative semi-structured interviews using video-consultation software lasting up to 1 hour. Interview topic-guides explored the perceived benefits of bereavement training, the extent to which the current training fulfilled clients’ requirements, and recommendations for future bereavement training and bereavement policies in the workplace.
Data Analysis
Data were analysed thematically, providing the flexibility to interpret and situate findings in the practice context (Stroebe, 2015). Transcripts were initially coded by RT. All remaining authors (representing academic clinicians from primary and palliative care, and bereavement counsellors) subsequently met to discuss and review the codes. A coding frame was developed, adapted, and applied to the data. The research team met regularly to discuss, develop, and refine themes. Saturation was achieved when there were no new themes or codes emerging from the data.
Patient and Public Involvement
We formed a specific Patient and Public Involvement (PPI) group comprising of volunteers from St Oswald’s Hospice, who are all bereaved relatives. Members helped shape our research question, topic guide, data analysis and interpretation.
Ethics
Ethical Approval was granted by Newcastle University. Application number: 296746
Results
Thirteen women and three men were interviewed. With 80% of course participants overall being female, the interview ratio displayed near proportionality. Participants worked in: voluntary community sector organisations (Pitman et al., 2020); health-service providers (clinical and non-clinical) (Aoun et al., 2017); independent businesses (Stroebe, 2015); higher education institutes (Stroebe, 2015); and local authorities (Stroebe, 2015).
Results Were Organised Around Four Main Themes
The Unique Challenges Faced by Employees and Employers following a Bereavement
Participants acknowledged that there were a range of “business needs” that would have to be balanced against “employee needs”.
All participants acknowledged that bereavement has a differential impact on people over variable time durations. Respondents were unanimous in believing that people experienced difficulties or faced issues when they return to work following a bereavement. The majority believed this was exacerbated by a lack of support or understanding for the bereaved or because of a sense of awkwardness and ‘not knowing what to say’. …‘it was a real, eyeopener of a topic that people don’t really talk about delivered in a really accessible way that was – it was sensitively delivered. And really did raise awareness of an important topic that employers probably shy away from’.
Participants recognised that employers also faced a range of issues when an employee is bereaved, including reduced performance and focus and absences. ‘…they may suddenly be tearful or distracted or not focused, and it's understanding why and how to handle that is what really I took from the session’.
Practical difficulties might include the immediate availability of suitably qualified replacement staff in the face of sudden bereavement leave, and the issue of paying a replacement worker to do a job as well as paying another employee who is on bereavement leave.
There was a recognition that organisations which were “people-orientated” would look to support employees where there had been a bereavement, but how this was operationalised would often be influenced by managerial discretion rather than formal policy. Participants recognised that if organisations are “people orientated” and appropriately support bereaved employees, they would receive a “pay back” in a reduction in sick-days and a longevity of service.
The gap in bereavement training provision
There was a recognition amongst participants of the ‘gap’ in training. A considerable number of respondents thought that bereavement training is essential but that it just “didn’t usually happen” within the workplace. ‘…we didn't realise it was a gap …we suddenly thought, oh my goodness, what do we do? And I think we're all keenly aware that bereavement is something that is...it’s not, you know, it's not a unique situation….it was …. a case of we didn't realise we didn't have a way of handling it professionally’.
A key message was that training should be more widely available, and mandatory for people in certain roles. ‘…if somebody is dealing with the public, like most council workers do, I think it should be part of their statutory training’.
Participants highlighted that the COVID-19 pandemic had intensified the importance of the bereavement training: ‘…For me, it's very useful because I'm dealing with patients who perhaps are going through bereavement, and also colleagues. You know, during the pandemic, obviously we did lose a lot of lives. And you might know someone that you worked with, or a friend or a family member that, you know, did die because of COVID. So, I think it's really important for me to be up to date with information about that’.
Recommendations for Inclusion and Expansion
For the overwhelming majority of respondents, one of the main benefits of training was knowing how to begin a conversation with a bereaved person, how to handle the situation, what sort of words to use and what not to say. As one said: ‘I think it's just helped me be a little bit more open and knowing how to start conversations with people that have been bereaved….Before, I wasn't really sure what …And I think that training did give me a lot more insight as to what is the best approach to use and just generally made me feel more confident talking about bereavement’.
Others commented with suggestions for improvement, including longer training, with stronger interaction, case vignettes/scenarios and more information about specific situations like loss without death. ‘….I think it could have been a bit longer as well. …there was a part missing where, if a carer loses someone to an illness, not because of a death, but ….advanced dementia or stroke… they're grieving for that person. They’re still alive, but they're still grieving for them. Or they could be grieving because the person has gone into a care home …’
There was some corroboration of the duration issue, with this comment from another respondent: ‘Yes….there was a lot of information… could have done with being a bit longer or perhaps having a bit more time to think things through’.
There were a few other suggestions for change. One respondent thought that the training package would benefit from the use of ‘real life’ examples: ‘...sort of scenarios or things so that people can then put – you know, it makes it a bit more real for people when they’re thinking about it. Particularly if you’re a new manager I suppose you might not have come across it before and it can be a bit tricky because then you don’t have much practice until somebody does have a bereavement and then you don’t want to be practising on someone, you want to be able to support them well from that first time’.
An interactive format was also suggested: ‘…It could have done… with a little bit more interaction or breakout discussions….for me’.
Training should be tiered and bespoke (but basic training should be delivered universally)
Participants recognised that everyone will face issues relating to bereavement, and therefore training on the subject is beneficial for all. One said: ’ ….yes. It shone light on……..grey areas, where you'd be kind of trying to feel your way through it….people were impressed by it’. one respondent thought that ‘….there should be as standard throughout, for every organisation, for every workforce… There isn’t unfortunately…’.
There was overwhelming agreement from the respondents that tiered and bespoke bereavement education packages are required. It was acknowledged that certain groups of people, or organisations may deal with death and bereavement frequently, and for those training should be more involved and should cover the support of employees and colleagues as well as patients, clients or members of the public.
Many participants, especially those in the third sector and in the NHS highlighted that they experience the issue of bereavement on a frequent basis and yet had received no previous training on the issue. ‘…for our patient caseload…I have a few patients that have suffered a bereavement and I haven't had any specific training for that….I just wanted to help with that, knowing how to engage these patients in those situations’. ‘…. I think the general principles cover everybody, but….where you’ve got front line staff who were dealing with certain things or conditions I suppose it might be helpful to have something a bit more bespoke for them’
There was a widespread perception that variable training packages may be useful for different categories of worker and that training in bereavement is particularly useful for those in managerial positions or those responsible for supervising other people and supporting them to return to work after a bereavement. ‘.…it's useful for employees to have that training, you know, for support if you lose one of your peers. Or it's useful for employers to have it, to deal with employees who are going through the process. And useful for the likes of myself, as a worker, dealing with patients that might suffer from bereavement. So, there would be different kinds of categories…that would be beneficial’.
Participants were clear in their message to those who had the power to make policy decisions that bereavement training should be encouraged or, even, mandated.
Change in (organisational and governmental) bereavement policies are required.
Most respondents reported that their employing organisation did not have a clear bereavement policy, though some did speak of related policies, such as wellness action plans or special leave arrangements. ‘…I know there's been times where we've had people off ….we all just group together and do what can be done….the case manager would do a random check in with that person’.
Interviewees were clear that bereavement training for those who have the power to make policy decisions should be encouraged or even mandated.
Participants reported that minor changes in policy had been made since they attended the training such as ‘…a crib sheet for handling bereavement...the key points, what you do and we don't do’. The majority had fed their learning into policy groups and policies were due to be amended at the next “cycle”. A wider beneficial ‘externality’ was reported as general messages from the training were filtered down through organisations. One manager stated that she had disseminated some of what she learned, specifically the importance of peer support in the workplace and staff feeling free to talk to managers about sensitive issues. ‘….Give them room to communicate on a regular basis.…check-ins to see how they're getting on….if they ever feel overwhelmed, give them the space to take a step back in their work’.
The predominant feeling was that there should be national recommendations/requirements, and that organisations should have policies in place outlining their commitments to leave entitlement. There was a strong sense among the respondents that organisations should be supportive and flexible in response to bereavement, echoing the theory proposed by Aoun et al. (2017) that bereavement care needs to be individualised as different people will need different levels of support. The importance of those in managerial positions being “approachable and accommodating” was highlighted repeatedly. The predominant feeling was that organisations should have policies in place which outline commitments to leave entitlement, but that also demonstrate flexibility, recognising that people’s responses and needs are different. ‘Everybody’s circumstances are different…So it's understanding a situation. So, the policies have got to be one of understanding and appreciating’.
Alongside these above issues, there was a view that policies on issues such as rights and leave should be clear. As one respondent put it: ‘…it will come under like a workforce health and wellbeing….. as leave entitlement, so …. there should be something written in to say, if you have experienced a loss and you are returning to work, this is what you can expect from us as an organisation’.
And another: ‘….they should have a policy for bereavement leave and clear advice of how they're going to be supported when they do return, whether it should be a phased return. Maybe change their role….it's acceptable not to go back into the job that you're doing if it could cause extreme upset. And I don't think that should be judged by your manager’.
There was also a feeling that taking time off because of bereavement should not be detrimental in relation to organisational targets for absenteeism. As one respondent said: ‘…They should have a standard bereavement policy which outlines what leave and such like will be offered….hive off absence related to a bereavement, from general sickness, so it didn’t count towards... an absence target….So, you couldn’t go on to a disciplinary for absence because of a bereavement’. ‘… people that are coming back to work..[should]…feel fully supported by the company and...if they do need additional time off, or if it has affected them within their mental health, they feel as if they're not scared that it’s going to go down as, you know, sickness and then, sort of, you know, trigger points and things, and looking at performance reviews. Because people think it goes negatively against them if they take time off. So, I think we should have something that’s quite robust to say, look, this is what we can do to support a person and they don't have to be frightened to take time off, because that is... ultimately, they’re going to come back at the right... because if they get rushed to come back when they’re not ready then they’re going to ultimately then go back off again probably’.
The importance of an accommodating manager, or perhaps a designated person or ‘buddy’ in the organisation with whom a bereaved person can talk, was recognised strongly. ‘I think policies and procedures should be making sure that ….you can speak to your manager no matter what… whether that manager is qualified to hear the bereavement side of it, they may well not be’. ‘I mean it’s just basically you need to have an approachable manager, somebody you can talk to…. And, if not, somebody in your team you can talk to…it might be a good idea to have like a type of buddy type of scheme’.
Discussion
Interviewed participants, from a wide range of public and private sector organisations, felt bereavement training in the workplace was beneficial for individuals, employing organisations, and society in general. Despite this, participants highlight a lack of training and support in bereavement. They recommend that tiered and bespoke training should be widely available. Participants suggested that a basic level of training was required for all regardless of their position or their employment sector, and that higher levels of training were required for those in managerial positions and those in organisations where exposure to death and dying is frequent such as those in health and social care. Finally, participants recommend that bereavement policies need to change, the responsibility of which lies with both individual organisations and the government.
Recent literature has highlighted the role public and private sector employers can play in strengthening the bereavement support sector. Public health frameworks describe sequential levels of bereavement need, the appropriate care responses required, and the knowledge and skills needed to deliver these (ACAS, 2018; Wales, 2021). The bereavement care four level pyramid is a public health model and helpful framework used to describe the different levels of need, the appropriate care responses and knowledge and skills required at each level. It fits with the model adopted by the National Institute for Health and Care Excellence (NICE) which describes three levels (combining the two higher support levels) (National Institute for Health and Care Excellence, 2004) this corresponds to risk levels of prolonged grief disorder described by Aoun et al. (2015).
Levels of Bereavement Need and Potential Role of the Workplace.
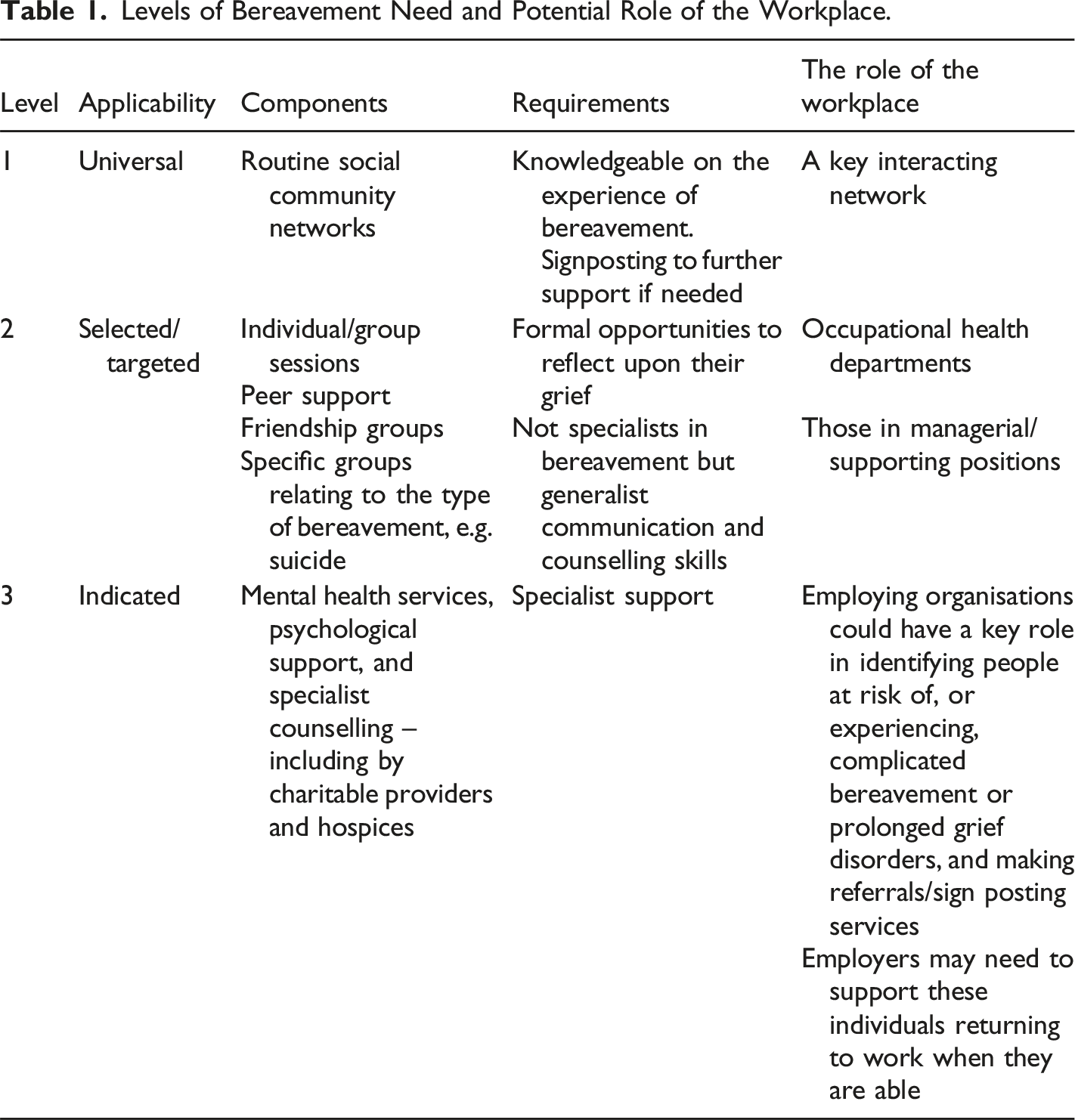
When considered in this way employers play a key role in ensuring communities are more compassionate. Appropriate training, best practice guidance, policy recommendation and legislation is required to enable adequate support of bereaved employees. Widespread education initiatives should aim to improve social networks, grief literacy including opportunities for remembrance, communication skills and awareness of support options. Partnerships between organisations that provide and require bereavement training and support provision may be mutually beneficial particularly in the VCSO sector (ACAS, 2018; Wales, 2021).
Strengths and Limitations
Consultation with our Patient and Public Involvement group dictated our methodology. The group felt that the experiences of bereaved relatives, returning to work are overlooked and their needs poorly understood. They stated that they felt organisations’ ability to provide support is often lacking and the reasons for this are often complex and heterogeneous including poor skills and inappropriate policies. It was felt that in depth semi-structured interviews would allow individuals’ and organisations’ training needs to be comprehensively explored, allowing a greater level of understanding of this complex topic and comprehensive exploration of key issues including the needs of the bereaved and organisations’ ability to provide support. Basing the topic guide around the recently delivered training allowed the subject to be contextualised. We captured a diverse range of opinions from a group with varying professions, seniority and backgrounds. The research team was multidisciplinary, contributing to the analysis and discussions from distinct and contrasting positions.
This was a small qualitative study, and its limitations are duly recognised. We make no claims to have recruited a sample representative of the general population; it is also recognised that people reflecting positively on the training may have been more likely to participate in the research, leading to a potential overstatement of its significance and importance. Due to the small nature of the sample, purposive sampling in relation to professional sector representation meant we did not capture the views of multiple people within a professional sector. It is recognised that the views of the individual participant may not represent the views of all participants within the sector they represent. This approach did not allow us to capture different views between individuals with differing roles within the same sector. The use of online interviews may have excluded potential participants uncomfortable with, or unable to access, requisite technology.
Future Recommendations
Future work is needed to evaluate whether bereavement training makes a significant difference to employees returning to work following a bereavement. Evaluation should consider changes to policy and support structures as well as evaluations of the mental and physical health of the employees themselves and the productivity of organisations. Longitudinal studies assessing the longer-term effects of workplace bereavement training should be considered to inform future policy changes, and ensure that workplace bereavement support models are able to be responsive to an organisations’ changing needs.
Conclusion
Employees of varying grades and professions recommend tiered bereavement training for employing organisations. It is an important consideration for the development truly compassionate communities and improved grief literacy. Perceived benefits include improved support for, and consequently mental and physical health of bereaved employees and enhanced efficiency of organisations. Recommendations for organisational and governmental bereavement policies include; the availability of in-house and external support, paid leave as standard with flexibility to respond appropriately to individual situations.
Footnotes
Acknowledgments
The authors would like to: Acknowledge the contribution of the participants, we are very grateful for the time they dedicated to the project and thank them for sharing their personal experiences. Their insights are invaluable. Express our gratitude to our PPI contributors for their thoughtful feedback throughout the research process. Finally, the authors would like to thank St Oswald’s bereavement team for supporting our participants when they needed it.
Author Contributions
All authors made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data. FD and RT drafted the original article. All authors approved the final version to be submitted. All authors have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This report presents independent research funded by the National Institute for Health and Care Research (NIHR) North East and North Cumbria Applied Research Collaboration (NIHR200173). The views expressed are those of the authors and not necessarily those of the NIHR. Instituational Review Board Statement.
Ethical Statement
Data Availability Statement
Anonymised data is stored by Newcastle University and can be accessed on request.