
Abstract
Multiple losses in wartime, both death-related and non-death-related, require multidimensional assessment to encompass both the event and the multiple levels of interpersonal and societal involvements within which individuals are embedded. We present a case study in which the traumatic death of a family member is a central, but not exclusive, element in understanding the bereavement process. The traumatic death originated with the events of October 7, 2023 and the ensuing war which were part of an overwhelming surge of traumatic losses in Israel. The bereaved’s response met the criteria for Post-Traumatic Stress Disorder (PTSD) and Prolonged Grief Disorder (PGD). We recommend that multiple losses and their unique significance for the bereaved should be directly addressed in the assessment and formulation of therapeutic interventions. Therefore, we propose an approach to clinical assessment in cases of mass trauma and multiple losses, grounded in the Two-Track Model of Bereavement and the Systemic-Ecological Perspective.
Keywords
War-torn regions, such as those affected by the current Russian-Ukrainian war (Chudzicka-Czupała et al., 2023; Shevlin et al., 2022), the Syrian civil war (Bryant et al., 2021; Mclntyre, 2020), and the war that followed the events of the Seventh of October 2023 in Israel, are characterized by the fact that coping often extends beyond response to a single traumatic event to encompass multiple traumas and losses. These may include both multiple losses due to death (of more than one person) and various other—tangible and symbolic—losses not necessarily resulting from direct death (Manevich et al., 2023). Examples include ambiguous loss (Boss, 2017) experienced by the families of hostages, the losses endured by those suffering physical and psychological injuries and their loved ones (Yehene et al., 2021), and disenfranchised grief (Doka, 2008) experienced by many evacuees who have become “refugees in their own country” due to the loss of their homes.
In the face of war experienced first-hand, no words in the lexicon can adequately capture the horrors, terror, and brutality of the destruction and the potential for such events to profoundly shattered the fundamental beliefs of many regarding humanity and the world (Janoff-Bulman, 1992). Beyond the immediate impact of the attacks and the ensuing multi-front war on daily life and mental health across all affected populations (Aldabbour et al., 2024; Levi-Belz et al., 2024), the full scope of long-term consequences remains difficult to predict. However, it is clear that the ramifications are extensive and affect diverse populations. As the circles of interpersonal loss in traumatic circumstances expand, so do the number of individuals requiring professional support tailored to the unique constellation of these losses. Given this reality, the present paper opens with a composite case study that illustrates the multi-dimensional nature of war related trauma and bereavement that began with the October 7, 2023 Hamas attack on Israel. Following the case description, we set forth principles and rationale for the multidimensional assessment of multiple losses and traumatic bereavement in wartime based on the Two-Track Model of Bereavement and the use of the Systemic-Ecological Perspective on the individual in context (Bronfenbrenner & Ceci, 1994). Next, we return to the case and highlight how its components are manifest in the theoretical-clinical perspective we have described.
Case Study
Joseph, a 28-year-old man, married and the father of two young children, underwent a psychiatric evaluation approximately one year after the events of October 7,2023 1 . He was born and raised in one of the Israeli communities in the Gaza border region and had two siblings: a twin sister and an older brother. On October 7, his wife, Shila (26), was in the final stages of pregnancy, and they were young parents to a one-year-old baby daughter. At the time, they were living in a housing unit on the outskirts of their community alongside Shila’s parents.
Joseph recounted that on the morning of the “black Sabbath” of the 7th of October, he awoke to a phone call. The connection was poor, but he believed he heard the voice of his twin sister. Shortly after, the call was disconnected, and in the background, air raid sirens began to sound alongside shouting and gunfire. Joseph, his wife, their infant daughter, and Shila’s parents immediately ran to the small shelter (MAMAD) and locked themselves inside. However, the sounds of gunfire and shouting grew louder as they slowly approached. Joseph, who had served as a combat paramedic, wanted to go outside with his first aid kit to assist anyone in need. However, there were no firearms in the house, and Shila pleaded with him not to leave her, fearing she might go into labor at any moment. Joseph gave in to her pleas and remained in the shelter. Hours passed slowly, and anxiety overwhelmed him. He was particularly worried about his twin sister, who also lived in a nearby community.
The confinement in the small, crowded shelter with his in-laws triggered intense feelings of physical and emotional suffocation, anxiety, distress, and above all, helplessness in the face of the realization that they were surrounded by terrorists. Time dragged on until, after 14 hours, noises were heard in the house. Everyone tensed up until they heard a knock on the fortified room’s door and shouts of “We are IDF (Israel Defense Forces) soldiers!” Joseph cautiously approached the door, asked for identifying details, and only after being convinced, opened it.
Upon leaving the shelter, Joseph received a phone call informing him that his sister was missing. He immediately started making plans to search for her but was soon informed that she had been kidnapped. Two days later, he was told that her body had been found. The funeral was held shortly after the final identification, which took a few additional days. Following these events, Joseph withdrew into himself, lost his appetite, and was consumed by fears and thoughts about how these experiences might negatively affect the upcoming birth and his newborn child.
Joseph and his family were relocated to an apartment in central Israel. A week after their arrival, Shila gave birth to a healthy baby girl in a natural delivery. Initially, Joseph was filled with joy and relief that the birth had been complication-free. However, within days, he sank into profound grief. Additionally, he was informed that he had missed the final year of his studies and lost his internship placement.
For 10 months, Joseph, his family, and his in-laws lived in the small relocated rented apartment. However, once their government-subsidized housing assistance ended, they were forced to return to their home in the Gaza border region. Upon their return, Joseph’s post-traumatic symptoms intensified. These symptoms increasingly affected his daily life and included heightened anxiety and fear, intrusive memories of the gunfire and screams from October 7, nightmares about his sister and others who had been murdered, avoidance of going outside at night, refusal to watch news reports or recordings of the events, and an overall withdrawal from reminders of the attack. Moreover, the ongoing war and his re-exposure to the home where the traumatic events had occurred, combined with the proximity to the sounds of combat from Gaza in the present, exacerbated his reactions. His intrusive thoughts, anxiety, concentration difficulties, irritability, and avoidance behaviors intensified, leading to significant distress and impairment in his functioning and social relationships. His clinical presentation met the diagnostic criteria for Post-Traumatic Stress Disorder (PTSD) (American Psychiatric Association [APA], 2022).
Alongside his PTSD symptoms, Joseph exhibited a cluster of grief-related reactions associated with his sister’s death. His deep sorrow was accompanied by overwhelming longing that worsened over time, along with intrusive thoughts and mental imagery regarding the circumstances of her violent death, both while awake and in nightmares. He experienced persistent guilt over being able to save her, and that he had survived while she had not. Even though he recognized that these thoughts were not rational, he was unable to free himself from them. He constantly replayed in his mind the days when her fate was unknown, the uncertainty about whether the recovered body was truly hers, and the fleeting hope that she had “only” been kidnapped rather than killed.
The story of her death that he constructed in his mind left him in unbearable distress. He was preoccupied with her passing, avoiding looking at videos or photos of her, and refused to talk about her or their shared past. His self-created imagery was fueled by fragmented stories he had heard about others who had died that day. Paradoxically, the lack of precise details about her final moments gave room for persistent fantasies and recurring nightmares. This clinical picture corresponds to complicated grief (Rubin et al., 2008), now recognized as Prolonged Grief Disorder (PGD) (APA, 2022; World Health Organization [WHO], 2021).
Joseph’s clinical condition also included symptoms of depression, feelings of worthlessness, and suicidal thoughts. His home and community felt shattered, his future seemed uncertain, and he perceived himself as lost. In addition to his personal struggles, his wife and children needed him, but he felt incapable of fulfilling his responsibilities toward them, further exacerbating his guilt, shame and self-criticism. His trust in the military and governmental institutions was profoundly shaken, leaving him with a persistent sense of abandonment that had remained since the outbreak of the war.
The case presented brings with it many features of both bereavement and trauma. Within the clinical and research domains, there is growing recognition of the bidirectional relationship between trauma and grief, manifesting in a distinct syndrome known as “traumatic bereavement”. This syndrome underscores the overlap and mutual influence between trauma experiences and the bereavement process (Neria & Litz, 2004; Rubin et al., 2020).
In responding to both military and civilian exposure to traumatic bereavements, the diagnostic importance of identifying cases of complex trauma and loss and emphasize the necessity of developing targeted assessment and intervention programs. These programs aim to alleviate human suffering and reduce the risk of psychiatric disorders, with a particular focus on Post-Traumatic Stress Disorder (PTSD), Major Depressive Disorder (MDD), and Prolonged Grief Disorder (PGD) (APA, 2022; WHO, 2021). Such interventions should be grounded in a systemic and multidisciplinary understanding of trauma and loss, with special attention to the unique challenges posed by extreme traumatic circumstances. In the next section, we turn to the first of our assessment matrices, the Two-Track Model of Loss and Bereavement.
The Two-Track Model of Loss and Bereavement (TTMB)
The Two-Track Model offers an integrative approach that combines a focus on biopsychosocial functioning, including elements of stress, trauma, and life changes with equal attention to the ongoing interpersonal attachment bond with the deceased (Rubin, 1981, 1999; Rubin et al., 2012). This model provides a multidimensional framework for developing interventions in crises caused by interpersonal loss and has significantly contributed to research and clinical practice in thanatology, particularly within the Continuing Bonds paradigm (Klass et al., 1996; Klass & Steffen, 2018). The model conceptualizes the experience of loss as encompassing two parallel, distinct, yet complementary processes: the first addresses the impact of loss and/or trauma on biological, psychological, and social functioning including physiological, behavioral, cognitive, and emotional responses (Track I). These manifestations include anxiety, depression, changes in interpersonal relationships, alterations in meaning-making processes, as well as experiences of personal growth, positive transformation, and the promotion of psychological resilience.
The second track focuses on the characteristics of the ongoing bond with the deceased and the integration of the “death story” (Track II). The ability to manage an ongoing internal psychological connection with the deceased that serves as a source of solace and support is an important feature of relationships with significant attachment figures whether living or dead. Attention to the nature of the psychological connection with the deceased and the cognitive and emotional elements of the connection are important components of this domain.
The loss of a loved one under extreme circumstances (e.g. due to war, mass murder, terrorist attacks or abuse) is recognized as a significant risk factor for complications in adaptive grief processing. Such circumstances increase the likelihood of impaired functioning and the emergence of emotional or physical symptoms (Buur et al., 2023; Malkinson, 2001). Furthermore, experiencing life-threatening conditions concurrently with the death event further disrupts the recovery process, hindering the capacity for adaptive mourning that brings solace.
Traumatic circumstances involving the bereaved and/or the deceased heighten the risk for responses that meet criteria for PTSD on the one hand (Track I), and impact the “death story” in ways that hinder integration and acceptance of the death so as to allow connection with the deceased and the “life story” that had been present. Extreme circumstances can produce a “frozen” or flooding traumatic experience that fails to transition into a coherent narrative that reflects a cognitively and emotionally balanced experience. Instead, it may be perceived as an overwhelming and engulfing event with a fragmented narrative marked by intrusive emotions and thoughts. Moreover, avoidance or emotional detachment from the event’s story can also hinder adaptive grief processing. Both reactions obstruct access to memories of the deceased’s life and the relationship shared with them.
Accordingly, the application of the Two-Track Model of Bereavement in the assessment of response to loss examines adaptive and maladaptive responses across both tracks: Biopsychosocial difficulties and strengths on Track I, and the quality of the psychological relationship with the deceased and the processing of the loss narrative on the other. Each of these components plays a central role in evaluation and the development of personalized therapeutic interventions.
The primary objective of traumatic bereavement therapy, therefore, is to identify, assess, and support the promotion of adaptive mourning by addressing the patient’s core difficulties while mobilizing their unique resources. In other words, the therapeutic task is to create a balance between engagement in the bond with the deceased “the presence of the missing”, and reconnection with “life itself” (e.g., Neimeyer, 2016; O’Connor, 2022; Stroebe & Schut, 2010).
Multiple Losses and the Two-Track Model
Trauma affects the grieving process both when the bereaved has personally experienced direct danger and when the death occurred under traumatic circumstances—especially when both conditions are met simultaneously. These situations increase the risk of impaired functioning and symptomatic distress within the bereavement response (Track I). Additionally, horrific circumstances of death can render the “death story” traumatic, obstructing access to memories of the deceased’s life and the relationship shared with them (Track II). In such cases, the ability to integrate the “death story” into the bereaved’s personal narrative may be disrupted, delaying or even preventing the cognitive and emotional reprocessing of the bond with the deceased (Witztum et al., 2023).
Circumstances of multiple losses (see Figure 1) trigger simultaneous grieving processes that may manifest at varying intensities and paces. The presence of multiple, parallel focal points increases the risk of significant complications in processing multiple losses and may contribute to the development of a clinical profile consistent with PGD. Multi-focal grief process.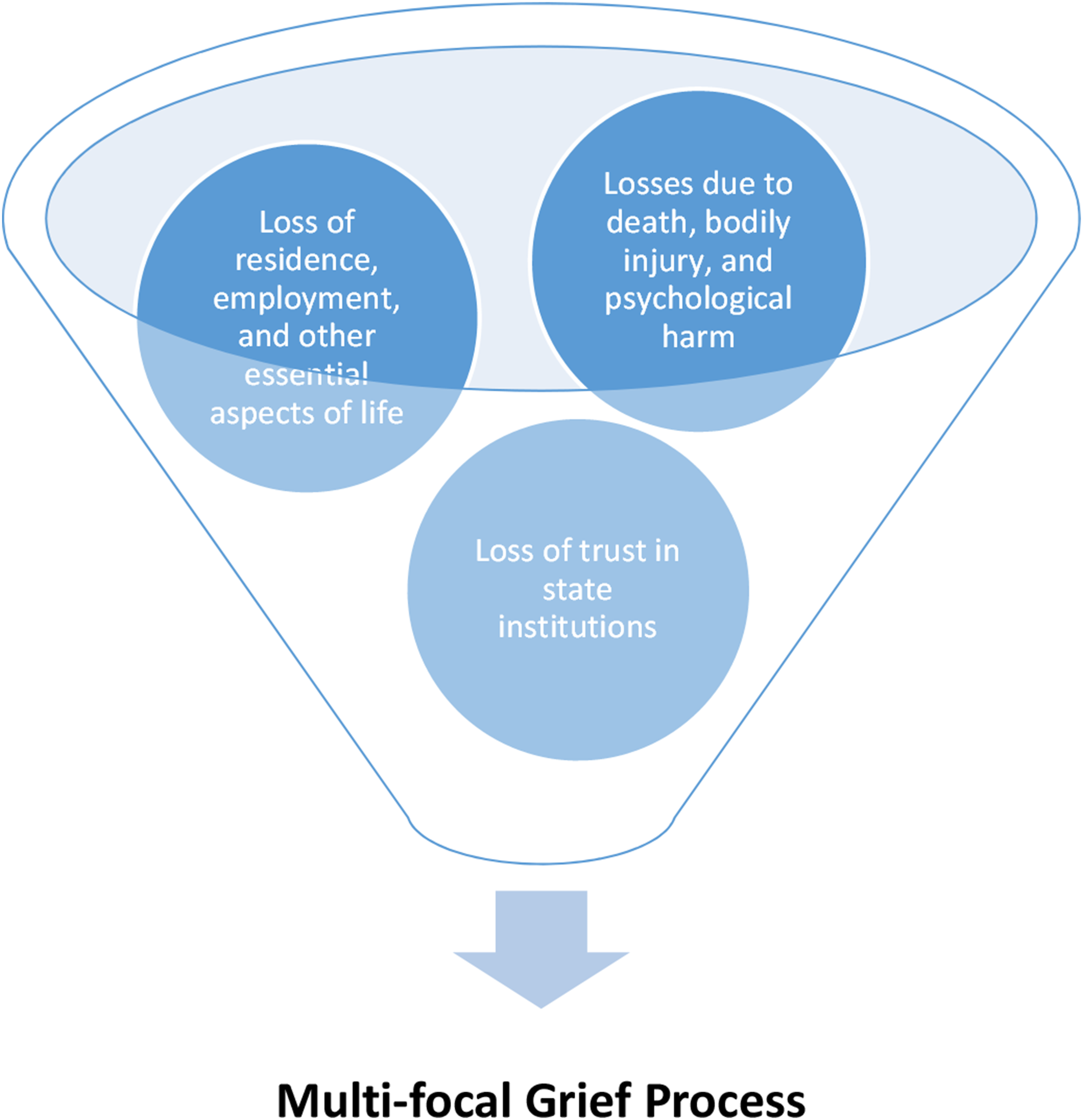
Furthermore, the multiplicity of challenges and domains of coping highlights the necessity of adapting and applying existing models and concepts to address this unique reality. Based on the Two-Track Model, it can be argued that in such contexts, Track II may encompass multiple, parallel focal points that require clinical attention. This underscores the importance of advancing theoretical conceptualizations regarding potential complications in grief and mourning processes, which may evolve into what could be termed “multi-focal PGD.” Additionally, it calls for the integration of insights from diverse theoretical approaches to facilitate a more comprehensive understanding of the phenomena described.
The following section will provide a concise overview of systemic-ecological approaches and their relevance to the assessment of multiple losses and traumatic bereavement, particularly in light of the events of October 7 and the subsequent war.
Multiple Losses and the Two-Track Model from a Systemic-Ecological Perspective
From a systemic perspective, “the whole is greater than the sum of its parts” (Bateson, 1962). Generally, systemic models emphasize the interactive component—the interrelationships between different elements of the system that both influence and are influenced by one another—in understanding various phenomena. The model proposed by Bronfenbrenner and Ceci (1994) focused on understanding human development within the context of an individual’s relationships with their environment.
This systemic-ecological perspective describes the reciprocal interactions between individuals and their surroundings, proposing that the environment is structured into four primary levels, ranging from the microsystem (the immediate environment) to the macrosystem (which encompasses broad cultural, economic, and social influences). The model conceptualizes the ecological environment as a circular system, placing the individual at its center, and asserts that an understanding of the interactions among these four environmental layers is crucial for comprehending human development over time (Bronfenbrenner & Ceci, 1994).
In mass trauma and multiple losses situations it is impossible to examine an individual’s experiences without considering the broader socio-political climate and contextual influences. That is, while an intrapsychic perspective remains valuable, an exclusive focus on it may overlook the full range of challenges faced by individuals coping with multiple and traumatic losses. Accordingly, a multi-systemic and ecological perspective has increasingly been applied in understanding responses to life transitions, bereavement, and trauma. This approach enables assessment and intervention planning that considers the individual within their personal, familial, community, and sociocultural contexts (e.g., Chachar et al., 2021; Franco & Malkinson, 2021; Hoffman & Kruczek, 2011; Kurdi et al., 2024).
The systemic-ecological perspective examines and highlights the bidirectional influences between different levels of the system—both as a coping resource in the aftermath of loss and trauma and in cases where the traumatic event disrupts and fractures these levels, necessitating a reevaluation of their interconnections. In other words, in a reality where multiple layers and systems—previously available as coping resources—have been profoundly impacted, individuals may find themselves without the supportive structures essential for adaptive grieving. Consequently, the remaining levels and systems in their lives require restoration to allow for a rebalancing of the ecological system and the promotion of adaptive mourning processes. As a paraphrase of Dorit Tzameret’s poem “The Wheat Grows Again” (1974), which poetically conveys the potential for post-bereavement growth, one might say metaphorically that just as the wheat requires time to regrow, so too must the farmer and the broader community undergo a process of healing and renewal.
Given these considerations, we propose that the integration of the Two-Track Model within a systemic-ecological framework holds substantial potential for providing a more holistic and comprehensive mapping of responses to multiple and traumatic losses. This approach aims to facilitate tailored therapeutic interventions that address the individual’s mourning process while simultaneously incorporating broader contexts. In other words, this model highlights how grief processing reverberates across all levels of an individual’s life—the personal, immediate social environment, community, and broader sociocultural system (see Figure 2). Systemic-ecological perspective.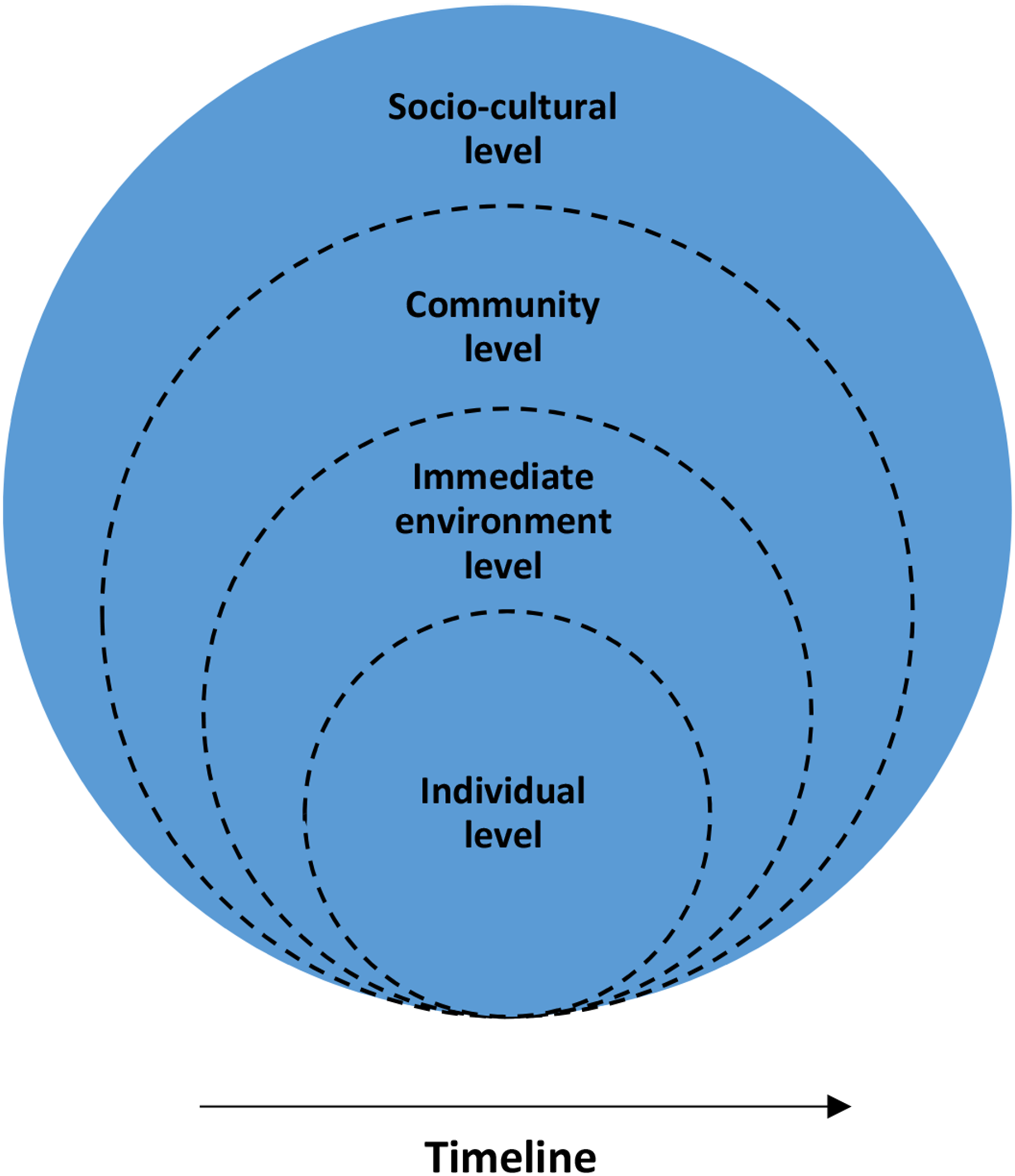
Assessment and Conceptualization toward Developing an Integrative Intervention Based on the Two-Track Model and the Systemic-Ecological Perspective
We now return to the case study described at the beginning of the article, attempting to evaluate Joseph’s difficulties, resilience, and resources in the wake of the multiple losses he experienced on and after October 7. This analysis is framed through the Two-Track Model and the Systemic-Ecological Perspective.
At the individual level, a Two-Track clinical picture emerges. Concerning Track I, what initially manifested as an Acute Stress Reaction progressed into Acute Stress Disorder and, over time, developed into full PTSD (APA, 2022; WHO, 2021). As described earlier, Joseph’s symptoms included hyperarousal, heightened vigilance, nightmares, avoidance behaviors, and re-experiencing of the traumatic event. His functioning was much limited by his anxiety, his difficulties with concentration, and his withdrawal from social connections. His work productivity was far below what it had been before the events described. This further sapped his sense of self that was registering failure to fulfill his role as husband, father, brother, son in the nuclear family, together with his withdrawal from community involvement and social elements of the workplace.
Regarding Track II, Joseph’s experience of loss began as an ambiguous loss due to the disappearance and uncertainty surrounding the potential abduction of his twin sister. This eventually transformed into a definitive loss upon the discovery and identification of her body. This loss triggered an acute grief response, which evolved into a complicated and traumatic bereavement process, eventually meeting the full diagnostic criteria for PGD (APA, 2022; WHO, 2021). His deep sorrow, his longing for her, his guilt over not having attempted to save her were ongoing features of his grief. Rumination about how she might have suffered before she died, and the ways in which this may have occurred resulted in a string of scenarios—and the only thing that was consistent in these variations was his belief that he should have been there to try to save her. His ongoing connection with his sister, expressed through accessibility to memories of their shared life and his ability to derive comfort from them, had not yet been established.
At the immediate environment level, Joseph has suffered an overwhelming number of losses. Beyond the unbearable death of his twin sister, he has also lost close friends, his home, the stability of his family structure, and his academic and professional security. Each of these losses represented severed threads in the rich tapestry of connection and meaning that had been heavily damaged by the magnitude and breadth of the assault on Joseph and his matrix of connections and psychological understanding of who he was and what he was a part of.
At the community level, Joseph lost neighbors and acquaintances and, more broadly, endured multiple losses associated with displacement and forced relocation. He was severed from the communal life and settlement where he had lived. Moreover, he later had no choice but to return to the very home where his life had been upended—his personal “Ground Zero”—which triggered retraumatization. In contrast to the immediate environmental level described above, the community level is less intimate, but its presence serves as container that allows for the formation and maintenance of the more personal connections. The partial destruction and month’s long evacuation of his township raised its presence as a background of safety. And when he had to return there, with his family and the portion of the community residents who were alive, able and willing to return, the communal experience was heavily shadowed by the memory of the attacks and the strong presence of the abducted and deceased as foremost in the minds of the residents.
Finally, at the socio-cultural level, Joseph was confronted with a national trauma stemming from the October 7 events and the ongoing war that continued to provide almost daily additions of countrymen, wounded and deceased, together with ongoing attention to the plight of the hostages. The hostilities that began on October 7 and the turmoil associated with them were experienced by Joseph as well as by many other citizens as occurring in the context of a major culture clash regarding the extent of changes to be made in the social contract of the country. The war exacerbated an unprecedented social divide in the country’s history. In this socio-political climate, Joseph perceived himself as betrayed, abandoned, and neglected by state institutions—such as the government, military, security services, and National Insurance Institute—despite his significant contributions to the country, which was supposed to ensure his and his loved ones’ safety. Here too, there was a string of non-death losses that served to breach another level of his containers of safety and meaning, and which was another cluster of things to grieve for.
What we have described here is a multifaceted and multilevel reality which at every level had brought with them an additional domain of things that were “lost” and which demanded recognition and a potential strand of grief work. We can all agree that any assessment of Joseph’s condition must address his grief process surrounding the loss of his twin sister who was a central attachment figure for him (Kosminsky & Jordan, 2024). However, it is most important to recognize the multiple tangible and symbolic losses — especially under traumatic circumstances related to war and terror — he has endured across various life domains, their associated grief processes, their reciprocal effects, and the unique clinical picture they create.
In other words, when grieving the death of a close person, Track II primarily focuses on the bereavement process and the reconstruction of a continuing bond with the deceased’s internalized presence. As can be seen based on Joseph’s story, in cases of multiple losses, the conceptualization of Track II must expand to include various losses and their distinct meanings for the bereaved individual. Furthermore, the manifestations of Track I in biopsychosocial dysfunction are also influenced by these numerous losses. Consequently, grief assessment and intervention planning must incorporate both tracks as expressed in the TTM as well as taking into account the multilevel systemic-ecological perspective in situations where losses are much more widespread and extend well beyond the focus on the death of an individual.
Thus far, we have applied the principles of clinical assessment based on the Two-Track Model and the Systemic-Ecological Perspective to Joseph’s case study. We now briefly explore possible therapeutic interventions for traumatic bereavement and multiple losses.
Therapeutic Interventions for Traumatic Bereavement and Multiple Losses
Increasingly, therapeutic approaches adopt an integrative perspective that evaluates both the facilitators and obstacles of the grief process, selecting intervention modules tailored to the individual bereaved client (e.g., Kaplow et al., 2023; Niemeyer, 2022; Saltzman et al., 2017; Shear et al., 2022; Timulak & Keogh, 2022). In a previous publication, we proposed a multidimensional and integrative intervention model applicable to cases similar to those under discussion (Malkinson et al., 2024).
This intervention model comprises various modules that can be flexibly combined according to the treatment goals: psychodynamic, cognitive-behavioral, and strategic components. Additionally, we outlined three stages serving as a “roadmap” for implementing the intervention and the core themes characterizing each stage: (1) assessment (elaborated upon in this article), establishing the therapeutic alliance, and setting shared goals; (2) modular intervention tailored to the focal points of treatment; and (3) preparation for termination and separation.
Ultimately, regardless of the specific therapeutic approach, we recommend a flexible intervention strategy tailored to the individual who experienced mass traumatic losses and his or her unique “death narrative” to enable a healing adaptive grieving. Additionally, it is essential to acknowledge that the therapist, may be immersed in the same apocalyptic reality as their client. As such, special attention must be given to self-reflection and awareness of the therapist’s personal experiences—acknowledging that the national trauma has affected them across different levels and systems—as they engage in therapeutic work.
Summary and Conclusions
This article has outlined an integrative approach in the context of war for clinical assessment of trauma, grief, and multiple losses—whether resulting from the death of significant others or from tangible and symbolic losses not necessarily associated with death. Tragically, this complex and multi-focal loss landscape has become highly relevant in the wake of the October 7 events in Israel, and the subsequent war. The assessment approach presented here is grounded in theory, research, and clinical practice, particularly drawing from the Two-Track Model of Bereavement and the Systemic-Ecological Perspective.
In this article, we sought to extend the discussion beyond the specific trauma, emphasizing the centrality of multiple losses among those seeking therapy following the October 7 events. When multiple losses are involved, Track II must be conceptualized more broadly to encompass the various losses and their unique meanings for the bereaved individual. Additionally, the biopsychosocial manifestations of Track I are influenced by these multiple losses. Accordingly, grief assessment and intervention planning must incorporate both tracks.
Finally, we wish to highlight concepts highly relevant to this discussion—concepts that we will explore in greater depth in a forthcoming article—namely, Post-Traumatic Growth (Tedeschi & Calhoun, 2004) and more specifically, Post-Bereavement Growth as an area requiring further exploration, development, and research. In other words, there is potential for adaptation, healing, and growth, which may be expressed across both components of the Two-Track Model of Bereavement and in the reconstruction of each systemic level in the lives of individuals coping with multiple traumatic losses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.