
Abstract
This study aimed to understand the drivers better to help minimise further risks of overtreatment for older people near the end of life (dysthanasia). A systematic scoping review of any publication types released in Medline, Embase, and Cochrane databases from January 2002 to January 2023 were used. Deductive thematic analysis was conducted independently and concurrently by paired reviewers. Risk of bias assessed for primary studies only using a modified version of the COREQ checklist. Twenty-one studies met the inclusion criteria. Determinants included healthcare system factors, patient-centered care, family and caregiver, and clinician perspectives. This review confirms that despite almost two decades of recognition of the potential harms of overtreatment near the end of life, society, patients, and health systems have a role to play in reducing and addressing the determinants. We offer a range of solutions for clinicians, health service managers, and members of the public to consider.
Introduction
The reality of widespread, non-beneficial treatments, procedures, and hospitalisations for people in the last stage of their natural lives has been well established for over a decade, to varying extents across countries and health systems (Cardona-Morrell et al., 2016; Downar et al., 2015; Jox et al., 2012). Such interventions can range; from administering intensive procedures that are not expected to improve survival, to repeat burdensome transfers from nursing homes to hospitals, (Szilcz et al., 2022), and overtreatments such as intensive care unit (ICU) admission that are against patients’ wishes or could potentially cause harm (Cardona et al., 2020; Lo et al., 2022). The questionable behaviours of extending life at all costs where the risks outweigh the benefits (Lo et al., 2022), are also known as dysthanasia when prolonging suffering leads to a bad death (de Menezes et al., 2009). Their extent is estimated for different specialties, part of the health services, or condition-specific subgroups. The practice continues and there is a knowledge gap in the in-depth identification of the drivers and proposed solutions for older multimorbid people near the end of life (EoL).
This article reports a sub-study of an umbrella review seeking to disentangle operational definitions, estimates, drivers, and potential solutions to non-beneficial or futile treatments near the EoL. It seeks to illustrate understanding, perceptions, and implications of end-of-life overtreatment modalities reported in hospitals and aged care facilities to sensitise clinicians on its undetected prevalence, enable timely recognition, and improve the EoL trajectory by reducing openings for dysthanasia.
Methods
We searched Medline, Embase, and Cochrane library for articles published in the past twenty years (January 2002 – January 2023) relating to people aged 60+ years receiving overtreatments in any level of the health system. The umbrella protocol is published (https://osf.io/bu54a) and the PubMed search strategy is presented in Supplemental 1 - Medline Search Strategy. The quantitative estimates and operational definitions are reported elsewhere. This paper deals with the qualitative studies or publications deemed includable if reporting definitions, drivers of overtreatment near EoL, and/or proposed solutions.
Study Selection and Data Extraction
Paired reviewers screened titles and abstracts to identify potentially eligible full texts. Full articles were screened for eligibility by one author and checked by another. Data extraction used a purpose-built standard form including publication characteristics (author, year, country, publication type, sample size, target population, description of overtreatment modality, drivers, potential solutions, and report conclusions).
Data Synthesis and Analysis
Using a systems evaluation theory framework (Renger, 2015) to identify the drivers and solutions, two reviewers took a deductive analysis approach and independently read all the full texts. One developed the coding without pre-determined themes to highlight text sections, terms, or concepts that answered the first research question on definition and drivers as emerging themes were identified. Two other authors revised the contents, and iteratively discussed and refined the themes to confirm the meaning was captured and their inter-relations understood. Risk of bias was undertaken only for primary studies using selected items of the Consolidated Criteria for reporting Qualitative studies checklist (Tong et al., 2007). The list of selected items is available in Supplemental 2 – Selected items from COREQ.
Results
Literature Search
From the database and grey literature search, 1,565 citations were generated. Following duplicate removal, title/abstract and full-text screening against eligibility criteria, 21 articles were included in the final review (Figure 1). Search results, screening process, and reasons for exclusion (PRISMA DIAGRAM).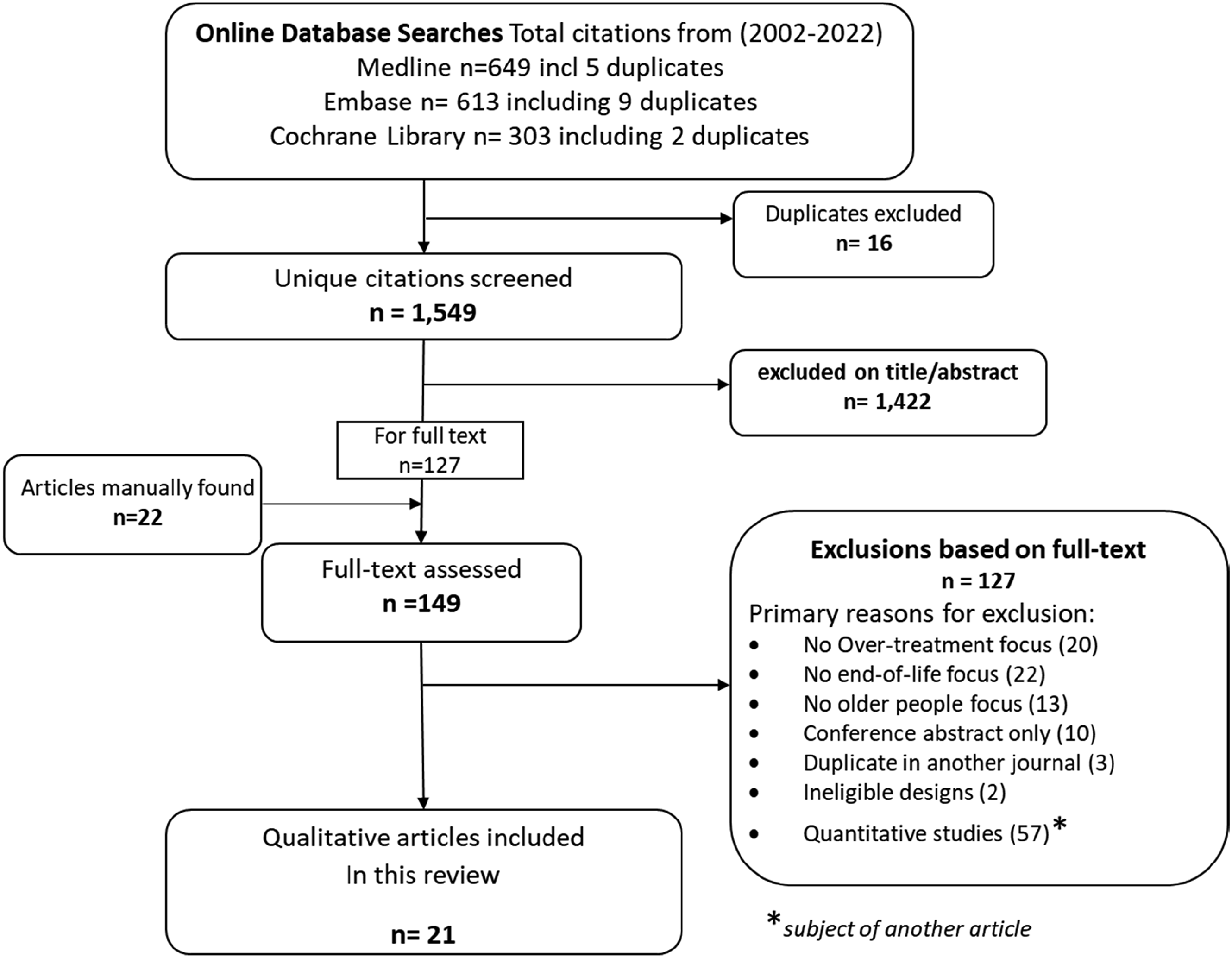
Study Characteristics
Characteristics of Eligible Studies (N = 21 Studies).
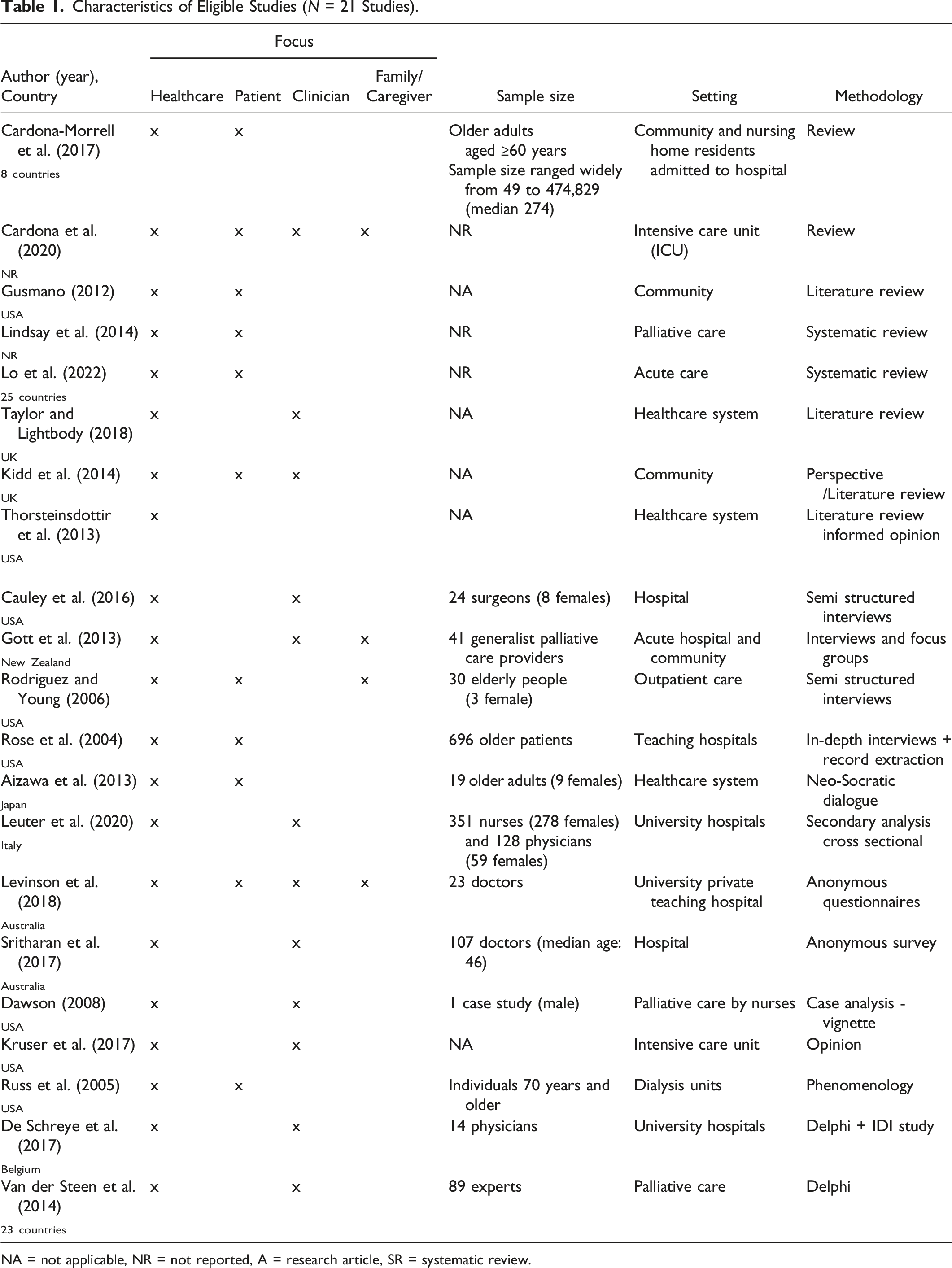
NA = not applicable, NR = not reported, A = research article, SR = systematic review.
Risk of Bias Assessment
Overall, the seven primary studies critically appraised (in-depth interviews, focus groups, and mixed methods including two Delphi consultations) had low risk of bias on the presentation of major themes or domains, exemplary quotes, and conclusions substantiated by findings. Unclear risk of bias was present in about half of the studies owing to lack of reporting of qualitative expertise of researchers or prior relationship with the study participants. High risk of bias was found in lack of discussion of saturation, which can be found in Supplemental 3 - Risk of Bias of eligible studies.
Determinants of Dysthanasia
Findings from the 21 included studies revealed four main themes determining instances of dysthanasia: healthcare system (20 articles), patient (10 articles), clinician (13 articles), and family / caregiver (5 articles), with all studies revealing more than one theme. A fifth overarching theme identified was the importance of shared decision-making and policy, bridging the preceding four themes. Each theme revealed contributing sub-themes, illustrated in a thematic map (Figure 2). Map of identified themes and subthemes determining instances of dysthanasia.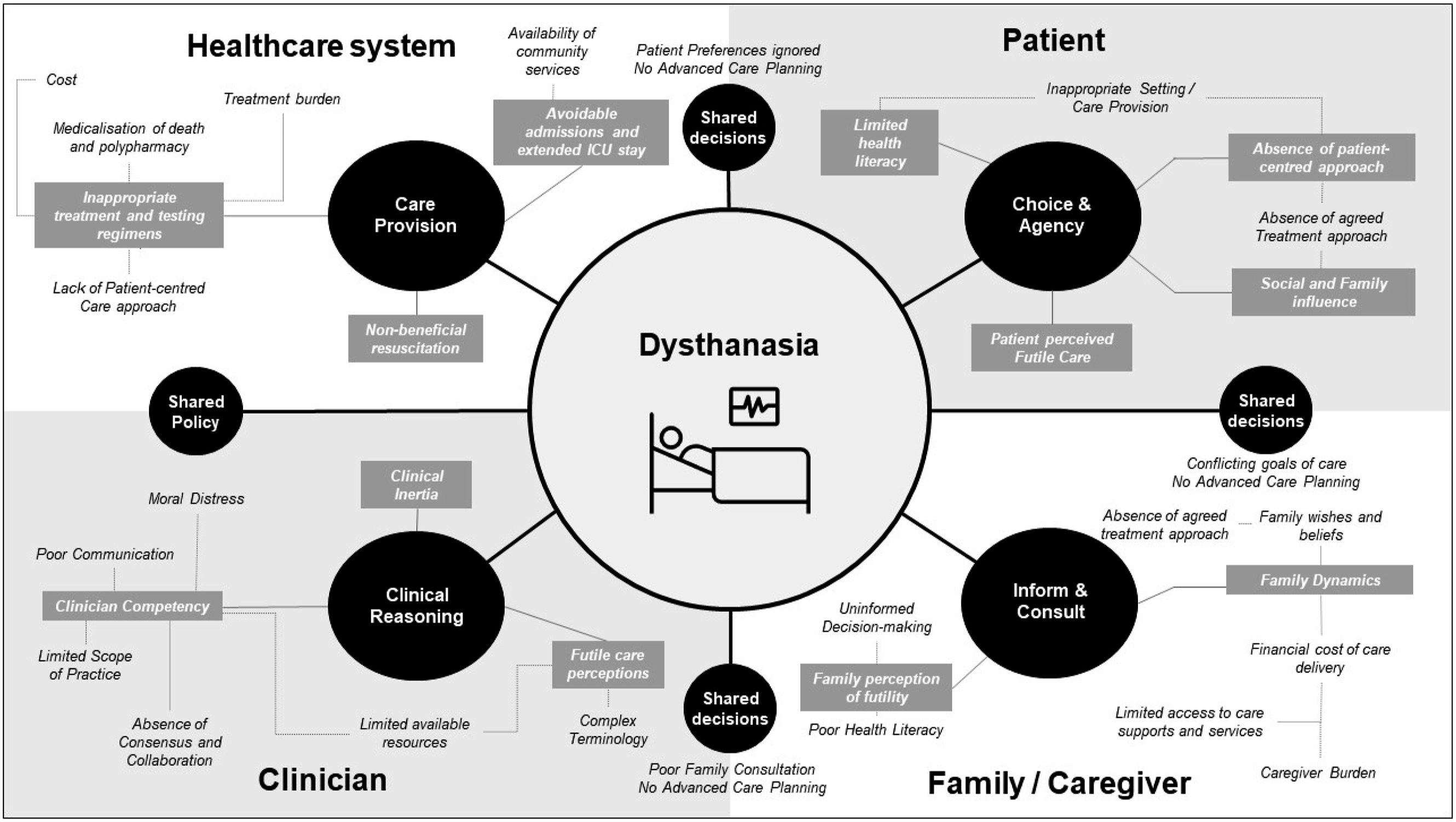
Healthcare System
Three sub-themes within the healthcare system were identified, each reflecting care provision and contributing towards the occurrence of dysthanasia:
Avoidable Admissions and Extended Stay in ICU
Avoidable admissions near the EoL may include situations where patients are admitted to the hospital for treatment that could have been provided in a community setting such as a hospice, or managed in their home if the resources existed to support this, or where the severity of the patient’s condition does not warrant a hospital admission (Cardona et al., 2020; Cardona-Morrell et al., 2017; Gott et al., 2013).
For nursing home residents, hospitalisation was deemed avoidable when actions in the aged care facility may have prevented the admission (Cardona-Morrell et al., 2017).This type of care can be inconsistent with patient and family values, as they may not accept the prognosis or may be in conflict with predictions made by medical professionals (Cardona et al., 2020). Such care can also be too aggressive, causing suffering for the patient, and may be cost-prohibitive (De Schreye et al., 2017). In these situations, it is deemed “inappropriate” to extend considerable resources when the benefits of treatment are unlikely to exceed the negative consequences (Lo et al., 2022).
A consequence of avoidable admissions included lengthy ICU stays; which were also a source of dissatisfaction, as the medicalisation of death has resulted in many ICU admissions deemed inappropriate from a medical perspective (Cardona et al., 2020).
Non-beneficial Resuscitation
The delivery of non-beneficial resuscitation, which is defined as cardiopulmonary resuscitation (CPR) attempts in which there is no likelihood of recovery, would appear to be a result of a failure of implementation rather than a failure of recognition (Levinson et al., 2018). This can happen when an order for “Do Not Resuscitate” (DNR) or “Not For Resuscitation” (NFR) has not been written by the medical team or results from a lack of attention to acute resuscitation planning. Medically futile CPR, defined as “an unacceptable survival rate after CPR”, can also be a source of non-beneficial treatment (NBT) (Kidd et al., 2014) but the term ‘futile’ has negative connotations and tends to be avoided in recent literature. The expression ‘non-beneficial treatment' has broader applications and is more acceptable but neglects the possibility that a medical intervention may also result in significant harm (Taylor & Lightbody, 2018). Another important consideration is the quality of survival after CPR. Post-CPR survival may be poor, with patients left with significant physical and cognitive impairments.
Failure of advance care planning is another factor that can contribute to the delivery of non-beneficial CPR (Dawson, 2008). Issues impeding decision-making around CPR often relate to poor knowledge of the law, particularly around consent and confounding NFR orders with provision of palliative care (Sritharan et al., 2017). Such barriers to the completion of NFR orders may expose older adult in-patients to futile and burdensome resuscitation events. Timely recognition of dying is crucial to avoid non-beneficial CPR (van der Steen et al., 2014).
Inappropriate Treatment and Testing Regimens
Financial cost is a significant factor in the delivery of non-beneficial treatments at the EoL (Cardona et al., 2020). Non-beneficial surgery and burdensome surgery at EoL can lead to a lack of understanding of the limitations of life-sustaining therapies (Cardona et al., 2020; Cauley et al., 2016). Cascade effects, which are triggered by an inciting event such as the ordering of a diagnostic test, can lead to multiple subsequent interventions that proceed along an automatic cascade without anyone stopping to consider alternative actions. Unrecognised cascade effects contribute to unwanted intensive care. Patient care dictated by cascade effects can lead to the rapid accumulation of interventions, bypassing opportunities to consider the patients’ preferences and likely outcomes (Kruser et al., 2017). When underlying chronic illness cannot be fixed, it is possible that polypharmacy, medications for primary and secondary prevention of other illnesses (based on a non-palliative life expectancy), or those with no short-term benefit are potentially inappropriate for these patients (Lindsay et al., 2014).
Several invasive procedures, such as tube feeding, may not prolong overall survival and reduce quality of life (Cauley et al., 2016; Gusmano, 2012). Intensive or burdensome medical intervention to prolong life in chronic critical illness can cause suffering for the patient (Kruser et al., 2017). The question of how treatment ends, and through whose agency, is a significant consideration that hangs over the process and emerges often in patients’ narratives about living on dialysis. Treatment decisions are often made with insufficient attention to patients' perspectives and wishes, and age is an important consideration. Findings indicate that hospitalised, seriously ill, older patients receive more documented discussions about treatment limitation and less aggressive care than do younger adult patients (Rose et al., 2004). NBTs have been reported as wasteful and costly, compromising the availability of resources for more appropriate supportive care (Taylor & Lightbody, 2018; Thorsteinsdottir et al., 2013).
Patient
Four sub-themes related to patient choice and agency were uncovered, each contributing towards collective instances of dysthanasia:
Absence of a Patient-Centred Approach
During the dying process, the goals and choices of patients are often overlooked. In those cases, the majority of participants consider the question of inappropriateness in relation to their own understanding of a good death (Dawson, 2008; Levinson et al., 2018). Understandings of a good death are culturally rooted, and patients struggle to discern an end or outer limit to their situation (Russ et al., 2005). The extent to which patients addressed such concerns with their clinicians is not clear. Patients reported that questions received overly vague or obfuscatory responses. For example, a shake of the head or a deferral of the topic to some later date (Russ et al., 2005). “Inappropriate” end-of-life care was defined by accounting for patient preferences, protecting their wishes, and even those of the family and patient’s inner circle; which speaks to the importance of clear communication (Lo et al., 2022).
Limited Health Literacy
During care planning conversations there is also the issue of limited health literacy among older adult patients and the community as a whole: one example of this is perceptions about CPR. Community-living individuals aged 15–65 years also show poor understanding of language around CPR and overestimate its success (Sritharan et al., 2017). Patients holding the view that CPR will be successful would have no reason to raise the topic of resuscitation with their doctor. Older medical in-patients aged 75 years have been shown to not understand the language, context, and efficacy of CPR (Sritharan et al., 2017). Most patients erroneously estimated the CPR survival rate in their age group to be at 50% or better (Sritharan et al., 2017). Such lack of understanding of the limitations of life-sustaining therapies can result in a lengthy ICU stay (Cardona et al., 2020).
Patient Perceived Futile Care
For older adults near EoL, the goal is to avoid overly aggressive, burdensome, or futile treatment (van der Steen et al., 2014) which are in some cases unwanted by the patients, who generally prefer less aggressive treatments at the EoL (Cardona et al., 2020; Cardona-Morrell et al., 2017).
Social and Family Influence
Family and caregiver beliefs and perspectives were shown to influence patient choice and agency. A failure of patients to agree to goals of care with their family/guardians contributes to inappropriate EoL care (Lo et al., 2022), especially when patient/family values differ (Cardona et al., 2020; Cardona-Morrell et al., 2017). Doctors are reliant on patients and family to broach discussions around EoLcare (Sritharan et al., 2017). Yet a failure to ensure that patients are free from coercion when making choices has been directly attributed to subsequent inappropriate care (Thorsteinsdottir et al., 2013).
Family/Caregiver
Two overarching sub-themes were revealed within the family and caregiver realm. Each has underlying elements impacting the ability to inform and consult, contributing to instances of dysthanasia:
Family Dynamics
Complex medical trajectories and challenging family dynamics contribute to dysthanasia (Dawson, 2008). Reasons can be grouped into the following themes: caregiver burden, when family carers could no longer cope; the ‘rescuer culture’ of modern medicine; the financing and availability of community services; and practice within aged residential care. For example, the lack of qualified staff or difficulties accessing GP’s urgently (Gott et al., 2013).
There are also multiple barriers to completion of NFR’s, including the family’s wishes, being time poor, the diffusion or deferral of responsibility, and poor documentation (Levinson et al., 2018). Experts, however, are not the only stakeholders in efforts to define medical futility or to decide whether to institute, withhold, or withdraw treatment: particularly the types of treatment that can be interpreted as either life-sustaining or death-prolonging interventions. Patients and family members or surrogate decision makers are also stakeholders (Rodriguez & Young, 2006). Conflicting goals of care between families and clinicians and absence of advance care planning leads to inappropriate care such as insistent requests for hospital admission, not accepting prognosis/conflict with prediction, and incongruence with patient/family values (Cardona et al., 2020; Cardona-Morrell et al., 2017). Additionally, there may be a lack of consultation with the patient or a lack of control by the patient’s family in these situations, as well as inadequate communication between medical professionals and patients/families.
Family Perception of Futility
When a family’s prognostic understanding is not established before an emergency, communication difficulties inherent in EoL care for ICU patients and their families can be a major issue (Cauley et al., 2016; Dawson, 2008). Overtreatment of patients in the ICU when hope of improvement has diminished is also a source of dissatisfaction (Dawson, 2008). The reason for dissatisfaction may be that patients or family members do not agree with the care plan, or they may feel that their needs are not being met by the medical team.
Patients and families are also unlikely to raise the topic of CPR with their physician if they are not familiar with the language used, not exposed to community discussion, and overestimate the effectiveness of CPR (Sritharan et al., 2017). The term ‘futile’ is often perceived as a value judgement implying ‘there’s nothing more that can be done’ or ‘we are giving up’, causing misunderstanding and distress to family members in particular (Taylor & Lightbody, 2018). It is this perception that gives the word ‘futile’ its pejorative meaning independently of its definition. There is a failure to help patients and families anticipate the likely trajectory of their illness condition and future circumstances (Thorsteinsdottir et al., 2013). From the patients and family/caregivers’ perspectives, curative or life-prolonging treatments that would not be consistent with the agreed goals of care can be defined as non-beneficial (Lo et al., 2022). Treatments that are counter to the patient’s or family/guardians’ wishes can also be deemed inappropriate (Lo et al., 2022).
Clinician
Three sub-themes within the identified clinician theme emerged, reflecting clinicians’ capacity for clinical reasoning, and contributing to instances of dysthanasia:
Clinician Competency
Inadequate communication between healthcare providers, patients, and their families is a significant theme that emerges in discussions of EoL care (Cardona et al., 2020). Clinicians may operate on a patient or subject patients to non-beneficial treatments to help families cope, even when clinicians do not believe the operation or treatment will benefit the patient (Cauley et al., 2016; Lo et al., 2022; Taylor & Lightbody, 2018; Thorsteinsdottir et al., 2013). This highlights the emotional and social needs of patients and their families becoming intertwined with the clinical parameters of care. Clinicians have reported moral distress when finding themselves in a position of delivering care that is inappropriate because the goals of care are unrealistic and unattainable (Taylor & Lightbody, 2018).
Clinical Inertia
Another theme is the concept of clinical momentum in the healthcare system and its influence on the provision of unwanted care. A conceptual model of clinical momentum describes how an automatic link between an abnormal clinical sign, symptom, or diagnosis and an intervention can build over time (Kruser et al., 2017). For patients who remain critically ill the accrual of multiple interventions reinforces this link: the probability of a favourable outcome decreases. This momentum can obscure the ability of patients, families, and clinicians to consider long-term outcomes and may lead to care that is outside the limits of professional standards, negligent, or compromising the clinician’s integrity (Kruser et al., 2017; Rodriguez & Young, 2006; Russ et al., 2005). The overall trajectory and ethos of treatment, framed as life saving and life-prolonging, may also operate to deny and conceal ends, making them practically, if not linguistically, inexplicable. For example, doctors believe that NFR orders alter the quality of care delivered by nursing staff (Sritharan et al., 2017).
Futile Care Perceptions
Futility refers to treatment that will provide no benefit to a patient, or where the burdens of treatment will outweigh the benefits. It can be considered both quantitatively, in terms of the chances of survival, or qualitatively, in terms of the quality of life of the patient if they do survive (Taylor & Lightbody, 2018).
Additionally, futility can be considered from a broader perspective that incorporates system factors, social, and family dynamics (Cardona-Morrell et al., 2017). The following factors need to be taken into account when discussing whether a treatment was acceptable and whether it should be implemented: effect on quality of life; emotional, financial and other costs; likelihood of success; and effect on length of life (Rodriguez & Young, 2006). The prevalence of futile treatment can range widely depending largely on non-clinical reasons; such as poor availability of alternative sites of care, or failure of preventive actions by other healthcare providers, family requests, or too late an admission to be of benefit (Cardona-Morrell et al., 2017). The definition of “end-of-life” varies depending on the context and the perspective of the person defining it (Cardona-Morrell et al., 2017). A person near the EoL is typically of advanced age, is frail, at risk of injury, and has an advanced incurable chronic condition or co-existing diseases that put them at risk of an exacerbation leading to hospital transfer (Cardona-Morrell et al., 2017). Futile care was also defined by clinicians as fixing an immediate problem in patients with underlying serious illness without focus on the outcome of treatment, including mortality and quality of life. Such care is considered non-beneficial and a waste of resources (Cauley et al., 2016).
Policies that shift incentives, combined with lack of ethical transparency, create a perfect storm of a return to implicit dialysis rationing (Thorsteinsdottir et al., 2013). Futility for frail older adult patients with end stage renal disease loses sight of all four core principles of biomedical ethics: respect for autonomy, beneficence, nonmaleficence, and justice. A further common problem identified was the provision of futile care at EoL to people with dementia (Gusmano, 2012).
The discrepancy of clinical language versus general laymen’s language, difference in expected outcomes between clinicians and treatment recipients, and available resources to continue or escalate, lead to excessive or aggressive care inhibiting a peaceful death or prolonging the suffering of dying (Lo et al., 2022; Taylor & Lightbody, 2018).
Shared Decision-Making and Policy
An overarching theme of shared decision-making and policy was also revealed; this intersected the preceding four themes and provided an underpinning connection across identified determinants of dysthanasia. This overarching theme is evident across subthemes encompassing restrictive policies and services (Cardona-Morrell et al., 2017; Kruser et al., 2017; Rose et al., 2004; Thorsteinsdottir et al., 2013); a lack/failure of advanced care planning (Dawson, 2008; Lo et al., 2022; Rodriguez & Young, 2006; Taylor & Lightbody, 2018; Thorsteinsdottir et al., 2013); insufficient consideration of patient preferences (Cauley et al., 2016; Lo et al., 2022; Rodriguez & Young, 2006; Rose et al., 2004; Russ et al., 2005; Thorsteinsdottir et al., 2013) or patient/family suboptimal health literacy (Cardona et al., 2020; Cauley et al., 2016; Dawson, 2008; Sritharan et al., 2017; Thorsteinsdottir et al., 2013); poor family consultation (Cardona et al., 2020; Rodriguez & Young, 2006; Sritharan et al., 2017); and conflicting goals of care within families/caregivers (Cardona-Morrell et al., 2017; Dawson, 2008; Thorsteinsdottir et al., 2013).
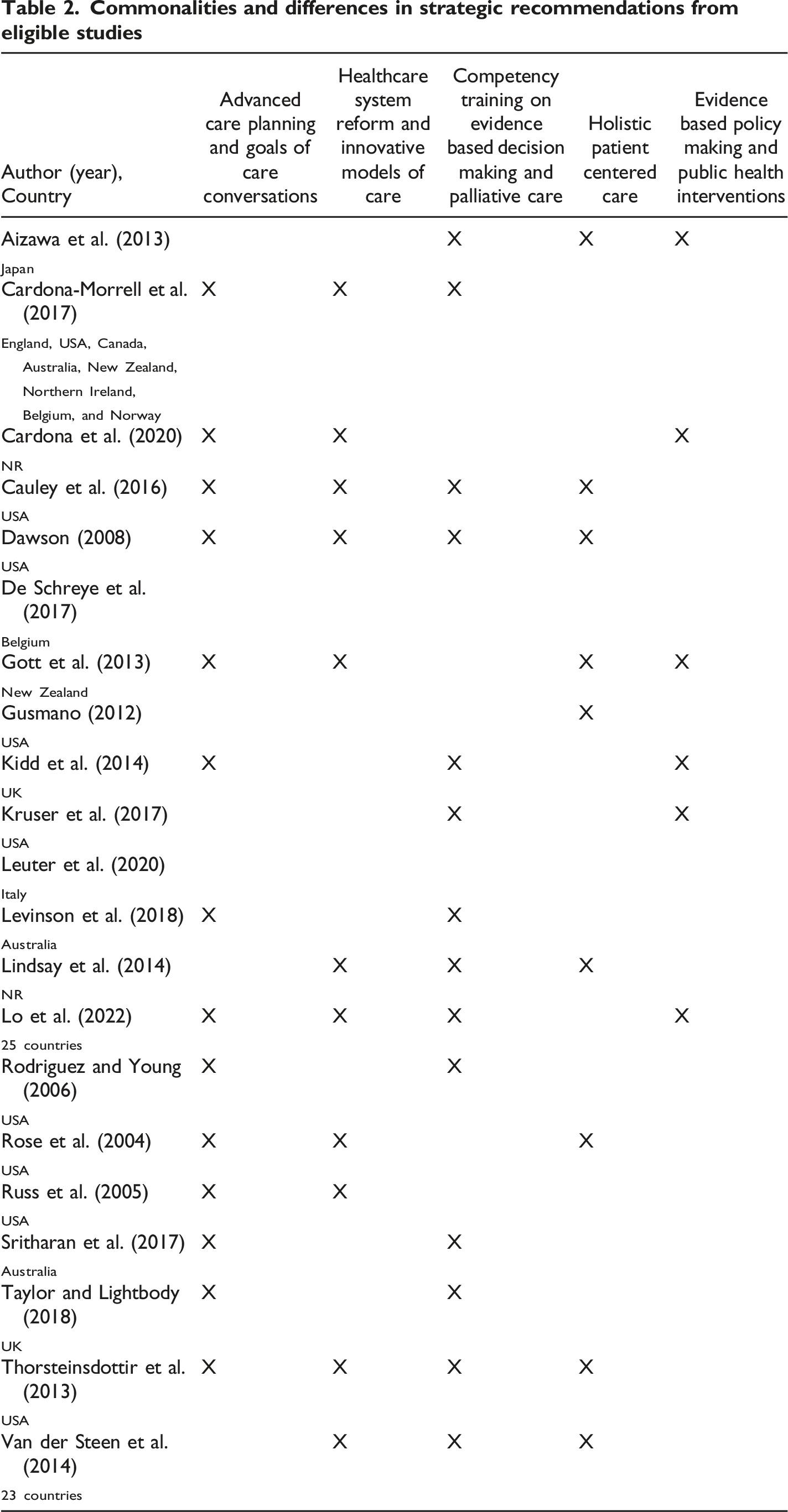
Recommendations to Reduce the Risk of Dysthanasia
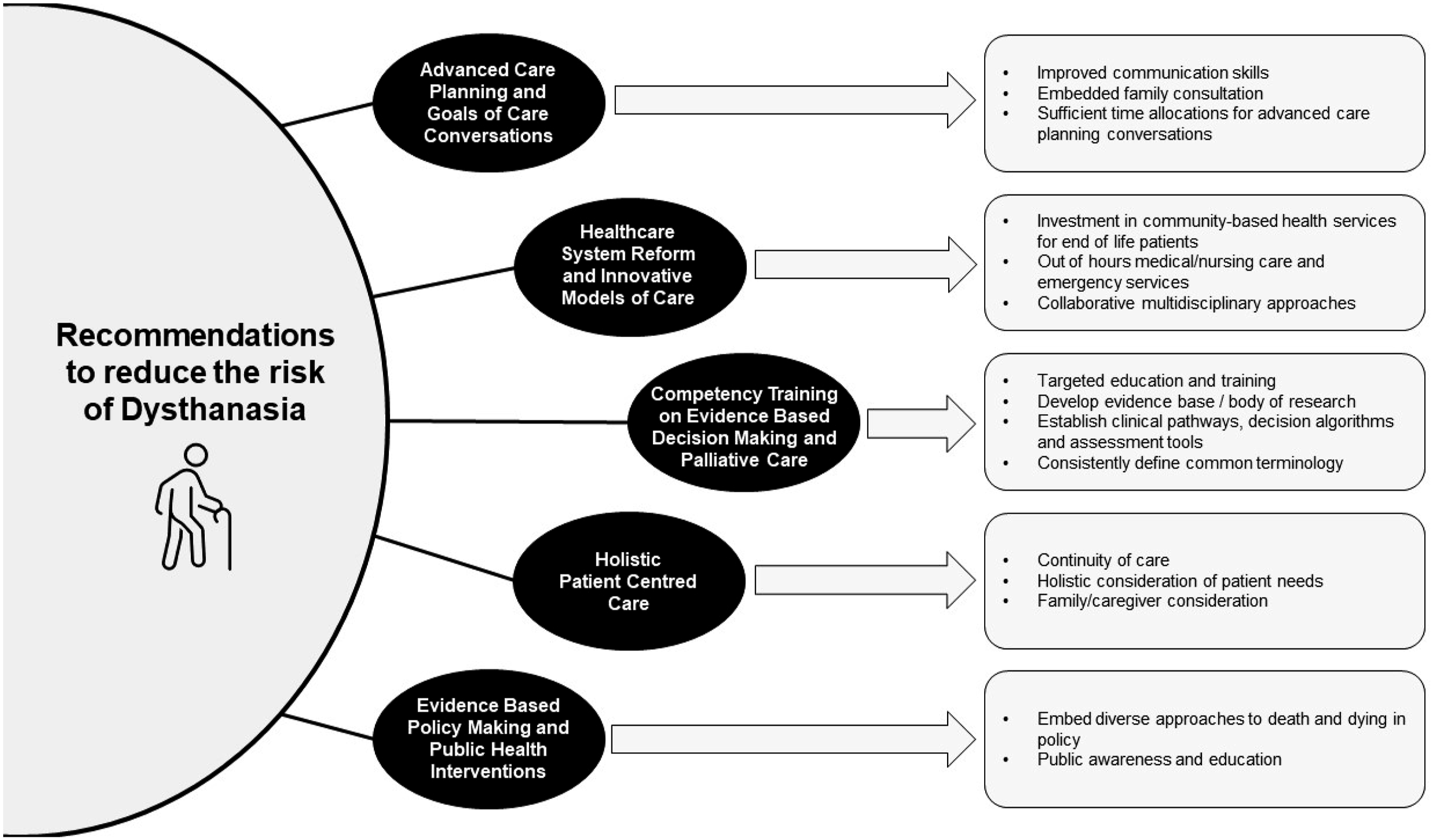
Findings from the included studies also highlighted five broad recommended actions which may reduce the risk of dysthanasia: Advance Care Planning and Goals of Care Conversations (14 articles), Competency Training on Evidence Based Decision Making and Palliative Care (15 articles), Healthcare System Reform and Innovative Models of Care (11 articles), Holistic Patient-centred Care (9 articles), and Evidence Based Policy Making and Public Health Interventions (6 articles). These recommendations are summarised in Figure 3 and Table 2. Recommendations to reduce the risk of dysthanasia.
Advance Care Planning and Goals of Care Conversations
Clinicians require improved skills and sufficient time to engage in vital conversations with patients and their families to improve shared decision making, advance care planning, and, in turn, improve the potential outcomes for patients and families. Skills to facilitate vital conversations such as goals of care discussions (both early goals and late goals) involve uncovering values, conducting family conferences, and offering prognostic information (Cardona et al., 2020; Cauley et al., 2016; Kidd et al., 2014; Levinson et al., 2018; Lindsay et al., 2014; Lo et al., 2022; Rodriguez & Young, 2006; Rose et al., 2004; Sritharan et al., 2017; Taylor & Lightbody, 2018; Thorsteinsdottir et al., 2013).
Healthcare System Reform and Innovative Models of Care
Across multiple articles a key component of strategies suggested to reduce hospitalisation of older adults near EoL was reform to the health care system through further investment in community-based health services as alternative sites to hospitals for managing EoL patients. Areas for further investment included out of hours medical and nursing care and community-based emergency services (Cardona-Morrell et al., 2017). That inadequate provision of support to family carers of people with palliative care needs can result in hospitalisations has been widely reported and lends weight to the argument to strengthen community-based supports (Gott et al., 2013). Further collaborative and interdisciplinary approaches in determining best care were suggested, such as surgical/ palliative care teamwork (Cauley et al., 2016) and reaching consensus across practitioner groups through multidisciplinary meetings (Lo et al., 2022). Changes to clinical culture and structures that help prepare a patient for death (Russ et al., 2005) were recommended: for example, avoiding the assumption that life extension is the only benefit to be considered (Thorsteinsdottir et al., 2013).
Competency Training on Evidence Based Decision Making and Palliative Care
Numerous authors advocated the increased application of evidence based palliative care practice by health workers as well as continued education and training to improve clinical decision making and prognostication. Cauley et al. (2016) suggested that more work is needed to develop robust data on patient-oriented outcomes after surgery, to familiarise surgeons with prognostic tools for seriously ill patients, and that surgeons would benefit from basic palliative care education to better fulfill their role as primary palliative care providers specifically in areas of perioperative discussions, decision management, and goal setting. Dawson (2008) suggested care providers need clinical pathways, decision algorithms, and assessment tools to successfully integrate palliative care within the ICU. Finally, Kidd et al. (2014) proposed that a deeper understanding and common terminology about the concept of futility and additional influences on the resuscitation decision-making process were important: such improved understanding of medical futility and other contributing factors when making do not attempt CPR orders would help to ensure that clinicians make appropriate and thoughtful decisions on whether to recommend resuscitation in a patient.
Holistic Patient-Centred Care
Authors advocated for holistic patient-centred care, including calling on practitioners to provide increased continuity of care and highlighting that having a historical understanding of the patient’s condition and treatment course is important in determining ongoing treatment options (Cauley et al., 2016). Responding holistically to the medical, emotional, social, and spiritual needs of dying patients (Dawson, 2008) was strongly advocated along with adjusting practices and approaches to care delivery according to local, patient, and family cultural practices. An example provided was to consider a family’s cultural sensitivities around treating intake problems and tailor information to better meet the unique needs of families in these circumstances (van der Steen et al., 2014). The important role of family in contributing to best care delivery was highlighted in severe dementia patients where distinguishing between sources of discomfort (e.g., pain or being cold) is facilitated by integrating views of caregivers (van der Steen et al., 2014).
Evidence Based Policy Making and Public Health Interventions
Kruser et al. (2017) suggested that addressing the problem of unwanted EoL medical care requires a comprehensive understanding of the processes and patterns that promote such care. However, diversity is not reflected in current policy, and indeed, it can be argued that there is a culture clash between policy and societal views of the role of acute hospital at the EoL: which clash is shaped, in part, by the wider forces of medicalisation. Some articles made recommendations such as: greater public awareness and education campaigns, promoting awareness and education of what constitutes non-beneficial treatment, and appropriate decision making at EoL (Lo et al., 2022). Improving education for older adults may lead to more informed decision making (Kidd et al., 2014). Cardona et al. (2020) argues for public health interventions such as enhancing families understanding of the consequences of inappropriate ICU care either before admission to ICU or via public information campaigns.
Discussion
This review documents four different drivers of overtreatment for older people near the EoL, patients, their families, clinicians, and healthcare system factors. The complexity of potentially harmful overtreatment calls for multifaceted solutions. Multiple countries engage in non-beneficial treatments. Lo et al. (2022) suggests that the problem persists, and it is perceived from differing perspectives by those affected by it and those delivering it. Some recent studies corroborate earlier findings from the last decade on drivers of dysthanasia (Fleming et al., 2016; Tjernberg & Bökberg, 2020), suggesting that interventions have not achieved a reassuring reduction.
Shared decision making plays a crucial role in the healthcare system, particularly when it comes to older adults and complex medical decisions. Involving patients, clinicians, and family/caregivers in the decision-making process empowers all involved to actively participate in caring for the older adult and helps to ensure that the older adults’ values, preferences, and goals are taken into consideration. Older adults often face multiple chronic conditions so complex treatment options with shared decision making becoming even more critical in this process.
Dysthanasia is a complex and sensitive issue that requires careful reflection and open dialogue between all abovementioned stakeholders. By engaging in meaningful discussions, older adults can gain a better understanding of their conditions, potential treatment outcomes, and the associated risks and benefits. An Australian group has developed a web-based interface for clinicians to guide this conversation with patients and families of patients including the estimated patient risk of death, their personal values, and treatment preferences for chronic kidney disease and dementia in preparation for decision-making (Cardona et al., 2023). This collaborative approach fosters a sense of autonomy and enables older adults to make informed choices aligned with their personal values, resulting in improved satisfaction with care and potentially better health outcomes.
Additionally, investments in research and innovation are crucial to advance knowledge in this topic and develop evidence-based interventions and strategies to improve the health and well-being of older adults (Abdi et al., 2019; Hao et al., 2020). By prioritising investment in healthcare for older adults, we can address the unique needs of this population and strive to achieve optimal quality end of life for older individuals.
Strengths
This review incorporated the perspectives of the healthcare system, patients, family/caregivers, and clinicians. Collectively, the studies identified in this review span 25 countries, suggesting that the identified themes and recommendations have widespread/international relevance and application.
Limitations
We acknowledge that the treatment at EoL is not specific to older people. However, we report them as they derive from studies focusing only on older adults. A limitation of this review is the publications were limited to English language and included primary studies as well as perspective, opinion, and vignette analyses.
Future Directions
The findings underscore the significance of advance care planning, healthcare system reform, competency training, holistic patient-centred care, and evidence-based policy and public health interventions. Implementation of these strategies has the potential to improve end-of-life care outcomes and enhance patient and family experiences. Further research and collaboration among healthcare professionals, policymakers, and researchers are necessary to translate these recommendations into effective interventions in order to provide information and appropriate support and resources to older people in their decision-making process near EoL.
Conclusion
This review provides an up-to-date overview of the identified themes and sub-themes contributing to dysthanasia, emphasising the importance of shared decision-making and policy in addressing this issue. The findings highlight the need for improvements in healthcare systems, patient-centred care, communication between clinicians and patients/families, and support for caregivers. A range of solutions for addressing these determinants are also proposed to reignite efforts to reduce instances of inappropriate prolongation of life and promote more compassionate EoL care.
Supplemental Material
Supplemental Material - Overtreatment of Older People Near End of Life: A Qualitative Scoping Review of Modalities, Drivers, and Solutions
Supplemental Material for Overtreatment of Older People Near End of Life: A Qualitative Scoping Review of Modalities, Drivers, and Solutions by Samantha Fien, Emily Plunkett, Daniel Wadsworth and Magnolia Cardona in OMEGA - Journal of Death and Dying
Footnotes
Acknowledgements
We thank Dr David Lim for his insights into our early stage of thematic analysis planning and our hospital librarian Sarah Thorning for assistance refining the search strategy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Dr Wadsworth is supported by a Postdoctoral Research Fellowship from Manna Institute, a Commonwealth-funded institute. All other authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.