
Abstract
Suicide has been a serious international public mental health problem and is one of the top twenty leading causes of death worldwide. This study aims to investigate the impact of social expenditure on suicide deaths in Turkiye as a developing country from 1982 to 2019. The Bounds Testing Approach to Cointegration and Autoregressive Distributed Lag (ARDL) methods were used. The results indicated that social expenditure has a statistically significant and negative effect on total suicide and female suicide deaths, but it has a statistically insignificant and negative impact on male suicide death. The contribution of this study is to examine for the first time whether social expenditure has an impact on total, female, and male suicide mortality in Turkiye. Policymakers should regard increasing social spending in the government budget to prevent suicide deaths in Turkiye.
Introduction
Suicide has been a serious international public health problem and remains one of the leading causes of death worldwide. Every year, more than 700.000 people worldwide lose their lives due to suicide (WHO, 2023). Although suicide has been a global public health issue, close to 80% of suicides occur in low and middle-income countries, where approximately 84 % of the world population lives (WHO, 2019). Thus, suicide can be considered one of the most critical mental health problems in developing countries.
The Sustainable Development Goals (SDGs), established by the United Nations, aim to address global challenges and promote sustainable human development. They consist of 17 global goals designed to achieve a better and more sustainable future for all, addressing issues such as poverty, inequality, climate change, and good health and well-being. Goal 3 (SDG 3) specifically targets ensuring healthy lives and promoting well-being for all ages. It includes a range of targets such as reducing maternal and child mortality, combating epidemics of communicable diseases, addressing non-communicable diseases, and ensuring universal health coverage. An important indicator within Goal 3 is Indicator 3.4.2, which focuses on reducing the suicide mortality rate. This indicator reflects the broader objective of improving mental health and decreasing the incidence of suicide through enhanced mental health services and preventive measures (UN, 2024).
Economic development and sustainable human development are intrinsically interconnected, as economic growth provides the essential resources needed to improve health, education, and overall living standards, which are foundational to human development. Sustainable human development ensures that economic progress translates into long-term benefits for the population, including enhanced mental health outcomes. In developing countries, insufficient social expenditure often exacerbates issues such as poverty and inequality, which in turn lead to increased stress and mental health problems. The correlation between a lack of investment in social infrastructure and services and higher suicide mortality rates underscores the urgent need for economic policies that prioritize sustainable and inclusive development. These policies aim to establish robust social safety nets, enhance access to mental health services, and tackle the socio-economic factors that influence mental health, ultimately fostering a healthier and more resilient population (Da Costa et al., 2022; Helliwell et al., 2020; Patel & Gonsalves, 2019; United Nations Development Programme (UNDP), 2019).
Understanding the complexities of suicide deaths involves consideration of both psychological and non-psychological determinants, with increasing attention given to the latter (Mental Health Europe, 2008; Yur’yev et al., 2012). Particularly crucial for vulnerable groups is social support, as they face challenges in accessing necessary resources to navigate social and economic upheavals, placing them at heightened risk of social isolation (Kyonne, 2013, 2019). Social protection programs, designed to mitigate economic and social vulnerabilities within societies, serve as a pivotal mechanism. Governments, as key stakeholders, play a crucial role in providing the requisite social support to address unmet needs.
Durkheim (1897) introduced the concept of social integration to elucidate variations in suicide rates across different societies, portraying suicide as indicative of the extent to which institutions bind individuals to broader social structures. According to Durkheim, social integration gauges the strength of an individual’s ties to society as a whole. MacRae (1985) further expounded on social integration, conceptualizing it as a contextual variable inherent in social systems, akin to social capital—a framework encompassing norms, habits, and attitudes within family, social, and community relations that promote collective action towards shared objectives (Coleman, 1988). Bonding social capital, characterized by support from family, friends, clinicians, and counselors during challenging life events, enhances psychological, social, and physical well-being (Myers, 1999; Thoits, 1995). It facilitates connecting individual behaviors with broader societal dynamics, particularly in how governmental institutions legitimize decisions—such as public social expenditures on welfare states—to address the psychological distress associated with suicide (Shneidman, 1993, 2001). Thus, the concept of social integration not only elucidates suicide rates across societies, but also informs policy strategies aimed at mitigating the underlying social and psychological contributors to suicide (Zimmerman, 2002).
Effective governments and public policies play a crucial role in shaping successful health systems. By prioritizing primary healthcare, enhancing service accessibility and equity, and focusing on the well-being of women and children, governments can significantly improve health outcomes. The specific government spending has been linked to positive impacts on maternal, child, and adult mortality rates, as well as life expectancy. Government expenditure on public services such as education and social assistance, for example through cash transfers and job training programs, can potentially lead to improvements in socioeconomic factors such as income and employment. This is particularly beneficial for individuals with low income. Consequently, such investments in the non-medical social determinants of health can have a positive impact on the overall well-being of individuals by addressing the conditions in which people are born, grow, live, work, and age (Lurie, 2002; Wilensky & Satcher, 2009).
The impact of public policies, particularly expenditures on public assistance, on suicide rates is a recent subject of academic scrutiny. One compelling rationale is that a strong governmental safety net could alleviate severe poverty and economic despair, which are often associated with higher suicide risks. Essentially, more generous welfare benefits serve to protect individuals from the unpredictable and severe impacts of market dynamics, potentially reducing the factors that contribute to suicidal ideation (Flavin & Radcliff, 2009).
The social causation theory asserts that individuals who lack adequate social, economic, and personal resources often face challenges in adapting to dynamic social environments. This inadequacy can lead to heightened stress levels associated with their precarious socioeconomic status (Aneshensel, 1992; Peng, 2009). In response to these challenges, strong national social welfare provisions play a crucial role by providing a stable safety net, which becomes especially vital during periods of economic downturns and social turmoils. Investments in welfare programs are pivotal as they enhance the accessibility and effectiveness of social support mechanisms. When welfare systems are well-funded and efficiently administered, individuals experiencing socioeconomic hardships are better equipped to cope with stressors and mitigate the negative impacts of financial instability. By alleviating financial and social strains, welfare programs reduce the psychological burden associated with economic insecurity and social exclusion. Consequently, individuals experiencing distress are less likely to resort to extreme measures such as suicide (Yur’yev et al., 2012).
The concept of permanent income suggests that individuals base their financial decisions not only on their current income but also on their expected future income over their lifetime. Hamermesh and Soss (1974) argue that higher levels of permanent income are associated with increased economic stability and security, thereby increasing expected cumulative lifetime utility—measuring satisfaction or well-being derived from consumption choices over time. However, sustained reductions in financial resources, often resulting from austerity measures, can create a lasting impression of diminished ability to maintain one’s standard of living. This perception of reduced economic security heightens feelings of anxiety, stress, and hopelessness among affected individuals, potentially increasing their susceptibility to suicidal behavior. Government expenditure plays a crucial role in bolstering this stability through investments in public goods such as education and social welfare. Therefore, an increase in government social expenditure, a decrease in austerity measures, and heightened personal economic security positively influences individuals’ mental health outcomes (Antonakakis & Collins, 2014, 2015).
The allocation of government expenditures to public services like healthcare, education, and social support has also the potential to significantly impact the socio-economic well-being of impoverished and marginalized populations. The relationship between social expenditure and public mental health is nuanced: an increase in social spending may reduce the risk of suicide by offering economic aid to vulnerable groups (Matsubayashi et al., 2020). Conversely, a decrease in social expenditure might elevate the risk of suicide by amplifying economic insecurity and reducing access to healthcare services (Kentikelenis, 2017; Stuckler et al., 2017).
When society lacks sufficient social assistance, individuals grapple with economic and social challenges. Insufficient social support impedes the swift acquisition of goods and services, hinders active participation in communal life, and diminishes the overall enjoyment of life (Yur’yev et al., 2012). Consequently, the magnitude and scope of social expenditures emerge as pivotal factors influencing population health, underscoring the essential role of governmental policies and resource allocation in shaping the mental well-being of communities.
Turkiye, positioned as a significant developing country, has coped with the complex issue of suicide death, making it a compelling case for investigating the correlation between suicide mortality and social expenditure. Serving as a pivotal crossroads between Europe and Asia, Turkiye holds membership in the OECD and has pursued accession to the EU, marking it as a country in the midst of dynamic geopolitical and economic shifts. A transformative economic evolution unfolded in Turkiye during the 1980s was catalyzed by the Stabilization Decisions of January 24, 1980. This pivotal moment marked a shift from an import-led industrial production model to export-oriented economic growth, ushering in trade liberalization and reshaping Turkiye’s economic landscape. The integration of Turkiye’s financial system with global markets in 1989, facilitated by the removal of exchange rate market barriers through Decree No. 32 on the Protection of the Value of the Turkish Lira, further entrenched Turkiye’s position in the world economy (Pamuk, 2009; Öniş, 2010).
The ensuing financial and trade liberalization processes witnessed since the 1980s resulted in a diminished role of the government in economic and social spheres. Economic problems and financial crises during the 1980s and 1990s prompted policymakers to adopt populist measures, leading to a substantial increase in welfare spending, particularly in social expenditures (Aybars & Tsarouhas, 2010; Eder, 2010). The political landscape shifted with the 2002 election, bringing a new administration that embraced free-market policies, introduced social assistance programs, and allocated substantial resources to social protection initiatives. Concurrently, government expenditures surged, with a notable focus on bolstering the healthcare system (OECD, 2021; Oguz, 2020).
Despite the implementation of social welfare programs to boost access to resources mitigating the adverse impacts of social and economic crises, suicide deaths in Turkiye have displayed fluctuations. Unique to Turkiye, in contrast to European Union (EU) and Organization for Economic Co-operation and Development (OECD) countries, which are predominantly Christian, suicide is deemed Haram, forbidden by Islamic faith. This religious perspective adds an additional layer of complexity to the understanding of suicide within the Turkish context, highlighting the interplay between social and economic factors in shaping the country’s experience with suicide mortality (Lester, 2006). Examining Turkiye’s intricate trajectory provides valuable insights into the multifaceted dynamics influencing suicide mortality trends in a rapidly evolving socio-economic and cultural landscape.
Literature Review
Over the last couple of decades, the relationship between social expenditure and health has garnered significant attention among scholars and policymakers. Studies in the existing literature on the socioeconomic determinants of suicide mortality have produced mixed evidence (Dunn et al., 2005; Kim & Jennings, 2009; Stuckler et al., 2010). Additionally, a plethora of studies have examined the nexus between social spending and mental health, yet the results remain inconclusive. These mixed and conflicting findings can be attributed to differences in sample populations and methods used. Considering these differences, empirical literature can be categorized into three distinct parts.
The first part focuses on the link between social expenditure and suicide mortality in the United States (US). This body of research explores how variations in social spending affect suicide mortality within the US context, providing insights specific to this country’s unique socio-economic environment. The second part encompasses studies conducted in developed nations, such as European countries and member nations of the OECD. These studies investigate how social expenditure influences suicide deaths across a diverse range of economically developed countries. In the final part of this section, the literature specific to Turkiye is presented. This part provides a comprehensive review of studies examining the relationship between the unique social, economic, and political factors and suicide deaths in Turkiye.
Social Expenditure & Assistance and Suicide Mortality Nexus in the US
The US has witnessed a dramatic increase in suicide deaths over the last 20 years, prompting a comprehensive debate about the impact of social expenditure and social assistance on suicide mortality. For instance, Zimmerman (1995, 2002) examined the relationship between welfare expenditure and suicide mortality across the 50 US states and found that state welfare expenditure negatively affects suicide rates. Zimmerman (2002) reported that a $1 increase in states’ public welfare per capita expenditure leads to a decrease in suicide rates by 0.004 per 100,000 persons. Similarly, Minoiu and Andrés (2008) reconsidered the link between state welfare expenditure and suicide mortality in the US states, observing that state public spending and welfare expenditures significantly negatively affect suicide incidence. Additionally, Kim (2016) studied the 48 US states between 1979 and 1987, examining the relationship between public welfare education spending and suicide deaths, finding that additional public welfare education expenditure reduces suicide mortality. Flavin and Radcliff (2009) assessed the impact of public assistance per capita expenditure on suicide mortality in the 50 US states from 1990 to 2000, using the Ordinary Least Squares (OLS) regression technique. They found that per capita expenditure on transfer payments, medical benefits, and family assistance negatively influences state suicide deaths.
In a recent study, Rambotti (2020) examined the effect of social assistance programs and Earned-Income Tax Credits on suicide mortality in the 50 US states, using the Supplemental Nutrition Assistance Program (SNAP) as a measure of social assistance for the poor. Employing panel data two-way fixed effects technique, the study concluded that increased SNAP participation is associated with lower overall and male suicide deaths, with one standard deviation increase in SNAP participation correlating with a decrease of 31,600 suicide mortality. Furthermore, Gertner et al. (2019) analyzed the effect of minimum wages on suicide deaths in the 50 US states between 2006 and 2016. Using a panel data model with fixed effects, they found that a $1 increase in the minimum wage leads to a 1.9% decrease in the state’s overall suicide deaths. Similarly, Cylus et al. (2014) applied a panel fixed effect method and a negative binomial model to test the effect of unemployment insurance on suicide death in the 51 US states, finding that unemployment benefit insurance negatively affects suicide rates. Conversely, Ross et al. (2012) explored the relationship between public mental health expenditure and suicide mortality in the 51 US states, finding no statistically significant impact of public mental health expenditure on state suicide deaths. In line with Ross et al. (2012), Zimmerman (1987) found that public social expenditure in the US states does not have a statistically significant effect on state suicide mortality.
In conclusion, the body of research examining this relationship between social expenditure and assistance and suicide mortality in the US offers a mix of findings that underscore the complexity of the issue. Studies by Zimmerman (1995, 2002) and Minoiu and Andrés (2008) provide evidence that state welfare expenditure can significantly reduce suicide rates. Conversely, studies like those by Ross et al. (2012) and Zimmerman (1987) present a different perspective, finding no statistically significant impact of public mental health expenditure and general social expenditure on suicide deaths.
Social Expenditure & Assistance and Suicide Mortality in the OECD and EU
The repercussion of social expenditure on suicide has also been debated in the existing literature for developed nations, with considerable interest directed toward European countries and OECD members. For instance, Baumbach and Gulis (2014) explored the impact of the 2008 financial crisis on health outcomes in eight European countries, particularly scrutinizing the effect of social spending on suicide mortality. They found that unemployment has a higher impact on suicide deaths in countries with lower social spending. Similarly, Stuckler et al. (2009) used multivariate regression methods to investigate the association between welfare programs and suicide mortality in 26 EU countries, providing evidence that a $10 increase in social expenditures per person in labor market programs causes a 0.038% decrease in unemployment-led suicides. Further supporting these findings, Yur’yev et al. (2012) examined the link between social exclusion and suicide deaths in 26 European countries, taking social exclusion as the predictor of suicide rates and measuring it as public social expenditure as a percentage of GDP. They concluded that social expenditures have a strong negative impact on both male and female suicide mortalities. Yur’yev et al. (2013) extended this research to cover 20 European countries from 1980 to 2015, finding that the correlation between social welfare spending and suicide deaths was negative for both genders in almost all countries, with positive correlations reported only for Ireland, Poland, and Spain.
In another study, Antonakakis and Collins (2014) investigated the association between fiscal austerity and suicide mortality in Greece over the period of 1968–2011. Using public expenditure to represent fiscal austerity, they found that reductions in public welfare expenditure did not affect female suicide deaths but did have gender-specific impacts on overall suicide deaths. Antonakakis and Collins (2015) expanded their analysis to Greece, Italy, Portugal, and Spain from 1968 to 2012, using panel bias-corrected least-squares dummy variable regression technique. They found that a 1% decrease in government expenditure in Eurozone periphery countries is estimated to increase suicide mortality among the 65–84 age group by 1%, with significant adverse effects on female suicide deaths as well. Recent studies further emphasize these patterns. Matsubayashi et al. (2020) applied a panel data fixed effect method to examine the link between public spending and suicide mortality across 47 municipalities in Japan from 2001 to 2014. They found that a 1% increase in per capita local public expenditure leads to a 0.2% decrease in both male and female suicide mortality. Matsubayashi and Ueda (2011) also examined the influence of national suicide prevention programs on suicide mortality in 21 OECD nations, demonstrating that such programs are particularly effective for youth and elderly populations.
In South Korea, Kyonne (2019) found that increased government expenditures correlate with decreased suicide deaths, while Cheong et al. (2012) concluded that regional social welfare spending has no statistically significant impact on regional suicide mortality in their study of 248 regions from 2006 to 2008. Park et al. (2009) similarly found no relationship between public social expenditure and suicide deaths in 27 OECD countries. From a different perspective, Reeves et al. (2015) examined the nexus between social protection and suicide incidence in 20 European countries from 1981 to 2011. They found that while social protection per person has no modifying impact on the unemployment-suicide link, active labor market programs do influence this relationship.
To sum up, the literature on the impact of social expenditure and assistance on suicide deaths in developed countries presents mixed findings. While several studies indicate that increased social spending, especially in welfare and labor market programs, can reduce suicide mortality, others find no significant effect.
Socioeconomic Determinants of Suicide Deaths in Turkiye
The empirical research on suicides in Turkiye has predominantly centered around socioeconomic determinants such as income, unemployment, divorce, urbanization, and alcohol consumption. However, there’s been a significant oversight regarding the impact of social expenditure on suicide mortality. Several studies have investigated the unemployment-suicide mortality relationship along with other socioeconomic determinants. For instance, Kutbay and Buyrukoğlu (2018) analyzed the dynamic relationship between tax burden, unemployment, divorce, and suicide deaths in Turkiye from 1974 to 2016, utilizing various econometrics methods such as Johansen Cointegration Test, Granger Causality Test, OLS, and Vector Error Correction Mechanism (VECM). Their findings indicate a positive relationship between unemployment and suicide mortality, with a notable increase in suicide rates with higher unemployment and divorce rates. Similarly, Alptekin et al. (2010), Bayrak (2018), and Tunalı and Özkaya (2016) explored the link between suicide deaths and unemployment, establishing a causal relationship between the two. Also, Topbaş (2007) confirmed this causality, emphasizing the impact of unemployment on suicide mortality in Turkiye. Furthermore, various studies have examined the role of economic growth, typically measured by GDP or GDP per capita, in suicide mortality. Durğun and Durğun (2017) found a unilateral causal relationship between GDP per capita and suicide deaths, indicating that an increase in GDP per capita leads to a rise in suicide mortality. Akyuz and Karul (2023) investigated the impact of industrial production, inflation, and investment on suicide mortality in Turkiye using Fourier cointegration tests and dynamic ordinary least squares regression. They found that industrial production and investment significantly reduce suicide mortality, whereas inflation is associated with a significant increase in suicide mortality. These findings underscore the critical role of macroeconomic factors such as industrial production, inflation rates, and levels of investment in shaping societal conditions and influencing psychological well-being, which contribute to fluctuations in suicide rates over time.
Other socioeconomic factors such as urbanization, divorce, and alcohol consumption have also been investigated. Altinanahtar and Halicioglu (2009) highlighted the significant impact of urbanization on suicide deaths, surpassing that of income and liquidation. Varol and Karagöz (2020) explored multiple determinants including alcohol consumption, urbanization, and unemployment, finding significant associations with suicide mortality. Additionally, other studies have examined the impact of economic crises on suicide deaths in Turkiye. Ayla et al. (2019) found that economic disruptions during crises have a statistically significant effect on suicide mortality, while Atila and Çelikkaya (2020) identified a causal relationship between economic crises, GDP fluctuations, and suicide deaths. Furthermore, Karasoy (2024) examined the impacts of uncertainty and the Misery Index on suicide mortality. This study concluded that both uncertainty and the Misery Index are significant factors contributing to increased rates of suicide deaths.
In summary, conflicting results were obtained across studies, indicating the complexity of the relationship between socioeconomic indicators and suicide deaths in Turkiye. Additionally, while a considerable body of literature exists on the socioeconomic determinants of suicide mortality in Turkiye, there is a gap in understanding the influence of social expenditure on suicide mortality. This paper seeks to fill this void by estimating the impact of social expenditure on suicide mortalities across genders from 1982 to 2019 using the Bounds Testing Approach to Cointegration and the ARDL method. This research makes a significant contribution in two key dimensions: firstly, it is the first attempt to explore the association between social expenditure and suicide deaths in Turkiye, shedding light on a previously unexplored aspect of this critical issue. Secondly, the study extends its focus across the entire liberalization period (1982–2019), emphasizing the role of social expenditures in shaping the dynamics of suicide mortality in Turkiye. This study disaggregates suicide mortality rates by gender, enabling a nuanced analysis of the distinct responses of male and female suicide deaths to social expenditure. The central hypothesis driving this research to be tested is that an increase in social spending causes a reduction in total, female, and male suicide deaths. By testing this hypothesis, this research aims to provide evidence-based policy suggestions, offering valuable insights into the potential role of social expenditure in mitigating suicide mortality in Turkiye
Data and Methods
Data
We selected the period of 1982–2019 based on data availability. Suicide deaths were sourced from the Turkish Statistical Institute (TURKSTAT) Database. Using the standard procedure, we converted the numbers of total, female, and male suicide deaths to crude suicide mortality rates per 100.000 persons. In light of empirical evidence highlighting distinct gender-specific effects of socioeconomic factors on suicide (Helliwell, 2007; Kposowa, 2000; Kunce & Anderson, 2002), we conducted separate analyses for males and females. The primary independent variable in our study is public social spending, represented as public social expenditure % of GDP and obtained from the OECD Social Expenditure Database. According to OECD’s definition, public social expenditure includes “cash benefits, direct in-kind provision of goods and services, and tax breaks with social purposes” (OECD, 2021). Targeting the amelioration of economic conditions among marginalized groups and facilitating income redistribution within societies, these social assistances play a pivotal role. Consequently, this variable stands as a robust proxy, offering insights into the degree of social equity and serving as a potent preventive measure against suicide deaths influenced by social, demographic, and economic factors (Minoiu & Andrés, 2008).
Model control variables included GDP growth, unemployment, alcohol consumption, divorce, and urbanization. Data on GDP, unemployment, and urbanization were taken from World Bank (WB), 2021, World Development Indicators (WDI) database, alcohol consumption was taken from the OECD database, and the crude divorce rate was obtained from the TURKSTAT database. Mixed findings have characterized the exploration of the complicated link between income and suicide. While some studies assert a positive correlation between income and suicide (Hamermesh & Soss, 1974), others propose an inverse relationship, contending that suicide deaths decrease with higher income levels (Brainerd, 2001; Chuang & Huang, 1997). Unemployment emerges as a robust indicator of economic conditions, standing out as the most significant risk factor for suicide globally (Goldman-Mellor et al., 2010). The rationale lies in the contraction of goods and services consumption during periods of unemployment, contributing to an elevated risk of suicide. However, the empirical literature has provided mixed results on the association between suicide and unemployment, with some studies highlighting a positive association between suicide and unemployment (Yang, 1992; Yang et al., 1992) while others suggest a negative correlation (Brainerd, 2001; Chuang & Huang, 1997; Neumayer, 2003, 2004). Recognizing the diverse nature of the economic factors influencing suicide, this study incorporates GDP growth rate and unemployment variables to control for their effects on suicide mortality. In addition, according to the seminal work of Durkheim (1897), social integration plays a vital role in preventing suicide. In this context, divorce is considered a potent indicator of weakened social ties, diminishing social connections and family bonds. Building on the works of Minoiu and Andrés (2008), Neumayer (2003), and Stack (1980), a positive correlation was found between higher divorce rates and increased suicide deaths. Furthermore, a substantial body of research, including the studies by Neumayer (2003), Andrés (2005), and Stack (2000), underlines the association between alcohol consumption and elevated suicide rates. Finally, to account for the effect of urban life on suicide, the urbanization growth rate is included as a control variable in our comprehensive analysis. This study is conducted on original data. A description of the variables and descriptive statistics used in the dataset are displayed in Appendix.
Methods
The Bounds Testing Approach to Cointegration is a well-established econometric method in time series analysis and has increasingly been applied to estimate the relationship between variables in public health studies (Atilgan et al., 2017; Wang, et al., 2019). Compared to conventional cointegration tests, Bounds Testing to Cointegration has several advantages. First, all variables are not limited to having the same order of integration. In other words, stationary and non-stationary series can be used in the same model. Second, even if the sample size is small, Bounds Testing to Cointegration provides robust and sensitive results (Pesaran et al., 2001). To cointegration relationship between suicide deaths and social expenditure, the ARDL model can be defined as:
The short run behavior of variables is investigated by following error correction representation of Shahbaz (2013) as follows:

We estimate econometric models by assuming that total, female, and male suicide deaths are determined as a linear function of the presence of social expenditure and other socioeconomic factors. Then the model is as follows: If public social expenditure has an anticipated impact on decreasing suicide mortality, the coefficient of public social expenditure in equation (1) is expected to be negative.
Results
Unit Root Test and Stationarity Test Results.
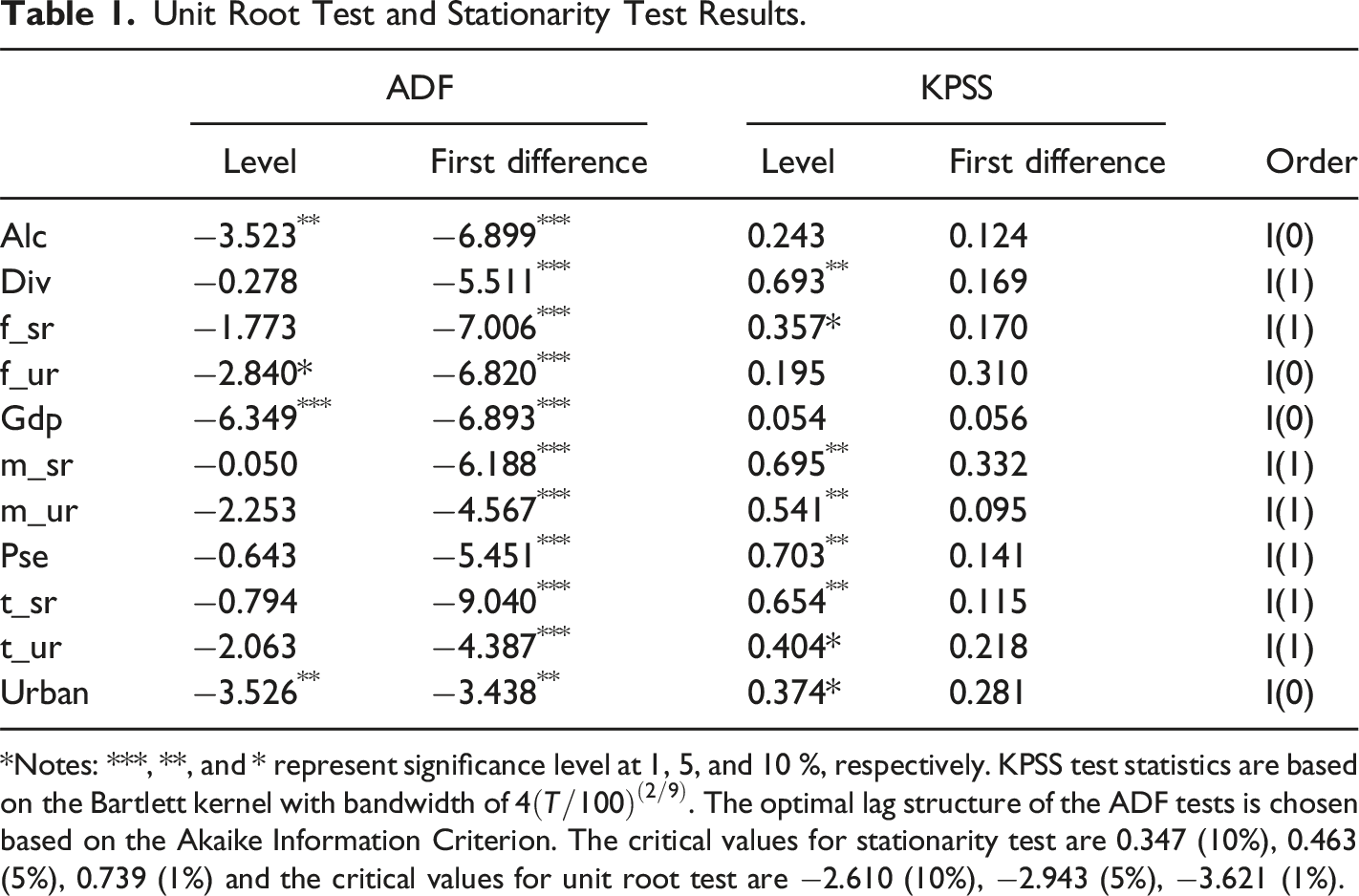
Notes: ***, **, and * represent significance level at 1, 5, and 10 %, respectively. KPSS test statistics are based on the Bartlett kernel with bandwidth of
ARDL Cointegration Test Results.
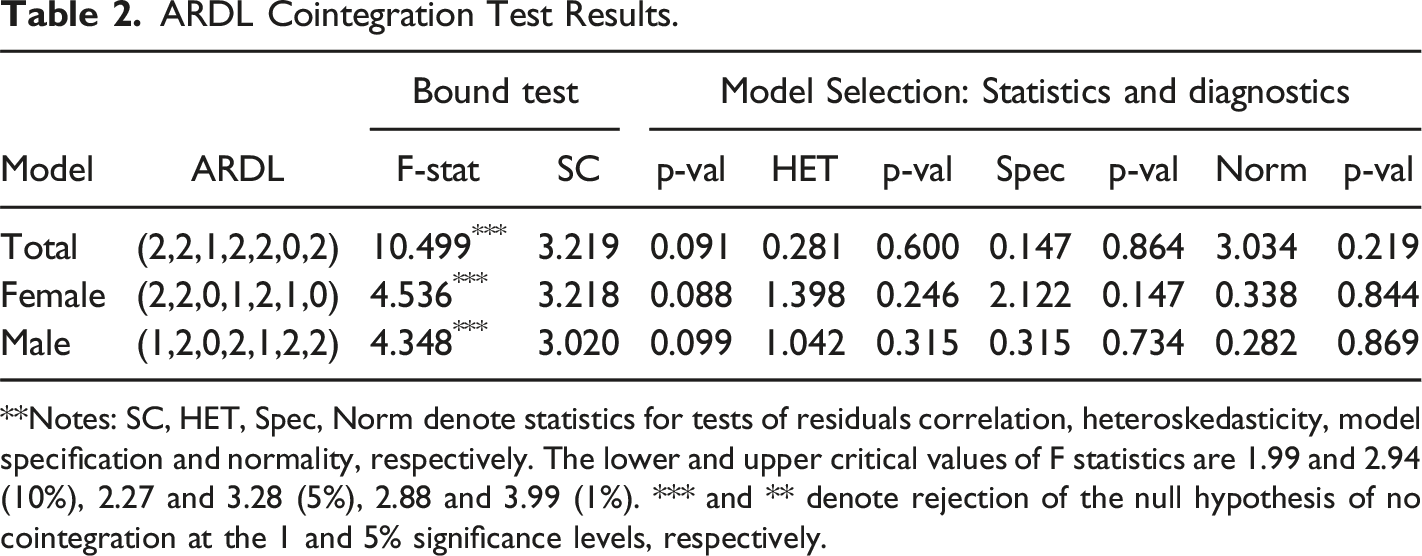
Notes: SC, HET, Spec, Norm denote statistics for tests of residuals correlation, heteroskedasticity, model specification and normality, respectively. The lower and upper critical values of F statistics are 1.99 and 2.94 (10%), 2.27 and 3.28 (5%), 2.88 and 3.99 (1%). *** and ** denote rejection of the null hypothesis of no cointegration at the 1 and 5% significance levels, respectively.
Estimation Results.
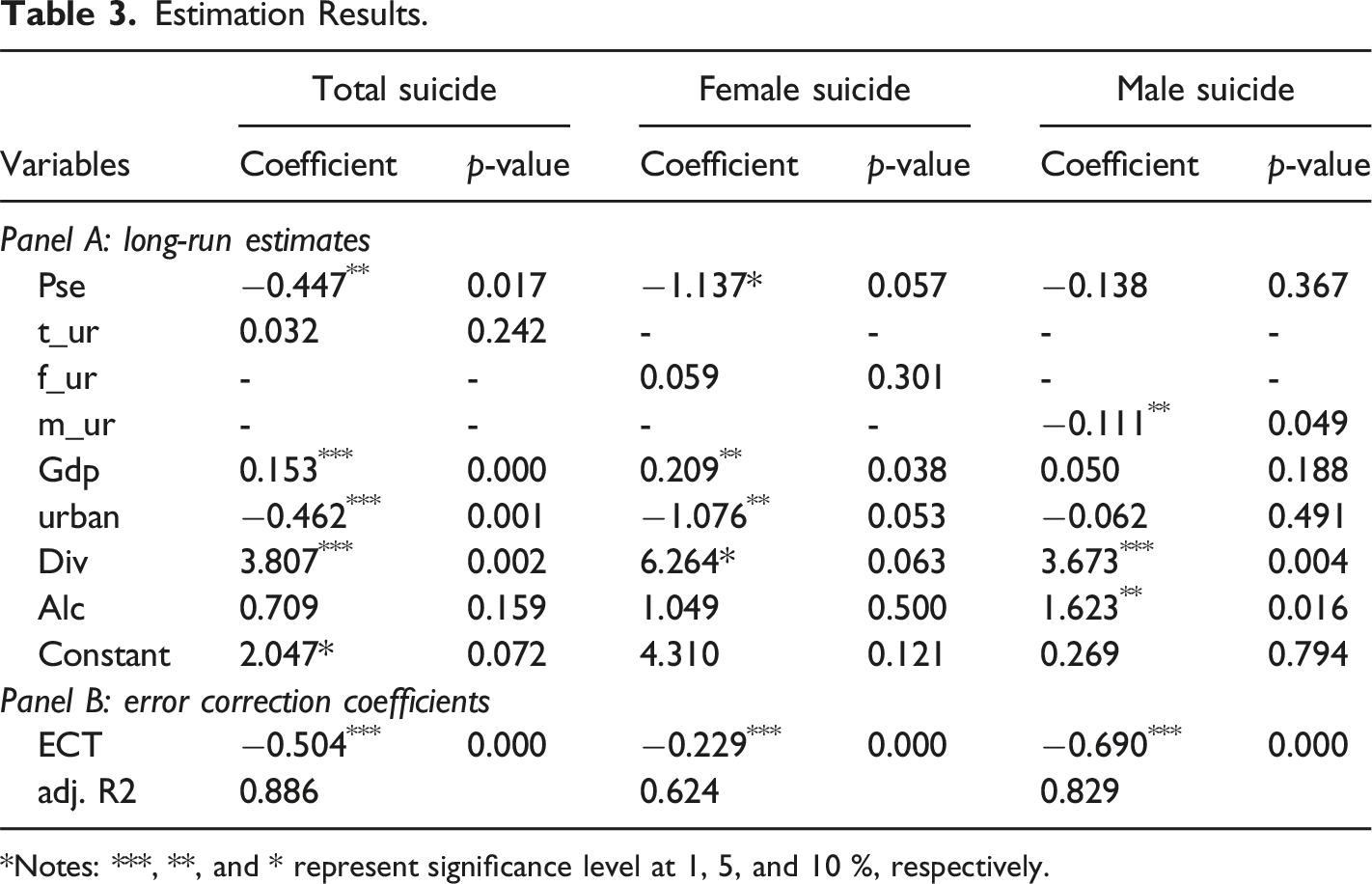
Notes: ***, **, and * represent significance level at 1, 5, and 10 %, respectively.
In order to determine the short-run impact of public social expenditure on suicide mortality in Turkiye, we estimate Error Correction Model (ECM) associated with the respective long-run relationships. Panel B, Table 3 presents the short-run coefficients of the impact of social expenditure on suicide mortality in Turkiye. The Error Correction Term (ECT) represents the speed of adjustment that restores equilibrium in the dynamic model after a disturbance. We found that the coefficient of lagged ECT is between 0 and −1 showing significance at 1% level. It entails that significance of error term shows the speed of adjustment towards long run from short span of time and confirms our ascertained long run relationship. The sign of estimated coefficients of ECT for total, female, and male suicide models are −0.504, −0.229, and −0.690, respectively. This indicates that change from the equilibrium level of suicide mortality is corrected by 50.4%, 22.9%, and 69% per year.
Discussion and Conclusion
We tested the hypothesis that the level of social expenditure provided by the government is correlated with suicide death in Turkiye from 1982 to 2019 by employing the Bounds Testing Approach to Cointegration and ARDL estimation techniques. This study finds robust evidence that public social expenditure has a statistically negative effect on total suicide and female suicide deaths but statistically insignificant on male suicide mortality.
Our results align with the previous studies that determined the negative relationship between social expenditure and suicide death (Flavin & Radcliff, 2009; Kyonne, 2019; Minoiu & Andrés, 2008; Zimmerman, 2002). We found that public social expenditure has a negative and statistically significant impact on the total suicide mortality rate. A 1 % increase in public social expenditure is associated with a 0.44 % decrease in total suicide mortality.
Our results, however, are in sharp contrast with the findings provided by Ross et al. (2012), Zimmerman (1987), and Park et al. (2009). Furthermore, we found evidence that public social spending was statistically significant on female suicide death, whereas the effect of social expenditure was statistically insignificant on male suicide death rates. Higher social expenditure predicted lower female suicide mortality rates. Each additional 1% increase in public social expenditure predicted a 1.13 % decrease in female suicide mortality. For female suicide mortality, our findings are in line with the results obtained by Yur’yev et al. (2012), Yur’yev et al. (2013), and Matsubayashi et al. (2020) who examined the link between suicide deaths and social welfare spending for EU and Japan, respectively. For male suicide mortality, nevertheless, the results of our study are in sharp contrast with the findings of recent empirical studies conducted by Yur’yev et al. (2012), Yur’yev et al. (2013) and Matsubayashi et al. (2020). This can be explained by the Intersectionality Theory, which suggests that, on average, women are more disadvantaged than men, so that they may benefit more from welfare generosity (Gkiouleka, et al., 2018). Also, the magnitude of the impact is significant. While a 1% increase in social expenditure leads to a 0.44% decrease in total suicide mortality, a 1 % increase in social spending is associated with a 1.13% decrease in female suicide death. This finding is intuitive because socioeconomic factors may cause a detrimental effect on women, and social assistance given to women is more likely to have a much more negative effect on suicide. Furthermore, contemporary research underscores a consistent pattern wherein suicide mortality exhibits an upward trajectory during economic contractions (Miller et al., 2009; Reeves et al., 2012; Ruhm, 2000; Stuckler et al., 2009). In contrast, Andrés (2005) found a robust positive correlation between GDP and suicide deaths, challenging the prevailing economic downturn concept. Our research aligns with the findings of Andrés (2005), reinforcing the notion that an upswing in income levels corresponds to an increase in suicide mortality. Overall, the results obtained in our study support the hypothesis that social expenditure can be considered one of the significant factors for the objective of suicide prevention programs.
This study found that social expenditure significantly reduces suicide mortality, particularly among females. Therefore, policymakers should prioritize increasing social expenditure in government budgets to address this public health issue effectively. This could involve enhancing welfare programs, providing more substantial social assistance, and investing in public services such as healthcare and education to mitigate the adverse effects of economic and social crises. Given that social expenditure has a more pronounced impact on female suicide mortality, targeted interventions should be designed to support vulnerable and disadvantaged groups, especially women. Programs offering financial assistance, mental health support, and resources to improve socioeconomic conditions can be instrumental in this regard. For instance, expanding access to affordable childcare and ensuring job training and placement services can help alleviate the economic pressures that disproportionately affect women.
Strengthening social ties and community support can reduce the risk of suicide. Increasing public social expenditure aimed at enhancing social integration—such as funding community-building initiatives, support groups, and programs that encourage social participation—can help individuals feel more connected and supported. Policies could include developing community centers, organizing local events, and promoting volunteerism to foster a sense of belonging and mutual support within communities. Integrating mental health services with social assistance programs can provide a comprehensive support system for individuals at risk. Increasing the public share in social expenditure should focus on enhancing access to mental health care, reducing stigma, and providing support for those experiencing mental health issues. This could involve expanding mental health services in primary care settings, implementing public awareness campaigns to combat stigma, and providing training for social workers and healthcare providers to recognize and address mental health issues effectively.
Moreover, a multi-sectoral approach involving collaboration between government agencies, non-profits, and private sectors can enhance the effectiveness of these interventions. For example, partnerships with non-governmental organizations (NGOs) can facilitate the delivery of tailored mental health services and community support programs, while private sector involvement can help fund and sustain these initiatives. To ensure the sustainability and effectiveness of these policies, continuous monitoring and evaluation should be implemented. This includes collecting data on the outcomes of various interventions, conducting regular assessments, and adjusting strategies based on evidence and feedback. By adopting a dynamic and responsive policy framework, policymakers can better address the evolving needs of the population and make significant strides in reducing suicide mortality.
The study covers the period from 1982 to 2019. Data from earlier periods are unavailable, which may limit the understanding of historical contexts. Another limitation is that this study focuses on gender-specific suicide mortality rates; however, age-specific suicide mortality rates were not explored. Future research should examine the impact of social expenditure on suicide mortality across different age groups. This could help identify age-specific vulnerabilities and tailor interventions accordingly. The findings are specific to Turkiye and may not be directly applicable to other developing countries with different social, economic, and cultural contexts. Conducting comparative studies between Turkiye and other developing countries can provide insights into the generalizability of the findings and highlight best practices in reducing suicide mortality through social expenditure. Future studies should evaluate the effectiveness of specific social policies and programs in reducing suicide mortality. This could involve analyzing the impact of various types of social assistance, such as unemployment benefits, housing support, and mental health services.
Footnotes
Acknowledgements
The author would like to thank Asst Prof. Dr Simone Rambotti for his comments on the initial manuscript for this study. Thanks to the agreement between Sage Publishing and ANKOS, the open-access article processing charge for this research has been substantially lowered. The author sincerely appreciates the contributions of both parties in facilitating this arrangement and their support in making open-access publication more affordable.
Disclosure
The author reports that there are no competing interests to declare.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.