
Abstract
This scoping review explores findings from the psychological and medical literature on the adaptive grieving experiences of bereaved dementia family caregivers and integrates what healthcare professionals can do to support bereaved dementia family caregivers transition into a post-death role. Bereaved dementia family caregivers are particularly susceptible to prolonged grief disorder post-death due to the protracted caregiving demands and progressive course of the illness. The mention of caregiver grief while the person with dementia is living is quite common in the literature; however, limited research focuses on the bereaved dementia family caregiver and the methods they use to grieve adaptively. Three overarching adaptive grieving themes emerged from the review: 1) social health, 2) emotional and spiritual fitness, and 3) reclaiming activities. Given the growing prevalence of bereaved family dementia caregivers, understanding how they might most adaptively grieve and experience the greatest possible well-being should be a top focus for research.
Keywords
Introduction
Most bereaved dementia family caregivers (friends, family, and fictive kin) demonstrate remarkable resilience in adjusting to the death of their care recipient. For the majority, depressive and other grief-related symptoms rapidly return to nearly normal levels within a year of death (Schulz et al., 2003). For bereaved dementia family caregivers to move forward with their lives without the deceased, some suggest a need to integrate their grief through the process of incorporating the experience of death into a new life (Shear, 2012). A significant capacity to adjust in a positive direction while having sufficient support resources available despite destabilizing experiences (i.e., resilience) is necessary to successfully manage such shifts (Jensen et al., 2020). However, 9-25% of bereaved dementia family caregivers experience complicated grief (CG) or prolonged grief disorder (PGD) following the death of their care recipient. CG and PGD represent a debilitating type of mourning characterized by a deep longing for the deceased, inescapable thoughts of the person who died, unrelenting sorrow, retreat from former social connections, having trouble accepting the death, and a feeling that there is no point to life (Newson et al., 2011; Schulz et al., 2006; Simon, 2013). PGD and CG are not perfectly analogous, but they represent maladaptive, closely related grieving forms (Romero, 2021). Because this review focuses on recommendations for bereaved dementia family caregivers to ameliorate maladaptive grieving and pursue more adaptive grieving, we incorporated findings using both conceptualizations. Likewise, past literature (e.g., Arruda & Paun, 2017; Chan et al., 2013; Crawley et al., 2022) has found good utility in understanding the experiences of bereaved dementia family caregivers of people with these CG and PGD in concert. Therefore, we treated the concepts as closely related and tried to reflect the language used in the original publications when describing specific studies. In this review, we explore the adaptive grief experiences of a wide range of bereaved family caregivers of people with Alzheimer’s disease and Alzheimer’s disease-related dementias (hereafter “dementia”).
As dementia advances, providing care for a person with dementia (PWD) necessitates constant adjustment and adaptation (Chenoweth & Spencer, 1986; Reinhard et al., 2008). Caregivers may feel as though they are “losing him or her twice” (Supiano et al., 2022, p. 369) because dementia robs both the care recipient and the family members of many components of their relationship. Some have suggested considerably more than two losses are possible during dementia. These losses exist for the PWD (e.g., loss of memory, loss of autonomy, loss of role, loss of identity, and loss of selfhood) as well as those who care for the PWD (e.g., loss of the person as they knew them prior to dementia, loss of future hopes and expectations, loss of home, loss of social networks, loss of identity) (Doka, 2010). These changes can be challenging to accept and, combined with the death of the PWD, can lead to maladaptive post-death grief (Holland et al., 2013). Because of the long-term repercussions of caring for a family member with dementia, caregivers may be inadequately prepared to move into a post-death role (Jameson et al., 2020).
The best time to provide grief interventions for family dementia caregivers is before the PWD dies (Schulz et al., 2006; Supiano et al., 2022). But millions of bereaved dementia family caregivers already exist. Worldwide, dementia directly caused at least 1.62 million deaths in 2019 (Nichols et al., 2022) and 271,872 in the United States (“2023 Alzheimer’s Disease Facts and Figures,” 2023). And that number is necessarily an underestimate given that PWD commonly has other causes of death listed on their death certificates that were precipitated by their dementia (e.g., pneumonia caused by aspirating food into the lungs due to swallowing difficulties from dementia) (Weuve et al., 2014). 2011 United States deaths from Alzheimer’s disease (AD) were estimated at 700,000 (Weuve et al., 2014). Weuve et al. (2014) reported that dementia deaths are predicted to rise gradually over the next two decades, reaching 900,000 in 2030, 1.3 million in 2040, and 1.6 million in 2050.
Over 11 million caregivers provide care for a PWD in the United States (“2023 Alzheimer’s Disease Facts and Figures,” 2023), and that number is predicted to continue to rise due to the population growth of people over 65 who are particularly at risk for developing dementia (van der Flier & Scheltens, 2005). Although bereaved dementia family caregivers may be at risk for poor grief outcomes, research addressing the critical elements of dementia-related adaptive grieving is limited, albeit emerging (Corey & McCurry, 2018; Gibson et al., 2019; Groh & Saunders, 2020; Jameson et al., 2020; Jensen et al., 2020; Peacock et al., 2018; Rolbiecki et al., 2023; Vlachogianni et al., 2016). A broader study of adaptive grieving would also align with recommendations from the 2023 National Research Summit on Care, Services, and Supports for Persons Living with Dementia and Their Care Partners/Caregivers, which identified the importance of studying the care continuum that includes the post-caregiving period after the person living with dementia has died (National Institutes of Aging, n.d.).
Research efforts should aim to prevent the adverse outcomes that can be associated with dementia-related bereavement. Still, there needs to be adequate support for those family caregivers who are already bereaved for whom pre-death intervention is now impossible. This work focuses on those already bereaved individuals and their experiences and aims to answer the following research question.
What do we know about the strategies used by bereaved dementia family caregivers to facilitate adaptive grieving responses following the death of the person with dementia? We anticipate that by examining adaptive grief responses, we will be able to identify the actions and/or supports that bereaved dementia family caregivers require when grieving. We will then discuss how healthcare professionals might foster these adaptive grieving responses to help bereaved dementia family caregivers successfully transition into their post-care role.
Method
Literature and Search Protocol
A scoping review was conducted because specific adaptive responses that bereaved dementia family caregivers undertake independently, coupled with the formal support they use, are relatively underexplored concepts (Arksey & O’Malley, 2005; Arruda & Paun, 2017). The most recent review of dementia family caregiver grief (Crawley et al., 2022) used solely quantitative data to explore the relationship between pre-death factors, post-death grief, and the services used to address bereavement for dementia family caregivers. For this review, which explores all study methods used to analyze adaptive grief responses for bereaved dementia family caregivers, Arksey and O’Malley’s (2005) five stages for conducting a scoping review were employed: Stage 1: identify the research question; Stage 2: identify relevant studies; Stage 3: study selection; Stage 4: chart the data; Stage 5: collate, summarize, and report the results. This review followed the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) checklist and explanation (Tricco et al., 2018).
The databases searched were CINAHL, Scopus, PsycINFO, and PubMed between 2013 and October 2023. A consultation with an Arizona State University (ASU) health sciences librarian ensured accurate search conduct. One new study was found with the final search. The key search terms used within titles and abstracts were “Alzheimer*,” “Parkinson’s dementia,” “dementia,” informal caregiver,” “bereaved,” “grief,” “complicated grief,” “prolonged grief,” and “bereavement,” as well as using the MESH (medical subject headings) terms “caregiver,” “dementia,” and “grief.” The MESH terms for caregiver include informal caregiver (s), family caregiver (s), carer (s), and spouse caregiver (s). The MESH terms for dementia include AIDS dementia complex, Alzheimer’s disease, Aphasia Primary Progressive, Creutzfeldt-Jakob Syndrome, vascular dementia, multi-infarct dementia, diffuse neurofibrillary tangles with calcification, Frontotemporal lobar degeneration, Huntington’s disease, Kluver-Bucy Syndrome, Lewy Body disease and mixed dementias. The MESH terms for grief include grief and mourning. Reference lists of included studies were also reviewed. Figure 1 presents the PRISMA flow diagram. PRISMA flow diagram for scoping review. From: (Page et al., 2021).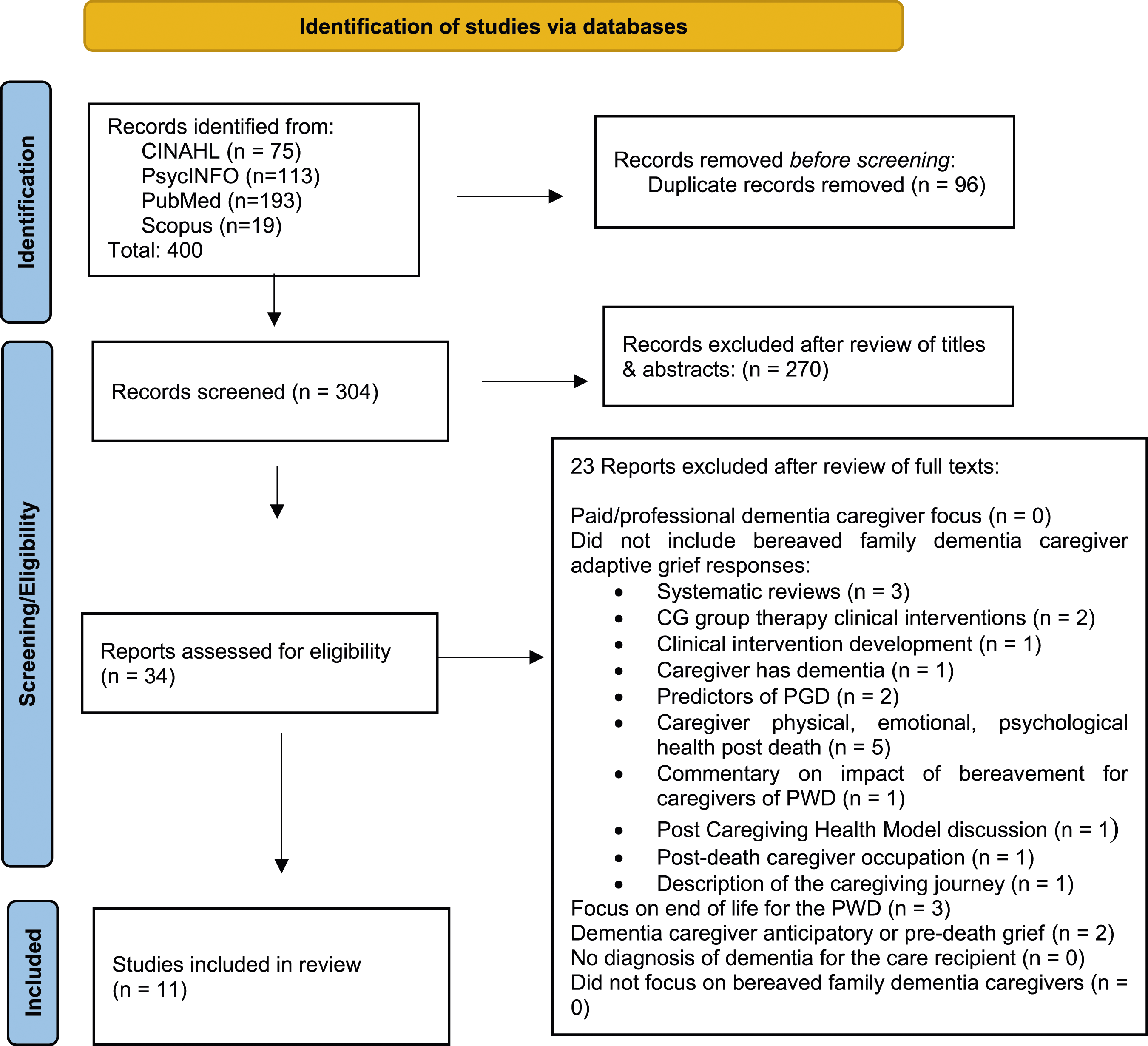
Inclusion and Exclusion Criteria
Articles were included if they were (a) peer-reviewed, (b) studies published in English that included family dementia caregiver post-death grief, services that supported post-death grief or effectiveness of caregiver interventions, (c) were quantitative, qualitative and/or mixed methods designs, (d) and focused on family or friend non-paid caregivers (aged 18 or over) of persons diagnosed with dementia who died at home, in the hospital, or assisted living, nursing home, with or without hospice services. Articles were excluded if (a) they focused on paid or professional dementia caregivers, (b) they did not include bereaved family dementia caregiver adaptive grief responses (e.g., systematic reviews, caregiver group therapy clinical interventions, or development of clinical tools, bereaved dementia family caregiver has dementia, predictors of PGD, bereaved dementia family caregiver health post-death, commentary on the impact of bereavement for caregivers of PWD, Post Caregiving Health Model discussion, post-death caregiver occupation, description of the caregiving journey) (c) the subject matter was exclusively on the end-of-life for the PWD, (d) they focused on dementia caregiver’s anticipatory or pre-death grief, (e) there was no diagnosis of dementia for the care recipient, (f) or they did not focus on bereaved dementia family caregivers.
Results
Overview of the Included Studies of Bereaved Dementia Family Caregivers' Experiences.
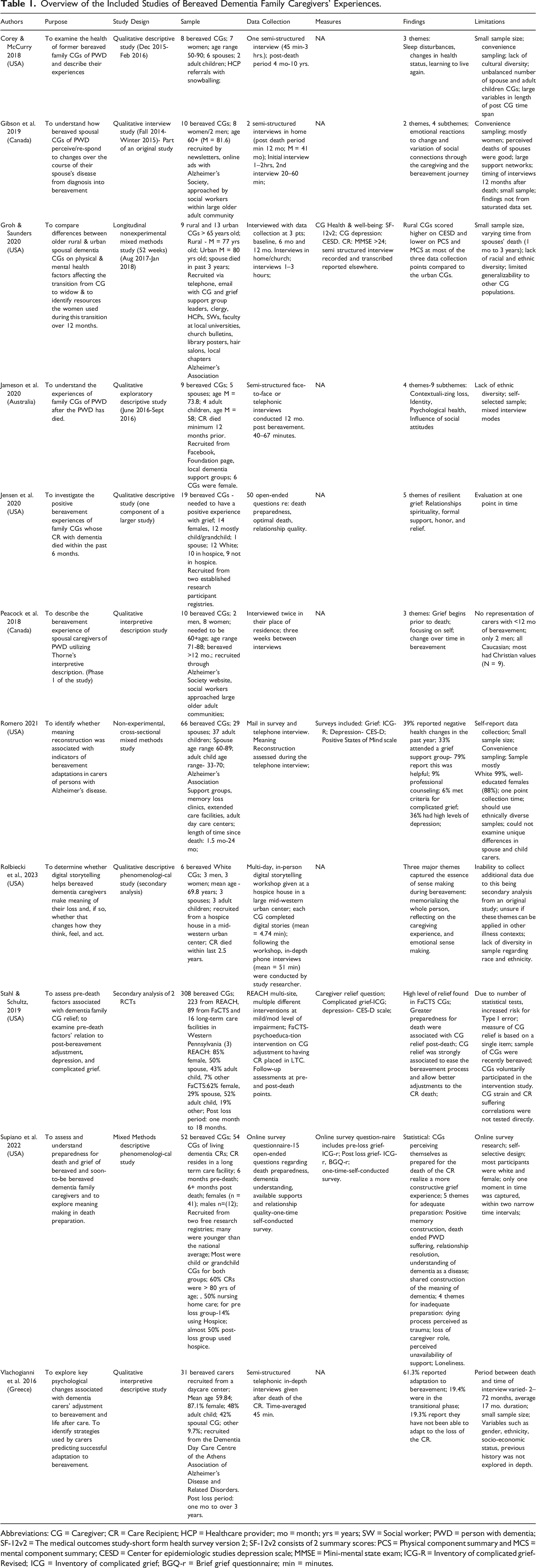
Abbreviations: CG = Caregiver; CR = Care Recipient; HCP = Healthcare provider; mo = month; yrs = years; SW = Social worker; PWD = person with dementia; SF-12v2 = The medical outcomes study-short form health survey version 2; SF-12v2 consists of 2 summary scores: PCS = Physical component summary and MCS = mental component summary; CESD = Center for epidemiologic studies depression scale; MMSE = Mini-mental state exam; ICG-R = Inventory of complicated grief-Revised; ICG = Inventory of complicated grief; BGQ-r = Brief grief questionnaire; min = minutes.
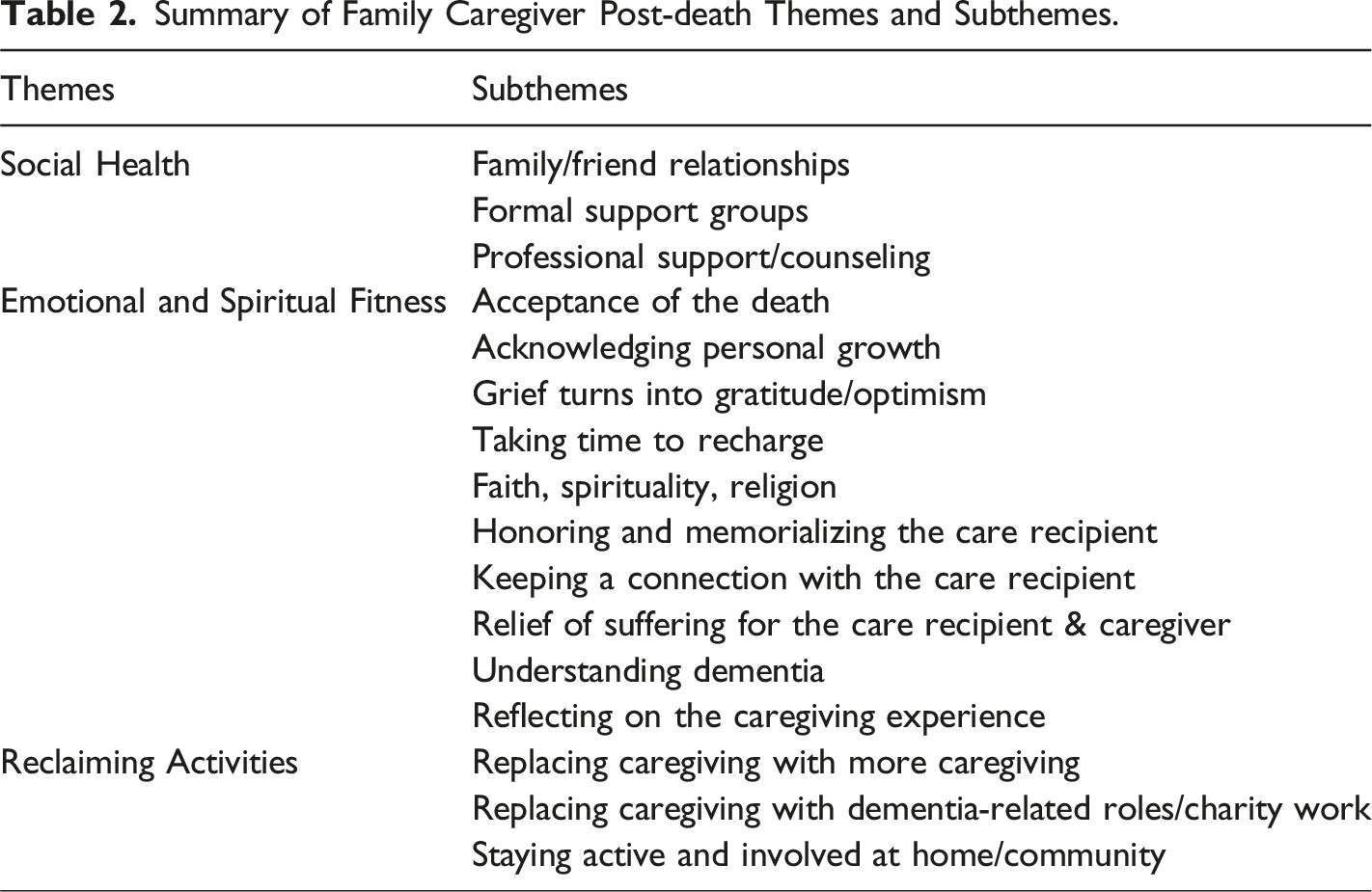
What do we know about the strategies used by bereaved dementia family caregivers to facilitate adaptive grieving responses following the death of the person with dementia? All eleven studies indicated adaptive grieving methods that bereaved dementia family caregivers employ post-death. Analysis of the articles resulted in the creation of three broad themes of caregiver focus that constitute a more adaptive grieving experience: social health, emotional and spiritual fitness, and reclaiming activities. Table 2 depicts a summarization of these themes and their subthemes.
Summary of Family Caregiver Post-death Themes and Subthemes.
Social Health
The concept of social health was associated with adaptive grieving in eight studies. We defined social health as the part of overall well-being that stems from connection and community (Smith & Christakis, 2008). It is about having close relationships with family and friends, feeling connected to groups, and feeling supported, respected, and loved. Within the theme of social health, three subthemes were evident: family and friend relationships, formal support groups, and professional support and counseling.
Family and Friend Relationships
Seven of the eleven reports emphasized the importance of family and friend support and closeness with adaptive grief experiences. Vlachogianni et al. (2016) found that most bereaved dementia family caregivers reported at least one positive improvement in their lives after the death, with support from friends and family and engaging in enjoyable activities being recognized as essential in coping. Maintaining social experiences with family, friends, and neighbors and sharing grief with others was associated with adaptive grief (Peacock et al., 2018). A crucial aspect of the participant’s caregiving and bereavement journey was social inclusion (Gibson et al., 2019). Social circles, community involvement, prior and new friends, and family support were vital resources during bereavement, alleviating feelings of stress and grief. Bereaved dementia family caregivers provided narratives that mentioned the fortitude and support of family and friends and their strong connection with the care recipient as conduits for a positive and adaptive bereavement (Jensen et al., 2020). Bereaved dementia family caregivers with better post-death grief outcomes expressed that the relationship closeness and bonding between family and the care recipient were highly valued and treasured (Supiano et al., 2022). Importantly, some aspects of people’s environments may help dictate the most feasible ways to maintain these essential relationships. Groh & Saunders, (2020) reported that compared to urban bereaved dementia family caregivers, rural bereaved dementia family caregivers used the Internet more frequently to keep in touch with family and friends.
Formal Support Groups
In three studies, bereaved dementia family caregivers stated a desire for regular contact with support organizations, citing a wish to discuss their experiences. Formal support groups (e.g., Hospice, Alzheimer’s Association, and Area Agencies on Aging) were the most commonly used community resource by rural and urban bereaved dementia family caregivers, while the number of participants who attended support groups gradually decreased over one 12-month study (Groh & Saunders, 2020). Romero (2021) found that a significant number of bereaved dementia family caregivers (79%) participated in grief support groups. Of those, 33% expressed that they helped get them through the grieving period (Romero, 2021). Online support groups were convenient for rural bereaved dementia family caregivers (Groh & Saunders, 2020) and allowed bereaved dementia family caregivers to share information and receive resources (e.g., Dementia Australia) (Jameson et al., 2020). Freely discussing the person who died with others helped bereaved dementia family caregivers with adjusting to post-care life (Jameson et al., 2020).
Professional Support and Counseling
Bereaved dementia family caregivers found strength and stability in the use of professional help, such as pastoral support (Groh & Saunders, 2020), bereavement counseling (Groh & Saunders, 2020; Jameson et al., 2020; Romero, 2021) and from their healthcare providers (Jameson et al., 2020). One bereaved dementia family caregiver stated that six months after the care recipient’s death, she “just suddenly fell into this hole” and immediately realized that her care recipient “wasn’t coming home” (Jameson et al., 2020, p. 2441). She said this feeling lasted two to three months until her physician placed her on antidepressants, which she said had helped. Another bereaved dementia family caregiver in the same study found that having access to her physician made it easier for her to reconcile what she had seen while providing care by helping her understand the experience of the care recipient’s death.
Emotional and Spiritual Fitness
Ten areas of emotion-focused coping strategies were indicated in these studies. We described emotional fitness as the ability to mentally recover from adversity and weather life’s ups and downs with moderate emotional stability (De Leersnyder et al., 2014). Robust emotional fitness requires a great deal of fortitude to build and sustain since it is built upon ongoing active decisions. It is a continuing mental exercise that can help to steer through some of life’s most difficult challenges with facility and balance. Spiritual fitness is defined as the integration of basic wellness, psycho/spiritual well-being, and stress reduction (Khalsa & Newberg, 2021).
Acceptance of the Death
Six studies revealed evidence that the bereaved dementia family caregiver accepted the person’s death and moved on. Many bereaved dementia family caregivers cited embracing death as an essential coping mechanism (Vlachogianni et al., 2016). Controlling their emotions, “reappraising” the death of a care recipient, and seeing caring as a positive experience were other helpful coping strategies. Shared grief processing was associated with adaptive grief. It generated themes such as positive memory construction of the care recipient, embracing that death as an end to the family member’s suffering, and voicing appreciation for the consideration of family members responding to the death of the PWD (Jameson et al., 2020; Supiano et al., 2022). In one study, half of the bereaved dementia family caregivers reported the importance of acknowledging sadness or anger triggers like people, locations, or things that prompted a memory of the care recipient (Corey & McCurry, 2018). Acceptance of the death helped bereaved dementia family caregivers make sense of their care recipient’s death as it was a natural process (Romero, 2021). In that same study, caregivers looked at the death positively and expressed that it helped them understand and empathize with others in the same situation. Bereaved dementia family caregivers stated that recognizing that their personal life continued after the death of their care recipient was a part of adaptive grief (Peacock et al., 2018). Many bereaved dementia family caregivers described the futility of being sad or grieving for too long.
Acknowledging Personal Growth
Five studies indicated that recognizing personal development due to the caregiving role supported adaptive grieving experiences. Bereaved dementia family caregivers found satisfaction and strength due to the care they gave (Vlachogianni et al., 2016). Participants used positive self-narratives to define themselves as independent, positive, and powerful individuals, which helped them cope with the death of their care recipient (Peacock et al., 2018). These positive self-narrative abilities were frequently described as innate characteristics. Many bereaved dementia family caregivers expressed that feeling optimistic and telling themselves to be strong and carry on were important in working through their bereavement (Gibson et al., 2019). Due to the care they provided, some bereaved dementia family caregivers reported changes in identity, discovering their own strength and compassion (Romero, 2021). According to bereaved dementia family caregivers, the positive aspects of caregiving were discovering one’s abilities when confronted with difficulties, which led to significant personal growth (Corey & McCurry, 2018).
Reflecting positively on the death of the PWD to get through the grieving process was a prominent finding in two studies. Bereaved dementia family caregivers found utility in thinking about the positive aspects of the person’s death and the care journey itself (Jameson et al., 2020). These positive reflections sometimes included reappraising of the care recipient’s death (i.e., they witnessed the care recipient’s decline for such a long time they had ample time to prepare for their death psychologically) (Peacock et al., 2018). Importantly, bereaved dementia family caregivers were able to positively reframe their recipient’s death for both the care recipient and themselves. This was partly based on bereaved dementia family caregivers' descriptions of their care recipient’s discomfort while living with dementia (especially near the end of life), which significantly impacted how they understood the death.
Grief Turned into Gratitude and Optimism
Many bereaved dementia family caregivers emphasized the value of gratitude and optimism (Gibson et al., 2019). The cultivation of gratitude enabled the processing of grief and enjoyment of past and present experiences. As a result, individuals could restore qualities of themselves that were valued before caregiving. One bereaved dementia family caregiver stated that her “grief turned into gratitude” because she had him as her spouse, and she could “transform deep grief into more gratefulness, for what was” (Gibson et al., 2019, p. 5). Another bereaved dementia family caregiver stated that grief should not be dwelled upon, that “you have to be optimistic,” and that “you need to be strong and carry on” (Gibson et al., 2019, p. 5). In addition, bereaved dementia family caregivers said that anticipating that loneliness would lessen with time helped them to adapt better to their grief.
Taking Time to Recharge
Following the death of the care recipient, all bereaved dementia family caregivers in one study said they needed time to recharge and reflect, such as requiring alone time and taking a break from obligations (Gibson et al., 2019). Recovery time ranged from one day to two years.
Faith, Spirituality, Religion
In three studies, faith, spirituality, or religion played a large part in helping bereaved dementia family caregivers grieve adaptively. One bereaved dementia family caregiver reflected on the devotion of her family member to Jesus, and this faith comforted her, knowing that her loved one had a peaceful death due to her ongoing faith (Jensen et al., 2020). Because of their spiritual convictions, bereaved dementia family caregivers were able to portray their care recipient’s death as peaceful (Peacock et al., 2018). Some bereaved dementia family caregivers who viewed death through spirituality or faith believed death is a natural part of life (Jameson et al., 2020). One bereaved dementia family caregiver stated that he felt blessed by God, that dementia was a journey that happened, and that if he received this type of ending to his life, then so be it.
Honoring and Memorializing the Care Recipient
Reflecting on the memories of the care recipient through funeral preparations, ensuring to fulfill the care recipient’s requests, and spending time with others in the family to honor the care recipient’s life provided peace and strength for bereaved dementia family caregivers (Jensen et al., 2020). Knowing they honored the care recipient provided consolation to these bereaved dementia family caregivers and supported a more adaptive bereavement. By memorializing the whole individual and their connection to the care recipient, a fuller picture of the deceased care recipient’s life and legacy emerged (Rolbiecki et al., 2023). One bereaved dementia family member explained his life with his wife by saying, “This is a story about unconditional love” and concluded his interview with a poem that read, “The old life that we lived so fondly together is untouched, unchanged” (Rolbiecki et al., 2023, p. 4-5). Some bereaved dementia family caregivers shifted their focus from remembering their family member solely as a PWD to reminiscing about various life stages, particularly before the illness took hold (Rolbiecki et al., 2023). One bereaved dementia family caregiver who lost her mother emphasized the significance of not only remembering the moment she died but also cherishing how she lived, showcasing her personal and professional achievements, family experiences and trips, and pre-dementia texting communications. Bereaved dementia family caregivers harmoniously interwove these diverse memories to construct a comprehensive understanding of their loved one’s life journey. Memorializing the whole person was one way that bereaved dementia family caregivers identified a more adaptive grief response (Rolbiecki et al., 2023).
Keeping a Connection with the Care Recipient
Bereaved dementia family caregivers maintained a bond with the care recipient after their death and reported that it was crucial to coping with their death (Vlachogianni et al., 2016). This connection was described as continuing to provide care, which included visiting their grave site, speaking to them, and occasionally feeling as though they were still alive. (Peacock et al. (2018) found that although grieving dementia family caregivers felt it was vital to accept the death and move on, the majority maintained a connection with their care recipient. Keeping a connection meant doing things their care recipient would have wanted them to do after their death, such as celebrating holiday traditions, donating their things to someone who needs them, and remaining affiliated with dementia-focused groups. Some bereaved dementia family caregivers adapted better by keeping memorable items of their care recipient around, such as photographs, cremation ashes, or personal belongings.
Relief of Suffering for the Care Recipient and Bereaved Dementia Family Caregiver
In eight studies, bereaved dementia family caregivers felt alleviation of suffering for the care recipient after their care recipient died. Peacock et al. (2018) reported that bereaved dementia family caregivers felt a particular sense of relief and started focusing on self-care. One stated, “It was a blessing for him, and for me, my burden was lifted a little” (Peacock et al., 2018, p. 86). Likewise, in Gibson et al.'s (2019) study, all bereaved dementia family caregivers expressed relief for themselves and their care recipients after death. The release of obligations linked with care provided relief. One bereaved dementia family caregiver said, “I think that if I’m totally honest, and I want to be, that I was relieved, rather than depressed, when he died. I know I was relieved because he was suffering” (Gibson et al., 2019, p. 5). However, this sensation of relief was accompanied by an internal fight to keep these emotions hidden from others. Bereaved dementia family caregivers believed they had a social expectation not to exhibit relief. Stahl and Schulz (2019) found that bereaved dementia family caregivers may resume neglected activities like leisure and socializing after experiencing relief following the death. A significant sense of relief followed the death since the care recipient was no longer in pain and the stress from providing care abated, which enabled bereaved dementia family caregivers to keep a positive outlook in the face of the death (Jensen et al., 2020). One bereaved dementia family caregiver’s readiness was bolstered by the knowledge that his grandmother was no longer suffering: “I’m glad she no longer struggles with ideas that agitated and upset her, such as needing to go home and help her mama and papa” (Supiano et al., 2022, p. 375). In another study, relief from caregiving stressors came once the care recipient died (Corey & McCurry, 2018). A recurrent theme among those who reported relief was the concept of “dual relief,” which refers to sentiments of relief for both themselves and the PWD who will no longer “suffer” (Vlachogianni et al., 2016, p. 818): “It was a difficult time, but he can now be free” (Vlachogianni et al., 2016, p. 818). Another bereaved dementia family caregiver explained, “I have accepted my father’s death; I thought about it so long, I was not sad but relieved” (Vlachogianni et al., 2016, p. 819). Bereaved dementia family caregivers experienced relief for the PWD since their suffering had ended and now believed they had the opportunity to concentrate on the care recipient’s happy memories and thus could transition more smoothly in the post-death period (Jameson et al., 2020).
Understanding Dementia
Bereaved dementia family caregivers who properly educated other family members about dementia felt supported in their grief (Supiano et al., 2022). These bereaved dementia family caregivers stressed the value of being in the company of relatives who comprehended dementia.
Reflecting on the Caregiving Experience
Following the loss of their care recipient, bereaved dementia family caregivers reflected on their years of caregiving (Rolbiecki et al., 2023). These reflections were rich with memories and assessments of their caregiving experiences, supporting a more adaptive grief response. Some expressed pride in their “excellent” caregiving and described their caregiving journey as a culmination of lifelong preparation. Ambivalence, coping, and complexity characterized the reflections, exemplified by one bereaved dementia family caregiver’s description of caregiving as both “impossible” and a task he would undertake again (Rolbiecki et al., 2023, p. 5).
Reclaiming Activities
Bereaved dementia family caregivers described post-caregiving reintegration activities as a transitional phase with three different, nonlinear subthemes: a) replacing caregiving with more caring, b) replacing caregiving with other value-added non-caring related activities, and c) staying active and involved within the home and community.
Replacing Caregiving with More Caregiving
One significant healing reaction to the loss of the caregiving role was replacing it with a purposeful activity that bereaved dementia family caregivers described as redefining their life purpose (Corey & McCurry, 2018). Sometimes, that gap was filled with additional caregiving activities for spouses and other relatives affected by chronic health conditions. This enthusiasm for providing care was defined as “a role, a mission, a purpose, and a life goal” (Corey & McCurry, 2018, p.e92). Vlachogianni et al. (2016) reported feelings of altruism by caring for other dependents as a significant feature of the post-caring lives of bereaved dementia family caregivers. According to one daughter, “Giving to others is very important in life since it makes you feel useful” (Vlachogianni et al., 2016, p. 819).
Replacing Caregiving with Dementia-Related Foundation Roles/Charity Work
Another key, meaningful activity that supported an adaptive grief response for bereaved dementia family caregivers was the active involvement in causes related to dementia advocacy groups (Corey & McCurry, 2018; Jameson et al., 2020). One bereaved dementia family caregiver explained that her devotion to supporting other family caregivers through writing, public speaking, facilitating support groups, and raising money for AD research is a passion “that chose me” (Corey & McCurry, 2018, p.e92). Another caregiver in this study expressed that her involvement in AD advocacy was a means to honor her care recipient (Corey & McCurry, 2018). After about 12 months post-death, some bereaved dementia family caregivers felt they could use their past caregiving experiences to help others, such as working with charities, providing education in long-term care facilities, or writing a book for caregivers (Jameson et al., 2020).
Staying Active and Involved at Home and Community
Five studies indicated that many bereaved dementia family caregivers found solace and happiness in various home and community activities. For their successful transition into life post-care, bereaved dementia family caregivers reintegrated into community involvement on their terms rather than according to society’s expectations (Gibson et al., 2019). Going back to former interests and activities, such as outdoor activities, taking vacations, and traveling, were characterized by bereaved dementia family caregivers as helping them get their “life back together” and “move on,” which was generally seen as a gradual process (Vlachogianni et al., 2016). A modest proportion of bereaved dementia family caregivers reported participating in local community groups and volunteering. One bereaved dementia family caregiver stated that they have always volunteered in the community, which is very much aligned with their principles and beliefs (Peacock et al., 2018; Vlachogianni et al., 2016) report that living a busy and involved life is essential to an adaptive grief response for bereaved dementia family caregivers. Bereaved dementia family caregivers preserved a sense of continuity by staying occupied with things like housework, physical exercise, volunteering, community activities, working, entertainment events, church involvement, and favorite hobbies (i.e., baking, gardening, knitting). Activities inside and outside their home were considered critical for reestablishing self and existence after the care recipient’s death (Peacock et al., 2018). Greater pleasure in leisure activities following a care recipient’s death was substantially correlated with bereaved dementia family caregiver relief (Stahl & Schulz, 2019). By 12 months post-death, one bereaved dementia family caregiver favored attending a senior center for bingo (Groh & Saunders, 2020).
Discussion
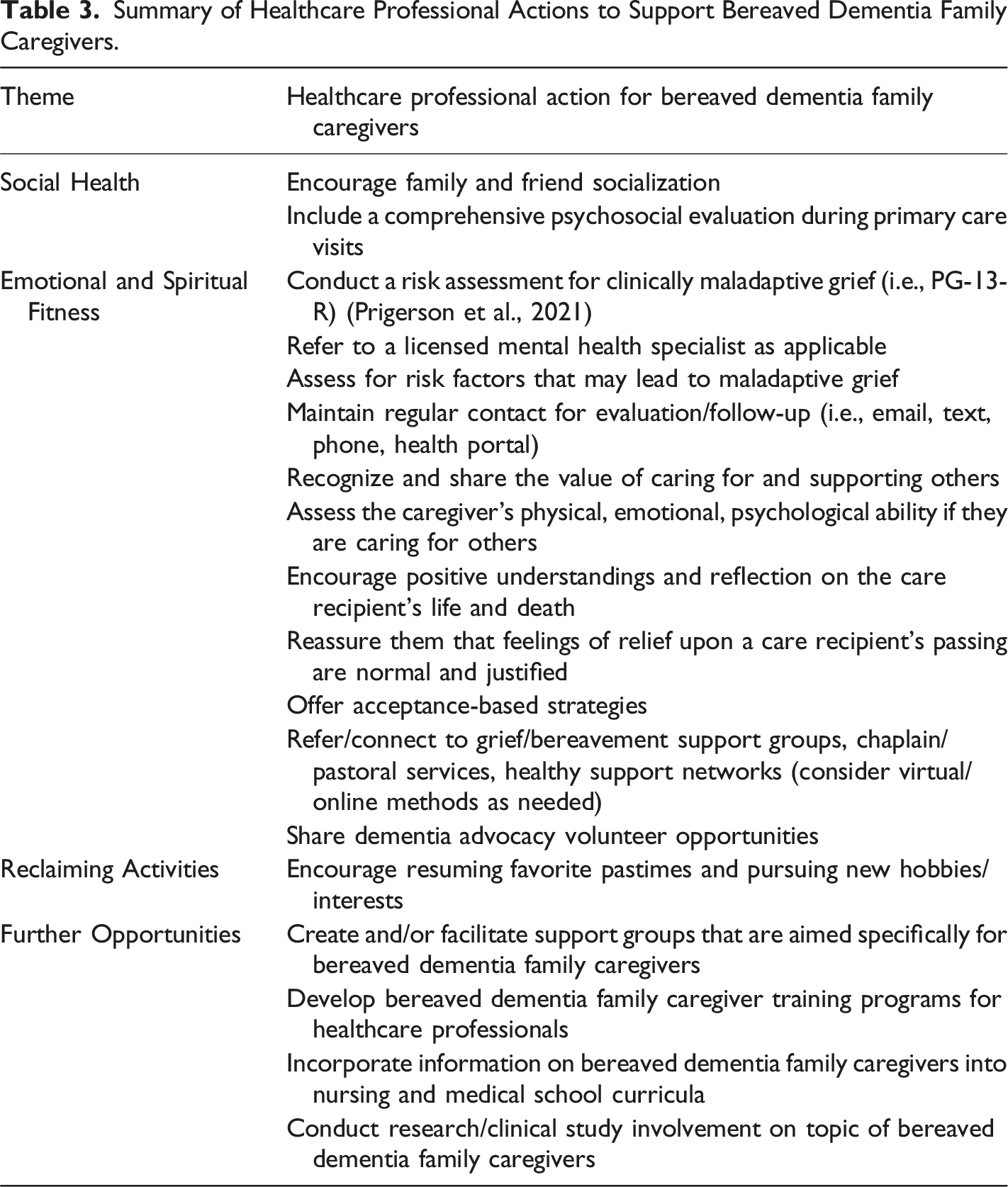
The results of this scoping review demonstrate that multiple facilitators can encourage adaptive grieving for bereaved dementia family caregivers. By incorporating some of these methods, bereaved dementia family caregivers might more adeptly navigate the post-death period. This review identified three primary categories of strategies that bereaved dementia family caregivers employed for a more adaptive bereavement: social health, emotional and spiritual fitness, and physical activities. In addition to utilizing these strategies, we outline how healthcare professionals might help inspire applying these strategies to increase adaptive grieving.
Summary of Healthcare Professional Actions to Support Bereaved Dementia Family Caregivers.
Social Health
Healthcare professionals can encourage family and friend socialization for bereaved dementia family caregivers (Groh & Saunders, 2020). Since 30% of dementia caregivers are 65 or older (“2023 Alzheimer’s Disease Facts and Figures,” 2023), early prevention and promotion of positive social connections can benefit older individuals' health and well-being before social isolation or loneliness becomes more acute following a PWD’s death (Suragarn et al., 2021). Some unique sources of social relationship enhancement that healthcare professionals might encourage bereaved dementia family caregivers to pursue include (1) intergenerational programs, (2) aging-friendly neighborhoods or communities, (3) community-based group physical activities, and (4) technology (i.e., virtual support and networks) (Suragarn et al., 2021).
Social inclusion by family and friends, from pre-death through post-death, was identified as a critical element for a positive post-care transition experience and reintegration back into the community. This finding coincides with the systematic review conducted by Crawley et al. (2022) and a study by Almberg et al. (2000), which indicated that social support for the bereaved dementia family caregiver positively impacted grief. Bereaved dementia family caregivers caring for a care recipient with dementia may succumb to the demands of caregiving and overlook their own psychosocial needs (Gibson et al. (2019). It is crucial to understand that social networks are vital during caregiving and grieving (Almberg et al., 2000). Bereaved dementia family caregivers who have lost their social networks may need extra care when identifying existing support networks or aid in developing new networks (Gibson et al., 2019).
There is limited research on social connection as a specific service for the health of caregivers for a family member with dementia (Van Orden & Heffner, 2022), and providing support for the bereaved dementia family caregiver is frequently neglected in caregiver services (Corey Magan et al., 2020). Rather than using a one-size-fits-all intervention method, activities to combat loneliness for bereaved dementia family caregivers may be most successful when considering caregivers’ opinions and input. For instance, assistance should take into account the particular elements that contribute to a bereaved dementia family caregiver’s loneliness, such as lack of social supports and resources (Bunt et al., 2017). Applicable support can be guided by asking bereaved dementia family caregivers what aspects of their relationships have changed due to providing care, what changes led to loneliness, and which parts of relationships they value most. Additional interpersonal functions, self-control, or stress management might also be targeted for optimized treatment to ensure a behavioral shift that promotes social interaction (Van Orden & Heffner, 2022).
Emotional and Spiritual Fitness
For those opportunities in the healthcare setting, the bereaved dementia family caregiver can be assessed for risks of clinically maladaptive grief. One validated tool that can be used is the Prolonged Grief −13-Revised (PG-13-R) (Prigerson et al., 2021). This tool can be used to address the concern about pathologizing normal grieving and identifying a grief-related disease “too soon” after the death per the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) (American Psychiatric Association, 2022). A referral to a licensed mental health professional is advised if the bereaved caregiver is found to be at risk for PGD.
When assessing bereaved dementia family caregivers at primary care visits during the early stages of bereavement, healthcare professionals can assess for risk factors that may lead to a clinically problematic grief response. In this manner, healthcare professionals can continuously provide early prevention and supplementation (Groh & Saunders, 2020). Health problems for bereaved family dementia caregivers may have continued or have started after the care recipient’s death; therefore, it is essential to consider applicable medical specialist referrals for those bereaved dementia family caregivers at risk of poor bereavement outcomes (Corey & McCurry, 2018; Grasel, 2002; Groh & Saunders, 2020; Vlachogianni et al., 2016). (Grasel, 2002) investigated the presence of somatic symptoms in bereaved dementia family caregivers and discovered that while reports of aching limbs, heart complaints, and physical exhaustion decreased 6 to 12 months after the care recipient’s death, the number of physician office visits increased. Maintaining regular contact with the bereaved dementia family caregiver for evaluation and follow-up is crucial, and this can be conducted via email, phone, or health portal.
When considering an adaptive grieving response, healthcare professionals should assess the bereaved dementia family caregiver’s physical ability, stamina, and emotional and psychological status if they render hands-on caregiving to another person (Corey & McCurry, 2018; Vlachogianni et al., 2016). In addition, recognizing the value to the bereaved dementia family caregiver in caring for and supporting others is essential. Bereaved dementia family caregivers who established new caregiving roles found tremendous value and self-satisfaction. (Larkin, 2009) found that 70% of their sample of post-death family caregivers were identified as “serial caregivers” (p. 1038). Serial caring connotates a cyclical nature to post-care for individuals. Some participants said it was a “lifestyle” for them and that “you can’t stop caring, really” (Larkin, 2009, p. 1038). Many bereaved dementia family caregivers felt obligated to resume caregiving duties for other family members due to familial ties and responsibilities. Evidence from this study suggests potential consequences of serial caring in which half of the serial caregivers suffered health difficulties after the care recipient’s death (Larkin, 2009).
When healthcare professionals engage with bereaved dementia family caregivers, adaptive grieving information, recommendations, and education can be provided, including encouraging positive understandings and reflection on the care recipient’s life and death (Peacock et al., 2018; Rolbiecki et al., 2023). Healthcare professionals can reassure bereaved dementia family caregivers that feelings of relief upon a care recipient’s passing are normal and justified (Stahl & Schulz, 2019). To assist bereaved dementia family caregivers in managing their thoughts so they can consider the positive aspects of grieving, healthcare professionals can offer acceptance-based strategies (i.e., “I am less stressed now and can focus on myself,” and “I now have time to enjoy the activities that I used to do before I was a caregiver.”) (Stahl & Schulz, 2019, p. 8).
Other recommendations for healthcare professionals are to refer and connect the caregiver to applicable resources such as grief counseling, grief or bereavement support groups, chaplain or pastoral services, and healthy support networks; consider online support groups for those in rural settings or unable to attend in-person meetings. Formal support was conducive to a more adaptive bereavement for bereaved dementia family caregivers (Groh & Saunders, 2020; Jameson et al., 2020; Jensen et al., 2020; Romero, 2021). Bergman et al. (2011) report that nearly a third of the participants in their study used counseling, support groups, or psychotropic medication to manage their grief, and 13% participated in a bereavement support group. Crespo et al. (2013) found that 16% of their sample of dementia family caregivers accessed bereavement services, and more than twice that number reported that they needed to attend one. Unfortunately, very little formal support is offered to dementia family caregivers post-death (Arruda & Paun, 2017). Due to a lack of support, family caregivers frequently endure emotional anguish, loneliness, and even social isolation for up to 18 months following the death of the PWD (Almberg et al., 2000). And for family caregivers whose PWD passed away in long-term care, formal support was found to be essentially absent (Arruda & Paun, 2017; Givens et al., 2011; Murphy et al., 1997).
Organizations such as the Alzheimer’s Association, Area Agencies on Aging, grassroots dementia organizations such as Hilarity for Charity, and hospice agencies offer support groups for bereaved dementia family caregivers. Using these resources shows a willingness to advance and accept assistance (Jensen et al., 2020). For those struggling with grief, healthcare professionals can consider bereaved dementia family caregiver participation in a program like the Meaning in Loss Group (12-week group therapy), which teaches participants how to cope with death, restore a link with the deceased, and live meaningful lives (Romero, 2021).
Another effective coping strategy “that filled the void” (Corey & McCurry, 2018, p.e92) for bereaved dementia family caregivers was volunteering for dementia-related organizations. Healthcare professionals can share dementia-related advocacy volunteer resources with the bereaved dementia family caregiver as applicable (Corey & McCurry, 2018; Jameson et al., 2020; Peacock et al., 2018). Greenwood et al. (2013) discovered that bereaved dementia family caregiver volunteers enjoyed their prior caregiving roles, citing satisfaction from putting their own previous caregiving experiences to good use. Peer support assisted both bereaved dementia family caregivers and peer volunteers in realizing that they were “not alone” in their feelings and experiences (Greenwood et al., 2013). Other volunteering advantages for bereaved dementia family caregivers included freely discussing painful situations and learning how others cope.
Reclaiming Activities
Healthcare professionals can encourage bereaved dementia family caregivers to resume their favorite pastimes and pursue new hobbies and interests (Peacock et al., 2018). Bereaved dementia family caregivers expressed that staying active in activities such as housework, church service, outdoor activities, entertainment, travel, and community centers had experienced a much more adaptive grieving post-death, but in their own time and when they felt ready. Providing other ideas healthcare professionals might suggest, Stahl and Schulz (2019) also explored the areas of sports, quiet time by oneself, attending clubs, church activities, hobbies, spending time with family and friends out at restaurants, friend, and family visiting, engaging in other fun things with people, going out of town on vacation, spending time outdoors and in settings like parks, and “unwinding” at the end of the day. Recommendations for timing this encouragement should be based on the individual caregiver.
Part of the bereavement process involves reestablishing treasured areas of life, which had often been placed on hold as the care recipient’s dementia progressed and required more care (Peacock et al., 2018). Bereaved dementia family caregivers should determine the timing for this reintegration; some find it vital to leap right back into their involvement in various activities after their care recipient died, whereas others need a period of respite to recharge or engage in more active grieving. Revisiting prior hobbies might help a bereaved dementia family caregiver through their grief path (Chattillion et al., 2012; Gibson et al., 2019). Healthcare professionals need to have an open discourse about reintegration between bereaved dementia family caregivers and their supports during the early stages of grieving, where flexibility in resuming community activity is encouraged.
Further Healthcare Professional Opportunities
External to providing services during healthcare visits or hospital stays, healthcare professionals may employ other opportunities to supplement and address an adaptive grief response for bereaved dementia family caregivers. Healthcare professionals can create and possibly facilitate support groups that are aimed specifically for bereaved dementia family caregivers (Corey & McCurry, 2018). For example, the Alzheimer’s Association offers free facilitator training for volunteers interested in leading bereaved dementia family caregiver support groups (“2023 Alzheimer’s Disease Facts and Figures,” 2023). Healthcare educators can raise awareness of the long-term implications of dementia caregiving on health by developing training programs for healthcare professionals, and they can incorporate information on bereaved dementia family caregivers into nursing and medical school curricula (Corey & McCurry, 2018). Healthcare professionals can conduct research or be involved in clinical studies that support adaptive grieving provisions for bereaved dementia family caregivers (Crawley et al., 2022).
Limitations and Future Directions
The reviewed studies had several commonalities that may inhibit generalizability. For example, the time between a care recipient’s death and the interview’s time varied considerably and ranged from one month to 10 years. Two studies reflected the care recipient’s death had occurred in the last six months of post-care (Jensen et al., 2020; Supiano et al., 2022). For those studies highlighting the samples of bereaved dementia family caregivers who were newly bereaved, a longer follow-up would allow insight into the long-term exploration of adaptive grief responses. These design differences may also make it difficult, at times, to determine whether some sources of adaptive grieving are better or worse to use in the post-death trajectory. A more comprehensive study longitudinally exploring the experiences of a wide swathe of bereaved dementia family caregivers (ideally including time before death) would be instructive in better understanding this population and how adaptive grief experiences change over time.
There was also a lack of ethnic and cultural diversity in the samples, with most participants being female and White. In part, this may be because several studies used convenience sampling. The field has been calling for improvement in the representativeness of bereaved dementia family caregiver research for many years, and we join those calls (Arruda & Paun, 2017; Chan et al., 2013). Relatedly, excluding non-English and gray literature might have resulted in the omission of understanding how other cultures deal with dementia-related deaths.
“Compassionate Communities” may be one promising avenue for bereaved dementia family caregivers to receive social supports. These initiatives create supports addressing the social epidemiology of grief and loss (Aoun et al., 2018). Compassionate Communities locate and foster neighborhood networks of compassion for the dying and their families. Additionally, Compassionate Communities normalize asking for and accepting assistance from family, friends, neighbors, schools, and places of employment. Compassionate Communities advocate that supporting those grieving is not only the responsibility of health and social services but also everyone’s duty (Aoun et al., 2018). The concept of Compassionate Communities has been discussed in the dementia friendly communities’ movement and represents an optimistic area for future study in the context of bereaved dementia family caregivers (Dumont et al., 2022).
Conclusion
Losing a family member to dementia after years of caregiving can be extremely challenging. But it is a challenge that has already been faced by millions who have discovered myriad ways to decrease the burden. We hope this work will help bereaved dementia family caregivers employ insights gained from studies of bereaved dementia family caregivers who have successfully faced the challenge of their bereavement. Opportunities for more adaptive grief responses largely fall into the categories of social health, emotional and spiritual fitness, and reclaiming activities. Recognition of bereaved dementia family caregivers' experiences by healthcare professionals is critical. Empowered with a better understanding of how this population might grieve more adaptively, those healthcare professionals might help encourage more adaptive grieving.
Footnotes
Acknowledgments
The authors thank Ms. Janice Hermer, Arizona State University Health Sciences Librarian, for her valuable contribution to the literature search.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Award Numbers R00AG073463. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.