
Abstract
Bereaved persons seeking help in bereavement counselling report generally high client satisfaction. However, qualitative research suggests that some clients also indicate dissatisfying experiences and negative effects. The aim of this study was to investigate the contribution of content-, counsellor- and client-related characteristics and negative effects to client satisfaction. Bereaved participants (n = 53) who had completed bereavement counselling were recruited either online or via counselling organizations. In an online survey, they provided information about client-, loss- and counselling-related variables, present grief severity, negative effects of counselling and client satisfaction. In a hierarchical linear regression analysis controlling for recruitment strategy, online-recruited participants were less satisfied. In a second step additionally considering number of sessions, grief severity and negative effects, experiencing more negative effects predicted lower client satisfaction. The results indicate that negative effects could play an important role for client satisfaction. More research is needed to investigate this phenomenon.
Introduction
Bereavement Counselling as a Preventive Intervention
The death of a loved one is a very significant, yet common life event. Most persons (about 60%) will adapt to bereavement with the support of family and friends and recover from their grief within a year (Aoun et al., 2015; Bonanno & Kaltman, 2001). However, there is a broad consensus that the remaining 40% may require some form of psychosocial support (Killikelly et al., 2021). Depending on the severity of the grief-related distress and/or the presence of a mental health problem, this support may take the form of bereavement counselling services or psychotherapy. Bereavement counselling services support persons experiencing a period of crisis after the loss of a loved one with the aim to prevent clinically relevant disorders and negative long-term health consequences. These services can take various forms, as described in the meta-analysis by Forte et al. (2004). Services differ significantly based on their target group (e.g., bereaved parents or people bereaved by terminal illness), format (e.g., group or individual format), content of the intervention (e.g., focus on providing information or on social interactions), facilitation (e.g., professional facilitator or self-help) and duration of the intervention (e.g., single activities or regular sessions). Other meta-analyses also note and examine the wide heterogeneity in bereavement interventions (Harrop et al., 2020; Kustanti et al., 2021). Previous research suggests that different factors may affect how much clients benefit from bereavement counselling services, such as loss-related variables (e.g., circumstances of the death), grief intensity (Johannsen et al., 2019) and characteristics of the intervention (e.g., method of referral) (Allumbaugh & Hoyt, 1999; Currier et al., 2008; Geron et al., 2003; Neimeyer & Currier, 2009).
Client Satisfaction With Bereavement Counselling
Client satisfaction in health care services in general tends to be highly positive and to demonstrate little variability (Edwards & Staniszewska, 2000). Previous studies have investigated different facets of client satisfaction with bereavement counselling. A first aspect concerns the subjective experience of distress reduction, which has been reported for physical symptoms and feeling the loss less intensively (Gallagher et al., 2005). As a second aspect, high satisfaction with the themes and contents of the counselling has also been demonstrated (Barlow et al., 2010; Diamond et al., 2012; MacKinnon et al., 2015). Third, previous research indicates the relatively high satisfaction with the person providing the counselling service, e.g., the skills of the counsellor (Gallagher et al., 2005). Other studies have assessed more broad aspects of client satisfaction such as satisfaction with the service in general (Mcgrath, 2001; Zainudin & Yusop, 2018), helpfulness of the service (McGuinness et al., 2015), or overall valence of the counselling experience (Henoch et al., 2016). All yield very favorable results. In contrast, however, a more recent population-based study asked 678 bereaved adults which sources of support they had used and how helpful they considered them. Interestingly, professional sources like individual counselling and support groups had the highest proportion of perceived unhelpfulness (23% resp. 41% a little/not helpful) (Aoun et al., 2018). In the qualitative studies of Gallagher et al. (2005) and deCinque et al. (2006) some clients described not being satisfied with the service. A minority of ex-clients stated that counselling was “not for them” (Gallagher et al., 2005) and two out of three parents after the death of a child reported that bereavement counselling did not provide any help to them (deCinque et al., 2006). Diamond et al. (2012) asked clients for suggestions to improve counselling service and found that some would have preferred more directive leadership by the counsellor and an earlier start of counselling after the loss. These studies indicate that although client satisfaction in general is very high, there seems to be a minority of less satisfied participants. Thus, investigating factors that contribute to client satisfaction is highly relevant.
Factors Influencing Client Satisfaction in Bereavement Counselling
Evidence regarding the factors contributing to client satisfaction comes from qualitative research. Among these studies (Aoun et al., 2018; Barlow et al., 2010; deCinque et al., 2006; Diamond et al., 2012; Geron et al., 2003; Henoch et al., 2016; Klasen et al., 2017; Mcgrath, 2001; Simonsen & Cooper, 2015), there are some noticeably consistent findings across different samples of clients. One of the most relevant factors that contributes to client satisfaction is a good counselling relationship, which is associated with different helpful aspects in previous studies. As one aspect, a respectful and trustful atmosphere provides reassurance and hope (Diamond et al., 2012; Klasen et al., 2017; Mcgrath, 2001). Another important aspect are positive qualities of the counsellor (e.g., being warm and friendly, a good listener and non-judgmental) (Diamond et al., 2012; Mcgrath, 2001). As a third aspect, social support, and the feeling of not being alone seem to be very helpful for most clients (Aoun et al., 2018; Diamond et al., 2012; Henoch et al., 2016). Fourth, understanding and sharing one’s experiences, especially with a person in the same situation and outside one’s social environment, is perceived as helpful (Barlow et al., 2010; Diamond et al., 2012; Henoch et al., 2016; Simonsen & Cooper, 2015). Other frequently named factors are gaining more insight in one’s feelings, thoughts and behavior associated with grieving, psychoeducation and challenging dysfunctional thinking, and gaining new perspectives (Barlow et al., 2010; Diamond et al., 2012; Gallagher et al., 2005; Klasen et al., 2017; McGuinness et al., 2015; Simonsen & Cooper, 2015). To summarize, previous research suggests certain content- and counsellor-related factors that contribute to client satisfaction. At the same time, quantitative studies systematically examining the predictors of client satisfaction are missing. Additionally, information about participant- and loss-related factors (e.g., age or relationship to the deceased) that may contribute to client satisfaction in grief counselling could be of great interest in determining who might benefit most from what type of grief counselling.
Negative Effects of Bereavement Counselling
An important factor that may contribute to client dissatisfaction is a potential negative effect of bereavement counselling. Negative effects might occur in almost any kind of intervention. For example, they are known to exist in psychotherapy and are the subject of current research (Herzog et al., 2019; Moritz et al., 2019; Schermuly-Haupt et al., 2018). Since bereavement counselling is a psychosocial intervention and therefore shares some characteristics with psychotherapy (e.g., the establishment of a therapeutic alliance requiring trust and openness from the client), it is reasonable to assume that negative effects could occur also in bereavement counselling.
There are various concurrent definitions of negative effects of psychosocial interventions that use different terminologies and vary with regard to what type of event should be considered a negative effect (Dimidjian & Hollon, 2010; Linden, 2013; Rozental et al., 2018). Following the seminal work of Hadley and Strupp (1976) negative effects represent adverse changes in the client’s condition that have a temporal and causal relation to the intervention. Negative effects can either be unintended detrimental consequences of properly applied interventions (side effects) or result from inappropriate applied interventions, e.g., unethical behavior and malpractice (Ladwig et al., 2014). More than a decade ago, Schut and Stroebe (2011) stated that one important task in the evaluation of bereavement counselling is to investigate potentially harmful side effects of counselling. Since then, various studies have contributed to our knowledge about potential negative effects. Some studies have reported that clients experience a worsening of their symptoms or develop new symptoms after counselling (Gallagher et al., 2005; Høeg et al., 2017). There are also accounts of negative experiences with the person providing the counselling. Aoun et al. (2018) asked bereaved persons about unhelpful aspects of different sources of support. Regarding professional help sources, the participants critically remarked upon the insensitivity of grief counsellors, a lack of empathy from the counsellor or poor advice from the counsellor. These could be indications of negative effects in the area of therapeutic malpractice according to Ladwig et al. (2014). Finally, based on studies demonstrating no or even negative effects for bereavement counselling (Currier et al., 2008; Neimeyer, 2010) one might speculate whether there are contraindications to counselling. In this vein, Johnsen et al. (2012) reported that participants with a diagnosis of prolonged grief disorder (PGD) taking part in a grief support group were less satisfied and experienced less positive effects than participants without PGD. Taken together, these findings suggest that not all clients are satisfied with bereavement counselling services and that the behavior and statements of the counsellor specifically could influence perceived dissatisfaction.
Importantly, the present data may underestimate the extent and relevance of negative effects of bereavement counselling (Edwards & Staniszewska, 2000). First, participants may give socially desirable answers, especially if the assessment is conducted by the service provider. Second, most of the present studies assess data in convenience samples at the end of the counselling process. However, clients with more negative experiences may leave the bereavement counselling early or may be less motivated to take part in an evaluation. Thus, more satisfied participants who have not experienced negative effects may be overrepresented. Third, even though many evaluation studies use open-ended questions to allow participants to indicate any unhelpful or negative aspect or suggestions for improvement regarding bereavement counselling, this option is typically used less or not at all, compared to mentioning helpful or positive aspects (Aoun et al., 2018; Diamond et al., 2012; Gallagher et al., 2005; Simonsen & Cooper, 2015).
Aims of the Current Study
Previous research demonstrates that many clients report high satisfaction with bereavement counselling. Qualitative studies have suggested that content- and counsellor-related factors may contribute to client satisfaction. However, quantitative studies that can identify the respective contribution of the various factors to client satisfaction are lacking. Additionally, little is known about the potential impact of negative effects of bereavement counselling on client satisfaction.
The present study therefore aimed to investigate the relative contribution of content-, counsellor- and client-related characteristics as well as negative effects of counselling to client satisfaction with bereavement counselling. As this was an exploratory pilot study, it examined whether there are general factors that contribute to client satisfaction, despite the wide variability of services.
Methods
Procedure and Recruitment
Ethical approval was obtained from the institutional review board. Data was collected between October 2020 and January 2022 using an online survey hosted by Qualtrics software (Qualtrics, Provo, UT, USA). Participants were recruited in two different manners: Organizations providing bereavement counselling services in Bavaria distributed the information and link to the study to former clients. Additionally, recruitment ads were posted online, e.g., in forums for grieving persons, on relevant websites or in social media groups. Once the participants accessed the online survey via the link, they were presented with a detailed study information including the purpose of the study, voluntariness of participation and confidentiality. Inclusion criteria were (1) age ≥ 18 years, (2) having experienced the death of a significant other, (3) having used bereavement counselling services in Germany and (4) having completed the counselling at the time of survey. Participants were excluded if they stated that they would feel too distressed by answering questions about their bereavement experience. Criteria for inclusion and exclusion were assessed via self-report. All participants provided written informed consent. They received no financial reward or incentive for their participation.
Measures
Participant and Loss-Related Variables
Participant data included age, sex and whether participants were recruited online or via a counselling organization. Participants also provided loss-related information. This included time since loss (indicated by date of death), relationship to the deceased (i.e., spouse, child, parent, other family member or other significant person), and cause of death (natural, unnatural).
Counselling-Related Information
Regarding the bereavement counselling service, participants indicated the date of their first session, the time since the loss when counselling started and the number of sessions. In addition, participants provided information regarding the general conditions of the bereavement counselling, such as the setting (individual sessions, group sessions, family sessions), the format (personal contacts, video contacts, telephone contacts) and the waiting period until the first session.
Grief Severity
The Inventory of Complicated Grief (Prigerson et al., 1995) was used in its German version (ICG-D; (Lumbeck et al., 2012) to assess grief severity. It consists of 19 items that describe cognitive, emotional and behavioral reactions relevant to prolonged grief (e.g., “I think about this person so much that it’s hard for me to do the things I normally do”). Participants rate these items concerning their frequency of occurrence within the past four weeks on a 5-point Likert scale ranging from never (0) to always (4). A total score is calculated by summing the individual items, with higher scores indicating higher grief severity. ICG-D scores ≥ 25 indicate clinically relevant grief symptoms (Lumbeck et al., 2012). The questionnaire shows satisfying reliability and validity (Lumbeck et al., 2012). In our sample, Cronbach’s alpha was .91.
Negative Effects of Counselling: The Modified INEP
The INEP (Inventar zur Erfassung Negativer Effekte von Psychotherapie) is a German questionnaire to assess negative effects of psychotherapy (Ladwig et al., 2014). It measures negative outcomes after psychotherapy in seven areas (intrapersonal changes, partnership, stigmatization and financial worries, family, friends, dependency, therapeutic malpractice). The INEP has demonstrated good reliability in patients after psychotherapy with Cronbach’s alpha = .86 (Ladwig et al., 2014). Significant correlations with a poor therapeutic alliance and unmet treatment expectations indicate its criterion validity (Herzog et al., 2019; Ladwig et al., 2014).
To the best of our knowledge, there is no respective questionnaire to assess negative outcomes in counselling. We therefore adapted four questions from the INEP in wording to the context of bereavement counselling that seemed the most suitable. Since the therapeutic relationship is a very important factor in bereavement counselling, we chose the subscales therapeutic malpractice and dependency (Aoun et al., 2018; Klasen et al., 2017; Morawetz, 2007) From the subscale therapeutic malpractice, we selected the two items with the highest rates of occurrence in previous research (Ladwig et al., 2014): “During counselling, my counsellor made hurtful statements” and “During counselling, my counsellor forced me to do things that I really did not want to do”. The subscale dependency consists of two items, which were both adopted (“Since completing my counselling, I have felt dependent on my counsellor”, “Since completing my counselling, it is more difficult to make decisions on my own”). Subjects rated these items on a four-point resp. five-point scale. The four items were summed to create a total score (range 0–13) with higher values indicating more negative outcomes after the counselling. In our sample, Cronbach’s alpha was .50.
Client Satisfaction: The Client Satisfaction Questionnaire-8
The Client Satisfaction Questionnaire-8 (CSQ-8; Attkisson & Zwick, 1982) assesses clients’ retrospective satisfaction regarding the service received using eight items. A German version has been established (Häring & Hüsing, 1992) and is incorporated into the questionnaire on educational and family counselling (FEF; Fragebogen zur Erziehungs- und Familienberatung; (Vossler, 2001). Items are rated on a four-point Likert-scale with different anchors depending on the respective question (e.g., “Did the counselling service fulfill your needs?”; Almost all, most, only some, none). A total score is calculated by summing all items and dividing the sum score by eight. The total score can range from one to four, with higher scores indicating higher client satisfaction. It shows satisfying results for reliability (Cronbach’s alpha = .94 for the subscale CSQ-8) and validity (Vossler, 2001). In our sample, Cronbach’s alpha was .94.
Sample
Sample Characteristics (n = 53).
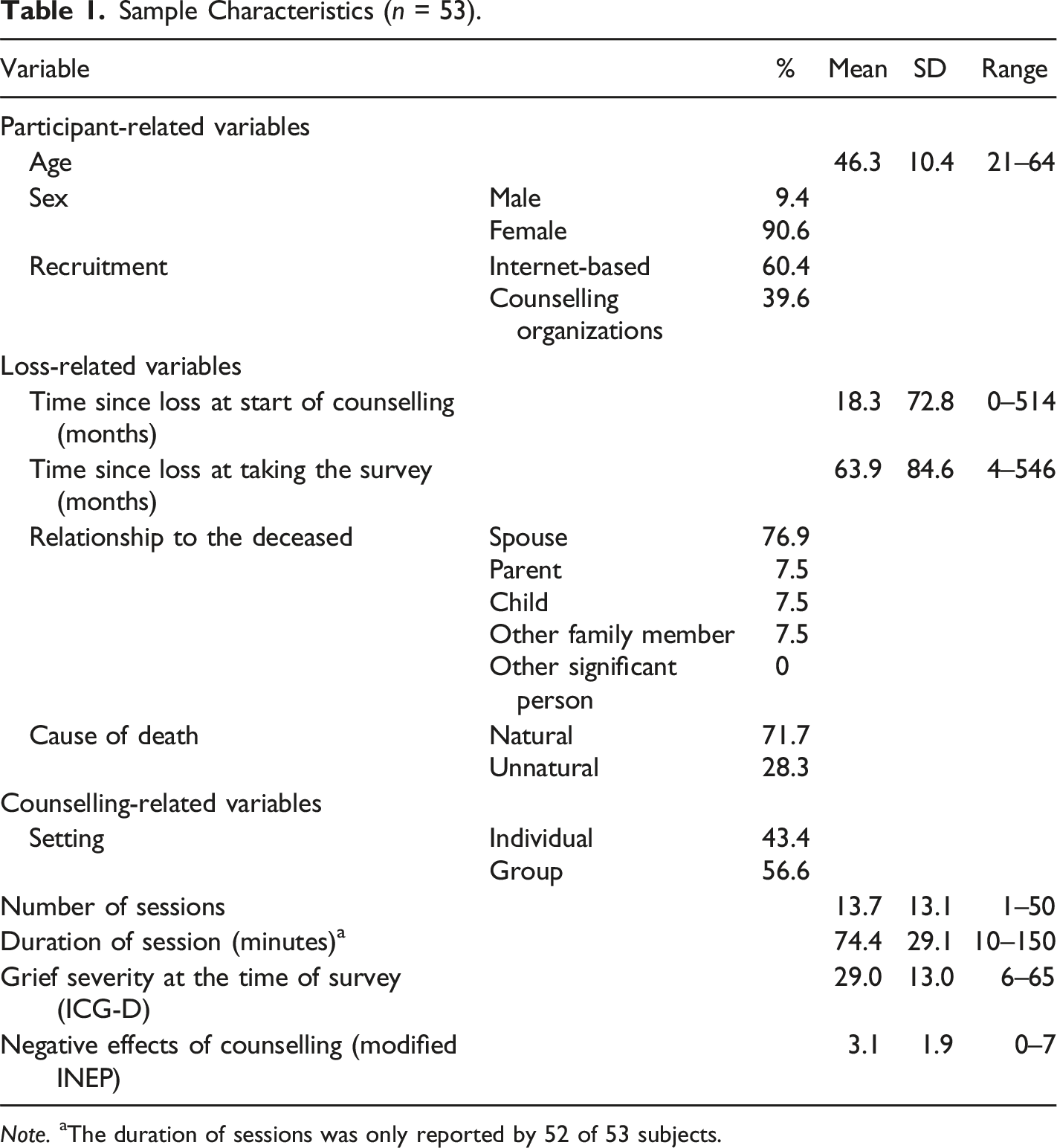
Note. aThe duration of sessions was only reported by 52 of 53 subjects.
Missing Data
One participant provided information for the ICG-D in all but one item. Likewise, two participants answered all but one item in the FEF and two participants filled out all but one item in the modified INEP. In these five cases, the missing values were replaced with the mean of the relevant questionnaire.
Analysis
Analyses were performed using IBM SPSS Statistics 25. Sample characteristics were summarized using descriptive statistics. In a first step, bivariate Pearson correlations and Spearman´s rho correlation coefficients explored the associations between client satisfaction and the client-related, loss-related, and counselling-related variables. Variables that demonstrated a significant bivariate correlation with client satisfaction (p ≤ .05, two-sided) were used as predictors in the multiple linear regression analysis with the criterion client satisfaction. Bonferroni-corrected p-values for the bivariate correlations were calculated. Variables were included blockwise in the regression model using the ENTER method. The first block contained the respective client-related variables, the second block the loss-related variables and the third block contained the counselling-related variables. The following variables were dummy-coded: recruitment (0 = via organizations, 1 = internet-based); cause of death (0 = natural, 1 = unnatural); setting (0 = individual, 1 = group). For the relationship to the deceased, participants could indicate whether the deceased person was a spouse/partner, a child, a parent, another family member, or another significant person. As no participant indicated the loss of an “other significant person”, the remaining possibilities were clustered in two categories for the dummy coding: any family member (0) and child (1). The loss of a child represented a distinct category because it has been shown to be a risk factor for complicated and prolonged grieving and is associated with unique cognitions and emotions (Djelantik et al., 2020; Kersting et al., 2011; Lundorff et al., 2017; Morris et al., 2019).
For the linear regression models, unstandardized coefficient B, standardized coefficient β, 95% confidence intervals (CIs), the adjusted determination coefficient adj. R 2 and the change in R 2 (ΔR 2 ) are reported. P- values below .05 are considered statistically significant (two-sided). The leverage value criterion (Stevens, 2009) and Cook’s distance values (Atkinson et al., 1983) identified no outliers or influential cases. Inspection of the VIF and tolerance of independent variables showed little multicollinearity. Normality of residuals and homoscedasticity were inspected visually by using a Q-Q-plot and a scatterplot presenting the standardized residuals against the predicted standardized values. Both assumptions can be considered as fulfilled.
Results
Correlates of Client Satisfaction With Bereavement Counselling
Bivariate Correlations
Bivariate Correlations Between Client Satisfaction (CSQ-8) and Client-Related, Loss-Related, and Counselling-Related Variables.
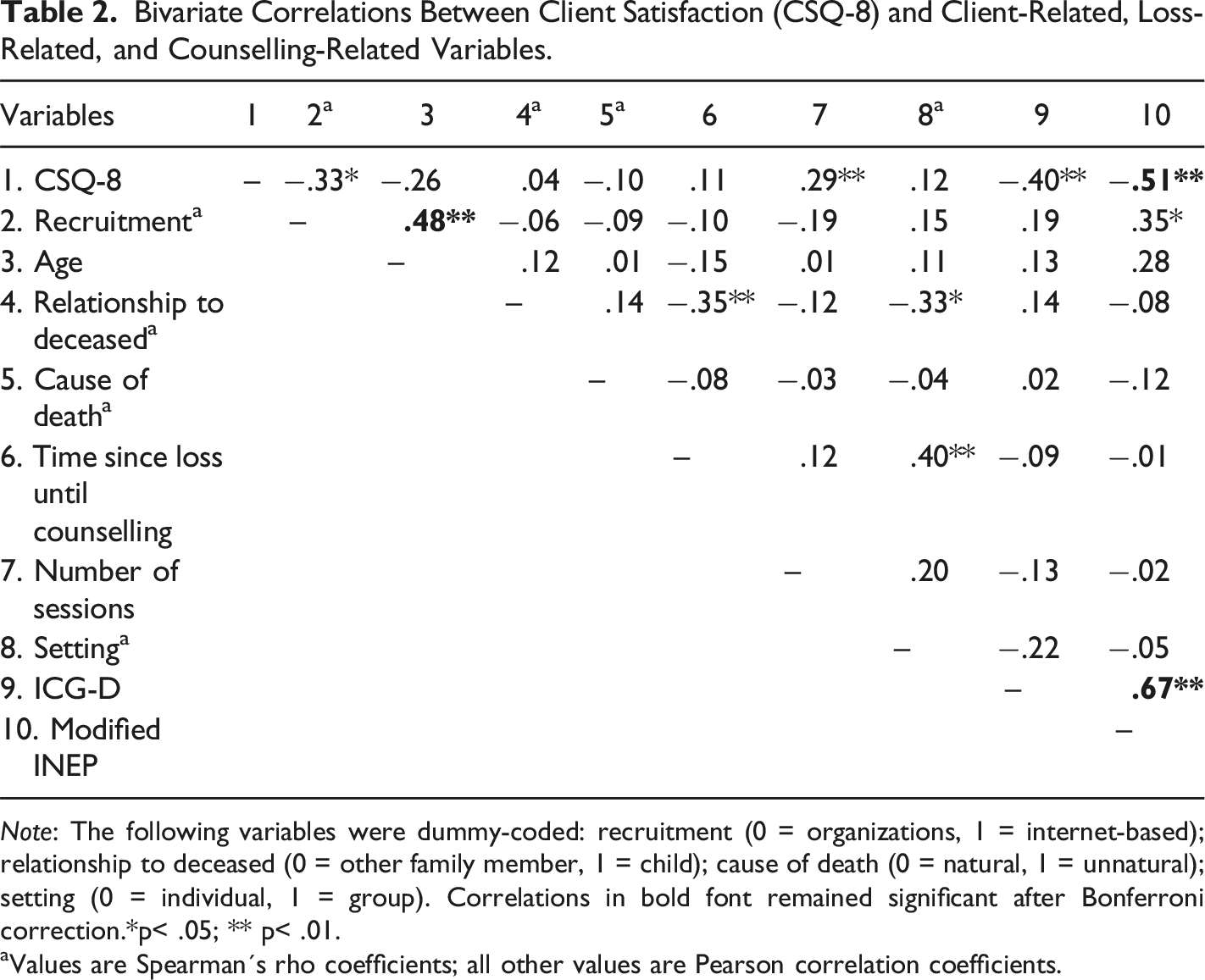
Note: The following variables were dummy-coded: recruitment (0 = organizations, 1 = internet-based); relationship to deceased (0 = other family member, 1 = child); cause of death (0 = natural, 1 = unnatural); setting (0 = individual, 1 = group). Correlations in bold font remained significant after Bonferroni correction.*p< .05; ** p< .01.
aValues are Spearman´s rho coefficients; all other values are Pearson correlation coefficients.
The correlation analysis also identified significant correlations among these potential predictors. Participants who were recruited online were older. Increased reporting of negative effects of counselling was associated with higher grief severity and online recruitment.
After Bonferroni-correction only three correlations remained significant (indicated by bold font). As Bonferroni correction is conservative and we did not want to exclude possible relevant predictors, we included all four variables in the subsequent regression analysis.
Multiple Linear Regression
Results of the Multiple Hierarchical Regression Analysis on Client Satisfaction With Counselling.
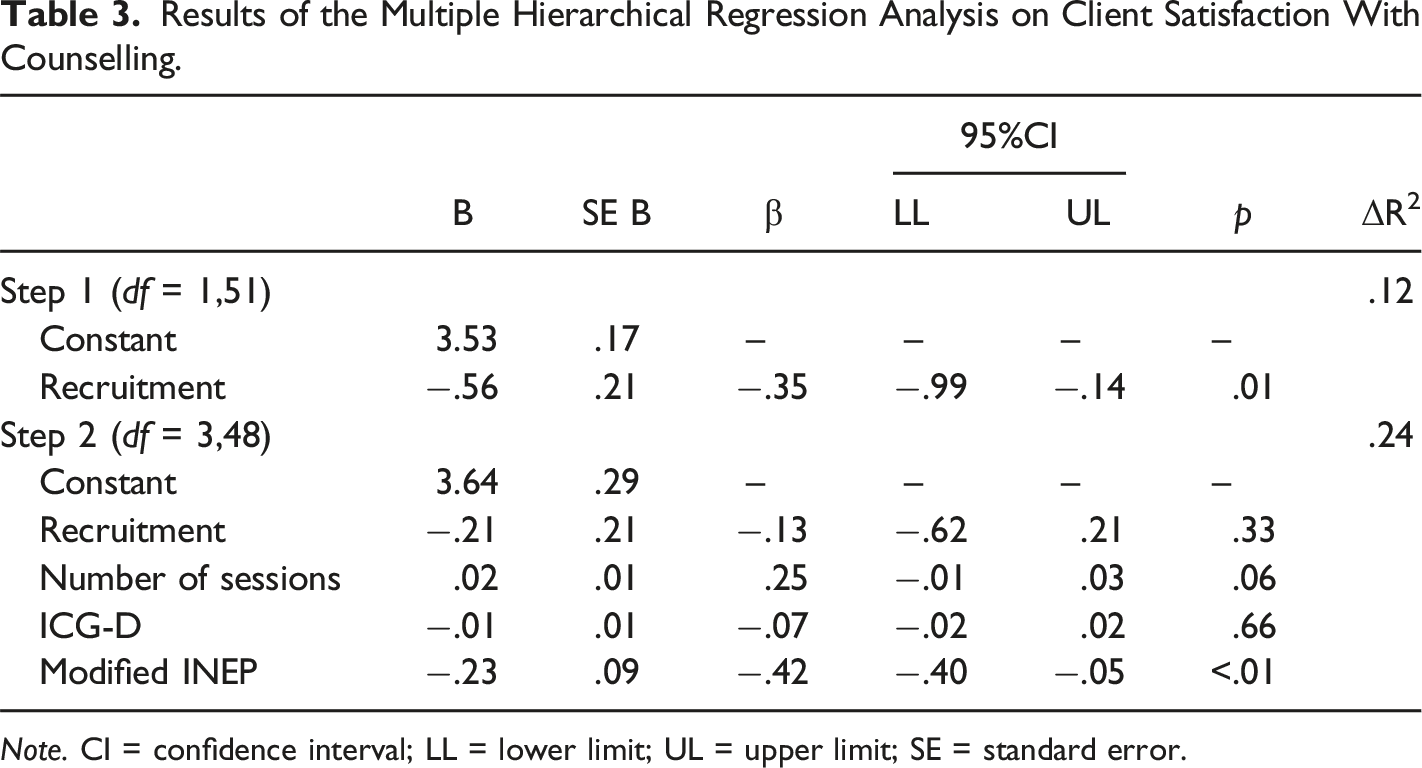
Note. CI = confidence interval; LL = lower limit; UL = upper limit; SE = standard error.
The hierarchical regression demonstrated in the first step that client-related variables significantly predicted client satisfaction [F (1,51) = 7.116; p = .01; adj. R 2 = .11]. Participants who were recruited online reported significantly less satisfaction. When entered in the next step, negative effects of counselling contributed significantly to client satisfaction, while the number of counselling sessions and grief severity (ICG-D) did not [F (3,48) = 6.678, p < .01; adj. R 2 = .30]. Thus, participants having experienced more negative effects of counselling were less satisfied. In this regression model, the predictor recruitment lost its previous significance.
Discussion
Summary of Results
In the present convenience sample of persons who had used bereavement counselling services in Germany, three counselling-related variables, namely the number of counselling sessions, the experienced negative effects in counselling and the intensity of grief symptoms after counselling were associated with the client satisfaction with bereavement counselling. Additionally, the method of recruitment for the study (internet-based vs. via counselling organizations) was associated with client satisfaction. When considering all variables simultaneously as predictors in a hierarchical regression analysis, only the experience of negative effects in counselling significantly predicted client satisfaction. The next sections discuss the results of the multivariate and bivariate analyses.
Multivariate Analysis
Overall, client satisfaction with the counselling services was high. Nevertheless, the present study shows that if negative effects are experienced, they are the single most important predictor for client satisfaction. The present study focused on only two aspects of negative effects, i.e. feeling dependent on the counsellor and experiences of malpractice, such as hurtful statements from the counsellor. In our sample, 30.2% of the clients reported at least one negative effect of bereavement counselling. Regarding psychotherapy, we have known for decades that negative effects can occur (Bergin, 1963), even though systematic research in this area is only nascent. Recent studies with different samples in different settings indicate that between 45% and 59% of inpatients (Rheker et al., 2017) and between 57% (Strauss et al., 2021) and up to even 93% (Ladwig et al., 2014) of outpatients report at least one negative effect of their therapy. Negative effects in psychotherapy thus do not represent a rare event. Our results suggest that they also occur in bereavement counselling. Surveys of clients at the end of counselling may underestimate the frequency of negative effects due to social desirability or self-selection biases (e.g., dissatisfied clients not providing feedback). On the other hand, the present study’s approach may overestimate these effects. Our study was conducted online and fully anonymous, so we had no possibility to control which clients participated. Clients who used bereavement counselling and were less satisfied with the service, probably also due to experienced negative effects, could seek further support in online-based services for bereaved persons and could be especially interested in participating in the study to share their personal experiences. Additionally, when specifically asked for negative effects, some clients could have indicated even mild and transient negative effects, which they would not consider as very stressful in the long term. To draw firmer conclusions regarding the prevalence of negative effects in counselling, larger and more representative samples are needed.
Interestingly, the most frequently reported items within the negative effects in our sample were items from the malpractice subscale (n = 15; 53% of all reported negative effects). For example, clients reported that their needs were not taken into account and or that the counsellor forced them to confront their negative emotions, although they did not want to and thus experienced the counseling as overwhelming. Importantly, such behavior may affect the therapeutic relationship (Strauss et al., 2021), which has been identified as one of the most important factors for client’s satisfaction (Aoun et al., 2018; Diamond et al., 2012; Henoch et al., 2016; Mcgrath, 2001). The present findings can be considered only preliminary due to the study’s methodological limitations as outlined below. Nevertheless, they highlight the need for future research to investigate this important phenomenon.
Bivariate Associations
In addition to the hierarchical multiple regression analysis, we also examined univariate associations with client satisfaction and report them since quantitative research of factors that contribute to client satisfaction in bereavement counselling is rare. In addition to negative effects of counselling, the number of sessions, recruitment method, and post-counselling grief severity significantly correlated with client satisfaction in our sample.
A higher number of sessions was significantly associated with higher satisfaction. This is in line with other studies demonstrating that dissatisfied clients used fewer sessions than more satisfied clients (Diamond et al., 2012; Relf, 2000). One possible explanation would be client’s commitment with the counselling sessions. More satisfied clients could reasonably be more committed and therefore use a higher number of sessions. Unsatisfied clients on the other hand may tend to terminate the counselling process prematurely.
For the present study, bereaved participants were recruited in two different ways: Either via organizations providing bereavement support services or via internet-based methods, like forums and websites for bereaved people. Clients recruited via internet-based methods were less satisfied with the counselling. One explanation could be that the organizations reached out to potential participants through their newsletters, news sections on their homepages or mailing lists. Probably, former clients will maintain contact with the organization if they have been satisfied with the service. The internet-based recruitment may have reached predominantly clients who had used bereavement counselling and found it not satisfactory, thus still seeking further support in forums, websites, and online-based services for bereaved persons. This hypothesis is supported by the fact that in our sample, online recruitment was also associated with higher grief symptoms after the counselling service and more negative effects of counselling. These results suggest that different recruitment methods reach different populations of participants. Previous studies using the same two recruitment strategies have also noted differences between the respective samples in terms of demographic and loss-related characteristics (Nager & Vries, 2004; Stelzer et al., 2020; Tolstikova & Chartier, 2009). For example, recruitment efforts through community institutions (like bereavement organizations) reached more male participants, whereas advertisement in print and electronic media (like social media platforms or websites) reached more female participants (Stelzer et al., 2020). Another study demonstrated that bereaved persons who were recruited via internet-based methods reported higher grief intensity than bereaved participants in studies without internet-based recruitment (Nager & Vries, 2004). Researchers should keep in mind that the different ways of recruiting participants especially in bereavement research may result in different sample characteristics and influence other bereavement-related variables.
Additionally, grief severity after the counselling was negatively associated with client satisfaction. In our sample, present grief severity, i.e. after the counselling, still seemed to be relatively high: 60% of the sample indicated an ICG-value above the cut-off (Lumbeck et al., 2012) with potentially clinically significant grief symptoms. Importantly, for the majority of the participants (94.3%), the loss dated back more than six months. While these data do not establish a diagnosis, it is possible that our sample included a substantial number of persons who would at present partly or even completely fulfill the criteria for PGD. Our data do not indicate how severe the participant’s grief reaction was at the beginning of the counselling. Nevertheless, the significant association between present grief severity and client satisfaction offers tentative support for the finding of Johnsen et al. (2012), i.e., that participants fulfilling the diagnosis of PGD were less satisfied with bereavement counselling. Future prospective research using clinical interviews to establish the diagnosis should investigate this hypothesis.
Future Directions
Our study suggests relevant directions for future research. One tentative finding is that a relevant number of former clients report having experienced negative effects of bereavement counselling. To substantiate or refute this claim, a properly designed instrument to measure negative effects especially in the context of bereavement counselling is needed, which should be validated accordingly. Lacking such an instrument, we focused on only two aspects of possible negative effects and assessed them with only two items. Thus, in a first step, future research is needed to define what constitutes negative effects in bereavement counselling to examine how frequently these effects occur. In a next step, future research can then shed more light on the processes that contribute to negative effects, e.g. client-, counsellor- or intervention-related variables. Furthermore, the associations of the client- and counselling-related variables with client satisfaction should be corroborated by prospective research in larger and more diverse samples of bereaved people. Future research should also assess additional factors that can contribute to client satisfaction, e.g., client’s expectations for bereavement counselling services, pre-existing psychological distress, and grief severity at entering the counselling service. Overall, client satisfaction with bereavement counselling services was high. It would be interesting to investigate whether this positive subjective evaluation is associated with objectively measured changes in grief severity or related quantitative measures after counselling. Therefore, high quality intervention studies, including intent-to-treat-analyses are needed.
Strengths and Limitations
When interpreting the results of this study, several limitations must be considered. First, the present study relies on a relatively small convenience sample, which limits the generalizability of the findings. Of our sample, 90% were female. The overrepresentation of female participants is a well-known phenomenon in bereavement research (Stelzer et al., 2020). In our sample, satisfaction with bereavement counselling was not associated with gender, however, the influence of a gender effect on the results cannot be ruled out. Additionally, the sample was relatively homogeneous regarding the loss-related variables, with more than two thirds of the subjects losing a spouse to a natural cause of death. Thus, the influence of loss-related variables would be difficult to detect in our sample. Second, there was no restriction with regard to the counselling services that the participants had used. Counselling services are highly diverse, ranging from individual sessions by professional counsellors to organized social activities such as bereavement weekends for specific groups of bereaved persons. We could not control for these differences in services, which are certain to affect client satisfaction. Third, the assessment of negative effects after bereavement counselling was based on four items from an existing questionnaire for negative effects in psychotherapy. The small number of items affected the measure’s internal reliability negatively and its validity for the context of counselling remains to be tested. Additionally, the participants reported the negative effects retrospectively; thus, memory biases cannot be excluded.
Our pilot study considered only a limited number of participant-, loss-, and counselor-related factors that can contribute to client satisfaction. Additionally, it was cross-sectional. However, across services, different factors could contribute to client satisfaction. Satisfaction with bereavement counselling services may be a multifaceted construct and its determinants may also vary dynamically. Factors that contribute to higher satisfaction at the beginning of the counselling may not do so at the end of the counselling (Chou et al., 2001; Hsieh, 2018; Nelson & Steele, 2006). Thus, our study only provides preliminary findings.
At the same time, the study shows some important strengths. To the best of our knowledge, this is the first study to systematically and quantitatively investigate negative effects experienced by clients in bereavement counselling. It complements the existing qualitative studies regarding the factors contributing to client satisfaction with bereavement counselling through a quantitative approach. The association between client’s satisfaction and negative effects has face validity and may seem obvious. Nevertheless, negative effects have received little attention in research on bereavement counselling, and there is no quantitative study that statistically quantifies this association. We used well-established quantitative measures wherever possible to investigate well-defined concepts like the grief severity and client satisfaction.
Conclusion
Client satisfaction with bereavement counselling is generally high. However, some clients also report negative effects of bereavement counselling. These negative effects seem to play an important role for client satisfaction. While our results remain tentative due to methodological limitations of our study, they highlight a need for further research. It is important to look at factors that contribute to lower satisfaction, such as experiencing negative effects, and to understand better who experiences negative effects in counselling and why. Ultimately, this research can contribute to the improvement of bereavement services and further optimize support for bereaved persons.
Footnotes
Acknowledgements
The authors would like to thank all counselling organizations for their support regarding the recruitment of clients as well as all bereaved participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Bavarian State Ministry of Family Affairs, Labour and Social Affairs.