
Abstract
Telephone bereavement support is recommended in bereavement care policy and practice; however, little is known about what constitutes best practice. To explore how best practice in telephone bereavement support is conceptualized by those who provide the service, 26 healthcare professionals working in Australian hospitals, hospices, and other palliative care settings were interviewed. Thematic analysis was used to construct seven themes: A Valuable Service with Limited Resources, The First Call, The Dance of Rapport, A Space to Share, Identifying and Responding to Risk, Maintaining Contact, and Training and Development Needs. Participants viewed telephone bereavement support as an effective and accessible tool in supporting individuals’ processing of and adaptation to loss; however, concerns remain regarding the quality and consistency of care provided. Greater resourcing of bereavement care is required, and telephone bereavement care providers’ perspectives offer a foundation to ensure the service is evidence-based, pragmatic, and supported by quality training.
Introduction
Bereavement is a universal human experience associated with psychological (e.g., sadness) and physiological (e.g., chest pain) experiences known as grief (Kowalski & Bondmass, 2008). While the intensity of grief typically dissipates over time, approximately 10% of bereaved individuals experience prolonged grief disorder (PGD; Lundroff et al., 2017), which is characterized by persistent yearning for the deceased alongside emotional suffering that may comprise feelings of numbness, mistrust, bitterness, confusion, avoidance, and/or difficulty moving on (Prigerson et al., 2009). In addition to distressing symptomology, PGD is associated with suicidality (Frumkin et al., 2021), increased substance use (Parisi et al., 2019), and reduced quality of life (Maccallum & Bryant, 2020). While many risk factors for PGD have been identified (Szuhany et al., 2021), high-quality, timely, and appropriate bereavement care is critical to identifying individuals who may be at risk of PGD (Aoun et al., 2020; Breen et al., 2017; Thomas et al., 2014) and is a key component of palliative care services (Breen et al., 2014).
Given the variable nature of bereavement experiences and subsequent support needs, three tiers of bereavement support have been proposed: universal intervention, comprising psychoeducation from healthcare professionals and social support from family and friends; targeted intervention, comprising non-specialist supports from volunteers, support groups, and community services; and indicated intervention, comprising specialist supports from mental health professionals and bereavement services (Aoun et al., 2012). Universal interventions provide information and compassion to all bereaved people, targeted interventions support individuals at risk of PGD via peer support or professional grief counseling, and indicated interventions target individuals who likely meet criteria for PGD and may benefit from specialized bereavement care and psychotherapy (Aoun et al., 2015; Rumbold & Aoun, 2015). Many psychotherapies for grief have been developed and tested as tertiary interventions, demonstrating positive effects (Johannsen et al., 2019); however, best-practices relevant to other tiers are less well-established.
Common to all tiers of intervention is telephone-based support (Guldin et al., 2015; Kobel et al., 2019; Mather et al., 2008). With telehealth services increasingly adopted due to the COVID-19 pandemic (Menichetti Delor et al., 2021; Moreno, 2020; Taylor et al., 2021), telephone-based bereavement support is likely to remain a central component of palliative care services. However, these services often lack systematic and formalized contact with clients, are inconsistent in the types and duration of care given, and rarely use validated screening tools as part of service allocation and delivery (Aoun, 2020; Guldin et al., 2015; Sealey and Breen et al., 2015; Sealey and O'Connor et al., 2015; Thompson et al., 2017). Although encouraged by practice standards (Hudson et al., 2018), there is minimal guidance as to what telephone support should comprise (Thompson et al., 2017), and little is known about what constitutes best practice. In absence of clear best-practice guidelines, there is potential for telephone-based bereavement supports to offer limited value to clients or even cause harm.
Despite the clear need for bereavement supports, and its status as a priority research area (Palliative Care Australia, 2018), services frequently fall short of practice guidelines (Aoun et al., 2017; Taylor et al., 2021). Standard procedures for telephone-based bereavement care would provide consistency in care; however, the format, content, and credibility of current practice is unknown. In the present study, we aimed to explore bereavement care providers’ perceptions of best practice in telephone bereavement support.
Method
Research Design
A qualitative research design was used and an interpretivist epistemology was adopted (Angen, 2000). Semi-structured interviews were conducted to explore participants’ experiences of providing telephone bereavement support and perceptions of what constitutes best practice. The Consolidated Criteria for Reporting Qualitative Research (COREQ; Tong et al., 2007) were used to support transparency in conducting and reporting this study. The COREQ is a checklist outlining 32 criteria that guide reporting of qualitative studies. We used this checklist to ensure our reporting was comprehensive and explicit across the three reporting domains of research team and reflexivity, study design, and analysis and findings. Trustworthiness was established using the guidelines for thematic analysis (Nowell et al., 2017), and included a detailed audit trail, documentation of researcher reactions, thoughts, and positioning, triangulation through cross-coding and team meetings, and reflexive journalling throughout.
Participants
Participants’ Roles, Pseudonyms, and Settings.
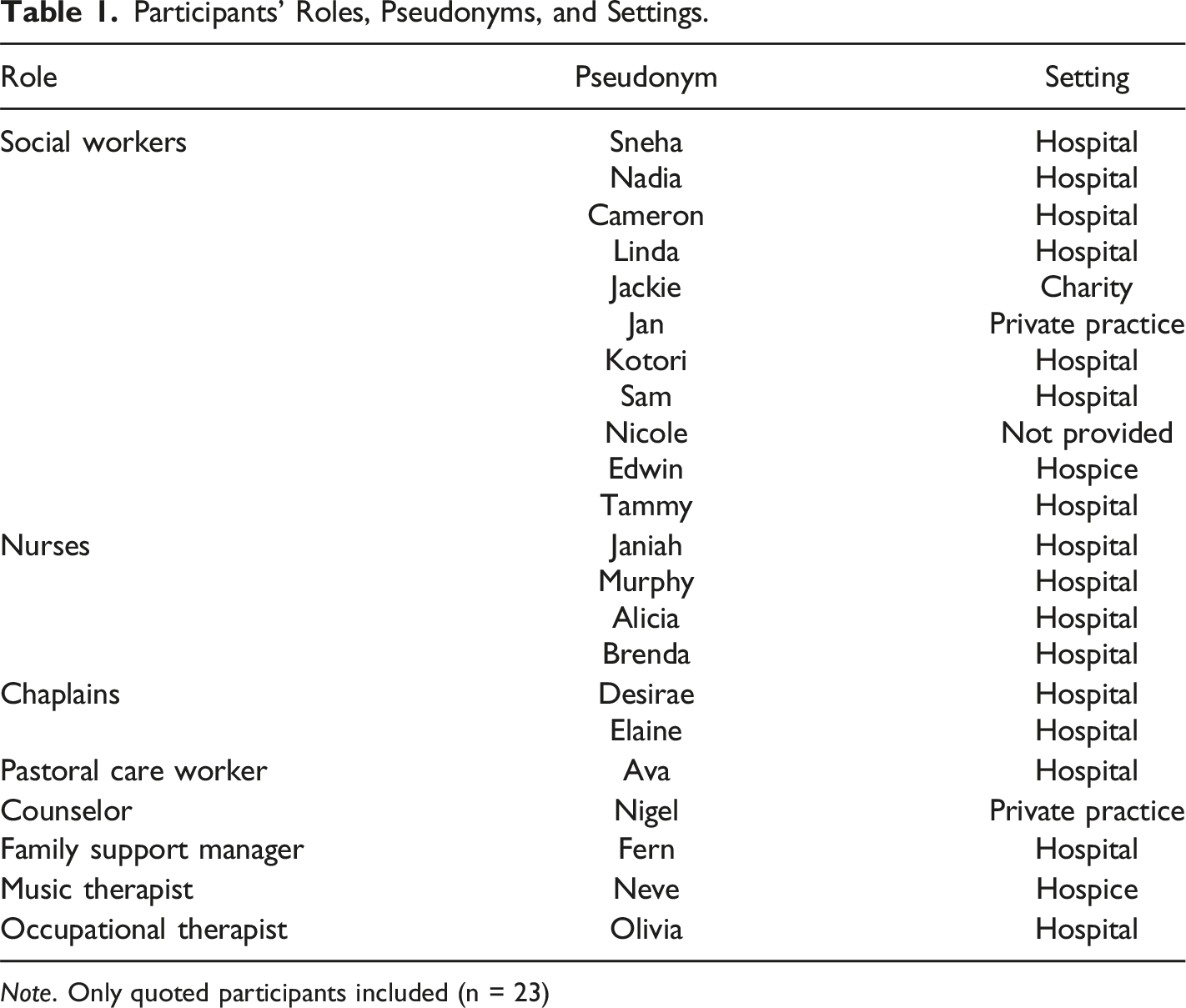
Note. Only quoted participants included (n = 23)
Materials
A semi-structured interview guide was developed by three authors. Informed by the literature, questions were designed to facilitate participants’ descriptions of their experiences as telephone bereavement providers. Questions related to their training, current practices, the benefits and challenges of providing telephone bereavement support, and what ideal bereavement support might include (e.g., “What kind of things do you listen out for during your conversation?” and “What challenges do you face with telephone bereavement calls?”). Prompts and follow-up questions were used to encourage elaboration (e.g., “What if they are not coping?” and “What about people who don’t engage?”). Prior to commencing the interview, sociodemographic data were collected, including participants’ current professional role and the context within which they provided bereavement support.
Procedure
Following approval from the University’s Human Research Ethics Committee (approval number: HRE2019-0586), recruitment commenced through social media (e.g., Facebook, LinkedIn). Interested participants contacted the study coordinator via email, who responded with the participant information and consent forms, which were completed and returned via email. Interviews lasted between 45 and 60 minutes and were conducted by a registered psychologist or social worker via telephone or face-to-face at the University, the participant’s workplace, or a café. In the workplace and university settings, interviews were conducted in a private room to ensure confidentiality. The interview conducted at a café took place at a quiet time and in an area removed from other patrons to ensure privacy and confidentiality. Signed written consent was obtained prior to commencing the interviews, which were audio-recorded, then transcribed verbatim by a professional transcription service. All participants were offered a $25 (AUD) shopping voucher for their time. The interview transcripts, audio-recordings, and participant details were stored digitally in password protected files, with each participant assigned a unique code to ensure confidentiality.
Data Analysis
Following checks of transcript accuracy, reflexive thematic analysis was conducted (Braun & Clarke, 2006, 2019). Following data familiarization, transcripts were analyzed line-by-line and codes were generated inductively. Codes with similar meaning were clustered to develop preliminary themes, which were reviewed and refined iteratively.
Findings
Seven themes were constructed during thematic analysis: A Valuable Service with Limited Resources; The First Call; The Dance of Rapport; A Space to Share; Identifying and Responding to Risk; Maintaining Contact; and Training and Development Needs (see Figure 1). Each theme is described in detail below and illustrated with data extracts. Pseudonyms are used to protect participant identities (see Table 1 for participants’ pseudonym, role, and work setting). Thematic map of best practice in telephone bereavement support.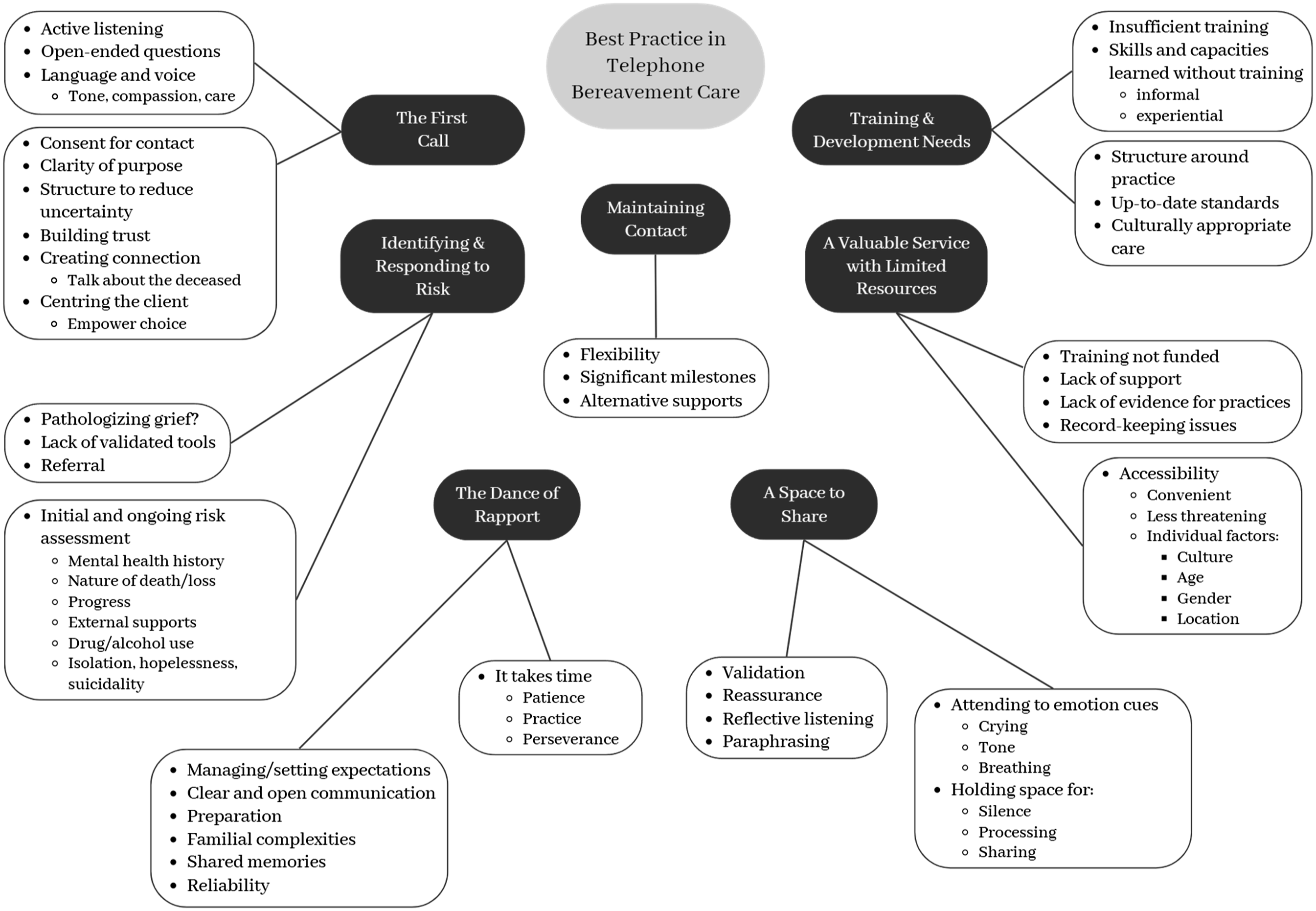
A Valuable Service with Limited Resources
Telephone bereavement support was consistently acknowledged as a valuable service. The distant nature of telephone support was described as potentially “less threatening” to clients. Jan explained that clients, “can keep us at arm’s length, they can control how deep we go, they can hang up whenever they want to.” In this way, the telephonic mode may offer clients more control over their participation, which could make it easier for individuals feeling unsure or anxious. The ability for clients to take calls on mobile also expanded the reach of bereavement services. Desirae explained, “mobile phones have meant that sometimes they can put me on speaker and so I can actually speak to the mum and dad at the same time.” Similarly, Jan noted that technology “like Skype and FaceTime” offered a face-to-face experience: “you’ve still got that access and convenience and so on, but you’re actually able to see them and they can see you… and engage as well.”
Participants described that the suitability of telephone bereavement support may differ depending on client characteristics. Sneha highlighted generational differences in telephone usage and its impact on suitability: We tend to engage really well with the parents of the young people who [are] in their 40s, 50s, 60s. They're happy to talk on the phone [but] talking on the phone can be really awkward for people in their 20s and under.
In addition to age, participants identified clients’ gender as relevant to how telephone bereavement support was provided and received. Janiah described that compared to men, “I find that women are much more able to be in the moment and sit with the silences.” Similarly, Sam reflected that “with males, sometimes I’ve read that they’re not interested... not really wanting to pursue the conversation, but then I’ve left it for a little bit longer and then the conversation’s actually gone on for an hour.”
Geographic location was another client characteristic that appeared relevant to the suitability of telephone bereavement support, with clients living in regional or rural areas reliant on remote services. Nadia explained, “I’ve got some families who are 8 hours drive away. So, I can’t go and see them all the time, but I either do telephone or tele-health kind of counseling with them.” With telephone support being so widely accessible, its inherent challenges appeared to outweigh its benefits. Indeed, Jan noted: “I’d say over 90% of my bereavements… would be by phone and that seems to be because it works well for the client.” Some cultural groups may find telephone bereavement support particularly helpful. As explained by Elaine, outward expressions of grief may not be culturally appropriate, and the telephone service allows an opportunity to share and grieve: I've had a lot of Hindu ladies who don't talk to their families or their friends because they feel they've got to put on a front for them... Can't get off the phone from them because… they can put that ‘mask’ down.
Despite some challenges in engaging clients, it was generally observed that the calls were well-received. For example, Jan described that clients often respond with, “Oh, thanks for phoning, oh thanks for thinking of me. Oh, that’s really nice that you touched base, I really appreciate that.”
Although participants believed in the value of telephone-based bereavement support, they expressed frustration with limited resourcing of the service. Desirae explained that while “a lot of bereavement services were rarely conducting routine follow-up phone calls [there was] a general lack of support for the process… on the grounds that is was resource intense.” Telephone bereavement services may be unsupported due to insufficient resources available to provide it and limited evidence underpinning it. For example, Desirae lamented that “there seemed to be a lack of evidence on the benefit of the calls.” This challenge was also reflected in participants’ difficulty accessing training to improve their skills. Eva shared, “I wanted to do one of those courses, but they weren’t going to fund it here, and I didn’t have the couple of thousand US dollars to do it,” demonstrating motivation for further training but lack of accessibility. Participants also identified procedural challenges to telephone bereavement support. Cameron described how record-keeping issues have implications for privacy legislation: This is a systemic problem… we're not meant to record in the medical record of a deceased person… The person who has died is the one who was the patient or the client and the family, in palliative care, is meant to be part of that system of care, and they are kind of the clients but then they're kind of not…
While palliative care is typically delivered within the family unit, privacy legislation presents a barrier to continuity of this care after death (Sealey, O'Connor, et al., 2015). Lack of clarity in how to classify clients receiving bereavement support complicates the provision and reporting of the service.
The First Call
Participants described several key elements of initial contact that were necessary for the development and maintenance of engagement, including clarity of purpose, centering the client, and creating a connection. Ensuring that the bereaved person has agreed to be contacted for bereavement support was emphasized, with Sam explaining her approach: I get a lot of family members saying, ‘Look, I'm worried about this person, will you give them a call?’ And my line of approach with that is ‘look, I would need their consent before making that call, so how about you give them my phone number and get them to call me when it's suitable for them?’
This way, the client is likely to be receptive to the service before being called. Other participants suggested a self-referral process to ensure that clients were actively willing to engage in the service. Desirae explained that this approach confirms “that people are making contact with us because they want some support. They want to be here. So, they make that first phone call and then we will arrange an appointment with them afterwards.”
When initiating contact with a client, participants identified that “the first contact is universal.” Nadia explained that this is “mostly because families are happy to be guided about what they need because they don’t know what they need (or don’t want) at that stage either.” During the first call, clients may be uncertain, and a structured approach could help to reduce that uncertainty. Participants described strategies to manage this uncertainty. For example, Cameron described that when faced with client hesitancy, they ask, “is there another day that’s better to call? Or would it be better if I contact you by email?” Offering alternatives gives the client choice in how and when they would prefer to be contacted. Similarly, Murphy described:
[clients] often say, ‘It doesn’t suit me’, and you can hear the emotion in their voice, and I’ll just quickly say, ‘Would you like to call another day? That’s perfectly okay’. But sometimes they’ll say, ‘No, I can’t cope with it’, so I let it go.
Giving the client power to consider and choose appears important to initiating bereavement support; however, client preferences were not always possible. For example, Jan shared, “Every so often when we’ve been heavily involved with a family they will say, ‘I want to see so-and-so’ for bereavement,” highlighting that while telephone bereavement counselors can do their best to center the client’s needs, this is not always possible.
Establishing the purpose of the call was identified as critical to initiating bereavement support. To ensure that the client was aware and available, Sam explained that they “prefer to text [the client] first and get an actual time and date to give them a call that’s appropriate and suitable for them.” Then, during the call, Sam suggested setting the scene by “saying where you’re from and making sure it’s a suitable time and my role and why I’m calling.” Participants also considered the timing of the calls, avoiding known busy times, such as school pick-up hours. Using these approaches, best practice means that the client is in the best position to receive the call and therefore more likely to engage with and benefit from the service.
In addition to being clear about the nature and purpose of the initial call, participants noted the importance of how they speak to clients, including the language they use and the tone and timbre of their voice. When reflecting on their approach to initial calls, Sam shared, “Empathy and compassion over the phone are huge, so is active listening. I think I build trust very quickly with people based on me being able to show that… we genuinely do care.” Likewise, Cameron shared that, “you kind of convey the empathy from your tone as well as the words.” The ability to convey empathy, compassion, and care appears central to establishing a connection with the client. While achieving this over the phone may be more challenging than in-person, active listening and tone of voice were highlighted as best practice skills. Jan suggested it is important to “listen to how they’re going, reflect, just inquire about the basics” to establish initial connection, and Adwin suggested that connection is made “by extending your sympathy and condolences in a way that’s using their language. Ask them open-ended questions.” Taken together, these quotations capture that listening, using suitable and appropriate language, and being mindful and deliberate with tone of voice are key best practice skills.
Managing discomfort was also discussed in the context of initiating telephone bereavement support. Participants highlighted the need to be open to talking about the deceased. Lidia shared, “you’re not avoiding saying the child’s name or that they’ve died. You’re being quite open,” and Kotori highlighted the benefits of sitting with silence: “I’ve learned to just hold the silence that the jewels come out within a conversation.” Other participants suggested focusing on other people as point of connection. For example, Lidia shared that she talks with clients about their other children “because we as parents are much more comfortable talking about our kids than ourselves.” Approaching the first call with openness and finding a relevant and appropriate point of connection appear critical for initiating bereavement support.
The Dance of Rapport
Rapport was prominently discussed by participants as central to best practice in telephone bereavement support, as noted by Nicole: “I don’t think anyone wants to talk to somebody who doesn’t sound like they know them.” However, rapport was not necessarily easy to develop and could be challenging regardless of the format of communication. Kotori described, “I think for any relationship, whether it’s face-to-face, or phone, or even email, it takes time to learn to do the dance together.” This was further captured in Nadia’s experience: “I think, oh great I’ve established a great rapport and then I ring the person a week later and… I feel like they don’t even remember us having had the conversation.” Developing and maintaining rapport is an ongoing process requiring patience, perseverance, and practice.
Participants identified good preparation as a facilitator to developing and maintaining rapport. As described by Nicole, “You can’t always remember people’s names, family members’ names and siblings’ names. So, I will make sure that I have them [client details]. I can build rapport again that way and talk to them that way.” Participants also highlighted the need to set aside sufficient time and a suitable location to make bereavement support calls. Janiah stated, “don’t try and do a quick conversation. Don’t think ‘I’m just going to fit this in, I’ve got 10 minutes.’ You are going to need at least half an hour, but you possibly might need even an hour.” Likewise, Linda shared, “if I’m doing a bereavement call, I’ll go into a focus room… it gives me quiet time and focus… I just think that bereavement calls are important, and they deserve your focused attention.” The time and space to focus allows for the client’s needs to be prioritized, fostering trust and rapport.
Unsurprisingly, participants described that building rapport over the phone was easier when there was a pre-existing relationship with the client. Participants described that they could use information learned during face-to-face interactions to inform subsequent telephone support. Adwin explained, “I’ve gotten to know them a bit, so I can match what’s in their voice with what I’ve experienced face-to-face.” This was also reflected in Maria’s experience of supporting a bereaved parent: “you’ll share memories about the child, and often they want to talk about some happy memories or the memories of the shared experience you’ve got of their child.” In this way, support was facilitated through a shared connection with the deceased. Even brief face-to-face contact provided foundational rapport. As noted by Jackie, “Often it’s not really extensive contact… it’s usually, they come in and we know this is not going to end well, so it’s a couple of days [of contact].” This suggests that even a once-off face-to-face interaction could strengthen subsequent telephone support; indeed, Jan shared, “I always start with a phone call, but I actually specifically request to visit first,” suggesting that the face-to-face visit is important to developing an ongoing supportive relationship.
Contrarily, extended contact with the bereaved client did not necessarily translate into service engagement, especially when there were familial complexities at play. For example, Sneha described “dealing with families that you know really well and you know that there’s complex family dynamics and you know that there’s stuff happening behind the scenes. However, they’re not willing to engage.” While extended contact may be expected to lead to subsequent engagement, this is not necessarily the case; however, the knowledge of background complexities gave insight into why the client was unwilling to engage.
Sometimes, developing rapport was difficult not just because of the telephone context, but because of expectations from the client about who would be providing bereavement support. This was captured in Sam’s experience: One person was very upset because he was expecting a phone call from another team that was heavily involved with his wife's care and he was angry that I had called and I wasn't the other team that had called, who he knew very well, and he was very upset that they hadn't called.
A Space to Share
When describing the kind of support offered in telephone bereavement care, participants identified that they offer clients a space to share experiences and emotions, and within that space, provide reassurance and validation. While participants identified that the absence of non-verbal cues (e.g., eye contact, nodding) sometimes made it difficult to read clients’ emotions, they also discussed strategies for dealing with this. Sneha described, “[it is] hard with telephone… you can’t see the reaction from other people… I’ve had silent spaces of a couple of minutes on the phone where I’m like, have they hung up on me?” But these spaces were described by others as important for honing-in on other cues of emotions. Fern described that even though she cannot see the client, “you can still feel or perceive emotion over a phone line… you can still just hear breathing and tone of voice and stuff… when things are shifting or processing,” and Sam stated that “you quite often can hear someone crying and that’s obvious but sometimes people cover the phone and there is that blank, that silence.” By holding space for silence, bereavement counselors could notice their client’s emotion and respond with empathy and kindness. Part of this response included reflecting back. Sam described her practice involves “little verbal cues of going mm, ah, yeah, and reflective listening I suppose or paraphrasing what they’re saying so that they understand that I’m listening… clearly hearing what they’re saying,” and Cameron explained that “people respond to that and then they regroup a little bit, and they’re able to resume the conversation.”
Offering reassurance and validation was commonly described as the approach when clients voiced worries or concerns. Cameron shared that “[Some clients will say] ‘I can forget about it for an hour and then, 2 hours later, I’m in floods of tears. Is that normal? And so, we’re able to reassure people: ‘Yeah. I know it’s really hard, but it is really normal’.” Similarly, Sam suggested normalizing grief by “giving them some education around the value of continuing bonds, to know it’s okay to still be talking to your loved one’s photo,” and Maria described her efforts to “allay that fear that their child has not made a difference or not mattered, or not been remembered.” While responding to worries and concerns was common, Jan highlighted that bereavement counselors, “don’t have to know the answers to the problems, they don’t have to fix any of them”, suggesting that the primary goal of telephone bereavement care is to offer a space for sharing and processing. This was highlighted further by Nadia, who shared that they say, “I’m hearing that you’re feeling quite overwhelmed at the moment, and whilst that’s really natural, that must be really hard and horrible to be feeling this way.” In this way, best practice involves validation of the client’s thoughts and feelings.
Identifying and Responding to Risk
Participants discussed the importance of assessing clients’ wellbeing and identifying suicide risk as part of telephone bereavement support. Doing this happened at various stages of the service. Sometimes risk was identified prior to the first call. For example, Nadia described that “On some occasions I’ve actually been asked to ring literally the next day by health staff who feel like that family member is at risk of suicide or significant mental health concerns.” Responses demonstrate that best practice involves timely support and that those providing bereavement care must be equipped with the skills, resources, and professional support needed to offer this care. In less obvious cases, participants identified the need to listen out for and follow-up on the risk factors. For Sam, this involved identifying “if someone’s either isolated through family and friends, or physically isolated, or geographically isolated. As to whether they disclose any drug or alcohol consumption, previous mental health difficulties and also the nature of the death.” This is because these factors may indicate that a client is at risk of developing mental health difficulties and therefore, knowledge of them highlights a need for more support.
Assessing clients’ mental health was an ongoing component of providing telephone bereavement care. Neve described that they evaluate how a client is progressing by considering, “are they able to shift in their thinking about their child? Are they actually able to have any thoughts about the future or are they stuck in the day-to-day?” Similarly, Olivia shared that “[I’ll] look at things like how are they sleeping? Do they have external supports in the community? Are they eating? How [are] the kids coping? Have they asked any questions? Have they noticed any changes with their behavior?” When risk was identified, participants described how they inquire further to better understand the nature of the risk. For example, Nadia shared that if a client discloses suicidality, they explore this by asking, “Do you actually have a plan? Do you have an intention? Are you really struggling with those overwhelming thoughts that just say let’s just end this now?” These kinds of questions may assist bereavement counselors to better understand their clients’ wellbeing and identify whether they may need referral to more specialized care.
The risk of developing ongoing mental health difficulties was also considered by participants. Linda described concern about a client who was “constantly by the grave side talking to him, saying that he is speaking to her and giving her messages,” which she identified as evidence of “ongoing mental health issues.” Given the role of bereavement counselors to provide mental health support, skills to accurately assess and identify risk are needed. However, as noted by Desirae, “there really aren’t any validated assessment tools to assess those who might be at risk”, which presented a barrier to identifying clients who needed further support and the potential for judgments to be made based on misguided opinion or belief rather than evidence.
While participants identified the importance of monitoring clients’ mental health, they also expressed concern with pathologizing grief. Sam shared, “I think the system fails people when they’re telling people… there’s a mental health concern when what they’re grieving is actually normal but it’s so far into them and it’s so extreme, like any grief response is.” She further shared that while she explains to clients the process of accessing a Mental Health Care Plan though their general practitioner, she clarifies with the client, “just please know that’s nothing to do with you having mental illness or anything along those lines, it’s just purely so you can get a Medicare rebate.” Thus, Sam appeared concerned that the financial assistance support for bereavement care being attached to Mental Health Care Plans by definition, positions grief as a mental disorder rather than a normal response to loss.
Maintaining Contact
When discussing the frequency of their contact with clients, participants identified that flexibility was needed to ensure they were meeting the client’s needs. For example, Brenda shared: “I struggle with the formal call at one month, call at three months, call at six months, call at 12 months... I don’t think that works for every family… [they] are so individual.” To manage the diversity in need, Brenda explained that her approach is “on a case-by-case basis” and that when deciding how frequently to make contact, “I judge it on the responses I’m getting from the family and their level of engagement or how they respond to getting that call. Nothing’s set in stone.” Here, Brenda considers the dynamic nature of grief in the family context and how she can take a flexible approach to offering support that acknowledges changing needs. Similarly, Janiah explained that she contacts clients at times known to be challenging: I'll be in contact at typically known, difficult time points; so, that could be beginning of the school year when their child's name is not on a class list. Depending on their religion, whatever religious festivals, but I'm going to go with more Christian ones, which is Easter, Christmas, their birthday, date of anniversary or any other significant milestone for them.
Maintaining contact with clients was not always straightforward, with some participants describing difficulty moving clients on to other supports. Maria shared, “I have a mother who just rings me fairly constantly and we try and do the best we can to provide that support while also trying to link [her] in with community support.” Maria explained that this was because the alternative supports “didn’t know their child, and they want the support from somebody who knew their child.” While this example speaks to the power of the connection between a bereavement counselor and their client, it also highlights the need to have clearly established protocols for counselors and identified pathways through the support system for clients.
Training and Development Needs
Participants acknowledged that telephone bereavement services require a specialist skillset but noted that there was limited guidance and training available to them. Nadia explained that “Telephone has its barriers. And it does require a completely difference skillset. And tele-health – another skillset altogether.” Participants wanted to advance their knowledge, but faced barriers to access; for example, Ava described, “I wanted to do one of those courses, but they weren’t going to fund it here, and I didn’t have the couple of thousand US dollars to do it.” The desire for more guidance and training was highlighted by Nicole, who stated, “It’d be nice to have some guidelines and some standards… it’s nice to have the structure around practice.” For participants who had access to guidelines, there was concern with their recency, with Olivia describing that, “we’ve got lots of palliative care standards and bereavement standards that we can go through… [but] some of them aren’t necessarily up-to-date.” In addition to more contemporary standards, Janiah identified the need for “more information on culturally appropriate bereavement follow-up for all different nationalities, religions… Because everyone’s individual and different, and no one can be lumped in as the same just because you’re associated with one group.” Having a better understanding of cultural and religious needs may provide bereavement counselors with more confidence to offer support to a more diverse range of individuals.
Most participants relied on informal and experiential learning to improve their skills. Kotori shared that “You learn a lot by listening to other colleagues,” and Brenda described the role of experience and feedback: “you learn from previous mistakes or previous experiences, and feedback from families… they let you know what was important or valuable to them, then you kind of carry that forward.” Participants felt their qualifications had not prepared them to provide bereavement care. Jackie shared that during her training as a social worker, “there wasn’t anything, like, mandatory in terms of grief bereavement follow up,” and that while “you’re kind of expected to follow through this manual and the policy… you’re not really sure how you’re going to go.” This quotation captures the uncertainty that telephone bereavement counselors may experience in providing a service they have not been adequately trained for. Likewise, Alicia reflected that, “I think I do an okay job, but I have had no training.” She explained further: You could be doing it really well and have that empathy and what you've learnt from your reading and experience, but I think there does need to be a level of formal training. We've all been to courses on open-ended questions and communication style and role-play activities and things, but I don't think that it's formal education.
This sentiment was echoed by Kotori, who, after acknowledging that not everyone has the capacity to provide effective telephone bereavement support, suggested “going through an assessment process and a training program so that we have insight into those people that had capacity.” Formalized training and assessment may strengthen confidence in the skillsets of counselors providing telephone bereavement support. This may also provide an opportunity for prospective bereavement counselors to better understand the nature of the role. As Olivia noted, “looking at the vicarious trauma that we go through, I think providing education about that is really important, so there’s no burnout.” Formalized training may offer an opportunity to clarify not just an individual’s skillset to perform the counseling role, but also their psychosocial capacity to do so effectively perform the role.
Discussion
The importance of meaningful follow-up support after bereavement has been established (Lichtenthal, Sweeney, et al., 2015); however, a significant gap remains in our understanding of what this follow-up support should comprise and how it should be delivered. In the current study, we explored how providers conceptualize best practice in telephone bereavement support as a key step in developing an evidence-base for the development of practice guidelines. Through thematic analysis of 26 interviews, seven themes were identified to capture participants’ perceptions of telephone bereavement services and associated challenges, their recommendations for best practice, and the resources required to provide effective support.
Overall, participants agreed that telephone bereavement support is a valuable and accessible service that is acceptable to clients with varying backgrounds and needs. The service was conceptualized as a space for bereaved individuals to share, process, and be validated in their experiences, thoughts, and emotions related to their bereavement. While the lack of face-to-face contact was not without challenges, participants recognized that the telephonic format could be less confronting for individuals not familiar or comfortable with traditional in-person counseling. Furthermore, this format enabled clients access to support without the need for travel or Internet access, which is particularly important for individuals living in regional or remote areas who would otherwise require long commutes to access bereavement services face-to-face.
Components of Best Practice
Best practice was captured in how telephone bereavement counselors prepare for and deliver their support sessions. Strategies for effective preparation included allocating sufficient time, securing a quite space free of interruptions, and (re)familiarizing oneself with client details. Strategies for effective delivery included clarifying purpose, centering the client, creating connection, using open-ended questions, matching language, listening for subtle cues (e.g., change in breathing), reflecting, verbalizing listening cues (e.g., saying “mmhmm” instead of nodding), holding space for silence and discomfort, and avoiding problem-solving mode. These strategies map onto findings from research on the key benefits of post-bereavement follow-up, which include the opportunity to ask questions, process loss, and remember the deceased, to feel reassured and validated, and to work on meaning-making (Diamond et al., 2012).
Participants also discussed the importance of ongoing assessment of clients’ wellbeing to determine their safety and level of need. However, in absence of standardized risk assessment tools readily amenable for telephone administration, providers relied on prior knowledge of risk factors (e.g., social isolation, difficulties sleeping and/or eating) and verbal clues (e.g., language such as “I can’t do this anymore”) to evaluate client wellbeing. Similarly, when responding to increased risk, providers drew on prior experiences or advice from colleagues to inform their responses. To ensure that best practice in telephone bereavement care is possible, providers need access to and training in comprehensive but short and easily administered assessment tools (Hudson et al., 2018). Lack of screening and assessment is commonly identified as a gap in bereavement care (Keegan et al., 2021; Wiener et al., 2018), and while there are many measures of grief available (Sealey and Breen et al., 2015), most are unsuitable for the telephone bereavement support context due to length and purpose.
While general patterns in best practice were identified, participants also highlighted that each client has individual needs and that a flexible, responsive, and client-centered approach was required to offer high quality telephone bereavement care. Participants provided insight into the needs of particular client groups. For example, difficulty reaching young people via telephone suggests that text-based support services may be more suitable to them. Indeed, a recent review by Breen et al. (2023) found that young people wanted more accessible online and app-based grief supports. Similarly, participants reflected that men may require more time and space to ease into the bereavement support call compared to women. This may be explained by grieving styles and gender expectations, whereby women are more likely to express grief emotionally, while men are more likely to express grief cognitively and behaviorally (Doka & Martin, 2010). Understanding the continuum of grieving styles and how they may present in bereavement support may be useful information to include in training and aligns with work on grieving styles showing that people may express grief differently and that bereavement services need to be diverse in their approach and accessibility.
Research with bereaved individuals about their experiences of bereavement support consistently highlights the need for individualized and culturally safe care (Egerod et al., 2019). Best practice in bereavement support requires a balance between tailoring one’s approach and adhering to procedures of care (Wiener et al., 2018). Further, participants spoke of supporting families, yet most had one point of contact in the family, who was almost always a woman. Assuming that one person can be the proxy for all members of the family is problematic and aligns with calls to bring the family-level focus into grief and bereavement care (Breen et al., 2019).
Requirements for Best Practice
In terms of what is required to offer best practice care, participants concurred that bereavement services are inadequately resourced and providers are typically insufficiently trained. Insufficient resource allocation may impact not only the frequency of support calls being made but also the quality of support provided by bereavement counselors, who wish to improve their skills but are not adequately funded to do so. This is highly concerning given the vulnerability of both provider and client. Bereavement counseling is an emotionally demanding job; lack of training and support contributes to provider burnout and distress, negatively impacting their health and wellbeing (Yang & Hayes, 2020). High levels of stress and low levels of self-efficacy impair providers’ ability to deliver high-quality bereavement care (Lin & Fan, 2020), negatively affecting clients’ psychosocial outcomes (Yang & Hayes, 2020). Clients accessing bereavement services are often at risk of PGD, anxiety and mood disorders, and suicidality (Aoun et al., 2015); therefore, it is crucial that providers of bereavement counseling are comprehensively trained and supported to ensure high-quality care that protects both provider and client.
To feel adequately prepared and supported, participants identified a need for specialized training on risk assessment, and updated, evidence-based guidelines specific to telephone bereavement support. These suggestions align with those presented by Lichtenthal et al. (2021), who call for implementation trials to inform best practice standards, greater resource allocation, and evidence-based training programs for bereavement care providers. Without appropriate training and ongoing supervisory support, bereavement counselors are likely to be ill-equipped to provide what should be acknowledged as a critical service.
Limited resourcing and support of bereavement care illustrates its position in healthcare services, which is reflected in results from an Australian survey of 506 bereaved relatives, who described the support they received as “generic”, with long follow-up times and inconsistent services (Aoun et al., 2017). In the present study, limited integration of bereavement support into healthcare was flagged by participants as a barrier to effective care. Participants described challenges associated with ‘cold-calling’ clients (being a stranger to the client at first contact), which impeded service engagement and rapport-building, particularly when the client was expecting to hear from a member of the healthcare team. This finding is reflected in research showing the importance of post-bereavement follow-up from a member of the medical team known to the family (Jensen et al., 2017). It also points to the need for greater integration of bereavement supports into healthcare, and greater communication between medical teams and clients about bereavement supports (Laranjeira et al., 2022) so that bereavement care is no longer the “poor cousin” (Aoun, 2020) in palliative care.
Strengths and Limitations
Through interviews with 26 bereavement support providers spanning social work, nursing, and various counseling professionals, we captured a range of perspectives and experiences to inform our understanding of best practice in telephone bereavement services. However, the sample comprised mostly female social workers practicing in acute, intensive, and palliative care settings in Australia. The heterogeneity of our sample limits the transferability of our findings to other bereavement support contexts and providers. Additional elements of best practice may be captured through interviews with providers with differing backgrounds working in differing contexts. While we were able to gain multiple provider perspectives, our findings do not capture perceptions of best practice among clients of telephone bereavement services. As such, there may be additional facets of best practice missed. Indeed, research suggests that not all people find bereavement services to be helpful (Lichtenthal, Corner, et al., 2015) and there is a need to better understand the needs of individuals receiving this support.
Implications and Future Directions
Our findings have important implications for telephone bereavement supports, pointing to key aspects of best practice that can inform the development of endorsed guidelines. In line with the findings of Keegan and colleagues’ (2021) Delphi study, key aspects of best practice related to training and evaluation, screening and risk assessment, and integration of bereavement supports into wider healthcare services. Underlying this is the need for appropriate resources to fund the development, implementation, and evaluation of bereavement supports.
Guidelines and training are needed along with validated tools to support ongoing assessment of client wellbeing and suicide risk. Participants identified experience and observation as their primary methods of learning – both of which are readily implemented in training courses through role-play and video resources. Competencies assessments could also be embedded within such training to ensure that bereavement support providers are sufficiently skilled to provide quality care. Likewise, evaluation of bereavement support interventions is required, which necessitates efficient, relevant, valid, and reliable measures of client outcomes. Recent research suggests that coping and wellbeing are the key outcomes that need to be captured in such measurements (Harrop et al., 2020). This is especially necessary given the recent findings from Ainscough et al. (2022) systematic review of bereavement support interventions. They found that of the nine eligible studies, only three reported improvements in any of the 23 measured outcomes. A manualized intervention package could be a potential solution to the highly variable nature of current bereavement supports; however, it will be necessary to incorporate culturally safe practices and flexibility in delivery to ensure individual needs can be met. The development, testing, and implementation of such an intervention should be co-produced with consumers.
Further research is needed into the impacts on providers of delivering telephone bereavement support. As participants identified, providing bereavement support is challenging and at times confronting, requiring skill and expertise to effectively support bereaved individuals and maintain self-care. In addition to developing and evaluating quality bereavement support for the benefit of clients, the support needs of bereavement support providers must be identified and met.
Conclusion
The findings of the present study contribute an important perspective to the ongoing discussion of best practice standards in telephone bereavement care. Participants highlighted their desire for specialized training and updated, evidence-based procedures that guide the delivery of bereavement services. The need for better resourcing was also highlighted as key to the development, implementation, and evaluation of services. Our findings are congruent with other research exploring best practice in bereavement care, suggesting that practice guidelines and training packages are acceptable and applicable. Centering clients’ needs is essential and care consistency is needed to ensure that individuals who may benefit from bereavement support are able to access high-quality, evidence-based care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.