
Abstract
In this multimethod study, we examine bereaved parents’ capacity for mentalizing the temporal dimension of their grief. The theoretical assumptions of our study draw on the clinical and anthropological perspectives on the passage of time in grief. Parents’ mentalization of their experience of grief was measured both in the attachment context, using the Adult Attachment Interview (AAI) and using the narrative Child Loss Interview (CLI). We used thematic analysis to code parents’ mentalizing utterances in order to categorize time-related changes during the grieving process. Parents generally mentalize their grief-related experiences at a lower level of reflective functioning than their general attachment experiences. However, a higher general ability to mentalize contributes to a higher level of RF and greater coherence in mentalizing their grief. Parents experience time in grief through oscillation between the past with the deceased child and a restricted form of existence in the present reality.
In this paper, we describe parental mentalization of grief and the experience of time in grieving parents. We consider time as an implicit dimension of clinical and psychological theories of grieving and contrast it with the anthropological non-linear perspective of time. We treat mentalizing capacity in parents as a source of insight into their internal experience of time and related changes in the grieving process. We refer to the experience of time as this dimension is particularly pronounced in descriptions of parents as a population of grievers. Their grief-related distress symptoms are reported to persist longer than in other grievers, sometimes even remaining throughout the parent’s life (e.g. Gennep et al., 2019; Klass, 2006; Lichtenthal et al., 2010; Malkinson & Bar-Tur, 2005; Pohlkamp et al., 2019; Rando, 1993).
In his classic conceptualization of complicated grief, Parkes (1965) identified three types of complicated grief reactions: chronic grief, inhibited grief and delayed grief. This conceptualization implicitly indicates how the temporal dimension is involved in grief complications, particularly when intensive grief becomes prolonged or grief reactions are seen as postponed. Likewise, in contemporary psychiatric classifications, grief is considered to be a phenomenon that is expected to evolve and change; the definition of prolonged grief disorder (APA, 2020) indicates that if symptomatic grief reactions are intense and long-lasting, it becomes problematic for the mental health or well-being of the griever. In many cultures, the length of the mourning period is precisely codified, which means that there are expectations as to the duration of grief and expressions of mourning as well as to the sequentiality of the successive stages (Gennep et al., 2019; Rosenblatt, 2013).
Time in grief is often seen as linear, comprising consecutive stages, which in the Kubler-Ross model (1969) includes final grief resolution; the last stage of grief is described as acceptance. Linear models have been criticized for not corresponding to current research knowledge or to clinical experience and imposing unjustified expectations on grievers (Stroebe, Shut, Boerner, 2017). In models of grief inspired by attachment theory, undergoing the successive stages of grieving emphasizes transformation rather than closure (Bowlby, 1969, 1980; Rando, 1993). Attachment models of grieving are based on the premise of a dissonance between the external reality – the physical absence of an attachment figure – and an internal reality in which the deceased is longed for, called upon and sensed as present (Bowlby, 1980; Shear et al., 2008). This very fundamental dissonance between the griever’s internal and external realities may be understood as an alternation between the past and the present. The alternation between past and present in grief is also implicitly involved in the dual process model conceptualized by Stroebe and Schut (1999, 2010), in which orientation to loss is seen as orientation to the past as the griever. A more present- and future-focused process is restoration of well-being and social reintegration.
Drawing on this idea of shifting between past and present in the process of grief resolution, we look at the concept of time in grief through the lens of anthropological theory that also involves non-linear conceptualizations of time. In these, time is seen as a ‘pendulum’ or ‘alternation’ rather than a linearity (Leach, 1961). Anthropologists claim that in many societies ‘time is experienced as something discontinuous, a repetition of repeated reversal, a sequence of oscillations between bipolar opposites: night and day, winter and summer, drought and flood, age and youth, life and death (Leach, 1961, p. 126). Significantly, Leach (1961) underlines that this oscillation between opposites implies the existence of a subject of these oscillations, a person who is shifting between these two states. In line with this, Gell (2020) defines the duration of time from the perspective of the subject that experiences it; in his view the passage of time is a process situated within the individual self (Gell, 2020, Kindle Locations 3321-3324). In accordance with this, following the exhortation of Stroebe et al. (2017, pp. 467–468) that the next step for researchers to take [is] to reflecting the experience of bereaved persons, their thoughts and feelings (Stroebe et al., 2017), our work focuses on the subjective experience of time in the group of grieving parents.
As much as 33% of parents are reported to suffer from a prolonged grief disorder for up to 5 years post-loss (Pohlkamp et al., 2019). These symptoms may be contingent upon difficulties in finding meaning in their loss (Lichtenthal et al., 2010). Grieving parents also remain attached to the deceased child by re-invoking the past with them, for example, preserving the child’s personal possessions (Reeves, 2011; Cacciatore & Flint, 2012). ‘Holding on’ to memories is seen as positioning them between wanting to ‘move on’ with life and the desire to ‘hold on’ to the memories of their child (Dias et al., 2017). This oscillation between ‘holding on’ and ‘moving on’ with life highlights their way of being suspended between the past and the future.
The above conceptualizations indicate the omnipresence of the implicit temporal dimension in theories of grief. In this paper, we are interested in the extent to which parents are able to gain access to their mind when describing changes related to time in their experience of grieving. Therefore, in designing our research, we drew on parents’ ability to mentalize their experience of time during the grieving process. The notion of mentalization originates from attachment theory (Bowlby, 1969, 1980). Securely attached parents use their mentalizing capacity while interacting with their infants by mirroring and ‘reading’ their emotional state. This type of responsiveness and emotional support develops children’s capability to mentalize their own mental states (Fonagy et al., 2002). Mentalization is generally defined as the ability to make sense of one’s experience in terms of intentional mental states (Fonagy et al., 2002). Effective mentalization helps the individual to experience emotionally charged situations without becoming overwhelmed by their emotions or shutting them down (Slade, 2005). This capacity might be crucial while grieving. Being able to mentalize one’s grief-related separation distress (being overwhelmed by intense yearning and longing) (O’Connor, 2013) might contribute to better emotional regulation of this distress. Mentalization in grieving is largely uncharted territory, and there are many unanswered questions regarding the way in which mentalizing capacity operates in grievers in relation to their experience. The study of Janusz et al. (2020) showed that reevoking the memory of traumatic loss in a couple therapy session may hinder mentalization capacity in parents in the course of the first year after the loss of a child.
Grievers are reported to suffer both general and attachment-related stress response (O’Connor, 2013; Luyten & Fonagy, 2015). Therefore, in the acute phase of grief, they may not be able to reflect on their grief-related thoughts and emotions, particularly when their general level of mentalization is compromised. Moreover, it would be reasonable to expect that grievers who can mentalize effectively are able to give meaning to their attachment-related stress, since more adequate self-reports or perceptions of attachment relationships are seen as conditioned by mentalizing (Fonagy et al., 1998).
The research into narration shows that mentalization contributes to a coherent self-image and a cohesive autobiographical story (Köber et al., 2015), which may be a particularly important resource in the emotionally laden verbal talk related to the death of a loved one. Grief researchers claim that adaptation to loss involves transforming the physical attachment to the deceased child (Klass, 2006) and restoring coherence to the autobiographical narrative (Neimeyer, 1998). As effective mentalizing is seen as encompassing the processes involved in interpreting one’s own mind (Fonagy, et al., 2002), we consider high mentalizing capacity in a griever to be a resource that can offer insight into the temporal aspects of the attachment relationship with the deceased child. We also consider that good mentalization may be a resource that can be used to establish a more internalized than externalized bond to the deceased (Klass, 2006).
Neimeyer et al. (2014) draw attention to the duality of the temporal dimension of narrations related to the experience of grief: the link to the past with the deceased person, and the present impacted by their loss. Both dimensions are crucial to the autobiographical narration, highlighting in particular the personality development of the narrator to the present (see Köber et al., 2018) and invoking attachment representations of their life narratives (cf. Köber et al., 2019). It seems that grief temporarily renders the relationship with the deceased attachment figure central to the life of the griever, as it engenders fundamental transformations in their life. Köber et al. (2015) emphasize that life narratives require interpretive connections between various events that explain how those events reveal new aspects of the self. This kind of autobiographical capacity seems to require effective mentalizing, which may be employed when reasoning about the course of one’s life, shifting between one’s past and present, including the impact of traumatic events on it. The findings of Köber et al. (2019) show that people spontaneously use RF while telling stories other than attachment interviews. An individual’s ability to mentalize is thus seen as a factor that contributes to a better understanding of their past life, by making their own mental states appear more meaningful, facilitating a coherent interweaving of past events and the former self with the current self (Köber et al., 2019).
In order to understand the impact of grief on parents’ mentalization of their child’s death, we investigate parents’ general levels of mentalization using the Adult Attachment Interview and the narrative Child Loss Interview so as to describe their capacity to mentalize their attachment to the deceased child. Therefore, in the quantitative part of our research we focus on the question of whether a parent’s general mentalization level may be compromised when the topic of child’s death and their grief is evoked in the talk. We hypothesize that grieving-related stress compromises mentalizing. In the second, qualitative part of the research we rely on mentalizing capacity as a resource offering insight into temporal aspects of parents’ attachment to the deceased child. Our second research aim is to describe grieving parents’ subjective experiences related to the passage of time after the loss of the child.
Study Methodology
Participants
Participants Characteristics.

Note. Survey date refers to time between children’s death and conducting survey.
Study Design
Adult Attachment Interview – Reflective Functioning Scale
The Adult Attachment Interview (AAI; George et al., 1996) and Reflective Functioning Scale (Fonagy et al., 1998) serve to measure mentalization. The AAI is a semi-structured interview that focuses on childhood attachment experiences (George et al., 1996). The Reflective Functioning Scale (RFS; Fonagy et al., 1998) was applied to the AAI to evaluate parents’ RF. The RF coding is based on four main criteria: A. Awareness of the nature of mental states, B. explicit effort to tease out mental states underlying behaviour, C. recognition of developmental aspects of mental states and D. mental states in relation to the interviewer that indicate an interviewee’s good mentalizing capacity.
After the AAI was rated, the interview was assigned an overall rating, which generally ranges from −1 to 9 (Fonagy et al., 1998). The lower ratings indicate, respectively: −1 (negative), 2 (unintegrated and lacking) and 3 (questionable or low) reflective functioning. The higher ratings indicate, respectively: 5 (ordinary), 7 (marked) and 9 (exceptional) reflective functioning. In the interviews rated 5, speakers have a model of the mind of their attachment figures as well as of their own mind that is relatively coherent. The results from the two interviews (see CLI below) were divided into two groups: 1–3 (low mentalizing group) and 4–8 (stronger mentalizing group).
Child Loss Interview – Reflective Functioning Scale
As parents’ capacity to mentalize the loss of a child is a central phenomenon in the present study, we wanted to explore it in more detail than is possible by relying solely on AAI. Several investigators have used RF assessment to investigate autobiographical accounts (e.g. Köber et al., 2019). Following this line of research, for the purposes of this study we constructed the Child Loss Interview (CLI). The CLI is a narrative interview comprising three open-ended questions, which were asked in the following order: (1) Could you tell us about your behaviour/feelings/experiences after your child’s death? (2) Could you tell us about the changes in your behaviour/feelings/experiences from the moment of your child’s death till now? (3) Are you able to identify any changes related to time in your way of experiencing the loss of your child? These open-ended questions were asked in order to stimulate the parent’s narration regarding the child and its death. During the interview, the researchers mostly used typical continuers like ‘Mhm’ and asked questions to clarify parents’ earlier utterances or develop issues that they had only touched on.
Thematic Analysis
In their recent papers, Braun and Clarke (2020) defined their method as reflexive thematic analysis (TA), emphasizing the importance of both the researcher’s subjectivity as an analytic resource and their reflexive engagement with theory, data and interpretation. The main deliverable of the analysis is considered to be the themes that it reveals, and these capture meanings or central ideas in the talk (Braun & Clarke, 2006). The themes generated as a result of the researcher’s active involvement in interpretation of the data, and his/her reflexivity, give an overview of the subject under scrutiny.
Thematic analysis was used to identify themes in the AAI interviews (loss-related section) and CLI interviews. We coded only parents’ mentalizing utterances because we presupposed that parents manifest their insight into their grieving-related mental processes in these utterances, particularly their experience of time. In coding the mentalizing utterances, we took into consideration the context of the entire interviews. In the next step, we generated sub-themes from previously coded transcripts and then analytically constructed the central themes that are the main results of the analysis. Our analysis was deductive in the sense that we were interested in how effective mentalizing may make it possible to recognize and express the grieving-related experience. The thematic analysis described in this paper was informed by assumptions rooted in the conceptualization of grieving as employed in the attachment approach as well as by a mentalization research framework.
Statistical Analysis
All the analyses were performed using the R statistical environment (2018). The inter-rater consistency of the CLI scores as measured by an inter-class correlation coefficient of 9 ratings provided by two assessors was moderate (ICC(1) = .64). In the case of the AAI scores, 8 ratings were provided by two assessors, and the inter-class coefficient indicated good consistency (ICC(1) = .80). Association between the AAI and the CLI was measured using the Pearson correlation and the Student’s t-test.
Procedure
Participants were recruited by the first and second authors in cooperation with the staff of two children’s hospices. In the first step of the research procedure, the hospice staff members asked parents of deceased children whether they would be willing to take part in the study. Directly thereafter, the first author contacted those who were initially open to participation in order to discuss the research procedure and their potential participation. The interviews were conducted in the parents’ homes by two researchers together. Both interviews were conducted during the same visit. The narrative CLI was less structured and was introduced after informal warm-up talk with both parents. The researchers always granted the parents’ wishes regarding participation together or separately in this first part of the research, but both parents were asked to answer the questions separately. The AAI interviews were administered separately to each participant by one of two researchers (the first or the second author of the paper).
Ethics
Informed and written consent was obtained from each participant. The participating parents gave their written informed consent to the use of the data for research purposes. The names and personal details in all presented examples have been changed to maintain confidentiality. The study was approved by the Bioethics Committee of Collegium Medicum at XXXXX University (KBET/149/B/2013 of June 6, 2013). Both the researchers who conducted the interviews are family therapists with experience in therapy for grieving families. After the interview, parents were offered family counselling for grief, which would take place directly after the interview or later.
Data Analysis
Both interviews (AAI and CLI) were transcribed and rated in terms of the parents’ RF. The first author of the paper rated all the interviews, and the third author rated 30% of the AAI and 30% of the CLI to ensure the reliability of the rating. We applied RFS to the narratives obtained through CLI, assigning RF ratings from −1 to 9 according to the general guidelines in the main RF manual (Fonagy et al., 1998). We assigned an overall RF rating for each interview, which allowed us to assess RF on loss and grieving experience for each parent (1–4: none–low mentalizing group and 5–9: stronger mentalizing group). Finally, we isolated segments of talk rated 5 and above and coded them according to the rules of Thematic Analysis. While coding them, we took into account the local conversational context in which these utterances emerged. In the last step, all utterances that were rated 4 or above in terms of reflective functioning were coded according to the thematic analysis procedure using Nvivo 11 software. The first author of the paper did most of the initial coding of the data; thereafter, all three authors of the paper took part in the coding process and discussed their ideas and assumptions throughout the coding procedure.
Results
General and Grief-Related Mentalization in Parents
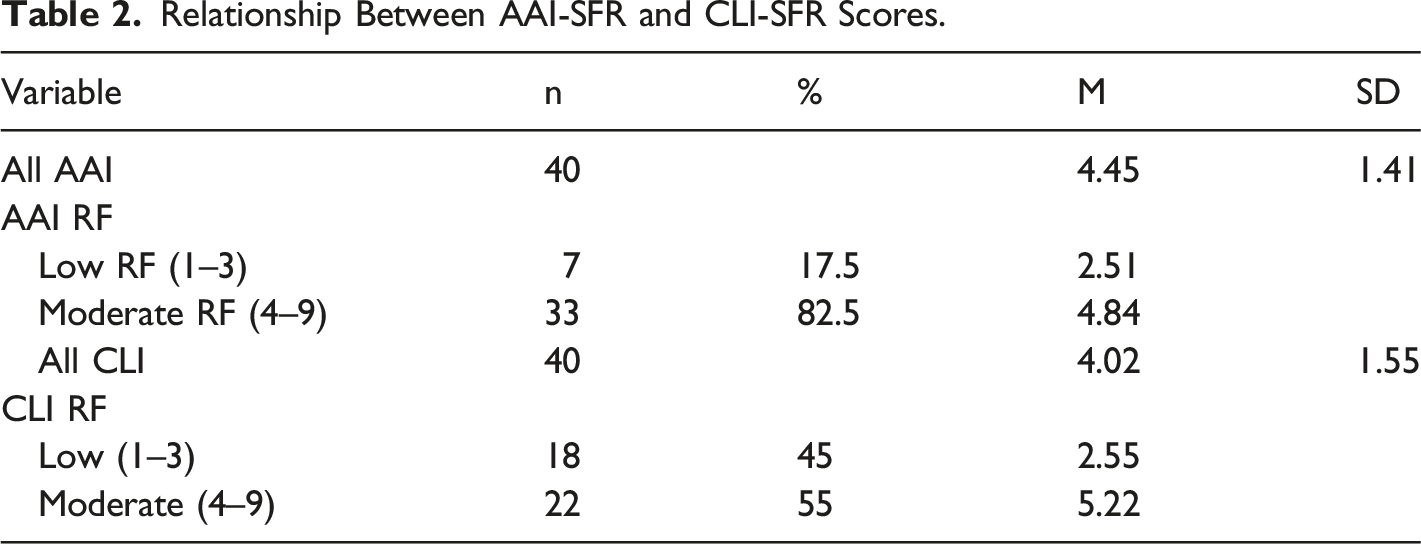
We analysed the relationship between the low mentalizing (1–3) and high mentalizing (5–8) RF in the CLI (Child Loss Interview) and the AAI (Adult Attachment Interview) scores.
Relationship Between AAI-SFR and CLI-SFR Scores.
The Specifics of Grief-Related Mentalization in Parents
In those CLI interviews that were rated RF>4, parents were able to describe their experience coherently, which was indicated by bottom-up analysis of the entire interview (for types and frequency of mentalizing categories in parents see Supplementary material (1). Interestingly, this coherence tended to emerge through their explicit references to changes of their experience at particular points in time. Below we present two examples of such consistency.
Mother 1: Excerpt from the beginning of the interview: I don’t think so much about it nowadays, but there were months, I don’t know how long it went on, if it was months or years, but I simply kept talking to him. And an excerpt from the end of the interview (later point of grieving): At one point I just stopped.... Of course, time also makes you stop seeing him in your mind’s eye, you’re unable to remember, to recreate his face, his features, his smell. (RF=6). In this example, the consistency and continuity of experience is achieved by the mother describing her maintenance of active contact with her deceased son and indicating that at some point she had stopped being in such active contact as before.
And the first example from the second mother’s talk: You see, I don’t remember the 4 months after her death at all, not a single day (...) I don’t remember my August from that period (...). The second example from her talk comes from a later point of grieving: I would sit with August in his room, he would be playing and I was just in another world (...) those thoughts, that Rita was not there, were crushing me. At that time I was going through a period like that.. (RF= 7). And finally, an excerpt, in which the mother refers to her here and now: I would look around to see whether I was me here and now, so to speak, or behind that glass again. But now (...) as soon as I feel that, I think of a way (…) to get out of the house and be with people (RF= 6). In this second case, the mother achieves coherence of narration by describing how her experience changed over time. She first points out impossibility of remembering events in early period of grieving. Thereafter, she tells about moments when she was able to recall the reality around her (her son playing) but at the same time being immersed in her thoughts about her deceased daughter Finally, she is aware of the impending risk of becoming immersed in her internal reality and taking preventative measures.
The Perception of Time in Grieving Parents
We identified three main themes related to parental grieving (for the frequency of the codes, main themes and subthemes, see Supplementary material (2). In their reflective utterances, parents predominantly portrayed their grieving as a process of mentally shifting back into the past (‘mentally back to the child’). At the same time, they needed to manage the tensions caused by being at once immersed in the past and living in the present reality around them (‘here and in another world’). Their sense of being stuck in the past and their ways of overcoming it was also reflected in the recurrent existential questions, anger and disappointment encompassed by the topic ‘managing the discontinuity of time and of the world’.
‘Mentally Back’ with the Child
The phenomenon of being ‘mentally back with the child’ predominantly takes the form of involuntary mental activity (see the ‘mentally back with the child’ and ‘awareness of automatically returning to the child’s illness’ subthemes). However, participants in our study were often able to identify these automatic thoughts retrospectively and pinpoint the mental states that were related to them. By employing reflective functioning, parents were able to posit the possible reason for this involuntary returning to the child’s illness and death as a kind of ‘mental digestion’ or catharsis: so I was kind of digesting all Piotr’s death again, [it was] as if he was dying again, in effect (...), and so I think my body, and my mind, had to work through all the things that were most stressful for me again. (RF = 6).
Another aspect of being ‘mentally back with the child’ involved projecting ex-post expectations concerning the course of the child’s medical treatment (‘awareness of projecting wishful scenarios onto the pre-death period’). These expectations involve the wish to have been a better parent who would have been able to save the child’s life: Perhaps I should have done more, or perhaps it was because of me, because perhaps I should have gone to one particular CTG monitoring (RF=4), and another example: I just blamed myself that it could have been… I could have done certain things better (RF=5). This kind of regret reveals re-enactment of alternative scenarios related to the child’s treatment in the parent’s mind. In such cases, however, parents were able to identify their underlying feelings, particularly the sense of guilt or regret.
Another phenomenon within the theme ‘mentally back with the child’ involves identification of the connections between concrete reminders of the child, the mental image invoked by them and the underlying emotions (‘insight into the pain of being confronted with reminders’). It was triggered by particular places, clothes, toys, other children, or experiences. To get to our cemetery, you have to go along this road where you pass the preschool (…) I would see the children running around, and it broke my heart (RF=6), or another example: Whenever I was tenderizing schnitzel cuts for dinner, somewhere in my mind’s eye I would see her little fingers, because she would always lick the seasoning off, and I would always say, ‘Rita, that’s raw meat, no!’, and so I could be hammering those schnitzels and standing there howling (RF=7).
In some instances, however, the phenomenon of being ‘mentally back’ was deliberately induced by parents in order to experience closeness to the deceased child (‘awareness of seeking a connection to the child’). This might involve spending time in the child’s room, breathing in the smell of their clothes, frequently looking at photographs of the child, or generally spending time in places where the child had often been before its death. To the end of my life, I will always associate the blue Lenor with death, you see, because that was how my Rita, her nightshirt, smelled. And for example I had this thing about going to Rossmann, and that Lenor [would be there] somewhere, and I would smell it, and at once it was as if I was going back, you know, in time, kind of, and then I was [standing] over her by that bed of hers, and I could see that nightshirt of hers (RF=6).
The theme of this phenomenon of being ‘mentally back’ with the child shows parents’ mentalizing insight into the ways in which they became re-immersed in the past. This ‘mentally back’ phenomenon may be invoked by guilt, regret, or resentment, but predominantly by longing for the child. Going ‘mentally back’ may be seen as a repetitive mental enactment of the period of the child’s illness and treatment that may contribute to emotional regulation through ‘mental digestion’, or momentary fulfilment of the longing for the child.
Now and in Another World
The topic ‘now and in another world’ shows parents’ sense of only partially living in the present, as their reality is overshadowed by the past and a different reality in which they seek contact with their child and experience its loss (‘awareness of being disconnected from ongoing life by the pain of the loss’). The past is represented by sensations and thoughts that take them ‘mentally back to the deceased child’, while the present is designated by the surrounding reality. The idea of ‘another world’ means that parents do not participate fully in the reality around them as their mind seeks connection to the deceased child (‘awareness of being disconnected from ongoing life due to returning to the child’s illness’) and they mentally return to the period when the child was still alive. I live in two realities now; there is the reality in which Robert is present here and there(...) But there is the reality that is also going on here and now. (RF=7) (‘recognizing religion as a source of help’).
The parents noticed this underlying tension related to not fully living in the present ‘here’ both at the interactional level – shifting into ‘withdrawal from social contact’ – and in their cognitive processes (‘blurred cognition and sensual feelings’), where they recognized in particular that their memory and attention were blurred. This was reported as having been particularly intense in the initial weeks and months after their child’s death, thus impairing their engagement with the reality around them. I don’t remember my August [her son] from that period, I don’t remember those months at all. (...) Where I went and what I did, I don’t know, I swear to you that all I remember is that every evening I cried on her bed because she was not there anymore (RF=6).
Interestingly, in some cases, the parents referred directly to experiencing the existence of an internal barrier in them, which separated ‘here’ from ‘another world’,: When Karolina died, to be able to take care of Joanna, I also had to manage somehow, I couldn’t allow myself to mourn Karolina. So I remained behind a wall (RF=7). The parents interpreted the creation of this barrier as a necessary means of being able to function in a task-oriented way in the reality around them, but also as a kind of mental asylum that meant they were not living fully in the world around. In this second case, some parents reported their ways of overcoming this state of disconnectedness from the external reality: I was just in another world (...) those thoughts, that Rita was not there, were crushing me. At that time I was going through a period like that (...). And just now, recently, at times, at some moments, I feel like I’m cutting out. (RF= 7).
The theme ‘Now and in another world’ involves dynamic tension between being stuck in the past, in the subjective experience of clinging to the child or re-experiencing the loss and the competing reality of the present. Interestingly, parents also explicitly gave time dynamics: You see I don’t remember the 4 months after her death at all, which means that in retrospect they recognize that their feelings of disconnection from the life around them was particularly intense at certain times.
Managing the Discontinuity of Time and the World
‘The discontinuity of the world’ means that parents may be stuck by temporarily being unable to deal with the question ‘Why did it happen?’, which incorporates protest, anger, questioning the reasons, etc. (‘being lost in the world and grievances towards God’). As a result, they feel different than the people around them and out of place in ordinary life: I had phases where I would be walking along the street and I would think ‘Geez, where are they all hurrying to, you know, where are they running to, these people, the buses, the cars.’ That my child had died, …, I don’t know how to say it, that this tragedy of mine, Rita’s death, that it was unimportant in the daily life of the whole world, you know, that children die, children are born. (RF=6).
Through ‘why’ questions, parents implicitly oriented themselves back into the more remote past or longer span of their life, as their child’s death caused them to question their overall attitude to life (‘“why” questions and seeking meaning’). M: Yes, I think that this is a question that you ask yourself from the beginning, when he first fell ill – Why him, a child who is innocent? (...). Then again, on the other hand, if children didn’t suffer and we wanted to exclude anybody from anything, the world wouldn’t be real (RF= 5). Interestingly, such utterances also incorporate existential answers that go beyond the parents’ orientation toward the past in the direction of finding meanings in a more general perspective, that are seen as ‘managing the ‘discontinuity of time and the world’. Therefore, the ‘discontinuity of time and the world’ theme touches on a broader, more general temporal perspective that is rooted in the feeling of being stuck in the past (‘the experience that time has stopped’) and involves the discontinuity of previously accepted meanings (‘the experience that part of the self has been lost’). Such discontinuity, however, is managed by the experience of ‘change and continuity in the self’, which refers to the preservation of some personal characteristics: Your life has been turned upside down completely, and that’s all there is to it. One stage is over, you – I – am completely, well, of course, character traits remain, you are still in a sense like you were, but your thinking about life and all the rest is completely overturned (RF = 6). In this utterance, the explicit references to changes are accompanied by equally explicit references to continuity: you are still in a sense like you were.
The ‘experience of change and continuity in the self’ sub-theme (example given above) indicates that the emergent changes in the self were prompted by parents’ feeling of discontinuity in the way they had experienced the world before the child’s death. Paradoxically, such discontinuity seems to stimulate grieving parents to ‘recognize and initiate’ changes in their mental world by provoking them to answer ‘why questions ‘and seek meaning in religion’. These active strategies seem to make them focus on the ongoing reality ‘here and now’ and on the future perspective. Therefore, their ‘mentally shifting into to the past’ may become less frequent and intrusive (‘the receding need for a sensual connection to the child’).
Summary of the Results
The quantitative results show that parents’ mentalization in grieving was compromised when the topic of their child’s death and their grief comes up in the talk. Nevertheless, their mentalization of grief correlates with their general mentalization level, which means that better mentalizers on a general level still have better capacity to mentalize their grief. Interestingly, the narrative coherence in Child Loss Interviews indicates that explicit references to time-related changes in parents’ experience of grief require effective capacity to mentalize these internal transformations.
The phenomenon of ‘mentally back with the child’ shows how the passage of time is temporarily arrested during certain periods of grief, causing parents to become immersed in the past by re-experiencing it in the present. The theme ‘now and in another world’ shows that the past invades their experience of the everyday reality of the present, resulting in a sense of mental absence and blurred cognition. The theme of ‘managing the discontinuity of time and the world’ predominantly refers to parents’ experience of the suspension of time through repeated ‘why?’ questions. This theme also indicates the shift into the present – the reality of the grieving parents, in which their existential questions are partly answered. To sum up, the multimethod research design enabled us to describe in what way good mentalizing capacity contributes to parents’ insight into the discontinuity of their grieving experience but at the same time to preserving the chronological continuity of their autobiographical accounts.
Discussion
The research profiled here shows that grieving parents who are generally good mentalizers were able to describe their ongoing and retrospective experience of grief coherently. This might mean that moderate to high levels of general mentalization contribute to better emotional regulation (see Slade, 2005) in confronting the loss of a child. We thus concluded that perception of time in grief is marked by a discontinuity of experience that manifests itself in re-living the past, marginalizing the present reality and a disrupted experience of self and the world around. This is in line with anthropological conceptualizations of time as ‘pendulous’, where a sequence of events is seen through its discontinuities (see Leach, 1961; 133–134). Nevertheless, our analysis shows that grieving parents were able to ‘mobilize’ their mentalizing capacity in order to describe the waves of disruption to their sensual and cognitive experiences during the grieving period.
This research shows that bereavement and the grieving process temporarily interrupt parents’ experience of the linear passage of time. However, effective mentalizing and the narrative coherence of parental accounts make it possible to track time-related changes in their grieving. In their narrations, parents shift back and forth in time: sometimes they report the decreasing intensity of their longing and pain; other times they talk about their ways of relating to the surrounding reality. One might also speculate that coping with grief, for example, fluctuating between loss-oriented and restoration-oriented coping (see Stroebe & Schut, 2010), could enhance the narrative coherence of grievers.
Our analysis confirms the claim of Stroebe et al. (2017) that linear models of stages in grief are not consistent with the subjective experience of discontinuity of time in grievers. The analysis described here shows that parents tend to return in their minds to the period when the child was still alive; this means that although they are ‘here and now’ physically, they are often ‘then and there’ mentally. However, independently of this temporal discontinuity, parents are partly able to manage their pain or gain new perspectives that are different from those that appear at earlier stages after their child’s death. In this sense, they gradually accommodate the self-related discontinuities in their life (see Rando, 1993), and their shifts between the surrounding reality and closeness with the child seem to become less disruptive.
Limitations and Directions for Future Research
The research group comprised parents who had experienced the death of their child after an illness, and as such, the possibility of mentalization of the loss of a child after traumatic losses and the way in which time is experienced by parents in this group are areas that require further attention. In their mentalizing utterances, parents tended to indicate that they made active mental effort to overcome this sense of being stuck in the past, but it remains unclear to what extent mentalization-related insight can help them to establish a mental relationship with the deceased child (Bowlby, 10980) or to revise their grief (Shear, et al., 2008). There is also a need for examination of the extent to which mentalizing capacity can help parents to overcome the sense of being stuck in their loss and contribute to transformation and maintenance of continuity in the self. And finally, it should be acknowledged that although both mothers and fathers were investigated, the gender differences between them were not addressed in this research.
Clinical Implications
Activating thoughts and memories related to the deceased person by means of proximity-seeking behaviours appears to turn the griever back repeatedly to that period in their own life, thereby creating ambiguity and a sense of the suspension of time. The process of adjustment in grief may be seen as a way of accepting and then reducing this oscillation between the griever’s past and their present. This is in line with the concept of revision of the internalized representation of a lost loved one by incorporation of the reality of the loss (Shear & Shair, 2005), which seems to anchor the griever in the ongoing here and now of their life.
Given that failure to integrate the loss into the survivor’s autobiographical memory may result in complicated grief (Boelen et al., 2006), and that adaptation to loss involves the capacity to assimilate this experience into a ‘macro-narrative’ story (Neimeyer et al., 2014) we claim that drawing on grievers’ mentalizing capacities to create coherent autobiographical narrative may contribute to the adjustment process in grief. Clinicians should normalize this ‘disruption of the self and the world’ and disruption of the experience of time in grieving parents. This is in line with research by Dias, Doherty, and Brandon (2017) showing that grieving parents face a role-identity conflict as they become aware that the absence of their child challenges their identity as a parent. Therefore, working on disruptions in the self would seem to be particularly important in this group of grievers. In the same way, working on disruption of the worldview and the general time frame of life should be acknowledged. This corresponds to research showing that the loss of a child is considered especially disruptive to an individual’s structures of meaning, threatening their sense of identity and purpose in life (Davies, 2004) and evoking a unique existential crisis (Wheeler, 2001). The awareness that in the grieving process time is experienced as alternation may help clinicians to create ‘a transitional space’ where this experience can be relived back and forth in order to be understood and gradually integrated. This integration process may involve creating connections between disrupted parts of the self and developing ways of experiencing the surrounding world, with an evolution of the connection to the deceased child occurring in parallel.
Supplemental Material
sj-pdf-1-ome-10.1177_00302228211062369 – Supplemental Material for Time in Grief: How do Bereaved Parents Mentalize It?
Supplemental Material, sj-pdf-1-ome-10.1177_00302228211062369 for Time in Grief: How do Bereaved Parents Mentalize It? by Bernadetta Janusz, Joanna Jurek and Karolina Dejko-Wańczyk in OMEGA-Journal of Death and Dying
Supplemental Material
sj-pdf-2-ome-10.1177_00302228211062369 – Supplemental Material for Time in Grief: How do Bereaved Parents Mentalize It?
Supplemental Material, sj-pdf-2-ome-10.1177_00302228211062369 for Time in Grief: How do Bereaved Parents Mentalize It? by Bernadetta Janusz, Joanna Jurek and Karolina Dejko-Wańczyk in OMEGA-Journal of Death and Dying
Footnotes
Acknowledgements
We thank Pawel Dobrzynski and Jolanta Grabowska Markowska for their contribution to contact with parents of deceased children.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.