
Abstract
The Concerns of Grieving Caregivers Scale (COGCS) is the first of its kind to explore caregivers’ concerns about their own parenting, as well as their relationships with, and specific behaviours of their bereaved child(ren). Using exploratory factor analysis, we evaluate grieving parents’ and caregivers’ concerns using data collected across clinical populations from two community organizations supporting grieving families (i.e., a children’s grief centre and a community hospice). Two identified factors were established: Concerns about Caregiving and Concerns about the Child. The COGCS demonstrates good internal consistency and criterion validity in its application with two distinct clinical samples. The use of this scale could be of value to clinicians supporting bereaved caregivers and their families as they can integrate concern-specific resources into their practice to better support their clients’ presenting concerns.
Grieving parents and primary caregivers simultaneously balance the unique, mutually-influencing challenges of living with their own grief, while parenting a grieving child. It has been well-established that communication scaffolds children’s understanding and coping with serious illness and death, and that both what and how parents communicate with their children about these topics tends to be informed by parents’ own grief, their hopes and fears about how their children would react, and their ultimate drive to protect them from stress and harm (see Christ & Christ, 2006; Dalton et al., 2019; Webster & Skeen, 2012). Recent research (Alvis et al., 2020) explored and measured how caregivers may mitigate or facilitate their child’s grief reactions through their positive (e.g., communication and activities) and negative (e.g., avoidance and emotional suppression) parenting behaviors using the Grief Facilitation Inventory. However, minimal research has been conducted specifically on the topic of caregivers’ concerns about their parenting self-efficacy in the context of bereavement and their grieving children’s psychosocial needs. Exploring the influence of parental concerns in the context of grief can provide a more nuanced understanding of parental grief perceptions and how these concerns about caregiving and their children’s grief reactions influence their own psychosocial outcomes, which, may reciprocally inform their parenting behaviors with their bereaved children. In this study, we develop and evaluate a scale of grieving parents’ and caregivers’ concerns using data collected across two agencies supporting grieving children and families in Ontario, Canada: Dr Jay Children’s Grief Centre and Heart House Hospice.
Children who are living with the dying or death of a family member are at increased risk for a variety of emotional and psychological impacts such as isolation, uncertainty, anxiety and depression; conduct, internalizing and/or externalizing disorders; and impaired social and academic functioning (Birenbaum, 2000; Luecken et al., 2014; McCarthy et al., 2010; Worden & Silverman, 1996). Bugge et al. (2014) explain that children’s grief can manifest as behavioral changes, somatic symptoms, fears related to separation from, and the perceived vulnerability of their caregivers. These manifestations can be concerning for parents as children’s grief and mourning often presents differently than in it does for adults (Christ & Christ, 2006). Simultaneously, grieving parents wrestle with the competing demands of understanding and meeting their children’s needs during their own intense psychological reactions (Bugge et al., 2014; Christ & Christ, 2006; Rogers et al., 2008). These experiences can be understood through a variety of frameworks. For example, in Attachment theory (Bowlby, 1969), the caregiving system is at the intersection of parenting and parental grief and evolves in parallel to the child’s attachment system, to promote the child’s safety and security (George & Solomon, 1996, 2008). Caregiving systems are activated when parents perceive a physical or emotional stressor or threat towards their child, triggering elevated stress and a protective drive (Cassidy, 2008; George & Solomon, 2008). A family member’s serious illness or death acts as a stressor that parents cannot subdue, amplifying feelings of helplessness and vulnerability, driving them to find opportunities to defend their children against physical, psychological, or emotional suffering (Bugge et al., 2014; Dalton et al., 2019; Kars et al., 2008). Insofar as parents and caregivers define the parameters of their children’s presence, inclusion in, communication, and support related to dying and grief, their concerns influence their children’s experiences.
Competence in parenting a bereaved child reportedly mediates children’s bereavement outcomes after the death of a parent (Christ & Christ, 2006), as does open-communication (Dalton et al., 2019; Librach & O'Brien, 2011; Luecken et al., 2014); though many surviving parents admittedly seek guidance to address their concerns about how to competently understand their child’s behaviors, reactions, and how to communicate with their child about death and the person who is dying/has died. At a time when parents’ capacities to meet their children’s needs are strained by their own grief, their behaviors and emotional expressions have been shown to significantly affect their children (Luecken et al., 2014). However, in the context of grief and heightened protective instincts, parental competence can be undermined and communication is often limited and challenging (Bugge et al., 2014; Librach & O'Brien, 2011). Within this context, the magnitude and level of concern that the parent feels for their child’s coping and their parenting ability may influence the quality of the child-caregiver relationship, access to services for their child, and may either be a substantial precursor or deterrent for more communication and inclusion regarding their child’s experience of grief.
Parents have identified a multitude of fears influencing whether and how they talk with their children about death and grief, including their own distress, fear of upsetting the child, and feeling discomfort of uncertainty about their ability to discuss or support their child in understanding and coping with these issues (e.g., Dalton et al., 2019). Animating the proverbial “elephant in the room,” children’s awareness of illness, dying and death often exist even in the absence of communication, perpetuating a “mutual pretense” in which the shared awareness is not discussed by parents or children, in an effort to avoid distressing one another (Bluebond-Langner, 1978; Dalton et al., 2019). However, avoiding communication may seem to align with parents’ instincts to shield their children, it inadvertently contributes to lasting, negative psychological outcomes for both children and parents, including anxiety, depression, isolation, as well as parental regrets, and heightened fears and perceptions of their children’s needs (Bluebond-Langner et al., 2010; Christ & Christ, 2006; Dalton et al., 2019; Eklund et al., 2020; Kaplow et al., 2014; Kreicbergs et al., 2004 Webster & Skeen, 2012).
In these and other complex ways, parents’ fears, perceptions and concerns influence their approach to parenting a bereaved child including their communication with, inclusion, and support for their grieving children. Only within the last decade have researchers begun to explore the effects of parental concerns, specifically when the parent themselves had an illness such as cancer (e.g., Muriel et al., 2012). Parenting status has largely been overlooked in cancer-related research and clinical care, though a substantial proportion of cancer patients identify as parents. Muriel and colleagues’ (2012) described parenting as both the caregiver’s primary role and an aspect of their identity, noting that established psychometric scales examining quality of life or concerns rarely explore caregivers’ concerns related to children in particular; either overlooking this altogether or reducing this exploration to a single-item question. This lack of representation is problematic as it limits the understanding of the perceived impact of illness and death on the child, the parent-child relationship, and how the combination of these factors may be concerning to parents. To address this gap, Muriel and her team conducted qualitative focus groups with parents diagnosed with cancer to develop the basis of their Parenting Concerns Questionnaire (PCQ), a scale designed to explore parental concerns about their own anticipated death and its impact on their child(ren). Building on this foundational research and established scale, there is a need to specifically examine parents’ and caregivers’ concerns for their children and their parenting in broader contexts, such as the dying and death of a family member. Exploration of potential relationships between concerns and communication about death and grief has been largely unaddressed in the literature and can hold important clinical implications relating to parents and caregivers of bereaved children.
Context of the Present Study
The potentially important role of caregiver concerns on both the outcomes of the child and the caregiver highlights the need for a valid and reliable measure of concerns for a wider array of parents and caregivers beyond terminal cancer patients. The goal of the current study was to report on the development, factorial validity, criterion validity, and internal reliability of a new measure of caregiver concerns in the context of grief and bereavement.
Methods
Procedures
Recruitment for two samples occurred separately across two charitable organizations, both located in large, urban centers in Ontario, Canada, offering their services free of charge to culturally-diverse clientele, both within their homes and at their respective agencies. In total, 512 individuals participated across the two sample locations.
Participants from both agencies completed a survey package online as part of the intake process; this survey (named the Parenting and Grief Evaluation Survey; PaGES) includes both the Concerns of Grieving Caregivers Scale (COGCS) as well as an additional set of questions exploring the frequency of caregiver-child communication about various aspects of grief and dying, outlined below. Participants used a unique code rather than their names in order to protect confidentiality, and to denote the specific center from which they were accessing services. In addition to these measures, the grief center asked a series of questions about the frequency of the bereaved caregivers’ positive and difficult or challenging feelings, as well as measures specifically exploring anxiety and depression.
Sample 1 (Community Hospice)
Heart House Hospice’s programs support dying patients’ and their family members’ health and wellness, including psychosocial wellbeing and bereavement supports in individual and group formats. In addition to their center-based programming, the hospice offers a variety of holistic, clinician-, and volunteer-led in-home services, including counselling for dying individuals and their families, social visits, spiritual care, relaxation therapies and bereavement support. The HUUG Program was launched to support children and youth impacted by serious illness, dying and grief. Although the program was first targeted to young family members of hospice clients, it has since expanded to include grieving children in the community who do not have adult family members served by the hospice. Eligible children and youth may be grieving the dying or death of a sibling, parent, grandparent, or other extended family member or important person in their lives, from any cause. Participants for this study were recruited from the HUUG program.
Sample 2 (Children’s Grief Center)
The Dr Jay Children’s Grief Centre (DJCGC) provides counselling to children, youth (21 and younger), and families focused on preparation, communication, emotional expression, and maintaining connections before and after the death of an immediate family member. The DJCGC also offers group-based support for young people, their parents, and caregivers. In addition to families facing terminal illness, the center serves families grieving a diverse array of deaths, including sudden deaths due to suicides, homicides, accidents, overdose, and medical emergencies, but also deaths due to cancer and other health or medical circumstances.
Participants
Measures
The modified version of the PCQ was originally used at the grief center as an initial clinical assessment tool to guide clinical priorities and target support; a measure of change over time for individual families and an opportunity to refocus service provision in consultation with a counsellor; and as a program evaluation tool to understand clients’ most common or pressing concerns and communication frequency, how these shift over time, and any correlations with demographic or other variables. Revisions were made and piloted over time, in consultation with the clinical team in order to be responsive to changing service delivery, referral trends, and clientele.
The two agencies entered into a data sharing agreement to support collaborative data generation to better understand their clients’ experiences and concerns. Slightly different wording was utilized to reflect the populations they served; specifically, the hospice included references to a family member’s “illness” in addition to death/dying, whereas the grief center used the latter (see Supplementary Table 15 in supplementary materials for comparison of items). Thus, the scale has a degree of flexibility related to the type of death/illness that is being addressed.
The Concerns of Grieving Caregivers Scale (COGCS) was specifically designed to ascertain the degree of caregiver concerns about their child and their own parenting in the context of grief. The original item pool for this scale was 12 items, and we excluded two of those items because of reasons described below as part of the item refinement. Caregivers are asked to reflect on their concerns from the past month and questions are differentiated based upon whether the concern was related to the child, or themselves. Seven child-concern questions ask about emotional reactivity, changes in behavior, and fears that others will also become ill or die. Five caregiver-concern questions explore parenting confidence, self-efficacy, perceived ability to communicate with and understand the child, as well as their fears about the impacts of grief on parenting and their parent–child relationships. Likert-type scale responses range from 1 (not at all) to 5 (extremely concerned); a list of questions from the survey can be found in Supplementary Material (Supplementary Table 15). As indicated in our analysis section, the final version of the scale contained 10-items, with five each for caregiver concern and child concern.
Results
Exploratory factor analysis (EFA) was performed using the Maximum Likelihood (ML) estimator and Promax rotation in SPSS (version 26). Factor retention was decided upon using a combination of Kaiser’s criterion, Scree plot inspection, and Parallel Analysis (O’Connor, 2000). Items for factor analysis were retained if they loaded sufficiently high (i.e., above .40) and with communalities above .20 but ideally >.40 (Child, 2006; Osborne et al., 2008). Internal consistency reliability of the scale was estimated using both Cronbach’s Alpha and the Omega Coefficient (i.e., an index of internal consistency reliability that resolves many methodological issues inherent to Alpha) using JAMOVI (The Jamovi Project, 2021). To validate the new scale, we utilized correlational and regression analyses to provide evidence to support criterion validity, and t-tests to demonstrate similarities/differences across caregiver and child gender groups. Data analyses were conducted separately for each location’s sample.
Data Screening
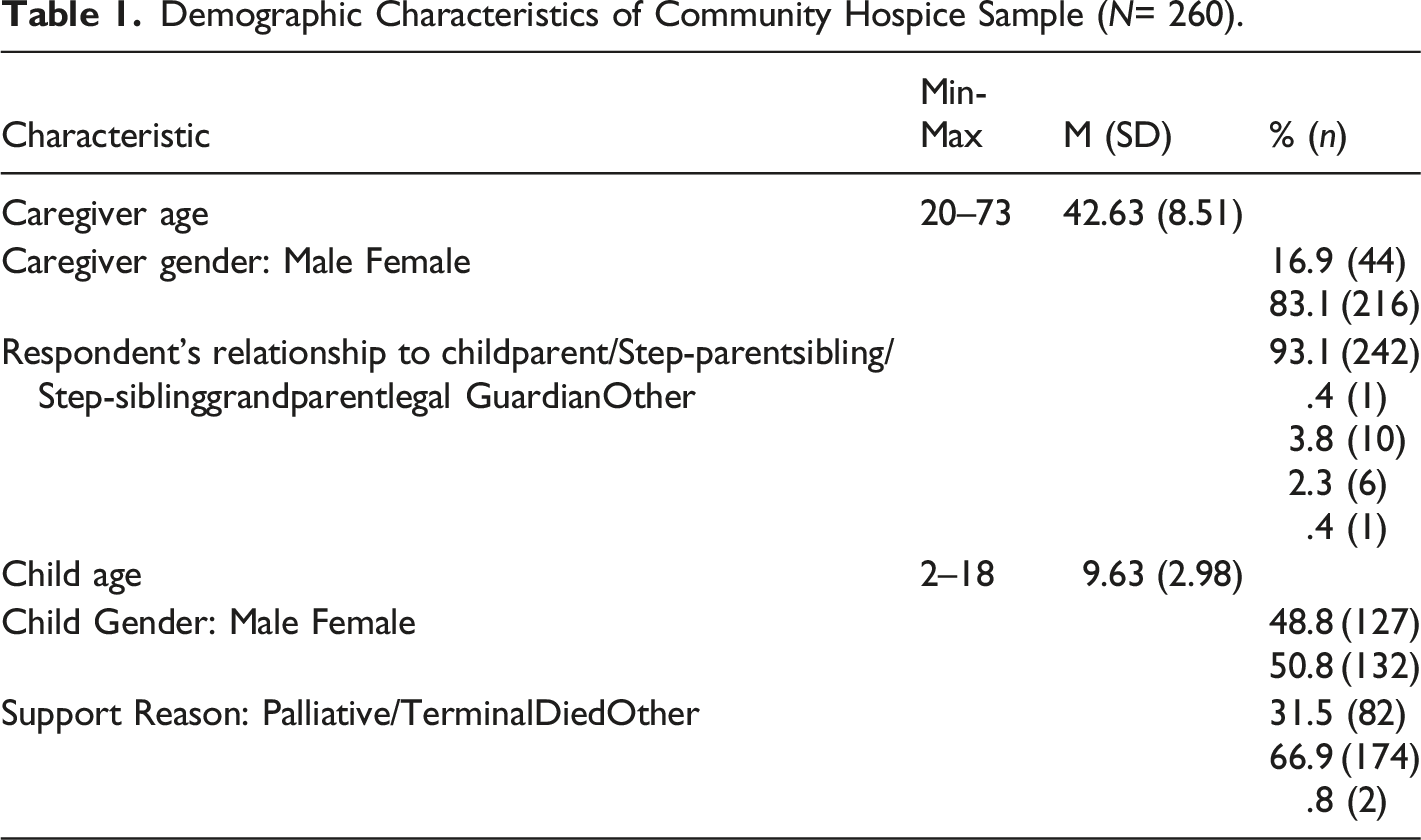
Demographic Characteristics of Community Hospice Sample (N= 260).
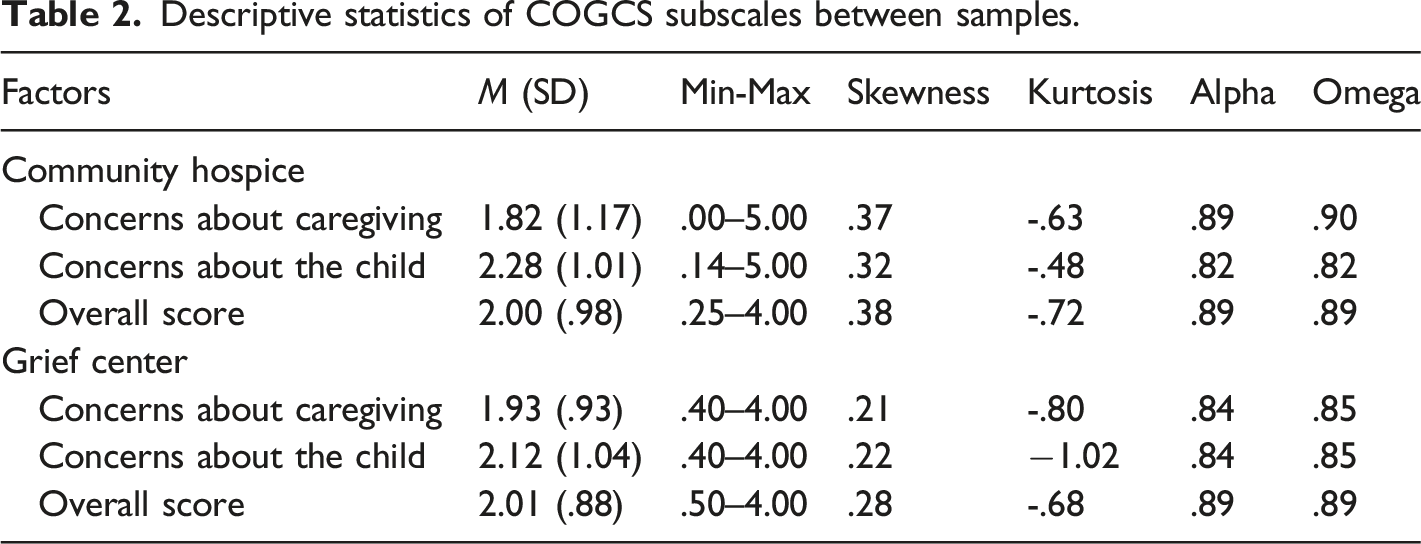
Descriptive statistics of COGCS subscales between samples.
Factor Analysis
Factor Loadings and Communalities.
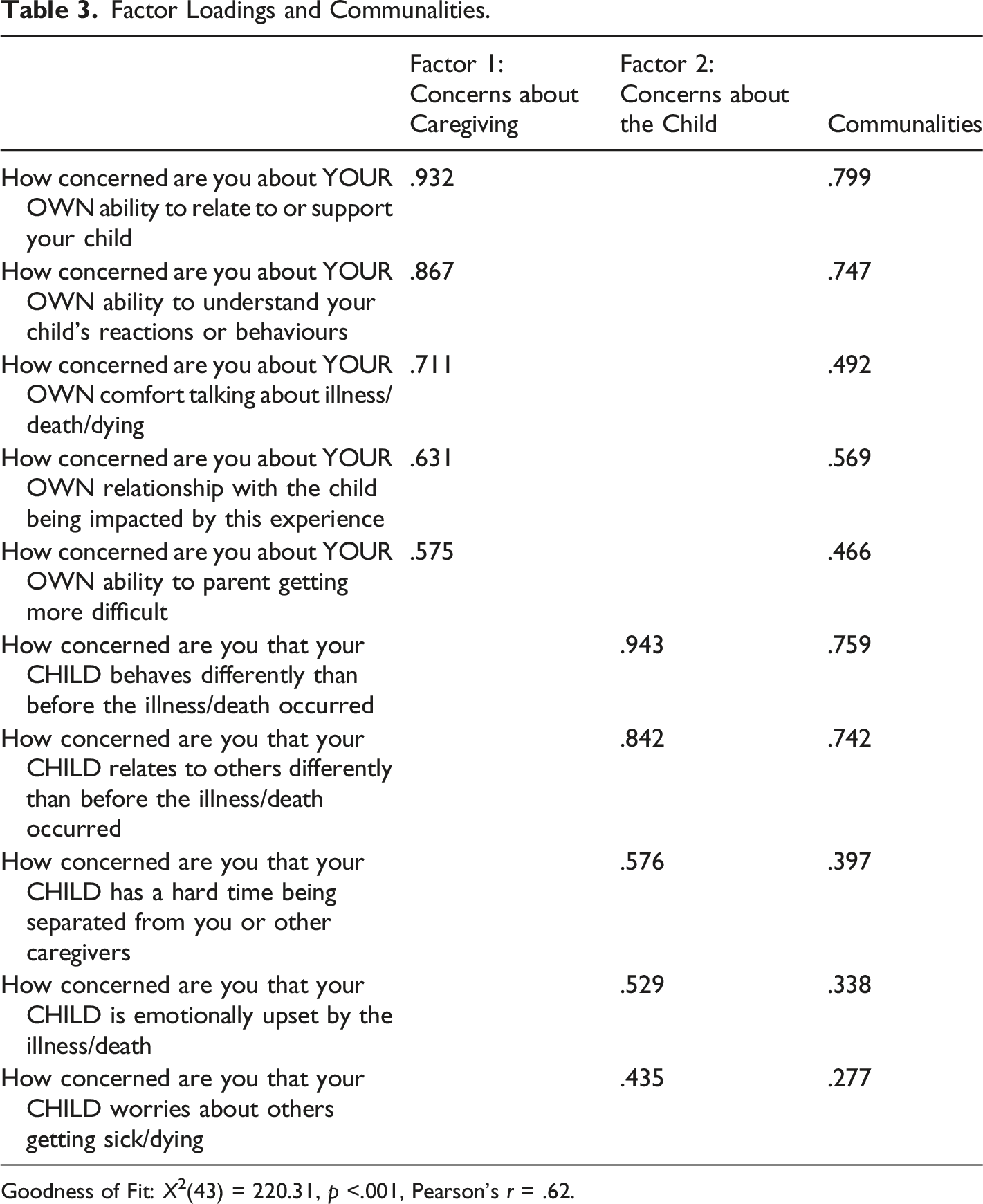
Goodness of Fit: X2(43) = 220.31, p <.001, Pearson’s r = .62.
The two items that did not load in this model were “how concerned are you that the child does not understand the illness/death?” and “how concerned are you that the child will get upset when you talk about the person who is ill/dying/has died?” Their low factor loadings may reflect a dissonance between the other questions’ foci on broader emotional and relational impacts of the dying and death, whereas these two were, respectively, oriented towards the child’s understanding of the illness, and their reaction to a particular conversation rather than to the broader experience of illness or death. These items correlated with each other (see Table 10, supplementary material), as well as with the other child-reaction item, “how concerned are you that your child is emotionally upset by the illness/death?.” Despite their low factor loadings suggesting a lack of fit with the other items, we believe that these two items still hold value for clinicians working with bereaved families and can be asked as supplementary questions to this scale.
Factor 1 was labelled Concerns about Caregiving as the items (e.g., “How concerned are you about your own ability to relate to or support your child?”) all seemed to query a central idea of relational concerns and/or how caregivers respond to their grieving child. Likewise, Factor 2 was titled Concerns about the Child because these items (e.g., “How concerned are you that your child behaves differently than before the illness or death occurred?”) seemed centered around the child’s reactions and behaviors in response to their bereavement. Clinicians at the grief center were consulted and expressed their agreement with the semantic and practical meaning of the items underlying the factors as well as the labelling of the factors.
Analyses with Community Hospice Sample
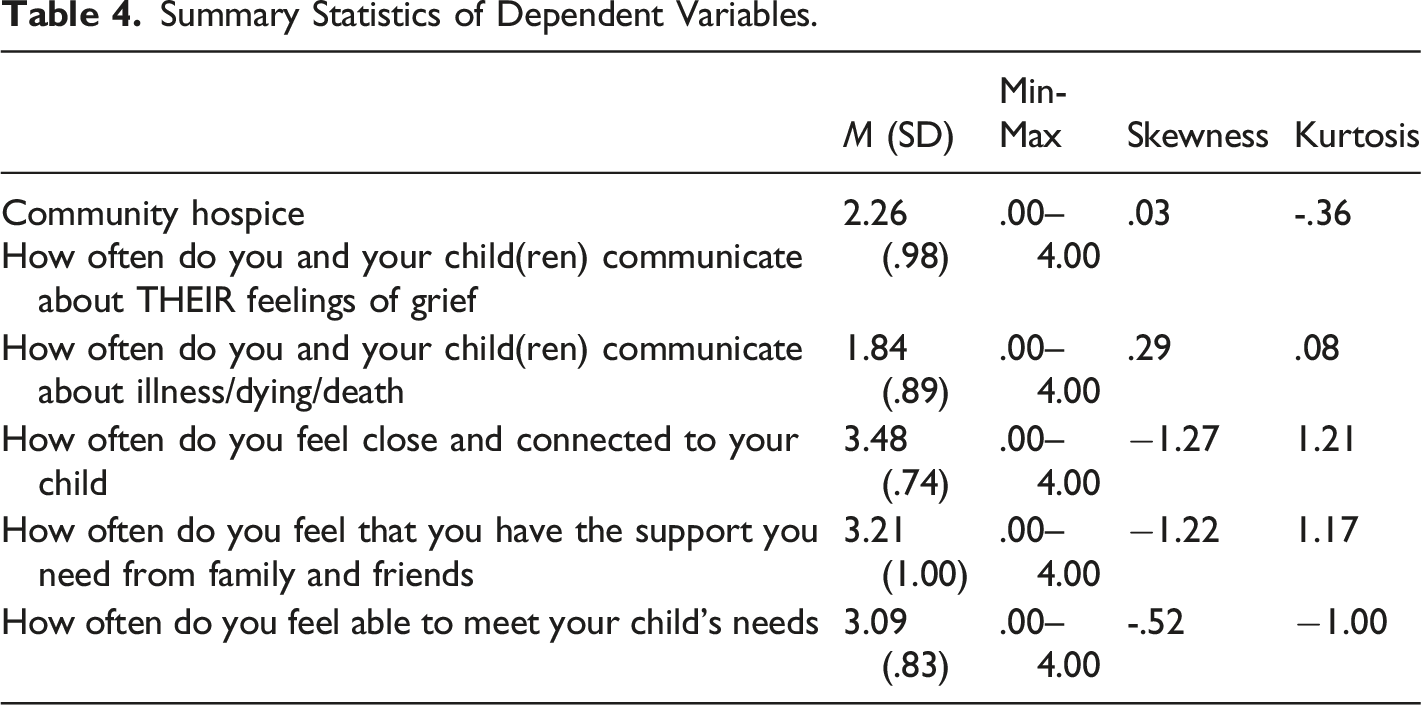
Summary Statistics of Dependent Variables.
Summary of Standard Multiple Regression Analysis with “How often do you and your child(ren) communicate about THEIR feelings of grief” as the dependent variable and Concerns about Caregiving, Concerns about the Child, Caregiver Age and Child Age, and the independent variables (N=244).
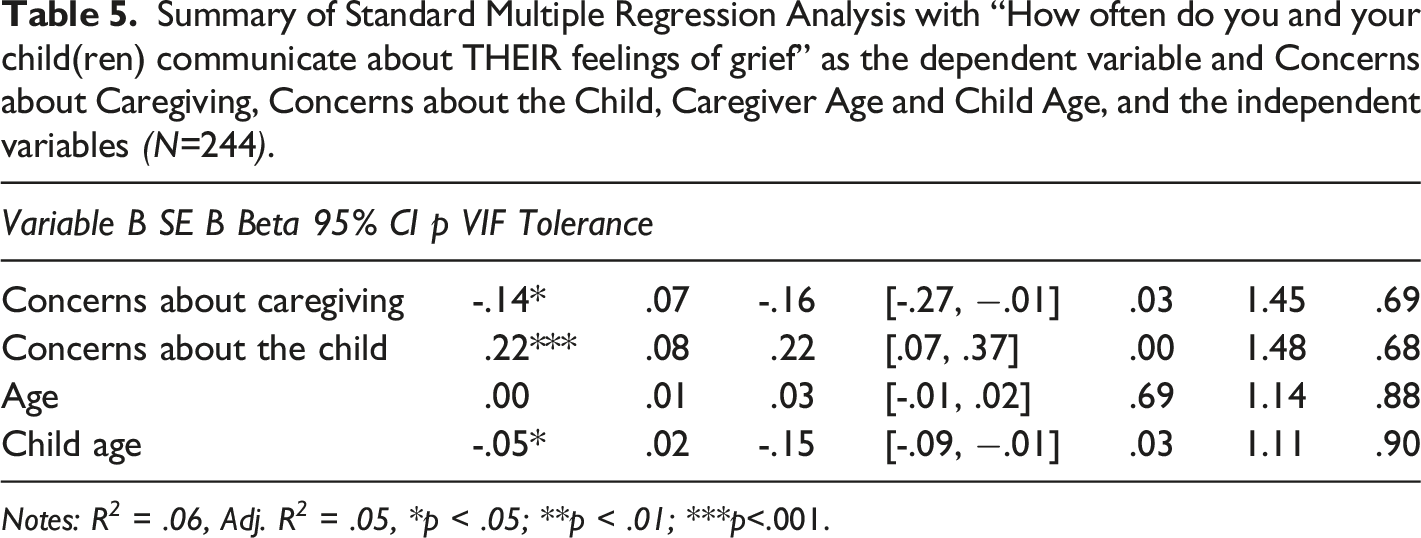
Notes: R 2 = .06, Adj. R 2 = .05, *p < .05; **p < .01; ***p<.001.
Summary of Standard Multiple Regression Analysis with “How often do you and your child(ren) talk about illness/death/dying” as the dependent variable and Concerns about Caregiving, Concerns about the Child, Caregiver Age and Child Age and the independent variables (N=242).
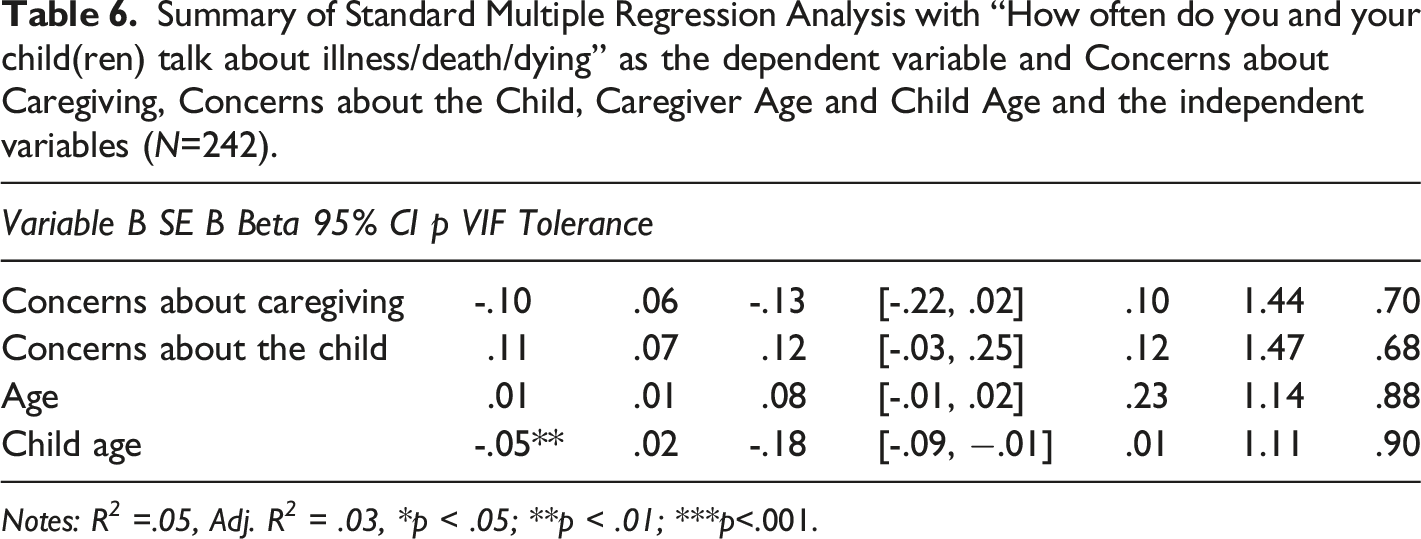
Notes: R 2 =.05, Adj. R 2 = .03, *p < .05; **p < .01; ***p<.001.
Summary of Standard Multiple Regression Analysis with “How often do you feel close and connected to your child” as the dependent variable and Concerns about Caregiving, Concerns about the Child, Caregiver Age and Child Age and the independent variables (N=245).
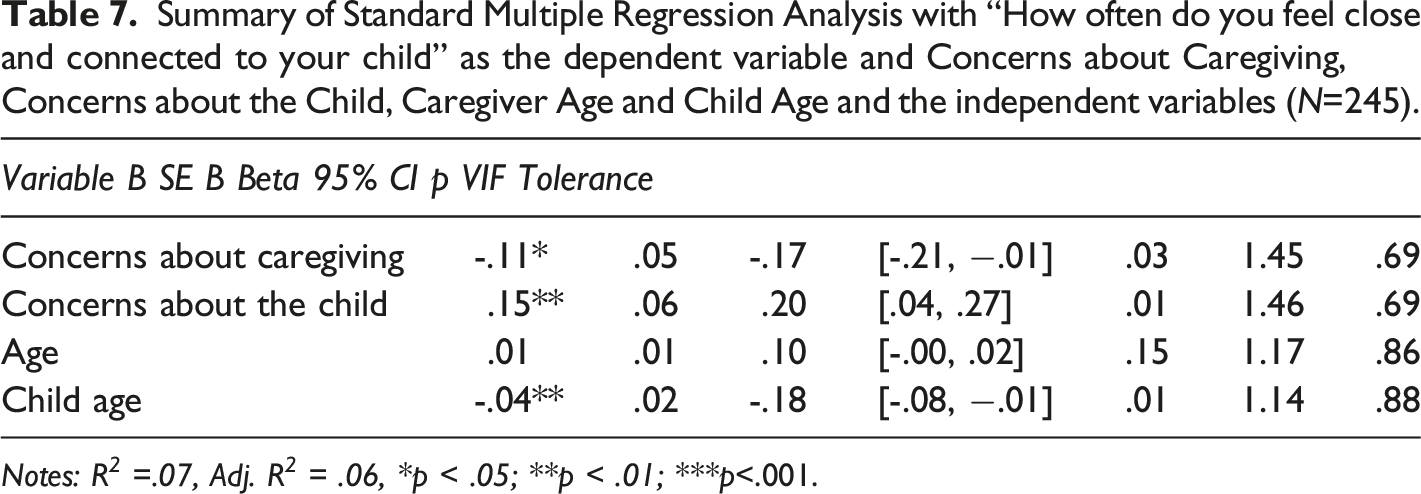
Notes: R 2 =.07, Adj. R 2 = .06, *p < .05; **p < .01; ***p<.001.
Summary of Standard Multiple Regression Analysis with ‘How often do you feel that you have the support you need from family and friends’ as the dependent variable and Concerns about Caregiving, Concerns about the Child, Caregiver Age and Child Age and the independent variables (N=242).
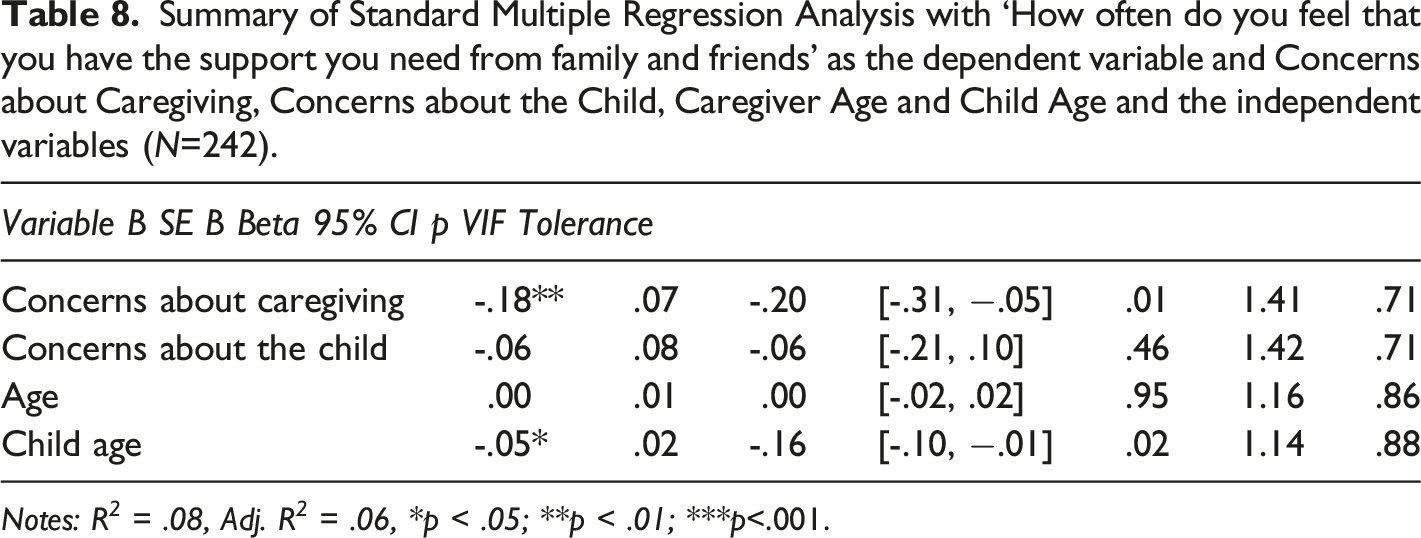
Notes: R 2 = .08, Adj. R 2 = .06, *p < .05; **p < .01; ***p<.001.
Summary of Standard Multiple Regression Analysis with ‘How often do you feel able to meet your child’s needs” as the dependent variable and Concerns about Caregiving, Concerns about the Child, Caregiver Age and Child Age and the independent variables (N=241).
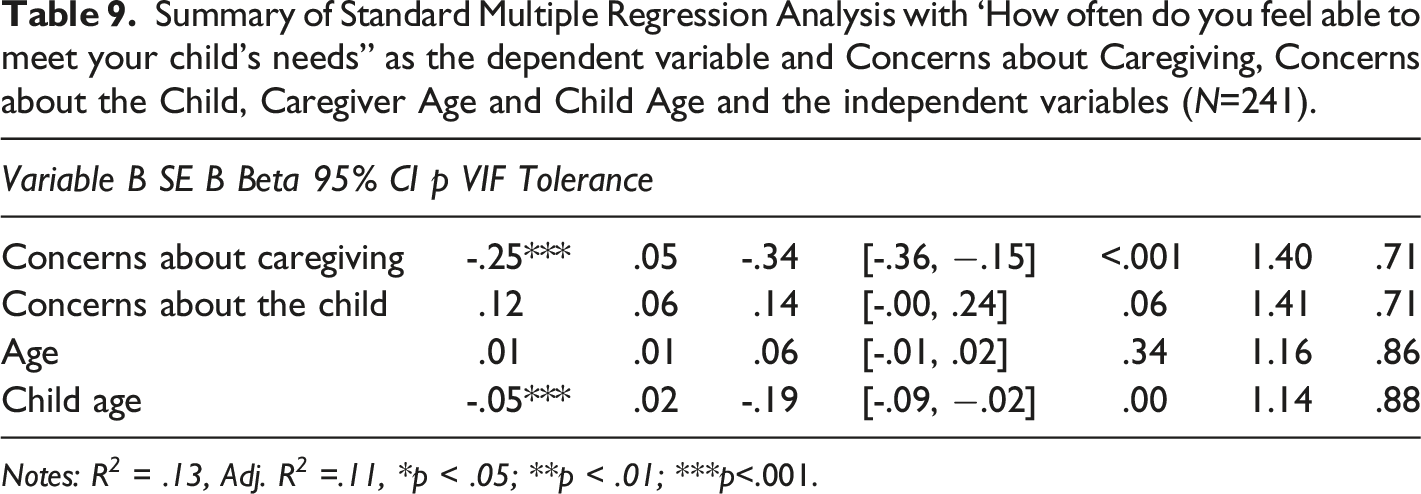
Notes: R 2 = .13, Adj. R 2 =.11, *p < .05; **p < .01; ***p<.001.
Independent samples t-test based on caregiver gender.
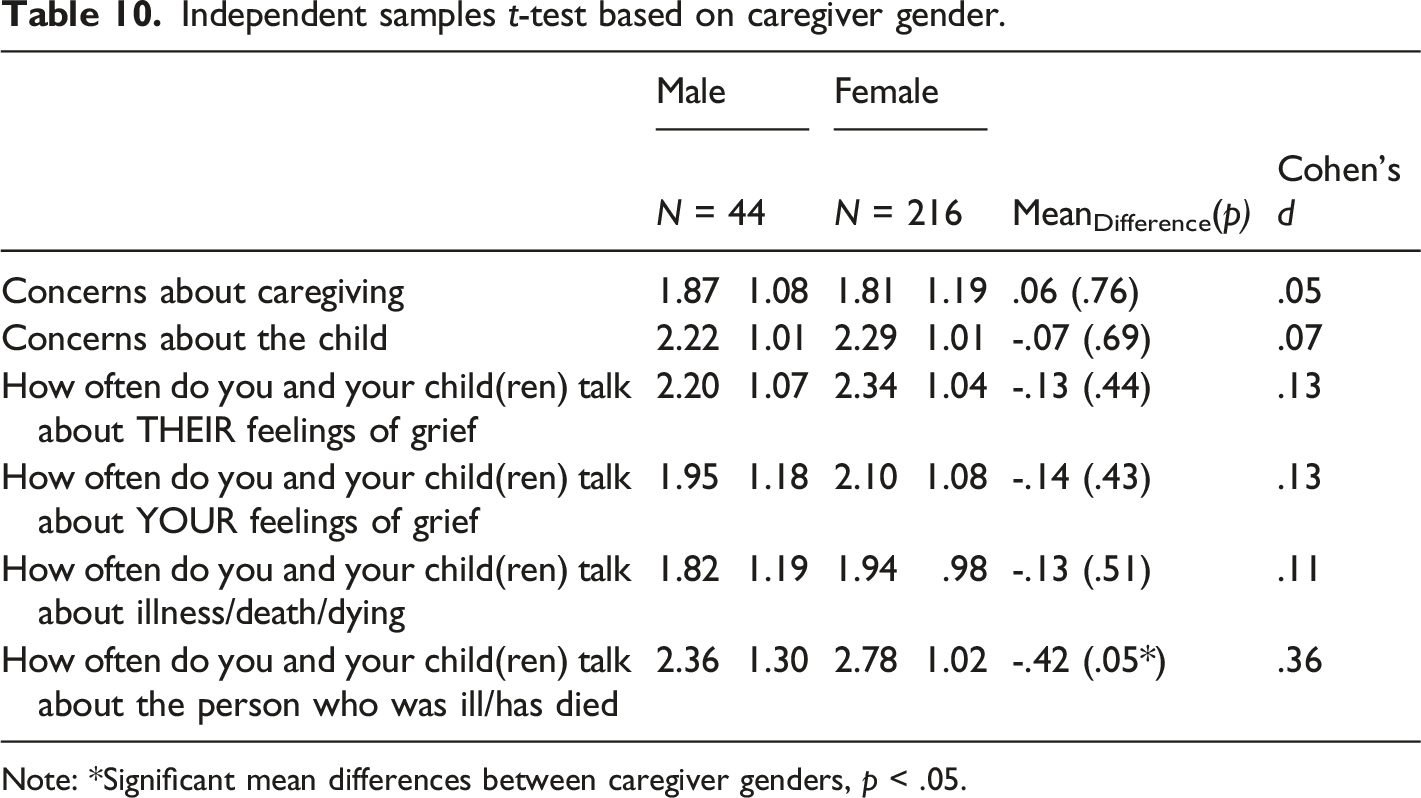
Note: *Significant mean differences between caregiver genders, p < .05.
Independent samples t-test based on child gender.
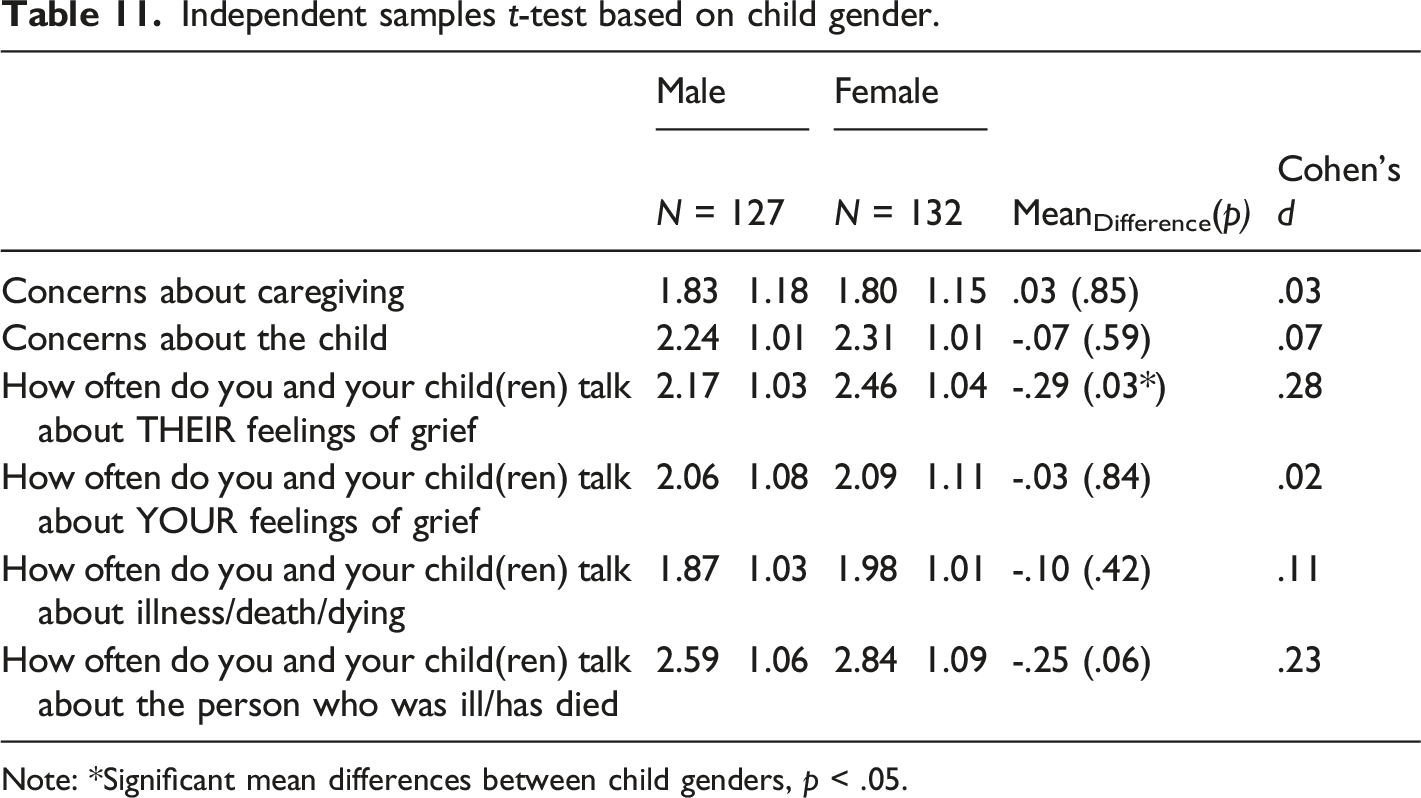
Note: *Significant mean differences between child genders, p < .05.
Grief Center Analyses
Factor analysis. An EFA model was estimated based on the grief center data (N = 72) with results shown in Supplementary Material 1 (Supplementary Table 16). Because the sample size of this analysis is insufficient for adequate statistical power in EFA (Tabachnick & Fidell, 2019; Costello & Osbourne, 2005), those results are not the focus of this study; however, the results and emergent factor structure were largely consistent with the community hospice sample.
Regression. Regression models were estimated for the grief center sample, predicting the frequency of communication about the child’s grief and the person who was ill/dying/had died, as well as anxiety and depression using the GAD-7 and PHQ-9, respectively. In each model, the predictors were the same as in the hospice analyses: concerns about caregiving, concerns about the child, controlling for caregivers’, and children’s ages. Caregiver and child age were included as covariates to account for any underlying differences that may be due to age. Tables for each regression model can be found in Supplementary Material 1 (Supplementary Table 18–23).
Predicting frequency of communication
Predicting depression (PHQ-9) and anxiety (GAD-7). Higher overall scores on the Concerns about Caregiving factor predicted higher average PHQ-9 scores, indicating greater depressive symptomology (R2 = .28). Neither Caregiver concerns, nor Child concerns were significant predictors of anxiety using the average GAD-7 score (although a very large amount of variance accounted for was observed).
Discussion
The Concerns of Grieving Caregivers Scale (COGCS) is the first of its kind to measure caregivers’ concerns about their own parenting, their relations with, and specific behaviors of their bereaved child(ren). The purpose of this study was to assess this newly created scale. Results supported the factorial validity of the COGCS across two community-based samples, which consists of two factors (Factor 1: Concerns about Caregiving; Factor 2: Concerns about the Child) in two samples of grieving caregivers. The structure was consistent with its theoretical conceptualization, the Muriel et al. (2012) scale from which it was inspired, and was approved via consultation with clinicians. The COGCS demonstrated good internal consistency reliability and criterion validity in these clinical contexts.
The concerns of grieving caregivers are important to assess for several reasons. Greater awareness of the unique experiences of grieving caregivers and their concerns will inform the creation and delivery of responsive clinical supports geared towards both the caregiver and the child. Based on clinical experiences at the grief center, parents, and caregivers may access services with their children’s needs in mind without recognizing, feeling justified, interested, or comfortable seeking support for themselves. Simultaneously reflecting and compounded by these feelings, the degree of caregivers’ concerns about their own adequacy and efficacy as parents, and concerns about their children, may be both indications and symptoms of their own equally pressing needs for support with the struggles of parenting while grieving. This notion aligns with previous research (e.g., Christ & Christ, 2006; Dalton et al., 2020) and suggests that caregivers’ concerns can either mitigate or intensify their interactions with, and their access to supports for their bereaved children, ultimately influencing the grieving child’s psychosocial outcomes.
In keeping with the emphasis of the interrelatedness of parents’ concerns and their child’s wellbeing, the established two-factor structure of the COGCS partially aligned with thematic results of Muriel and colleagues’ (2012) PCQ insofar as reflecting items pertaining to concerns about the child’s behaviors/reactions and one’s own parenting evaluation. Differences existed with regard to Muriel et al.’s focus on co-parenting as one of their three factors, which makes sense within their population of parents living with cancer rather than parents who are dying, bereaved, or widowed, as was the case with our sample. Both the COGCS and the PCQ demonstrated good internal consistency reliability and validity, suggesting that both scales can be used to explore caregiver concerns about death and dying, between a broad population of bereaved parents and caregivers (i.e., COGCS) and in parents with terminal cancer (i.e., PCQ).
Other comparisons between the COGCS and the PCQ (Muriel et al., 2012) can be made. For example, Muriel et al. (2012) explored relationships between parenting concerns and anxiety and depression scores using standardized instruments such as the HADS [Hospital Anxiety and Depression Scale], in addition to scores on the distress thermometer, and functioning based on the FACT-G [Functional Assessment of Cancer Therapy—General]). Moderate correlations between the PCQ and these assessments suggest that, “being concerned about parenting issues is related to anxiety, depression, functioning, and overall distress.” (p. 5675). Expanding on these results, the COGCS was able to predict depression in our sample using the PHQ-9, but neither of the subscales predicted anxiety. Although we do not find support for the associations between the COGCS and anxiety, the sample size limitations should be noted and thus, the lack of statistically significant effect may be due to low power in that sample. Due to the similarity of some items between the COGCS and the PCQ, it may be the case that in a larger sample size our results would mirror those of Muriel et al. (2012) with the COGCS predicting both depression and anxiety. Further, we identified differences related to both caregivers’ and children’s gender, with respect to communication and concern items. In all, these findings are consistent with the minimal existing research in this area, which suggest that mothers communicate more frequently than do fathers; however, child gender did not influence the degree of communication (Christ et al., 2005).
One of the most consistent findings throughout our analyses was that caregivers tend to communicate more with younger children about grief. This is congruent with previous research about parenting and grief communication (e.g., Christ et al., 2005); however, it is also potentially problematic as it may imply an assumption about the capacity of adolescents to independently cope with grief and mourning during a developmental period where they may be particularly vulnerable to the effects of bereavement (Layne et al., 2017). In line with this, results of this study support the use of the COGCS to assess the overall level of concern that caregivers feel for their parenting relationship and for their children’s grief reactions. A mindful approach that balances parents’ realistic concerns for their child’s grief processing, as well as their own caregiving concerns would be ideal to prevent deterioration of caregiver’s mental health and wellbeing. The COGCS can be used with this purpose in mind as supporting the caregivers’ capacity and wellbeing can ultimately support the bereaved child as well (Christ et al., 2005). Our results highlight the importance of the children’s age in the context of assessing caregiver behaviors in the grieving context.
Clinical implications can be differentiated according to the two identified factors in the COGCS, as supports for grieving caregivers and supports for the grieving child reflect the complexities of caregivers’ concerns about their own caregiving and their concerns about their child, respectively. Caregivers may benefit from resources and supports addressing their prominent concerns about their caregiving and the presentation of their own mental health needs. For example, information on bereaved children’s’ behavioral and relational presentations, support for caregivers’ identified difficulties with parenting, the impact of grief on their interpersonal relationships, and strategies for fatigue/sleep difficulties may be particularly beneficial. Specific resources for male-identifying caregivers may also help address disparities related to mental health and communication. In our two samples, the COGCS was administered upon intake which continues to make clinical sense as this would be the point in time where clinicians should be aware of caregivers’ concerns. As concerns accounted for a substantial amount of the variability in depression scores, providing caregivers with resources upon intake may help to mitigate some of the more elevated mental health concerns and outcomes, such as difficulties with sleep hygiene as a result of depressive symptomatology. Further, results related to gender differences may help inform clinicians’ assessments and provision of resources that are more responsive to their clients’ unique needs and experiences.
Differences between the two samples may exist in light of the greater proportion of sudden deaths experienced by clients of the children’s center compared with the hospice, and the hospice’s support when the death is outside of the child’s immediate family. These differences may reflect or contribute to different combinations of factors, barriers to access and other resources for clients of the two agencies, and subsequently, different parenting experiences and concerns. Nonetheless, the common focus on supporting grieving children, youth and their families and the similarities in their community contexts created a rich opportunity for collaboration and data generation. As such, the similarities between the models resulting from analyses with the hospice and grief center samples suggest both that this measure is relevant in multiple contexts with minor modifications to the wording to suit the specific population (i.e., “sick” and/or “dying”), and also that the factor structure may be stable across these contexts. Broadly, this suggests that the COGCS has utility in a variety of clinical samples to explore parents’ and caregivers’ concerns for themselves and for their grieving children across the trajectory of illness and death. Clinicians may find the results of this scale relevant for their therapeutic endeavors with clients, and may be able to integrate concern-specific resources into their practice. This measure may also be useful as a self-assessment by caregivers supporting children who are grieving a serious illness, dying or death, and may offer valuable opportunities for reflection, particularly if used over time. Future replication of these analyses is warranted to better understand its utility and relevance for families from diverse cultural backgrounds and geographic locations.
Limitations
Although a large sample was used for data collection, several important sociodemographic characteristics were not obtained. Notably, ethnicity and the relationship between the child and the person who was ill/dying/died were collected separately by the Hospice as an unlinked data set in order to maximize confidentiality in the completion of an online form. Details about the relationship between the dying/deceased person and the child would have illuminated additional relational impacts for the bereaved child and caregivers. Including participants’ identified ethnicity in the analyses would have enabled the beginning of a crucial examination of potential differences in concerns, in light of respondents’ ethnicity and racial inequities in the health and social systems. Further restricting our sample is the fact that the current survey was administered to English speakers and the likelihood of a selection effect by virtue of the availability, voluntary nature, and location of service organizations. As such, the generalizability of these results to non-clinical samples of individuals who have not sought out or received ongoing grief supports may be limited. Future work should investigate the factorial validity of this scale in a general community sample of grieving families from a variety of ethnic and socio-economic backgrounds, speaking a range of languages. Additionally, future research should investigate construct validity and if COGCS subscales are receptive to change via clinical intervention. Only having depression and anxiety data from the smaller sample means that inferences from this study regarding the effects of concerns on these important mental health outcomes may not be reliable and should be an aim of future research. Lastly, it is important to note that direct comparison between the community center and hospice samples is difficult because of the fundamentally different contextual factors between the two and the differing sample size (favoring the community hospice and the statistical inferences from that sample).
Conclusion
Understanding the concerns of bereaved caregivers is valuable within clinical settings that provide support to grieving families, as well as within the academic literature. As caregivers’ concerns can either mitigate or intensify their interactions with, and their access to supports for their bereaved children, this ultimately influences the grieving child’s psychosocial outcomes, as well as those of the caregiver. Examination of the newly generated Concerns of Grieving Caregivers Scale (COGCS) across two samples, a hospice and a community grief center, provided preliminary support for construct and criterion validity, as well as internal consistency reliability. The scale likely has utility in both clinical and non-clinical academic contexts, to promote the advancement in our understanding of the concerns that grieving caregivers may have, and how these concerns may influence their own and their child(ren)’s emotional wellbeing.
Supplemental Material
sj-pdf-1-ome-10.1177_00302228211053062 – Supplemental Material for Development and Psychometric Evaluation of the Concerns of Grieving Caregivers Scale (COGCS) with Two Clinical Samples
Supplemental Material, sj-pdf-1-ome-10.1177_00302228211053062 for Development and Psychometric Evaluation of the Concerns of Grieving Caregivers Scale (COGCS) with Two Clinical Samples by Samantha O’Leary, Christopher Quinn-Nilas, Victoria Pileggi and Ceilidh Eaton-Russell in OMEGA-Journal of Death and Dying
Footnotes
Acknowledgements
We would like to express our profound gratitude for the significant contributions of the intake, clinical and research teams from Heart House Hospice and Dr Jay Children’s Grief Centre for their central roles in data collection for this study, and for the crucial clinical supports that they provide with grieving families.
Author’s Note
Samantha O’Leary: Formal analysis, Data curation, Writing—original draft preparation, reviewing and editing, Investigation, Project administration. Christopher Quinn-Nilas: Formal analysis, Writing—original draft preparation, reviewing and editing, Methodology. Victoria Pileggi: Conceptualization, Methodology, Resources, Writing—reviewing and editing, Investigation. Ceilidh Eaton Russell: Conceptualization, Methodology, Resources, Writing—original draft preparation, reviewing and editing, Project administration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.