
Abstract
The sources of judicial dissatisfaction with, and criticism of, expert healthcare evidence are traced to unqualified, careless, overworked and unscrupulous experts and a failure on the part of some experts to work collaboratively with their instructing lawyers during the litigation process. The suggested remedies are: adherence to the clear professional standards that already exist, appropriate training for which the foundations should be laid during undergraduate medical education, continuing professional development, credentialing complemented by instructing solicitors and counsel ensuring that the expert is appropriate for the case and aware of their duties, collaborative working between expert and instructing lawyer, peer and institutional support and quality control including peer review of reports and case-based discussion of reports.
Keywords
Most healthcare professionals called upon to assist courts and tribunals with expert evidence fulfil this public duty competently. However, published judgments of courts and tribunals, in the United Kingdom generally, Jersey and the Republic of Ireland, reveal that a small number of healthcare experts cause judicial dissatisfaction and incur judicial criticism. Rix (in press 1 ) has identified those aspects of expert witness practice which have repeatedly caused such judicial concern. The purpose of this article is to explore how such concerns arise and suggest how they may be avoided.
In his 2011 Macfadyen Lecture, The Honourable Thomas A. Cromwell, a former Puisne Justice on the Supreme Court of Canada, said
2
: Clear professional standards, appropriate training, credentialing and quality control for expert witnesses have the potential to address more directly the sorts of problems that arise from the evidence of unqualified, careless, overworked or even unscrupulous experts.
Cromwell's reference to unqualified, careless, overworked or even unscrupulous experts goes a long way to explaining why and how expert healthcare experts have caused judges to be dissatisfied and have sometimes incurred judicial criticism.
The reasons for judicial dissatisfaction with, and criticism of, expert healthcare witnesses
The unqualified expert
Being qualified to act as a healthcare expert does not mean holding some sort of expert witness qualification or even having some particular clinical qualification. It means having sufficient skill, acquired through education, training or experience, to assist the court (R v Bunnis (1964) 50 WWR 422 3 ; Myers v The Queen [2015] UKPC 40 4 ). If the skill is insufficient, notwithstanding the person's education, training or experience, they do not qualify as an expert.
The qualification to give expert evidence is issue-specific. When the Court of Protection refused to admit the evidence of a physician in a COVID vaccination case (North Yorkshire Clinical Commissioning Group v E (Covid Vaccination) [2022] EWCOP 15 5 ), one of the reasons was that he ‘did not have any specialisation in virology, epidemiology, or any other field of practice that would be recognised as relevant to the issues that the court has to determine in this case’ (author's italics for emphasis). Relevance has a strict legal meaning derived from the sixteenth century Scots legal term meaning ‘legally pertinent’. 6 It must be logically probative or disprobative of something which requires proof; evidence which makes the matter requiring proof more or less probable (DPP v Kilbourne [1973] AC 729 7 ). A gynaecologist may have the knowledge and experience to assist in a gynaecological oncology case, but not be qualified to assist in a urogynaecology case.
The careless expert
Carelessness is one explanation for inaccuracy. It may also lie behind unclear reasoning, the misapplication of literature, absent or insufficient triangulation with medical or other records, failure to follow instructions or address issues, inadequate referencing and misuse of guidance. Overwork may also be responsible for some of these and, of course, manifest in carelessness.
The overworked expert
Overwork was clearly identified as a problem with the evidence of a histopathologist in London Borough of Hammersmith and Fulham v G [2024] EWHC 2200 (Fam) 8 (Hammersmith). This was a case in which there were issues related to rib fractures found at the post mortem examination of an infant who had died after she became entangled around her neck by a decorative scarf tied in the lower bars of a bunk bed. The expert missed a deadline for filing a report and, towards the end of his evidence, the court sensed that the reason was the number of cases with which he had to deal. He dealt with only the most pressing matters, those which were on the immediate horizon. It was with great regret that the court was left with a very real sense of an expert who was overburdened with work, who had thus made errors in his examination of the forensic material and who had closed his mind to possible or probable accidental causes for the injuries identified. It was with the greatest reluctance that the judge found himself unable to accept his opinions and conclusions. The judge recognised that he is, or was at the time, currently the only forensic consultant histopathologist accepting instructions in cases of suspicious death and/or alleged inflicted injuries in the United Kingdom. The consequence of this state of affairs, however, was that he had a huge workload. The court recognised that he is a highly respected and hugely experienced histopathologist. The judge had had the benefit of receiving his expert reports in many cases over the years and evidence which he had accepted. However, in this case, the court found that he had fallen below his own high standards as a forensic expert witness.
Hammersmith was a family court case and it was the shortage of medical experts willing to assist the Family Court that led the Family Justice Council to set up a ‘Working Group on Medical Experts in the Family Court’ to investigate the problem and make recommendations. It carried out a survey and identified the main factors acting as barriers or disincentives to acting as an expert witness as remuneration, court processes, lack of support and training, and perceived criticism by lawyers, judiciary and the press. 9 Lack of support may be on the part of NHS employers who make it difficult or impossible for doctors to engage in expert witness work and on the part of medical royal colleges and faculties.
The unscrupulous expert
One of the earliest descriptions of the ‘hired gun’ is in Lord Abinger v Ashton (1873) 17 LR Eq 358, where Sir George Jessel, the Master of the Rolls, said
10
: [U]ndoubtedly there is a natural bias to do something serviceable for those who employ you and adequately remunerate you. It is very natural, and it is so effectual that we constantly see persons, instead of considering themselves witnesses, rather considering themselves as paid agents of the person who employs them.
Although Lord Woolf's civil justice reforms, which came into effect on 26 April 1999, with the introduction of the Civil Procedure Rules (CPR) for the High Court and county courts in England and Wales, have to a large extent driven the hired gun out of town, it is clear that some healthcare experts see themselves as hired guns and some unashamedly so. Given that such behaviour is fundamentally contrary to the primary duty of the expert being to the court, and not to the party instructing them, it is entirely appropriate to label such behaviour as unscrupulous. More than unscrupulous, and as the Medical Practitioners Tribunal has found, it is dishonest to seek to influence the outcome of a case by fabricating evidence or seek to mislead the court by giving false evidence as to the duration of an assessment (Moodliar v General Medical Council [2025] EWHC 913 (Admin) 11 ).
The reasons for such unscrupulous and dishonest behaviour on the part of expert healthcare witnesses are complex and probably ones that explain other forms of unscrupulous and dishonest behaviour by doctors. Writing more than 40 years ago about the problem of the irresponsible or unscrupulous expert witness in the United States, a paediatrician who specialised in congenital malformations, said that 12 : The educational community also bears some responsibility for the phenomenon of the irresponsible expert witness.
A failure of collaboration
A common factor probably connects a number of these aspects of expert practice. There is much more to being a medical expert witness than providing an expert report and then, if at all, turning up to court to give oral testimony. Acting as a healthcare expert witness is best regarded as a process and ‘justice will be best served if there is a close collaboration between a healthcare specialist and a lawyer from as soon as the need for expert evidence is appreciated and thereafter through the litigation process’ 13 .
In Hepworth v Coates [2025] EWHC 1907 (KB) 14 (Hepworth), the expert in neurological rehabilitation instructed by the claimant stated during cross-examination that he did not have the claimant's witness statement when he prepared his report, nor when he met with the defendant's expert and when their joint statement was prepared. In fact, he was only provided with it a few days before the trial. The court said that it was not his fault if he was not provided with the witness statements and other reports, and so by implication it was the fault of his instructing solicitors, but that he did not ask to see them before finalising his report was regarded by the court as a serious omission.
As Hepworth illustrates ‘it takes too to tango’ and a failure of collaboration may be entirely the fault of the legal professionals. An anonymous reviewer of this article observed that ‘last minute-ism’ – the provision of critical material immediately before a hearing – is too commonly an issue in expert witness practice and there are occasional lawyers whose engagement with the expert is not much more than a simple nod as the expert goes into the witness box.
Righting the wrongs
Cromwell 15 has called for clear professional standards, appropriate training, credentialing and quality control for expert witnesses to address more directly the problems with expert evidence. To these can be added support and continuing professional development.
Clear professional standards
Standards of expert witness practice are most highly codified in England and Wales, principally in the procedural rules and practice directions of the different jurisdictions. However, as these rules and practice directions are rooted in case law that is influential in the jurisdictions of the other countries that make up the British Isles, this means that they are standards likely to be applied throughout the British Isles and also in other common law countries. For medical professionals these standards are also reflected in the General Medical Council's (GMC) Providing Witness Statements or Expert Evidence as Part of Legal Proceedings 16 (PWSEE) and, to a lesser extent, in the Irish Medical Council's Guide to professional conduct & ethics for registered medical practitioners. 17 They are also reflected in generic codes of practice or guidance, such as the Joint Code of Conduct of The Academy of Experts (TAE) and the Expert Witness Institute (EWI) 18 and the speciality guidance of medical royal colleges and faculties and medical professional associations.
For a medical expert there can be nothing clearer than the GMC's statement that ‘you must …’. Equally clear, but permitting a properly reasoned disregard in certain circumstances, is the statement ‘you should …’.
By way of example, a common reason for criticising healthcare experts is for being partisan (Rix, in press
19
). One explanation is suggested by an anonymous reviewer of this article who referred to the risks associated with the expert's own temperamental characteristics and the fact that some people are natural ‘prosecution experts’ and others natural ‘defence experts’. The Guidance for the instruction of experts in civil claims
20
states: Provide opinions which are independent, regardless of the pressures of the litigation. Useful test: the expert would express the same opinion if given the same instructions by another party. Do not promote the point of view of the instructing party or engage in the role of advocate or mediator.
An expert may not be able to change their personality any more than a leopard its spots but trying to achieve an equal balance of claimant/defendant or prosecution/defence cases can mitigate its effects. Although in criminal cases, because the prosecution often only instructs experts in response to cases advanced by the defence, it may be difficult to achieve a balance but in civil cases this can be achieved by having separate claimant and defendant waiting lists. The importance of such balance is reflected in how often it is the subject of a question at the beginning of examination-in-chief or cross-examination.
Appropriate training
In the Family Court it is a requirement that an expert has undertaken appropriate training.
21
The foundations for expert witness training should be laid during undergraduate medical education
22
: ‘Few medical schools, residencies, or graduate schools prepare their graduates for participation in the judicial process […] The role of the expert witness should be taught in medical and graduate school. Testimony should be treated as a scholarly endeavor […].’
Expert witness training is widely available in the British Isles. Generic training provided by organisations, such as Bond Solon, with its links to Aberdeen University and Cardiff University, and Ireland's Expert Witness Site, and expert witness bodies such as TAE and the EWI has the advantage that healthcare experts can learn from experts from outside healthcare. If a healthcare expert's report cannot be understood by a gemmologist or forensic entomologist, it may not be understood by a judge and there will be a question as to whether a jury will understand evidence based on it.
But appropriate training means at least appropriate to the jurisdiction in which the evidence is to be given and appropriate to the expert's healthcare specialty. Again expert witness organisations and bodies can train experts about the requirements of different jurisdictions. Medical royal colleges and faculties and medical professional associations also provide training for different healthcare specialists. Allam 23 has not only described such training for psychiatrists in Scotland but demonstrated objectively how it results in psychiatrists being much more confident about undertaking expert witness work.
Unsurprisingly an anonymous reviewer of this article observed that there are limitations on what training courses can offer or how much they will really help. They say that their own experience in medico-legal work is that the expert largely learns by doing and virtually every psychiatric expert to whom they have ever spoken on this topic has said the same. There is now a diminishing cohort of healthcare experts who had no choice but to learn by doing and also to learn from their mistakes, a cohort that includes some who competently assist courts and tribunals with evidence of the highest quality without having had any, or more than a little, formal training. So, what is the value of training?
A common reason for judicial criticism is ignorance or failure to comply with procedural rules and guidance. 24 In Hamed v Ministry of Justice (Cambridge County Court, 7 June 2024, unreported), 25 the judge urged an orthopaedic expert to undertake some further training in expert report writing to ensure that he fully understands his obligations and duty to the court. Compliance with procedural rules and guidance must be in spirit as well as words. In Bolitho v City and Hackney Health Authority [1998] AC 232, 26 Lord Brown Wilkinson said that ‘A “responsible” expert is one [..] who adheres to the spirit as well as the words of his professional declaration’.
Although some healthcare experts, such as paediatricians, pathologists and psychiatrists, gain experience of giving oral testimony relatively early, often in their higher training, there are some specialisms whose experts can wait decades for their first experience of oral testimony. So, cross-examination training can be of value for even experienced healthcare experts.
There is no requirement as to how often training should be repeated but, in a report for the Royal College of Pathologists and the Royal College of Paediatrics and Child Health, prepared by a working group convened by Baroness Helena Kennedy KC, 27 it was recommended that judges should establish whether the expert has received training in the role of the expert witness in the past 5 years.
Continuing professional development
Cromwell does not mention continuing professional development (CPD) but there is a requirement in the Family Court to undertake not only appropriate training but also appropriate updating. 28 The GMC in PWSEE cross refers to its Good Medical Practice and states: ‘You must keep up to date with guidelines and developments that affect your work’. 29 It follows that healthcare experts should have plans for CPD that encompass not only the updating of the professional knowledge and skills for their clinical practice but also the experience and knowledge necessary to act as an expert witness.
Credentialing
Credentialing is the process of ascertaining that someone is competent to perform a particular role. In the field of healthcare, most if not all healthcare experts will have evidence of their competence as a healthcare professional in a particular area of practice by virtue of being registered with, and in some cases also licensed by, a healthcare regulator such as the GMC or the Health and Care Professions Council (HCPC). The acid test is clinical experience. ‘When, doctor, did you last see a patient with this condition in your clinical practice?’ Simon Britten, an orthopaedic surgeon, says that lawyers want the expert to smell of the operating theatre. 30
However, a healthcare expert has to be competent to perform not only their role as a healthcare professional but their role as an expert witness. The expert's role is to assist the court. A healthcare professional may have a wealth of knowledge and experience but if they cannot write a report that is admissible in evidence and carries sufficient weight and give oral testimony that stands up to testing, they may be of little or no assistance to the court or even confuse the court and risk a miscarriage of justice. In Hepworth, 31 the unfortunate consequence of the neurorehabilitation expert's failings, was that although, in theory he was the more suitable expert to opine on the claimant's neurological rehabilitation, including both prognosis and further needs, and his experience made him potentially better suited to opine on such matters generally than the defendant's expert, the court concluded that it was unfortunate that it could not rely on his evidence. He failed to assist the court.
Recognised credentials include accreditation or certification by a recognised expert witness body, such as TAE or the EWI, or certification by a reputable expert witness training organisation, such as Bond Solon.
The potential expert must ask himself or herself, and honestly answer, the question: ‘Do I have sufficient familiarity with and knowledge of the field in question to render my evidence potentially of value in resolving any of [the] issues?’ (Davies v Ford [2020] EWHC 3063 (Ch) 32 ). However, there is a complementary and clear obligation on an instructing solicitor and counsel to ensure that the expert is appropriate for the case and aware of their duties (Kennedy v Cordia (Services) LLP [2016] UKSC 6 33 ).
Credentialling is not to be confused with the registration and regulation of experts about which there have been discussions. They risk expert healthcare witness work becoming increasingly confined to a limited number of experts who achieve registration and submit to regulation and who may then be under pressure, or tempted, to offer opinions on matters that are not within their expertise if a suitable expert cannot be found. This is not to say that professional bodies should not hold lists of members willing to offer expert evidence. Healthcare experts are already regulated by the GMC and HCPC.
Working collaboratively
Without joining the litigation team or becoming, as the parties are, partisan, it is incumbent upon both the expert and the instructing lawyers to work collaboratively and for experts to be prepared to take a proactive role. Such collaboration includes, but is not limited to, negotiation of instructions; clarification of instructions, issues and the expert's field of expertise; making sure that the expert understands and applies appropriately any legal test; keeping the expert informed of developments with witness evidence, including other expert evidence and ensuring that, if necessary, the expert's own evidence is updated; ensuring the report complies with procedural rules and that the opinions are satisfactorily explained; identification by the expert of any missing evidence, particularly medical records and witness statements; ensuring that the expert's sources are cited and cross-referenced sufficiently for the court readily to identify and locate the facts or literature on which the expert is relying; and ensuring that the expert is aware during the trial of procedural or evidential developments, which may include a requirement for the expert to hear evidence or consider transcripts thereof.
Peer and institutional support
Expert healthcare witnesses often tread a lonely furrow. Cases can be emotionally and intellectually demanding. It can be helpful to belong to a medico-legal peer group. There is mutual support. Ideas about education and training can be discussed. Personal development and CPD plans can be approved. The group can be a forum for case-based discussions and ‘in-house’ case presentations and talks.
Support is also required from employers and professional bodies. Recommendations of the FJC Working Group included
34
: “Royal Colleges could consider appointing a lead clinician/officer for expert witnesses.” “Encouragement to the Royal Colleges/Professional bodies to engage with commissioners and or trusts to promote a more supportive environment to medical professionals […] who wish to undertake expert witness work.” “The Royal Colleges […] and the FJC to engage with NHS England and clinical commissioning groups to seek changes to contracting arrangements to enable healthcare professionals to undertake expert witness work within the parameters of their employment contracts.”
Although assisting the delivery of justice is a doctor's public duty 35 not all healthcare professionals are suitable or able to do so. This means that it is incumbent upon employers and professional bodies such as the medical royal colleges and faculties to ensure that there are sufficient healthcare professionals to fulfil this duty competently and with necessary expedition. The failure of all but a few of the colleges and faculties to appoint an expert witness lead indicates that more is to be done to ensure that they provide the support that their members need.
Quality control
Again it is the Family Court which is most prescriptive. Standard 9 of the Annex to FPR 25 BPD, 36 with which experts must comply, states: ‘The expert has undertaken appropriate training, updating or quality assurance activity – including actively seeking feedback from cases in which they have provided evidence – relevant to the role of expert in the family courts in England and Wales within the last year.’ Even in the Family Court, where experts can expect to receive a copy of judgments in cases in which they have provided evidence, it is not enough to receive and file away a copy of the judgment.
Although feedback can be obtained upon conclusion of a case by writing to instructing solicitors, what is often more informative is multi-source feedback obtained anonymously from a number of the professionals involved in the case: instructing solicitor, the instructing party's counsel, solicitors and counsel acting for the other party/ies, other experts and, if oral testimony is given, the judge. If feedback is provided by only one respondent, to protect the respondent's identity, it can still count towards cumulative feedback. ‘Multi-source Assessment of Expert Practice’ 37 is an example of multi-source feedback designed specifically for expert witnesses. Feedback domains are: Professionalism/Professional demeanour; Ethics; Skills; Reliability of opinion; Presentation of opinion/report; Understanding of law, procedure and rules of evidence; Oral testimony; and Business manners and affairs.
MAEP does not provide a means of obtaining feedback directly from the subject of an expert assessment. There is provision for subject feedback to be obtained indirectly through the subject's legal representative or another feedback participant, such as a barrister. The reasons for not incorporating direct subject feedback are legal, empirical, ethical and practical, as explained on the MAEP pages of the Royal College of Psychiatrists’ website. 38
Another form of quality control is peer review of expert reports. ‘[E]xperts should be encouraged to seek peer review of their opinions and not to testify secretly and in isolation’. 39
Peer review before a report is finalised has to comply with two important judgments. Pinkus v Direct Line Group [2018] 1 WLUK 3 40 requires an expert to disclose the fact and nature of any discussion of ‘the content of a proposed report in detail with another expert under a peer review arrangement’. This only applies where the peer provides ‘constructive input’; it does not apply to proof-reading. R v Pabon [2018] EWCA Crim 420 41 permits an expert to research a topic to enhance their existing expertise by obtaining ‘the views of others, including work colleagues, so long as he records where he went for that advice’. In OXR v Mid and South Essex Hospital NHS Foundation Trust [2023] EWHC 2006 (KB) 42 an ear, nose and throat surgeon was judged to be ‘vulnerable to challenge on the grounds that he had sought the views of unidentified colleagues and allowed them to inform his opinion on breach of duty’. The key is to avoid a detailed discussion of the case and ensure that the peer reviewer has no constructive input into the case. If, as might happen, the peer reviewer identifies a need for a detailed discussion or considers it advisable to provide constructive input, this should be recorded and the peer reviewer identified.
Peer review that takes place after the case is concluded can take the form of a case-based discussion either on a paired or group basis. The pairing system was developed at The Grange Consulting Rooms, Cleckheaton, West Yorkshire. 43 An even number of experts are randomly paired twice, but without the same two experts being paired together twice. The first-named expert in each pair provides the second-named expert with a copy of a report along with usually nothing more than the letter of instruction. Choice of the report can be delegated to the expert's personal assistant who is asked to select a case randomly. At the peer review meeting, scheduled for 2 hours, each expert spends an hour providing a critique of the other expert's report and an hour being provided with a critique of their own report by a different colleague.
The results of the discussion are set out on an evaluation form that allows the expert and their report to be rated on the items listed in Table 1. Some items are rated on a three-point scale: ‘Requires attention/improvement’ – ‘Adequate’ – ‘An example to others’. For others, it is a two-point scale. For example, it is or it is not within their expertise.
Items rated in case-based discussion of an expert report.
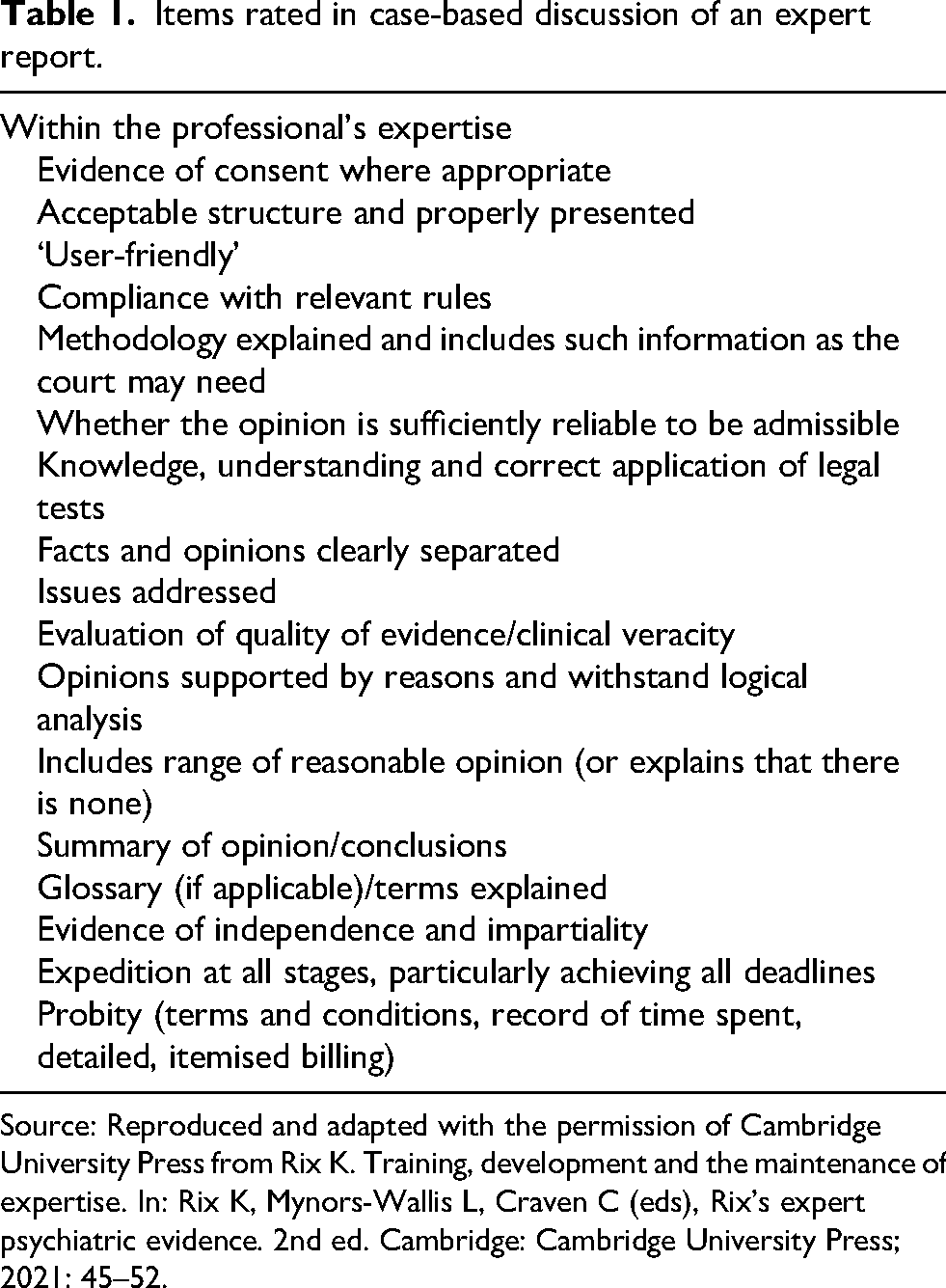
Source: Reproduced and adapted with the permission of Cambridge University Press from Rix K. Training, development and the maintenance of expertise. In: Rix K, Mynors-Wallis L, Craven C (eds), Rix's expert psychiatric evidence. 2nd ed. Cambridge: Cambridge University Press; 2021: 45–52.
This is a formative experience with emphasis on improvement and the pursuit of excellence. It is not a pass/fail test. The free text section of the form begins with ‘Good practice’; it starts with the most positive and affirming outcome. It then moves on to: ‘Suggestions for improved practice’. When these sessions are incorporated into a conference with a plenary session, or followed by an experts’ meeting, examples of good practice can be collated and difficulties discussed. However, the content of the discussions is confidential between the evaluator and the evaluee. The forms are signed by both the evaluator and the evaluee.
Spoto has described how eight experts were brought together for regular CBDs. 44 He says that their meetings were soon used by members to discuss matters of mutual interest and so the group evolved into a peer group.
Healthcare professionals who are subject to appraisal, or such other performance assessment that informs revalidation or relicensing, can incorporate the results of their multi-source feedback and case-based discussions in their appraisal or performance review submission.
Conclusion
The causes of judicial dissatisfaction with, and criticism of, healthcare experts and their evidence reflect failings on the part of individual healthcare professionals who may be unqualified, untrained, insufficiently knowledgeable to assist as to the issues in the case, overworked or even unscrupulous or dishonest. They may reflect failings on the part of their peers to provide support, mentoring or supervision. They may reflect failings on the part of employers to understand that healthcare professionals have a public duty to assist in the delivery of justice, including in cases brought against healthcare services, and who consequently limit or even prohibit their employees from undertaking expert witness work. They may reflect failings on the part of medical royal colleges and faculties sufficiently to prioritise their specialism's role as a source of expert assistance to courts and tribunals. They may reflect a failure on the part of university undergraduate and postgraduate medical schools to introduce students and trainee doctors to the duties and responsibilities of acting as an expert healthcare witness.
The remedies for these failings require healthcare professionals to undergo training as expert witnesses, adhere to their duties and discharge their responsibilities as experts, including acting only within their field of expertise, obtain and provide peer support, and engage in quality control. Medical royal colleges and faculties and healthcare providers need to be more aware of the importance of supporting members or employees in their expert witness practice and of their obligation to assist in ensuring that there are sufficient experts from their specialism to fulfil their duties to the court when assistance is required from their specialism. University medical schools, and other educational institutions, must be prepared to lay the foundations to ensure that every healthcare professional is aware of their profession's duty and sufficient are competent and willing to discharge that duty.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author designed the feedback tool Multisource Assessment of Expert Practice which is available on subscription from the Royal College of Psychiatrists but he has not received, and does not receive, income from it. He is grateful to the anonymous reviewer of this article for his comments and with whom he would have gladly shared authorship.