
Abstract
The majority of healthcare professionals discharge satisfactorily their civic duty to aid the execution of public justice by assisting courts and tribunals and may have their assistance gratefully acknowledged in a judgment that is on the public record. However, the conduct of a minority causes judicial dissatisfaction and sometimes criticism. The British and Irish Legal Information Institute (BAILII) online resource for the period September 2019 to August 2025 has been used to identify such cases. Examples are given of healthcare expert practice which have repeatedly caused concern: absent, insufficient or unclear reasoning; misuse, or failure to cite, literature; inaccuracy; failure to triangulate self-reported history with other evidence; failure to keep up with evidence; inappropriate language; late introduction of evidence; disregard, omission or misrepresentation of instructions; inadequate treatment of issues; failure to comply with procedural rules and guidance; partisanship; absent or inadequate referencing; incomplete range of opinion; misunderstanding of legal test; ignorance or disregard of procedural rules or guidance; disregard of, or challenge to, previous factual findings; acting outside expertise; omitting evidence that undermines opinion; unwillingness to make reasonable concessions; misuse of, or failure to refer to, relevant clinical guidelines; criticism of other experts; and dishonesty. Expert healthcare witnesses whose conduct results in judicial dissatisfaction or criticism appear to be unaware of, or to misunderstand, the duties of an expert witness or to act in disregard of them.
An eight-month old boy suffered a multi-focal subdural haematoma (A (Child: Fact Finding Hearing) [2025] EWFC 219 (B)
1
). In subsequent Family Court proceedings, the court received expert medical evidence and the parties agreed the child was the victim of a ‘shaking’ event. In his judgment, His Honour Judge Willans said: The Court has received expert evidence from a haematologist, neuroradiologist, neurosurgeon and paediatrician […] There was no suggestion of dogmatism on the part of any expert witness and they demonstrated a willingness to be flexible in their thinking considering other potentials. I am grateful to each of these witnesses for helping me. Without such experts the Family Court could not function. My judgment should be copied to them as per the Rules.
Every month in the British Isles a judge makes a similar comment, echoing Dame Elizabeth Butler-Sloss who said, writing in the Journal of the Royal Society of Medicine: ‘Expert witnesses are a crucial resource. Without them we [the judges] could not do our job’. 2
Doctors, and other healthcare professionals, who provide such evidence fulfil what an early 19th century medical ethicist described as an office, ‘required from them as citizens qualified by professional knowledge, to aid the execution of public justice’.
3
Not many years before, Dr Andrew Duncan Senior, in his ‘Heads of lectures on medical jurisprudence’ at Edinburgh University had written
4
: Many questions come before the Courts […] where the opinion of medical practitioners is necessary either for the exculpation of innocence or the detection of guilt […] an opinion consistent with truth and with justice.
The nature and scale of this indebtedness is the important context in which to consider judicial criticism of healthcare experts and dissatisfaction falling short of actual criticism.
At one end of the range is dissatisfaction or criticism such as in Palmer v Mantas [2022] EWHC 90 (QB) 5 (Palmer). The court acknowledged counsel's powerful observation that adverse criticism of a pain management expert might have a ‘career-damaging effect’. But the judge said that he had absolutely no desire to do that; he hoped that the necessary criticism could be limited to that particular case. In Hamed v Ministry of Justice (Cambridge County Court, 7 June 2024, unreported) 6 (Hamed), the judge urged an orthopaedic expert to undertake some further training in expert report writing to ensure that he fully understands his obligations and duty to the court. At the other end of the range is such serious criticism that it results in erasure from the General Medical Council's (GMC) Medical Register.
The purpose of this study was to identify aspects of expert healthcare witness practice which repeatedly result in adverse judicial comment or criticism.
Methods
The British and Irish Legal Information Institute (BAILII) online resource was used to identify reports of cases decided by courts and tribunals, in the United Kingdom generally, Jersey and the Republic of Ireland between September 2019 and August 2025, in which expert evidence was given. This search was supplemented by consideration of a small number of judgments in unreported cases provided to the author by lawyers and experts.
Results
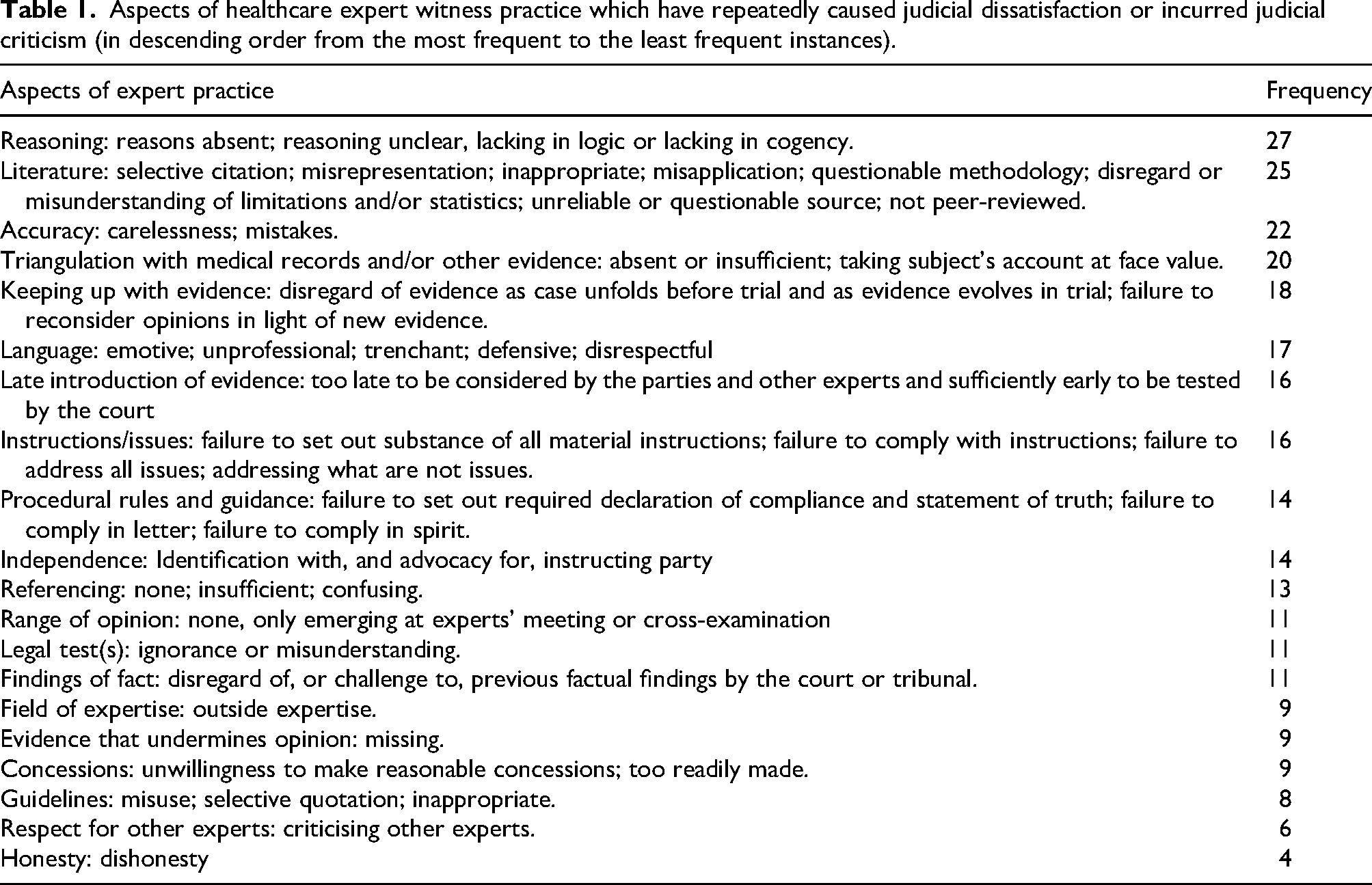
This was a quantitative study only insofar as its focus was on aspects of expert healthcare witness practice that were more than once of concern during the study period. Frequency figures are included in Table 1 to give an impression of what most commonly, and what least often, result in judicial criticism.
Aspects of healthcare expert witness practice which have repeatedly caused judicial dissatisfaction or incurred judicial criticism (in descending order from the most frequent to the least frequent instances).
Illustrative cases
Each unsatisfactory aspect of expert practice is now illustrated by reference to what is expected of experts. There is some overlap.
Reasoning
Courts make findings of fact. To do so, they not only have regard to an expert's opinion but the reasons for it because ‘[p]roper evaluation of the opinion can only be undertaken if the process of reasoning which led to the conclusion, including the premises from which the reasoning proceeds, are disclosed by the expert’ (Coopers (South Africa) (Pty) Ltd v Deutsche Gesellschaft für Schädlingsbekämpfung mbH, 1976 (3) SA 352). 7 ‘If the reasons stand up, the opinion does. If not, not’ (Pearce v Ove Arup Partnership Ltd (Copying) (2002) 25(2) IPD 25011). 8
A vascular surgeon was criticised in Kennett v East Kent Hospitals NHS Foundation Trust (Canterbury County Court, 31 July 2018, unreported) 9 for failing to provide reasons. When his answers to questions were unacceptably terse in Beatty v Lewisham and Greenwich NHS Trust [2023] EWHC 3163 (KB) 10 (Beatty), the judge said that the obligation to provide reasoning ‘exists even if the reasons seem blindingly obvious to the maker of the opinion’.
Literature
The expert has a duty to consider published literature in their specialism (R v Abadom [1983] 1 WLR 126 11 ). In Jarman v Brighton and Sussex University Hospitals NHS Trust [2021] EWHC 323 (QB) 12 , an orthopaedic expert was found to be ‘unconvincing when challenged for failure to cite any literature […] in support of propositions which could and should have been supported in that way’. In Pelosi v Lanarkshire Housing Association Ltd [2024] ScotCS CSOH 56, 13 where a toxicologist's conclusions were not underpinned by appropriate reliance on relevant literature, the court concluded that the adverse party's toxicology evidence was of greater force.
In Jones v Ministry of Defence [2020] EWHC 1603 (QB), 14 a case concerning a delay in the diagnosis of the claimant's HIV status, a medical epidemiologist referred to a ‘short paper’ by ‘ Stevens et al’ in the Journal of the American Medical Association (JAMA), which he described as the world's ‘number two medical journal […] It's very prestigious.’ The judge acknowledged JAMA's status but found that the document relied upon was not however an academic paper, let alone the type of peer-reviewed study upon which JAMA reputation is founded. Rather, it was a one-page document ‘HIV Infection: The Basics’ on the ‘JAMA patient page’; in medical publication terms, the antithesis of a peer-reviewed study. To describe it as a ‘paper by Stevens et al’, emphasising JAMA's prestigious standing, the judge said, was to seek to give an impression of its status neither its single author (Stevens), nor JAMA, could possibly have intended. That this was one of the key ‘papers’ relied upon by the expert did nothing to strengthen the robustness of his conclusions. His attempts to elevate its importance did little to instil confidence in his analysis of the epidemiology generally.
Accuracy
The GMC states: ‘You must make sure any statement or report you write, or oral evidence you give, is accurate and not misleading’. 15
In AME (Egypt) v Secretary of State for the Home Department [2024] UKAITUR UI2024002449, 16 it appears that the expert's report stated that the appellant's partner had said that the appellant had been ‘stabbed’ by members of the Muslim Brotherhood. The FIrst-tier Tribunal (F-tT) rejected that evidence and appeared to draw a significant adverse inference from the fact that the appellant had no scars to corroborate this. However, the appellant nowhere said that she was ‘stabbed’; she said that she was ‘attacked’ by the Muslim Brotherhood. The Upper Tribunal therefore found that the F-tT was likely led astray by a less than clear passage in the expert report.
In Re AA (Re Children Act 1989) [2023] EWFC 278, 17 the advocates pointed out a number of factual errors in a clinical geneticist's report and had to ask him to clarify if he was absolutely certain that he had properly checked his opinion in light thereof. One matter of concern was that he appeared to be confused as to the status of the paediatric expert, describing her as the treating paediatrician at the local hospital, and asserting that he had read her report, although it had not been filed until after the date of his report.
In Beatty 18 the expert vascular surgeon confused two doctors, which, the judge said, should not happen in expert clinical negligence reports.
In the case of a prisoner who was stabbed multiple times by another prisoner with a kitchen knife, causing an incomplete spinal lesion at T5 to T7 (Wilson v Ministry of Justice [2024] EWHC 2389 (KB) 19 ) (Wilson), a spinal surgeon made errors about prognosis in the experts’ joint statement. He also had to accept that his statement in his report that ‘I did not find [Mr Wilson] to have any balance or weakness issues’ was a mistake, given that he had consistently reported Mr Wilson as having poor balance.
Triangulation
In Berry v McCowans Ltd [2005] ScotCS CSOH 66, 22 it was submitted that ‘any orthopaedic surgeon producing a proper objective report, would have gone through the GP and medical records in detail to describe the history of the case and, where appropriate, compare the evidence therein with the account given by the patient’.
The immigration and asylum case JMPS v Secretary of State for the Home Department [2022] UKAITUR PA018492019 23 (JMPS) illustrates the failure to triangulate. There was simply no engagement at all by the psychiatric expert with the medical records. Instead, he accepted without question the appellant's claim to have engaged with his general practitioner and been prescribed regular psychotropic medication, despite it also being contrary to the medical records available. His credibility was significantly undermined.
Keeping up with evidence
When Wells Harbour silted up in the 18th century, there was objection at the subsequent legal proceedings to a marine engineer giving evidence because he was ‘going to speak, not to facts, but as to opinion’ (Folkes v Chadd (1782) 3 Doug KB 157 24 ) but it was admitted because ‘[t]hat opinion, however, is deduced from facts’; ‘the whole case is a question of opinion, from facts agreed upon’.
But facts can change. John Maynard Keynes is widely credited with saying: ‘When the facts change, I change my mind. What do you do, sir? 25 ’ The earliest version is even more apposite: ‘The inactive investor who takes up an obstinate attitude about his holdings and refuses to change his opinion merely because facts and circumstances have changed is the one who in the long run comes to grievous loss’. 26
Mr Allard claimed damages for injuries allegedly caused by breathing in a noxious chemical at work (Allard v Govia Thameslink Railway Ltd [2024] EWHC 2227 (KB) 27 ). A respiratory medicine expert listened in court to evidence of fact as to the details of the incident. This did not affect his conclusion; the judge did not say he was obstinate, but he did ‘say at once that [he] found this somewhat surprising’. Despite there being no dispute between the experts as to the duration of exposure and the concentration of the vapour being highly influential to the probability of consequences, the expert did not re-evaluate his conclusions.
In Leonard v Leonard [2024] EWHC 321 (Ch), 28 a testamentary capacity case, a psychiatrist did not mention that he had heard some factual evidence whilst sitting in court, which undermined at least one of the opinions in his report. The judge said that he should have mentioned this when he first went into the witness box.
Language
A pain expert had to accept that he was ‘over-zealous in his use of language from the outset […] and when I re-read my reports […], I winced and thought I could have been a little bit more reflective and kinder’ (Palmer 31 ).
In Towuaghantse v General Medical Council [2021] EWHC 681 (Admin) 32 ) the judge commented that the expert's language was not the measured, temperate, moderate and balanced prose expected of an expert; rather, it was colourful, rhetorical, intemperate and unrestrained.
Late introduction of evidence
The overriding objective of the Civil Procedure Rules
33
(CPR) includes enabling the court to deal with cases justly (r 1.1(1)), which includes ‘ensuring that the parties are on an equal footing’ (r 1.1(2)(a)). That equal footing is disturbed when an expert introduces facts or opinions too late for the parties and other experts to consider them. As the judge said in Merck KGaA v Merck Sharp & Dohme LLC [2025] EWHC 2376 (Ch)
34
: Where there has been a lengthy expert report process […] the court is entitled to expect that the parties’ cases, on the issues considered by the experts, will be presented on the basis of the evidence that emerges through the expert report process […] [T]he joint meeting […] provides an opportunity for the experts to revise their opinions as appropriate, and the court expects the experts to engage properly and objectively with the evidence of the other side. If an expert fails to do so, but then changes their position on a particular point during the course of cross-examination, the court must then determine the case having regard to that change of position. The party relying on that expert cannot expect the court to allow it to attempt to salvage its position by advancing an entirely new case at that stage, on the basis of an analysis that has not previously been considered by either of the experts in their reports.
This happened in Stansfield v British Broadcasting Corporation [2021] EWHC 2638 (QB) 35 (Stansfield), where perhaps the most concerning aspect of an audio-vestibular expert's evidence was the introduction of a wholly new theory partway through cross-examination. Asked why he had not raised it in the joint statement, he sought to blame the other expert for not anticipating it. The judge said that he could not begin to explain the omission, and it was frankly not sensible to suggest it was for the other expert to anticipate a point he might later rely on rather than for him properly to deal with it in his written evidence and to raise it in the experts’ meeting.
In Scarcliffe v Brampton Valley Gp Ltd [2023] EWHC 1565 (KB), 36 the judge said that a pain expert's late evidence, devoid of any adequate analysis, represented an ‘elephant trap’ for an unwary judge.
Instructions and issues
In civil cases, expert reports must ‘contain a statement setting out the substance of all facts and instructions which are material to the opinions expressed in the report or upon which those opinions are based’. 37
When the North Yorkshire Clinical Commissioning Group applied for an order that it was in the best interests of a learning-disabled man to receive COVID-19 vaccinations, his brother applied to adduce the evidence of a physician (North Yorkshire Clinical Commissioning Group v E (Covid Vaccination) [2022] EWCOP 15 38 ) (North Yorkshire). One reason the court refused was because ‘he did not state what records or other documentation he had been provided with or the nature of his instructions’.
In an immigration and asylum case (BM (Iraq) [2024] UKAITUR UI2023005210) 39 ), the Upper Tribunal found that the expert's failure to provide clarity as to instructions impacted upon a clear understanding of the report; it said that there is an expectation that details of relevant instructions are provided.
Instructions to experts include issues. The obstetric expert in Woods v Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust [2024] EWHC 1432 (KB) 40 was described as having ‘a rather casual approach to the issues’. In another obstetric case, an expert failed to address adequately what was clearly the claimant's most important issue (Astley (A minor) v Lancashire Teaching Hospitals NHS Foundation Trust [2023] EWHC 1921 (KB) 41 ).
Procedural rules and guidance
The orthopaedic surgeon in Hamed 45 failed to comply with CPR r 35.10(3) 46 ('state the substance of all material instructions’), acted in contravention of CPR 35 PD 3.2(6) 47 (provide details of the range of opinion) and acted in contravention of CPR 35 PD 3.2(2) 48 (provide details of any literature relied upon), this only emerging in his oral testimony.
Failure to comply with CPR r 35.10 49 might lead to the evidence being ruled inadmissible or the court disregarding the evidence altogether. If admitted the court may have regard to the failures when deciding what weight to attach to the evidence.
Independence
CPR 35 PD 2.2 50 states: ‘Experts should assist the court by providing objective, unbiased opinions on matters within their expertise, and should not assume the role of an advocate’.
Evidence of partisanship may be recognised in an expert's oral testimony. An expert in neurological rehabilitation was described in MJF v University Hospitals Birmingham NHS Foundation Trust [2024] EWHC 3156 (KB) 51 as ‘demonstrably partisan’. The partisanship of the vascular surgeon in Beatty 52 was revealed when he referred to ‘cases I was involved in we didn't win’.
In HA, 53 the court noted correspondence between a psychiatrist and instructing solicitors where he referred to ‘tests for the client to fill out that were crucial […] to make our case’ and ‘vital for our case’.
Referencing
CPR 35 PD 3.2 requires the expert to ‘give details of any literature or other material which has been relied on in making the report’ and ‘[i]t is clear and well-established procedural law that experts provide a list of published literature’ (Saunders v Central Manchester University Hospitals NHS Foundation Trust [2018] EWHC 343 (QB)). 54
In a historical child sexual abuse case (F v Chalmers [2025] CSOH 23 55 ), the defender's experts relied on a follow-up study of sexually abused children. However, they had not cited it in their reports and so it had not been discussed with the pursuer's experts at the experts’ meeting. As it was not introduced in evidence until after one of the pursuer's experts had given their evidence, this left it to be considered by only one of the pursuer's experts.
Ivory, R (On the Application Of) v Welwyn Hatfield Borough Council [2025] EWCA Civ 21 56 was the judicial review of a local council's rejection of an application under the Housing Act 1996 by a tenant who, it was submitted, was suffering from a mental breakdown, severe depression and anxiety affecting her ability, and making it difficult for her, to pay rent arrears. As a result of the expert psychiatrist not giving details of the material relied upon in preparing their report, questions arose: ‘How was this provided to [the psychiatrist]? Were the relevant documents provided, or was this information provided anecdotally by Ms Ivory or other parties?’
Range of opinion
In the Covid vaccination case (North Yorkshire 58 ) the court found no hint that there might be a range of reasonable expert opinion and no recognition that there was any available evidence to support the contrary view that vaccination might be effective in preventing or reducing the symptoms caused by COVID-19, or that there might be medical opinion that vitamins are not effective in preventing the contraction of COVID-19, reducing the symptoms, or in preventing hospital admissions from COVID-19, for example.
A range of opinion that only emerges after an experts’ meeting, or which in oral testimony an expert refuses to acknowledge, can call into question the objectivity and independence of an expert.
The legal test(s)
An NHS Trust sought a third-party costs order against an expert witness, a spinal surgeon, who had been engaged as an expert by the claimant in clinical negligence proceedings. At trial, he was unable to articulate the applicable test in determining breach of duty in clinical negligence cases and the claimant's case failed (Thimmaya v Lancashire NHS Foundation Trust [2020] 1 WLUK 437 60 ). Had he understood and applied the legal test, it is probable that the case would not have gone to trial and the trust's expense defending it avoided.
Previous factual findings
Sometimes courts and tribunals make findings of fact before experts are instructed. In JMPS, 61 the psychiatrist's opinion that the appellant was suffering from depression and post-traumatic stress disorder (PTSD) was based on the appellant's claim that he had been tortured and detained. However, this had been rejected by a previous tribunal in 2013, as set out in documents provided to the psychiatrist. The diagnosis of PTSD, including reference to avoidance, flashbacks and nightmares, was significantly undermined by the events that these were said to refer to not having been found to have actually happened.
In care proceedings (Liverpool City Council v Ms A [2025] EWHC 1474 (Fam) 62 ), a clinical psychologist not only failed to consider the court's findings but challenged their validity, calling into question the soundness of the evidence on which they were based.
In The Secretary of State for the Home Department v CC [2025] UKAITUR UI2024005955, 63 the appellant had been convicted of a sexual offence committed in 2015 when aged 17 years. A psychiatrist's risk assessment was a central evidential plank of his case that he could rebut the presumption that he represented a danger to the community in the UK. The psychiatrist elicited this history: he met a female who allowed him to speak to her, he did not know how drunk she was, he took her to the bus stop to help her and he touched her face and breasts. He said that he should not have done it and it was his mistake. This contrasted with the summary of the offence in the tribunal's 2017 determination. The police were called to a female who was half-naked and stating that somebody had tried to rape her. She was crying and visibly shaken. Her top appeared to be ripped, and she was holding up her brassière with her hands. Also, in the 2017 determination, the appellant had been found to have been responsible for two further sexual attacks on female strangers around the time of the index offence. The psychiatrist concluded that the appellant's current and future risk of sexual offending was low and could safely be managed in the community.
The court found force in counsel's submission that the expert appeared to take on the role of advocate in critiquing the tribunal's previous determination that he presented a very high risk of re-offending as opposed objectively and impartially to taking this important previous judicial analysis into account. The case was remitted for rehearing, and consideration was to be given to the instruction of a different psychiatric expert.
Expertise
The spinal surgeon in Wilson 65 accepted stepping outside his area of expertise, being neither a pain expert nor a psychiatrist, and making a mistake in stating in the joint statement that, ‘if the Court accepts the findings and opinions of Dr Edwards then Mr Wilson's spasticity had a “non-organic (functional) element” which was ‘unrelated to the claim’.
In Rawson v TUI UK Ltd [2025] EWHC 2093 (KB), 66 the judge preferred the evidence of one gastroenterologist because the other had a tendency to express views on matters that were outside his expertise.
Another reason for not admitting the evidence of the physician in the COVID vaccination case (North Yorkshire 67 ) was that the physician did not have any specialisation in virology, epidemiology, or any other field of practice that would be recognised as relevant to the issues in the case. Having given vitamins to individuals did not make him an expert in the treatment of COVID-19. There was no analysis of that cohort of his patients and their health profiles, nor any comparison with patients who had not received vitamin treatments. He had not published any relevant research or papers related to COVID-19 in recognised medical or scientific publications.
In Duffy v McGee [2022] IECA 254, 68 a toxicologist ‘expressed a view (in trenchant terms) as to the cause of the plaintiffs’ respiratory inflammation’ which contradicted the views of the respiratory physician. For this and other reasons, the court referred to his ‘wholesale abdication’ by him of his duties as an expert witness.
Evidence that undermines opinion
In Thorvaldsen v Dundee City Council [2021] ScotCS CSOH 120, 70 the case of a teacher struck on the head by a wooden partition seeking to recover damages from his employer, the court noted that one expert seemed inexplicably to have ignored a particular entry in the general practitioner records which undermined her opinion.
It seemed to the judge in Stansfield 71 that the audio-vestibular expert simply rejected evidence that did not fit his opinion.
The issue in Lunt v BAC Impalloy Ltd [2025] EWCC 49 72 (Lunt) was whether, notwithstanding the claimant's use of vibrating tools in the employ of the defendant, he had hand-arm vibration syndrome. The evidence of the vascular surgeon called by the claimant was that he had its ‘typical symptoms in the form of tingling and numbness (sensory-neural symptoms) and blanching’. It was the defendant's case that he had carpal tunnel syndrome (CTS). The defendant called a hand surgeon who omitted, in his first report, to note that it is unusual for the little finger to show blanching in the presence of only CTS. He accepted, in answer to written questions from the claimant, that it was unusual with CTS for the little finger to show such clear-cut blanching as shown by Mr Lunt's photographs. The court found that this was a material fact which he should have mentioned in his first report and undermined the reliability of his opinion.
A forensic odontologist in R v Hedges [2025] EWCA Crim 1051 73 relied on a number of scientific reports, which, in his opinion, undermined the integrity and safety of bite mark evidence. However, he failed to refer to other publications which addressed concerns about those articles and studies. The court found this unfortunate and said that it is the duty of any expert to draw the court's attention to research which might contradict that used by the expert in forming his views.
Concessions
Making reasonable concessions is an indication of an expert's independence and objectivity and a recognition of their duty to the court rather than to their instructing party.
Willingness to make reasonable concessions distinguished the obstetric experts in Freeman v Pennine Acute Hospitals NHS Trust [2021] EWHC 3378 (QB). 74 The defendant's expert struck the judge as the more careful and balanced; he made concessions and admitted some points were neutral. This supported his fairness and balance. The claimant's expert seemed more reluctant to make even uncontroversial concessions and seemed more partisan. Moreover, the judge noted that he ignored a slight but important shift in the claimant's account.
Y v NHS Grampian (Court of Session) [2024] CSOH 72 75 (NHS Grampian) was the case of a child, her parents and her siblings who sought a declaration that in consequence of the actions of two paediatricians there had been a violation of their art. 8(1) right to respect for private and family life under the European Convention on Human Rights. The case centred on the paediatricians’ concerns that there might have been a degree of fabricated or induced illness in at least some of the child's presentations. The pursuers’ paediatric expert had not only not viewed the child's general practitioner records but was reluctant to concede that they could have contained any relevant information, when clearly they did.
In Price v Marston's PLC [2024] EWHC 1352 (KB), 76 the court concluded that an anaesthesia and intensive care expert had adopted a position and was not prepared to concede there was even a possibility of other conclusions being reached.
Guidelines
The paediatrician in NHS Grampian 78 had summarised guidance from the Royal College of Paediatrics and Child Health (RCPCH) on ‘Perplexing Presentations (PP)/Fabricated or Induced Illness (FII) in Children’. 79 As indicated, he had not viewed the child's general practitioner records. The RCPCH guidance stated that the health chronology should include information from primary care and that it was crucial to liaise with the general practitioner. He could not explain why this paragraph had not made it into his summary.
An issue in Thorp v Mehta [2024] EWHC 652 (KB) 80 was whether Amanda Thorp's death from a large intracranial and subarachnoid haemorrhage was caused by the negligence of general practitioners in not prescribing antihypertensive drugs. One expert failed from the outset to take into adequate account the NICE recommendations as a result of which his subsequent analysis became incoherent.
In Deakin-Stephenson v Behar [2024] EWHC 2338 (KB), 81 where the claimant had diverticulitis with a localised perforation, there was an issue as to when the claimant should have been advised that a Hartmann's procedure was a ‘safer and more definitive procedure’ than a laparoscopic lavage. The difficulty with the position of the claimant's colorectal expert was that he relied on guidelines published in 2020 and 2021, after the surgery in 2016. Given the divergence between the two experts, the court preferred the evidence of the defendant's colorectal surgeon as the claimant's expert relied on guidelines that were not in existence at the time of the case.
Criticising other experts
There was an absence of such respect in Lunt 83 ; the vascular surgeon was prepared to, and did, defer to the hand surgeon on matters within his expertise, but when giving oral evidence, the hand surgeon was not prepared to afford the vascular surgeon the same respect as regards her expertise with vascular conditions.
In an appeal against a murder conviction (R v Foy [2020] EWCA Crim 270 84 ), the court said that more disconcerting than the trenchant tones of a psychiatrist's written reports was how occasionally he made unwarranted criticisms of other experts: for example, in terms accusing another expert of not considering the appellant's progress in prison when he had in fact done so, causing that expert, not unreasonably, to refer in a later report to the expert's ‘haste to berate me’.
In Palmer, 85 the pain management expert made what the court considered an unfair attack on a neurology expert which. to his credit, he accepted, stating ‘This is my fault, I apologise to the Court’. But he further criticised the neurologist by stating that he ‘Opined that all of [the Claimant's] ongoing complaints were resultant from the brain injury’, which was incorrect and which he ought to have been aware of, as parts of the neurologist's report were joined into his own report. Again, he conceded an error and apologised to the court.
Dishonesty
The first of the ten key principles in Providing witness statements or expert evidence as part of legal proceedings 86 is: ‘You must act with integrity, honesty and objectivity, in whatever role you carry out in the legal process.’ This follows from Good Medical Practice which states: ‘You must be honest and trustworthy’ and specifically applies this to ‘giving evidence or acting as a witness’. 87
In her report for an employment tribunal, a medical expert reported that the employee had said certain things during her examination, which he had not said, reported that his speech was heavily peppered with expletives, which was untrue, and maintained at the hearing that the report was accurate, when she knew that it was not (McLennan v General Medical Council [2020] CSIH 12 88 ). She had also attributed direct quotations to him which she had known to be false. Evidence led by the respondents, which appears to have been based on a covert recording of the consultation, demonstrated that a significant proportion of what the expert had attributed to the employee in her report had not been said. Rejecting her appeal against erasure from the Medical Register, the court said that it was not possible to categorise the Medical Practitioners Tribunal (MPT) finding of dishonesty as plainly wrong in those circumstances.
The MPT ordered a 12-month suspension of a general practitioner who had provided a medical report containing false statements and a dishonest statement for use in personal injury litigation. Upon appeal by the GMC, the suspension was replaced with erasure (General Medical Council v Zafar [2020] EWHC 846 (Admin) 89 ).
A psychiatrist was found to have been dishonest in copying sections of another expert's report and submitting them as her own and in her evidence to the Crown Court confirming that she had assessed the subject of her report for one and a half hours when the evidence was that she had been on the ward for approximately 30 min. She unsuccessfully appealed against the MPT's erasure of her name from the Medical Register (Moodliar v General Medical Council [2025] EWHC 913 (Admin) 90 ).
Conclusion
Expert healthcare witnesses whose conduct results in judicial dissatisfaction or criticism appear to be unaware of, or to misunderstand, the duties of an expert witness or to act in disregard of them.
A companion paper considers the causes of, and remedies for, poor expert practice by healthcare professionals.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.