
Abstract
The transversus abdominis plane (TAP) block is an ultrasound guided regional anaesthetic technique used to provide analgesia to the abdominal wall. Research in humans and cats has demonstrated that TAP blocks reduce pain and post-operative opioid requirements after abdominal surgery. To date TAP blocks have not been described in rats. The optimal technique to employ when performing TAP blocks is controversial with single point injection techniques failing to reliably provide adequate coverage of the cranial abdominal wall. It has been suggested that performing a two point injection may provide more reliable coverage of the cranial abdominal wall.
The objective of this study was to determine the feasibility of performing ultrasound guided TAP blocks in rat cadavers and to evaluate whether performing a two point technique provides greater spread of injectate than a one point technique when administering the same total volume of methylene blue solution.
Twenty-three, four-month-old, female Sprague Dawley rat cadavers weighing 506 ± 78 g were used. TAP blocks were performed using a total of 1 ml/kg of methylene blue solution.
Overall success rates for injections were 21.7% (13.6–32.8%). Single point injection area of spread was 87.8 ± 32 mm2 compared with 102.4 ± 17 mm2 for the two point injection technique.
Due to the low success rate the use of TAP blocks using the current technique cannot be recommended. Two point injection technique appears to provide greater spread; however, additional data is required to draw meaningful conclusions.
Introduction
Acute pain has been shown to have a multitude of negative effects which may impair research outcomes as well as animal wellbeing. These negative effects may include impairment of sleep, decreased ability to perform physical tasks and an overall decrease in quality of life. 1 Pain also produces a stress response which may lead to multiple physiologic changes including tachycardia, increased oxygen consumption, tachypnoea, increased susceptibility to infection and hyperglycaemia as well as causing anxiety and depression. 2 Importantly, multiple studies have shown that increasing severity of pain increases the risk for development of chronic pain conditions.3,4
The question of which analgesics are most appropriate to employ for specific procedures and types of pain, as well as the optimal dose rate and frequency of drug administration in rats, remains open. A study assessing the use of analgesics in research rodents reported worrying rates of analgesic use, with 46% of rats undergoing painful surgical procedures not reported as receiving analgesic agents, while only 21% of rats were recorded as receiving analgesics that were not administered for sedative or anaesthetic purposes. 5 In addition to these findings, this paper reported that out of 172 papers describing painful surgical interventions, none reported the use of multimodal analgesic techniques, and no articles described the use of targeted regional analgesic techniques. 5 Both of these techniques are considered standard practice in current clinical veterinary medicine. 6
Materials and methods
Ethical approval was obtained from the University of Edinburgh Veterinary Ethics Committee (VERC 59.20) following development of the protocol. Cadaveric studies using other species were used to determine sample sizes.7–9 Twenty-three freshly frozen, four-month-old, entire female rat cadavers weighing approximately 500 g were obtained after being euthanized as part of a different research protocol, AEC:1852. Rat cadavers were thawed at room temperature for a minimum of 24 h prior to use. None of the selected animals had undergone interventions affecting the abdomen prior to enrolment in this study. All imaging and injections were performed by a single investigator trained and experienced in ultrasound guided local anaesthetic techniques. Animals were weighed and marked for identification prior to any interventions. Animals were then placed in dorsal recumbency and the abdomen shaved from the level of the last rib to the pubis. A random number generator (www.random.org, Dublin, Ireland) was used to determine the side of the abdomen to be injected first. The first injection performed was always a single point block; this was followed by the two point block on the contralateral side.
A 15–8 MHz linear ultrasound transducer attached to an ultrasound machine (Sonosite, Fujifilm, WA, USA) was placed in a transverse orientation approximately mid-way between the last rib and the level of the wing of the ileum (Figure 1). The ultrasound image was optimized by using the zoom-in function, and the three layers of the abdominal wall were visualized and identified from outer to inner layers as the external abdominal oblique, internal abdominal oblique and the transversus abdominis muscle (Figure 2). A 22G, 2.5 inch spinal needle (BD Medical, Australia) was inserted using an in-plane technique until the needle tip could be visualized at the level of the fascial plane between the internal abdominal oblique and the transversus abdominis muscle. A small test dose of approximately 0.05–0.1 ml methylene blue solution was then injected to confirm placement. If the injection was found to be in the incorrect area the needle was readjusted prior to administering another small test dose. The remainder of the volume was then administered for a total of 1 ml/kg once the needle was visualized as being in the correct place (Figure 3). The ultrasound probe was then placed on the opposite side of the abdomen just below the level of the last rib and then just cranial to the hip and the procedure was repeated for the two point block, injecting 0.5 ml/kg total per injection site (1 ml/kg total volume).

Rat cadaver placed in dorsal recumbency. The line on the left of the image shows the injection site for the one point transversus abdominis plane (TAP) block. The two lines on the right show the cranial and caudal injection sites for two point TAP blocks.
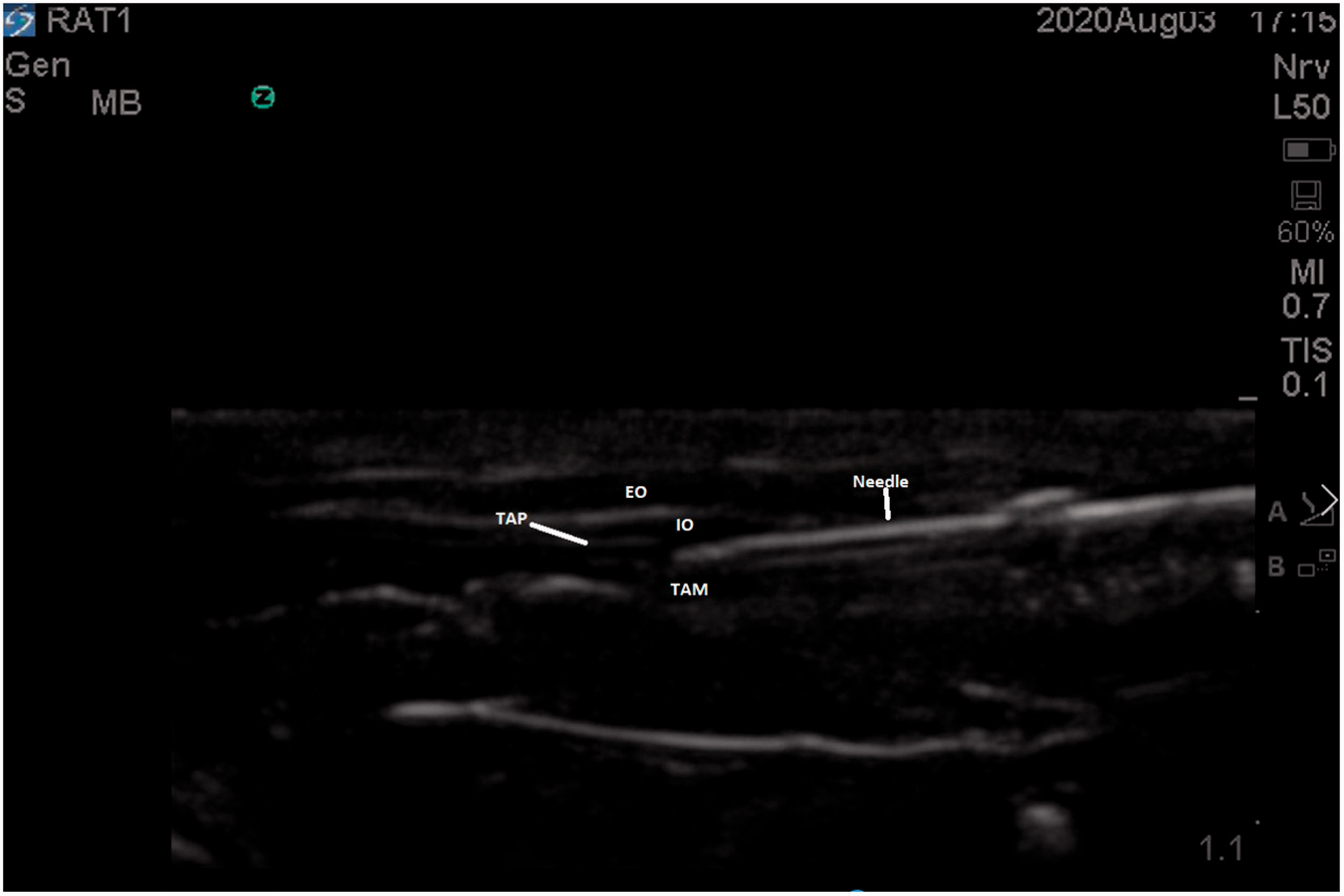
Ultrasound image of a rat cadaver abdomen with the left of the image located towards the midline of the abdomen and the right of the image the lateral aspect of the abdomen. The needle is inserted from the lateral aspect and positioned at the level of the TAP. The top of the image represents the skin surface.
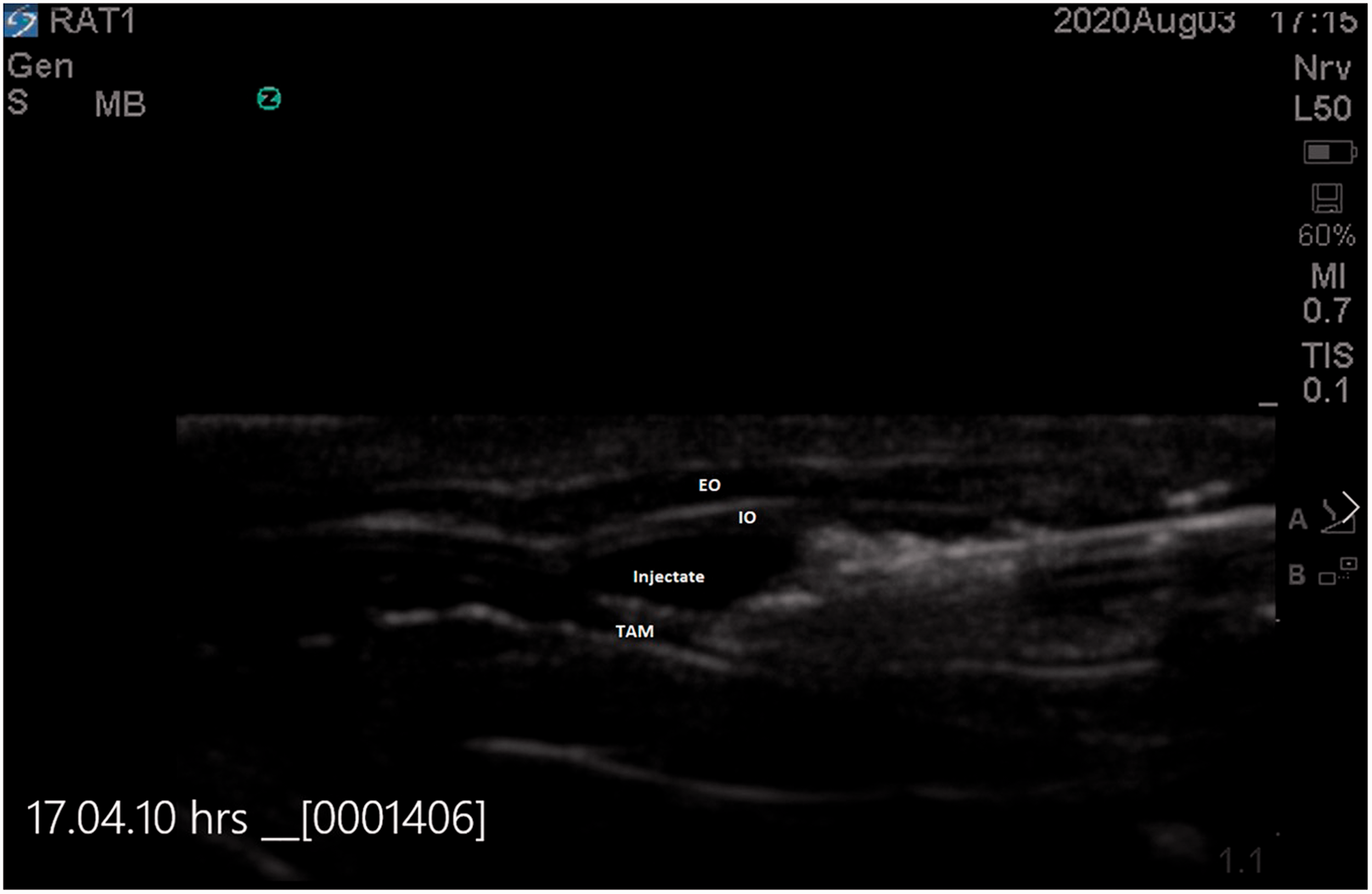
Ultrasound image of successful TAP block. Note the ventral displacement of the external oblique (EO) & internal oblique (IO) and dorsal displacement of the transversus abdominis muscle (TAM) caused by the injectate which appears as a hypoechoic area not present on the previous image (Figure 2).
Dissection was performed between five and 15 min following all injections. A midline incision was made using a number 11 scalpel blade and the three muscle layers were inspected to determine the location of injection (Figure 4). The abdomen was then explored for evidence of intra-abdominal injection. Photos of the spread of injectate were taken against a 30 cm ruler to provide scale for further evaluation using imaging software to determine the size of the area of spread. Images of all injection sites were analysed using ImageJ® software (National Institutes of Health, WI, USA) to measure the visible area of spread for each block and the area of injectate spread was calculated in mm2.
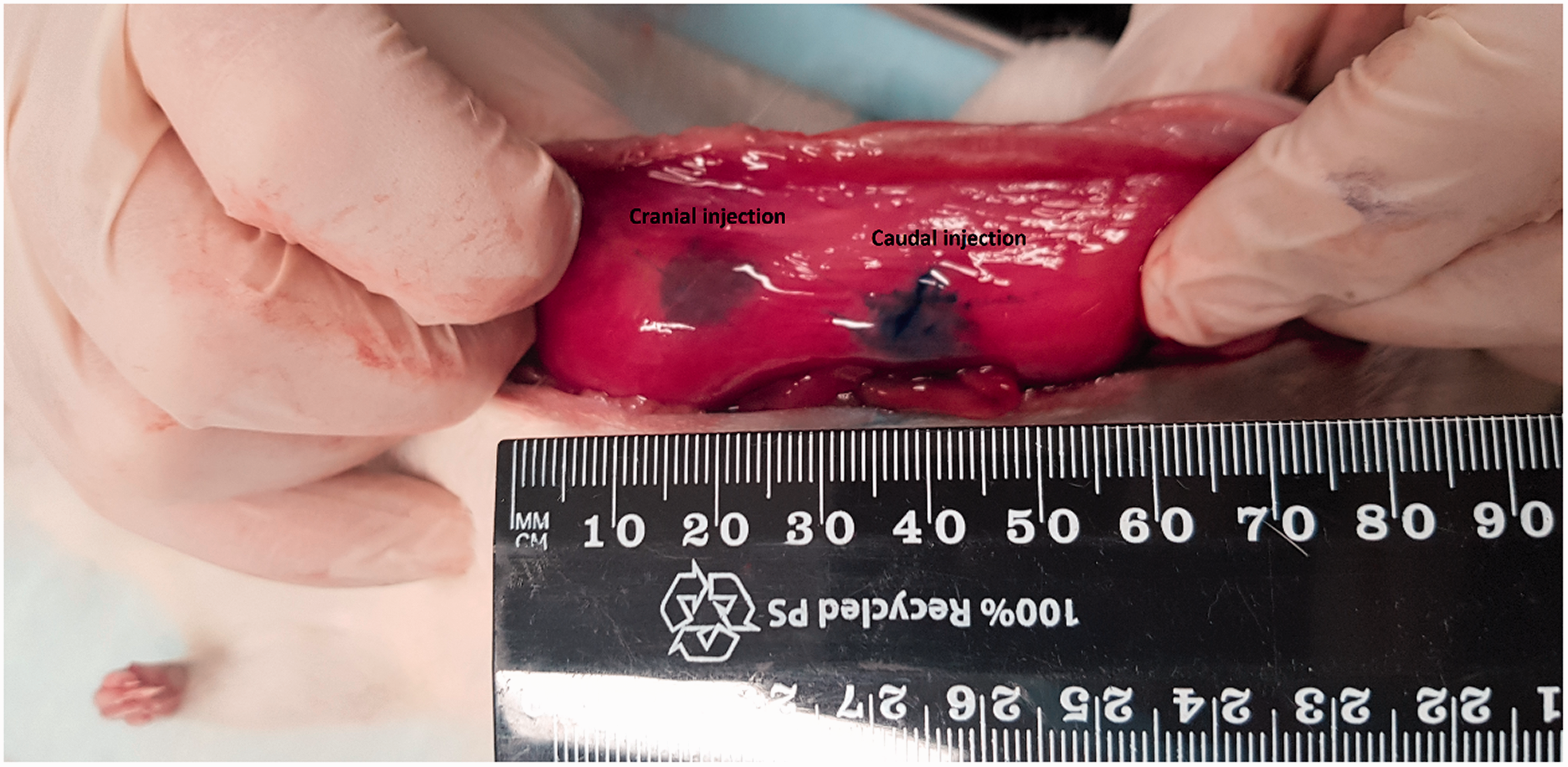
Photo of dissected rat cadaver abdominal wall following two point transversus abdominis plane block.
Comparison of results for one point and two point techniques.

aPer injection refers to a single needle insertion.
Data was entered into Microsoft Excel® and tidied. Descriptive statistics including mean and standard deviation were calculated for age and weight. Mean, standard deviation and 95% confidence intervals were calculated for spread of injectate. Success rates with 95% confidence intervals were calculated for each injection technique. The location of injectate was recorded and calculated as an overall percentage of all injections to determine the number of successful injections as well as the number of injections made intramuscularly or intraperitoneally. Success rates were then calculated for the first 15 injections and compared with the subsequent injections to identify whether a learning curve affected overall success rates. Based on these results a power calculation was performed to determine the additional number of successful injections that would be required to provide statistically significant results.
Continuous data is presented as mean ± SD, proportions are presented in percentage (95% confidence interval).
Results
Mean and standard deviation weight for the rat cadavers used in the study was 506 ± 78 g.
The three layers of the abdominal wall were able to be visualized and the transversus abdominis plane (TAP) identified in all 23 cadavers. Overall, five out of 23 single point injections, five out of 23 cranial two point injections and five out of 23 caudal two point injections were successfully injected into the correct fascial plane, accounting for a 21.7% (13.6–32.8%) success rate for all injection attempts. The success rate for right sided versus left sided injections was similar, with 8/69 (11.6% (5.9–21.2%)) successful injections on the right side and 7/69 (10.1% (5.0–19.5%)) injections on the left side of the abdomen. Injection success rate for the first 15 injections was 20.3% (12.5–31.2%) while the following 15 injections recorded a success rate of 13.0% (7.0–23.0%).
Location of injectate was recorded for each injection with 21.7% (13.6–32.8%) of injections being deposited purely into the TAP, 21.7% (13.6–32.8%) being observed in both the TAP and muscle, 27.5% (18.4–39.0%) of injections being deposited into the abdominal cavity, 2.9% (0.8–9.9%) being deposited into muscle and the abdominal cavity and 26.1% (17.2–37.5%) injected into muscle. Injectate could not be located in 1.4% (0.3–7.8%) of injections.
The spread of injectate for the successful one point blocks was 87.8 ± 32.7 mm2 while the spread for the successful two point blocks was 102.4 ± 17.6 mm2. These results are summarised in Table 1. Based on these results a power calculation was performed which revealed that a further 14 rats with all injections performed being successful would be required to generate statistically significant results.
Discussion
The aim of this study was to investigate the viability of performing TAP blocks in rat cadavers, while also evaluating the hypothesis that performing two point injection techniques would provide a greater area of injectate spread than one point injection techniques. In the present study only 21.7% of injections were successful. Two point injection techniques demonstrated a greater area of spread than one point techniques, 102.4 ± 17.6 mm2 and 87.8 ± 32.7 mm2 respectively, with more successful injections required to gain statistically significant results.
Cadaveric studies in veterinary species have shown particularly promising results, with TAP injections generally being successful in close to 100% of attempts.7–9 One paper, however, reported significantly lower success rates, with 73% of injections deposited purely into the TAP, 23% combined intramuscular and TAP injections and intraperitoneal injections in 4% of cases. 10 These results may be explained by the relative inexperience of the investigator performing the technique, who was a resident in training.
In contrast to this, results from our study have demonstrated significantly greater failure rates with only 21.7% of injections successfully injecting dye into the TAP, 23% injected into both the muscle and the TAP, and 31% of injections being deposited intraperitoneally.
Multiple factors may have combined in our study to reduce the success rate in these rats.
In this study all injections were performed by one investigator. While it is possible that the low success rate may be attributable to the person performing the injections, it is unlikely that this is the case. The investigator chosen to perform the technique for this study has received formal training in ultrasound guided regional anaesthetic techniques and has been successfully performing this technique in clinical small animal cases for several years. Despite this, performing injections in significantly smaller animals undoubtedly involves a learning curve as the smaller anatomy is adjusted to and any necessary adjustments in technique are developed.
Learning curves for ultrasound guided blocks have been reported as being particularly steep, with the curve for residents learning to perform brachial plexus nerve blocks plateauing after 10 to 15 attempts. 11 Therefore, it may be assumed that the presence of a learning curve in this study may have negatively affected the results. The effect of this learning curve, however, appears to be insignificant in this case, as the recorded success rate was similar between the first and second group of 15 injections.
The rats’ small size in this study may have served to make identification of important landmarks and the TAP itself more difficult. However, using this ultrasound probe and the zoom-in function, the three muscle layers and the TAP were adequately visualized in all cases. While the operator rated all images as adequate for injection it is possible that the use of a higher frequency probe, and the higher resolution picture provided by this probe, may have aided in the identification and guidance of the needle, which may have improved the overall success rate.
It is likely that the small size of the TAP in these rats, approximately 0.5 mm, and the needles used to perform the injections have contributed to the low success rate. In this study the instance of combined TAP and intramuscular injection, that is, injectate observed both in the TAP and intramuscularly after a single injection, was 27.5%. This is likely due to the relatively large bevel of commonly used needles when compared with the size of the TAP space in rats. Considering this, it appears likely that even successful injections may deposit some of the injectate intramuscularly, making it harder to predict the total amount of injectate delivered into the TAP space. This may cause more variability in spread of injectate in this model as the actual amount injected into the TAP is likely to vary between animals. The availability of specifically designed needles with smaller bevel lengths may be required to approach success rates reported in other species.
The use of Tuohy needles has been previously described in successful TAP blocks in two chinchillas. 12 In this report, with the animals in lateral recumbency and a 18 MHz linear ultrasound probe used to visualize the three abdominal muscle layers, a 22G Tuohy needle was then used to perform the injections. Tuohy needles were originally designed in 1945 for use in epidural anaesthesia. Like Quinke needles, these needles have a relatively long bevel compared with the TAP width in rats. However, unlike Quinke needles they have a curved, blunt tip that ends with the needle orifice. Originally designed to minimize the risk of dural puncture, these needles provide more tactile feedback when passing through tissue planes. 13 In addition to this, the shaft is marked in centimetre gradients, which, combined with ultrasound depth markings, may help users to confirm they are at the desired depth prior to performing injections. The blunt curved tip combined with the centimetre markings may make it a suitable option for this technique as the curved tip may be more likely to remain entirely within the TAP in rats. Additionally, the extra level of tactile feedback provided by the needle may help the user identify when they are passing through the different muscle planes as has been described in the original landmark based injection studies performed in humans. 14
As mentioned previously, veterinary cadaveric studies have reported success rates which mostly approach 100%. While this study demonstrated significantly lower success rates, more worrying is the number of injections that resulted in injectate entering the abdominal cavity. In this study 31% of injections had injectate noted in the abdominal cavity on inspection compared with other veterinary cadaveric studies in which the presence of injectate in the abdomen following injection is generally a rare occurrence.
To date complications from TAP blocks have not been reported in the veterinary literature. In the human literature, trauma of the liver with associated minor haemorrhage has been reported when using only anatomical landmarks, 15 while liver laceration and subsequent septic peritonitis requiring blood transfusion has been reported when performing ultrasound guided TAP blocks. 16 Considering the small size of rats and the ease with which they may be moved while performing injections, coupled with multiple injection locations required for the two point TAP block, it is feasible that trauma to a range of abdominal organs may be possible with this technique. Associated complications, as in the human literature, may have minor to major consequences for the animal. Considering the high rate of intraabdominal and intramuscular injection the risk of complications using this technique in rats is likely to be significantly higher than has been reported in the human literature.
These findings may be particularly relevant to other small animals, such as chinchillas, that have been reported as receiving TAP blocks as part of their clinical treatment. While successful injection was noted on ultrasound evaluation in these cases, thorough intraabdominal evaluation was not performed. The possibility that at least partial peritoneal puncture may have occurred, as in our study, should be considered. Considering the large percentage of animals in this study that received intramuscular or intraperitoneal injections, it would be highly recommendable to perform cadaveric studies on these animals to assess for potential complications.
Unfortunately, in this study there were not enough successful injections to allow investigators to draw any conclusions as to whether two point injections provide greater spread of injectate than one point injections when delivering a total volume of 1 ml/kg. Our results showed that the two successful two point injections appeared to provide a greater area of spread than the successful one point injections, which is in agreement with other preliminary studies.7,17 However, a power calculation following these results showed that another 14 rats with completely successful injections would be required to corroborate statistically this difference. When considering whether a one or two point injection is required for abdominal surgery it is important to consider the area undergoing surgical manipulation. For animals undergoing laparotomy for ovariohysterectomy a single point injection technique may be adequate as the area being surgically manipulated is relatively small. This hypothesis is supported by the study performed by Skouropoulou et al., 18 which demonstrated the efficacy of single point TAP blocks as part of a multimodal analgesic protocol for post-operative pain control in cats undergoing ovariohysterectomy.
This study has multiple limitations. The use of defrosted cadavers may not accurately recreate interactions with live tissues, which may alter the spread of the methylene blue solution used. 9 Additionally, the use of methylene blue solution has been shown to provide greater spread when injected in cadaveric TAP block models than mixtures containing methylene blue and bupivacaine. 19 This may lead to a larger area of spread than may be expected clinically using common local anaesthetic drugs. The use of defrosted cadavers may also affect image quality, which, due to the small size of the animals being used, may be particularly significant in this study. 20
In the current study, 5–15 min was allowed between injection of methylene blue and dissection of cadavers for evaluation of spread of injectate. This may have led to differences in spread between subjects as some cadavers may have had significantly more time for the injectate to spread compared with others. In addition to this, work with human cadavers has demonstrated that methylene blue injectate does not reach the peak of spread for 40 min or longer post injection when performing TAP blocks, further supporting the possibility that spread may be artificially decreased In this study. 21 Finally, while the success rate in this study was very low, it is possible that having an investigator who is very experienced in this technique in cats and dogs may have artificially inflated the success rate. It is reasonable to expect that success rates may be lower when this technique is being performed by non-experts.
Conclusion
The use of TAP blocks in rats using this technique cannot currently be recommended due to an unacceptably low success rate and the potential risk of complications associated with the high number of intraabdominal injections. Due to this low success rate, conclusions cannot be drawn regarding the hypothesis that two point injection techniques will provide superior spread of injectate when compared with one point injections techniques when using the same total volume of injectate. Further research should be conducted with the aim of increasing success rates.
Footnotes
Data availability
Study data is available via the corresponding author if requested via email:
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.